Emergency & Toxicology · Emergency & Toxicology
Drowning
Also known as Submersion injury · Non-fatal drowning · Fatal drowning · Immersion incident · Post-immersion respiratory distress
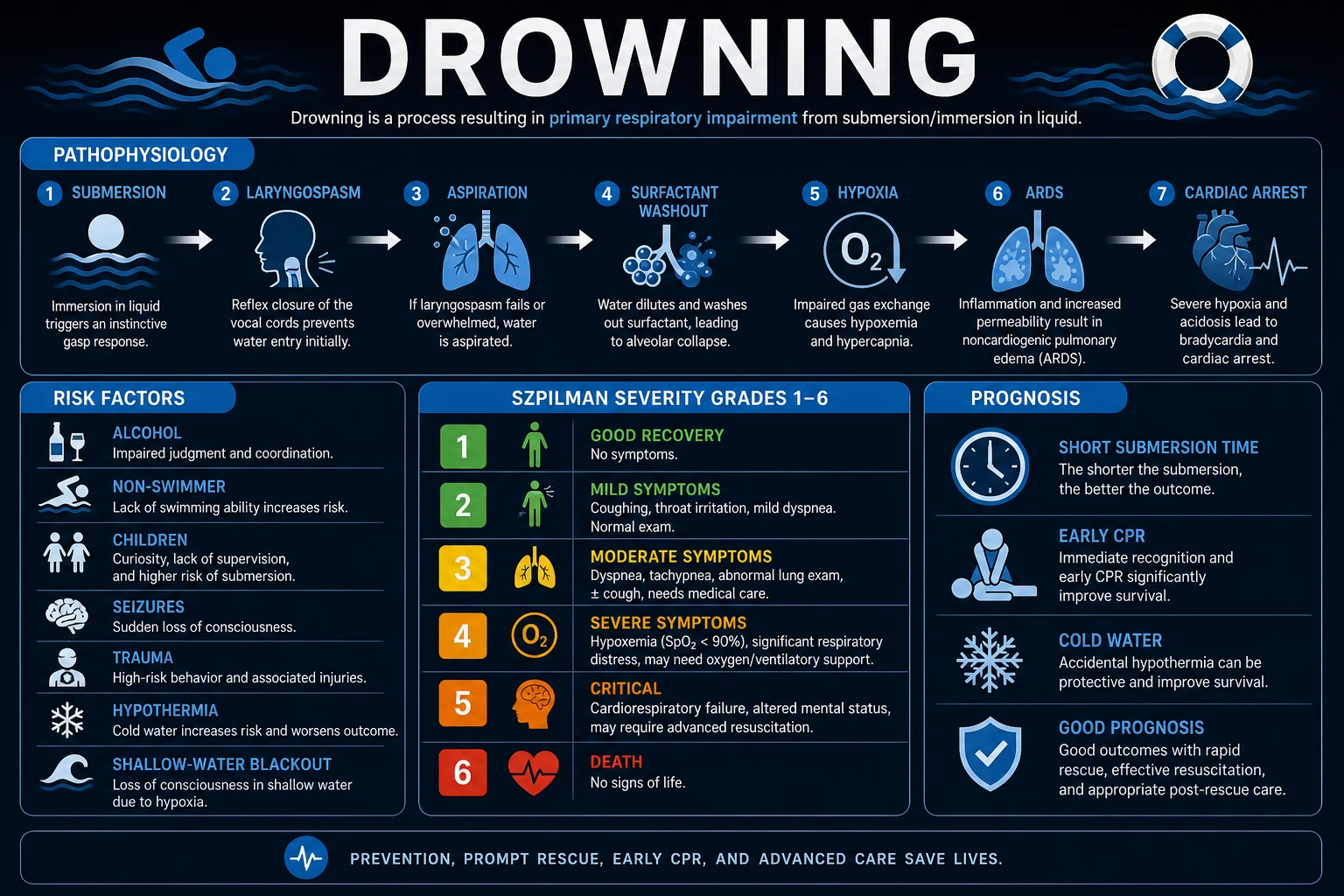
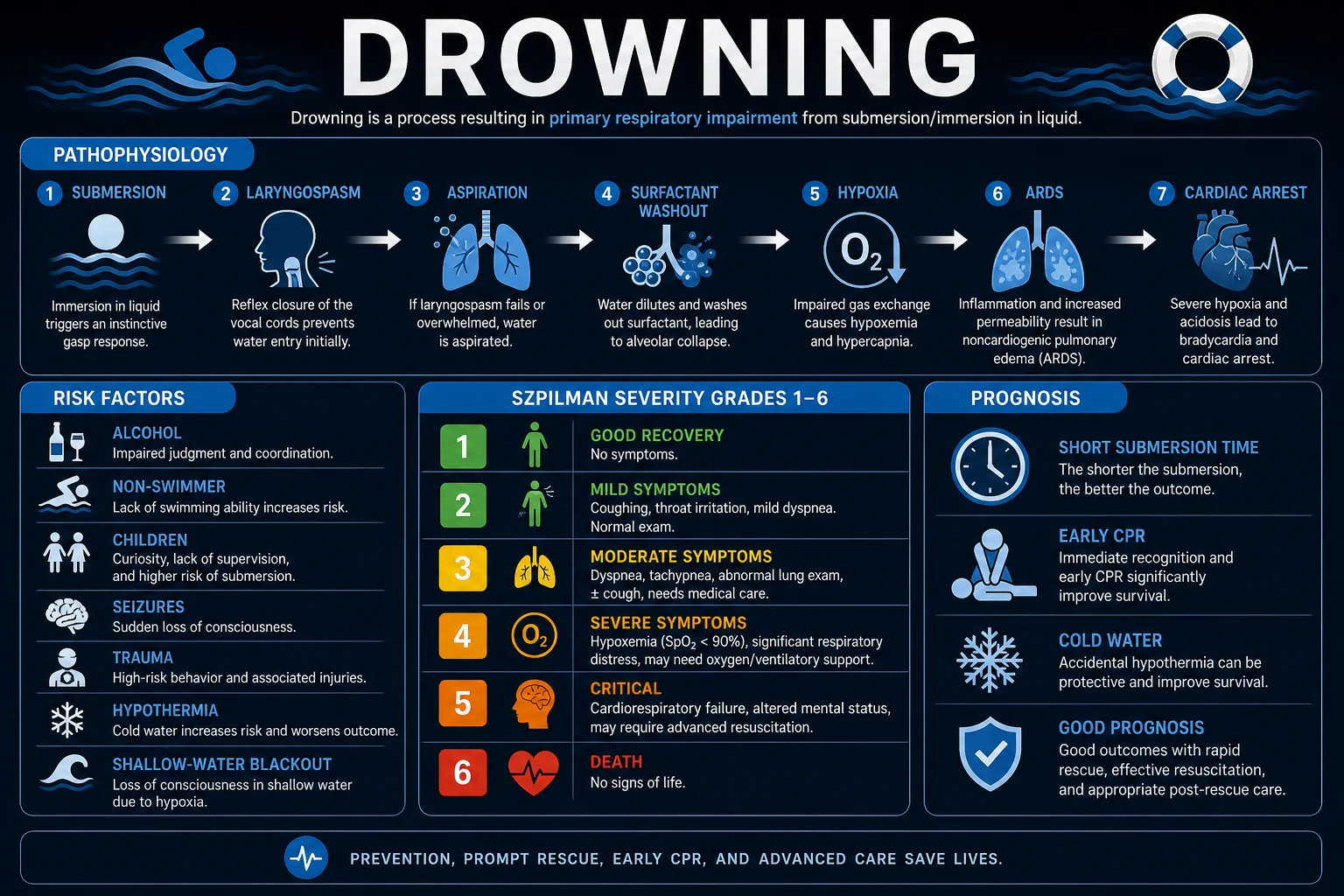
Drowning is defined by the WHO as the process of experiencing respiratory impairment from submersion or immersion in liquid; outcomes are fatal drowning, non-fatal drowning with morbidity, or non-fatal drowning without morbidity (a rescue). The old terms 'near-drowning', 'dry drowning', 'wet drowning', 'active drowning' and 'secondary drowning' are obsolete. The primary injury is hypoxia produced by laryngospasm and/or aspiration of liquid into the alveoli, which washes out surfactant, collapses alveoli, causes non-cardiogenic pulmonary oedema and ventilation-perfusion mismatch, and may evolve over hours into acute respiratory distress syndrome (ARDS). The downstream killer is hypoxic cardiac arrest, which in drowning is asystolic or PEA — NOT ventricular fibrillation. The defining management principle is therefore oxygenation first: in cardiac arrest give 5 initial rescue breaths before chest compressions, then continue 30:2; for the hypoxic but breathing victim give high-flow oxygen, escalate to CPAP/NIV or intubation, and observe for at least 6 to 24 hours because ARDS can develop after rescue. Never use the Heimlich manoeuvre, do not routinely immobilise the cervical spine (only if a concerning mechanism), give no routine prophylactic antibiotics or corticosteroids, and do not terminate resuscitation prematurely in the hypothermic victim ('not dead until warm and dead'). Risk factors: alcohol, inability to swim, unsupervised children, seizures, trauma (diving), hypothermia, and hyperventilation before a breath-hold dive (shallow-water blackout); swimming is also a recognised trigger of arrhythmia in long-QT syndrome, Brugada syndrome and CPVT, so an unexplained drowning demands an ECG and family screening.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Overview & Definition
Drowning is one of the commonest causes of unintentional injury death worldwide and is the leading cause of accidental death in young children in many countries. Despite this it was, for decades, a public-health orphan: definitions were inconsistent, data were un-comparable across countries, and clinicians taught a confusing taxonomy of 'near-drowning', 'dry' and 'wet' drowning that did not map onto either physiology or outcome.[1]
In 2002 the World Congress on Drowning, backed by the WHO, adopted a single uniform definition that was published in 2005 by van Beeck and colleagues and is now used worldwide: drowning is the process of experiencing respiratory impairment from submersion or immersion in liquid. The word process is deliberate — drowning is a continuum, and the outcome is recorded as fatal drowning (death), non-fatal drowning with morbidity, or non-fatal drowning without morbidity (a simple rescue).[1] The Utstein-style consensus later extended this with a standardised dataset for reporting drowning resuscitation, so that studies and registries can be compared.[2]
The clinical skill in drowning is to recognise three things and act on them in order. First, drowning is fundamentally a hypoxic event — the lung is the primary organ injured, and the brain and heart fail because oxygen delivery fails; the priority is therefore oxygenation, not circulation. Second, the lung injury can worsen over hours after rescue (post-immersion ARDS), so even a well-looking victim needs observation. Third, several entrenched practices are obsolete or harmful — abdominal thrusts, routine cervical-spine immobilisation, routine antibiotics, and the 'dry vs wet' distinction — and must be discarded.[3][5]
Classification
Drowning is classified along three axes that each change either communication, triage, or management.[3]
By outcome (the WHO / Utstein taxonomy that replaced the old near-drowning language):[1][2]
Fatal drowning
- Death from drowning
- Replaces the obsolete 'drowning' (meaning death) vs 'near-drowning' (meaning survival) pair
- Recorded on the death certificate as a drowning death
Non-fatal drowning with morbidity
- Survival with injury (hypoxic brain injury, lung injury, disability)
- Replaces the term 'near-drowning with injury'
- Severity graded by organ involvement and by the Szpilman scale
Non-fatal drowning without morbidity
- Survival without any injury — a 'rescue'
- Replaces 'near-drowning without injury'
- May still require a period of observation (ARDS can evolve hours later)
By Szpilman clinical severity grade (a 6-point scene/ED classification based on clinical findings, used to triage, decide on ventilation, and prognosticate):[3]
Grade 1
- Asymptomatic or only coughing
- Normal exam, normal oxygenation
- Observe 6-24h, discharge if remains well
Grade 2
- Wheeze or crackles, mild dyspnoea
- SpO2 normal or near-normal on air
- Observe; supplemental oxygen if needed
Grade 3
- Pulmonary oedema (frothy sputum, crackles), SpO2 under 90 percent on air
- Hypoxaemic but conscious
- High-flow oxygen +/- CPAP/NIV; admit
Grade 4
- Frank pulmonary oedema with respiratory failure
- Often needs intubation
- ICU; mechanical ventilation with PEEP
Grade 5
- Respiratory arrest (apnoea) but pulse present
- Imminent cardiac arrest
- Immediate bag-valve-mask ventilation, prepare to intubate
Grade 6
- Cardiac arrest (no pulse)
- Asystole or PEA (rarely VF)
- 5 rescue breaths then 30:2 CPR; full ALS
By water type (physiologically interesting but clinically the distinction matters little, because both fresh and salt water ultimately produce the same surfactant-dysfunction/hypoxia picture):[3]
- Freshwater (hypotonic) — washes out and inactivates surfactant, is rapidly absorbed across the alveolar-capillary membrane, and (in massive aspiration) can haemolyse red cells. Clinically it produces atelectasis and shunt.
- Saltwater (hypertonic) — draws fluid from the circulation into the alveoli by osmotic gradient, worsening pulmonary oedema and hypovolaemia. Clinically it produces a haemodilution-style injury of the alveolus.
- The clinically important point: in real life the volume aspirated is small (a few mL/kg), so the spectacular electrolyte and haemolysis derangements once taught are uncommon. Treat both the same — oxygenate.[5]
Epidemiology & Risk Factors
The WHO Global Report on Drowning estimated roughly 235,000 to 372,000 drowning deaths per year worldwide, making it among the top causes of unintentional injury death — and drowning is heavily concentrated in low- and middle-income countries (over 90 percent of deaths) and in children and young men. In high-income countries the age distribution is bimodal: a large under-5 peak (toddlers around home water) and a second 15 to 25 year-old peak (young men in open water, often with alcohol). Drowning is a leading cause of injury death in children globally.[4]
[4]The host and situational risk factors are exam staples because each suggests a mechanism and a prevention message:[3][4]
| Risk factor | Mechanism / why it matters | Prevention |
|---|---|---|
| Alcohol / drugs | Impairs judgement, balance, swim ability, and the dive reflex; a contributor in up to half of adult drowning deaths | Boating and water alcohol policy |
| Inability to swim | Direct | Swim and water-safety instruction |
| Unsupervised young children | Toddlers can drown silently in a few centimetres of water (baths, buckets, toilets, pools) | Four-sided isolation pool fencing; constant supervision |
| Seizure disorder | Seizure in water -> submersion; bathtubs are the high-risk site in epilepsy | Shower instead of bath; supervised swimming |
| Trauma / diving | Cervical spine injury -> quadriplegia and apnoea; also head injury | Feet-first entry; depth-check before diving |
| Hypothermia | Exhaustion, arrhythmia, but may also be neuroprotective | Wetsuits, limiting immersion time |
| Shallow-water blackout | Hyperventilation blows off CO2 before O2 drops -> diver loses consciousness underwater without warning | Never hyperventilate before a breath-hold dive |
| Channelopathy (LQTS, Brugada, CPVT) | Swimming / cold-water / exertion trigger polymorphic VT / VF -> sudden death underwater | ECG and family screening of unexplained drowning victims |
Shallow-water blackout deserves a sentence of mechanism because examiners love it. Normally the urge to breathe is driven by rising arterial CO2, not by falling O2. If a diver hyperventilates before submerging, they blow off CO2 (lowering the starting PaCO2) so that, during the breath-hold, PaCO2 takes longer to reach the breath-hold-breaking threshold — but PaO2 may fall below the level needed to maintain consciousness before the urge to breathe becomes overwhelming. The diver loses consciousness underwater with no warning dyspnoea, inhales water, and drowns. The message: never hyperventilate before a breath-hold dive.[4]
Pathophysiology
The drowning injury is a cascade with a single common end point — hypoxia — and the central exam insight is that everything downstream (brain injury, cardiac arrest, multi-organ failure) flows from that hypoxia. The sequence after the face is submerged is:[2][3]
- Submersion + breath-holding + panic/struggle. Conscious breath-holding is voluntary only briefly; as PaO2 falls and PaCO2 rises, the urge to breathe becomes irresistible.
- Either laryngospasm or aspiration. In about 10 to 20 percent of victims water touching the larynx provokes intense laryngospasm (reflex glottic closure) so little water enters the lung — the old 'dry drowning'. In 80 to 90 percent, water is aspirated into the tracheobronchial tree and alveoli — the old 'wet drowning'. Laryngospasm is self-limiting (it relaxes as the victim becomes hypoxic and the airway relaxes), so even 'dry' drowning usually proceeds to aspiration if the victim is not rescued quickly.
- Hypoxia. Both pathways converge: the alveoli are either not ventilated (laryngospasm) or flooded and dysfunctional (aspiration) -> falling PaO2 -> unconsciousness within 1 to 2 minutes.
- Hypoxic cardiac arrest. The hypoxic myocardium first slows (bradycardia from the diving reflex and from hypoxia) then stops in asystole or pulseless electrical activity (PEA). Ventricular fibrillation is uncommon as the presenting rhythm because the arrest is asphyxial, not primary cardiac — this is the single most important resuscitation point.
- Brain injury. The brain is the organ most vulnerable to hypoxia. After 4 to 6 minutes of anoxia at normothermia, neuronal death begins; reperfusion generates further injury (reperfusion injury, cerebral oedema). Hypoxic-ischaemic encephalopathy is the single biggest determinant of long-term outcome.[6]
Aspirated water in the alveolus damages the lung in four ways that together produce surfactant dysfunction, atelectasis, non-cardiogenic pulmonary oedema, ventilation-perfusion mismatch and shunt — culminating, in a substantial minority, in acute respiratory distress syndrome (ARDS):[3]
- Surfactant washout and dysfunction — water dilutes, washes away, and functionally inactivates pulmonary surfactant. Alveolar surface tension rises, alveoli collapse (atelectasis), and the lung becomes stiff and non-compliant.
- Non-cardiogenic pulmonary oedema — capillary-alveolar injury increases permeability; fluid, protein, and inflammatory cells leak into the alveolar space, producing the pink, frothy sputum of pulmonary oedema. (In saltwater aspiration, the hypertonic fluid also osmotically pulls water from the circulation into the alveolus.)
- Ventilation-perfusion mismatch and shunt — blood continues to perfuse non-ventilated, flooded or collapsed alveoli, producing shunt that is poorly responsive to supplemental oxygen (a key reason severe cases need positive pressure).
- Inflammation and ARDS — the injured alveolus mounts an inflammatory response; over hours this can amplify into full ARDS, the basis of delayed post-immersion respiratory failure.[7]
Why asystole/PEA and not VF? A primary cardiac arrest (ischaemic, channelopathic) begins as an electrical event in a well-oxygenated myocardium and so tends to present as a shockable rhythm (VF/pVT). A drowning arrest begins as asphyxia: the myocardium becomes progressively hypoxic and bradycardic before it finally stops, and the rhythm at arrest is asystole or PEA. This is why the defibrillator is rarely the first tool in drowning and why ventilation must come first.[5][6]
Cold water and the diving reflex. Cold water on the face triggers the mammalian diving reflex: apnoea, bradycardia, and peripheral vasoconstriction that shunt blood to the brain and heart, slowing oxygen consumption. In children especially, cold-water submersion can produce a state of profound hypothermia with preserved core organ perfusion that allows neurological survival after very long submersions — the basis of the maxim "not dead until warm and dead": never terminate resuscitation in a hypothermic drowning victim until the core temperature is at least 32 degrees C and asystole persists despite rewarming.[6]
Autonomic conflict and channelopathies. Cold-water immersion produces an abrupt cold-shock response (gasping, tachycardia, sympathetic surge) at the same moment the dive reflex is driving bradycardia — simultaneous sympathetic and parasympathetic discharge ('autonomic conflict') that can trigger arrhythmia in a susceptible heart. In long-QT syndrome, Brugada syndrome and catecholaminergic polymorphic ventricular tachycardia (CPVT), swimming (the combination of cold water, exertion, and the dive reflex) is a recognised trigger of sudden death. This is why an unexplained drowning warrants an ECG (QTc) and family screening — the index victim may be dead, but a living relative may have a treatable channelopathy.[2][8]
Clinical Presentation
The presentation depends on the severity of the submersion and on how rapidly the victim was rescued. The vast majority of rescued victims are alert and breathing at presentation; a minority arrive in respiratory failure or cardiac arrest. The features below are graded by Szpilman severity.[3]
Mild (grade 1 to 2) — the victim is alert, may be coughing, anxious, or shivering. Respiratory examination may reveal wheeze or basal crackles, but oxygen saturation is normal or near-normal on room air. Skin may be cold and pale from immersion.[7]
Moderate (grade 3 to 4) — the victim is hypoxaemic: tachypnoea, accessory-muscle use, cough productive of pink, frothy sputum (pulmonary oedema), diffuse crackles and/or wheeze, and SpO2 under 90 percent on room air. In grade 4 the patient is tiring and may be approaching respiratory arrest.[6]
Severe (grade 5 to 6) — respiratory arrest (apnoea with a pulse — grade 5) or cardiac arrest (no pulse — grade 6). The arrested victim is unconscious, apnoeic, cyanotic, often with water or foam in the mouth; the pulse is absent. Agonal gasps are NOT breathing.[6]
Delayed post-immersion respiratory distress ('secondary drowning'). A victim who was well on rescue (or after a brief observation period) can develop cough, dyspnoea, chest tightness, wheeze, haemoptysis, and progressive hypoxia over minutes to 24 hours as surfactant dysfunction and inflammation progress to ARDS. This is the reason every drowning victim, however well they look, needs a defined observation period.[3][4]
Hypothermia frequently accompanies drowning (cold water, prolonged immersion). Look for the cold, pale, possibly rigid victim; arrhythmia; slow, shallow breathing; depressed conscious level. Severe hypothermia can mimic death — check a core temperature before declaring.[3]
Atypical presentations.
- Children may present after an un-witnessed brief submersion with only vague symptoms (cough, lethargy, vomiting) and still deteriorate — a lower threshold to observe is essential.
- The elderly may drown in the bath after a syncopal event (cardiac, orthostatic, medication-related); the drowning is secondary to the collapse.
- Patients with epilepsy may be found submerged after a seizure; the seizure is the precipitant and the drowning the consequence.
- Intoxicated victims may have a depressed conscious level from alcohol or drugs as well as from hypoxia — assume hypoxia until proven otherwise.[5]
Differential Diagnosis
A person pulled unresponsive from water is not always a straightforward drowning — distinguish the common and the dangerous:[3]
Primary drowning
- Witnessed submersion with aspiration
- Hypoxia, cough, frothy sputum, pulmonary oedema
- Usually young, healthy; cold/wet on retrieval
- Differentiator: the history of submersion with respiratory distress
Cardiac arrhythmia (LQTS, Brugada, CPVT, ischaemia)
- Sudden collapse IN the water (may be the cause of submersion, not the result)
- Possible prior syncope, family history of sudden death
- ECG: long QTc, Brugada pattern, ischaemic changes
- Differentiator: arrhythmia first, drowning second; screen the ECG and the family
Cervical spine injury (diving)
- Diving into shallow water, head strike
- Apnoea from diaphragm paralysis, sensory level, hypotension without tachycardia
- Differentiator: mechanism (diving) and neurological signs; immobilise the spine
Seizure with submersion
- Known epilepsy, in-water seizure, post-ictal state
- Differentiator: prior seizure history, post-ictal features; treat both the seizure and the drowning
Hypoglycaemia / intoxication / overdose
- Collapse at the water's edge or in the bath
- Differentiator: glucose check, alcohol/drug history; reversible cause
Dive-related arterial gas embolism / barotrauma
- Breath-hold or scuba diver surfacing, rapid onset neuro deficit, chest pain
- Differentiator: dive history, focal neurology, pneumothorax; needs recompression
The can't-miss mimics are cardiac arrhythmia (because it changes resuscitation and demands family screening), cervical spine injury (because it changes airway handling and demands immobilisation), and arterial gas embolism in a diver (because it needs hyperbaric therapy). All three are screened for by a focused history (mechanism, past history, medications) plus ECG and (where indicated) imaging.[5]
Clinical & Bedside Assessment
Safe rescue first. The first decision is whether the rescuer enters the water: a would-be rescuer who drowns is a classic and tragic pattern. Reach or throw before you go — use a pole, rope, buoy, or boat. Enter the water only if trained, with a flotation aid, and never alone. In-water rescue breaths (one every 5 seconds while towing) may be given by a trained lifeguard to an apnoeic victim, but chest compressions are not effective in the water and should be reserved for dry land.[5]
Immediate bedside assessment on dry land follows ABCDE, with two drowning-specific caveats: give 5 rescue breaths before compressions in arrest, and immobilise the cervical spine only when indicated.[5]
- Airway/breathing — open the airway; look, listen, feel for breathing for up to 10 seconds; if there is spontaneous breathing, give high-flow oxygen and assess for pulmonary oedema; if there is no normal breathing but a pulse, give rescue breaths (1 breath every 5 to 6 seconds, about 10 to 12 per minute); if there is no pulse and no breathing, start CPR (5 rescue breaths, then 30:2).
- Circulation — check the carotid pulse for up to 10 seconds (longer in hypothermia, where the pulse may be slow and faint). Agonal gasps are not breathing — start CPR.
- Cervical spine — immobilise (manual in-line stabilisation, then collar/blocks/board) only if the mechanism suggests trauma: diving, water-slide, surf-board, fall from a height, suspected seizure with head strike, signs of injury, or unexplained/unwitnessed submersion in an adult with alcohol. Routine immobilisation of all drowning victims is NOT recommended — it hampers CPR and rescue breathing, and most submersions in swimmers are non-traumatic.[5][6]
- Disability/exposure — record GCS/AVPU, pupils, and a core temperature; fully expose to look for signs of injury, but protect from further heat loss.
- Hypothermia staging — use core temperature and clinical signs: HT I (mild, 35 to 32 degrees C, conscious, shivering), HT II (32 to 28 degrees C, altered consciousness, may not shiver), HT III (28 to 24 degrees C, unconscious), HT IV (under 24 degrees C, rigid, vital signs barely detectable, may appear dead). Below 30 degrees C the heart is highly irritable and defibrillation is unreliable — rewarm before repeated shocks.[6]
Can the victim be sent home? Asymptomatic at the scene, with normal observations and normal examination, a reliable adult can be observed for at least 6 hours (some guidelines 4 to 6 hours); any symptom (cough, dyspnoea, vomiting, chest pain) or any abnormal observation (SpO2 under 95 percent, tachypnoea) means admission and observation for up to 24 hours.[3][4]
Investigations
Investigations are driven by severity. The well-looking victim needs observation and serial observations; the symptomatic or arrested victim needs a fuller workup.[3]
Bedside and first-line:[3]
- Continuous pulse oximetry and serial vital signs — the most important single monitor; a falling SpO2 is the earliest sign of evolving ARDS.
- Arterial or venous blood gas — typically shows hypoxaemia (low PaO2) with a combined respiratory and metabolic acidosis (CO2 retention from hypoventilation plus lactic acidosis from hypoxia and shock). The base deficit / lactate is a marker of the severity of the hypoxic insult and prognostic.
- Blood glucose — hypoglycaemia is common in children and in cold-exposed victims; treat.
- Core temperature — low-reading thermometer essential in suspected hypothermia.
- 12-lead ECG (once stable) — to screen for arrhythmia, QTc prolongation, Brugada pattern, or ischaemia, especially in unexplained or exertional/young drowning.
- Electrolytes (Na, K), urea, creatinine, full blood count, coagulation — to detect the uncommon but real derangements (especially after saltwater aspiration or massive aspiration), rhabdomyolysis, acute kidney injury, or disseminated intravascular coagulation.[7]
Imaging:[3]
- Chest X-ray — the first-line imaging of the lung. Findings range from normal (early) to perihilar infiltrates, patchy alveolar opacities, or frank bilateral pulmonary oedema in aspiration/ARDS. A normal initial CXR does NOT exclude later deterioration — post-immersion ARDS can develop over hours; repeat if symptoms evolve.
- CT brain — indicated in the comatose victim to look for cerebral oedema, loss of grey-white differentiation, or hypoxic-ischaemic injury, and to exclude an alternative (haemorrhage, stroke). Early CT may be normal; MRI is more sensitive for hypoxic-ischaemic injury but does not usually change acute management.
- CT cervical spine — when a concerning mechanism is present (diving, fall, alcohol, unwitnessed adult) and the spine cannot be cleared clinically.[7]
Reproduced verbatim — the Szpilman severity classification (used at scene and ED to grade severity, guide ventilation, and prognosticate):[3]
- Grade 1 — coughing, normal breathing, no findings on chest exam.
- Grade 2 — crepitations or wheeze in upper lung fields; SpO2 normal.
- Grade 3 — pulmonary oedema (crepitations throughout); SpO2 under 90 percent on air.
- Grade 4 — frank pulmonary oedema with respiratory failure; SpO2 under 90 percent despite oxygen.
- Grade 5 — respiratory arrest (apnoea), pulse present.
- Grade 6 — cardiac arrest (no pulse).[6]
Why is "wet vs dry" or a big electrolyte disturbance no longer central? Because (i) the volume aspirated in human drowning is small (a few mL/kg), so the dramatic electrolyte and haemolysis changes of animal experiments rarely occur in real patients, and (ii) the dry/wet distinction does not change management — both are treated by oxygenation. The retained classification is by clinical severity, not by water volume or type.[1][3]
Management — Resuscitation
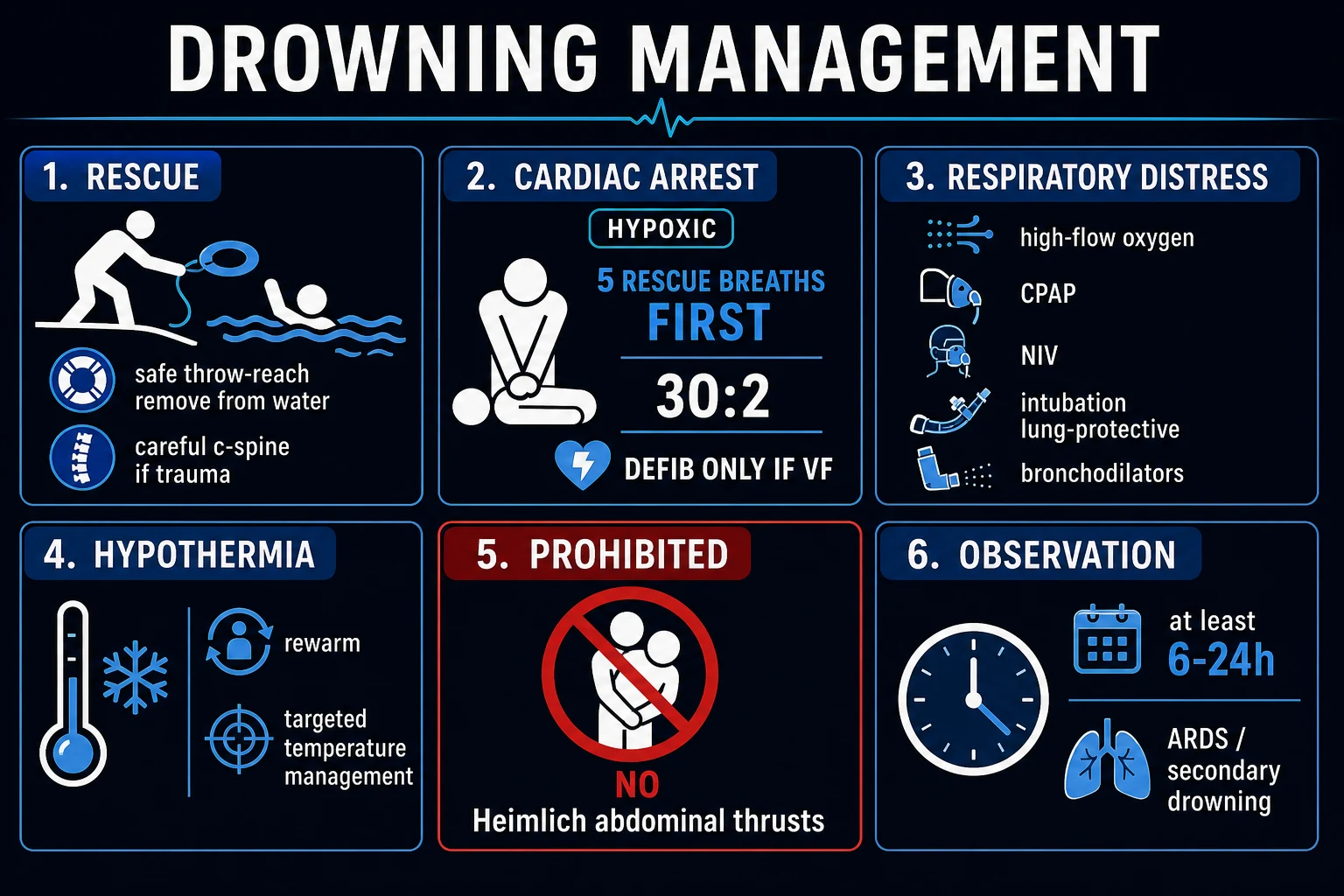
Drowning resuscitation is built around a single physiological fact: the arrest is hypoxic, so ventilation comes first. The sequence is:[5][6]
BLS for drowning cardiac arrest
Safe rescue (reach/throw before go); remove from water carefully; do NOT compress in the water.
Assess responsiveness, then breathing for up to 10 s (agonal gasps are NOT breathing).
Give 5 initial RESCUE BREATHS (each ~1 s, enough to make the chest rise) — oxygenate the flooded, hypoxic lungs FIRST.
Check for a pulse; if no pulse, start chest compressions at 30:2.
Continue CPR; attach an AED as soon as available (DRY the chest first); defibrillate ONLY if a shockable rhythm (VF/pVT) — uncommon.
Use bag-valve-mask + oxygen as soon as available; prepare for early intubation if ongoing arrest.
Consider the cause: hypothermia, trauma/cervical spine, channelopathy; rewarm, immobilise if indicated.
Do NOT use abdominal thrusts / Heimlich; do NOT attempt to drain water from the lungs.
Why 5 rescue breaths first? In drowning the lungs are flooded, collapsed, and full of shunt; the first few breaths go into recruiting and oxygenating alveoli before there is any point in circulating blood through them. The AHA/AAP and ERC therefore recommend 5 initial rescue breaths before chest compressions in drowning — a deliberate departure from the standard primary-cardiac-arrest sequence that begins with compressions.[5][6]
Why NO Heimlich / abdominal thrusts? Abdominal thrusts do not remove significant water from the lungs (water is in the alveoli and distal airways, not the upper airway), they delay CPR, and they cause regurgitation, aspiration, and intra-abdominal injury. Water that is present in the upper airway drains out with the airway open and the patient on the side; do not delay CPR to "drain" the lungs.[5]
The hypoxic but breathing victim. For the grade 3 to 4 patient with pulmonary oedema and hypoxia, the priority is oxygenation, escalating as needed:[5]
- High-flow oxygen via non-rebreather mask (15 L/min) to target SpO2 of 94 to 98 percent.
- CPAP or NIV (non-invasive ventilation) early for pulmonary oedema and moderate ARDS — early NIV reduces the need for intubation in paediatric drowning pulmonary oedema.[7]
- Intubation and mechanical ventilation if the patient is comatose, failing NIV, in respiratory arrest, or with refractory hypoxia — use lung-protective ventilation (low tidal volume 6 mL/kg ideal body weight, PEEP titrated, permissive hypercapnia).
Oxygenation targets. Aim for SpO2 94 to 98 percent in most victims; in known CO2 retainers (COPD) 88 to 92 percent. Avoid both profound hypoxia (which worsens brain injury) and hyperoxia (which may worsen reperfusion injury after cardiac arrest).[5]
Hypothermia during resuscitation. Rewarm gently but effectively; do NOT withhold CPR for a slow faint pulse in hypothermia; defibrillate up to 3 shocks if VF/pVT, but if the rhythm does not convert and the core temperature is under 30 degrees C, withhold further shocks until rewarming has raised the core temperature above 30 degrees C (the cold myocardium is unresponsive to defibrillation and to adrenaline). "Not dead until warm and dead" — continue resuscitation until the core temperature is at least 32 degrees C and asystole persists.[6]
AED use. Apply as soon as the chest is dry and the victim is on a hard surface; the value is mainly to detect the uncommon shockable rhythm in a drowning arrest (and any primary cardiac cause). Dry the chest before applying pads.[5]
Management — Definitive & Stepwise
Once the immediate threat is controlled, definitive management is organ-supportive — there is no antidote, no specific drug, and no manoeuvre that "cures" drowning. The aim is to prevent further hypoxic injury, support the injured lung and brain, and treat complications. The stepwise in-hospital approach is:[3][5]
1. Continued oxygenation and ventilation. Maintain SpO2 94 to 98 percent (or 88 to 92 percent in COPD); for intubated patients with ARDS use a lung-protective strategy: tidal volume 6 mL/kg ideal body weight, plateau pressure under 30 cmH2O, PEEP titrated to optimise oxygenation (high PEEP is often needed to recruit collapsed alveoli), and permissive hypercapnia (allow PaCO2 to rise to maintain low tidal volumes) provided the pH is acceptable. In severe refractory hypoxaemia, consider prone positioning and inhaled pulmonary vasodilators (nitric oxide) as for any severe ARDS.[3]
2. Haemodynamic support. Most symptomatic victims are hypovolaemic (fluid loss into the lung, vasodilation, capillary leak). Give balanced crystalloid (Hartmann's or Plasma-Lyte) boluses of 10 to 20 mL/kg titrated to perfusion (lactate, capillary refill, urine output over 0.5 mL/kg/h, MAP over 65 mmHg); avoid excess crystalloid in established pulmonary oedema. Use noradrenaline as first-line vasopressor for refractory shock; add adrenaline if myocardial stunning dominates. Correct hypoglycaemia and electrolyte derangements.[5]
3. Targeted temperature management (TTM) after cardiac arrest. For the drowned victim who has return of spontaneous circulation (ROSC) but remains comatose, apply the same TTM as for any post-cardiac-arrest patient — target 32 to 36 degrees C for 24 hours, followed by controlled normothermia (avoid fever). This reduces hypoxic-ischaemic brain injury. In the hypothermic drowning victim, do not actively cool an already-cold patient — instead rewarm to the target TTM range and then maintain.[5][6]
4. Neuroprotection and neuroprognostication. The brain is the organ that decides outcome. Maintain adequate cerebral perfusion (avoid hypotension), normoglycaemia, normocapnia (both hypo- and hypercapnia raise intracranial pressure), and treat seizures. Do not prognosticate before 72 hours of normothermia, and use a multimodal assessment (clinical exam, somatosensory evoked potentials, EEG, neuroimaging, biomarkers) — single predictors are unreliable, especially after hypothermia.[6]
5. Antibiotics — selective, NEVER routine. Prophylactic antibiotics are NOT recommended for the routine drowning victim: most aspiration is sterile chemical pneumonitis, and empirical antibiotics select resistant organisms. Do give antibiotics when there is clinical evidence of infection (fever, rising inflammatory markers, purulent sputum, new infiltrate after 48 hours), gross aspiration of contaminated water (sewage, stagnant or contaminated water, hot-tub/whirlpool), or a positive culture. Cover oral flora plus Gram-negatives (e.g., piperacillin-tazobactam 4.5 g IV every 8 hours or ceftriaxone 2 g IV daily + metronidazole 500 mg IV every 8 hours); add cover for Aeromonas, Vibrio, and Pseudomonas in brackish/sea-water or contaminated water (consider ciprofloxacin + a beta-lactam); adjust to cultures.[3]
6. Drugs NOT recommended routinely. Corticosteroids do not improve outcome in drowning ARDS or aspiration and are not recommended. Exogenous surfactant has theoretical appeal (the injured lung is surfactant-deficient) but is not recommended routinely; small studies are inconclusive. Barbiturate coma, deep sedation beyond standard TTM, and aggressive hyperventilation are not supported.[3][5]
7. Extracorporeal life support (ECMO / ECPR). In refractory cardiac arrest, severe refractory hypoxaemia, or profound hypothermia unresponsive to conventional rewarming, veno-arterial ECMO (and in hypothermia, extracorporeal rewarming) can be life-saving — particularly in the hypothermic victim with circulatory arrest, where ECMO both rewarms and supports the circulation. Referral criteria: witnessed arrest, brief no-flow time, good-quality CPR, age under 70 typically, reversible cause, and a centre capable of cannulation within ~60 minutes. ECMO rewarming is the method of choice for hypothermic cardiac arrest under 28 degrees C with circulatory arrest.[6]
8. Cervical spine clearance. In victims with a concerning mechanism, obtain a CT cervical spine and immobilise until cleared; in the unresponsive patient, imaging rather than clinical clearance. Do not let immobilisation delay oxygenation or CPR.[5]
9. Observation and discharge. A symptomatic victim (any cough, dyspnoea, vomiting, abnormal saturation or respiratory rate) is admitted and observed for at least 6 to 24 hours with serial observations and repeat CXR if symptoms evolve. An asymptomatic victim with normal observations and examination can be observed for 6 hours and discharged if well, with safety-net advice to return immediately if cough, breathlessness, chest pain, or drowsiness develops.[3][4]
10. Prevention bundle (the public-health intervention that actually saves lives): four-sided isolation pool fencing (the most evidence-based single intervention), constant adult supervision of children (within arm's reach, no distraction), lifejacket use on the water, alcohol avoidance in and around water, swimming and water-safety instruction, and trained lifeguard presence.[4]
Specific Subtypes & Scenarios
Cold-water submersion / hypothermic drowning. Especially in children, very prolonged cold-water submersion can be survived neurologically intact because the diving reflex plus hypothermia reduce cerebral metabolic rate. Resuscitate aggressively and do not terminate until the patient is warm and asystolic. Use extracorporeal rewarming for hypothermic arrest under 28 degrees C. Beware afterdrop (core temperature continues to fall after rescue as cold peripheral blood returns) and rewarming shock (vasodilation).[6]
Paediatric drowning. Children are the largest single group. Differences: smaller airway (use age-appropriate airway adjuncts and tube sizes; weight-based drug doses — adrenaline 10 microgram/kg IV/IO every 3 to 5 minutes in arrest, amiodarone 5 mg/kg for refractory VF/pVT), higher surface-area-to-mass (cool and dehydrate faster), and a lower threshold for hypoglycaemia (check and treat glucose). Observation and the prevention message (four-sided pool fencing, supervision) are paramount. Early NIV is effective in paediatric drowning pulmonary oedema.[7]
Shallow-water blackout (breath-hold diver). The diver (often a fit young man, often a swimmer or spear-fisher) is found unconscious underwater after hyperventilating to prolong the dive. Mechanism (PaO2 falls below the consciousness threshold before PaCO2 rises to the breath-hold-breaking threshold) is detailed above. Recognition is by the history; management is standard drowning resuscitation. Prevention — never hyperventilate before a breath-hold dive — is the entire public-health message.[4]
Diving / scuba-related drowning with arterial gas embolism. A breath-hold or scuba diver who surfaces and develops sudden neurological deficit (confusion, weakness, collapse, seizure) within minutes of ascent has arterial gas embolism from pulmonary barotrauma until proven otherwise. Give 100 percent oxygen, position supine (or left lateral if vomiting), exclude and treat pneumothorax (chest decompression if tension), and arrange urgent hyperbaric recompression. This is a separate disease from simple drowning but commonly co-presents.[3]
Seizure-related drowning. The seizure is the precipitant; bathtubs are the highest-risk site in epilepsy. Manage both the seizure (benzodiazepine if ongoing) and the drowning; counsel about showering instead of bathing and supervised swimming.[4]
Suspected channelopathy drowning (unexplained, exertional, or young). Any unexplained drowning — especially in a young, apparently healthy swimmer, exertional, or with a family history of sudden death — warrants an ECG (QTc), consideration of Brugada and CPVT, and cascade family screening. The index victim may be dead, but a living relative may have a treatable channelopathy (beta-blocker, left cardiac sympathetic denervation, ICD depending on the syndrome).[2][8]
Secondary drowning / post-immersion respiratory distress. The victim deteriorates hours after rescue with cough, dyspnoea, hypoxia, and infiltrates. Workup: SpO2, ABG, CXR, bloods; admit, oxygenate (escalate to NIV or intubation as needed), treat as ARDS. This is the rationale for the mandatory observation period.[3]
Complications & Pitfalls
Pulmonary: ARDS (the main morbidity in survivors), aspiration pneumonia (especially after contaminated-water aspiration), pneumothorax / pneumomediastinum (from barotrauma, especially in divers), and lung abscess / empyema from infected aspiration. Cardiovascular: arrhythmia (from hypoxia, hypothermia, or channelopathy), myocardial stunning. Neurological: hypoxic-ischaemic encephalopathy (the dominant determinant of outcome), seizures, cerebral oedema, persistent vegetative state; rhabdomyolysis and acute kidney injury (from prolonged immersion, hypoxia, or cold); disseminated intravascular coagulation; hypothermia and its complications.[3]
Classic pitfalls (examiner favourites):[3]
Prognosis & Disposition
Outcome is driven overwhelmingly by the severity and duration of hypoxia, summarised by the duration of submersion, the promptness and quality of resuscitation, the victim's temperature, and the initial rhythm.[3][5]
Favourable prognostic factors: submersion time under 5 to 10 minutes, bystander CPR started promptly (especially rescue breaths), good-quality neurological status at scene, cold water (paradoxically — hypothermia is neuroprotective, particularly in children), sinus rhythm or a shockable rhythm at first contact, and young age.[3]
Poor prognostic factors: submersion over 10 to 25 minutes, no bystander CPR or delayed CPR, asystole at scene, warm water, high blood lactate / severe acidosis, persistent coma, and GCS under 5 at any point.[3][8]
When to stop resuscitation. In a normothermic victim, an absence of ROSC despite 20 to 30 minutes of good-quality advanced life support is generally the basis to stop, provided reversible causes have been addressed. In the hypothermic victim this rule does not apply — continue (and consider ECMO) until rewarming to at least 32 degrees C and persistent asystole.[6]
Disposition:
- Home — asymptomatic after 6 hours of observation, normal observations and exam, reliable carer, safety-net given.
- Ward — symptomatic but stable (mild hypoxia, cough, observation required), monitoring and serial observations.
- HDU/ICU — moderate-to-severe hypoxia, ARDS, intubated/ventilated, post-cardiac-arrest coma, vasopressor requirement, severe hypothermia.[3]
Special Populations
- Children — leading cause of injury death; weight-based doses (adrenaline 10 microgram/kg, amiodarone 5 mg/kg, fluid bolus 10 to 20 mL/kg); smaller airway; check and treat hypoglycaemia; early NIV effective in pulmonary oedema; prevention is four-sided isolation pool fencing, constant supervision, and water-safety instruction.[4][7]
- Pregnancy — drowning resuscitation in pregnancy follows standard ALS with manual left uterine displacement (or 15 to 30 degree left lateral tilt) from 20 weeks to relieve aortocaval compression; target SpO2 over 94 percent for the fetus; perimortem Caesarean (resuscitative hysterotomy) at over 20 weeks gestation if no ROSC within 4 minutes, performed within 5 minutes of arrest — it can save both mother and fetus and improves maternal venous return.
- Elderly — atypical presentation, comorbidity, polypharmacy (especially QT-prolonging drugs and beta-blockers), higher hypothermia risk; consider a primary cardiac or syncopal cause.
- The channelopathy family — any unexplained, exertional, or youthful drowning: ECG (QTc), genetic and clinical cascade screening of first-degree relatives; treatable conditions (beta-blocker, denervation, ICD) may be found.[2]
- Immunocompromised / contaminated-water aspiration — broader antibiotic cover (oral flora plus Gram-negatives plus, for sea/brackish water, Aeromonas, Vibrio); higher index of suspicion for pneumonia and sepsis.[3]
- Rural / LMIC context — emphasise bystander rescue breaths and CPR (the biggest modifiable factor), early notification of EMS, prevention (fencing, supervision, lifejackets, swim instruction), and realistic triage where ECMO is unavailable.
Evidence, Guidelines & Regional Differences
The 2024 AHA/AAP Focused Update on Resuscitation Following Drowning (Dezfulian et al., Circulation 2024) consolidated and updated the resuscitation evidence. Key points: confirm 5 initial rescue breaths then 30:2 for drowning BLS; do not routinely immobilise the cervical spine; do not use abdominal thrusts; use an AED once the chest is dry; emphasise early oxygenation and NIV; and apply TTM 32 to 36 degrees C after ROSC. It also reinforced the role of ECMO/ECPR in selected refractory cases and the imperative to continue resuscitation in hypothermia.[5]
The ERC 2021 'Cardiac arrest in special circumstances' guideline (Lott et al.) covers drowning with the same principles — 5 rescue breaths first, no Heimlich, selective C-spine immobilisation, rewarm before stopping, ECMO for refractory hypothermic arrest, and TTM after ROSC.[6]
The Utstein-style consensus (Idris et al., 2015/2017) and its 2018 review (Venema et al.) standardised the dataset and terminology, allowing drowning studies and registries to be compared — a precondition for evidence-based practice.[2][8]
Controversies:
- Routine prophylactic surfactant or corticosteroids — current evidence does NOT support routine use; surfactant remains a research question in severe ARDS.
- In-water CPR — in-water rescue breaths (not compressions) by a trained lifeguard may help an apnoeic victim during a long tow, but is not generally recommended for untrained rescuers because of the risk to the rescuer.
- ECPR/ECMO — emerging evidence supports ECMO for refractory drowning arrest in expert centres; selection (witnessed, brief no-flow, young, reversible) determines outcome; not universally available.
- Prognostication — no single factor reliably predicts outcome; multimodal assessment after 72 hours of normothermia is required, and survival with good neurological outcome after very prolonged submersion (especially in cold water and children) means early prognostication is unreliable and dangerous.[3]
Australia and New Zealand have among the highest drowning-awareness programmes globally (Royal Life Saving, Surf Life Saving). Prevention emphasises patrolled beaches, flags, lifejackets, pool fencing (legislated four-sided isolation fencing is mandatory in Australia and NZ), and rock-fishing lifejacket laws (NZ).
The WHO Global Report on Drowning (2014) and its 2017 implementation guide frame drowning as a neglected public-health problem and recommend community-based interventions: install barriers controlling access to water, provide safe places to swim, teach school-age children basic swimming and safe-rescue skills, train bystanders in safe rescue and resuscitation, strengthen public awareness, and enforce boating and water-transport safety. LMICs carry over 90 percent of the burden and benefit most from low-cost prevention.
Exam Pearls
DROWNING
One-liners examiners reward:[5]
- "Drowning is an asphyxial arrest — give 5 rescue breaths first, then 30:2; defib only if VF (rare)."[5]
- "The primary injury in drowning is hypoxia; the brain dies first; the heart arrests in asystole or PEA, not VF."[3]
- "'Near-drowning', 'dry drowning', 'wet drowning' and 'secondary drowning' are obsolete — use fatal/non-fatal drowning with or without morbidity."[1]
- "Never hyperventilate before a breath-hold dive — it causes shallow-water blackout."[4]
- "Not dead until warm and dead — continue resuscitation in the hypothermic drowning victim."[6]
- "No Heimlich; no routine antibiotics or steroids; no routine C-spine immobilisation."[5]
Frequently misremembered — correctly stated:[5]
- The aspirated volume in real human drowning is small; gross electrolyte disturbance and massive haemolysis are uncommon — do not expect or treat for them routinely.
- The 'dry vs wet' distinction does not change management — both are treated by oxygenation. The retained distinction is by clinical severity (Szpilman grade).
- A normal initial chest X-ray does NOT exclude later ARDS — observe and repeat.
- Cold water is paradoxically neuroprotective — prolonged submersion in cold water can be survived neurologically intact, especially in children; do not prognosticate early.
- In-water rescue breaths (not compressions) may be given by a trained lifeguard during a long tow; chest compressions are ineffective in the water.[3]
Exam application bank (NEET-PG / INICET)
One-line answer
Drowning is defined by the WHO as the process of experiencing respiratory impairment from submersion or immersion in liquid; outcomes are fatal drowning, non-fatal drowning with morbidity, or non-fatal drowning without morbidity (a rescue). The old terms 'near-drowning', 'dry drowning', 'wet drowning', 'active drowning' and 'secondary drowning' are obsolete. The primary injury is hypoxia produced by laryngospasm and/or aspiration of liquid into the alveoli, which washes out surfactant, collapses alveoli, causes non-cardiogenic pulmonary oedema and ventilation-perfusion mismatch, and may evolve over hours into acute respiratory distress syndrome (ARDS). The downstream killer is hypoxic cardiac arrest, which in drowning is asystolic or PEA — NOT ventricular fibrillation. The defining management principle is therefore oxygenation first: in cardiac arrest give 5 initial rescue breaths before
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard.[1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes.[5]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change.[1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each.[1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory.[5]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Drowning.
References
- [1]van Beeck EF, Branche CM, Szpilman D, Modell JH, Bierens JJ. A new definition of drowning: towards documentation and prevention of a global public health problem. Bulletin of the World Health Organization, 2005.PMID 16302042
- [2]Idris AH, Bierens JJLM, Perkins GD, Wenzel V, et al. 2015 revised Utstein-style recommended guidelines for uniform reporting of data from drowning-related resuscitation: An ILCOR advisory statement. Resuscitation, 2017.PMID 28728893
- [3]Szpilman D, Morgan PJ. Management for the Drowning Patient. Chest, 2021.PMID 33065105
- [4]Mott TF, Latimer KM. Prevention and Treatment of Drowning. American Family Physician, 2016.PMID 27035042
- [5]Dezfulian C, McCallin TE, Bierens J, et al. 2024 American Heart Association and American Academy of Pediatrics Focused Update on Special Circumstances: Resuscitation Following Drowning: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation, 2024.PMID 39530204
- [6]Lott C, Truhlar A, Alfonzo A, Barelli A, Gonzalez-Salvado V, Hinkelbein J, Nolan JP, Paal P, et al. European Resuscitation Council Guidelines 2021: Cardiac arrest in special circumstances. Resuscitation, 2021.PMID 33773826
- [7]Sik N, Senol HB, Caglar A, Yilmaz D, Duman M. Early application of non-invasive ventilation for children with pulmonary edema after drowning. Pediatrics International, 2022.PMID 34057774
- [8]Venema AM, Absalom AR, Idris AH, Bierens JJLM. Review of 14 drowning publications based on the Utstein style for drowning. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine, 2018.PMID 29566700