Emergency & Toxicology · Emergency & Toxicology
Paracetamol (Acetaminophen) Overdose
Also known as Paracetamol overdose · Acetaminophen overdose · Acetaminophen toxicity · N-acetylcysteine · NAC · Paracetamol poisoning · Rumack-Matthew nomogram · King's College Criteria
Paracetamol (acetaminophen) overdose is the commonest cause of acute liver failure (ALF) in the developed world. At therapeutic doses paracetamol is safely metabolised by glucuronidation and sulfation; in overdose these saturate and the CYP2E1 pathway generates the toxic intermediate NAPQI (N-acetyl-p-benzoquinone imine), which depletes glutathione and produces centrilobular (zone 3) hepatic necrosis. The diagnostic pivot is a serum paracetamol level at 4 hours post-ingestion plotted on the treatment nomogram (Rumack-Matthew 150 mg/L line or UK 100 mg/L line); above the line = treat with IV N-acetylcysteine (NAC), which replenishes glutathione and is nearly 100 percent protective if given within 8 hours. Staggered, unknown-time, modified-release, or repeated supratherapeutic ingestion INVALIDATES the nomogram — treat empirically with NAC. King's College Criteria (arterial pH under 7.3 OR INR over 6.5 plus creatinine over 300 micromol/L plus grade III/IV encephalopathy) trigger urgent liver transplant referral.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Overview & Definition
Paracetamol (acetaminophen, N-acetyl-p-aminophenol) is the most widely used analgesic-antipyretic in the world. It is also the single most important poisoning to master for any medical exam and any clinical practice — it is common, potentially lethal, and, crucially, almost entirely preventable and treatable when N-acetylcysteine (NAC) is given early. Across the developed world it is the leading cause of acute liver failure (ALF), ahead of all other drug-induced and viral causes combined.[6]
The clinical skill in paracetamol overdose rests on six decisions, made in sequence: (1) take a precise time of ingestion (or recognise a staggered or unknown-time presentation); (2) draw a paracetamol level at 4 hours (never before — absorption is incomplete); (3) plot the level on the treatment nomogram and decide if it lies above the line; (4) start NAC immediately if above the line, or empirically if the nomogram does not apply (staggered, unknown time, modified-release, repeated supratherapeutic, or established hepatotoxicity); (5) monitor ALT, INR, creatinine, lactate, pH and glucose across the 24-to-72-hour window when hepatotoxicity declares itself; and (6) recognise King's College Criteria for urgent transplant referral.[1][4]
The signature trap of this overdose is its asymptomatic early phase: at 4 to 12 hours the patient looks and feels well, liver enzymes are normal, and yet NAPQI is already forming covalent adducts on hepatocyte proteins. Reassuring such a patient and discharging them without a 4-hour level is one of the classic and lethal pitfalls in clinical toxicology.[9]
Classification
Paracetamol overdose is classified by the pattern of ingestion, because the pattern dictates whether the nomogram can be used and whether treatment is empirical.[6]
Acute single ingestion
- Entire dose taken within a defined, short window (typically under 1 hour)
- Nomogram VALID from 4 to 24 h post-ingestion
- Most common pattern in deliberate self-harm
- Best studied; NAC within 8 h gives near-100 percent protection
Staggered overdose
- Multiple doses over more than 1 to 2 hours
- Nomogram INVALID
- Treat empirically with NAC
- Higher case-fatality than single ingestion — delayed presentation, cumulative glutathione depletion
Repeated supratherapeutic ingestion (RSI)
- Supra-therapeutic dosing over days (e.g. for fever in an alcoholic, fasting patient)
- Nomogram NOT used
- Treat if paracetamol detectable AND ALT over 50 U/L, OR ALT over 50 U/L with clear history
- Commonest pattern in unintentional US ALF
Chronic therapeutic dosing in a high-risk host
- Standard doses (4 g/day) in a patient with induced CYP2E1 or low glutathione
- Risk factors: chronic alcohol misuse, fasting/malnutrition, enzyme inducers (rifampicin, phenytoin, isoniazid), eating disorders
- Use the lower (100 mg/L) treatment line
- Often presents late, in established hepatotoxicity
Modified-release (MR) overdose
- Optizorb, 665 mg 'Osteo' modified-release preparations
- Delayed AND double-peak absorption
- Levels required at 4 AND 8 h (sometimes 12 h)
- Prolonged NAC course often needed
Two operational definitions anchor the topic. Hepatotoxicity is defined as an ALT (or AST) above 1000 U/L in the right clinical context following paracetamol exposure. Paracetamol-induced acute liver failure (ALF) is defined by INR at least 1.5 PLUS any grade of encephalopathy in a patient with paracetamol hepatotoxicity. The treatment line on the nomogram is the single most important number in management: 150 mg/L at 4 h on the US Rumack-Matthew line, or 100 mg/L at 4 h on the UK (and aligned ANZ/European) line.[1][7]
Epidemiology & Risk Factors
Paracetamol overdose is among the commonest deliberate self-poisoning agents worldwide and is the single largest cause of acute liver failure in the United States, the United Kingdom, Europe, and Australasia.[6] In the United States Acute Liver Failure Study Group (ALFSG) registry, paracetamol accounts for roughly 46 percent of all adult ALF, and the majority are unintentional (supratherapeutic ingestions over days rather than single deliberate overdoses).[10] The United Kingdom records roughly 70,000 to 90,000 paracetamol overdoses per year, leading to roughly 200 to 300 deaths.[6]
The single most important population-level prevention intervention is the 1998 UK legislation limiting pack size (maximum 16 tablets in non-pharmacy outlets, 32 in pharmacies), which reduced paracetamol-related deaths and liver unit admissions by roughly 20 to 40 percent.[12] No comparable federal limit exists in the United States, where the contribution of unintentional supratherapeutic ingestion to ALF is correspondingly larger.
Toxic thresholds — single acute ingestion
- Adult: hepatotoxicity uncommon under 150 mg/kg or 12 g (whichever is less)
- Risk rises steeply above 250 mg/kg or 15 g
- Child: under 150 mg/kg rarely toxic; treat above 200 mg/kg
- High-risk host: toxic at lower doses
High-risk host (lower toxic threshold)
- Chronic alcohol misuse (induced CYP2E1, low glutathione)
- Fasting and malnutrition (low glutathione)
- Eating disorders / chronic starvation
- Concurrent enzyme inducers: rifampicin, phenytoin, carbamazepine, phenobarbital, isoniazid, efavirenz, nevirapine, St John's wort
- HIV, febrile illness with repeated dosing, the elderly with polypharmacy, pregnancy
The dose-response is steep. In a healthy adult the toxic threshold for a single acute ingestion is roughly 150 mg/kg or 12 g (whichever is less); risk rises sharply above 250 mg/kg or 15 g, and the lethal range is roughly 250 mg/kg and above.[1][2] Children are relatively protected — a single accidental ingestion under 150 mg/kg rarely causes hepatotoxicity — but adolescents with intentional overdose are managed as adults.[8]
Pathophysiology
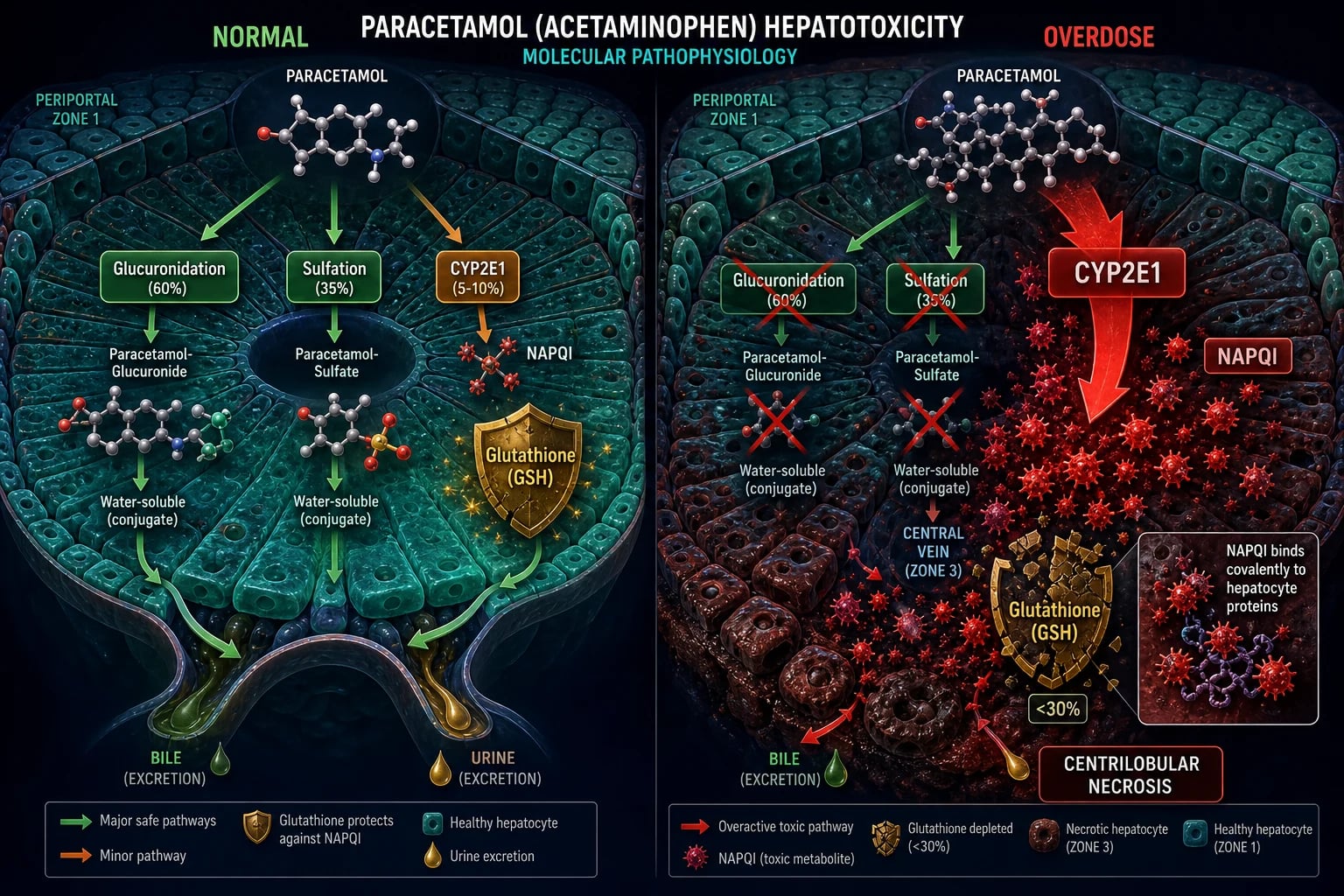
The molecular cascade of paracetamol toxicity is one of the best-elucidated in clinical toxicology, and it explains every aspect of the clinical syndrome — the early well window, the centrilobular necrosis, the 24-to-72-hour lag, and the mechanism of the antidote.[3]
At therapeutic doses (10 to 15 mg/kg per dose, up to 4 g/day in adults), paracetamol is metabolised in the liver along three routes:[5]
- Glucuronidation (about 40 to 67 percent) via UGT1A1 and UGT1A6 — produces an inactive, water-soluble glucuronide conjugate excreted renally.
- Sulfation (about 20 to 46 percent) via SULT1A1, SULT1A3 and SULT1A4 — produces an inactive sulfate conjugate excreted renally.
- A small oxidative fraction (about 5 to 10 percent) via CYP2E1 (with minor contributions from CYP1A2 and CYP3A4) — generates the reactive intermediate NAPQI (N-acetyl-p-benzoquinone imine).[6]
In health, every molecule of NAPQI is immediately conjugated with the sulfhydryl group of glutathione (GSH) to form a non-toxic mercapturic acid conjugate (cysteine and mercapturate) that is excreted in urine. The intracellular GSH pool is large enough that this minor oxidative fraction is harmless.[3]
In overdose, two things happen. First, sulfation saturates (it has a lower capacity than glucuronidation), then glucuronidation saturates, so a larger fraction of paracetamol is shunted through CYP2E1. NAPQI production rises sharply. Second, the GSH pool is consumed — hepatotoxicity ensues when hepatic GSH falls to under 30 percent of normal. Once GSH is depleted, free NAPQI binds covalently to cysteine residues of hepatocyte cellular proteins, forming NAPQI-protein adducts.[3]
The downstream cellular injury is mitochondrial: NAPQI-protein adducts damage mitochondrial proteins, open the mitochondrial permeability transition pore (mPTP), disrupt ATP synthesis and intracellular calcium homeostasis, and generate reactive oxygen and nitrogen species (superoxide, peroxynitrite). The result is mitochondrial dysfunction, hepatocyte oncotic (necrotic) and apoptotic cell death, amplified by a secondary inflammatory wave — Kupffer-cell activation, TNF-alpha, IL-1, and neutrophil recruitment.[10]
The injury is zonally restricted. CYP2E1 and the cytochrome P450 system are most concentrated in centrilobular (zone 3) hepatocytes (near the central vein), and zone 3 has the lowest oxygen tension in the liver acinus. The histological signature of paracetamol toxicity is therefore classical centrilobular (zone 3) coagulative necrosis, with sparing of the periportal (zone 1) hepatocytes — a pattern that explains both the extreme transaminase elevation (massive zone 3 cell death) and the eventual complete regeneration (zone 1 cells survive and repopulate).[5]
The renal mechanism parallels the hepatic one. Renal cortical cells express CYP2E1 and generate local NAPQI, producing acute tubular necrosis (ATN) in roughly 1 to 2 percent of overdoses. Notably, renal injury may occur without or before overt liver injury.[1]
N-A-P-Q-I
Clinical Presentation
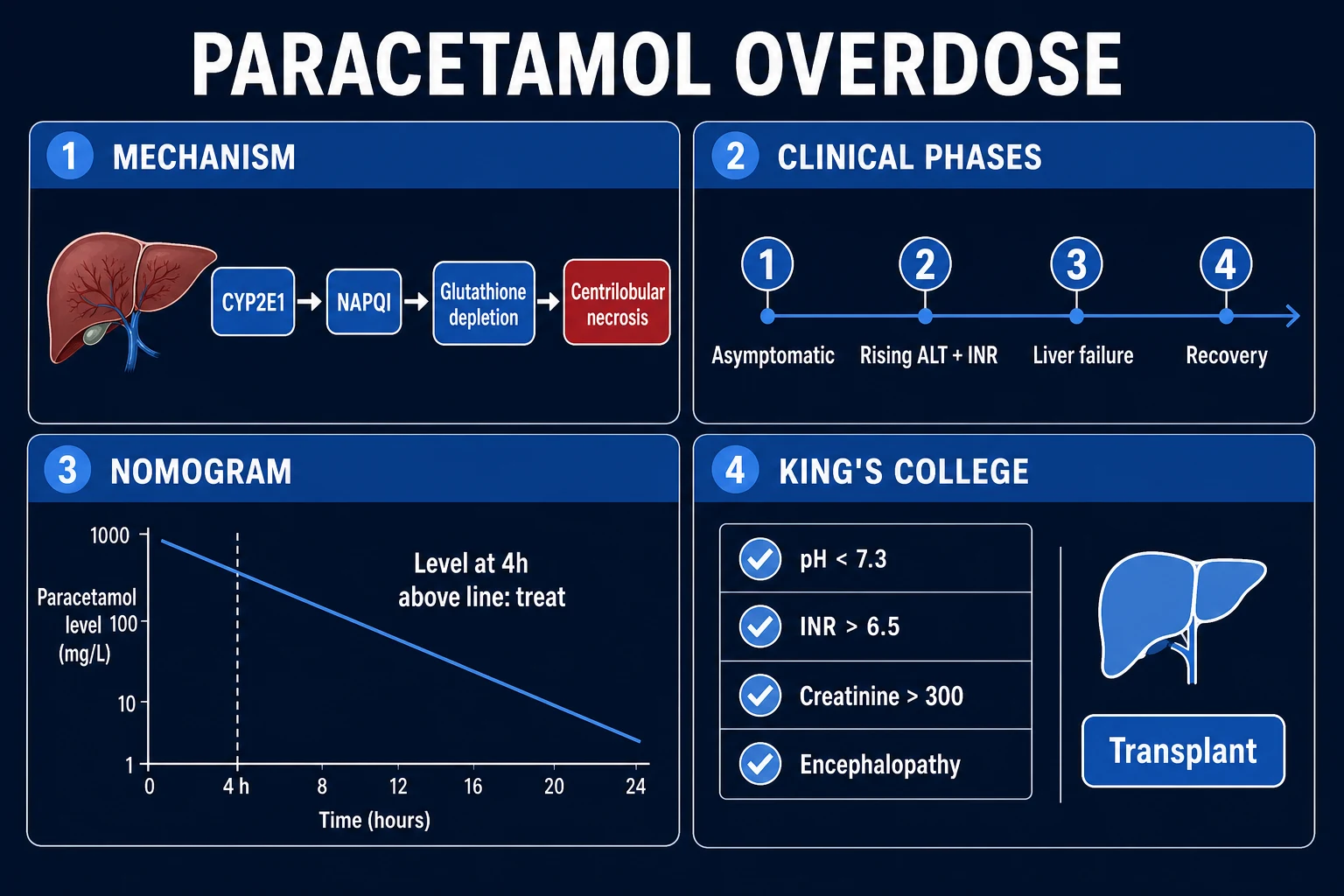
The clinical course of untreated paracetamol toxicity unfolds in four classical phases, each with its own diagnostic and prognostic weight. Knowing the phase by the clock is what allows the clinician to anticipate injury before it declares itself.[6]
Phase 1 (0 to 24 h) — the "well window". The patient is typically asymptomatic or has only mild nausea, vomiting, pallor, malaise, and diaphoresis. Liver enzymes, INR, and bilirubin are normal. The patient looks and feels well — and this is precisely the danger, because NAPQI is already forming hepatocyte adducts that will declare themselves 24 to 48 hours later. The single most dangerous management error at this phase is reassurance and discharge.[10]
Phase 2 (24 to 72 h) — hepatotoxicity declares itself. Right-upper-quadrant pain and tender hepatomegaly appear. ALT and AST rise — often above 1000 U/L, and frequently above 10,000 U/L with an AST greater than ALT pattern. INR begins to rise (the earliest and most sensitive marker of hepatic synthetic dysfunction). Oliguria and a rising creatinine signal ATN. This is the phase in which injury is occurring; the patient is no longer well.[10]
Phase 3 (72 to 96 h) — peak hepatotoxicity / acute liver failure. The full syndrome of ALF emerges: jaundice, coagulopathy, hypoglycaemia (impaired gluconeogenesis), metabolic (lactic) acidosis (impaired lactate clearance plus hypoperfusion), hepatic encephalopathy progressing from grade I (mild confusion, sleep disturbance) through grade II (drowsiness, disorientation) and grade III (somnolence but rousable, agitation) to grade IV (coma), cerebral oedema (Cushing's triad of hypertension, bradycardia, irregular respirations), renal failure, and multi-organ failure. Death is from cerebral oedema or sepsis.[10]
Phase 4 (4 days to 2 weeks) — recovery. In survivors, ALT, INR, and symptoms resolve over 1 to 2 weeks; complete histological recovery occurs over weeks to months WITHOUT cirrhosis — the liver regenerates fully because zone 1 hepatocytes are preserved.[10]
Atypical presentations
Examiners test atypical presentations deliberately. The elderly present non-specifically with comorbidity and polypharmacy; the pregnant patient has fetal risk and a lower threshold to treat; the chronic alcoholic or malnourished patient develops severe hepatotoxicity at low doses via RSI; the child presents after accidental ingestion and needs a level; the patient on enzyme inducers (rifampicin, phenytoin, isoniazid, antiretrovirals) is toxic at lower doses; and the staggered or unknown-time patient presents at 24 to 72 h already in phase 2 or 3 with no reliable early history.[6]
The anaphylactoid reaction to NAC
A separate clinical event is the anaphylactoid (non-IgE) reaction to intravenous NAC itself: flushing, urticaria, pruritus, occasionally bronchospasm or hypotension, typically during the first hour (the concentrated loading infusion), in roughly 10 to 20 percent of patients. It is more common when the paracetamol level is low (because high paracetamol inhibits the reaction), more common with rapid loading, and more common in atopic patients. It is not true IgE anaphylaxis and is managed by slowing or briefly stopping the infusion plus an antihistamine (chlorphenamine 10 mg IV or diphenhydramine 25 to 50 mg IV), then resuming at a slower rate. NAC should not be abandoned, since its life-saving benefit outweighs the reaction.[7]
Differential Diagnosis
The differential of an acute hepatitis picture with ALT over 1000 U/L, coagulopathy, and encephalopathy is broad, but a clear paracetamol history plus a measurable paracetamol level usually settles it. When the history is uncertain, the following must be distinguished.[10]
Other drug-induced liver injury (DILI)
- Idiosyncratic: amoxicillin-clavulanate, isoniazid, NSAIDs, statins, antifungals
- Variable latency (days to weeks)
- Paracetamol level undetectable
- Often mixed hepatocellular/cholestatic pattern
Ischaemic hepatitis ('shock liver')
- Profound hypotension episode (cardiac arrest, massive haemorrhage, septic shock)
- AST/ALT over 1000 that normalise within days
- Often concomitant kidney injury
- Shock + ALT over 1000 = ischaemic hepatitis
Viral hepatitis (A, B, E, HSV, EBV, CMV)
- Prodromal flu-like illness, jaundice
- ALT rises over days to weeks (vs hours for paracetamol)
- Viral serology positive
- HSV may cause fulminant hepatitis in immunocompromised/pregnant
Wilson disease presenting as ALF (young patient)
- Coombs-negative haemolytic anaemia
- Low ceruloplasmin (may be normal in ALF), high urinary copper
- Kayser-Fleischer rings
- High index of suspicion — mandates transplant
Other toxins
- Amanita phalloides mushroom: similar bimodal course but massive diarrhoea and foraging history
- Herbal/supplement toxicity
- Mixed overdose: paracetamol PLUS salicylate, opioid, ethanol, TCA, toxic alcohol
Two intra-paracetamol distinctions matter for management. Single acute ingestion (nomogram valid) must be distinguished from staggered ingestion (nomogram invalid, treat empirically) and from repeated supratherapeutic ingestion (use the RSI criteria, not the standard nomogram).[6]
Clinical & Bedside Assessment
The history is the single most important step in paracetamol overdose, and it must be precise. Establish: (1) the exact time of ingestion (to the hour — the nomogram depends on it); (2) the total dose in mg (and mg/kg, dividing by body weight); (3) the formulation (immediate release versus modified release); (4) whether single or staggered (over more than 1 to 2 hours); (5) co-ingestants (alcohol, salicylate, opioid, TCA, toxic alcohol); (6) regular medications (especially enzyme inducers); (7) alcohol and fasting history; (8) intent (deliberate self-harm versus accidental); and (9) the patient's weight.[6]
The focused bedside examination follows ABCDE: Airway (patency, especially with a co-ingested sedative); Breathing (rate, SpO2 — risk of aspiration); Circulation (HR, BP, capillary refill — hypotension suggests late ALF or co-ingestant); Disability (GCS — normal early; coma suggests co-ingestant or late cerebral oedema); and Exposure (stigmata of chronic liver disease, jaundice at 24 to 72 h, needle marks, evidence of self-harm).[6]
A bedside capillary glucose must be checked in every paracetamol overdose — hypoglycaemia at any phase is a red flag for hepatic failure. Mental-state and suicide-risk assessment is mandatory; no deliberate-self-harm patient should be left unattended, and psychiatric assessment is required once the patient is medically stable.[5]
The early-phase examination is typically normal — and this is the trap. At 0 to 24 h there may be nausea, vomiting, pallor and diaphoresis but no hepatomegaly, no jaundice, no encephalopathy. At 24 to 72 h, right-upper-quadrant tenderness, hepatomegaly, jaundice and dark urine appear. At 72 to 96 h the picture of ALF is unmistakable: encephalopathy, asterixis (liver flap), fetor hepaticus, and signs of cerebral oedema (Cushing's triad).[4]
Investigations
The essential blood panel in every paracetamol overdose is: serum paracetamol level (timing critical), U&E (sodium, potassium, creatinine), LFTs (ALT, AST, bilirubin, albumin), coagulation (INR/PT), venous or arterial blood gas (pH, lactate, bicarbonate), capillary glucose, FBC, and a salicylate level (to exclude co-ingestion). Group and Save if INR is elevated.[6]
The paracetamol level — timing is everything
The serum paracetamol level must be drawn at 4 hours (or later) after a single acute ingestion. Levels drawn before 4 h are uninterpretable because absorption is incomplete. The level can be plotted on the nomogram from 4 to 24 hours post-ingestion.[1]
The treatment nomogram
Plot serum paracetamol (y-axis, log scale) against hours post-ingestion (x-axis, linear). Above the treatment line = treat with NAC. The treatment line is:[7]
- US Rumack-Matthew line: 150 mg/L at 4 h (the original 200 mg/L line was revised down to 150 for safety).[1]
- UK / ANZ / European line: 100 mg/L at 4 h (UK changed from the historical 200/100 double line to a single 100 mg/L line in 2012; ANZ aligned in 2013).[7]
The line is a straight extrapolation assuming a paracetamol half-life of roughly 4 h. Below the line = no NAC (provided the timing is correct and the patient is well).[1]
When the nomogram CANNOT be used
The nomogram is invalid in:[6]
- Staggered ingestion (doses over more than 1 to 2 h).
- Unknown time of ingestion.
- Modified-release paracetamol.
- Repeated supratherapeutic ingestion.
- Presentation more than 24 h post-ingestion (the nomogram stops at 24 h).
- The patient already has established hepatotoxicity.[9]
In all of these situations, treat empirically with NAC — do not wait for a level or a nomogram decision.[6]
King's College Criteria (KCC) — for paracetamol-induced ALF
The King's College Criteria (O'Grady 1989) identify patients with paracetamol-induced ALF who have over 80 percent mortality without transplant and require urgent transplant referral.[4]
[5]Laboratory hallmarks of established hepatotoxicity
- ALT/AST markedly raised — often over 1000 U/L, may exceed 10,000 U/L, with an AST greater than ALT pattern.
- INR rising — the earliest and most sensitive marker of hepatic synthetic dysfunction. Check at baseline and at least every 12 to 24 h.
- Hyperbilirubinaemia, hypoglycaemia, metabolic (lactic) acidosis, raised lactate, acute kidney injury.[4]
The combination of ALT over 1000 U/L plus a rising INR in the right clinical context is essentially diagnostic of paracetamol hepatotoxicity.[6]
Monitoring schedule
For an admitted patient: ALT, INR, creatinine, venous lactate, venous pH at baseline then every 12 to 24 hours (more frequently if any abnormal); continuous cardiac monitoring during the NAC loading dose; capillary glucose every 1 to 2 h if hypoglycaemic. A low or undetectable paracetamol level in late or staggered ingestion does not exclude toxicity.[6]
Additional investigations as indicated: salicylate level, ethanol level, toxic alcohol screen (if osmolar gap), pregnancy test, viral hepatitis serology (if differential uncertain), and — at specialist centres — the paracetamol-cysteine adduct assay (a specific biomarker of paracetamol exposure when timing is unclear).[10]
Management — Resuscitation
The time-critical resuscitation bundle for any significant paracetamol overdose is:[6]
- ABCDE assessment, IV access, baseline bloods (paracetamol level at 4 h, INR, ALT, creatinine, lactate, pH, glucose, salicylate, FBC, U&E).
- Do not be reassured by an asymptomatic patient in the well window.
- Treat hypoglycaemia — 50 mL of 50 percent dextrose IV in adults (or 200 mL of 10 percent dextrose); in children, 2 to 5 mL/kg of 10 percent dextrose.
- Correct hypovolaemia with crystalloid; treat hypotension aggressively (a marker of late ALF or co-ingestant).
- Identify co-ingestants — salicylate level, ethanol level, opioid reversal if needed, ECG for TCA QRS prolongation.[6]
GI decontamination
Activated charcoal 50 g orally (1 g/kg in children) within 1 hour of ingestion (some guidelines extend to within 2 h) reduces paracetamol absorption by roughly 30 to 50 percent and does not interfere with oral NAC.[6] Multi-dose activated charcoal is not indicated. Gastric lavage is reserved for life-threatening ingestions within 1 h with a protected airway. Ipecac is contraindicated.
Activated charcoal is an adjunct to NAC, not a substitute. The pivotal early decision is whether the patient needs NAC at all, and that decision should be made within 8 hours of ingestion to maximise efficacy.[2]
Indications for immediate empirical NAC (do not wait for level/nomogram)
[9]Resuscitation of established ALF
If the patient presents in established ALF, follow standard liver-failure protocols: head elevation 30 degrees, mannitol 0.5 g/kg IV for cerebral oedema (after excluding renal failure and checking osmolality under 320 mOsm/kg), hypertonic saline to keep sodium 145 to 155 mmol/L, maintain normoglycaemia and normovolaemia, treat sepsis, intubate for grade III/IV encephalopathy, and urgent transplant referral if KCC met.[4]
There is no role for fomepizole, haemodialysis (except for very high levels, renal failure, or mixed overdose with metabolic acidosis), or any other antidote beyond NAC in standard paracetamol overdose.[5]
Management — Definitive & Stepwise
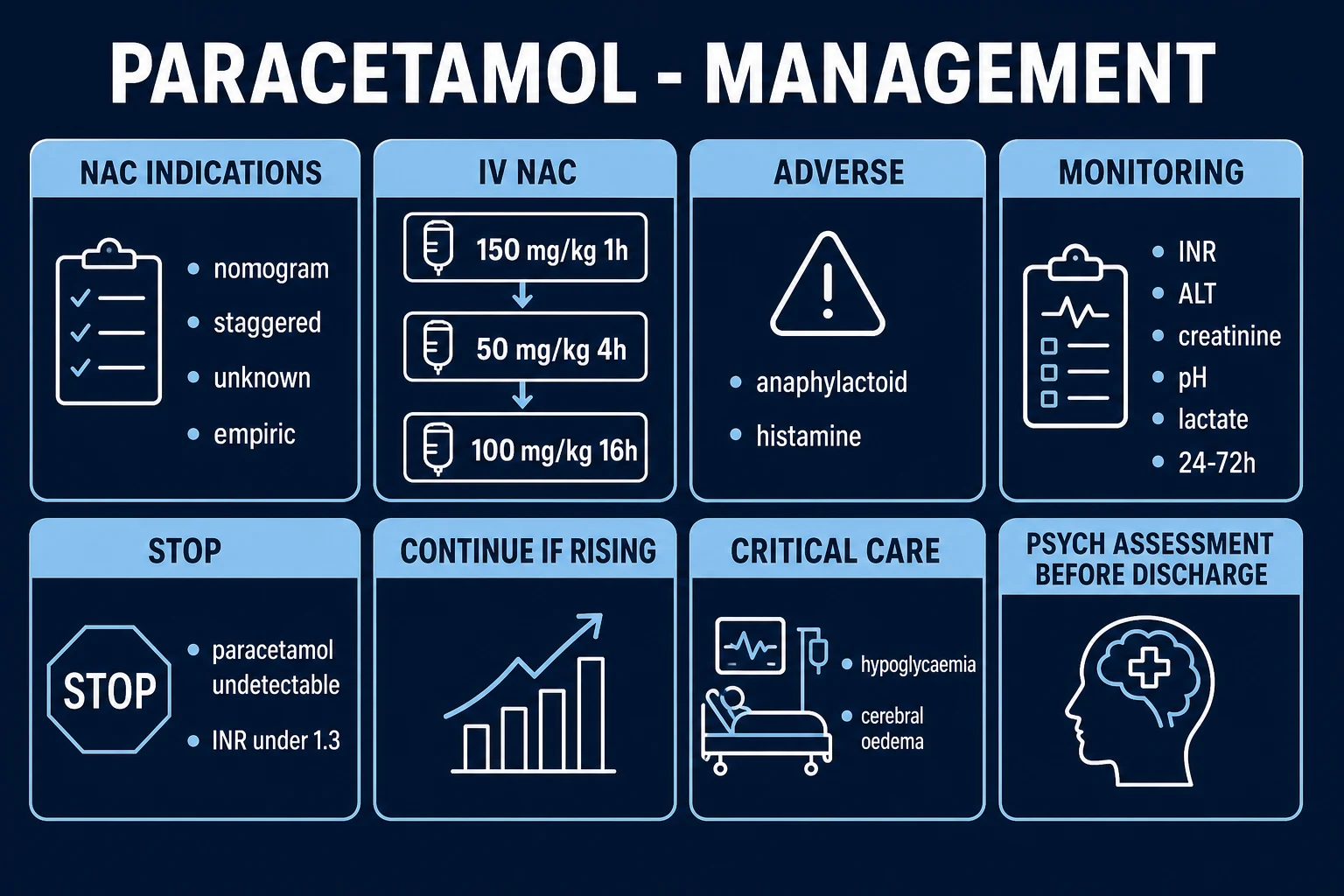
The IV NAC 21-hour three-bag regimen
This is the standard UK and international regimen, derived from Prescott 1979.[3]
In children, the diluent volumes must be reduced (use a more concentrated NAC preparation) to avoid fluid overload and hyponatraemia, especially in those under 20 kg or under 5 years.[7]
The rationale for the three-bag regimen: the loading dose achieves a high plasma NAC concentration quickly to drive glutathione synthesis; the lower subsequent infusions maintain therapeutic levels while minimising adverse reactions.[3]
When to continue NAC beyond 21 hours
Stop NAC at 21 h if ALL:
- Paracetamol level undetectable
- ALT static or falling
- INR under 1.3
- Clinically well
Continue NAC beyond 21 h if ANY:
- ALT above the upper limit of normal AND rising
- INR over 1.3
- Paracetamol level still detectable
- Any clinical concern
When continuing, give at the bag-3 rate (100 mg/kg over 16 h, i.e. roughly 6.25 mg/kg/h) and recheck ALT/INR every 12 h. Stop when ALT/INR are falling AND INR under 1.3.[2]
The oral NAC regimen (where IV unavailable)
Loading 140 mg/kg, then 70 mg/kg every 4 hours for 17 doses (total 1300 mg/kg over 72 hours).[2] Often vomited, so give with an antiemetic (metoclopramide 10 mg IV or ondansetron 4 to 8 mg IV). IV NAC is now preferred worldwide due to efficacy, tolerability, and shorter duration.
Managing the NAC anaphylactoid reaction
Most reactions are mild (flushing, urticaria, pruritus) during the first-hour loading.[7]
- Pause the infusion.
- Give chlorphenamine 10 mg IV (or diphenhydramine 25 to 50 mg IV). Hydrocortisone is not routinely needed for a pure non-IgE reaction.
- Resume the infusion at a slower rate (e.g. over 2 h) once symptoms settle.
- For severe reactions (bronchospasm, hypotension), stop, treat with adrenaline if anaphylaxis, then resume with caution.
- Do NOT abandon NAC — its life-saving benefit outweighs the reaction risk.[6]
Premedication is not routinely recommended but may be considered in patients with a history of reaction, asthma, or atopy.[7]
Scenario-specific management
Modified-release paracetamol
- Levels at 4 AND 8 h (sometimes 12 h)
- Treat with NAC if EITHER level above 100 mg/L (or 10 mg/L at 12 h) OR any hepatotoxicity
- Consider a PROLONGED NAC course (2 x 21-h cycles or until levels undetectable and INR normal)
- Observe for at least 24 h
Repeated supratherapeutic ingestion (RSI)
- Use the RSI criteria, NOT the standard nomogram
- Treat empirically if paracetamol detectable AND ALT over 50 U/L
- Identify and address the precipitant (starvation, alcohol, enzyme inducer)
Escalation triggers to ICU
- Any grade of encephalopathy
- INR over 2.0
- Arterial pH under 7.3
- Hypotension unresponsive to fluids
- Lactate over 3.0 mmol/L
- AKI requiring renal replacement therapy
- Need for intubation
- Any patient meeting King's College Criteria
King's College Criteria met — what to do
Once KCC are met, urgent transplant centre referral is time-critical (the window is short).[4]
- Continue NAC — it remains beneficial even in established ALF (Keays 1991 showed improved survival in established ALF).[5]
- Manage cerebral oedema (mannitol, hypertonic saline, head elevation, intubation for grade III/IV).
- Treat sepsis — paracetamol ALF patients are functionally immunosuppressed; surveillance cultures and a low threshold for antibiotics.
- Do NOT correct the INR with FFP or vitamin K before transplant assessment — this confounds the prognostic INR, which is the key KCC variable. Correct coagulopathy only if actively bleeding or before an invasive procedure.[4]
De-escalation and discharge
Discharge only when: NAC course complete, ALT and INR falling, INR under 1.3, clinically well, psychiatric assessment completed (for deliberate self-harm), and a safety plan in place. Counsel the patient that hepatic recovery is complete and there is no chronic liver damage.[6]
Psychiatric assessment is mandatory before discharge in all deliberate self-harm overdoses — in many jurisdictions (including India under the Mental Healthcare Act 2017) it is a medico-legal requirement.[1]
Specific Subtypes & Scenarios
Acute single ingestion in a healthy adult
Take a precise time, give charcoal within 1 h, draw a level at 4 h, plot on the nomogram, give NAC if above the line. Efficacy is near 100 percent if NAC within 8 h.[1][2]
Staggered overdose
The nomogram is invalid. Give NAC empirically. Admit and monitor ALT/INR at 12 to 24 h. Outcome is generally worse than single ingestion due to delayed presentation — this group has a higher rate of KCC-positive ALF and transplant.[6]
Modified-release paracetamol
Levels at 4 AND 8 hours. Treat if either is above 100 mg/L. Use a prolonged NAC course (often two 21-h cycles). Observe for at least 24 h.[9]
Repeated supratherapeutic ingestion
Use the RSI criteria (paracetamol detectable AND ALT over 50 U/L, OR ALT over 50 U/L with a clear history). Treat with NAC. Identify and address the precipitant.[7]
Pregnancy
Paracetamol crosses the placenta; the fetal liver has lower CYP2E1 but lower glutathione reserves, so the fetus is at risk. NAC is safe in all trimesters and crosses the placenta. Do not delay NAC. Use a lower threshold to treat. Obstetric and fetal-medicine input. Paracetamol overdose is NOT an indication for termination.[6]
Children
Accidental single ingestion under 150 mg/kg is usually benign — check a level at 4 h. Intentional/adolescent deliberate self-harm is managed as adult. Weight-based NAC dosing (150/50/100 mg/kg). Use smaller diluent volumes to avoid hyponatraemia (especially under 20 kg or under 5 years). Continuous monitoring. Palatable oral NAC for the rare oral regimen. Child-protection assessment for any suspicious or repeated presentation.[8]
Chronic alcoholic and malnourished/starved
Induced CYP2E1 and low glutathione double the risk of toxicity at lower doses. Consider using the lower (100 mg/L) treatment line even for single ingestion. Do not use the historical "alcohol nomogram". NAC dosing unchanged. Assess and manage alcohol withdrawal; give thiamine 100 mg IV before any glucose.[7]
Patient on enzyme-inducing drugs
Rifampicin, phenytoin, carbamazepine, phenobarbital, isoniazid, efavirenz, nevirapine, St John's wort, zidovudine. Lower threshold to treat; consider the lower treatment line. NAC dosing unchanged.[7]
Established ALF / King's College Criteria met
Urgent transplant referral, transfer to a liver unit, continue NAC, manage cerebral oedema, coagulopathy, hypoglycaemia, renal failure, and sepsis.[4][5]
Mixed overdose
Paracetamol plus salicylate has a higher mortality than either alone. Paracetamol plus ethanol — chronic ethanol potentiates toxicity (CYP2E1 induction) but acute ethanol co-ingestion may transiently protect (competitive CYP2E1 inhibition). Treat each component.[6]
Complications & Pitfalls
Disease complications
Hepatic
- Acute liver failure with cerebral oedema (leading cause of death)
- Coagulopathy and bleeding
- Hypoglycaemia
- Portopulmonary complications in severe ALF
Renal
- Acute tubular necrosis (ATN) in roughly 1 to 2 percent
- May occur WITHOUT liver injury
- Recovery is usual
Neurological
- Cerebral oedema with intracranial hypertension
- Cushing's triad: hypertension, bradycardia, irregular respirations
- Loss of brainstem reflexes in terminal phase
Other
- Sepsis (impaired immunity, line infections)
- Aspiration pneumonitis (vomiting or co-ingestant)
- Multi-organ failure
- Pancreatitis (rare)
- Complete hepatic recovery WITHOUT cirrhosis in survivors
Classical pitfalls
F-O-U-R-P-I-T
Cerebral oedema of ALF
Increased intracranial pressure, Cushing's triad (hypertension, bradycardia, irregular respirations), pupillary changes, loss of brainstem reflexes. Management: head elevation 30 degrees, mannitol 0.5 g/kg IV (if not in renal failure and osmolality under 320), hypertonic saline to sodium 145 to 155 mmol/L, hyperventilation to PaCO2 30 to 35, induced hypothermia 33 to 34 degrees in severe cases, and urgent transplant.[4]
Coagulopathy
Paracetamol-induced coagulopathy is a synthetic defect (impaired hepatic factor production), not a consumptive defect. INR is the most sensitive prognostic marker. Do NOT correct with FFP unless actively bleeding or before a procedure. Recombinant activated factor VII has been used before procedures.[4]
NAC anaphylactoid reaction
More common with low paracetamol levels (high paracetamol inhibits the reaction), more common with rapid loading infusion, and more common in atopic patients. Managed as above.[7]
Medicolegal pitfall
Deliberate self-harm overdoses require a formal psychiatric assessment and, in many jurisdictions, mandatory psychosocial assessment. Preserve the bottle/container and document the history.[6]
Prognosis & Disposition
The prognosis of paracetamol overdose is excellent when NAC is given within 8 h of a single acute ingestion: the rate of hepatotoxicity falls from roughly 50 to 60 percent (untreated) to under 5 percent, and mortality is near zero.[1][2]
Prognosis worsens with later presentation: NAC at 8 to 16 h gives roughly 15 to 30 percent hepatotoxicity; NAC at 16 to 24 h gives roughly 30 to 50 percent. But NAC remains beneficial even after hepatotoxicity has developed — Keays 1991 showed improved survival (48 percent versus 20 percent) when NAC was given in established paracetamol-induced fulminant hepatic failure.[5]
Established paracetamol ALF meeting King's College Criteria has a mortality over 80 percent without transplant; emergency liver transplantation reduces this to under 30 percent one-year mortality.[4]
Predictors of poor outcome
Delayed presentation (over 24 h), staggered ingestion, co-ingestion of enzyme inducers, chronic alcohol misuse, malnutrition, presentation already in ALF, arterial pH under 7.3, INR over 6.5, creatinine over 300 micromol/L, grade III/IV encephalopathy, arterial lactate over 3.5 mmol/L.[4]
Disposition
Discharge from ED
- Single acute ingestion, level below treatment line at 4 h
- ALT/INR normal, clinically well
- Medical AND psychiatric clearance completed (for self-harm)
- Safety plan and crisis numbers given
Observation / short-stay unit
- Single acute ingestion, treated with 21-h NAC
- ALT/INR normal at end of course
- No hepatotoxicity
Inpatient admission
- Any hepatotoxicity (ALT rising, INR over 1.3)
- Staggered / unknown-time / modified-release
- Any abnormal bloods requiring continued NAC
- Co-morbidity or co-ingestant
ICU and urgent liver-unit transfer
- Any grade of encephalopathy
- INR over 2.0 or arterial pH under 7.3
- Hypotension unresponsive to fluids
- Lactate over 3.0 mmol/L
- AKI requiring RRT
- Need for intubation
- Any patient meeting King's College Criteria
Safety-net on discharge
Complete hepatic recovery is the rule — no cirrhosis. Advise about the dangers of further paracetamol use. Safety plan and crisis numbers for deliberate self-harm patients. The high-risk patient (alcoholic, on enzyme inducers, eating disorder) should be advised to limit or avoid paracetamol. All deliberate self-harm cases require documented psychiatric follow-up and risk assessment before discharge.[6]
Special Populations
Pregnancy
- Paracetamol crosses placenta; fetus at risk (low glutathione)
- Full-dose IV NAC, safe in all trimesters, crosses placenta
- Do NOT delay NAC; lower threshold to treat
- Not an indication for termination
- Maternal outcome is principal determinant of fetal outcome
Children
- Accidental under 150 mg/kg usually benign — check level at 4 h
- Weight-based NAC dosing (150/50/100 mg/kg)
- More concentrated NAC dilution under 20 kg to avoid fluid overload and hyponatraemia
- Child-protection assessment for suspicious or repeated presentations
Elderly
- Atypical presentation, comorbidity, polypharmacy
- Reduced hepatic reserve; lower threshold to treat
- Watch for drug interactions
- Assess cognitive impairment and safeguarding in accidental overdoses
Chronic alcoholic / malnourished
- Induced CYP2E1, low glutathione — toxic at lower doses
- Consider the lower (100 mg/L) treatment line
- Do NOT use the 'alcohol nomogram'
- NAC dosing unchanged; assess alcohol withdrawal; thiamine 100 mg IV before any glucose
On enzyme-inducing drugs
- Rifampicin, phenytoin, carbamazepine, phenobarbital, isoniazid, efavirenz, nevirapine, St John's wort
- Lower threshold to treat; consider lower treatment line
- NAC dosing unchanged
Immunocompromised
- No specific change in management
- Lower threshold given comorbidity
- Check for drug interactions (azoles, antiretrovirals)
Anticoagulated (warfarin, DOAC)
- INR unreliable as hepatotoxicity marker — already abnormal
- Trend INR from baseline; LFTs and clinical picture more important
- Consider factor assays; consult haematology
Obese
- NAC dosed on ACTUAL body weight
- Some protocols cap the dose at 110 to 125 kg to avoid overdose
- Consult local guidelines
Evidence, Guidelines & Regional Differences
The evidence base
The Rumack 1981 paper (Archives of Internal Medicine, 662 cases with oral acetylcysteine) is the foundation of the modern nomogram: it established that the serum paracetamol level plotted against time predicts hepatotoxicity, and that oral NAC given within 8 to 10 h prevents it.[1]
The Smilkstein 1988 NEJM study of oral NAC in 2542 patients established that NAC within 8 h gives near-100 percent protection and that NAC is beneficial even when given late (up to 24 h).[2]
The Prescott 1979 BMJ paper introduced intravenous NAC as "the treatment of choice" for paracetamol poisoning — establishing the IV route and the loading-dose principle that evolved into the modern 21-h three-bag regimen.[3]
The Keays 1991 BMJ randomised controlled trial of IV NAC in paracetamol-induced fulminant hepatic failure (50 patients, established ALF) showed improved survival (48 percent versus 20 percent) and improved haemodynamics even when NAC was given AFTER hepatotoxicity had developed — this is why NAC is continued (or started) in established ALF.[5]
The O'Grady 1989 Gastroenterology paper (King's College) derived the King's College Criteria for paracetamol-induced ALF transplant referral — pH under 7.3 OR the triad of INR over 6.5 plus creatinine over 300 plus grade III/IV encephalopathy. This remains the standard transplant trigger worldwide, with sensitivity and specificity roughly 70 to 90 percent for mortality.[4]
Regional deltas
[12]Australia and New Zealand (ANZ). Post-2013 the 100 mg/L treatment line aligned with the UK. The 2020 MJA updated guideline (Chiew) introduced weight-based and two-bag NAC variants (e.g. 200 mg/kg over 4 h then 100 mg/kg over 16 h) that reduce adverse reactions and length of stay, and clarified management of modified-release preparations.[7]
Europe (EurofiTox / Swedish MPA). Sweden uses a 100 mg/L treatment line and a 100 mg/kg threshold for empirical treatment; many European centres use a 100 mg/L line. India (AIIMS / National Poisoning Centre): paracetamol is a leading agent in urban deliberate self-harm; access to NAC and transplant is variable; nomogram use per UK/US conventions but NAC often given empirically for staggered/unknown-time ingestion given unreliable history. The Mental Healthcare Act 2017 decriminalises self-harm attempts but mandates psychosocial assessment.
Controversies
The 150 mg/L (US) versus 100 mg/L (UK/ANZ/Europe) treatment-line controversy: the 100 mg/L line treats more patients (some over-treatment) but is safer; the 150 mg/L line misses some high-risk patients. Most of the world now favours 100 mg/L.[7]
The optimal NAC regimen: the 21-h three-bag regimen versus the 12-h two-bag ANZ regimen (200 mg/kg over 4 h then 100 mg/kg over 16 h, or stop if low-risk at 4 h) — both effective; the two-bag ANZ regimen reduces adverse reactions and length of stay.[7]
The paracetamol-cysteine adduct assay is an increasingly used specific biomarker of paracetamol exposure at specialist centres when timing/history is unclear.[10]
Exam Pearls
[5]PHASES
Must-know numbers
- 4 h: time of first useful paracetamol level
- 150 mg/L: US Rumack-Matthew treatment line at 4 h
- 100 mg/L: UK/ANZ/European treatment line at 4 h
- 150 mg/kg or 12 g: adult toxic single dose
- 150/50/100 mg/kg: the three NAC bags
- 21 h: total NAC course duration
- 300 mg/kg: total NAC dose
- pH 7.3 / INR 6.5 / creatinine 300: King's College Criteria
Frequently misremembered (correctly stated)
- NAC works by REPLENISHING GLUTATHIONE (cysteine donor), NOT by binding paracetamol
- The liver RECOVERS completely after single overdose — no cirrhosis
- Anaphylactoid reaction is NON-IgE; do NOT abandon NAC
- Activated charcoal does NOT block oral NAC
- INR is the earliest/most sensitive prognostic marker
- MR paracetamol: levels at 4 AND 8 h
Exam application bank (NEET-PG / INICET)
One-line answer
Paracetamol (acetaminophen) overdose is the commonest cause of acute liver failure (ALF) in the developed world. At therapeutic doses paracetamol is safely metabolised by glucuronidation and sulfation; in overdose these saturate and the CYP2E1 pathway generates the toxic intermediate NAPQI (N-acetyl-p-benzoquinone imine), which depletes glutathione and produces centrilobular (zone 3) hepatic necrosis. The diagnostic pivot is a serum paracetamol level at 4 hours post-ingestion plotted on the treatment nomogram (Rumack-Matthew 150 mg/L line or UK 100 mg/L line); above the line = treat with IV N-acetylcysteine (NAC), which replenishes glutathione and is nearly 100 percent protective if given within 8 hours. Staggered, unknown-time, modified-release, or repeated supratherapeutic ingestion INVALIDATES the nomogram — treat empirically with NAC. King's College Criteria (arterial pH under 7.3 OR[9]
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard.[1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes.[9]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change.[1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each.[1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory.[1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Paracetamol (Acetaminophen) Overdose.
References
- [1]Rumack BH, Peterson RC, Koch GG, Amara IA. Acetaminophen overdose. 662 cases with evaluation of oral acetylcysteine treatment. Archives of Internal Medicine, 1981.PMID 7469629
- [2]Smilkstein MJ, Knapp GL, Kulig KW, Rumack BH. Efficacy of oral N-acetylcysteine in the treatment of acetaminophen overdose. Analysis of the national multicenter study (1976 to 1985). New England Journal of Medicine, 1988.PMID 3059186
- [3]Prescott LF, Illingworth RN, Critchley JA, Stewart MJ, Adam RD, Proudfoot AT. Intravenous N-acetylcystine: the treatment of choice for paracetamol poisoning. British Medical Journal, 1979.PMID 519312
- [4]O'Grady JG, Alexander GJ, Hayllar KM, Williams R. Early indicators of prognosis in fulminant hepatic failure. Gastroenterology, 1989.PMID 2490426
- [5]Keays R, Harrison PM, Wendon JA, Forbes A, Gove C, Alexander GJ, Williams R. Intravenous acetylcysteine in paracetamol induced fulminant hepatic failure: a prospective controlled trial. BMJ, 1991.PMID 1954453
- [6]Bateman DN, Dart RC, Dear JW, et al. Fifty years of paracetamol (acetaminophen) poisoning: the development of risk assessment and treatment 1973-2023 with particular focus on contributions published from Edinburgh and Denver. Clinical toxicology (Philadelphia, Pa.), 2023.PMID 38197864
- [7]Chiew AL, Reith D, Pomerleau A, Wong A, Isoardi KZ, Soderstrom J, Tomas C, Gosselin S, Graudins A. Updated guidelines for the management of paracetamol poisoning in Australia and New Zealand. Medical Journal of Australia, 2020.PMID 31786822
- [8]Peterson RG, Rumack BH. Age as a variable in acetaminophen overdose. Archives of Internal Medicine, 1981.PMID 7469631
- [9]Spyker DA, Tong TG, Spiller D, Novak MJ Population pharmacokinetic analysis of acetaminophen overdose with immediate release, extended release and modified release formulations. Clinical Toxicology (Philadelphia), 2022.PMID 36106921
- [10]MacDonald AJ, Vento AE, Gustafson MC, Tomiyama AJ, Bhushan D, Bradley KA, Yee HF Jr, Lee WM. Clinical and Neurologic Outcomes in Acetaminophen-Induced Acute Liver Failure: A 25-Year Multicenter Cohort. Clinical Gastroenterology and Hepatology, 2021.PMID 32920216
- [11]Chiew AL, Reith D, Pomerleau A, Wong A, Isoardi KZ, Soderstrom J, Tomas C, Gosselin S, Graudins A. Summary statement: new guidelines for the management of paracetamol poisoning in Australia and New Zealand. Medical Journal of Australia, 2015.PMID 26852051
- [12]Bateman DN. Pack size and paracetamol overdose: 16 years later. Clinical Toxicology (Philadelphia), 2014.PMID 25200452