Emergency & Toxicology · Emergency & Toxicology
Salicylate (Aspirin) Overdose
Also known as Salicylate overdose · Aspirin overdose · Salicylism · Salicylate poisoning · Aspirin poisoning · Oil of wintergreen poisoning · Methyl salicylate poisoning · Done nomogram · Urinary alkalinisation
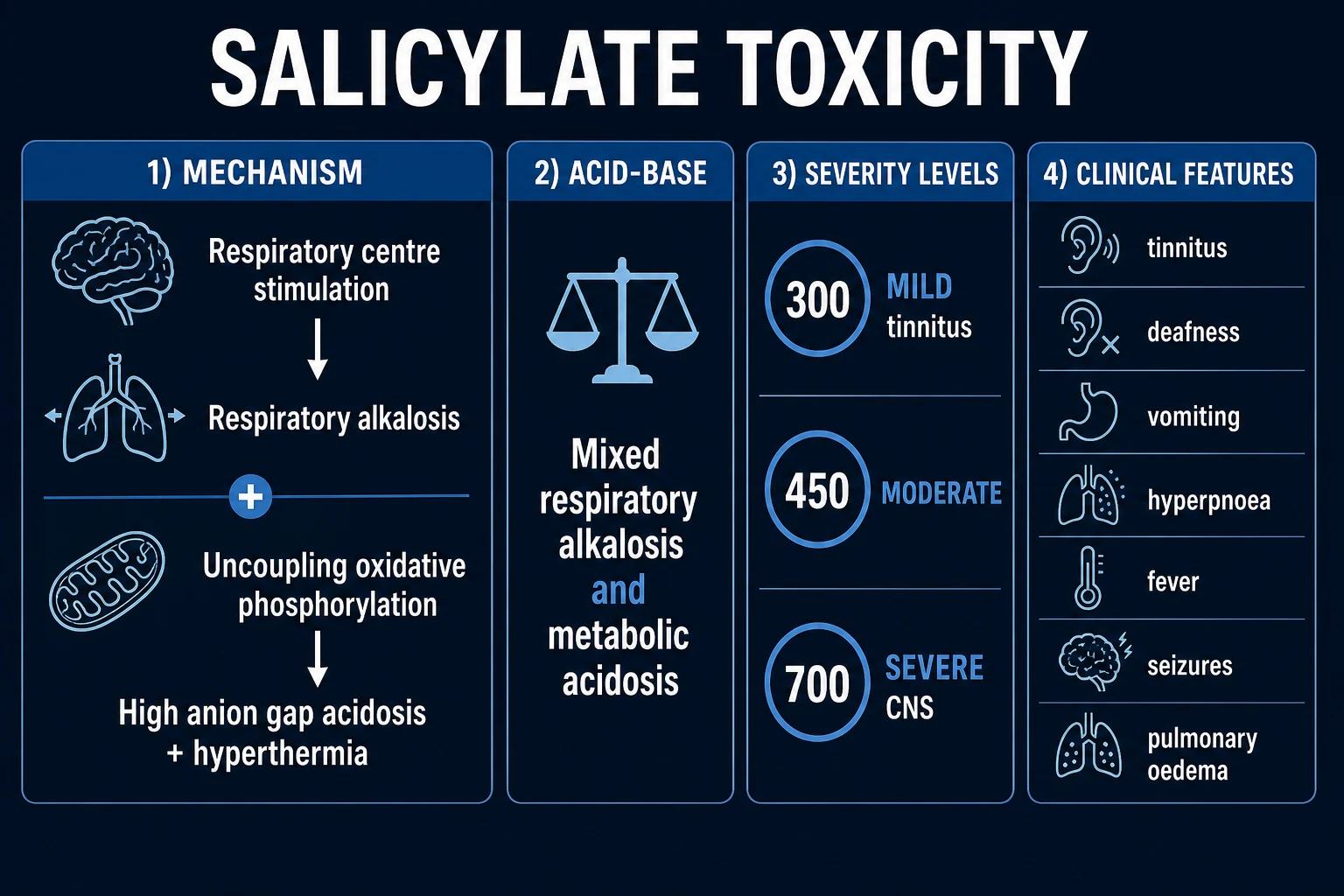
Salicylate (aspirin) overdose produces a characteristically MIXED acid-base disorder through three mechanisms: direct stimulation of the medullary respiratory centre (hyperventilation, primary respiratory alkalosis), uncoupling of oxidative phosphorylation in mitochondria (hyperthermia, increased oxygen consumption, lactate), and disturbance of the Krebs cycle (ketoacids and organic acids), together producing a high anion-gap metabolic acidosis. The classic adult blood gas is therefore primary respiratory alkalosis PLUS high anion-gap metabolic acidosis with tinnitus. Early features include tinnitus, deafness, nausea, vomiting, hyperpnoea, fever, sweating; severe poisoning causes agitation, confusion, seizures, hyperthermia, coma, non-cardiogenic pulmonary oedema and acute kidney injury. Diagnosis rests on a serum salicylate level (over 300 mg/L toxic, over 700 severe) with serial measurements and an arterial blood gas. The key non-dialysis treatment is urinary alkalinisation with intravenous sodium bicarbonate to a urine pH of 7.5 to 8.0 (with potassium correction) which ion-traps salicylate in the alkaline tubular urine. Haemodialysis is indicated for a level over 700 mg/L (acute) or over 600 mg/L (chronic), severe acidosis, CNS signs, pulmonary oedema, or renal failure. AVOID intubulation (loss of the hyperventilatory compensation causes fatal acidosis); if intubated, maintain hypocapnia. Give glucose even if plasma glucose is normal (cerebral hypoglycaemia). Beware rebound after stopping urinary alkalinisation.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags

Overview & Definition
Salicylates are a family of drugs derived from salicylic acid — the parent compound isolated from willow bark (Salix alba) and synthesised chemically by Felix Hoffmann at Bayer in 1897 as acetylsalicylic acid (aspirin). Salicylate-containing products in modern use include aspirin (analgesic, antipyretic, anti-inflammatory, antiplatelet), methyl salicylate (oil of wintergreen) — a topical counter-irritant and flavouring, bismuth subsalicylate (Pepto-Bismol), salicylamide, salsalate, sulfasalazine, and several combination analgesics. Salicylate poisoning is toxicity from any of these, with aspirin and methyl salicylate accounting for the majority of serious cases.[7][9]
Salicylate toxicity produces a syndrome that is physiologically distinctive and clinically dangerous: a direct stimulation of the medullary respiratory centre (early respiratory alkalosis), uncoupling of oxidative phosphorylation and disturbance of intermediary metabolism (high anion-gap metabolic acidosis, hyperthermia, dehydration), and — in severe poisoning — non-cardiogenic pulmonary oedema, CNS toxicity, and cardiovascular collapse. The hallmark blood gas in adults is a mixed respiratory alkalosis and high anion-gap metabolic acidosis, often accompanied by tinnitus.[7]
The clinical skill in salicylate overdose rests on seven decisions, made in sequence: (1) recognise the toxidrome (hyperpnoea, tinnitus, mixed acid-base disorder, fever, dehydration); (2) draw a salicylate level and repeat it serially (single levels mislead); (3) resuscitate with IV fluids that include dextrose; (4) correct hypokalaemia (without it, urinary alkalinisation will fail); (5) institute urinary alkalinisation with IV sodium bicarbonate to a urine pH of 7.5 to 8.0; (6) recognise the indications for urgent haemodialysis; and (7) avoid the two lethal traps — intubation without maintaining hypocapnia, and premature discharge without ruling out rebound.[7][8]
The signature trap of this overdose is the well-looking patient who is compensating perfectly. Early on, the patient is agitated, hyperventilating, and sweaty — but may be oriented and able to give a history. The danger is that this is a compensated state: the metabolic acidosis is being offset by hyperventilation, and any loss of that compensation (sedation, intubation, exhaustion) causes a rapid, fatal acidosis as salicylate shifts into the central nervous system.[11]
Classification
Salicylate overdose is classified by serum level (severity), by clinical pattern (acute versus chronic), and by formulation — because each axis changes the threshold for treatment and dialysis.[7]
Acute single ingestion
- Entire dose taken within a defined short window
- Commonest in adolescents/young adults (deliberate self-harm) and young children (accidental)
- Toxic dose above 150 mg/kg or 6.5 g adult
- Classic mixed respiratory alkalosis + high anion-gap metabolic acidosis
- Done nomogram historically applicable (now superseded by serial levels)
Chronic salicylism (repeated dosing)
- Repeated supratherapeutic or therapeutic dosing over days to weeks
- Commonest in the elderly on long-term aspirin/analgesics
- MORE toxic at any given serum level (greater tissue distribution, less protein binding, more CNS toxicity)
- Often misdiagnosed as delirium, dementia, sepsis
- Lower threshold for haemodialysis (level over 600 mg/L)
Mixed (acute on chronic)
- Acute overdose in a patient already taking regular salicylate
- High baseline tissue levels; severe toxicity at lower apparent acute dose
- Lower dialysis threshold
- Always treat as severe
Two operational definitions anchor the topic. A toxic ingestion is an acute aspirin dose above 150 mg/kg or 6.5 g in an adult (lethal range generally above 10 to 30 g or 250 mg/kg).[7] An oil of wintergreen (methyl salicylate, approximately 98 percent) ingestion of as little as 4 mL in a child — or 30 mL in an adult — can be lethal, because methyl salicylate is far more concentrated than aspirin tablets: 1 mL of oil of wintergreen equals roughly 1.4 g of aspirin.[10]
The four toxic syndromes of salicylism — (1) respiratory alkalosis, (2) metabolic (high anion-gap) acidosis, (3) mixed disturbance (the hallmark in adults), and (4) non-cardiogenic pulmonary oedema — are not mutually exclusive but unfold over time: respiratory alkalosis first, then a rising metabolic acidosis, then (in severe poisoning) pulmonary oedema and CNS depression.[11]
Epidemiology & Risk Factors
Salicylate poisoning is among the commonest pharmaceutical overdoses worldwide and was historically the leading cause of fatal poisoning in children before the introduction of child-resistant packaging in the 1970s (United States, United Kingdom).[7][9]
Acute poisoning is commonest in adolescents and young adults (deliberate self-harm) and in young children (accidental ingestion of flavored aspirin or oil of wintergreen liniments). Chronic salicylism is commonest in the elderly on long-term antiplatelet or analgesic therapy, who develop insidious toxicity that is frequently missed.[3][7]
The most important population-level prevention intervention is the replacement of aspirin with paracetamol (acetaminophen) and ibuprofen as the first-line paediatric antipyretic, following the recognition that aspirin given to children with viral illness (especially influenza and varicella) is linked to Reye syndrome — a mitochondrial hepatopathy and encephalopathy with high mortality. Aspirin is now contraindicated in children under 16 unless specifically indicated (e.g. Kawasaki disease, juvenile idiopathic arthritis, rheumatic fever).[10]
Toxic thresholds — acute ingestion
- Adult: toxicity uncommon under 150 mg/kg or 6.5 g
- Risk rises steeply above 250 mg/kg or 10 g
- Lethal range above 10 to 30 g (or 500 mg/kg)
- Child: treat any ingestion above 150 mg/kg; check a level
Risk factors for severe toxicity at any given dose
- Elderly (reduced clearance, less albumin binding, acidosis)
- Dehydration, fever, metabolic acidosis (greater tissue partitioning)
- Co-ingestion of acidosis-producing agents (ethanol, methanol, ethylene glycol)
- Chronic ingestion (saturable kinetics, greater tissue distribution)
- Renal failure, hypoalbuminaemia
- Enteric-coated or sustained-release formulations (delayed, prolonged absorption)
- Methyl salicylate (oil of wintergreen) — highly concentrated
- Children under 5 with influenza/varicella (Reye syndrome)
The dose-response is steep. In a healthy adult an acute ingestion of aspirin above 150 mg/kg or 6.5 g is toxic; risk rises sharply above 250 mg/kg or 10 g, and the lethal range is roughly 10 to 30 g (or 500 mg/kg).[7] Methyl salicylate (oil of wintergreen, approximately 98 percent) is the most dangerous formulation by volume: 1 mL equals roughly 1.4 g of aspirin, so 4 mL in a child or 30 mL in an adult can be fatal.[10]
Pathophysiology
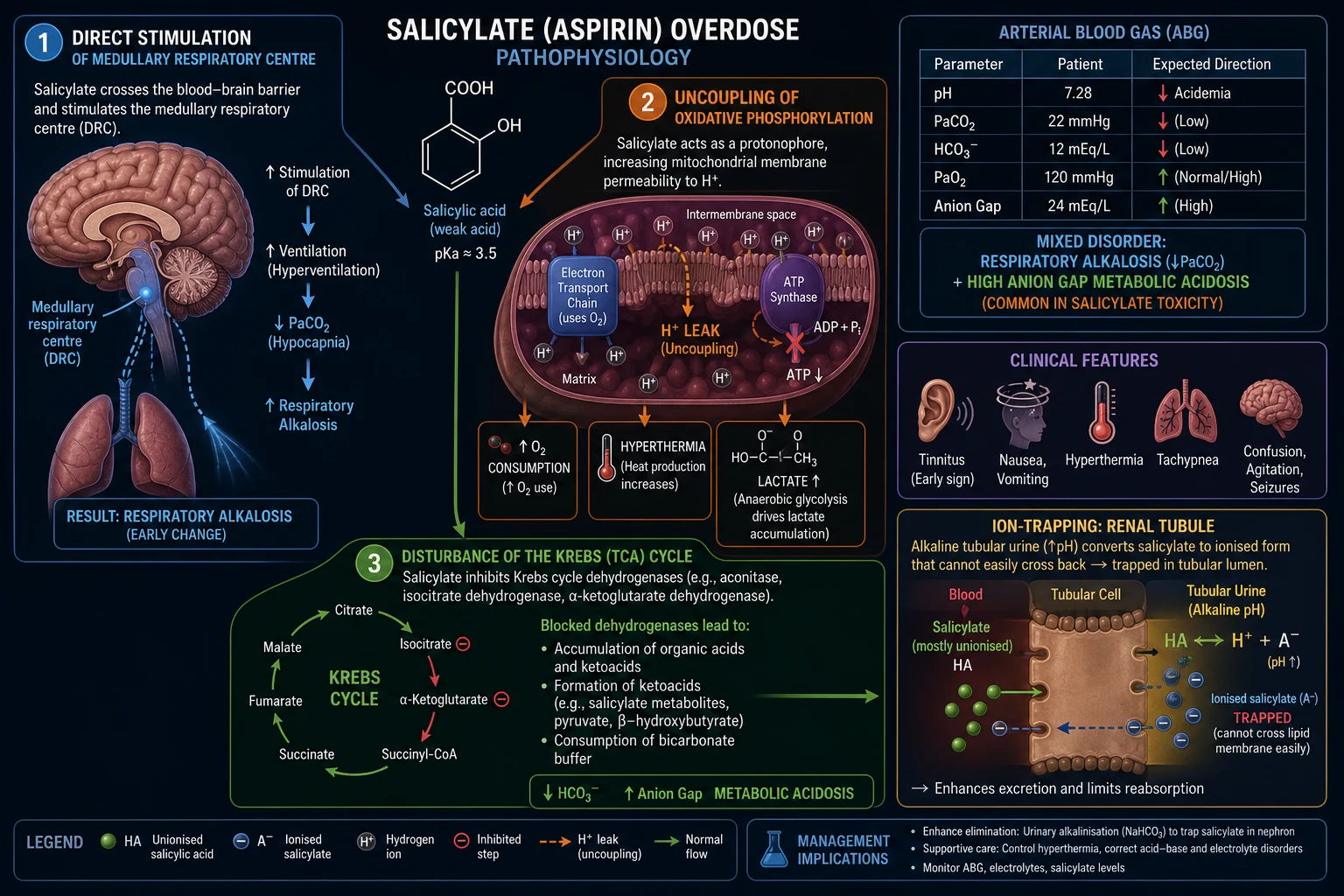
The molecular and cellular cascade of salicylate toxicity is one of the best-understood in clinical toxicology, and it explains every feature of the syndrome — the early respiratory alkalosis, the high anion-gap metabolic acidosis, the hyperthermia, the dehydration, the CNS toxicity, and the rationale for every treatment.[1][6]
Salicylic acid is a weak acid with a pKa of about 3.0. At physiological pH (7.4) it is almost entirely ionised and bound to albumin (the free fraction is small). In acidosis (systemic, respiratory, or local), in hypoalbuminaemia, in hyperthermia, and in dehydration, the free (unionised) fraction rises and salicylate crosses the blood-brain barrier and partitions into tissues (including CSF and brain) — explaining CNS toxicity and the paradoxical central (CNS) hypoglycaemia with a normal plasma glucose.[4]
Three principal mechanisms
1. Direct stimulation of the medullary respiratory centre. Salicylate directly stimulates the neurones of the medullary respiratory centre in the brainstem, increasing both the rate and depth of ventilation (true hyperpnoea, not just tachypnoea). The result is a primary respiratory alkalosis with a low PaCO2. This is the earliest and most consistent effect in acute adult poisoning, and it is why the patient is classically deep-sighing and rapid-breathing (a Kussmaul-like pattern).[7]
2. Uncoupling of oxidative phosphorylation. Salicylate acts as a protonophore — it carries hydrogen ions (protons) across the inner mitochondrial membrane, bypassing the FoF1 ATP synthase. The proton-motive force that normally drives ATP synthesis is dissipated as heat. The result is accelerated electron transport and oxygen consumption without commensurate ATP production, driving up heat generation (hyperthermia) and forcing a switch to anaerobic glycolysis (lactate accumulation). This is the same mechanism as 2,4-dinitrophenol (DNP), the banned weight-loss agent.[7]
3. Disturbance of intermediary (Krebs cycle) metabolism. Salicylate inhibits several Krebs-cycle (TCA) dehydrogenases — including isocitrate dehydrogenase and alpha-ketoglutarate dehydrogenase — and disrupts amino-acid transamination. The Krebs cycle slows, intermediates accumulate, and ketoacids and other organic acids are generated. These, together with lactate (from uncoupling) and the salicylate anion itself (which contributes 3 to 5 mmol/L to the anion gap), produce the high anion-gap metabolic acidosis.[7]
The classic adult blood gas — a MIXED disorder
Because salicylate simultaneously drives a respiratory alkalosis (centre stimulation) and a high anion-gap metabolic acidosis (uncoupling plus Krebs-cycle disturbance), the classic adult blood gas is a MIXED respiratory alkalosis + high anion-gap metabolic acidosis.[7]
Early in the course, the respiratory alkalosis dominates (low PaCO2 with a low or normal bicarbonate — but the bicarbonate is already lower than expected for the PaCO2 alone, a clue that a metabolic acidosis is brewing). Later, the metabolic acidosis dominates as lactate, ketones, and the salicylate anion accumulate. A normal or near-normal bicarbonate in a tachypnoeic salicylate patient is already abnormal — bicarbonate should be low from respiratory alkalosis, so a "normal" bicarbonate means a metabolic acidosis is being masked.[11]
Why the kidney matters — the ion-trapping principle
This is the rationale for urinary alkalinisation, the key non-dialysis treatment.[6]
Salicylic acid (HA, unionised) is lipid-soluble and crosses biological membranes by non-ionic diffusion. In an alkaline tubular urine (pH 7.5 to 8.0), HA entering the tubule is deprotonated to the salicylate anion (A-), which is charged and cannot back-diffuse across the tubular epithelium. The salicylate is therefore trapped in the urine and excreted. Renal clearance of salicylate rises roughly 5-fold at urine pH 8 versus urine pH 5 — this is why a small change in urine pH produces a large change in clearance.[11]
Why hypokalaemia blocks urinary alkalinisation
Hypokalaemia (common in salicylate toxicity from vomiting, secondary hyperaldosteronism, and urinary losses) causes the distal tubule to reabsorb potassium in exchange for secreting hydrogen ions (the distal H+/K+ exchange). The net effect is urinary acidification — the kidney cannot achieve a urine pH of 7.5 to 8.0 if the serum potassium is low. Potassium MUST be corrected (to over 4.0 mmol/L) before urinary alkalinisation will work.[7]
Fluid, glucose, and dehydration
Salicylate produces severe dehydration through three mechanisms: direct gastric irritation (vomiting), hyperventilation and fever (insensible losses), and an obligate solute diuresis (salicylate itself). Dehydration reduces renal salicylate clearance and perpetuates acidosis. Intravenous fluid resuscitation is mandatory and must include dextrose, because — despite a normal or even high plasma glucose — the brain is starved of glucose (cerebral hypoglycaemia from inhibition of cerebral glucose utilisation). Glucose-containing fluid is mandatory even when plasma glucose is normal or high.[7]
Non-cardiogenic pulmonary oedema
In severe poisoning, salicylate damages pulmonary capillary endothelium (a direct toxic effect compounded by acidosis), increasing capillary permeability and producing non-cardiogenic (permeability) pulmonary oedema. The chest radiograph shows bilateral infiltrates with a normal heart size and JVP. This complication classically appears in severe poisoning, in chronic salicylism, and in the elderly; it predicts a worse outcome and is an indication for haemodialysis.[11]
Central nervous system toxicity
CNS features — tinnitus, high-frequency hearing loss, agitation, slurred speech, confusion, hallucinations, seizures, coma — arise from a combination of direct brainstem and cortical salicylate effect, CSF acidosis, cerebral oedema, and paradoxical CNS hypoglycaemia (low CSF glucose with a normal plasma glucose, due to inhibition of cerebral glucose utilisation).[7]
S-A-L-I-C-Y-L-A-T-E
Clinical Presentation
The clinical course of salicylate toxicity unfolds in a spectrum of severity rather than discrete phases (unlike paracetamol). The features can be grouped as early (mild), moderate, and severe, and the pattern differs sharply between adults and children, and between acute and chronic poisoning.[7]
Early (mild) features
The earliest and most consistent features are: tinnitus (ringing in the ears), high-frequency hearing loss (often unrecognised by the patient), nausea, vomiting (direct gastric irritation), diarrhoea, diaphoresis (sweating), flushing, hyperpnoea (deep, rapid, sighing breathing — not simply tachypnoea), mild agitation, and headache. The patient is alert, oriented, and often able to give a history — but is compensating against an evolving metabolic acidosis.[7]
Tinnitus correlates with serum level (begins around 200 to 300 mg/L) and is a useful bedside severity marker if a level is unavailable.[7]
Moderate features
As the level rises (450 to 700 mg/L), marked hyperventilation, fever, dehydration, lethargy, agitation, restlessness, mild confusion, tremor, and a mixed respiratory alkalosis + metabolic acidosis with hypokalaemia develop.[7]
Severe features
In severe poisoning (over 700 mg/L) the full syndrome emerges: confusion, delirium, hallucinations, slurred speech, seizures, coma, hyperthermia, hypotension, non-cardiogenic pulmonary oedema, oliguria and acute kidney injury, severe metabolic acidosis, hypoprothrombinaemia with bruising and bleeding, hypoglycaemia (especially in children), cerebral oedema, ARDS, cardiovascular collapse, and death.[7][11]
Atypical presentations — the examiner's favourites
Examiners test atypical presentations deliberately.[9]
The elderly (chronic salicylism) present with an insidious, neuro-predominant picture: confusion, slurred speech, agitation, hallucinations, staggering gait — WITHOUT the classic hyperventilation and tinnitus. They are frequently misdiagnosed as delirium, dementia, sepsis, stroke, or primary psychiatric illness, and this misdiagnosis contributes to the highest case-fatality of any salicylate presentation.[3][7]
Children differ in two key ways: hyperventilation may be absent or less marked, and metabolic acidosis predominates (often the dominant and earliest acid-base finding, unlike adults). Hypoglycaemia is common and dangerous, and seizures and coma appear early.[4]
Pregnancy: salicylate crosses the placenta, and the fetus is acidotic relative to the mother — so salicylate ion-traps in fetal tissues (especially CNS). Maternal toxicity is associated with high fetal mortality.[9]
Diabetic or chronic kidney disease patients may have a superimposed ketoacidosis or uraemic acidosis; the high anion-gap metabolic acidosis may be wrongly attributed to DKA or uraemia, missing the salicylate diagnosis.[9]
Non-cardiogenic pulmonary oedema is a specific severe-salicylate presentation: dyspnoea, hypoxia, bilateral infiltrates, normal heart size and JVP — it predicts severe poisoning and is an indication for haemodialysis.[11]
Differential Diagnosis
The differential of hyperpnoea + metabolic acidosis + agitation/fever is broad, but the mixed respiratory alkalosis + high anion-gap metabolic acidosis with tinnitus is highly characteristic of salicylate toxicity. When the history is uncertain, the following must be distinguished.[7][9]
Sepsis / septicaemia
- Fever, tachypnoea, confusion, metabolic acidosis, leucocytosis
- PRIMARY metabolic acidosis with respiratory compensation (NOT primary respiratory alkalosis)
- Identifiable source (chest, urine, abdomen, line)
- No tinnitus; salicylate level negative
Diabetic ketoacidosis (DKA)
- Hyperglycaemia, ketosis, high anion-gap acidosis, hyperventilation
- PRIMARY metabolic acidosis (Kussmaul breathing) — NOT a primary respiratory alkalosis
- Hyperglycaemia and ketones; no tinnitus
- May CO-EXIST with salicylate — check both levels
Other high-anion-gap acidoses (MUDPILES / GOLD MARK)
- Methanol/ethylene glycol: osmolar gap elevated
- Uraemia: high creatinine/urea
- Propylene glycol, iron, lactate (shock, metformin)
- All produce high anion-gap acidosis — but ONLY salicylate ALSO gives a primary respiratory alkalosis
- Check lactate, osmolar gap, salicylate, iron
Dinitrophenol (DNP) — uncoupling agent
- Also uncouples oxidative phosphorylation: hyperthermia, tachypnoea, acidosis
- History of weight-loss pill/bodybuilding supplement
- Usually NO tinnitus
- May cause FALSE elevation of salicylate assay
Theophylline toxicity
- Tachycardia, hyperventilation, agitation, seizures, hypokalaemia, metabolic acidosis
- Supraventricular arrhythmias and marked hypokalaemia
- Theophylline level elevated
- Check theophylline level in any tachypnoeic agitated patient
Carbon monoxide / cyanide / metformin (lactic acidosis)
- CO: carboxyhaemoglobin, cherry-red skin, exposure history
- Cyanide: soot/industrial exposure, bitter-almond
- Metformin: diabetic, AKI, profound lactic acidosis
- No tinnitus; salicylate level negative
Two intra-salicylate distinctions matter for management. Acute poisoning must be distinguished from chronic salicylism — chronic is more toxic at any given level (greater tissue distribution, more CNS toxicity) and needs a lower dialysis threshold.[3] And non-cardiogenic pulmonary oedema of salicylate toxicity must be distinguished from cardiogenic pulmonary oedema (normal heart size and JVP, no gallop, no response to diuretics).[11]
Clinical & Bedside Assessment
The history is the single most important step in salicylate overdose, and it must be precise. Establish: (1) the agent (aspirin, methyl salicylate/oil of wintergreen, combination products, bismuth subsalicylate, sulfasalazine, salsalate); (2) the dose in mg/kg (and the formulation — enteric-coated or sustained-release); (3) the timing of ingestion; (4) whether acute or chronic (over days to weeks); (5) co-ingestants (paracetamol, ethanol, opioid, toxic alcohols, theophylline); (6) regular medications (especially long-term aspirin, anticoagulants, diuretics); (7) comorbidity (renal, hepatic, cardiac, diabetes, pregnancy); (8) intent (deliberate self-harm versus accidental); and (9) the patient's weight.[7]
The focused bedside examination follows ABCDE: Airway (patency, especially with a co-ingested sedative); Breathing (rate AND depth — hyperpnoea is the cardinal sign, not simply tachypnoea; SpO2; auscultate for pulmonary oedema); Circulation (HR, BP, capillary refill, JVP for dehydration — the patient is almost always volume-depleted; temperature for hyperthermia); Disability (GCS, pupils, tremor, tinnitus reported by the patient); and Exposure (signs of self-harm, bruising from hypoprothrombinaemia, aspirin bottles in the bag).[7]
A bedside capillary glucose must be checked in every salicylate-overdose patient (especially children) — hypoglycaemia and cerebral hypoglycaemia can be present even when plasma glucose is normal.[7]
Recognise the cannot-miss clinical gestalt: a febrile, hyperpnooeic, agitated, sweaty patient with a mixed respiratory alkalosis and high anion-gap metabolic acidosis is salicylate-toxic until proven otherwise.[7]
Mental-state and suicide-risk assessment is mandatory; no deliberate-self-harm patient should be left unattended, and psychiatric assessment is required once the patient is medically stable.[10]
Investigations
The essential blood panel in every salicylate overdose is: serum salicylate level (repeat at 2 to 4 h initially, then serially), arterial OR venous blood gas (pH, PaCO2, bicarbonate, base excess, lactate), U&E (sodium, potassium, creatinine, urea), LFTs, coagulation (PT/INR), capillary glucose, FBC, paracetamol level (to exclude co-ingestion), and — as indicated — ethanol, toxic alcohols (osmolar gap), theophylline, pregnancy test, and a chest radiograph.[7]
The salicylate level — units and thresholds
The serum salicylate level is the cornerstone of severity assessment, but the units must be confirmed before interpreting.[7]
[7]The Done nomogram (1960) — historical context
The Done nomogram (Done 1960, Pediatrics) is a graph of serum salicylate (mg/dL, log scale, y-axis) against hours post acute single ingestion (x-axis), divided into zones predicting none, mild, moderate, or severe toxicity if untreated.[1]
Its limitations are such that it is now largely obsolete: it is valid only for a single acute ingestion, with a known time, of an immediate-release formulation; it is invalidated by chronic or repeated dosing, by enteric-coated or sustained-release formulations (delayed absorption), and by symptomatic patients. Modern practice uses serial salicylate levels with clinical assessment rather than the nomogram.[7]
The arterial blood gas — interpret with care
The classic adult blood gas is a mixed respiratory alkalosis + high anion-gap metabolic acidosis.[7]
- Early (acute adult): primary respiratory alkalosis — low PaCO2 with low or normal bicarbonate. A normal bicarbonate in a tachypnoeic salicylate patient is already abnormal — bicarbonate should be low from respiratory alkalosis, so a "normal" bicarbonate masks a metabolic acidosis.
- Developing: mixed respiratory alkalosis + high anion-gap metabolic acidosis — raised lactate, ketones.
- Late / severe: predominant metabolic acidosis (and a falling pH).
- Children: metabolic acidosis often dominates from the outset.[10]
Anion gap = Na - (Cl + HCO3); normal 8 to 12; it is raised in salicylate toxicity (lactate, ketoacids, the salicylate anion itself).[9]
Other laboratory findings
- Hypokalaemia — common, from vomiting, secondary hyperaldosteronism, and urinary losses; must be corrected before urinary alkalinisation will work.
- Hypoprothrombinaemia / INR elevation — salicylate impairs vitamin-K-dependent factor synthesis; distinguish from paracetamol or warfarin co-ingestion.
- Hyperglycaemia or, especially in children, hypoglycaemia.
- Acute kidney injury — pre-renal and direct.
- Leucocytosis — non-specific.[6]
Serial levels — the modern standard
A single salicylate level is never enough — repeat at 2 to 4 h initially to detect ongoing absorption and a rising level (especially with enteric-coated or sustained-release formulations, or bezoar formation).[7]
Chronic salicylism: the salicylate level does not always correlate with severity — chronic toxicity at a level of 400 to 500 mg/L may be far more dangerous than acute toxicity at 600 mg/L because of greater tissue distribution and CNS effects.[3][7]
After treatment: recheck the level every 2 to 4 h until it is falling and the patient is clinically well, because of REBOUND after stopping urinary alkalinisation.[12]
Management — Resuscitation
The time-critical resuscitation bundle for any significant salicylate overdose is:[7]
- ABCDE assessment, IV access, baseline bloods (salicylate level, ABG/VBG, U&E, INR, glucose, paracetamol, FBC).
- High-flow oxygen if hypoxic — caution: do NOT blunt the hyperventilatory compensation (avoid over-sedation).
- Cardiac monitoring, continuous SpO2.
- Capillary glucose immediately.
- IV fluid resuscitation — the patient is almost always volume-depleted; use a balanced crystalloid (Hartmann's or 0.9 percent saline) with dextrose (5 percent dextrose or dextrose-saline) to maintain normoglycaemia and prevent cerebral hypoglycaemia. DO NOT withhold glucose even if plasma glucose is normal or high.
- Correct hypokalaemia with intravenous potassium chloride — potassium MUST be over 4.0 mmol/L for urinary alkalinisation to work.[6]
GI decontamination
Activated charcoal 50 g orally (1 g/kg in children) within 1 hour of acute ingestion reduces salicylate absorption.[7] May be considered up to 2 hours with large ingestions or delayed absorption (enteric-coated). Multiple-dose activated charcoal (50 g every 4 h) enhances salicylate elimination by gut dialysis and may be used in moderate to severe poisoning.
Whole-bowel irrigation with polyethylene glycol is considered for large ingestions of enteric-coated or sustained-release aspirin where absorption is delayed.[10]
Gastric lavage is reserved for life-threatening ingestions within 1 hour with a protected airway. Ipecac is contraindicated.[1]
Indications for urgent haemodialysis (treat as time-critical)
[11]The two lethal traps
Intubation is a high-risk intervention in salicylate toxicity. Salicylate-toxic patients rely on hyperventilation to compensate their metabolic acidosis; sedation, paralysis, and a normally-set ventilator cause PaCO2 to rise, pH to fall, salicylate to shift into the CNS, and the patient to crash.[7]
If intubation is unavoidable (failure of oxygenation/ventilation, profound coma, cardiac arrest): (1) give a bicarbonate bolus and optimise pH pre-intubation; (2) pre-oxygenase; (3) use rapid-sequence intubation; (4) set the ventilator to MAINTAIN hypocapnia (respiratory rate 20 to 30, minute ventilation matched to pre-intubation); (5) have haemodialysis ready, because acidosis will worsen.[7]
Seizures: treat with IV benzodiazepines (lorazepam 4 mg or diazepam 10 mg, repeated); correct hypoglycaemia and acidosis; escalate to haemodialysis — seizures are a marker of severe poisoning.[10]
Hyperthermia: treat with active cooling (cooling blankets, evaporative cooling); antipyretics have NO role (the hyperthermia is from uncoupling, not a hypothalamic set-point).[7]
Management — Definitive & Stepwise
Urinary alkalinisation — the key non-dialysis treatment
The cornerstone of enhanced elimination in salicylate poisoning is urinary alkalinisation with intravenous sodium bicarbonate, titrated to a urine pH of 7.5 to 8.0.[6]
Mechanism: unionised salicylic acid (HA) diffuses across the tubular epithelium into the alkaline tubular urine, where it is deprotonated to the impermeant salicylate anion (A-) and ion-trapped for urinary excretion. Renal clearance rises roughly 5-fold at urine pH 8 versus pH 5.[6]
Evidence base: the Prescott 1982 BMJ study (Diuresis or urinary alkalinisation for salicylate poisoning?) established that alkalinisation of urine — not large fluid volumes — is the active component of enhanced elimination.[6] This shifted practice away from forced alkaline diuresis (large fluid volumes with bicarbonate and potassium, now discouraged due to pulmonary-oedema risk) toward urinary alkalinisation alone with modest fluid replacement.
Stepwise management ladder
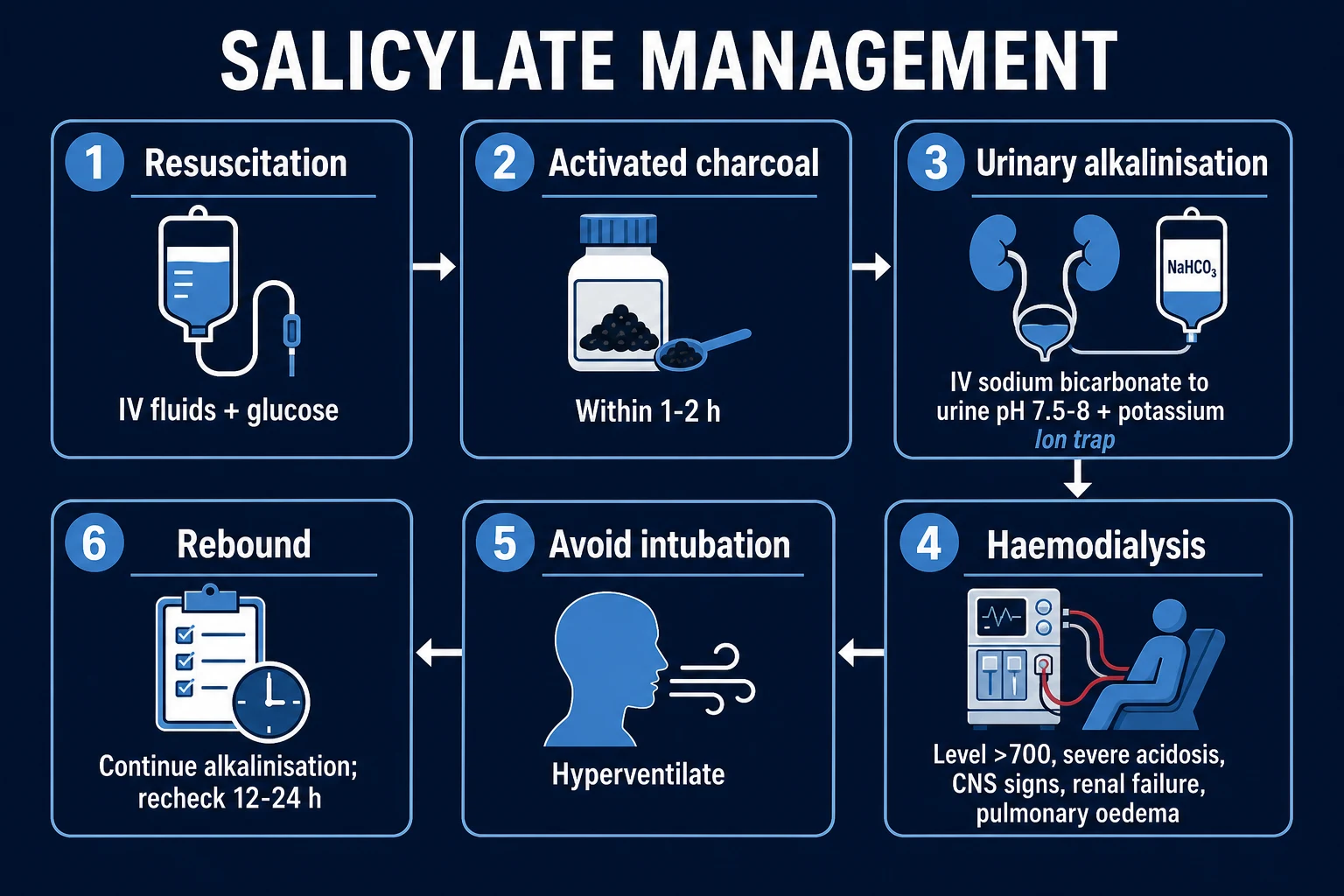
1. Resuscitate
- ABCDE; IV fluids WITH DEXTROSE; baseline bloods
- Cardiac monitoring; capillary glucose
- High-flow oxygen if hypoxic
2. GI decontamination
- Activated charcoal 50 g (1 g/kg child) within 1 to 2 h
- Multiple-dose charcoal 50 g every 4 h in moderate/severe
- Whole-bowel irrigation for large enteric-coated ingestion
3. Correct hypokalaemia
- IV potassium chloride; serum K+ must be over 4.0 mmol/L
- Without this, urinary alkalinisation will FAIL
4. Urinary alkalinisation
- IV sodium bicarbonate bolus plus infusion
- Titrate to urine pH 7.5 to 8.0
- Continue until level falling and patient well
5. Serial salicylate levels
- Every 2 to 4 h until falling
- Detect rising level (ongoing absorption) and rebound
6. Haemodialysis
- Level over 700 acute / over 600 chronic
- Severe acidosis, CNS signs, pulmonary oedema, renal failure
- Bicarbonate-based dialysate; single 4 to 6 h run
7. Post-dialysis
- Continue alkalinisation
- Recheck level (rebound)
- Repeat run if rebound
8. Admit and monitor
- Mild: short-stay with serial levels
- Moderate/severe: ICU
- Psychiatric assessment for self-harm
Haemodialysis — modality and dose
Intermittent haemodialysis is the modality of choice (EXTRIP class 1, grade 1D), clearing salicylate at roughly 80 to 100 mL/min and correcting acidosis, fluid overload, and electrolytes simultaneously.[8] A bicarbonate-based dialysate is preferred. A single 4 to 6 hour run usually reduces the level substantially. Post-dialysis, continue urinary alkalinisation and recheck the level because of REBOUND.[8][12]
When to stop treatment
Stop urinary alkalinisation and consider discharge when ALL of: (1) patient asymptomatic (no tinnitus, hyperpnoea, agitation, CNS signs); (2) salicylate level clearly falling on serial measurement; (3) normal acid-base; (4) no pulmonary or CNS signs.[7]
Continue alkalinisation for 12 to 24 h after the level falls, and recheck the level every 2 to 4 h for at least 12 h after stopping, to detect and prevent rebound.[12]
Drugs with NO role
There is NO role for N-acetylcysteine, fomepizole, ethanol, flumazenil, naloxone, or any other antidote in pure salicylate poisoning — recognise co-ingestants and treat each component.[7]
Forced alkaline diuresis (large fluid volumes) is now discouraged in favour of urinary alkalinisation alone, due to fluid-overload and pulmonary-oedema risk.[6]
Specific Subtypes & Scenarios
Enteric-coated or sustained-release aspirin
Absorption is delayed and prolonged. Levels required at 4, 6, 8, and 12 h. Consider whole-bowel irrigation with polyethylene glycol for large ingestions. Longer observation (24 h).[7]
Methyl salicylate (oil of wintergreen)
Highly concentrated — 1 mL equals roughly 1.4 g of aspirin; 4 mL may kill a child, 30 mL an adult. Rapid severe toxicity. Charcoal within 1 h; aggressive urinary alkalinisation and early haemodialysis; paediatric ICU.[10]
Chronic salicylism (the elderly)
Lower dialysis threshold (level over 600 mg/L); prominent CNS toxicity; often misdiagnosed as delirium. Correct dehydration; aggressive urinary alkalinisation; consider early dialysis.[3][7]
Pregnancy
Salicylate crosses the placenta; the fetus is acidotic relative to the mother so ion-traps salicylate in fetal CNS — high fetal mortality. Maternal alkalinisation protects the fetus (alkalinising the mother alkalinises the fetus, reducing fetal salicylate trapping). Urgent delivery if maternal toxicity severe; haemodialysis may be needed. Obstetric and neonatal input. Salicylate poisoning is NOT per se an indication for termination, but severe maternal toxicity may necessitate urgent delivery.[9]
Children
Hypoglycaemia is the dominant metabolic threat — check glucose frequently, give dextrose. Metabolic acidosis dominates (unlike adults). Weight-based fluid and bicarbonate; charcoal 1 g/kg; urinary alkalinisation with care to avoid hypernatraemia/alkalaemia; child-protection assessment for any suspicious/repeated presentation; paediatric dialysis circuit if needed.[4][5]
Non-cardiogenic pulmonary oedema
Oxygen, CPAP/non-invasive ventilation if tolerated (caution with hyperventilation compensation), avoid fluid overload (urinary alkalinisation NOT forced diuresis), urgent haemodialysis; mechanical ventilation if needed with attention to maintaining hypocapnia.[11]
Seizures / coma
IV benzodiazepines; correct acidosis and hypoglycaemia; intubate and ventilate (maintaining hypocapnia); urgent haemodialysis; ICU.[7]
The patient requiring intubation
Pre-intubation: give a bicarbonate bolus and optimise pH; pre-oxygenase. Use rapid sequence. Set the ventilator to MAINTAIN hypocapnia (respiratory rate 20 to 30, EtCO2 matched to pre-intubation). Have haemodialysis ready — acidosis will worsen on loss of hyperventilation.[7]
Mixed overdose
Salicylate + paracetamol: treat both (paracetamol nomogram, NAC; urinary alkalinisation for salicylate). Salicylate + ethanol: chronic ethanol may impair metabolism but acute ethanol co-ingestion rarely changes management. Salicylate + opioid: naloxone for the opioid component. Salicylate + toxic alcohol (methanol/ethylene glycol): fomepizole, urinary alkalinisation, dialysis.[9]
Rebound toxicity
Tissue stores redistribute into the blood after dialysis or cessation of alkalinisation, sometimes to toxic levels. Recheck the level every 2 to 4 h for 12 to 24 h after stopping; resume alkalinisation or repeat dialysis if the level rises.[12]
Complications & Pitfalls
Disease complications
Neurological
- Cerebral oedema with intracranial hypertension
- Seizures and status epilepticus
- Coma and CNS depression
- Tinnitus and high-frequency hearing loss (usually reversible)
Respiratory
- Non-cardiogenic pulmonary oedema / ARDS
- Aspiration pneumonitis (vomiting or co-ingestant)
Metabolic
- Severe metabolic acidosis
- Hypokalaemia
- Hypoglycaemia (especially children, CNS)
- Hyperthermia
Renal
- Acute kidney injury (pre-renal and direct)
- Rebound after stopping alkalinisation
Haematological
- Hypoprothrombinaemia (low vitamin-K-dependent factor synthesis)
- Bruising, bleeding, GI haemorrhage
Cardiovascular
- Arrhythmia in severe poisoning
- Cardiovascular collapse and death
Classical pitfalls
S-A-L-I-C-Y-L-A-T-E P-I-T-F-A-L-L-S
The unit-confusion pitfall
Salicylate reported in mg/L (SI), mg/dL (US — divide by 10 for mg/L), or mmol/L (1 mmol/L = 138 mg/L). A level of 70 mg/dL = 700 mg/L = 5.1 mmol/L = dialysis threshold. ALWAYS confirm the local unit before deciding on dialysis.[7]
The rebound phenomenon
Salicylate distributes widely into tissues. After dialysis or cessation of alkalinisation, tissue salicylate redistributes into the blood, sometimes to toxic levels. Recheck the level every 2 to 4 h for 12 to 24 h after stopping alkalinisation; resume alkalinisation or repeat dialysis if the level rises.[12]
Medicolegal pitfall
Deliberate self-harm overdoses require a formal psychiatric assessment and, in many jurisdictions, mandatory psychosocial assessment. In India, the Mental Healthcare Act 2017 decriminalises self-harm attempts but mandates psychosocial assessment. Preserve the bottle/container and document the history.[9]
Prognosis & Disposition
The overall prognosis of acute salicylate poisoning recognised and treated early is good — mortality under 1 percent. Severe poisoning with CNS signs, pulmonary oedema, or acidosis carries significant mortality, and chronic salicylism in the elderly has the highest case-fatality.[3][7]
Predictors of poor outcome
Chronic poisoning, elderly, acidosis (arterial pH under 7.3), CNS signs (confusion, seizures, coma), pulmonary oedema, renal failure, very high level (over 700 mg/L acute, over 600 chronic), delayed presentation, intubation, co-ingestants.[7][8]
Disposition
Discharge from ED
- Asymptomatic, level clearly falling on serial measurement
- No CNS or pulmonary signs, normal acid-base
- Psychiatric assessment completed (for self-harm)
- Safety plan and crisis numbers given
Observation / short-stay unit
- Mild to moderate poisoning on urinary alkalinisation
- Serial levels every 2 to 4 h
- At least 12 to 24 h after level falling
ICU
- Severe poisoning (level over 700)
- CNS signs (confusion, seizures, coma)
- Non-cardiogenic pulmonary oedema / ARDS
- Severe acidosis (arterial pH under 7.25)
- Need for intubation
- Need for haemodialysis
Safety-net on discharge
Discharge only when the level is clearly falling, the patient is asymptomatic (no tinnitus, hyperpnoea, agitation, CNS signs), the acid-base is normal, and psychiatric assessment is complete (for self-harm). Document a safety plan and crisis numbers. Counsel the patient on the dangers of further salicylate use.[9]
Special Populations
Pregnancy
- Salicylate crosses placenta; fetus acidotic relative to mother so ion-traps in fetal CNS
- High fetal mortality; maternal alkalinisation protects the fetus
- Treat aggressively (urinary alkalinisation, dextrose, early dialysis)
- Obstetric and neonatal input; not per se an indication for termination
Children
- Hypoglycaemia is the dominant metabolic threat
- Metabolic acidosis dominates (unlike adults)
- Weight-based charcoal 1 g/kg and fluids
- Paediatric dialysis circuit; child-protection assessment
Elderly (chronic salicylism)
- Insidious neuro-predominant presentation (confusion, slurred speech, hallucinations)
- Lower dialysis threshold (over 600 mg/L)
- Correct dehydration and comorbidity; low threshold for ICU
- Highest case-fatality — do not miss
Chronic kidney disease / cirrhosis
- Lower clearance; altered protein binding; more free salicylate
- Lower threshold to dialyse
- Check for interactions (NSAIDs, anticoagulants)
Anticoagulated (warfarin, DOAC)
- Additive bleeding risk with hypoprothrombinaemia
- INR may be elevated by salicylate directly
- Haematology input; reverse anticoagulation per protocol if life-threatening bleed
Diabetes
- DKA may coexist; check ketones, glucose
- Treat both; insulin per protocol once glucose known
- Salicylate alone may cause hyperglycaemia
Oil of wintergreen (child)
- Treat as life-threatening regardless of small volume
- Charcoal; ICU; aggressive alkalinisation; early dialysis
- Notify poison centre
On long-term low-dose aspirin who acutely overdose
- High baseline tissue levels; treat as acute-on-chronic
- Lower dialysis threshold
Evidence, Guidelines & Regional Differences
The evidence base
The Done 1960 paper (Pediatrics) — Salicylate intoxication. Significance of measurements of salicylate in blood in cases of acute ingestion — is the foundation of the Done nomogram: a graph of serum salicylate against time post acute single ingestion predicting severity if untreated.[1] Its limitations (single acute ingestion only; invalidated by chronic, repeated, enteric-coated, sustained-release ingestion) are such that serial levels with clinical assessment now supersede the nomogram.[7]
The Prescott 1982 BMJ study — Diuresis or urinary alkalinisation for salicylate poisoning? — established that alkalinisation of urine, not large fluid volumes, is the active component of enhanced elimination.[6] This shifted practice away from forced alkaline diuresis (large fluid volumes with bicarbonate and potassium, now discouraged due to pulmonary-oedema risk) toward urinary alkalinisation alone.
The Temple 1981 Archives of Internal Medicine review — Acute and chronic effects of aspirin toxicity and their treatment — laid out the distinction between acute and chronic aspirin toxicity and the principles of management.[2]
The Gaudreault 1982 Pediatrics study — The relative severity of acute versus chronic salicylate poisoning in children — demonstrated that chronic salicylism is more toxic at any given serum level than acute poisoning, with greater CNS effects and worse prognosis.[3]
The EXTRIP 2015 recommendations (Juurlink et al., Annals of Emergency Medicine) — Extracorporeal treatment for salicylate poisoning: systematic review and recommendations from the EXTRIP Workgroup — give a class 1, grade 1D recommendation to use intermittent haemodialysis for severe salicylate poisoning (level over 700 mg/L acute / over 600 chronic, refractory acidosis, CNS toxicity, pulmonary oedema, renal failure).[8]
The Chan 1996 Postgraduate Medical Journal paper — The risk of severe salicylate poisoning following the ingestion of topical medicaments containing methyl salicylate — highlighted the danger of oil of wintergreen ingestions, especially in children.[10]
The Schou 2012 Lakartidningen paper drew attention to non-cardiogenic pulmonary oedema as a specific and under-recognised complication of acute salicylate poisoning.[11]
The O'Keefe 2023 Clinical Toxicology paper — Incidence of rebound salicylate toxicity following cessation of urine alkalinization — quantified rebound after stopping urinary alkalinisation, justifying the practice of rechecking levels for 12 to 24 h after cessation.[12]
Regional deltas
[6] [6]Australia and New Zealand (ANZ). Management aligned with EXTRIP and Toxbase conventions; bicarbonate infusion; intermittent haemodialysis for severe poisoning.
India (AIIMS / National Poisoning Centre). Salicylate (aspirin, combination analgesics, methyl salicylate liniments) is a common agent in deliberate and accidental poisoning. Serum levels are variably available; urinary alkalinisation with 8.4 percent sodium bicarbonate; haemodialysis access is variable in rural settings (and transport to a centre with dialysis may be needed). The Mental Healthcare Act 2017 decriminalises self-harm attempts but mandates psychosocial assessment. Europe (EurofiTox / Swiss Tox Info): urinary alkalinisation preferred over forced alkaline diuresis; haemodialysis indications per EXTRIP 2015.
Controversies
The forced alkaline diuresis versus urinary alkalinisation alone controversy: modern practice favours alkalinisation alone (Prescott 1982), as large fluid volumes add little to elimination beyond what alkalinisation achieves and increase pulmonary-oedema risk.[6]
The dialysis threshold controversy (700 mg/L acute versus 600 mg/L chronic) and the role of clinical severity over absolute level: clinical status (CNS, acidosis, pulmonary oedema) trumps the number — a symptomatic patient at 500 mg/L may need dialysis, an asymptomatic patient at 750 mg/L may not.[8]
The Done nomogram is now largely obsolete in favour of serial levels with clinical assessment.[7]
Exam Pearls
[6]GOLD MARK
Must-know numbers
- Toxic level: over 300 mg/L
- Severe: over 700 mg/L acute / over 600 chronic
- Toxic dose: above 150 mg/kg or 6.5 g adult
- Oil of wintergreen: 4 mL lethal in a child (1 mL equals 1.4 g aspirin)
- pKa: 3.0 (weak acid; ionised at physiological pH, unionised HA crosses BBB in acidosis)
- Urine pH target: 7.5 to 8.0
- Serum K+ target: over 4.0 mmol/L (or alkalinisation fails)
- Dialysis: over 700 acute / over 600 chronic, acidosis, CNS, pulmonary oedema, renal failure
Frequently misremembered (correctly stated)
- The adult blood gas is MIXED respiratory alkalosis + metabolic acidosis (NOT pure metabolic acidosis)
- Urinary ALKALINISATION, not forced alkaline DIURESIS (large fluid volumes cause pulmonary oedema)
- Give GLUCOSE even if blood sugar is normal (cerebral hypoglycaemia)
- Correct POTASSIUM before bicarbonate will work
- AVOID intubation; if intubated, hyperventilate to maintain pre-intubation PaCO2
- Antipyretics have NO role in the hyperthermia (it is uncoupling)
- Done nomogram is largely OBSOLETE — use serial levels
- Chronic salicylism is MORE toxic at the same level — lower dialysis threshold
Exam application bank (NEET-PG / INICET)
One-line answer
Salicylate (aspirin) overdose produces a characteristically MIXED acid-base disorder through three mechanisms: direct stimulation of the medullary respiratory centre (hyperventilation, primary respiratory alkalosis), uncoupling of oxidative phosphorylation in mitochondria (hyperthermia, increased oxygen consumption, lactate), and disturbance of the Krebs cycle (ketoacids and organic acids), together producing a high anion-gap metabolic acidosis. The classic adult blood gas is therefore primary respiratory alkalosis PLUS high anion-gap metabolic acidosis with tinnitus. Early features include tinnitus, deafness, nausea, vomiting, hyperpnoea, fever, sweating; severe poisoning causes agitation, confusion, seizures, hyperthermia, coma, non-cardiogenic pulmonary oedema and acute kidney injury. Diagnosis rests on a serum salicylate level (over 300 mg/L toxic, over 700 severe) with serial measur[11]
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard.[5]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes.[6]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change.[3]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each.[3]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory.[12]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Salicylate (Aspirin) Overdose.
References
- [1]Done AK. Salicylate intoxication. Significance of measurements of salicylate in blood in cases of acute ingestion. Pediatrics, 1960.PMID 13723722
- [2]Temple AR. Acute and chronic effects of aspirin toxicity and their treatment. Archives of Internal Medicine, 1981.PMID 7469627
- [3]Gaudreault P, Temple AR, Lovejoy FH Jr. The relative severity of acute versus chronic salicylate poisoning in children: a clinical comparison. Pediatrics, 1982.PMID 7122154
- [4]Snodgrass WR. Salicylate toxicity. Pediatric Clinics of North America, 1986.PMID 3960612
- [5]Snodgrass W, Rumack BH, Peterson RG, Holbrook ML. Salicylate toxicity following therapeutic doses in young children. Clinical Toxicology, 1981.PMID 7237957
- [6]Prescott LF, Balali-Mood M, Critchley JA, Johnstone A, Proudfoot AT. Diuresis or urinary alkalinisation for salicylate poisoning? British Medical Journal (Clinical Research Edition), 1982.PMID 6291695
- [7]O'Malley GF. Emergency department management of the salicylate-poisoned patient. Emergency Medicine Clinics of North America, 2007.PMID 17482023
- [8]Juurlink DN, Gosselin S, Kielstein JT, Ghannoum M, Lavergne V, Nolin TD, Hoffman RS; EXTRIP Workgroup. Extracorporeal treatment for salicylate poisoning: systematic review and recommendations from the EXTRIP Workgroup. Annals of Emergency Medicine, 2015.PMID 25986310
- [9]Greene SL, Dargan PI, Jones AL Acute poisoning: understanding 90% of cases in a nutshell. Postgraduate medical journal, 2005.PMID 15811881
- [10]Chan TY The risk of severe salicylate poisoning following the ingestion of topical medicaments or aspirin. Postgraduate medical journal, 1996.PMID 8871462
- [11]Schou M, Jönsson AK. Acute salicylate poisoning may cause non-cardiogenic pulmonary oedema. Lakartidningen, 2012.PMID 22530469
- [12]O'Keefe M, Stanton M, Feldman R, Theobald J. Incidence of rebound salicylate toxicity following cessation of urine alkalinization. Clinical Toxicology (Philadelphia), 2023.PMID 37427892