emergency-toxicology · emergency-toxicology
Opioid Overdose
Also known as Opioid overdose · Opiate overdose · Heroin overdose · Naloxone reversal · Fentanyl overdose · Opioid toxicity · Opioid poisoning · Narcotic overdose
Opioid overdose produces the opioid (narcotic) triad: depressed consciousness/coma, respiratory depression (bradypnoea), and pinpoint pupils (miosis). Diagnosis is clinical plus response to naloxone. Resuscitate with bag-valve-mask ventilation and oxygen FIRST, then give naloxone (a competitive mu-opioid receptor antagonist) titrated to respiratory rate, not full alertness. Because naloxone's half-life (1 to 2 h) is shorter than most opioids, monitor for re-narcotisation for at least 2 to 4 h (24 to 48 h for methadone, sustained-release formulations, and fentanyl).
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Overview & Definition
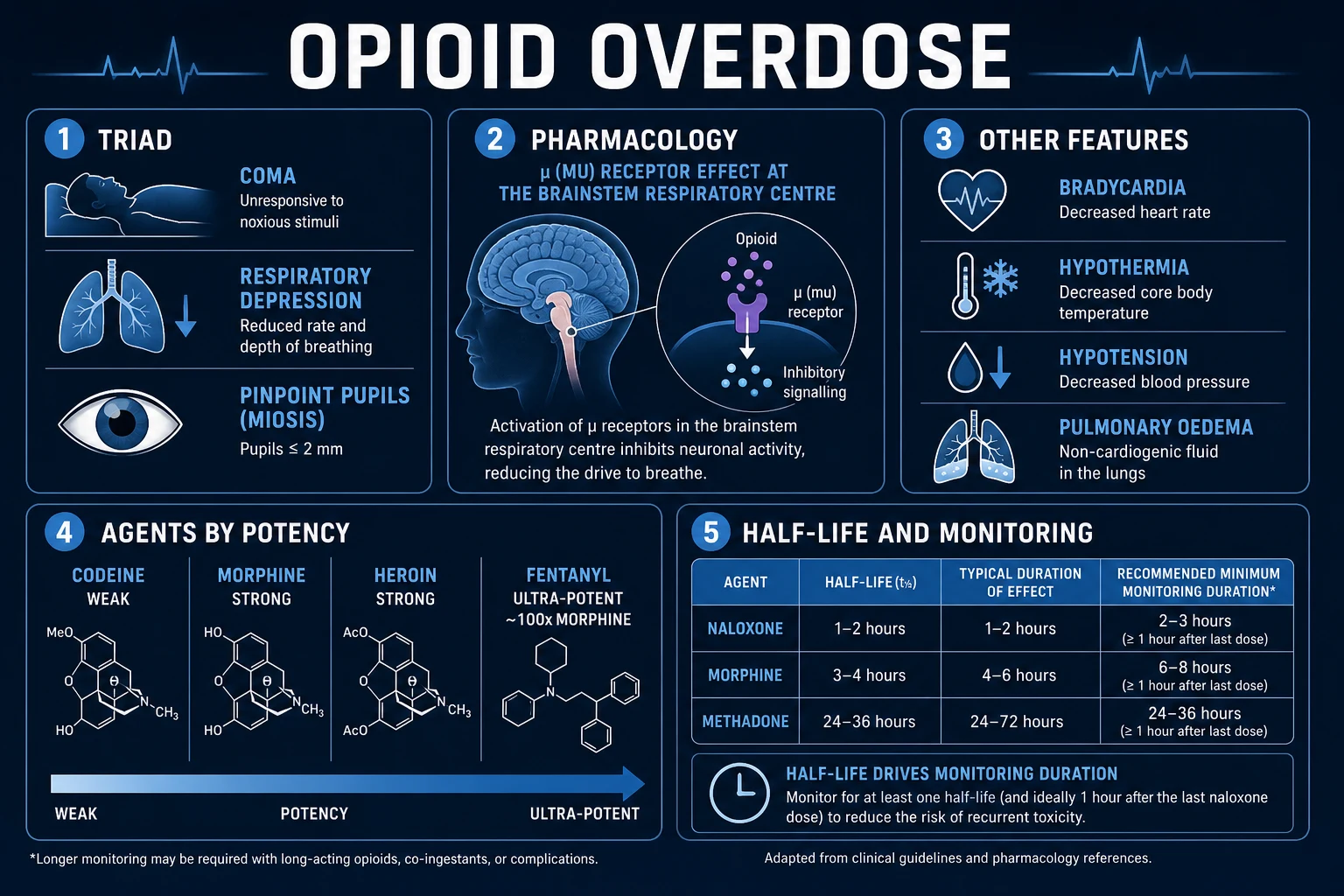
Opioid overdose is the toxic state produced by an excessive dose of any opioid agonist — prescription agents such as morphine, oxycodone, hydrocodone, fentanyl, methadone, tramadol, codeine, and pethidine (meperidine), and the illicit opioid heroin (diacetylmorphine). The defining clinical picture is the opioid (narcotic) toxidrome, the opioid triad: depressed level of consciousness (drowsiness to coma), respiratory depression (bradypnoea, shallow breathing, or apnoea), and pinpoint pupils (miosis). It is one of the most common and most lethal poisonings worldwide and a leading cause of preventable death in adults of working age.[1]
The clinical task is to recognise the triad within seconds, protect the airway and ventilate with oxygen, and give naloxone promptly — a competitive mu-opioid receptor antagonist that restores respiratory drive within 1 to 2 minutes intravenously. Two truths frame everything that follows. First, opioid overdose is a clinical diagnosis: a bedside response to naloxone is confirmatory, and waiting for a drug screen costs lives. Second, the single trap that kills patients is re-narcotisation — naloxone is a short-acting antagonist (half-life 1 to 2 h) whereas most opioids act for many hours, so a patient who initially recovers can re-sedate and stop breathing again. [1]
Classification
Opioids are classified along three axes that each carry overdose-management implications: receptor affinity (efficacy), origin, and potency / duration of action. These axes decide how aggressively respiratory depression develops, whether the agent is naloxone-reversible, and how long the patient must be observed. [1]
Full agonists (most dangerous)
- Morphine, heroin (diacetylmorphine), codeine, oxycodone, hydrocodone, fentanyl, methadone, pethidine/meperidine, propoxyphene
- Maximal mu-receptor activation → dose-dependent respiratory depression
- Fully naloxone-reversible (may need high/repeated doses for fentanyl and carfentanil)
Partial agonist (buprenorphine)
- High MOR affinity but low intrinsic activity; ceiling effect on respiratory depression
- Overdose: large naloxone doses may be needed (tight receptor binding); naloxone only partially reverses
- Can precipitate withdrawal if given to a full-agonist-tolerant patient
Mixed / atypical (tramadol)
- Weak MOR agonist PLUS serotonin and noradrenaline reuptake inhibition
- Causes seizures, serotonin syndrome (with SSRIs/MAOIs), QT prolongation
- Naloxone may precipitate seizures by unmasking the monoamine effect
Pure antagonists (the antidotes)
- Naloxone (short-acting, IV/IM/intranasal), naltrexone (long-acting oral, relapse prevention)
- No opioid effect; used to reverse overdose
- Precipitate acute withdrawal if given to opioid-tolerant patients
By origin: natural alkaloids (morphine, codeine — from the opium poppy Papaver somniferum); semi-synthetic (heroin, oxycodone, hydrocodone, buprenorphine — chemically modified from natural alkaloids); and fully synthetic (fentanyl, methadone, tramadol, pethidine, propoxyphene — synthesised de novo). The synthetic agents, particularly fentanyl and its analogues, now dominate overdose mortality in North America.[3]
Epidemiology & Risk Factors
Opioid overdose is a global public health emergency and among the leading causes of accidental death in adults of working age across multiple continents. Synthetic opioids — chiefly fentanyl and its analogues — are now the dominant driver of opioid-related death in North America and an increasing share of European mortality, because they are cheap, extraordinarily potent, and frequently adulterate heroin, cocaine, methamphetamine, and counterfeit pills without the user's knowledge. A person who believes they are injecting heroin or taking a counterfeit benzodiazepine tablet may in fact receive a lethal dose of fentanyl.[1][3]
In India and South Asia, the opioid crisis has a different face: it is driven less by fentanyl and more by pharmaceutical opioids (the legacy of over-prescription and diversion), heroin and charas, with tramadol and buprenorphine injection featuring prominently among people who inject drugs. Poppy-cultivation regions, poorly regulated pharmacies, and the diversion of prescription opioids from household medicine cabinets all contribute to availability. Globally, the World Health Organization recognises opioid overdose as a major and largely preventable cause of death.[4]
Risk factors for fatal opioid overdose
Other well-established risk factors: depression, suicidality, and other psychiatric comorbidity (overdose may be deliberate); chronic pain with high-dose opioid prescriptions (over 50 morphine-milligram-equivalents per day); hepatitis C, HIV, and other comorbidity; renal or hepatic impairment (impaired clearance of morphine and its metabolites); older age and frailty with increased receptor sensitivity and polypharmacy; sleep-disordered breathing (obstructive sleep apnoea magnifies opioid-induced respiratory depression); and social isolation — no bystander to administer naloxone or call for help.[2]
Pathophysiology
Opioids act principally at the mu-opioid receptor (MOR, MOP), a Gi/o-coupled seven-transmembrane G-protein-coupled receptor densely distributed in the brain, spinal cord, and periphery. The kappa (KOR) and delta (DOR) receptors contribute less to the classic overdose picture: KOR agonism causes dysphoria, miosis, and spinal analgesia; DOR has a smaller role in analgesia and in seizure threshold modulation. The classic opioid toxidrome — analgesia, euphoria, sedation, miosis, respiratory depression, and constipation — is overwhelmingly a mu-receptor phenomenon, which is why the pure mu-antagonist naloxone reverses it.[1]
The molecular cascade at MOR is: [1]
- Opioid binds MOR → activates inhibitory Gi/o protein.
- Gi/o inhibits adenylate cyclase → intracellular cyclic AMP (cAMP) falls.
- GIRK (Kir3) potassium channels open → membrane hyperpolarisation.
- N-type (and P/Q-type) voltage-gated calcium channels close → reduced neurotransmitter release. [1]
The net effect is neuronal inhibition at the sites where MOR is expressed, and the clinical syndrome follows from which centres are inhibited: [1]
- Analgesia — inhibition of the descending pain pathway (periaqueductal grey, nucleus raphe magnus, dorsal-horn substantia gelatinosa).
- Euphoria and reward — disinhibition of the ventral tegmental area (VTA) dopamine neurons, the basis of addiction.
- Miosis (pinpoint pupils) — activation of MOR in the Edinger-Westphal nucleus (parasympathetic oculomotor nucleus), increasing parasympathetic tone to the pupillary sphincter. Miosis is not reversed by naloxone in some patients if hypoxia has damaged the pathway.
- Sedation and coma — inhibition of cortical and thalamic arousal circuits and the reticular activating system.
- Respiratory depression (the lethal effect) — direct inhibition of the medullary respiratory centre, especially the pre-Bötzinger complex and the ventral respiratory group. Opioids reduce both the respiratory rate and the ventilatory response to carbon dioxide (shift the CO2-response curve down and to the right). Death occurs when bradypnoea progresses to apnoea and then hypoxic cardiac arrest.
- Cough suppression — inhibition of the medullary cough centre.
- Gastrointestinal — increased sphincter tone, reduced peristalsis → constipation and reduced bowel sounds; sphincter of Oddi spasm.
- Histamine release — especially morphine → urticaria, pruritus, vasodilation (contributes to hypotension). [1]
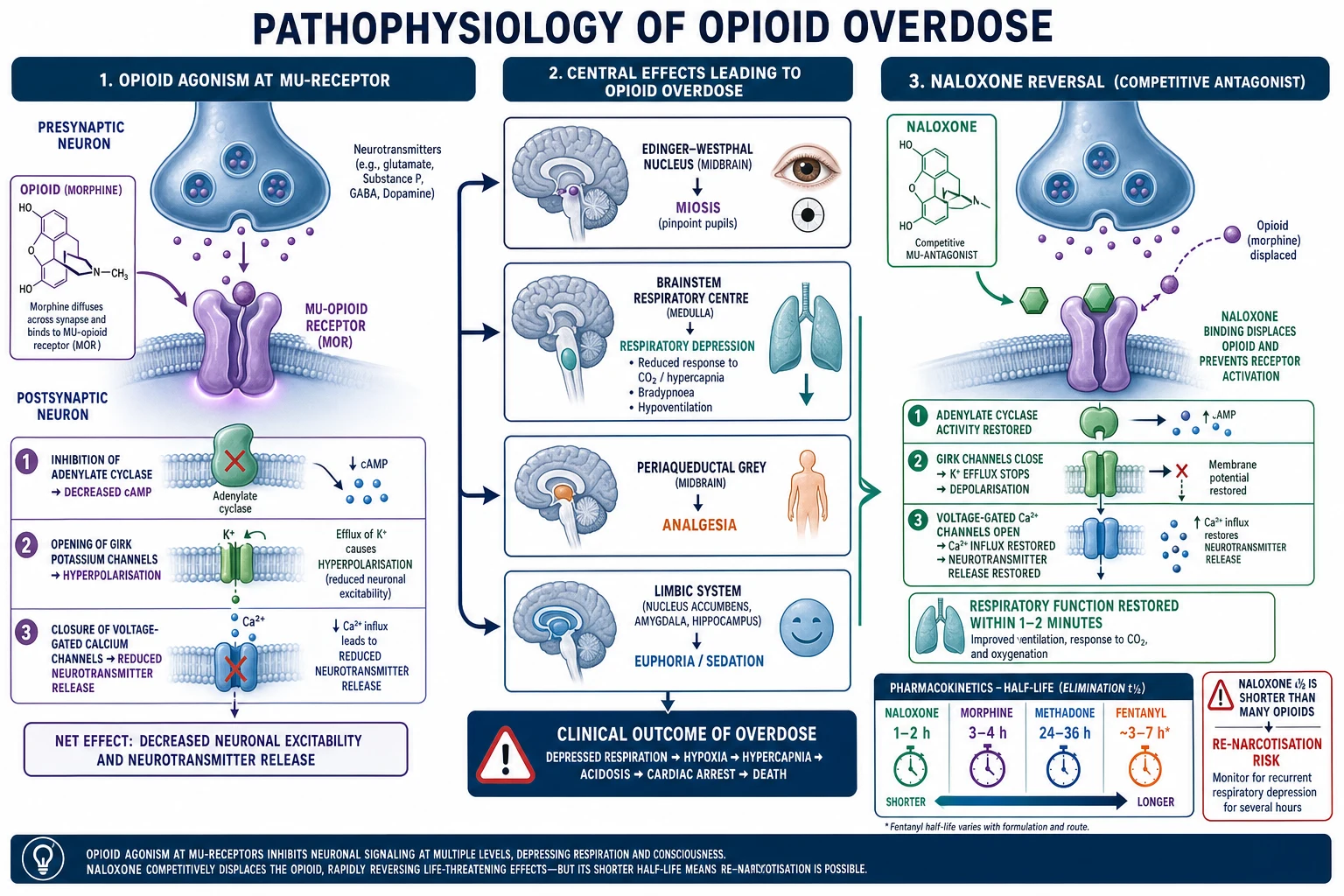
Naloxone is a competitive MOR antagonist with no agonist activity of its own. By occupying the receptor it displaces the opioid (and any endogenous endorphins), restoring respiratory drive within 1 to 2 minutes intravenously (2 to 5 minutes IM/SC, 3 to 5 minutes intranasal). Because the antagonism is competitive, the dose can be titrated: a small dose partially reverses respiratory depression without provoking withdrawal, whereas a large dose abruptly strips the opioid off receptors in opioid-tolerant patients and precipitates acute withdrawal.[2]
Re-narcotisation follows directly from pharmacokinetics. Naloxone has a half-life of 1 to 2 h (duration of action 20 to 90 min) while most opioids persist far longer — morphine 3 to 4 h, heroin's active metabolites 3 to 4 h, sustained-release morphine/oxycodone up to 12 to 24 h, methadone 24 to 36 h (occasionally 60 h), and lipophilic fentanyl redistributes from tissue stores. Once naloxone clears, residual opioid re-occupies MOR and respiratory depression recurs — sometimes catastrophically, in a patient who appeared fully recovered. This is the single most important concept in opioid-overdose management.[1][2]
Fentanyl's anomalous pharmacology deserves specific mention. Fentanyl is 100 times more potent than morphine and highly lipophilic; it rapidly crosses the blood-brain barrier (explaining the near-instant "rush" on IV injection and the rapid onset of apnoea). Its high lipophilicity also means large tissue stores accumulate with repeated dosing or transdermal use, and the drug redistributes back into the circulation as naloxone wears off — a key mechanism of re-narcotisation and of the need for higher or repeated naloxone doses in fentanyl overdose.[3]
Clinical Presentation
The classic presentation is the opioid toxidrome, best remembered as the opioid (narcotic) triad: [1]
- Depressed level of consciousness — drowsiness progressing to stupor and coma. Glasgow Coma Scale is often under 8 in severe poisoning.
- Respiratory depression — rate under 12/min (bradypnoea), shallow breathing, periodic or gasping pattern, cyanosis; may progress to apnoea and respiratory arrest. Respiratory rate is the pivotal vital sign — the definition of significant overdose is a rate under 12/min, and under 8/min is critical.
- Pinpoint pupils (miosis) — pupils 1 to 2 mm and poorly reactive to light, via the Edinger-Westphal mechanism above.[1]
Accompanying signs: bradycardia, hypotension, hypothermia, hyporeflexia, dry mucous membranes, reduced or absent bowel sounds, snoring or upper-airway obstruction (from soft-tissue collapse), and — in IV users — needle-track marks or a fresh injection site. A transiently elevated blood pressure may appear as hypoxia drives catecholamine release. The skin may be cool and the patient profoundly flaccid. Pruritus and urticaria (histamine) occur especially with morphine. Urinary retention from increased bladder-sphincter tone is common.[1]
Atypical presentations — examiners test these deliberately
- Fentanyl without miosis — fentanyl frequently produces normal-sized or even dilated pupils; absence of miosis does not exclude an opioid. Treat the respiratory pattern, not the pupils.[3]
- Severe anoxia or co-ingestion of an anticholinergic (tricyclic, antihistamine) can produce midsize or dilated pupils despite opioid overdose.
- Tramadol / propoxyphene — seizures, myoclonus, serotonin syndrome (hyperthermia, clonus, hypertonia, hyperreflexia, agitation), and QT prolongation in addition to the opioid picture. Naloxone may unmask seizures.[1]
- Methadone — QT prolongation with risk of torsades de pointes; may present with syncope or cardiac arrest rather than the classic triad.[5]
- Buprenorphine — partial agonist; respiratory depression may be partial and only partially naloxone-reversible because of tight receptor binding.
- Delayed onset with long-acting or sustained-release formulations — a patient who ingested sustained-release morphine, a fentanyl patch, or methadone may present late and deteriorate over many hours.
- Non-cardiogenic pulmonary oedema — frothy pink sputum, bilateral crackles, hypoxia, developing during or after the overdose; may appear after naloxone.
Differential Diagnosis
A comatose patient with small pupils has a focused but critical differential. All must be considered at the bedside; the response to naloxone and the bedside glucose usually clarify the picture within minutes. The cardinal principle is: check glucose immediately, give naloxone, and ventilate while you think.[1]
Clonidine / imidazoline (alpha-2 agonist)
- Miosis, coma, bradypnoea, bradycardia, hypotension — mimics opioids almost exactly
- Children ingest clonidine tablets or brimonidine/tetrahydrozoline eye drops
- Naloxone may help but is unreliable; respiration is the priority
Pontine haemorrhage / stroke
- Pinpoint pupils + coma + abnormal respiratory pattern (ataxic or apneustic)
- Distinguishing: focal signs (hemiparesis, extensor plantars), marked hypertension, history, NOT responding to naloxone
- Requires urgent CT brain
Organophosphate / carbamate poisoning
- Miosis + respiratory distress BUT copious secretions (SLUDGE: salivation, lacrimation, urination, defecation, GI upset, emesis), fasciculations, bradycardia, garlic smell
- Treat with atropine and pralidoxime; the opposite pharmacology of an opioid
Phenothiazines / typical antipsychotics
- Can cause miosis and coma; distinguishing: extrapyramidal signs, QT prolongation, hypotension, temperature dysregulation
- Co-ingestion common in suicide attempts
Benzodiazepine / alcohol / GHB co-ingestion
- Additive CNS and respiratory depression; pupils usually normal (benzodiazepines) but alcohol/GHB can cause miosis
- No specific antidote (flumazenil is dangerous in chronic users — seizures); support airway and give naloxone
Hypoglycaemia
- The great mimic — coma, sweating, sometimes miosis; reversible with IV dextrose
- ALWAYS check bedside glucose in any comatose patient before naloxone
Post-ictal state
- Coma after a seizure; pupils may be small; resolves over minutes to hours
- History of epilepsy or witnessed seizure
When a comatose patient arrives the bedside glucose must be checked immediately (hypoglycaemia is the great mimic and is rapidly fatal if missed), and a paracetamol and salicylate level sent on every intentional overdose — because of co-ingestion of an over-the-counter analgesic that has its own specific antidote (N-acetylcysteine, alkalinisation). [1]
Clinical & Bedside Assessment
A rapid, structured assessment at the bedside secures the diagnosis and the priorities. The aim is to confirm an opioid cause within a minute and exclude the mimics in parallel. [1]
- Airway and Breathing — respiratory rate is the pivotal vital sign (define bradypnoea as under 12/min; critical under 8/min); assess depth, cyanosis, use of accessory muscles, and upper-airway obstruction (snoring). Pulse oximetry is useful but lags — a desaturating patient is already in trouble, so do not wait for a low SpO2 before acting. An arterial or venous blood gas shows respiratory acidosis (low pH, high PaCO2) — the biochemical signature of opioid respiratory depression.
- Circulation — bradycardia and hypotension (often mild); check capillary refill and temperature (hypothermia).
- Disability — GCS, pupil size and reactivity (pinpoint under 2 mm suggests opioid), and bedside glucose (the first test in any comatose patient).
- Exposure — search for a MedicAlert, a fentanyl or buprenorphine patch on the skin (remove it!), needle-track marks, drug paraphernalia, and signs of trauma (the overdose may follow a fall or assault).
- History — from paramedics, family, or the patient's belongings: which opioid, what dose, what route, what time, any co-ingestants, and whether the patient is on long-term opioid therapy or opioid agonist treatment (which dictates a lower naloxone starting dose). [1]
The naloxone challenge (diagnostic trial): a small dose of naloxone (e.g. 0.04 to 0.1 mg IV) that improves respiration within 1 to 2 minutes confirms an opioid overdose. No response at a cumulative dose of around 10 mg effectively excludes a pure opioid cause, prompting a search for alternatives (clonidine, pontine lesion, other toxins).[2]
Look actively for complications: aspiration pneumonitis (rales, wheeze, reduced air entry, fever if delayed), non-cardiogenic pulmonary oedema (bilateral crackles, frothy sputum, hypoxia, often after naloxone), and rhabdomyolysis (firm, swollen, tender muscle groups, dark urine, rising creatine kinase) from prolonged immobilisation on a hard surface. [1]
Investigations
Opioid overdose is a clinical diagnosis — no laboratory result is required to start treatment, and waiting for a drug screen costs lives. Investigations are used to confirm the bedside picture, exclude mimics and co-ingestants, and detect complications.[1]
- Capillary glucose (bedside) — the first test in any comatose patient; hypoglycaemia is the great mimic and needs immediate treatment with IV dextrose.
- Arterial or venous blood gas — respiratory acidosis (low pH, high PaCO2, normal or low PaO2) confirms significant respiratory depression; the baseline bicarbonate is normal unless there is coexisting metabolic acidosis (e.g. from seizures, hypoxia, or co-ingestion). Repeat after naloxone to confirm reversal.
- ECG — mandatory in all opioid overdoses. QTc prolongation is the signature of methadone (risk of torsades de pointes); also check for the QRS widening of tricyclic co-ingestion and the dysrhythmias of hypoxia.[5]
- Paracetamol and salicylate levels — sent on every intentional overdose, because co-ingestion of an over-the-counter analgesic is common and has a time-critical specific antidote.
- Serum and urine drug screen — qualitative; useful for confirmation and for detecting co-ingestants (benzodiazepines, cocaine, amphetamines), but does not change acute management and does not detect fentanyl reliably on standard immunoassay panels.
- Pregnancy test — in any woman of childbearing age, because naloxone use in pregnancy has specific considerations (see Special Populations).
- CK, urea, creatinine, electrolytes — to detect rhabdomyolysis and acute kidney injury from prolonged immobilisation.
- Chest X-ray — to detect aspiration, non-cardiogenic pulmonary oedema, and to check tube placement if intubated.
- CT brain — if the patient fails to respond to an adequate naloxone dose, or if focal neurological signs are present, to exclude a pontine or other intracranial lesion.
There is no single 'opioid level' of clinical use in the acute setting — opioid serum concentrations do not correlate well with clinical severity, and turnaround time is too long. Treatment is guided by physiology, not numbers. [1]
Management — Resuscitation
The resuscitation bundle is time-critical and must be delivered in parallel, in the following order of priority:[1][2]
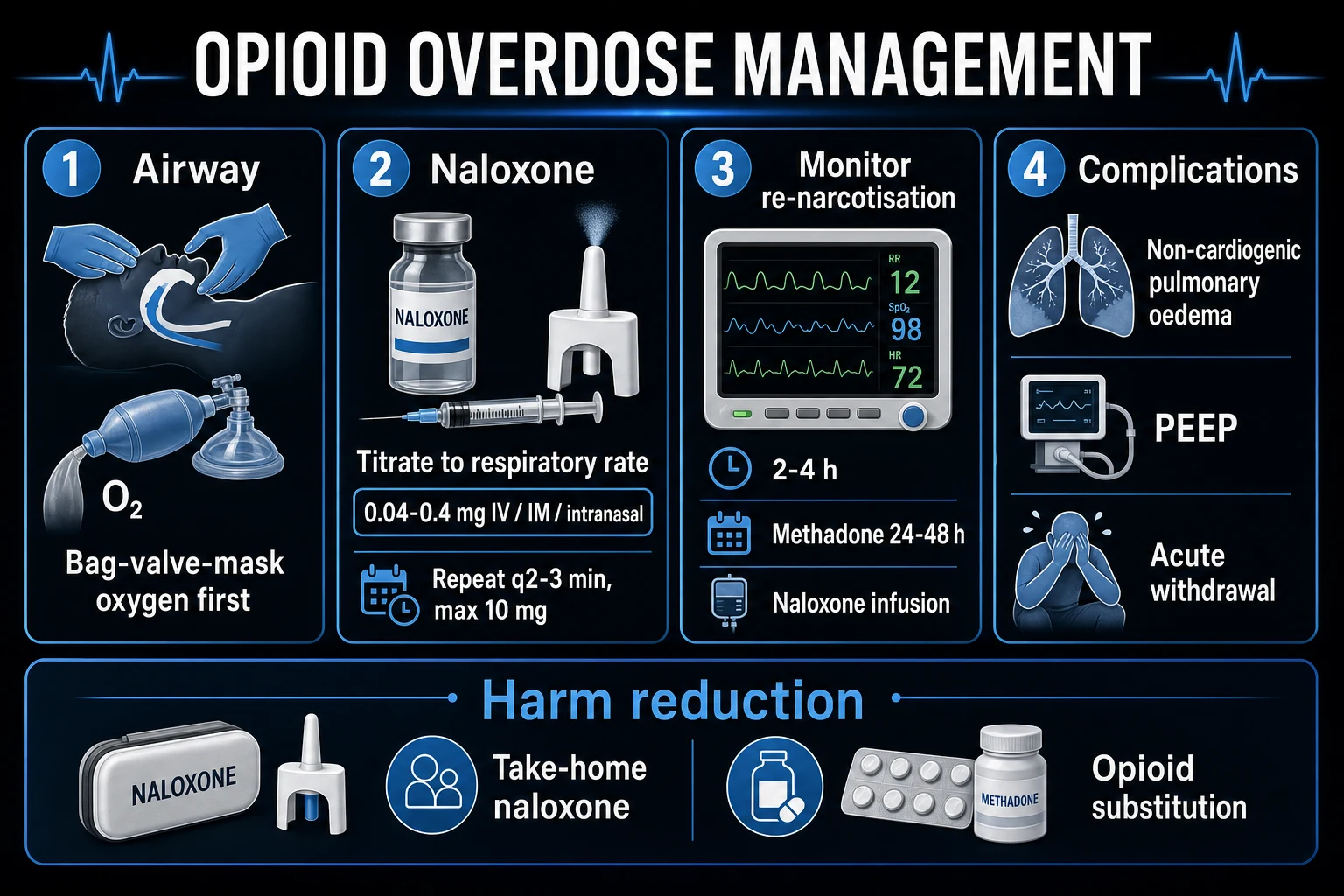
- Airway — protect and open. Clear the airway; consider a nasopharyngeal or oropharyngeal airway; position laterally if unprotected. Snoring = upper-airway obstruction from soft-tissue collapse — correct it immediately. Remove any transdermal fentanyl or buprenorphine patch and wipe the skin clean.
- Breathing — bag-valve-mask (BMV) ventilation with 100 percent oxygen, FIRST, before naloxone. A few effective breaths restore oxygenation and buy the time naloxone needs to work. Aim for an oxygen saturation over 94 percent and a normal PaCO2.
- Circulation — IV access; isotonic fluids for hypotension; cardiac monitoring (especially for methadone QT).
- Disability — bedside glucose, then naloxone. Check glucose immediately and treat hypoglycaemia; then administer naloxone titrated to respiratory rate.
- Exposure and history — identify the agent, dose, time, route, and co-ingestants. [1]
Why BMV before naloxone? The patient is hypoxic and hypercapnic; naloxone takes 1 to 2 minutes to work intravenously. A patient who arrests in that window was salvageable with a few breaths. Naloxone given to a profoundly hypoxic patient can also provoke a catecholamine surge, dysrhythmia, and pulmonary oedema. Ventilate first; reverse second.[1][2]
Endotracheal intubation versus naloxone — intubation is reserved for the patient who cannot be ventilated by BMV, who has failed to respond to an adequate naloxone dose (suggesting a non-opioid cause or a synthetic opioid refractory to naloxone), or who has a co-ingestant causing airway loss (e.g. severe benzodiazepine or alcohol overdose). In most pure opioid overdoses, naloxone avoids intubation and its complications (ventilator-associated pneumonia, sedation, ICU stay). [1]
Management — Definitive & Stepwise
Naloxone dosing
Naloxone is a competitive mu-opioid receptor antagonist with onset of 1 to 2 min IV, 2 to 5 min IM/SC, and 3 to 5 min intranasal; duration of action is 20 to 90 min.[1]
Naloxone dosing by route and context
Titration endpoint — respiratory rate, not full alertness. Aim for a respiratory rate over 10 to 12/min and adequate oxygenation. Reversing to full wakefulness in an opioid-tolerant patient precipitates acute withdrawal (agitation, vomiting, diarrhoea, tachycardia, piloerection, lacrimation, rhinorrhoea, muscle cramps, pulmonary aspiration of vomit) and may make the patient discharge themselves against advice — only to re-narcotise and die outside the hospital.[2]
Repeat dosing: if the initial dose works but the patient re-sedates, repeat the dose every 2 to 3 minutes up to a cumulative total of about 10 mg. If there is no response at 10 mg, reconsider the diagnosis (clonidine, pontine stroke, other toxin) and secure the airway.[1]
Naloxone infusion for long-acting opioids
For long-acting opioids (methadone, sustained-release morphine/oxycodone, fentanyl patches, massive body-packer ingestion) that outlast a single naloxone dose, start a naloxone infusion: [1]
- Calculate the total naloxone dose that produced an adequate response (the "wake-up dose", e.g. 0.6 mg).
- Give two-thirds of that dose per hour as a continuous infusion (e.g. 0.4 mg/hr), diluted in dextrose or saline.
- Titrate to a respiratory rate over 10 to 12/min (not full alertness).
- Reassess hourly; the infusion typically runs for 12 to 24 h for methadone and sustained-release products. [1]
Decontamination
- Activated charcoal — only within 1 h (up to 2 h) of ingestion, only if the airway is protected (the patient is awake and cooperative or intubated), and only for oral ingestions. Of little use in the typical IV heroin overdose. Avoid in body-packers (may interfere with later imaging and surgery).
- Whole-bowel irrigation — for body-packers with intact packets, using polyethylene glycol solution, once the airway is secured.
- Haemodialysis — not effective for opioid removal (large volume of distribution, high protein binding, extensive tissue distribution); manage with supportive care and naloxone. [1]
Observation and disposition (re-narcotisation)
Because naloxone's half-life (1 to 2 h) is shorter than most opioids, every patient must be observed for recurrence of respiratory depression:[1][2]
- Short-acting opioids (heroin, immediate-release morphine/oxycodone, fentanyl without a patch) — observe for at least 2 to 4 h after the last naloxone dose; if asymptomatic with normal vitals (RR over 12, SpO2 over 94 percent on room air, GCS 15), consider discharge with harm-reduction advice.
- Long-acting opioids (methadone, sustained-release morphine/oxycodone, fentanyl patches, massive ingestions) — admit for at least 12 to 24 h, often 24 to 48 h, with cardiac monitoring for methadone. Start a naloxone infusion if needed.
- Patients needing more than one naloxone dose, or a naloxone infusion — admit regardless of the opioid.
- Non-cardiogenic pulmonary oedema, significant co-ingestants, recurrent apnoea, body-packers, or suicide intent — admit. [1]
Harm reduction (the discharge bundle)
Before discharge, every opioid-overdose survivor should receive: take-home naloxone (intranasal 8 mg) with overdose-recognition training for the patient and family; a referral to opioid agonist therapy (OAT) — methadone or buprenorphine — which is the single most effective intervention to reduce mortality; screening and treatment for hepatitis C, HIV, and other blood-borne infections; mental-health and suicide-risk assessment (overdose may be deliberate); and clear safety-netting advice.[1][4]
Specific Subtypes & Scenarios
Fentanyl and ultra-potent synthetic opioids
Fentanyl is 100 times more potent than morphine and highly lipophilic, so it redistributes rapidly from tissue stores and may require higher or repeated naloxone doses. The onset of apnoea after IV fentanyl can be near-instantaneous.[3] Carfentanil (10 000 times morphine potency, used in veterinary medicine and as a weaponised agent) can be naloxone-resistant, mandating repeated high-dose naloxone (titrating well above 0.4 mg boluses), prolonged ventilation, and prolonged observation. Healthcare workers should wear personal protective equipment — dermal or inhalational exposure to powder can itself cause toxicity. Miosis may be absent with fentanyl, so treat the respiratory pattern, not the pupils.[1][3]
Body-packers and body-stuffers
- Body-packers swallow carefully packaged drug (usually condoms or pellets) for smuggling; toxicity occurs if a packet ruptures, causing massive, often fatal overdose. Manage with whole-bowel irrigation once the airway is secured; surgery is indicated for bowel obstruction, packet rupture, or failure to pass packets. Serial CT imaging tracks packet transit.
- Body-stuffers hastily swallow loosely wrapped drug to avoid arrest; they are at higher and more immediate risk of rupture and toxicity. Observe, image, and decontaminate proactively. [1]
Tramadol overdose
Tramadol is a weak MOR agonist plus a serotonin and noradrenaline reuptake inhibitor. Overdose causes seizures (it lowers the threshold), serotonin syndrome (especially with SSRIs, MAOIs, linezolid, or triptans — hyperthermia, clonus, hypertonia, hyperreflexia, agitation, autonomic instability), QT prolongation, and respiratory depression. Naloxone may precipitate seizures by unmasking the monoamine effect, so it should be used cautiously and only for significant respiratory depression. Treat seizures with benzodiazepines; treat serotonin syndrome with cooling, benzodiazepines, and cyproheptadine in severe cases.[1]
Methadone overdose
Long half-life (24 to 36 h, occasionally up to 60 h) and QT prolongation (risk of torsades de pointes via hERG channel blockade) make methadone overdose particularly dangerous.[5] Requires a naloxone infusion and 24 to 48 h observation, plus continuous cardiac monitoring for the QTc. Correct electrolytes (potassium, magnesium); consider isoprenaline or overdrive pacing for torsades.[5]
Mixed / polysubstance overdose
Co-ingestion with benzodiazepines, alcohol, or gabapentinoids multiplies respiratory depression; pupils may be normal. Flumazenil is generally avoided in chronic benzodiazepine users (risks precipitating seizures, especially with tricyclic co-ingestion). Manage with ventilation, naloxone, and supportive care; treat the most dangerous co-ingestant specifically (e.g. N-acetylcysteine for paracetamol, sodium bicarbonate for tricyclic QRS widening, haemodialysis for salicylate). [1]
Buprenorphine overdose
A partial agonist with high receptor affinity and a ceiling effect on respiratory depression. Overdose is usually mild in adults but can be severe in children or with benzodiazepine co-ingestion. Because buprenorphine binds MOR tightly, large naloxone doses may be needed and reversal is often incomplete — be prepared to support ventilation rather than relying on naloxone alone. [1]
Complications & Pitfalls
Non-cardiogenic pulmonary oedema (NCOPE)
- Develops during the overdose, sometimes after naloxone — frothy sputum, hypoxia, bilateral crackles
- Mechanism: opioid-induced capillary permeability and/or catecholamine surge; naloxone does NOT reverse it
- Treat with oxygen and PEEP (CPAP/NIV or mechanical ventilation)
Precipitated acute withdrawal
- Caused by over-aggressive naloxone in opioid-tolerant patients
- Agitation, vomiting, diarrhoea, tachycardia, piloerection, lacrimation, rhinorrhoea, muscle cramps
- Avoid by titrating to respiratory rate (not full alertness); manage supportively
Aspiration pneumonitis / pneumonia
- Reduced gag reflex + vomiting (opioid-induced CTZ stimulation)
- Right lower lobe common; antibiotics only if bacterial pneumonia supervenes (usually after 48 h)
Rhabdomyolysis, AKI & compartment syndrome
- Prolonged immobilisation on a hard surface compresses muscle → myonecrosis → myoglobinuric AKI
- Aggressive IV fluids, monitor CK and renal function; fasciotomy if compartment syndrome develops
Anoxic brain injury
- From delayed ventilation; the chief determinant of long-term outcome
- Preventable by early BMV and naloxone; consider targeted temperature management post-cardiac arrest
QT prolongation / torsades (methadone)
- hERG channel blockade by methadone; dose-dependent QTc prolongation
- Correct K+/Mg2+, continuous monitoring, isoprenaline/overdrive pacing for torsades
Other pitfalls: relying on pulse oximetry (it lags — act on respiratory rate); assuming opioid because pupils are small (clonidine, pontine stroke, organophosphates); assuming not opioid because pupils are normal (fentanyl, anoxia, anticholinergic co-ingestion); discharging too early and losing the patient to re-narcotisation; failing to send a paracetamol/salicylate level in every overdose; forgetting to remove a fentanyl patch; and giving high-dose naloxone to an opioid-tolerant patient and precipitating violent withdrawal and self-discharge.[1][2]
Prognosis & Disposition
Prognostic factors: the time to effective ventilation (the chief determinant of anoxic brain injury), the presence of co-ingestants (which deepen coma and complicate management), the development of NCOPE or aspiration, and comorbidity (hepatic/renal impairment, sleep apnoea, age). Most pure opioid overdoses that are ventilated and given naloxone early make a full neurological recovery. Death is from hypoxic cardiac arrest when ventilation is delayed.[2]
Pre-hospital naloxone saves lives: community-based naloxone distribution to people who use drugs, their families, and first responders is associated with significant reductions in opioid-overdose mortality — this is the single most important public-health intervention. The time from apnoea to irreversible brain injury is short, so bystander naloxone and basic airway management are decisive.[1][4]
Safe discharge criteria (after a short-acting opioid overdose with a good response to naloxone):
- Asymptomatic for at least 2 to 4 h (some protocols 4 h) after the last naloxone dose;
- Respiratory rate over 12/min, oxygen saturation over 94 percent on room air, GCS 15;
- No pulmonary oedema, no co-ingestant of concern, normal ECG;
- Take-home naloxone and overdose-recognition training provided;
- Follow-up (addiction medicine, mental health) arranged. [1]
Admit/observe longer (24 to 48 h) for: long-acting opioids (methadone, sustained-release formulations, fentanyl patches); NCOPE; significant co-ingestants; recurrent apnoea after naloxone; body-packers; suicide intent needing psychiatric admission; and any patient needing a naloxone infusion. [1]
Special Populations
Children
Most paediatric exposures are accidental ingestion of a prescribed opioid or methadone belonging to an adult in the household. Children are far more sensitive to opioids mg-for-mg. Naloxone dose: 0.1 mg/kg IV/IM/intranasal (max 2 mg per dose), repeated every 2 to 3 minutes up to a total of 10 mg. Because methadone and sustained-release products have long half-lives, admit every child for 24 to 48 h observation even after a good response — re-narcotisation in a child is easily missed. Supervise all opioid medications in the home; a single adult tablet can kill a toddler.[1]
Pregnancy
Naloxone crosses the placenta but is safe in pregnancy — maternal resuscitation takes priority, and maternal hypoxia is far more dangerous to the fetus than naloxone. Avoid over-reversal, which can precipitate acute maternal withdrawal (and theoretically precipitate labour). Be alert to fetal bradycardia from maternal respiratory depression and monitor the fetus once the mother is stabilised. After birth, watch for neonatal opioid withdrawal syndrome (NOWS / neonatal abstinence syndrome) if the mother is opioid-dependent; manage with non-pharmacological care (swaddling, low-stimulation environment, frequent small feeds) and, if needed, morphine or methadone per a validated score (e.g. modified Finnegan).[1]
Opioid-tolerant and OAT patients
In patients on chronic opioid therapy, OAT (methadone/buprenorphine), or with opioid use disorder, titrate naloxone carefully (0.04 to 0.1 mg) to adequate respiration and avoid precipitating acute withdrawal. The goal is adequate respiration, not full reversal. Do not stop the patient's usual OAT — restart or continue it to prevent withdrawal, and involve the addiction-medicine team early, ideally before discharge.[2][4]
Elderly and frail
Increased receptor sensitivity, reduced clearance, and benzodiazepine co-prescription markedly increase the risk of fatal respiratory depression; use lower naloxone doses (start 0.04 to 0.1 mg) and longer observation. Frail elderly patients are also at higher risk of complications (aspiration, falls, delirium). [1]
Evidence, Guidelines & Regional Differences
WHO and CDC guidance emphasise three pillars of the response to opioid overdose: (1) prompt recognition and naloxone; (2) take-home naloxone programmes for people who use drugs, their families, and first responders; and (3) linkage to opioid agonist therapy (OAT) — methadone or buprenorphine — which is the most effective single intervention to reduce overdose mortality. The 2022 systematic review of hospital-based guidelines by Calcaterra and colleagues found broad consensus that hospitalised patients with opioid use disorder should receive medication for opioid use disorder (MOUD), naloxone at discharge, and screening for co-occurring conditions; the evidence for opioid withdrawal protocols and overdose-prevention education was also strong.[4]
Landmark trials and concepts: the concept of naloxone as a public-health tool (community distribution); the buprenorphine ceiling effect on respiratory depression; the recognition of fentanyl's anomalous pharmacology — rapid blood-brain barrier penetration, large tissue stores, and the limitations of standard naloxone doses — which now shapes the debate over higher-dose take-home naloxone;[3] and the recognition that methadone blocks the hERG channel, causing dose-dependent QT prolongation and a small but real risk of sudden cardiac death, mandating ECG monitoring in methadone patients.[5]
Regional differences in naloxone access and policy:
- United States / Canada — intranasal products (Narcan 4 mg / 8 mg) widely available over the counter and through community naloxone programmes; standing orders allow pharmacist supply; higher-dose products (8 mg) increasingly favoured because of fentanyl.
- United Kingdom — intranasal naloxone (Nyxoid 1.4 mg per spray) available on prescription and supplied through drug services; take-home naloxone programmes are established nationwide.
- Australia — intranasal naloxone available over the counter since 2016; government-subsidised take-home naloxone programmes.
- India / South Asia — naloxone is available in hospital but community take-home naloxone programmes are limited; opioid agonist therapy (buprenorphine, methadone) is available through government de-addiction centres but access is uneven.
- WHO (global) — endorses intranasal and intramuscular naloxone for community use; recommends naloxone be available to people likely to witness an overdose, not only health workers.
Controversies: the optimal naloxone dose for fentanyl (some authorities recommend higher initial community doses, others caution that high doses increase withdrawal and the risk of NCOPE); whether higher-dose take-home naloxone (8 mg intranasal) is necessary given the rise of fentanyl; whether to intubate or rely on naloxone in the resource-limited setting; and the balance between naloxone and supportive ventilation when resources are limited. The subcutaneous long-acting naltrexone (Vivitrol) and emerging opioid vaccines and naloxone analogues remain areas of active research.[2]
Exam Pearls
The opioid overdose reflexes — CRASH
CRASH
the opioid triad — recognise it instantly
before naloxone — restore oxygenation, prevent arrest
0.04 to 0.4 mg IV/IM, aim RR over 10 to 12/min, not full alertness
fentanyl/carfentanil may need higher/repeated naloxone
naloxone 1 to 2 h is shorter than the opioid — observe for re-narcotisation
- The opioid triad: coma + respiratory depression + miosis. If miosis is absent, think fentanyl, severe anoxia, or anticholinergic co-ingestion.
- Ventilate first (BMV + oxygen), then naloxone. Naloxone takes 1 to 2 min to work; a patient who arrests in that window was salvageable with a few breaths.
- Naloxone titrated to respiratory rate (over 10 to 12/min), NOT full alertness. Over-reversal precipitates acute withdrawal and self-discharge.
- The killer is re-narcotisation. Naloxone's half-life (1 to 2 h) is shorter than the opioid. Observe at least 2 to 4 h (24 to 48 h for methadone, sustained-release, fentanyl).
- Fentanyl is 100x morphine; carfentanil 10000x. Synthetics may need higher or repeated naloxone; miosis may be absent.[3]
- Methadone: long half-life + QT prolongation. Needs naloxone infusion, 24 to 48 h observation, and cardiac monitoring.[5]
- Tramadol: seizures and serotonin syndrome. Naloxone may precipitate seizures; use cautiously.
- Naloxone does NOT reverse non-cardiogenic pulmonary oedema. That needs PEEP/NIV.
- Always check glucose, paracetamol, and salicylate in any overdose.
- Harm reduction: take-home naloxone + OAT referral at discharge.
Exam application bank (NEET-PG / INICET)
One-line answer
Opioid overdose produces the opioid (narcotic) triad: depressed consciousness/coma, respiratory depression (bradypnoea), and pinpoint pupils (miosis). Diagnosis is clinical plus response to naloxone. Resuscitate with bag-valve-mask ventilation and oxygen FIRST, then give naloxone (a competitive mu-opioid receptor antagonist) titrated to respiratory rate, not full alertness. Because naloxone's half-life (1 to 2 h) is shorter than most opioids, monitor for re-narcotisation for at least 2 to 4 h (24 to 48 h for methadone, sustained-release formulations, and fentanyl).
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Opioid Overdose.
References
- [1]Britch SC, Walsh SL. Treatment of opioid overdose: current approaches and recent advances Psychopharmacology (Berl), 2022.PMID 35385972
- [2]van Lemmen M, Huser C, Dahan A, et al. Opioid Overdose: Limitations in Naloxone Reversal of Respiratory Depression and Prevention of Cardiac Arrest Anesthesiology, 2023.PMID 37402248
- [3]Kelly E, Sutcliffe K, Cavallo D, et al. The anomalous pharmacology of fentanyl Br J Pharmacol, 2023.PMID 34030211
- [4]Calcaterra SL, Bottner R, Martin M, et al. Management of opioid use disorder, opioid withdrawal, and opioid overdose prevention in hospitalized adults: A systematic review of existing guidelines J Hosp Med, 2022.PMID 35880821
- [5]El Sherbini A, Liblik K, Lee J, et al. Opioids-induced inhibition of HERG ion channels and sudden cardiac death, a systematic review of current literature Trends Cardiovasc Med, 2024.PMID 37015297