Emergency & Toxicology · Emergency & Toxicology
Lithium Toxicity
Also known as Lithium toxicity · Lithium poisoning · Lithium overdose · Lithium intoxication · Nephrogenic diabetes insipidus · SILENT syndrome
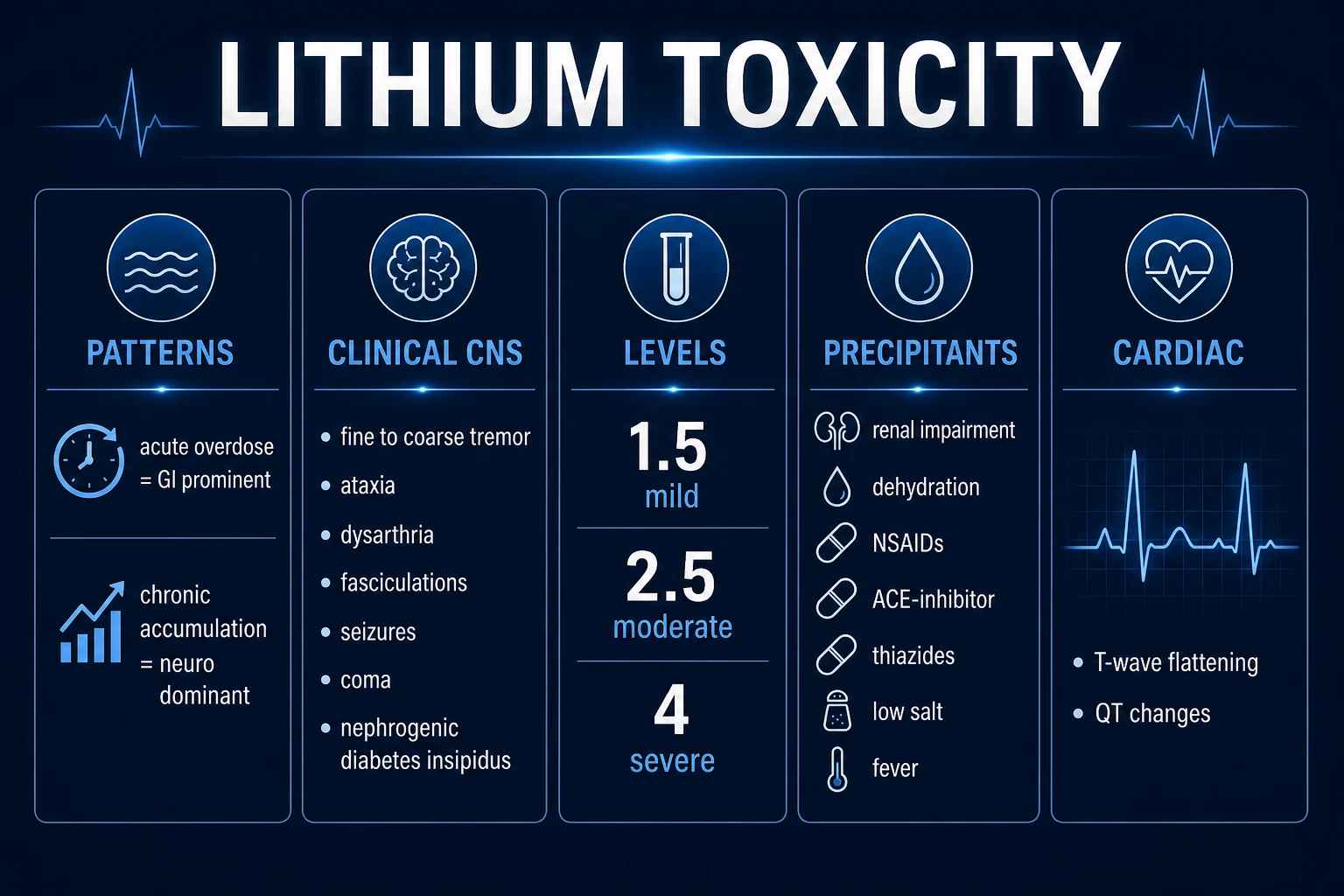
Lithium toxicity results from excess of lithium carbonate (the mood-stabiliser used for bipolar affective disorder prophylaxis), a drug with a narrow therapeutic index (therapeutic 0.6-1.2 mmol/L). Lithium is a small monovalent cation handled by the kidney like sodium — freely filtered, reabsorbed proximally, almost entirely renally excreted — so reduced GFR or sodium/water loss (dehydration, vomiting, diarrhoea, fever, low-salt diet) and interacting drugs (thiazides, NSAIDs, ACE-inhibitors/ARBs) are the classic precipitants of accumulation. Three patterns exist: acute overdose, acute-on-chronic, and chronic accumulation (the commonest and most dangerous). Toxicity is predominantly NEUROLOGICAL — fine tremor (earliest) progressing to coarse tremor, fasciculations, hyperreflexia, ataxia, dysarthria, seizures and coma — with nephrogenic diabetes insipidus (polyuria/polydipsia), GI (nausea/vomiting/diarrhoea, more in acute), cardiac (T-wave flattening, QT prolongation) and endocrine (hypothyroidism, hypercalcaemia) features. The key exam trap: acute overdose looks mild initially (distribution into the CNS lags serum by hours) whereas chronic toxicity is dangerous at lower levels (tissue already saturated) — so clinical correlation trumps the level. Diagnosis: serum lithium (over 1.5 mild, over 2.5 moderate, over 3.5-4.0 severe) plus renal function, electrolytes (Na, K, Ca), ECG, TFTs. Management: stop lithium, aggressive isotonic saline (the cornerstone — enhances renal excretion), haemodialysis for severe (EXTRIP criteria: impaired renal function with level over 4.0 mmol/L, or decreased consciousness/seizures/life-threatening dysrhythmia at any level), whole-bowel irrigation for sustained-release ingestion, and avoid activated charcoal (does not adsorb lithium), loop/thiazide diuretics, NSAIDs and ACE-inhibitors. Recheck levels after dialysis because of rebound.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Exam tags
Red flags

Overview & Definition
Lithium toxicity is the clinical and biochemical syndrome produced by an excess of lithium — almost always lithium carbonate, the mood-stabiliser used for prophylaxis of bipolar affective disorder. Toxicity is fundamentally a CLINICAL diagnosis correlated with the serum lithium level, not defined by the number alone, because the same serum value can be harmless (acute overdose in the distribution phase) or life-threatening (chronic tissue-saturated accumulation).[1]
Lithium remains a first-line maintenance mood stabiliser because of its proven efficacy against bipolar relapse and its unique anti-suicidal effect, but its use is constrained by a narrow therapeutic index — the toxic dose is only slightly above the therapeutic dose — and by complete dependence on the kidney for clearance. These two properties make toxicity common and frequently examined. The therapeutic serum range is 0.6-1.2 mmol/L (a tighter 0.6-0.8 mmol/L target is used in the elderly); toxicity is conventionally graded mild (over 1.5 mmol/L), moderate (over 2.5 mmol/L) and severe (over 3.5-4.0 mmol/L).[1]
The topic is high-yield for six reasons: the three temporal patterns of poisoning (acute, acute-on-chronic, chronic), the mechanistic link to sodium handling that explains the precipitants, the predominantly neurological clinical picture (tremor -> ataxia -> seizures -> coma), nephrogenic diabetes insipidus, the specific management (aggressive saline + haemodialysis, NOT charcoal or diuretics), and the EXTRIP dialysis criteria. The classic exam trap is the patient who looks well after an acute overdose (distribution incomplete) and then deteriorates at 6-12 hours — or the elderly bipolar patient on a diuretic whose "delirium" is chronic lithium toxicity.[3]
Classification
Lithium poisoning is classified by temporal pattern, and this classification is not a formality — it determines the relationship between the serum level and the body burden, and therefore the threshold for dialysis.[1]
Acute overdose
- Single large ingestion (deliberate self-harm, accidental, paediatric)
- GI features prominent early (nausea, vomiting, diarrhoea) — local irritation
- Neurological signs initially MILD — distribution into CNS incomplete
- Serum level may be very high but under-represents tissue burden
- Recheck level every 2-4 h; whole-bowel irrigation if sustained-release
- Dialyse by EXTRIP criteria (over 4.0 mmol/L, or ↓consciousness/seizures/dysrhythmia)
Acute-on-chronic
- Maintenance patient takes an EXTRA overdose on top of therapy
- Combines tissue saturation with a fresh load — often severe
- Neurology develops faster than pure acute (tissues already loaded)
- Manage as chronic — LOWER threshold for dialysis
Chronic accumulation (commonest, most dangerous)
- Tissue stores already saturated; toxicity at LOWER serum levels
- Driven by reduced renal clearance — renal impairment, dehydration, drug interactions
- Neurological features DOMINATE: coarse tremor, ataxia, fasciculations, seizures
- Usually unintentional — the precipitant is an illness or new drug
- The serum level under-represents body burden — clinical correlation key
Lithium toxicity is also classified by severity grade, reproduced verbatim because the thresholds are themselves the answer to many MCQs: [1]
Lithium — level thresholds
It is essential to grasp that the level and the pattern must be read together: a level of 2.0 mmol/L in a chronically toxic, tissue-saturated elderly patient with ataxia and seizures is far more dangerous than a level of 4.0 mmol/L drawn one hour after an acute overdose in an alert patient. Clinical correlation trumps the number.[1]
Epidemiology & Risk Factors
Lithium toxicity is common because the drug's therapeutic index is narrow and its clearance is entirely renal, concentrating risk in the elderly and in patients on interacting drugs. The chronic accumulative pattern is the commonest presentation — an unintentional build-up driven by reduced clearance in a treated patient — while acute deliberate overdose is less common but dramatic.[1]
Patient-related precipitants (reduced renal clearance):
- Renal impairment — lithium is almost entirely renally excreted (over 95 per cent), so falling GFR is the single biggest driver of accumulation. Dose and monitor by renal function.
- Advanced age — reduced GFR, sarcopenia (lower Vd raises the serum level), polypharmacy.
- Low lean body mass — lithium distributes into total body water; less water means a higher level for a given dose. [1]
Volume-status / sodium-status precipitants (the high-yield group):
- Dehydration — reduces filtered load and enhances proximal lithium reabsorption.
- Vomiting, diarrhoea — volume and sodium loss; the patient on lithium who gets gastroenteritis is a classic exam stem.
- Fever / sweating / heat exposure — salt and water loss.
- Low-salt diet — the proximal tubule conserves sodium (and therefore lithium); a low-salt diet or salt-losing state raises lithium levels.[2]
The mechanism behind these precipitants is lithium's sodium-like renal handling, which is the single most important concept in the topic: lithium is filtered at the glomerulus and then reabsorbed in the proximal tubule through the same sodium-transport pathways as sodium. Anything that increases proximal sodium reabsorption (volume depletion, low salt, NSAIDs, thiazides) increases lithium reabsorption and raises serum lithium — the kidney cannot tell lithium from sodium.[2]
Drug interactions that raise lithium levels (the high-yield list): [1]
Diuretics
- THIAZIDE — the classic exam precipitant; causes sodium/volume loss -> ↑ proximal lithium reabsorption; effect within days; halve lithium dose if a thiazide is essential
- LOOP — variable; can raise lithium; risk of late toxicity
- Osmotic diuretics (mannitol) actually increase lithium excretion — not used therapeutically for this
NSAIDs
- Reduce renal prostaglandin synthesis -> afferent arteriolar constriction -> reduced GFR and lithium clearance
- Diclofenac, indometacin, ibuprofen, naproxen — high risk
- Sulindac and the COX-2 selective NSAIDs (celecoxib) have a smaller, variable effect
ACE-inhibitors / ARBs
- Reduce angiotensin-II-mediated efferent arteriolar tone -> reduced GFR -> lithium retention
- Particularly risky in the volume-depleted patient; a frequent precipitant in the elderly
Others
- Metronidazole — reduces renal lithium excretion
- Some calcium-channel blockers (e.g. verapamil, diltiazem) — variable interaction
- Iodine / amiodarone — additive thyroid effect (not lithium level, but thyroid toxicity)
In many low- and middle-income settings (including much of India), sodium valproate is preferred over lithium for bipolar prophylaxis on grounds of cost, availability and the monitoring burden of lithium — but lithium toxicity still occurs and the recognition and management principles are identical.
Pathophysiology
The molecular and physiological mechanism is the single most frequently examined concept and must be reproduced in full, because it explains every precipitant, every clinical feature and every treatment decision.[2]
Step 1 — lithium is a sodium-substitute cation. Lithium is a small monovalent cation that substitutes for sodium (and, to a lesser extent, potassium, calcium and magnesium) in ion channels and transporters throughout the body. This single property underlies both its therapeutic action and its toxic profile across many organs.[2]
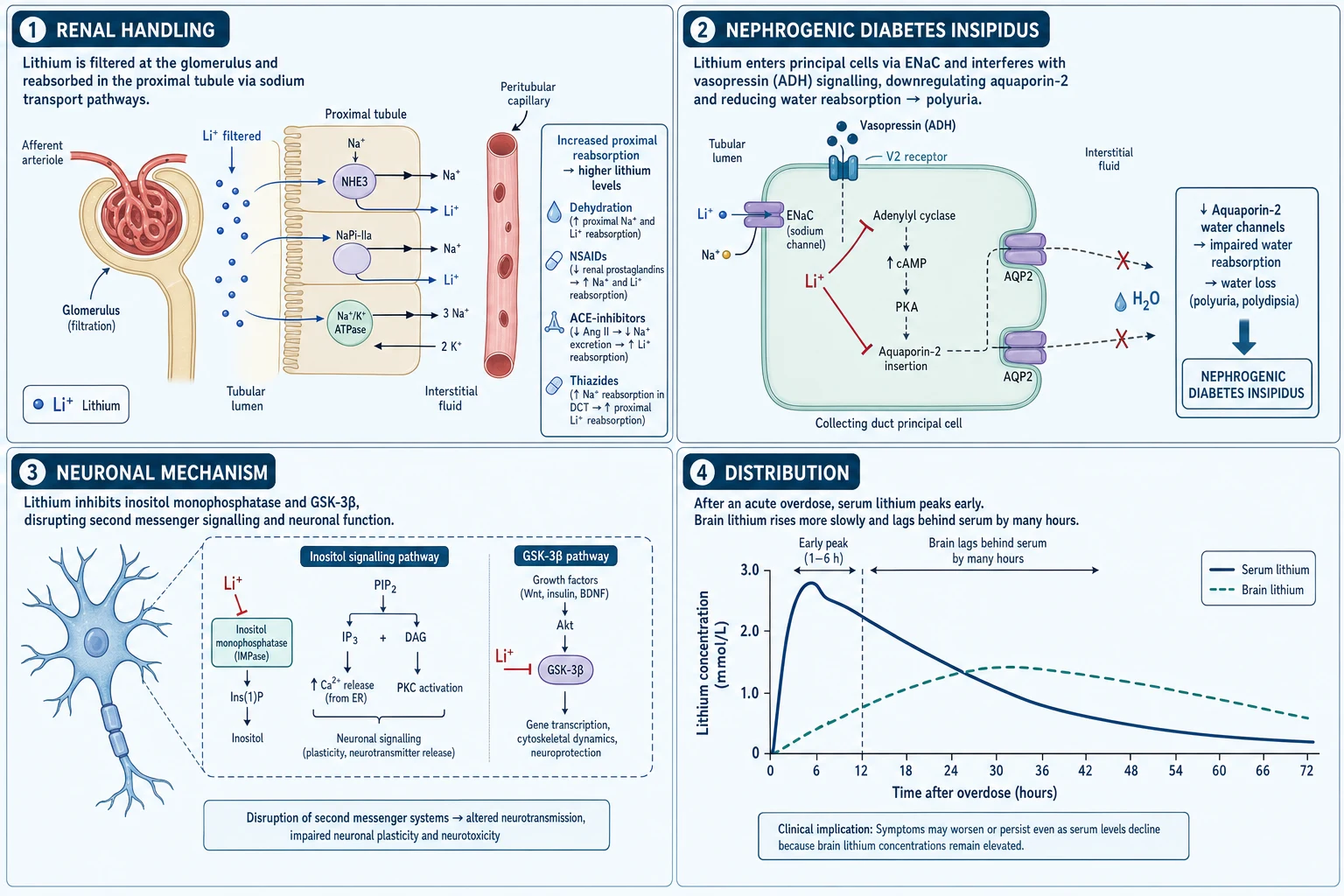
Step 2 — distribution kinetics explain the acute-vs-chronic difference. After ingestion, lithium distributes first into the extracellular fluid / total body water, then slowly into cells and across the blood-brain barrier into the CNS. Peak brain levels lag serum levels by 6-8 hours or more. The consequences are pivotal:
- In an acute overdose, the serum level is high but the tissue/CNS burden is initially low — the patient looks well and neurology is delayed. As distribution completes over hours, the patient can deteriorate dramatically.
- In chronic accumulation, the tissues are already saturated, so the serum level under-represents the body burden — toxicity occurs at lower serum levels, and neurological features dominate.[1]
Step 3 — renal handling explains every precipitant. Lithium is freely filtered at the glomerulus, then reabsorbed (60-80 per cent) in the proximal tubule through the same sodium-transport mechanisms as sodium — the sodium-hydrogen exchanger and, further downstream, the epithelial sodium channel (ENaC) in the collecting duct. Almost all filtered lithium is excreted in urine — there is no other significant clearance route. Therefore anything that increases proximal sodium reabsorption (volume depletion, low salt, NSAIDs, thiazides) increases lithium reabsorption and raises serum lithium; and anything that reduces GFR (renal impairment, ACE-inhibitors, NSAIDs) reduces lithium clearance. Restoring euvolaemia and filtered sodium load with saline enhances lithium excretion — the basis of the cornerstone treatment.[2]
Step 4 — nephrogenic diabetes insipidus. In the collecting duct, lithium enters principal cells via ENaC and, because the cell cannot extrude it as efficiently as sodium, accumulates intracellularly. It then blocks the vasopressin V2-receptor / Gs / cyclic-AMP signalling cascade, producing downregulation and mistargeting of aquaporin-2 (AQP2) water channels. The result is reduced water reabsorption — polyuria of dilute urine, polydipsia, and the free-water loss that can produce hypernatraemia. The polyuria and thirst drive further fluid/sodium disturbance, which in turn worsens lithium retention — a vicious cycle. Chronic lithium therapy also causes a chronic tubulointerstitial nephritis with long-term use.[2]
Step 5 — neuronal mechanism of toxicity. In the CNS, lithium inhibits inositol monophosphatase, depleting intracellular inositol and disrupting the phosphatidylinositol second-messenger cycle (this inositol-depletion is the basis of its antimanic action). It also inhibits glycogen synthase kinase-3β (GSK-3β). In excess, these effects — together with direct cation-substitution effects on neuronal excitability and neurotransmitter release — disrupt neuronal and especially cerebellar function, producing the characteristic tremor, ataxia, dysarthria, nystagmus, fasciculations, seizures and coma.[1]
Step 6 — why the cerebellum is vulnerable and why deficits may persist. The cerebellum is particularly sensitive to lithium, which is why cerebellar signs (ataxia, dysarthria, nystagmus) dominate the clinical picture. After severe or chronic poisoning, neurological deficits may persist for weeks or months after the serum level has normalised — the Syndrome of Irreversible Lithium-Effectuated Neurotoxicity (SILENT), which is uncommon but well described and carries a predominantly cerebellar and cognitive phenotype.[1]
Step 7 — endocrine and cardiac effects. Lithium inhibits thyroid hormone release (producing goitre and hypothyroidism), stimulates parathyroid gland activity (lithium-induced hyperparathyroidism with hypercalcaemia), and — by sodium-channel substitution in the heart — produces T-wave flattening/inversion, QT prolongation and sinus node dysfunction. These are usually mild but can occasionally produce significant bradyarrhythmia.[1]
Clinical Presentation
The clinical picture is predominantly neurological — the CNS is the target organ — with renal, gastrointestinal, cardiac and endocrine components. The tempo differs by pattern: chronic toxicity creeps in over days to weeks, acute overdose evolves over hours as distribution completes.[1]
Mild toxicity:
- Fine hand tremor — the earliest and most sensitive sign (also a common side-effect at therapeutic levels, but a worsening or coarsening tremor signals toxicity).
- Lethargy, mild confusion, generalised weakness.
- Mild polyuria (early nephrogenic DI).
- Mild GI upset. [1]
Moderate toxicity (the classic exam picture):
- Coarse tremor, muscle fasciculations, hyperreflexia.
- Ataxia (gait and limb), dysarthria, nystagmus — cerebellar dysfunction.
- Apathy, drowsiness, slowing cognition.
- Prominent polyuria/polydipsia (nephrogenic DI). [1]
Severe toxicity (the danger):
- Generalised tonic-clonic seizures.
- Impaired consciousness progressing to coma.
- Hyperthermia and neuromuscular irritability (myoclonus, rigidity).
- Risk of permanent neurological injury (SILENT). [1]
Lithium toxicity — neurological ladder
Gastrointestinal features — nausea, vomiting, diarrhoea — are more prominent in acute overdose (direct GI irritation) and are often absent or mild in chronic accumulation. Their presence or absence is therefore a clue to the pattern.[1]
Renal features:
- Nephrogenic diabetes insipidus — polyuria (often several litres/day) of inappropriately dilute urine, polydipsia, and hypernatraemia from free-water loss.
- Acute kidney injury during the toxic episode (volume depletion + direct toxicity).
- Chronic lithium therapy: chronic tubulointerstitial nephritis with gradual GFR decline. [1]
Cardiac features — usually mild but examined: T-wave flattening/inversion, QT prolongation, sinus node dysfunction/bradycardia; rarely significant arrhythmia. The ECG is a routine investigation in any suspected case.[1]
Endocrine features of chronic therapy:
- Hypothyroidism (often with goitre) — lithium inhibits thyroid hormone release.
- Hypercalcaemia — lithium-induced hyperparathyroidism (always check calcium in a lithium patient).
- Weight gain. [1]
Atypical / deceptive presentations (the traps):
- The elderly bipolar patient on a diuretic/NSAID presenting with "delirium" or falls — chronic toxicity is missed unless lithium is actively considered.
- The patient who looks well after an acute overdose (distribution phase) and then deteriorates at 6-12 hours — never discharge a lithium overdose on a single early level.
- The patient with a mildly elevated level but severe neurology — chronic tissue saturation; treat the patient, not the number.[1]
Differential Diagnosis
The differential is driven by the presenting feature: a bipolar patient with tremor, ataxia, confusion and seizures, or polyuria, or delirium.[1]
Metabolic encephalopathies
- HYPERCALCAEMIA — which lithium itself can cause (lithium-induced hyperparathyroidism); a confounder
- Hyponatraemia — worsens lithium retention; can itself cause seizures/encephalopathy
- Hypernatraemia — free-water loss from lithium-induced nephrogenic DI
- Uraemic / hepatic encephalopathy, hypoglycaemia, hypoxia
Other drug-toxicity syndromes (the psychiatric patient)
- NEUROLEPTIC MALIGNANT SYNDROME — lead-pipe rigidity, marked CK elevation, antipsychotic exposure, fever
- SEROTONIN SYNDROME — clonus, hyperreflexia, autonomic instability, serotonergic agent (SSRI/SNRI/tramadol)
- Anticholinergic toxicity, TCA toxicity (QRS widening), benzodiazepine/opioid overdose
- These can CO-OCCUR in the polypharmacy psychiatric patient — easy to miss lithium toxicity
Primary neurological disease
- Meningoencephalitis, post-ictal state, cerebellar stroke
- Wernicke encephalopathy (ataxia, confusion, ophthalmoplegia — give thiamine)
- Space-occupying lesion, subdural haematoma (the ataxic/confused alcoholic patient)
Causes of polyuria (the renal presentation)
- Central diabetes insipidus, primary polydipsia (psychogenic), hyperglycaemic polyuria
- Distinguish by water-deprivation test / desmopressin response where needed
- Note: lithium-induced NDI does NOT respond to desmopressin (nephrogenic)
The decisive distinction within the topic itself is acute overdose vs chronic accumulation: in acute overdose the serum level is high but the patient is often initially well (distribution incomplete) and GI features dominate; in chronic accumulation the serum level is lower (often only mildly elevated) but the patient is neurologically unwell because the tissues are saturated. The pattern dictates the threshold for dialysis, not the level alone.[1]
Always ask explicitly about lithium — including herbal preparations and family members' medications — in any bipolar patient with new neurological signs, because the patient may not report lithium as a "drug" or the prescription may be unknown to the assessing team.[1]
Clinical & Bedside Assessment
Focused history:
- Indication and dosing — bipolar prophylaxis; the current dose and formulation (immediate vs sustained release — the latter prolongs absorption and the window for whole-bowel irrigation).
- Adherence and any recent dose change — toxicity from accumulation implies chronic therapy.
- Concurrent drugs — diuretics, NSAIDs, ACE-inhibitors/ARBs, metronidazole, antipsychotics/antidepressants.
- Renal function and recent illness — vomiting, diarrhoea, fever, infection, dehydration.
- Diet/fluid intake — low-salt diet, reduced fluid intake.
- Time since any overdose — critical for interpreting the level and the decontamination window.[1]
Focused neurological examination (the core):
- Tremor — fine then coarse.
- Muscle fasciculations, hyperreflexia, tone.
- Ataxia — gait and finger-nose; dysarthria, nystagmus (cerebellar).
- Level of consciousness (GCS) — a key severity marker.
- Clonus, myoclonus, rigidity and an active seizure assessment. [1]
Volume status and temperature:
- Tachycardia, postural drop, dry mucosae indicate dehydration, which drives lithium retention and must be corrected.
- Hyperthermia is a severe sign and prompts aggressive cooling and ICU. [1]
ECG — obtain a 12-lead and a rhythm strip and recognise the lithium pattern: T-wave flattening/inversion, QT prolongation, sinus bradycardia/sinus node dysfunction, and rarely a significant arrhythmia. Establish continuous cardiac monitoring and IV access for any moderate-to-severe case, and chart serial GCS observations.[1]
Investigations
First-line investigations: serum lithium level (repeat at 2-4-hour intervals after an acute overdose to track distribution and the rising tissue burden), urea, creatinine, eGFR, electrolytes (sodium, potassium, calcium, magnesium), venous blood gas, glucose, 12-lead ECG with continuous monitoring, thyroid function tests, FBC, urine and serum osmolality (to characterise nephrogenic DI), and beta-hCG in women of childbearing potential; paracetamol and salicylate levels in any deliberate overdose. An abdominal X-ray may show radiopaque sustained-release tablets — a clue to a recent large ingestion and the need for whole-bowel irrigation.[1]
ECG and biochemistry interpretation:
- Hyponatraemia worsens lithium retention and itself causes encephalopathy — correct sodium cautiously.
- Hypercalcaemia suggests lithium-induced hyperparathyroidism — a chronic complication and a differential for the confusion.
- Hypernatraemia suggests free-water loss from nephrogenic DI — manage fluids carefully.
- Renal impairment is both a precipitant and a complication — it also lowers the threshold for dialysis.[2]
Reproduce the EXTRIP Workgroup indications for extracorporeal treatment (haemodialysis) verbatim — the dialysis criteria are themselves an MCQ:[3]
- Impaired kidney function AND serum lithium over 4.0 mEq/L — RECOMMENDED.
- Decreased level of consciousness, seizures, OR life-threatening dysrhythmias — at ANY serum lithium level — RECOMMENDED.
- Serum lithium over 5.0 mEq/L, OR significant confusion, OR expected time to reduce the level below 1.0 mEq/L exceeds 36 hours — SUGGESTED.
- Continue extracorporeal treatment until clinical improvement is apparent OR the level is below 1.0 mEq/L; continue for a minimum of 6 hours if the level is not readily measurable.
Management — Resuscitation
Begin with ABCDE: secure the airway (low GCS or seizures may compromise it), give high-flow oxygen if hypoxic, establish IV access, attach continuous cardiac monitoring, and identify and treat immediately life-threatening problems (airway, seizures, arrhythmia) first.[1]
Immediate non-drug measures:
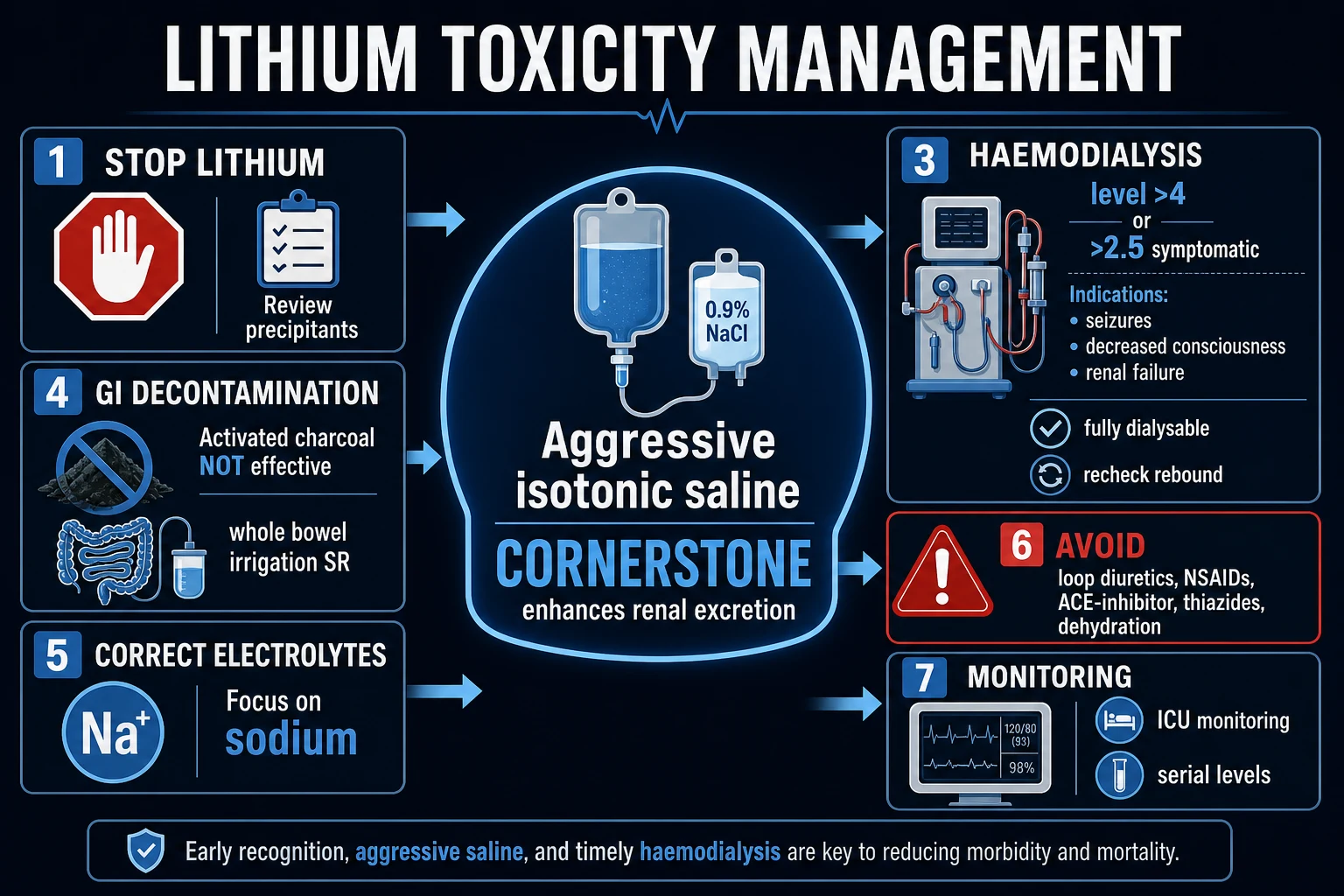
- STOP LITHIUM and review/stop the precipitants — NSAIDs, ACE-inhibitors/ARBs, thiazide/loop diuretics — and treat any underlying illness (infection, dehydration).[1]
Seizure resuscitation (seizures worsen outcome — control them aggressively):
- First-line IV benzodiazepine — lorazepam 4 mg IV (2 mg in the elderly) repeated at 5-10 minutes if needed, or diazepam 10 mg IV, or midazolam 10 mg IM if no IV access.[1]
The cornerstone resuscitative measure — aggressive isotonic saline. Give 0.9% sodium chloride IV to restore euvolaemia and the filtered sodium load, which enhances renal lithium excretion (the kidney handles lithium like sodium; restoring euvolaemia and filtered sodium promotes lithium clearance). Aim for euvolaemia then maintenance, monitoring closely for fluid overload (risk in renal failure or the elderly). This is the single most important intervention after stopping the drug.[2]
Airway / breathing / circulation support and an early critical-care referral for any decreased consciousness, seizures, significant arrhythmia, or renal failure.[1]
Management — Definitive & Stepwise
Stepwise ladder with escalation triggers:[1][3]
Lithium toxicity — stepwise management
Haemodialysis — the definitive modality for severe toxicity. Lithium is fully dialysable (small ion, negligible protein binding, small volume of distribution into the water compartment), so haemodialysis is highly effective at clearing it. Haemodialysis clears faster than continuous RRT, which is why EXTRIP prefers it for the index treatment; continuous RRT (CRRT) or sustained low-efficiency dialysis (SLED) are acceptable adjuncts to prevent the rebound that follows an isolated haemodialysis session.[3]
The rebound phenomenon — and how to manage it. After haemodialysis, lithium redistributes from the tissues back into the plasma and the serum level RISES again. Recheck the level at 4-6 hours after every dialysis session, and use SLED or CRRT as a follow-on to prevent rebound. The EXTRIP end-point is clinical improvement AND a level below 1.0 mEq/L.[3][4]
Decontamination — what works and what does not:
- Activated charcoal does NOT adsorb lithium effectively (lithium is a small metal cation). Do not give charcoal for an isolated lithium overdose — it is only useful if a relevant co-ingestant is suspected.
- Whole-bowel irrigation with polyethylene glycol 1-2 L/h via nasogastric tube is indicated for sustained-release formulations or a large recent ingestion, especially if tablets are visible on an abdominal X-ray.[1]
What to AVOID (high-yield):
- Dehydration — the kidney must clear the drug.
- NSAIDs — reduce renal lithium clearance.
- ACE-inhibitors / ARBs — reduce GFR and lithium clearance.
- Loop and thiazide diuretics — worsen renal lithium retention (loop is variable but risky; thiazide is the classic precipitant).
- Activated charcoal for isolated lithium overdose — ineffective. [1]
Urinary alkalinisation (sodium bicarbonate) has a limited and controversial role: it theoretically reduces proximal lithium reabsorption by altering the sodium gradient, but the evidence is weak and saline is the standard. It is not a substitute for saline or dialysis.[2]
Amiloride for lithium-induced nephrogenic diabetes insipidus — a specific, evidence-supported treatment: amiloride blocks ENaC channels in the collecting duct, reducing lithium entry into principal cells and ameliorating the aquaporin-2 downregulation. It is used on recovery / in the chronic NDI patient, not as an acute toxicity antidote.[2]
Escalation triggers to ICU: any decreased consciousness, seizures, significant arrhythmia, need for haemodialysis, renal failure, or haemodynamic instability.[1]
Specific Subtypes & Scenarios
- Chronic accumulation in the elderly/renal patient (the commonest scenario): vague neurological decline — coarse tremor, ataxia, confusion — with a precipitant (diuretic, NSAID, dehydration, infection). The serum level may be only moderately elevated but tissue is saturated. Management = stop, aggressive saline, dialyse if EXTRIP criteria met, correct electrolytes, review the maintenance dose and interacting drugs before any restart.[1]
- Acute deliberate overdose (suicidal): high serum level but neurological signs evolve over hours as distribution completes; GI features prominent early. Repeat the level every 2-4 hours to track the rising tissue burden; whole-bowel irrigation for sustained-release; dialyse by EXTRIP criteria (level over 4.0 mmol/L, or decreased consciousness/seizures/arrhythmia at any level). Never discharge on a single early level.[1]
- Acute-on-chronic overdose: a maintenance patient taking an extra overdose; combines tissue saturation with a fresh load and is often severe — manage as chronic (lower threshold for dialysis).[1]
- Lithium-induced nephrogenic diabetes insipidus: polyuria/polydipsia on therapy; confirm with urine/serum osmolality (inappropriately dilute urine despite raised serum osmolality/sodium; does not respond to desmopressin). Manage fluid balance carefully during the toxic episode (avoid hypernatraemia from free-water loss and avoid over-hydration in renal failure); consider amiloride on recovery.[2]
- The patient on lithium + diuretic/NSAID who becomes toxic: recognise the interaction as the precipitant; stop both drugs; counsel on avoidance at discharge (or reduce the lithium dose and monitor closely if the interacting drug is essential).[1]
Complications & Pitfalls
Neurological complications: seizures, coma, overlap with neuroleptic malignant syndrome / serotonin syndrome in the psychiatric polypharmacy patient, and the Syndrome of Irreversible Lithium-Effectuated Neurotoxicity (SILENT) — persistent cerebellar/cognitive deficits lasting weeks-to-months after the serum level has normalised, more common after chronic or severe poisoning.[1]
Renal complications: nephrogenic diabetes insipidus, chronic tubulointerstitial nephritis with long-term therapy (progressive GFR decline), and AKI from volume depletion and direct toxicity during the acute episode. [1]
Endocrine and metabolic complications: hypothyroidism (with goitre), hypercalcaemia (lithium-induced hyperparathyroidism), hypernatraemia (free-water loss from NDI), and weight gain.[1]
Classic pitfalls (high-yield):
- Treating the NUMBER, not the patient — chronic tissue-saturated toxicity is dangerous at lower serum levels than acute overdose.
- Relying on a SINGLE early level after acute overdose — distribution is incomplete; repeat every 2-4 hours.
- Giving activated charcoal for an isolated lithium overdose — it does not adsorb lithium.
- Giving a loop/thiazide diuretic or an NSAID — they worsen renal lithium retention.
- Missing the REBOUND after haemodialysis — recheck the level at 4-6 hours and use SLED/CRRT.
- Missing the concurrent nephrogenic DI and giving free-water incorrectly (hypernatraemia or overload).
- Missing the underlying precipitant interaction at discharge — the patient returns with the same problem. [1]
Why does a thiazide diuretic precipitate lithium toxicity?
A thiazide causes sodium and volume depletion, which makes the proximal tubule increase sodium reabsorption to conserve sodium. Because the kidney handles lithium through the same sodium-transport pathways, it reabsorbs more lithium too, raising the serum level — often within days. The correct response is to halve the lithium dose if a thiazide is essential, and monitor closely.
Prognosis & Disposition
Overall mortality of lithium poisoning is low (under 1 per cent in modern series), but the risk of prolonged morbidity — impaired mobility and cognition, nosocomial complications, and SILENT — is significant, especially after chronic or severe poisoning.[1]
Predictors of severity and poor outcome: chronic pattern, very high or rising serum level, advanced age, renal failure, decreased consciousness, seizures, delay to haemodialysis, and sustained-release formulation.[1]
Disposition:
- Asymptomatic / minimal toxicity with a corrected precipitant and a falling level — ward observation, hold the drug, recheck the level and renal function, restart at a reduced dose.
- Moderate-to-severe toxicity, any decreased consciousness, seizures, significant arrhythmia, or need for dialysis — ICU.
- After haemodialysis — monitor for rebound (recheck the level at 4-6 hours).[3]
Prevention at discharge: dose adjustment to renal function; avoid NSAIDs, thiazides and ACE-inhibitors/ARBs where possible (or reduce the lithium dose and monitor closely if essential); maintain hydration and salt intake during illness; counsel the patient to seek help with vomiting, diarrhoea or fever; establish regular monitoring of serum lithium, renal function, electrolytes and TFTs; and assess deliberate self-harm risk, referring to psychiatry where relevant.[1]
Special Populations
- Elderly: reduced renal clearance and GFR, polypharmacy (NSAIDs, ACE-inhibitors, diuretics), comorbidity and sarcopenia (reduced Vd raises the level) — the highest-risk chronic-toxicity group. Use a lower target level (0.6-0.8 mmol/L) and monitor closely.[1]
- Renal impairment: dramatically reduced clearance; the commonest driver of chronic accumulation. Dialyse by EXTRIP criteria. Long-term lithium risks chronic kidney disease — monitor eGFR every 3-6 months.[2]
- Pregnancy: lithium is teratogenic — Ebstein's anomaly (a malformation of the tricuspid valve and right heart, especially with first-trimester exposure) — so toxicity in pregnancy is doubly high-stakes. The management of toxicity is unchanged (saline, dialysis if EXTRIP criteria met). Involve obstetrics and perinatal psychiatry; note that lithium concentrates in breast milk.[2]
- Children / paediatric ingestion: even small numbers of adult tablets are dangerous; weight-based management; activated charcoal does not work; whole-bowel irrigation for sustained-release; dialyse by EXTRIP criteria.[1]
- Deliberate self-harm / psychiatric patient: assess intent, safeguarding and supply security; refer to psychiatry after medical stabilisation. The bipolar patient is at high baseline suicide risk.[1]
Evidence, Guidelines & Regional Differences
- EXTRIP Workgroup (Decker et al, CJASN 2015): the definitive systematic review and consensus on extracorporeal treatment for lithium poisoning, reviewing 166 articles (418 patients). It concluded that lithium IS dialysable (Level A) and issued the recommendations reproduced verbatim in the Investigations and Management sections — moving from a fixed level threshold to a clinical + kinetic approach (decreased consciousness, seizures, life-threatening dysrhythmia at ANY level), because chronic tissue-saturated toxicity is dangerous at lower serum levels than acute overdose. Haemodialysis is preferred for the index treatment; CRRT/SLED are acceptable adjuncts to prevent rebound.[3]
- Timmer & Sands (JASN 1999): the classic review of lithium intoxication that established the renal mechanism — lithium handled like sodium, proximally reabsorbed, causing nephrogenic diabetes insipidus through vasopressin/aquaporin disruption and chronic tubulointerstitial nephritis with long-term use.[2]
- Baird-Gunning et al (J Intensive Care Med 2017): the comprehensive modern review consolidating the three patterns, precipitants, clinical features and management, noting the low mortality but significant morbidity (SILENT) and the controversy over dialysis thresholds.[1]
- Waring (Toxicol Rev 2006): management review emphasising enhanced elimination for chronic and acute-on-therapeutic toxicity, the rebound phenomenon (haemodialysis clears circulating lithium effectively but serum rebounds, so repeated or prolonged treatment — including sustained haemodiafiltration over 16 hours — may be needed), and the threshold of chronic toxicity with level over 2.5 mmol/L for considering enhanced elimination.[4]
Controversies:
- The level threshold for dialysis — older recommendations used a fixed level (e.g. over 4.0 mmol/L); EXTRIP moved to a clinical + kinetic approach because the serum level alone does not reflect tissue burden in chronic toxicity.
- Haemodialysis vs continuous RRT vs SLED — haemodialysis clears fastest but causes the most rebound; CRRT/SLED clear slower but reduce rebound. Many units use haemodialysis followed by SLED/CRRT. The choice depends on availability and rebound risk.
- Urinary alkalinisation — theoretically reduces proximal lithium reabsorption, but evidence is weak; saline remains the standard.[3]
In many low- and middle-income settings (including much of India), sodium valproate is preferred over lithium for bipolar prophylaxis on grounds of cost, availability and monitoring burden, but lithium toxicity still occurs and the recognition and management principles are identical.
Exam Pearls
Lithium toxicity — LITHIUM mnemonic
LITHIUM
narrow index — 0.6-1.2 mmol/L therapeutic; over 1.5 mild, over 2.5 moderate, over 3.5-4.0 severe (dialysis)
thiazides, NSAIDs, ACE-i/ARBs, loop diuretics, metronidazole — raise lithium (handled like sodium)
neurological ladder: fine tremor (earliest) -> coarse tremor, fasciculations, ataxia, dysarthria -> seizures, coma
for severe — EXTRIP: impaired renal function + over 4.0, OR ↓consciousness/seizures/dysrhythmia at ANY level; recheck for rebound at 4-6 h
0.9% NaCl — the cornerstone; restores euvolaemia and filtered sodium -> enhances renal lithium excretion
nephrogenic diabetes insipidus — lithium blocks vasopressin signalling -> aquaporin-2 downregulation -> polyuria; amiloride on recovery
acute overdose looks mild initially (CNS distribution lags by hours); chronic is dangerous at LOWER levels — treat the patient, not the number
- Mechanism one-liner: lithium is a monovalent cation handled like sodium — renally excreted, proximally reabsorbed, distributed slowly into the CNS; toxicity is predominantly neurological.
- Three patterns: acute (GI early, neuro evolves), acute-on-chronic, chronic (commonest, neuro dominates at lower levels).
- Severity by level: over 1.5 mild, over 2.5 moderate, over 3.5-4.0 severe (dialysis).
- Precipitants: renal failure, dehydration/vomiting/diarrhoea/fever, low salt, thiazides, NSAIDs, ACE-i/ARBs.
- Nephrogenic DI: lithium blocks vasopressin signalling -> aquaporin-2 downregulation -> polyuria; amiloride is the specific treatment.
- Treatment: stop lithium + aggressive isotonic saline (cornerstone); haemodialysis for severe (EXTRIP); whole-bowel irrigation for sustained-release.
- Avoid: activated charcoal (ineffective), loop/thiazide diuretics, NSAIDs, ACE-i.
- Rebound after haemodialysis — recheck level at 4-6 h; SLED/CRRT to prevent.
- SILENT — Syndrome of Irreversible Lithium-Effectuated Neurotoxicity: persistent cerebellar/cognitive deficits after the level normalises.
- Chronic endocrine: hypothyroidism (goitre) and hypercalcaemia (lithium-induced hyperparathyroidism).
- Teratogenic: Ebstein's anomaly (right heart). Fully dialysable (small ion, no protein binding). [1]
Exam application bank (NEET-PG / INICET)
One-line answer
Lithium toxicity results from excess of lithium carbonate (the mood-stabiliser used for bipolar affective disorder prophylaxis), a drug with a narrow therapeutic index (therapeutic 0.6-1.2 mmol/L). Lithium is a small monovalent cation handled by the kidney like sodium — freely filtered, reabsorbed proximally, almost entirely renally excreted — so reduced GFR or sodium/water loss (dehydration, vomiting, diarrhoea, fever, low-salt diet) and interacting drugs (thiazides, NSAIDs, ACE-inhibitors/ARBs) are the classic precipitants of accumulation. Three patterns exist: acute overdose, acute-on-chronic, and chronic accumulation (the commonest and most dangerous). Toxicity is predominantly NEUROLOGICAL — fine tremor (earliest) progressing to coarse tremor, fasciculations, hyperreflexia, ataxia, dysarthria, seizures and coma — with nephrogenic diabetes insipidus (polyuria/polydipsia), GI (nausea/ [1]
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Lithium Toxicity.
[1] [1]References
- [1]Baird-Gunning J, Lea-Henry T, Hoegberg LCG, Gosselin S, Roberts DM. Lithium Poisoning J Intensive Care Med, 2017.PMID 27516079
- [2]Timmer RT, Sands JM. Lithium intoxication J Am Soc Nephrol, 1999.PMID 10073618
- [3]Decker BS, Goldfarb DS, Dargan PI, et al.; EXTRIP Workgroup. Extracorporeal Treatment for Lithium Poisoning: Systematic Review and Recommendations from the EXTRIP Workgroup Clin J Am Soc Nephrol, 2015.PMID 25583292
- [4]Waring WS. Management of lithium toxicity Toxicol Rev, 2006.PMID 17288494