Dermatology · Medicine
Stevens-Johnson syndrome and toxic epidermal necrolysis
Also known as Stevens-Johnson syndrome · SJS · Toxic epidermal necrolysis · TEN · SJS-TEN overlap · Epidermal necrolysis
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are a spectrum of life-threatening immune-mediated severe cutaneous adverse reactions (SCAR), characterised by widespread keratinocyte apoptosis producing epidermal detachment and mucosal erosions, most commonly triggered by drugs (allopurinol, anticonvulsants, sulfonamides, nevirapine, oxicam NSAIDs). Classified by percentage of body surface area (BSA) detached: SJS under 10%, SJS-TEN overlap 10 to 30%, TEN over 30%. Mortality is estimated using the SCORTEN score (calculated at 24h and 72h). Management is a dermatological emergency: immediate withdrawal of all drugs, transfer to ICU or burns unit, supportive care (modified Parkland fluid resuscitation, nutrition, wound care, infection surveillance), urgent mucosal care (ophthalmology within 24h, amniotic membrane for severe eyes), and controversial immunomodulation (IVIG, ciclosporin, etanercept). Fellowship-level assessment demands mastery of the SJS-TEN spectrum, the granulysin-dominant pathogenesis, the HLA associations (HLA-B1502 carbamazepine in Asians; HLA-B5801 allopurinol; HLA-A*3101 carbamazepine in Europeans), SCORTEN components and mortality strata, the differential from SSSS, pemphigus vulgaris, DRESS, AGEP and EM major, the modified fluid regimen that is NOT the same as burns, and the controversies of specific therapy.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Overview & Definition
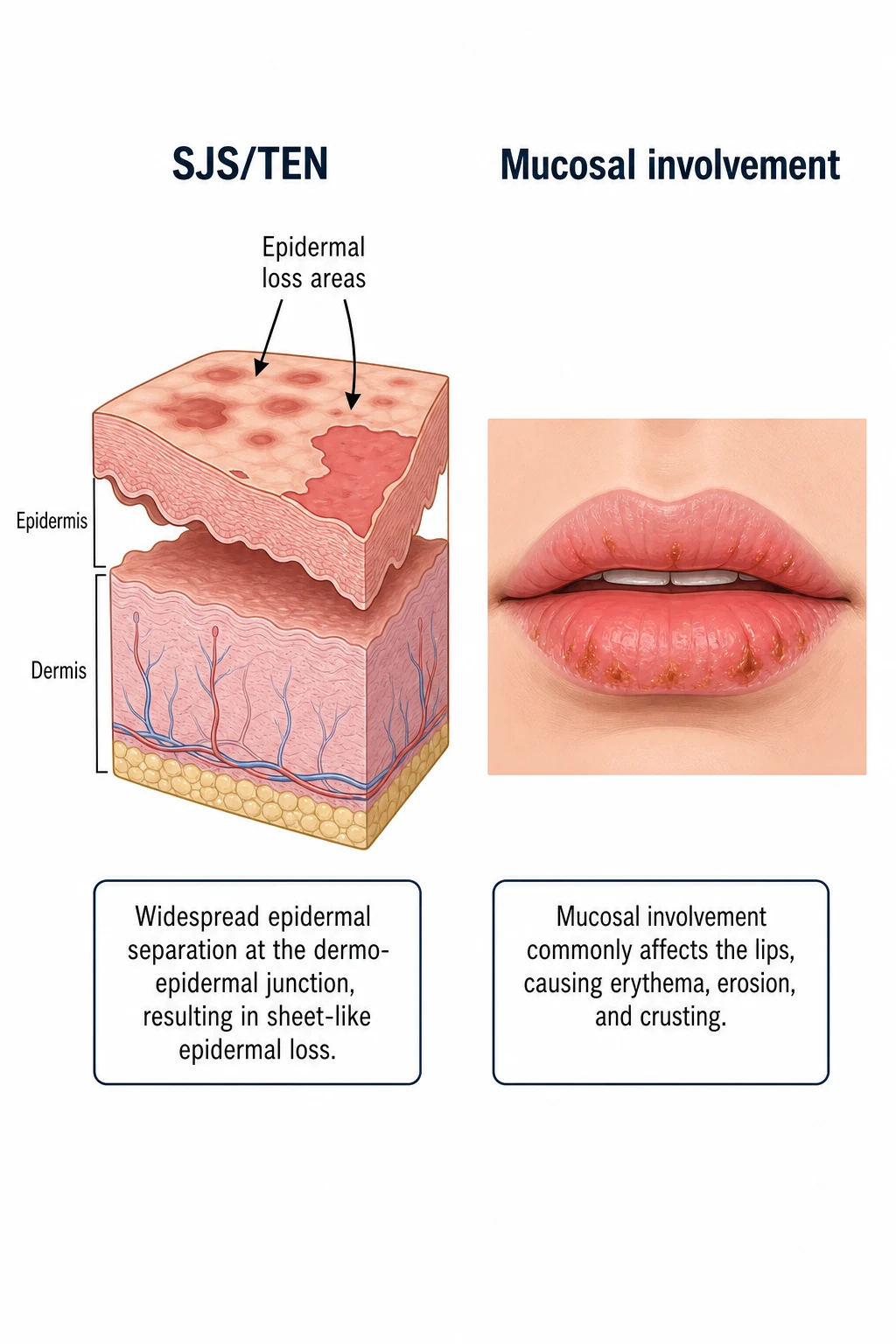
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) form one end of the acute severe cutaneous adverse reaction (SCAR) spectrum — a dermatological and medical emergency in which disseminated keratinocyte apoptosis strips the epidermis from the dermis over large body areas, producing a clinical picture that behaves like a severe burn. The hallmark is full-thickness (confluent) epidermal necrosis with sheet-like detachment, accompanied by mucosal ulceration of at least two sites and systemic toxicity.[1][2][4][10]
The two non-negotiable principles frame everything that follows. First, immediately stop every potentially causative drug — this is the single most important intervention in SJS/TEN and the only action that has never been controversial. Every day a causative drug is continued adds to the keratinocyte death toll. Second, recognise the disease early and transfer to a burns unit or intensive care when detachment exceeds 10 percent of body surface area; the level of supportive care, the ophthalmology input, and the infection surveillance are what determine survival, more than any specific immunomodulator. Ophthalmology from day one prevents the irreversible corneal scarring that is the most feared long-term complication of survivors.[9][10]
Classification
The classification is the Bastuji-Garin consensus spectrum, which arranges SJS and TEN on a single continuum defined by the percentage of BSA showing epidermal detachment. The spectrum replaced the older, confused separation of erythema multiforme major from SJS, and it carries prognostic weight: mortality climbs as detachment increases.[1][2]
Distinguishing SJS from erythema multiforme
A favourite examiner trap. Erythema multiforme (EM) is, despite the name, a separate disease now reclassified away from SJS. Classic EM minor has typical three-zone target lesions (a dusky centre, a pale oedematous ring, and an outer red ring), is usually triggered by herpes simplex virus, has minimal or no mucosal involvement, and runs a benign, relapsing course. EM major has typical targets plus mucosal involvement, often from HSV or Mycoplasma, but the lesions are true raised targets rather than the flat, purpuric, atypical targets of SJS, and there is no sheet-like epidermal necrosis. SJS/TEN, by contrast, is overwhelmingly drug-induced, has atypical (flat, two-zone, purpuric) target lesions, prominent mucosal involvement of at least two sites, and full-thickness epidermal necrosis with positive Nikolsky sign.[2][4]
Epidemiology & Risk Factors
SJS and TEN are rare. The combined annual incidence is approximately 1 to 2 per million population per year for SJS and 0.4 to 1.2 per million per year for TEN, with overlap cases sitting between; the German national registry, the largest population-based dataset, reports figures in this range.[3] Although rare, the disease is medically catastrophic when it occurs: case fatality is high, recovery is prolonged, and survivors carry lifelong sequelae.
Risk is concentrated in several groups. Slow acetylators, patients with HIV (a thousand-fold increased risk of sulfonamide reactions and a marked risk from nevirapine), patients with systemic lupus erythematosus, those with active malignancy or on chemotherapy, the elderly, and patients with renal or hepatic impairment all carry higher risk, the last because impaired drug clearance prolongs the window of immune exposure. Active cancer is also one of the SCORTEN variables. Critically, specific HLA alleles confer a very high genetic risk in particular populations, which is why pharmacogenomic screening before certain drugs is now a global guideline.[2][6][7]
Causative Drugs
The commonest culprit drug classes (the "ALDO-CANN-S" mnemonic) are worth memorising for exams:[2][4][6][7]
- Allopurinol — the single commonest drug cause worldwide; risk higher with renal impairment and high starting dose
- Lamotrigine, carbamazepine, phenytoin, phenobarbital — aromatic anticonvulsants; rapid titration increases risk
- Dapsone, sulfonamides (cotrimoxazole, sulfasalazine), oxicam NSAIDs (piroxicam, meloxicam)
- Oxicam NSAIDs
- Cotrimoxazole
- All the above + nevirapine, anti-TNF agents, immune checkpoint inhibitors
- Nevirapine — especially in HIV (first 6 weeks of therapy)
- NSAIDs (oxicam family)
- Sulfa drugs [1]
Drug latency is typically 1 to 8 weeks after drug initiation; recurrence on re-challenge is rapid (hours to days).[2][4]
Infection triggers (less common, mainly in children): Mycoplasma pneumoniae (SJS-like, sometimes called Mycoplasma-induced rash and mucositis or MIRM, now subsumed under reactive infectious mucocutaneous eruption, RIME), and Herpes simplex virus (erythema multiforme major — a distinct entity).[2][10]
Pathophysiology
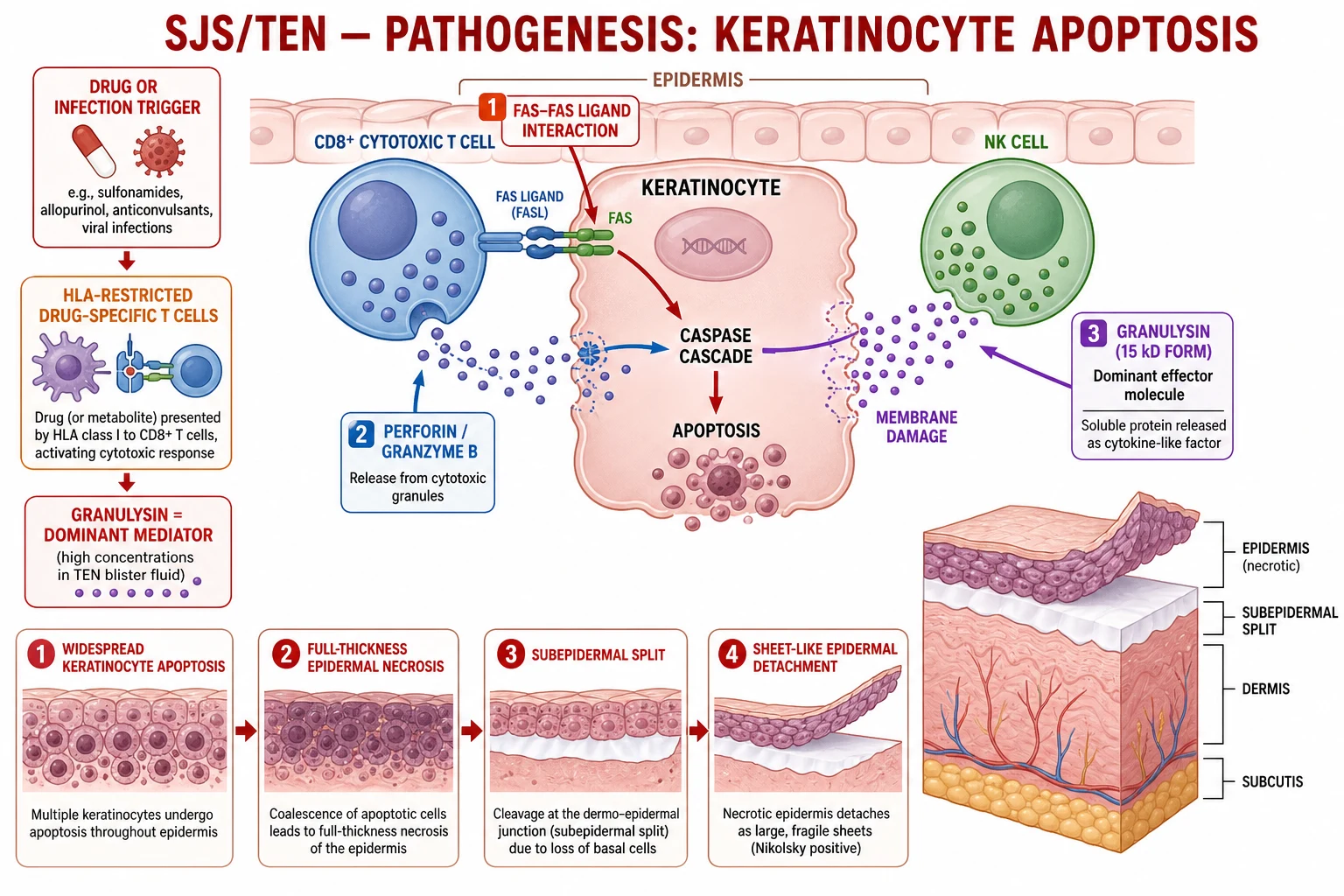
SJS/TEN is a type IV (delayed) hypersensitivity reaction mediated by drug-specific CD8-positive cytotoxic T lymphocytes that home to the epidermis and kill keratinocytes in a disseminated, confluent pattern. The offending drug (or its reactive metabolite) is presented by HLA class I molecules on the keratinocyte surface; the drug-specific T cell recognises the complex and unleashes its cytotoxic cargo, producing widespread keratinocyte apoptosis that within hours becomes visible as full-thickness epidermal necrosis.[5][10]
Four cytotoxic pathways converge on the keratinocyte, and the relative contribution of each is a high-yield viva topic. The dominant mediator is granulysin, a cationic cytolytic protein released by the cytotoxic T cell and natural killer cells. Chung and colleagues showed that granulysin is present in SJS/TEN blister fluid at concentrations two to four orders of magnitude higher than perforin or granzyme B, and that injecting recombinant 15-kDa granulysin into mouse skin reproduces the epidermal necrosis — establishing it as the principal effector of disseminated keratinocyte death in the disease.[5] The other three pathways are perforin-granzyme B (T cell releases perforin pores and granzyme B, which activates caspases), the Fas-FasL death-receptor pathway (drug-induced soluble Fas ligand engages Fas on the keratinocyte), and TNF-alpha (amplifies the apoptotic signal and recruits additional effectors).[5][10]
The four keratinocyte-killing pathways — and the one that dominates
GRAPE
The genetic susceptibility is now understood at a molecular level. The drug-HLA binding is not a uniform process: certain HLA alleles present the offending drug to the T-cell receptor with far greater efficiency. HLA-B1502 presents carbamazepine (and structurally related aromatic anticonvulsants) to cytotoxic T cells in Han Chinese and South-East Asians, which is why carbamazepine-induced SJS is so concentrated in these populations (odds ratio over 1000 in some cohorts).[6] HLA-B5801 presents allopurinol and its long-lived metabolite oxypurinol, explaining the strong allopurinol-SJS signal in Han Chinese, Thai and Korean patients (odds ratio over 500 in the original Hung 2005 paper).[7] In Europeans and Japanese, the carbamazepine signal is carried by a different allele, HLA-A*3101, which is the basis of the European Medicines Agency and Japanese screening recommendation. These are not merely associations — the peptide-binding groove of the specific HLA molecule physically accommodates the drug, which is the structural basis of the clinical signal.[6][7][10]
Clinical Presentation
The clinical course unfolds in two phases. Phase 1 is the prodrome, lasting one to three days: the patient is systemically unwell with high fever, malaise, arthralgia, upper-respiratory-tract symptoms and a burning, stinging sensation of the skin and eyes. The prodrome is easily misread as a viral illness, and the skin pain that precedes any visible rash is a cardinal clue. Phase 2 is the eruptive phase: dusky, purpuric atypical target lesions (flat, two-zone, dark-centred macules with a red halo) appear first on the trunk and proximal limbs, then coalesce. Within hours to a day, flaccid, easily ruptured bullae form over the dusky macules, and lateral pressure shears the epidermis off in sheets — the positive Nikolsky sign.[2][4]
The Nikolsky sign — the bedside manoeuvre that anchors the diagnosis
Nikolsky sign is the clinico-pathological correlate of full-thickness epidermal necrosis. The direct (lateral) Nikolsky: apply firm, sliding (lateral) pressure with a thumb to unblistered, apparently normal skin adjacent to a lesion; a positive sign is when the epidermis shears off, leaving a moist glistening base. The indirect (Asboe-Hansen) Nikolsky: apply vertical downward pressure to the roof of an intact blister; a positive sign is when the blister extends sideways into adjacent unblistered skin. A positive Nikolsky sign indicates that the entire epidermis is necrotic and loose — the histology of TEN. It is also positive in pemphigus vulgaris and SSSS, which is why the sign confirms "epidermolysis" but not the cause; the mucosal involvement, drug history and biopsy settle the differential.[2][4][10]
Mucosal involvement is the rule rather than the exception, occurring in over 90 percent of cases and involving at least two sites. The oral mucosa (lips, buccal mucosa, tongue) is involved earliest and most often, with painful haemorrhagic crusting of the lips that is almost pathognomonic. Ocular involvement (conjunctivitis, photophobia, purulent discharge, corneal epithelial sloughing) is the single most important site to manage aggressively because it determines long-term vision. Genital and urethral mucositis cause dysuria and may produce urinary retention, while tracheobronchial and oesophageal involvement predict respiratory and feeding compromise. Unlike staphylococcal scalded skin syndrome (SSSS), which spares mucosae, SJS/TEN always involves mucous membranes in over 90 percent of cases.[2][9]
What gives a positive Nikolsky sign? — the NIPLS list
NIPLS
Acute and late ocular involvement
Acute ocular SJS/TEN is graded by the Singh classification (mild conjunctival hyperaemia to severe pseudomembrane formation, corneal epithelial defect and limbal ischaemia). Even with optimal care, late ocular sequelae affect up to a third to a half of survivors: dry eye disease, symblepharon (adhesion of palpebral and bulbar conjunctiva), fornix shortening, trichiasis, entropion, corneal scarring, corneal opacification and, in the worst cases, blindness. The bundle that prevents these is well-defined: daily ophthalmology from day one, preservative-free lubricants hourly, topical antibiotics (chloramphenicol or ofloxacin), topical corticosteroids (prednisolone 0.5 percent), symblepharon lysis with a glass rod, and early amniotic membrane transplantation for severe involvement.[9]
Differential Diagnosis
The differential of an acute blistering or skin-sloughing rash with mucositis is short but the stakes are high, because the management of each diverges.[2][4][10]
Two rarer but important mimics to remember: paraneoplastic pemphigus (mucous membrane pemphigoid with underlying lymphoma, Castleman disease or thymoma — DIF positive, painful stomatitis and polymorphic skin lesions) and acute graft-versus-host disease (in bone-marrow transplant recipients; histology indistinguishable from SJS/TEN in some cases, donor T-cell mediated). The clinician who sees a bone-marrow recipient with sheet-like desquamation must consider both. Acute haemorrhagic necrotising encephalopathy is a separate neurological mimic that occasionally co-presents with severe mucocutaneous drug reactions but is a distinct entity.[2][4][10]
Clinical & Bedside Assessment
The bedside assessment has three aims: confirm the diagnosis clinically, quantify the percentage of BSA detached (which determines classification and the level of care), and screen for the complications that kill (sepsis, fluid loss, ocular damage, airway involvement). Begin with the drug history, which is the cornerstone — list every drug taken in the preceding eight weeks, paying particular attention to allopurinol, anticonvulsants, sulphonamides, oxicam NSAIDs, nevirapine and anti-TNF agents. The single most common mistake is stopping only the most recently started drug; the causative agent may have been started weeks earlier, so all drugs within the window must be reviewed.[2][4]
To estimate BSA detached, use the rule of nines as in burns (head and neck 9 percent, each arm 9 percent, each leg 18 percent, anterior trunk 18 percent, posterior trunk 18 percent, perineum 1 percent), or the palmar method (the patient's palm including fingers is approximately 1 percent BSA) for small scattered patches. Examine every mucosal surface — lips, oropharynx, conjunctivae, genitalia, urethra — and document ophthalmological findings (hyperaemia, pseudomembrane, corneal erosion). Look for signs of respiratory (cough, hypoxia, bronchial sloughing) and genitourinary (dysuria, retention) involvement. Calculate SCORTEN at admission and again at 72 hours, since the 72-hour score is more predictive.[1]
Investigations
SJS/TEN is fundamentally a clinical diagnosis, but investigations confirm the diagnosis, grade severity, and guide supportive care. There is no single blood test that diagnoses SJS/TEN; the skin biopsy is the confirmatory test.[2][4]
Skin biopsy
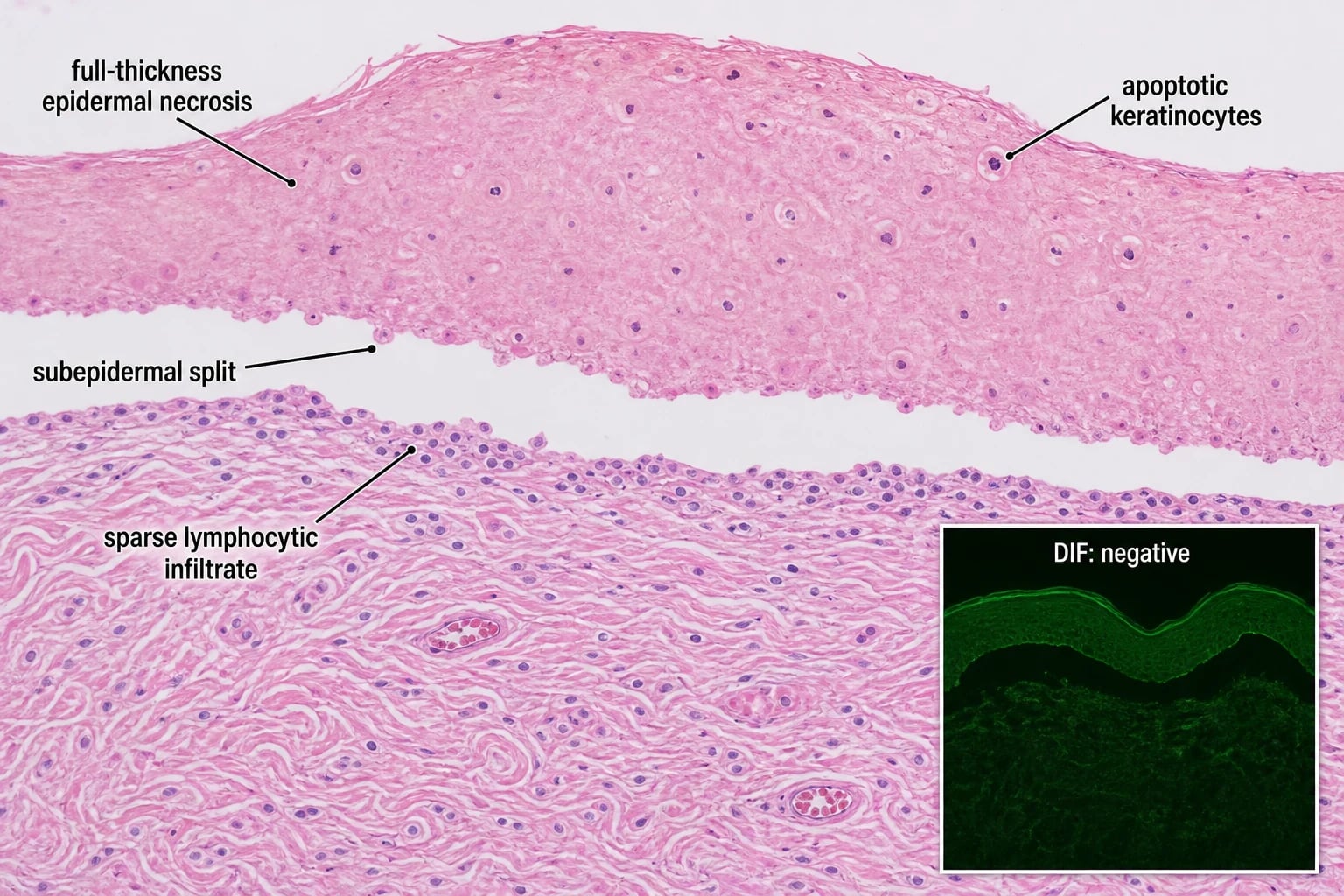
A 4 mm punch biopsy of the advancing erythematous border (including both affected and adjacent skin) shows the histological signature: full-thickness (confluent) epidermal necrosis with a sub-epidermal split, dead keratinocytes, and a sparse superficial perivascular lymphocytic infiltrate (the "many dead cells, few inflammatory cells" pattern). Direct immunofluorescence is negative or shows only non-specific deposition, which helps exclude pemphigus vulgaris (intercellular fishnet IgG) and bullous pemphigoid (linear basement-membrane IgG/C3). Frozen-section histology at the bedside can confirm TEN within an hour when the differential is genuinely uncertain.[2][4][10]
Bloods and severity grading
Send a full blood count (leucocytosis or leucopenia, eosinophilia occasionally, anaemia), urea and electrolytes (renal impairment raises SCORTEN), liver function tests, glucose, bicarbonate, serum lactate, C-reactive protein, and blood cultures (before antibiotics) to detect bacteraemia. A chest radiograph screens for aspiration and pulmonary involvement. Calculate SCORTEN twice — at admission and at 72 hours — because the 72-hour value recalibrates risk as the disease evolves.[1][4]
SCORTEN — Severity Assessment
The SCORTEN score (SCORe of Toxic Epidermal Necrolysis, Bastuji-Garin 2000) is the universally adopted severity score. Calculate at admission and again at 72 hours; the 72-hour value is more accurate. Each of 7 factors = 1 point:[1]
| Factor | Threshold | Point |
|---|---|---|
| Age | Over 40 years | 1 |
| History of malignancy | Yes | 1 |
| Heart rate | Over 120 / min | 1 |
| Initial detachment | Over 10 percent BSA | 1 |
| Serum urea | Over 10 mmol/L (over 28 mg/dL) | 1 |
| Serum bicarbonate | Under 20 mmol/L | 1 |
| Serum glucose | Over 14 mmol/L (over 252 mg/dL) | 1 |
SCORTEN 2 or more warrants ICU or burns unit transfer. A score of 4 or more predicts mortality over 50 percent and triggers aggressive supportive care plus consideration of specific immunomodulation. [1]
Management
Immediate actions (minutes)
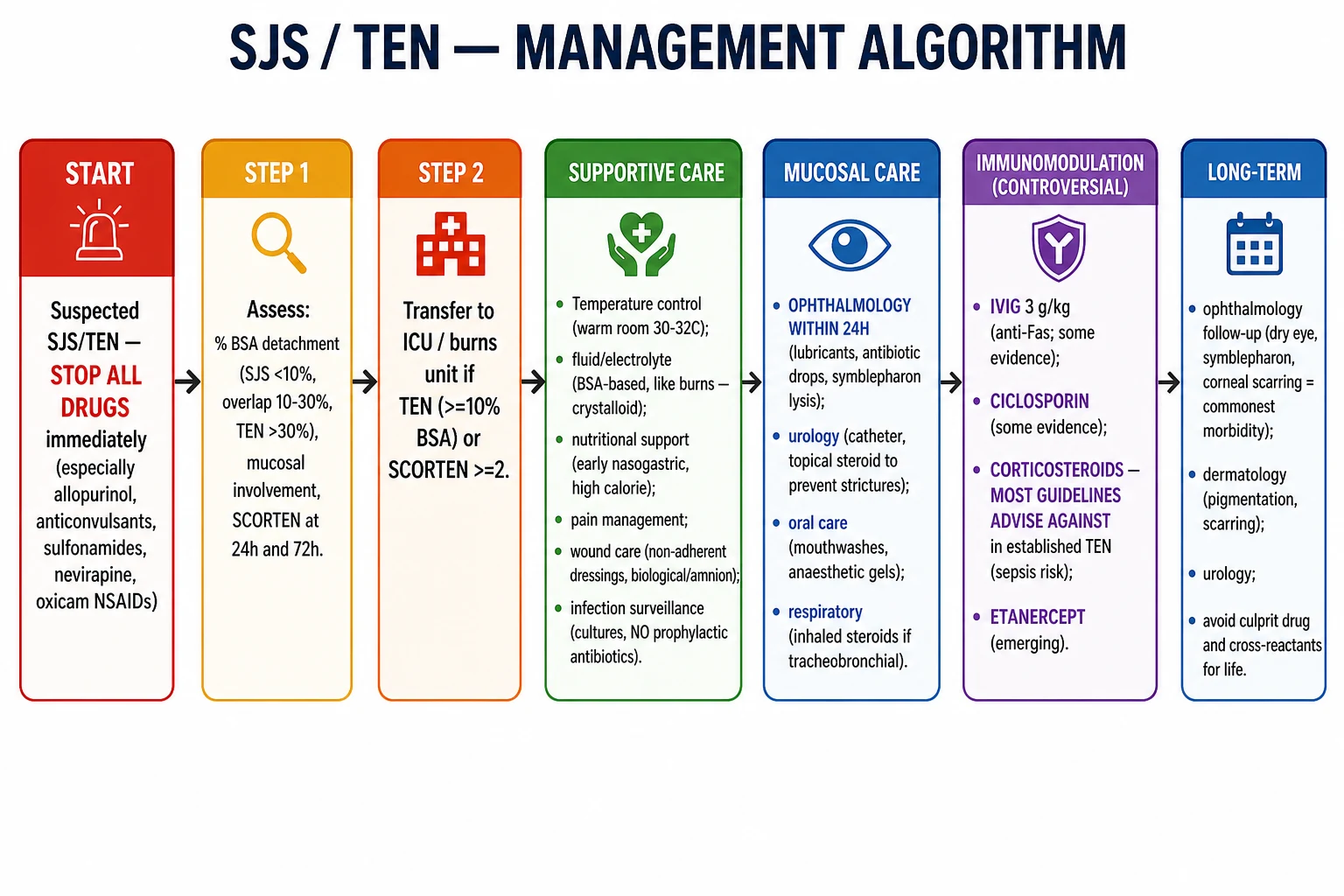
- STOP ALL DRUGS — especially those started in the last 8 weeks (the culprit and any unnecessary agents). Withdraw every drug started in the preceding eight weeks; if a single essential drug cannot be withdrawn, switch to a structurally unrelated alternative. Early withdrawal shortens disease progression and reduces mortality.[2][4][10]
- Decide the level of care by BSA detached — patients with over 10 percent BSA detachment (overlap and TEN), or with rapidly progressive SJS, airway involvement, renal failure, or a high SCORTEN, are transferred to a burns unit or intensive care unit. Burns units have the expertise in fluid management, wound care, temperature control and infection surveillance that determines survival in large-area epidermal loss.[2][4]
- Fluid and electrolyte resuscitation. The denuded dermis loses fluid, electrolytes and protein exactly as a burn does, but the insensible loss in SJS/TEN is less than in a comparable-sized thermal burn (the dermis is intact), so fluid needs are lower — give roughly two-thirds of the volume calculated by a standard burn formula. There is no universally validated formula; a modified approach uses about 1.5 mL/kg per percent BSA in the first 24 hours (versus 2 to 4 mL/kg per percent in the Parkland formula for burns), titrated to a urine output of 0.5 to 1.0 mL/kg/hour, with careful monitoring of sodium, potassium, magnesium, phosphate, albumin and renal function. Over-resuscitation causes pulmonary oedema and worsens outcome.[2][4]
- Analgesia and airway. Skin denudation is exquisitely painful; give intravenous morphine (titrated or patient-controlled) and address the airway — tracheobronchial involvement can cause epithelial sloughing and respiratory failure, and may require intubation by an experienced operator (the friable mucosa bleeds).[2][4]
Supportive care (the mainstay)
- Temperature: warm environment (30 to 32 degrees C) to minimise heat loss through denuded skin; warming blankets and overhead warmers as needed.
- Wound care: gentle debridement of necrotic epidermis, non-adherent dressings (paraffin gauze, silicone dressings, biosynthetic substitutes like Biobrane) that do not tear regenerating epidermis on removal. Topical silver sulfadiazine 1 percent twice daily has been widely used but is controversial — sulphonamide absorption through the denuded skin can itself provoke reactions and the evidence for benefit is weak; many burns units now prefer non-adherent dressings with petroleum-based emollients or biosynthetic dressings in patients with documented sulphonamide allergy.
- Nutrition: early enteral feeding via a nasogastric tube (within 24 to 48 hours); catabolism is severe and parenteral nutrition is associated with line sepsis. Caloric target about 1.5 times basal metabolic rate, with protein 1.5 to 2 g/kg/day.
- Infection surveillance: daily review, low threshold for blood cultures and broad-spectrum antibiotics (avoid prophylactic antibiotics as they select resistance). Sepsis is the leading cause of death in SJS/TEN, usually from gram-positive (Staphylococcus aureus) or gram-negative bacteraemia arising from the denuded skin, central lines, or lungs.[2][4]
- Venous thromboembolism prophylaxis: low molecular weight heparin unless contraindicated.
- Electrolytes and nutrition: monitor and replace magnesium, phosphate, calcium; correct hypoalbuminaemia with cautious albumin replacement when clinically indicated.[2][4]
Mucosal care (time-critical)
- Ophthalmology review WITHIN 24 HOURS — the single most important step to prevent long-term ocular sequelae. Lubricants, topical antibiotic drops (chloramphenicol or ofloxacin), topical corticosteroid drops (prednisolone 0.5 percent), and symblepharon lysis (daily breaking of adhesions with a glass rod) prevent irreversible corneal scarring and blindness. For severe ocular involvement, early amniotic membrane transplantation within the first few days reduces long-term complications dramatically.[9]
- Oral hygiene: chlorhexidine 0.2 percent mouthwash (diluted, swish and spit), topical anaesthetic mouthwashes (lidocaine viscous) for pain, and topical corticosteroids (triamcinolone in Orabase) for erosions reduce pain and allow feeding.
- Urinary catheter is usually required because urethral mucositis causes painful micturition and retention; strictures are prevented by gentle catheterisation and topical oestrogen or corticosteroid to genital erosions.
- Stool softeners prevent anal fissure from anal mucositis.
Controversial specific immunomodulation
The evidence base is limited and guidelines differ.[4][8][10]
[1]The Cochrane review of systemic interventions for SJS, TEN and overlap (2022) concluded that the evidence is insufficient to recommend any specific immunomodulator — IVIG, ciclosporin, corticosteroids, thalidomide or TNF-alpha inhibitors — over supportive care alone, and that high-quality randomised trials are needed. The only comparator with a positive signal was etanercept versus corticosteroids (low certainty).[8] The practical consequence: supportive care is the standard, and specific therapy is adjunctive, selected case by case, never a substitute for stopping the drug and burns-level support.
Quick self-test — the question that catches candidates
A 56-year-old man started allopurinol 6 weeks ago for gout and now has fever, painful burning skin, haemorrhagic lip crusting, conjunctivitis and dusky purpuric macules coalescing on the trunk with sheet-like epidermal peeling over 15 percent BSA. What is the diagnosis, what is the single most important immediate action, and what does his SCORTEN start to accumulate? [1]
The diagnosis is SJS-TEN overlap (15 percent BSA detachment, atypical targets, mucositis at oral and ocular sites, one to eight weeks after allopurinol). The single most important action is STOP ALLOPURINOL IMMEDIATELY (and review all other drugs started in the last 8 weeks) and transfer to a burns unit or ICU (over 10 percent BSA). His SCORTEN is accumulating: age over 40 (1 point), initial detachment over 10 percent BSA (1 point) — plus heart rate, urea, bicarbonate, glucose and malignancy status to be checked. Ophthalmology from day one, amniotic membrane for severe eyes, modified (reduced) fluid resuscitation, early enteral nutrition.
Specific Subtypes & Scenarios
Mycoplasma-induced rash and mucositis (MIRM) in children
In children and young adults, SJS-like illness can follow Mycoplasma pneumoniae respiratory infection, often with a one- to two-week lag. The phenotype is prominent mucositis (oral, ocular, urethral) with minimal skin lesions — historically labelled "atypical SJS" or "Fuchs syndrome". The modern term is reactive infectious mucocutaneous eruption (RIME), formerly Mycoplasma-induced rash and mucositis (MIRM). Drug cause is absent or weak. Management is supportive care plus a macrolide (azithromycin or clarithromycin) for the underlying Mycoplasma; the prognosis is better than drug-induced SJS but ocular complications still occur. Biopsy shows an interface dermatitis rather than confluent necrosis.[10]
Allopurinol-induced SJS and HLA-B*5801
Allopurinol is now the commonest single cause of SJS/TEN in Europe and the Americas. The reaction typically begins two to eight weeks after starting allopurinol, and the risk is dose- and renal-function-related (oxypurinol accumulates in renal impairment). HLA-B*5801 is a strong genetic marker, especially in Han Chinese, Thai and Korean populations (odds ratio over 500 in the original 2005 paper, 100 percent of allopurinol-SCAR cases positive), and screening is recommended before starting allopurinol in these groups.[7] The lesson for safe prescribing: start allopurinol low (100 mg/day, even lower in renal impairment) and titrate slowly, treat to a urate target, and never initiate allopurinol for asymptomatic hyperuricaemia outside guidelines.
Carbamazepine-induced SJS and HLA-B1502 / HLA-A3101
Carbamazepine-induced SJS is concentrated in Han Chinese and South-East Asian populations due to high HLA-B1502 carriage (up to 10 to 15 percent of Han Chinese, with odds ratio over 1000 in some cohorts).[6] Since the 2004 finding, the US FDA recommends HLA-B1502 screening before carbamazepine in Asian-ancestry patients, and screening is mandatory in Taiwan and Hong Kong. Oxcarbazepine, phenytoin and lamotrigine carry cross-reactivity and warrant caution in HLA-B1502-positive individuals. In Europeans and Japanese, the carbamazepine signal is carried by HLA-A3101, leading to EMA and Japanese screening recommendations. The pharmacogenomic lesson — screen before prescribing in at-risk populations — is one of the most tested modern facts in medical genetics.[6][10]
Drug reaction with eosinophilia and systemic symptoms (DRESS)
DRESS (also called drug-induced hypersensitivity syndrome, DIHS) is a separate severe cutaneous adverse reaction that is commonly confused with SJS in early exams. Onset is two to eight weeks after the causative drug (anticonvulsants, allopurinol, sulfonamides, minocycline, dapsone); features are a morbilliform rash, marked facial oedema, fever, lymphadenopathy, eosinophilia, hepatitis, and reactivation of human herpesviruses (especially HHV-6). Distinguishing it from SJS: DRESS has no sheet-like epidermal necrosis, no positive Nikolsky sign, and typically no mucosal ulceration. Treatment is systemic corticosteroids (prednisolone 1 mg/kg/day tapering over weeks).[2][4]
Complications & Pitfalls
Complications are acute (during the active illness) and long-term (in survivors), and the long-term ocular burden is the dominant quality-of-life issue.[2][4][9]
Acute complications. The commonest cause of death is sepsis — usually gram-positive (Staphylococcus aureus) or gram-negative bacteraemia arising from the denuded skin, central lines or lungs — followed by acute respiratory distress syndrome, acute kidney injury (hypovolaemia, sepsis, drug nephrotoxicity), gastrointestinal bleeding from mucosal ulceration, electrolyte disturbances (hyponatraemia, hypokalaemia, hypophosphataemia) and venous thromboembolism (prophylaxis is essential).[2][4]
Long-term complications in survivors. Ocular disease dominates: dry eye syndrome, symblepharon, fornix shortening, trichiasis, corneal scarring, corneal opacity and blindness affect up to a third to a half of survivors without optimal early eye care. Mucosal sequelae include oesophageal, urethral and anal strictures, labial synechiae and vaginal stenosis. Cutaneous sequelae include post-inflammatory hyperpigmentation or hypopigmentation, scarring and nail dystrophy (including anonychia). Chronic ocular disease can drive lifelong morbidity; long-term ophthalmology follow-up is essential.[9]
Pitfalls
Classic errors include delaying drug withdrawal until after biopsy confirmation, giving full Parkland-volume fluid (causing pulmonary oedema), using silver sulfadiazine in known sulphonamide allergy, neglecting the eyes (no early ophthalmology, no amniotic membrane), continuing an essential causative drug rather than switching to a structurally unrelated alternative, and using corticosteroids in established TEN (which masks sepsis and may raise mortality).[2][4]
Prognosis & Disposition
Mortality is driven by detachment extent and comorbidity, captured by SCORTEN: the admission score stratifies risk, and the 72-hour SCORTEN recalibrates it and is the more accurate predictor. Mortality bands are 3.2 percent for a score of 0 to 1, 12.1 percent for 2, 35.8 percent for 3, 58.4 percent for 4, and over 90 percent for 5 or more.[1] In general, SJS mortality is 1 to 5 percent, overlap 5 to 15 percent, and TEN 25 to 35 percent. Survivors re-epithelialise over two to six weeks as keratinocytes migrate from surviving appendages (hair follicles, sweat glands) and wound edges.[2][4]
Disposition follows severity. Mild SJS (under 10 percent BSA, low SCORTEN, no organ failure) may be managed on a dermatology ward with daily review. SJS-TEN overlap and TEN (over 10 percent BSA, or any organ failure, or SCORTEN of 3 or more) are managed in a burns unit or intensive care. Discharge is appropriate when re-epithelialisation is underway, sepsis is controlled, nutrition is established enterally, and ophthalmology and mucosal care plans are in place. Survivors need lifelong ophthalmology follow-up, strict avoidance of the causative drug and structurally related drugs (documented clearly in the medical record and a medical-alert bracelet), and HLA screening of first-degree relatives when a high-risk allele is identified.[2][9]
Special Populations
Children. SJS/TEN in children is less common and the drug cause is weaker — Mycoplasma pneumoniae infection (RIME / MIRM) is a leading trigger, often with prominent mucositis and minimal skin lesions. Management is supportive plus a macrolide for Mycoplasma; all drug dosing is weight-based (IVIG 1 g/kg/day, ciclosporin 3 to 5 mg/kg/day, morphine 0.1 mg/kg titrated). Children tend to have better outcomes than adults for a given detachment area.[2][10]
Pregnancy. SJS/TEN in pregnancy is rare; management is unchanged (stop the drug, supportive care, ophthalmology), but drug selection must account for teratogenicity — ciclosporin is relatively safe in pregnancy, IVIG is safe, and mycophenolate and thalidomide are avoided. Multidisciplinary involvement with obstetrics and neonatology is required; severe maternal illness threatens the fetus through hypovolaemia and sepsis.[2]
HIV. HIV-positive patients have a markedly increased risk of SJS/TEN, especially from nevirapine (highest risk in the first weeks of therapy, and in those with higher CD4 counts) and sulphonamides (cotrimoxazole). The immune dysregulation and polypharmacy of HIV cohorts compound the risk. Management is the same; drug avoidance and careful antiretroviral selection (with infectious-diseases input) are preventive.[2]
The elderly and the immunocompromised. Older patients have higher baseline SCORTEN (age over 40 contributes a point) and more comorbidity, so mortality is higher. Malignancy (a SCORTEN variable) and immunosuppression both raise the risk of drug-induced SJS/TEN and of fatal sepsis, demanding tighter infection surveillance.[1][2]
Bone-marrow transplant recipients. Acute graft-versus-host disease (aGVHD) is the principal mimic and can co-occur with drug-induced SJS/TEN; the histology is similar (apoptotic keratinocytes, sparse infiltrate). Donor T cells mediate the damage; management is high-dose corticosteroids plus calcineurin inhibitors, with the additional complexity of immunosuppression for the underlying transplant.[2]
Evidence, Guidelines & Regional Differences
The Cochrane verdict on specific therapy
The 2022 Cochrane review of systemic interventions for SJS, TEN and overlap concluded that the evidence is insufficient to determine whether IVIG, ciclosporin, corticosteroids, thalidomide or TNF-alpha inhibitors improve survival compared with supportive care alone; no drug showed a clear, reproducible benefit, and the quality of evidence was low or very low.[8] The single comparator with a positive signal was etanercept versus corticosteroids (1 RCT, 91 participants; etanercept 8.3 percent mortality vs corticosteroids 16.3 percent mortality, low certainty).[8] The practical consequence: supportive care is the standard, and specific therapy is adjunctive, selected case by case, never a substitute for stopping the drug and burns-level support.
Pharmacogenomic screening guidelines
Pharmacogenomic screening before high-risk drugs is one of the great translational successes of the HLA era. HLA-B1502 screening before carbamazepine is recommended by the US FDA (since 2007) for patients of Asian ancestry and is mandatory in Taiwan and Hong Kong; HLA-B5801 screening before allopurinol is recommended in Han Chinese, Thai and Korean populations (CPIC, Taiwanese and regional guidelines). The HLA-B*5701 screen before abacavir (for hypersensitivity, not SJS) is the other classic pharmacogenomic precedent. The unifying principle: in populations with high carriage of a high-risk allele, screen before prescribing.[6][7][10]
Regional deltas
| Region | Leading culprit drug | Preferred specific therapy | Guideline source |
|---|---|---|---|
| Europe (EuroSCAR / RegiSCAR) | Allopurinol | Ciclosporin favoured over IVIG in several French and German reference centres; corticosteroids generally avoided in established TEN | EuroSCAR / EADV |
| North America | Allopurinol rising, anticonvulsants, sulfonamides | IVIG more commonly used than ciclosporin in US centres despite conflicting evidence | US FDA, AAD |
| East Asia (Taiwan, Hong Kong, Korea, Japan) | Carbamazepine (now reduced by screening), allopurinol, anticonvulsants | Amniotic membrane transplantation pioneered and widely adopted | CPIC, local consensus |
| India and South Asia | Anticonvulsants, sulfonamides, nevirapine, rising allopurinol | Supportive care per European standard; pharmacogenomic screening where East-Asian ancestry applies | IADVL |
Recent (2024) consensus
The Chen et al. British Journal of Dermatology review (2024) proposes refined diagnostic criteria, synthesises the immunopathogenesis (drug-specific T-cell response, HLA polymorphism, necroptosis as an emerging pathway), and reviews the growing role of TNF-alpha inhibitors, particularly etanercept, in severe cases.[10]
Exam Pearls
The high-yield facts examiners reward, stated correctly: [1]
[1]Red Flags
Exam application bank (NEET-PG / INICET)
One-line answer
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are a spectrum of life-threatening immune-mediated severe cutaneous adverse reactions (SCAR), characterised by widespread keratinocyte apoptosis producing epidermal detachment and mucosal erosions, most commonly triggered by drugs (allopurinol, anticonvulsants, sulfonamides, nevirapine, oxicam NSAIDs). Classified by percentage of body surface area (BSA) detached: SJS under 10%, SJS-TEN overlap 10 to 30%, TEN over 30%. Mortality is estimated using the SCORTEN score (calculated at 24h and 72h). Management is a dermatological emergency: immediate withdrawal of all drugs, transfer to ICU or burns unit, supportive care (modified Parkland fluid resuscitation, nutrition, wound care, infection surveillance), urgent mucosal care (ophthalmology within 24h, amniotic membrane for severe eyes), and controversial immunomodulation (IVI
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Stevens-Johnson syndrome and toxic epidermal necrolysis.
[1]Prevention
The key preventive steps once a patient has had SJS/TEN: avoid re-exposure to the culprit drug and structurally related drugs for life; document in the medical record, on a medical-alert bracelet, and in the pharmacy record; offer HLA screening of first-degree relatives when a high-risk allele is identified (HLA-B1502 in Asians for carbamazepine; HLA-B5801 in Han Chinese, Thai and Korean for allopurinol; HLA-A3101 in Europeans and Japanese for carbamazepine); counsel about cross-reactive drugs (oxcarbazepine, phenytoin, lamotrigine in HLA-B1502-positive patients; allopurinol desensitisation is generally not safe and should be avoided).[6][7][10]
References
- [1]Bastuji-Garin S, Fouchard N, Bertocchi M, Roujeau JC, Revuz J, Wolkenstein P SCORTEN: a severity-of-illness score for toxic epidermal necrolysis J Invest Dermatol, 2000.PMID 10951229
- [2]Lerch M, Mainetti C, Terziroli Beretta-Piccoli B, Harr T Current Perspectives on Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis Clin Rev Allergy Immunol, 2018.PMID 29188475
- [3]Naegele D, Sekula P, Paulmann M, Mockenhaupt M Incidence of Epidermal Necrolysis: Results of the German Registry J Invest Dermatol, 2020.PMID 32353449
- [4]Frantz R, Huang S, Are A, Motaparthi K Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Review of Diagnosis and Management Medicina (Kaunas), 2021.PMID 34577817
- [5]Chung WH, Hung SI, Yang JY, Su SC, Huang SP, Wei CY, Chin SW, Hung SI, Chang WC, Lin CC, et al. Granulysin is a key mediator for disseminated keratinocyte death in Stevens-Johnson syndrome and toxic epidermal necrolysis Nat Med, 2008.PMID 19029983
- [6]Chung WH, Hung SI, Hong HS, Hsih MS, Yang JY, Tsai PC, Lee CY, Siao JL, Hsu CJ, Wei JC, Chen YT Medical genetics: a marker for Stevens-Johnson syndrome Nature, 2004.PMID 15057820
- [7]Hung SI, Chung WH, Liou LB, Chu CC, Lin M, Huang HP, Lin YL, Lan JL, Yang LC, Hong HS, Chen MJ, Lai PC, Wu MS, Chu CY, Wang KH, Chan CH, et al. HLA-B*5801 allele as a genetic marker for severe cutaneous adverse reactions caused by allopurinol Proc Natl Acad Sci U S A, 2005.PMID 15743917
- [8]Jacobsen A, Olabi B, Langley A, Beecker J, et al. (Cochrane Skin Group) Systemic interventions for treatment of Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), and SJS/TEN overlap syndrome Cochrane Database Syst Rev, 2022.PMID 35274741
- [9]Akgun Z, Can GD, Selver OB Ocular involvement in Stevens-Johnson syndrome and toxic epidermal necrolysis: A review of current management and changing trends Indian J Ophthalmol, 2025.PMID 41288622
- [10]Chen L, et al. Recent progress in Stevens-Johnson syndrome/toxic epidermal necrolysis: diagnostic criteria, pathogenesis and treatment Br J Dermatol, 2024.PMID 39141587