Endocrinology · Endocrinology
Hypoglycaemia
Also known as Low blood glucose · Hypo · Insulin reaction · Neuroglycopenia
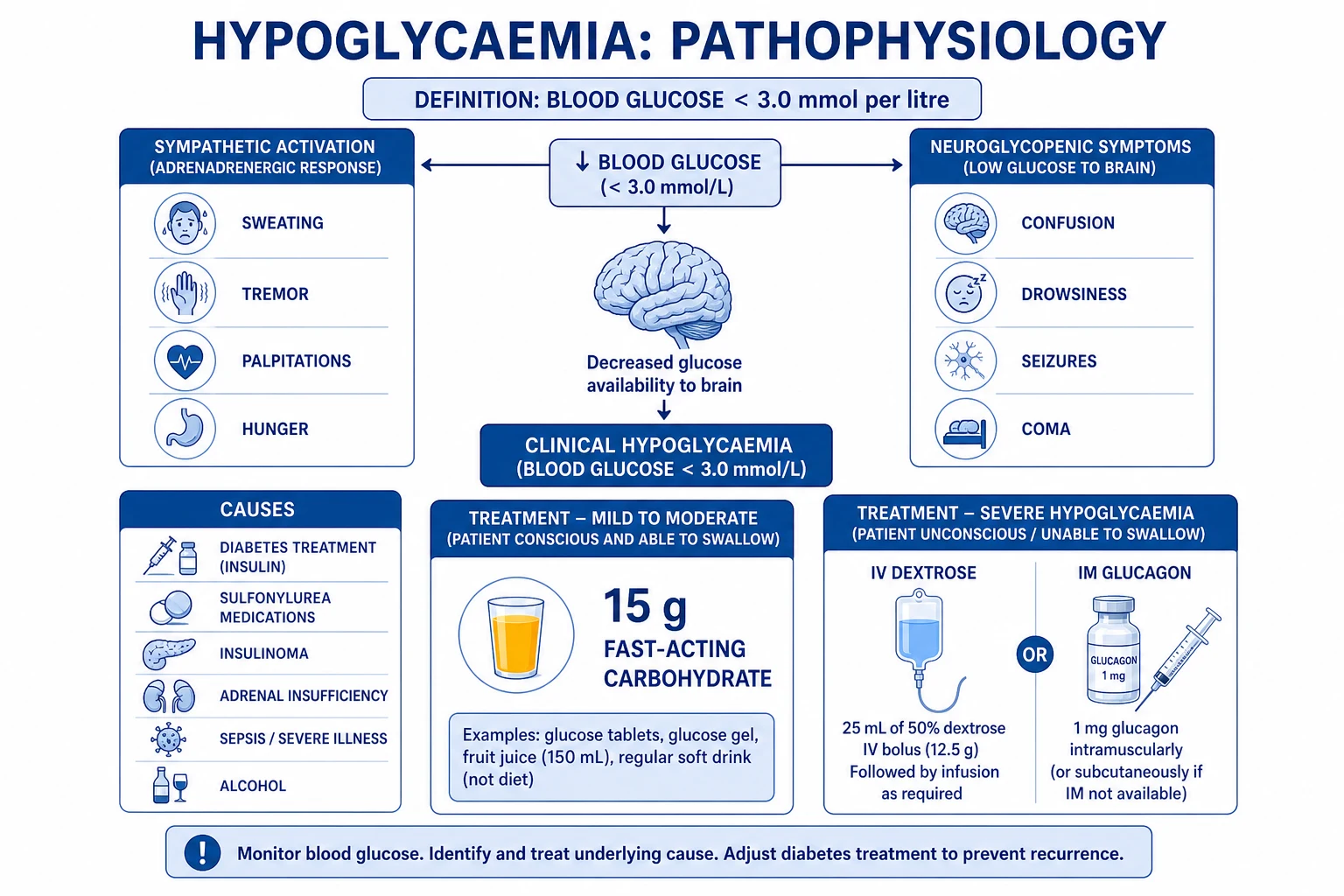
Hypoglycaemia is plasma glucose low enough to cause symptoms (typically under 3.0 mmol/L / 54 mg/dL). It produces a biphasic clinical syndrome: first autonomic / sympathetic activation (sweating, tremor, palpitations, hunger, anxiety) at glucose roughly 3.3 to 3.7 mmol/L, then neuroglycopenia (confusion, drowsiness, seizures, coma, and at its extreme, death) as glucose falls below 3.0 mmol/L. In adults in the community the dominant cause is glucose-lowering therapy in diabetes (insulin, sulfonylureas, glinides); in non-diabetics, insulinoma, non-islet cell tumour hypoglycaemia (IGF-II), adrenal insufficiency, alcohol, sepsis/critical illness, and autoimmune insulin syndrome must each be excluded. The diagnostic cornerstone is Whipple's triad (symptoms + low documented glucose + relief with glucose). Treatment is layered: mild — 15 g fast-acting oral carbohydrate, recheck at 15 minutes; severe (unconscious or unable to swallow) — IV 10% dextrose or IM/SC glucagon 1 mg, but glucagon is ineffective in sulfonylurea overdose and depleted glycogen states and octreotide is added for sulfonylurea poisoning. Recurrent hypoglycaemia causes hypoglycaemia-associated autonomic failure (HAAF) and hypoglycaemia unawareness, resetting the glycaemic threshold at which symptoms occur — the most dangerous complication of long-term insulin therapy. Avoidance through structured glucose targets, patient education, CGM, and the 15-15 rule prevents the morbidity that the ACCORD, ADVANCE and VADT trials linked to intensive glucose lowering.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Exam tags
Red flags
Overview & Definition
Hypoglycaemia is, formally, a plasma glucose low enough to produce symptoms or to warrant intervention. The brain depends on a continuous exogenous glucose supply because it neither stores nor synthesises glucose; when delivery falls, cerebral metabolism is impaired within minutes.[3][11]
The threshold for clinical hypoglycaemia is debated, but three concentric cutoffs are used:[1][2]
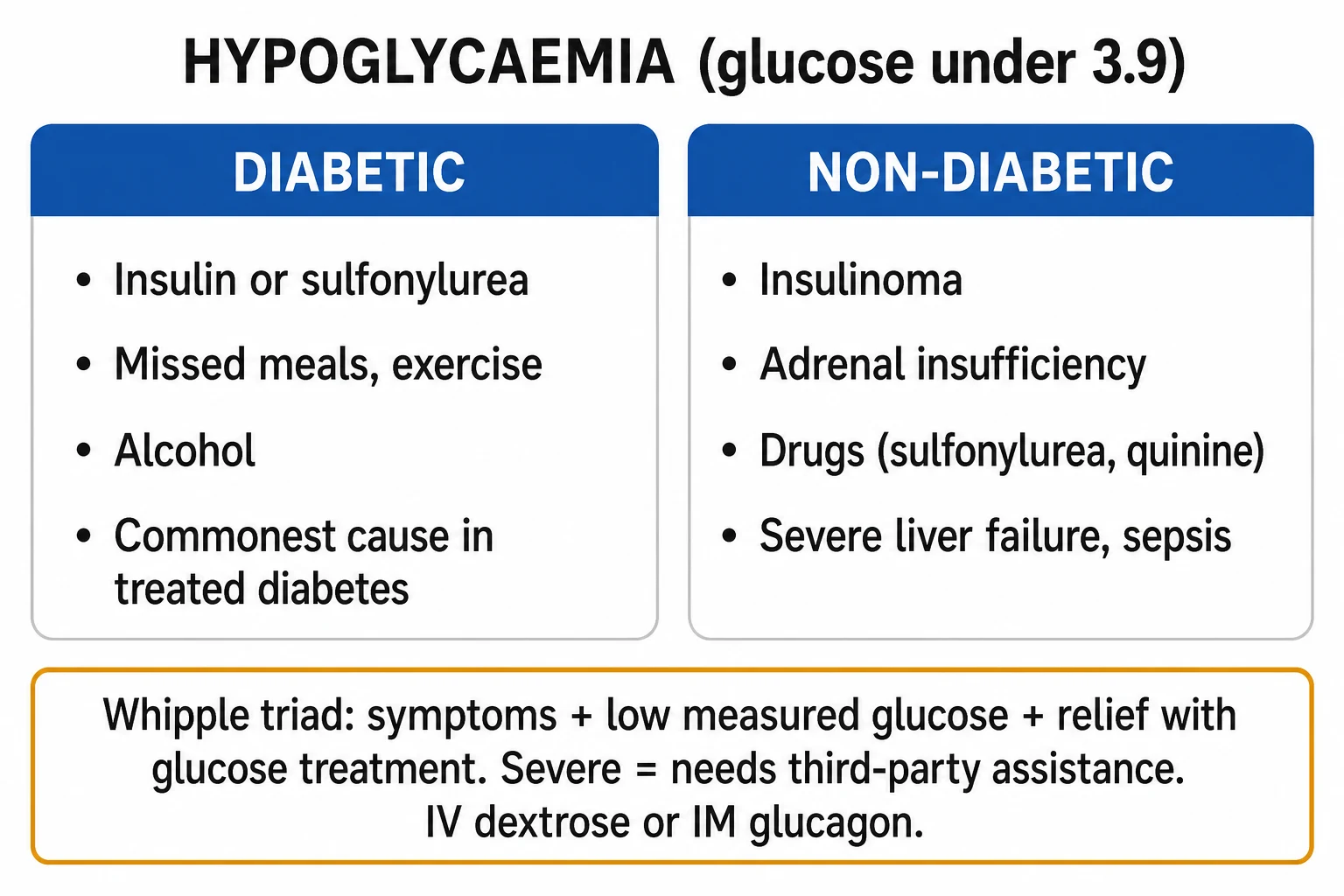
- Clinical hypoglycaemia (in people with diabetes) — glucose under 3.9 mmol/L (70 mg/dL). At this level counter-regulatory hormones already rise, and self-correction is advised.
- Alert / glycaemic alert value — glucose under 3.0 mmol/L (54 mg/dL). This is the International Hypoglycaemia Study Group alert threshold for clinically important hypoglycaemia to be reported in trials (endorsed by ADA, EASD, and the Endocrine Society).[2]
- Severe hypoglycaemia (operational definition) — an event requiring assistance of another person to actively administer carbohydrate, glucagon, or other resuscitative action; plasma glucose is often not measured, and recovery is judged by neurological recovery after treatment.[2]
The single overarching diagnostic principle is Whipple's triad, without which the diagnosis of true hypoglycaemia (and the justification for invasive investigation) cannot be made:[1][3]
The clinical skill in hypoglycaemia is not the bedside correction (that is a formula: glucose → recover → reassess) but rather (1) recognising it in the patient who presents with collapse, seizure, confusion, or odd behaviour; (2) treating before diagnostic confirmation when glucose cannot be measured; and (3) in non-diabetic or recurrent presentations, pursuing the cause aggressively with the correct samples drawn during the episode.[1]
Classification

Hypoglycaemia is classified in three complementary ways — by clinical severity, by glycaemic threshold, and by causative mechanism. The clinically most useful division is diabetic vs non-diabetic, because it dictates the diagnostic workup.[1][2]
By clinical severity (ADA/Endocrine Society, in diabetes)[2]
Level 1 — Glycaemic alert
- Glucose under 3.9 mmol/L (70 mg/dL) but at least 3.0 mmol/L
- Patient self-treats with oral fast-acting carbohydrate (no assistance needed)
- Includes asymptomatic low glucose detected on monitoring
Level 2 — Clinically important
- Glucose under 3.0 mmol/L (54 mg/dL)
- Indicates clinically significant hypoglycaemia — the threshold endorsed by the International Hypoglycaemia Study Group for trial reporting
- Sufficiently low to impair cognition; the patient can usually still self-treat
Level 3 — Severe
- Hypoglycaemia requiring assistance of another person (regardless of measured glucose)
- Often with confusion, seizures, or coma
- Treated with IV dextrose or IM/SC glucagon; neurological recovery defines success
By glycaemic threshold — the counterregulatory cascade
| Threshold (mmol/L) | Threshold (mg/dL) | What happens |
|---|---|---|
| 4.6 to 4.7 | 83 to 85 | Endogenous insulin secretion suppressed |
| 3.6 to 3.9 | 65 to 70 | Counter-regulatory hormones begin to rise (glucagon, adrenaline) — autonomic warning starts |
| 3.3 to 3.5 | 60 to 63 | Onset of autonomic / sympathetic symptoms (sweating, tremor, palpitations, hunger) |
| 2.8 to 3.0 | 50 to 54 | Onset of cognitive dysfunction and neuroglycopenia — symptom recognition itself becomes impaired |
| Below 2.5 | Below 45 | Confusion, drowsiness, behavioural change; EEG slows |
| Below 1.5 to 2.0 | Below 27 to 36 | Seizures, coma; risk of permanent neuronal injury if prolonged |
In a non-diabetic these thresholds are remarkably reproducible; in long-standing insulin-treated diabetes they are shifted to lower glucose values because of hypoglycaemia-associated autonomic failure (HAAF) (see Pathophysiology).[4]
By cause — the framework that drives the differential diagnosis
Diabetic (treatment-related)
- By far the commonest cause in clinical practice
- Insulin (especially in T1DM and basal-bolus T2DM regimens), sulfonylureas (glibenclamide most notorious), glinides (repaglinide, nateglinide)
- Skipped meals, exercise without carbohydrate adjustment, dose error, alcohol, renal impairment, interacting drugs (beta-blockers mask warning)
- Often amenable to education and regimen adjustment
Insulin-mediated non-diabetic
- Insulinoma (pancreatic beta-cell tumour) — classic 'whipple triad + high insulin, C-peptide, proinsulin'
- Autoimmune insulin syndrome (Hirata) — antibodies bind and then release insulin unpredictably; high total insulin, low free insulin
- Surreptitious/exogenous insulin abuse — high insulin, LOW C-peptide, low sulfonylurea screen
- Sulfonylurea ingestion (Munchausen/factitious) — high insulin, high C-peptide, POSITIVE sulfonylurea screen
Non-insulin-mediated non-diabetic
- Critical illness (sepsis, hepatic failure, severe heart failure, renal failure, malaria)
- Drug/toxin — alcohol, beta-blockers, quinine, salicylates, pentamidine, disopyramide, DJ-1103 Chinese herb
- Hormone deficiency — adrenal insufficiency (Addisonian crisis), hypopituitarism, isolated GH/cortisol deficiency in children
- Non-islet cell tumour hypoglycaemia (NICTH) — big tumours secreting incompletely processed 'big IGF-II' (e.g. solitary fibrous tumour, hepatoma, retroperitoneal sarcoma)
- Severe malnutrition, prolonged fasting, anorexia nervosa, inborn errors of metabolism
Reactive / postprandial
- Post-Roux-en-Y gastric bypass — late dumping and endogenous GLP-1-driven hyperinsulinaemic hypoglycaemia ('nesidioblastosis')
- Idiopathic postprandial syndrome — symptoms without documented low glucose (no true hypoglycaemia)
- Pre-diabetes / early T2DM — exaggerated late post-meal insulin surge
Paediatric / neonatal
- Neonatal: infant of diabetic mother, prematurity, intrauterine growth restriction, sepsis, inborn errors (galactosaemia, hereditary fructose intolerance, GSD, fatty-acid oxidation defects)
- Idiopathic ketotic hypoglycaemia of childhood — commonest cause after age 1 year; presents with fasting hypoketotic hypoglycaemia
- Congenital hyperinsulinism — ABCC8/KCNJ11 mutations, Beckwith-Wiedemann syndrome
Epidemiology & Risk Factors
Hypoglycaemia is the commonest acute complication of diabetes treatment and is the principal barrier to achieving good glycaemic control.[4][5]
In type 1 diabetes the average adult experiences about two episodes of symptomatic hypoglycaemia per week and one episode of severe hypoglycaemia per year; about 2 to 6 per cent of deaths in T1DM are attributable directly to hypoglycaemia (the so-called dead-in-bed syndrome).[4][10]
In type 2 diabetes the population-attributable burden is even greater because of its far higher prevalence; severe hypoglycaemia rates rise sharply with insulin use, sulfonylurea use, and longer duration of disease.[5]
Key numbers
Risk factors for hypoglycaemia in diabetes (a list an examiner expects verbatim):[2][5]
- Strict glycaemic control (HbA1c low or normal) — the ACCORD, ADVANCE and VADT trials all showed that intensive glucose lowering increases severe hypoglycaemia, and ACCORD was stopped early because of excess mortality in the intensive arm.[7][6]
- Prior severe hypoglycaemia — the strongest single predictor; one severe event multiplies the risk of the next.
- Hypoglycaemia unawareness — defective autonomic warning; affects ~25 per cent of T1DM and ~10 per cent of insulin-treated T2DM.[10]
- Long duration of insulin-treated diabetes (loss of glucagon response, autonomic neuropathy).
- Renal impairment — reduced insulin clearance and gluconeogenesis; common in elderly T2DM.
- Hepatic failure, heart failure, sepsis, malignancy — impaired gluconeogenesis and glycogen stores.
- Skipping meals, alcohol, exercise without carbohydrate adjustment.
- Drugs: sulfonylureas (especially glibenclamide due to long half-life), insulin, glinides, beta-blockers (mask warning, inhibit gluconeogenesis), ACE inhibitors, pentamidine (initial insulin release), quinine, salicylates.
- Extremes of age — neonates and the elderly have less effective counterregulation.
- Cognitive impairment, dementia — patient cannot recognise or self-treat.[2]
Risk factors for hypoglycaemia in non-diabetics are essentially the causes above; the prevalence of insulinoma is about 1 to 3 per million person-years, with a slight female predominance and a peak age range of 30 to 60.[8]
Pathophysiology
Understanding hypoglycaemia means understanding glucose homeostasis and its counterregulation. In the fed state, glucose is supplied from food. After 4-6 hours, hepatic glycogenolysis maintains glucose (stores are exhausted within ~24 hours), and thereafter gluconeogenesis from lactate, glycerol, and amino acids (driven by glucagon and cortisol) takes over. The brain consumes ~100 g glucose/day and cannot store it; if supply drops, symptoms begin within minutes.[3][11]
The counterregulatory cascade (normal)
When glucose falls, a tightly choreographed response is triggered, initiated by glucose-sensing neurones in the ventromedial hypothalamus and the brainstem. The hormones that protect glucose are released in a fixed sequence:[4][10]
- Suppression of endogenous insulin (glucose about 4.6 mmol/L) — the earliest, fastest signal; removes insulin's antigluconeogenic, antilipolytic effect.
- Glucagon release from pancreatic alpha-cells (about 3.6 to 3.9 mmol/L) — drives hepatic glycogenolysis and gluconeogenesis within minutes.
- Adrenaline release from the adrenal medulla (about 3.4 to 3.6 mmol/L) — supports hepatic glucose output, inhibits peripheral glucose utilisation, drives lipolysis and ketogenesis, and produces the autonomic symptoms (sweating, tremor, palpitations, hunger, anxiety) through beta-adrenergic and cholinergic pathways.
- Cortisol and growth hormone (about 3.0 mmol/L) — slower onset (hours); support gluconeogenesis. [1]
Why the brain fails
The brain, unlike muscle, does not require insulin for glucose uptake (GLUT-3 transporters are insulin-independent), so it is defenceless against low glucose. As glucose falls below about 3.0 mmol/L, synaptic transmission slows, EEG frequency decreases, and cognitive function deteriorates. By 2.5 mmol/L there is confusion and behavioural change; below 1.5 to 2.0 mmol/L there are generalised seizures and coma, and irreversible neuronal injury can follow prolonged or recurrent severe episodes.[11]
Hypoglycaemia-associated autonomic failure (HAAF) — the key chronic complication
In patients with long-standing insulin-treated diabetes, recurrent hypoglycaemia induces a maladaptive reset of the counterregulatory threshold: both the autonomic response and the glucagon response shift to lower glucose values, and may be abolished altogether. This is termed hypoglycaemia-associated autonomic failure (HAAF) or, clinically, hypoglycaemia unawareness.[4][10]
The mechanism is a central nervous system adaptation — antecedent hypoglycaemia reduces the sympathoadrenal response to subsequent hypoglycaemia (the brain learns to tolerate lower glucose). The clinical consequence is dangerous: the first warning the patient has is neuroglycopenia (confusion, coma) rather than the protective sweating/tremor, so episodes are missed until severe. [1]
HAAF is partly reversible with 2-3 weeks of strict hypoglycaemia avoidance — this is the rationale for relaxing glucose targets (e.g. HbA1c up to 64 mmol/mol / 8 per cent) and using CGM with low-glucose alarms after any severe event.[4]
The vicious cycle
The pathophysiology of hypoglycaemia in diabetes is a vicious cycle: intensive insulin therapy → recurrent mild hypoglycaemia → HAAF → unawareness → severe hypoglycaemia → further HAAF. Breaking the cycle (educating the patient, lowering insulin doses, CGM, screening for nocturnal hypoglycaemia) is the cornerstone of long-term management.[4]
Clinical Presentation
The clinical face of hypoglycaemia is the biphasic symptom complex — autonomic followed by neuroglycopenic. The tempo depends on the cause: insulin-induced hypoglycaemia is rapid (minutes); sulfonylurea, insulinoma, alcohol, and critical illness are slower (tens of minutes to hours). [1]
Autonomic (sympatho-adrenal) symptoms — the warning system
Sweating, tremor, palpitations, hunger, anxiety, irritability, pallor, tachycardia, piloerection, dry mouth, nausea. These usually appear at glucose 3.3 to 3.7 mmol/L and precede cognitive impairment. They are mediated partly by adrenaline and partly by acetylcholine (sympathetic cholinergic fibres to sweat glands). [1]
A time-honoured mnemonic: [1]
SWEATING
the commonest autonomic feature
generalised, with tremor
fatigue, lethargy
patient feels impending doom
fine, adrenergic
and mood change
and hunger, often intense
tachycardia
Neuroglycopenic symptoms — the danger zone
Difficulty concentrating, confusion, drowsiness, slurred speech, blurred vision, incoordination, ataxia, behavioural change (sometimes bizarre or aggressive), headache, seizures, focal neurological deficit (rarely hemiparesis), coma, death. These appear at glucose under 3.0 mmol/L and reflect direct neuronal fuel failure.[3]
A second mnemonic for neuroglycopenia: [1]
CONFUSION
and disorientation
drowsiness, drifting off
the unifying mechanism
generalised tonic-clonic; rarely focal
the end-stage
and dysarthria, mimics stroke
ataxia, falls
bizarre, aggressive, alcohol-like
transient hemiparesis (rare)
Bedside clinical features at presentation
- Tachycardia, wide pulse pressure, pallor, sweating (sympathetic).
- Confusion, drowsiness, dysarthria, ataxia, seizures, coma (neuroglycopenic).
- Rarely, focal neurological signs (hemiplegic hypoglycaemia — a stroke mimic).
- In children: ** behavioural change, somnolence, seizures, early-morning convulsions**. [1]
Atypical and missed presentations (the exam corners)
- Hypoglycaemia unawareness — long-standing T1DM with HAAF present with coma or seizure without warning; the first sign is often a relative finding the patient unconscious in bed (the dead-in-bed syndrome is sudden nocturnal death presumed to be arrhythmia from hypoglycaemia).[4]
- Nocturnal hypoglycaemia — patient may sleep through it or wake with morning headache, lethargy, or unrefreshing sleep; CGM detects many asymptomatic nocturnal dips.[10]
- The elderly diabetic — confusion, falls, focal signs, or functional decline mistaken for stroke or delirium; always check glucose in any altered elderly patient, especially on insulin or sulfonylurea.
- The alcoholic — stupor attributed to intoxication; the actual cause may be alcohol-induced hypoglycaemia, which can be fatal if untreated.
- The pregnant diabetic — tighter glucose targets increase risk; symptoms may be atypical; ketoacidosis can coexist with apparent normoglycaemia.
- Malignancy-driven (NICTH) — recurring fasting hypoglycaemia with a large tumour mass (often retroperitoneal, hepatic, solitary fibrous tumour); look for the low insulin, low C-peptide, low IGF-I but high 'big IGF-II' profile.[9]
- Autoimmune insulin syndrome (Hirata) — recurring postprandial hypoglycaemia with high total insulin and detectable insulin autoantibodies; classically in patients with autoimmune disease (Graves, SLE) or after exposure to sulfhydryl drugs (methimazole, captopril).
- Factitious / surreptitious — non-diabetic patients (often healthcare workers) who self-inject insulin or take sulfonylureas; the workup is identical to insulinoma but C-peptide distinguishes exogenous insulin (low) from endogenous (high).
Differential Diagnosis
The differential of a patient presenting with altered consciousness, collapse, or seizure is wide; hypoglycaemia is excluded in 60 seconds by a finger-prick glucose and that test must never be omitted.[1]
Hypoglycaemia
- Glucose under 3.0 mmol/L (severe, under 2.5 mmol/L)
- Onset often minutes (insulin) to hours (sulfonylurea, insulinoma)
- Autonomic + neuroglycopenic features; Whipple triad positive
- Resolves within minutes of IV/PO glucose
Diabetic ketoacidosis (DKA)
- Hyperglycaemia (typically over 11 mmol/L), ketosis, acidosis
- Kussmaul breathing, dehydration, ketotic breath
- Glucose high, ketones high, pH low
- Treated with IV fluids, insulin, K+ — opposite of hypoglycaemia
Hyperosmolar hyperglycaemic state (HHS)
- Marked hyperglycaemia (over 30 mmol/L), no ketosis, severe dehydration, often elderly T2DM
- Sodium often high, osmolality over 320 mOsm/kg
- Slower onset over days; neurological features prominent
Stroke / TIA
- Focal neurological deficit, hemiparesis, dysphasia
- Glucose normal; CT/MRI confirms
- Note: hypoglycaemia can MIMIC stroke — always check glucose first
Post-ictal state
- Confusion/drowsiness after witnessed seizure
- Glucose normal; may have bitten tongue, incontinent
- Hypoglycaemia is itself a seizure cause — measure glucose in EVERY seizure
Alcohol / drug intoxication
- History, smell of alcohol, opioid pin-point pupils, drug paraphernalia
- Co-ingestion common; alcohol itself causes hypoglycaemia — measure glucose
Sepsis with encephalopathy
- Fever, focus of infection, hypotension
- Glucose often high (stress response) but can be low in hepatic failure or malaria
Adrenal crisis
- Hypotension, hyponatraemia, hyperkalaemia, hyperpigmentation
- Hypoglycaemia is a feature — give parenteral hydrocortisone before tests
Head injury / intracranial event
- History of trauma, focal signs, decreased GCS
- Glucose normal; CT mandatory
- Always exclude hypoglycaemia first — it is the reversible mimic
Syncope (cardiac)
- Sudden brief LOC, no post-ictal confusion, pallor
- ECG, lying-standing BP; glucose normal
The can't-miss mimics in the unconscious patient — measure glucose in every patient with collapse, seizure, confusion, or reduced GCS:[1]
- Hypoglycaemia (the reversible mimic — 60 seconds to exclude).
- Opioid toxicity (pinpoint pupils — give naloxone).
- Meningitis/encephalitis (fever, neck stiffness — LP after CT).
- Intracranial haemorrhage (focal signs, hypertension).
- Sepsis. [1]
Clinical & Bedside Assessment
The focused assessment of suspected hypoglycaemia is rapid and combines bedside measurement with history and examination of the cause. [1]
The 60-second bundle
- Capillary (finger-prick) glucose — confirm a low value with two readings if the first is surprising (strip error, contamination). Treat before confirmation if glucose cannot be measured and the patient is symptomatic.[1]
- ABCDE — Airway (recovery position if unconscious); Breathing (rate, oxygenation); Circulation (pulse, BP, perfusion); Disability (GCS, pupils, blood glucose — this is the step where glucose is checked); Exposure (look for MedicAlert, insulin pump, sulfonylurea packet, injection sites).[1]
Focused history
- Diabetes? Insulin, sulfonylurea, glinide? When was the last dose? Skipped meal? Recent exercise? Alcohol?
- Renal, hepatic, cardiac, or adrenal disease?
- Time of onset, progression, autonomic vs neuroglycopenic phase.
- Previous severe events, hypoglycaemia unawareness, driving.
- Recent bariatric surgery, malignancy, autoimmune disease, drugs (sulfhydryl compounds — methimazole, captopril).
- Occupation (driving, machinery, healthcare worker → factitious). [1]
Focused examination
- Vitals (tachycardia, BP, resp rate, temperature — sepsis?).
- Skin — sweating, pallor (autonomic); hyperpigmentation, palmar crease darkening (Addison's); lipohypertrophy at injection sites (over-injected insulin).
- Hydration, perfusion, capillary refill.
- Neurological — GCS, pupils, focal deficit, seizure activity.
- Abdomen — hepatomegaly (glycogen storage, hepatic failure, malignancy), palpable mass (NICTH).
- Looking for insulin pump (failure, kink, occlusion), injection sites (lipohypertrophy), MedicAlert bracelet. [1]
Bedside manoeuvres and named signs
- Whipple's triad — the diagnostic standard (above).
- Hypoglycaemia unawareness — ask the patient: 'When your glucose is low, do you usually notice?' — a 'no' or 'sometimes' indicates impaired awareness (Clarke or Gold questionnaires quantify it).
- Glucose-reversal test — symptoms resolve within 10-15 min of raising glucose; if not, search for an alternative or coexisting cause. [1]
Investigations
The investigation strategy depends on whether the patient is a known diabetic (manage, then audit the regimen) or non-diabetic / recurrent (pursue the cause aggressively).[1][3]
Immediate (any patient)
- Capillary glucose (and a laboratory plasma glucose if there is any doubt — capillary readings are unreliable in shock, anaemia, and very high or very low glucose).
- Venous blood gas — glucose, lactate, ketones (β-hydroxybutyrate).
- ECG — exclude arrhythmia, silent MI; QT prolongation occurs with hypoglycaemia (risk of torsades).[11]
- U&E, FBC, LFT, CRP, blood cultures if sepsis suspected.
- Chest X-ray, urine dipstick looking for sepsis source.
In the diabetic (cause of the episode — audit)
- Review the regimen (insulin type, dose, timing; sulfonylurea, glinide).
- Review meal / exercise / alcohol around the event.
- HbA1c — overly tight control? a low HbA1c in a hypoglycaemia-prone patient is a red flag.
- Renal function — declining eGFR reduces clearance of insulin and sulfonylureas (especially glibenclamide — contraindicated if eGFR under 30).
- Consider CGM (or flash glucose monitoring) for 1-2 weeks to detect asymptomatic and nocturnal hypoglycaemia. [1]
In the NON-diabetic or recurrent patient — the diagnostic 'trough' samples
The single most important principle is that the diagnostic samples must be drawn DURING the spontaneous symptomatic episode, before any glucose is given. Once glucose is administered, insulin, C-peptide, proinsulin and β-hydroxybutyrate are no longer interpretable.[1][3]
The critical (trough) sample — during documented symptomatic hypoglycaemia (glucose under 3.0 mmol/L with Whipple triad):[1]
- Plasma glucose (laboratory).
- Insulin (raised in insulinoma, sulfonylurea, autoimmune; low in NICTH, adrenal insufficiency, critical illness).
- C-peptide (raised if endogenous insulin is the cause; low if exogenous insulin).
- Proinsulin (raised in insulinoma — unlike in surreptitious insulin).
- β-hydroxybutyrate — suppressed (under 2.7 mmol/L) when insulin is high (insulin suppresses lipolysis and ketogenesis); this is the single most useful discriminator.
- Sulfonylurea and meglitinide screen — positive in sulfonylurea-induced (factitious, accidental).
- Cortisol, growth hormone — exclude adrenal insufficiency, hypopituitarism.
- IGF-I, IGF-II, 'big IGF-II' — NICTH shows a high IGF-II : IGF-I ratio (over 10) and suppressed IGF-I.
- Insulin antibodies — autoimmune insulin syndrome.
- Blood alcohol, lactate, ammonia — exclude alcohol, inborn errors.
- Blood cultures, septic screen if sepsis. [1]
The 72-hour (actually 48-72 hour) supervised fast — insulinoma diagnosis
When spontaneous hypoglycaemia cannot be captured, perform a supervised fast in hospital (Endocrine Society):[1][3]
- Stop caloric intake; allow non-caloric clear fluids.
- Monitor capillary glucose every 1-2 hours, more often if symptoms.
- Draw the critical sample at the moment of symptomatic hypoglycaemia (glucose under 3.0 mmol/L with Whipple triad) — or at 72 hours if asymptomatic — and then terminate with glucose.
- 80 per cent of insulinomas declare by 24 hours, 90-95 per cent by 48 hours, virtually all by 72 hours.[3][8]
A mixed-meal test is used when the hypoglycaemia is postprandial (post-gastric-bypass): high-glucose meal, glucose and insulin measured for 4 hours; symptomatic postprandial hypoglycaemia with inappropriately high insulin supports late dumping / nesidioblastosis.[1]
Localising an insulinoma
Once biochemical diagnosis is made, localise:[8]
- Multiphase CT pancreas or MRI — first-line; sensitivity about 70-80 per cent.
- Endoscopic ultrasound (EUS) — most sensitive for small lesions (over 90 per cent); allows fine-needle aspiration.
- GLP-1 receptor PET/CT (⁶⁸Ga-DOTATATE or ⁶⁸Ga-exendin) — modern functional imaging; high sensitivity for occult lesions.
- Selective arterial calcium stimulation with hepatic venous insulin sampling (ASVS) — invasive, used when imaging is negative or multifocal disease suspected. [1]
Management — Resuscitation
Hypoglycaemia is a time-critical emergency. The principle is treat first, investigate after — never delay glucose while awaiting laboratory confirmation. The bedside rule of thumb: any unconscious or seizing patient gets a finger-prick glucose immediately, and a low value is treated as hypoglycaemia until disproven.[1][2]
The immediate bundle (ABCDE)
- Airway — recovery position if reduced GCS; airway adjunct if needed.
- Oxygen if hypoxic.
- Capillary glucose in every patient with collapse, seizure, confusion, or reduced GCS.
- IV access.
- Treat the glucose. [1]
Mild / moderate (patient conscious, able to swallow) — the 15-15 rule
The 15-15 rule is the patient-facing rule taught to every diabetic:[2]
- Give 15 g of fast-acting carbohydrate — examples: 3-4 glucose tablets (Dextrose 4 g each), 150-200 mL pure fruit juice or non-diet soft drink, 4-5 sugar cubes dissolved in water, 1 tablespoon honey or glucose gel (15 g), 3 teaspoons jam.
- Avoid chocolate and high-fat foods — fat slows absorption. Avoid foods with complex carbohydrates if the patient is severely symptomatic.
- Recheck capillary glucose at 15 minutes. If still under 4.0 mmol/L, give another 15 g.
- Once glucose recovers, give a long-acting carbohydrate snack (sandwich, biscuit, fruit, milk) — especially if a meal is more than an hour away, or after a sulfonylurea-induced event, to prevent relapse.
- In patients on alpha-glucosidase inhibitors (acarbose), pure sucrose is poorly absorbed — give pure glucose (dextrose), not table sugar. [1]
Severe (patient unconscious, fitting, or unable to swallow safely)
Two equally acceptable first-line agents; choice depends on IV access, the cause, and availability.[1][2]
IV dextrose — preferred where IV access is available: [1]
- Adults: 100 mL of 20% dextrose IV over 10-15 min, OR 150-250 mL of 10% dextrose; titrate to clinical response. (The historical 50% dextrose 25-50 mL is now avoided where possible — it is highly irritant, causes extravasation injury, and is hard to administer through a peripheral cannula; 10% or 20% are preferred.)[1]
- Children: 2 mL/kg of 10% dextrose IV bolus, then an infusion if needed.
- Effect: glucose rises within minutes; the patient usually wakes in 5-10 min.
- Caution: in malnourished or alcoholic patients, IV dextrose can precipitate Wernicke encephalopathy by exhausting thiamine — give IV thiamine (Pabrinex, 1 pair) before or with the dextrose in this group.[11]
- After the bolus, continue with a 10% dextrose infusion at a rate to keep glucose over 6 mmol/L (e.g. 100 mL/h) until the patient can eat and the underlying cause is addressed; recheck glucose every 15-30 minutes.
IM / SC glucagon — when IV access is impossible or being sought: [1]
- Adults and children over 8 years or 25 kg: 1 mg IM or SC (into the deltoid, thigh, or gluteal muscle).
- Children under 8 years or 25 kg: 0.5 mg IM or SC.
- Onset 5-15 minutes, peak effect 30 minutes; if no response by 15-20 minutes, give IV dextrose.
- After recovery, give oral long-acting carbohydrate to replete glycogen.
- Glucagon works by mobilising hepatic glycogen — therefore it is INEFFECTIVE in:
- Sulfonylurea / meglitinide overdose — the mechanism is endogenous insulin excess; glucagon may even stimulate further insulin release.
- Glycogen depletion (starvation, anorexia, severe liver disease, alcoholism, adrenal insufficiency).
- Endogenous hyperinsulinism (insulinoma) — partial, transient effect.
- Glucagon causes nausea and vomiting — beware airway in the obtunded patient. [1]
Buccal glucose gel (e.g. GlucoGel, 40% dextrose gel squeezed into the buccal mucosa) is useful as first aid in a conscious but uncooperative patient or in neonates; ineffective if mucosal perfusion is poor. [1]
Management — Definitive & Stepwise
Once the patient is resuscitated, the definitive management is cause-directed. The stepwise approach below addresses the common scenarios in turn. [1]
Step 1 — Stop ongoing offending agents
- Insulin overdose (self or iatrogenic) — adjust the dose; review injection technique and meal timing; check renal function; consider partial reversal if long-acting insulin (cannot reverse insulin in tissue, but a continuous dextrose infusion with hourly glucose monitoring for 12-24 h is required for glargine / detemir / degludec overdose).
- Sulfonylurea overdose — the most dangerous oral hypoglycaemic: it causes prolonged rebound hypoglycaemia for 24-48 h (glibenclamide is worst due to long half-life and active metabolites). Management:[2]
- Admit, monitor glucose hourly for 24-48 h.
- Octreotide 50-100 mcg SC every 8 h (suppresses insulin secretion; far more effective than dextrose alone at preventing rebound).
- IV 10% dextrose infusion titrated to keep glucose over 6 mmol/L.
- Avoid glucagon — it stimulates insulin release.
- Activated charcoal 50 g within 1-2 h of ingestion if a sustained-release preparation (e.g. glibenclamide SR).
- Haemodialysis is not effective (high protein binding).
- Glinide overdose — as for sulfonylurea but shorter half-life; usually 12-24 h observation.
Step 2 — Address the underlying cause
Insulinoma
- Surgical enucleation (laparoscopic or open) is curative for ~90 per cent of benign sporadic tumours
- Pre-operative medical control: **diazoxide 100-200 mg PO tds** (opens K-ATP channel, suppresses insulin); side-effects: oedema, hirsutism, nausea
- Alternative: **everolimus** (mTOR inhibitor) for malignant/metastatic insulinoma
- If unfit for surgery: diazoxide, everolimus, embolisation, RFA
- MEN1-associated insulinomas: screen for parathyroid and pituitary disease
Sulfonylurea overdose
- Stop the drug; admit 24-48 h (especially glibenclamide)
- Octreotide 50-100 mcg SC q8h + IV 10% dextrose
- Avoid glucagon; consider charcoal within 2 h
- Switch diabetes regimen to metformin/DPP4i/SGLT2i/GLP-1 RA/basal insulin after recovery
Adrenal crisis (primary or secondary)
- **IV hydrocortisone 100 mg stat, then 50 mg IV q6h** for 24 h, then taper
- IV 0.9% saline 1 L stat then 1 L over 2-4 h (often hypovolaemic, hyponatraemic)
- Continue dextrose as needed
- Confirm with short Synacthen test AFTER recovery; mineralocorticoid (fludrocortisone) added only once daily hydrocortisone under 50 mg
- Patient education, emergency hydrocortisone injection kit, steroid card, MedicAlert
Alcohol-induced hypoglycaemia
- Alcohol inhibits hepatic gluconeogenesis (NADH/NAD+ ratio shifts)
- **IV thiamine BEFORE dextrose** to avoid precipitating Wernicke
- IV 10% dextrose and fluids; correct electrolytes (Mg, K, PO4 — refeeding risk)
- Treat alcohol withdrawal if it emerges; refer for alcohol counselling
Sepsis / critical illness
- Identify and treat source (cultures, antibiotics within 1 h if septic)
- IV fluids, vasopressors, oxygen per Surviving Sepsis
- Dextrose infusion; correct hepatic/renal failure
- Exclude co-existing adrenal insufficiency if shock out of proportion
Non-islet cell tumour hypoglycaemia (NICTH)
- Tumour debulking/resection is definitive where feasible
- **Glucocorticoids** (prednisolone 30-60 mg/day or hydrocortisone) — suppress 'big IGF-II' secretion and raise glucose
- **Diazoxide, everolimus, somatostatin analogues** for inoperable tumours
- Frequent small meals, complex carbohydrate, cornstarch at night
- Often palliative — prognosis tied to underlying tumour
Autoimmune insulin syndrome (Hirata)
- Many cases remit spontaneously within months (autoantibody titre falls)
- **Frequent small, low-carbohydrate, high-protein meals** — avoids postprandial insulin surge
- **Diazoxide, glucocorticoids, immunosuppressants** for severe cases
- Plasmapheresis for acute severe refractory hypoglycaemia
- Stop offending drugs (sulfhydryl compounds: methimazole, captopril)
Post-bariatric hypoglycaemia
- Small, frequent, low-glycaemic-index meals; avoid simple sugars
- **Acarbose** (alpha-glucosidase inhibitor) reduces postprandial glucose surge and GLP-1
- **Diazoxide, somatostatin analogues (octreotide)** for refractory cases
- **Continuous subcutaneous insulin infusion rarely**; partial pancreatectomy in extreme cases
- Dietitian-led structured nutritional therapy first-line
Paediatric / neonatal
- Neonate: 2-10 mL/kg of 10% dextrose IV bolus, then infusion 6-9 mg/kg/min, titrate
- Buccal 40% dextrose gel (200 mg/kg) is first-line for at-risk neonates (avoid formula only)
- Idiopathic ketotic hypoglycaemia: avoid prolonged fasting; **uncooked cornstarch at bedtime**
- Congenital hyperinsulinism: **diazoxide 5-15 mg/kg/day**, glucagon infusion; **octreotide**; **near-total pancreatectomy** if refractory
- Inborn errors (GSD, FAO defects): dietary, enzyme-specific management with metabolic team
Step 3 — Prevent recurrence (the long view)
For the diabetic patient, recurrence prevention is the highest-yield intervention:[2][4]
- Relax glucose targets for 2-3 weeks after any severe episode — HbA1c target up to 64 mmol/mol (8 per cent) is acceptable to reverse HAAF.
- Review the regimen: reduce insulin doses (especially basal or nocturnal), consider switching sulfonylurea (especially glibenclamide) to a safer agent (DPP-4 inhibitor, SGLT2 inhibitor, GLP-1 RA, metformin).
- Education: the 15-15 rule, the importance of never skipping meals, pre-exercise carbohydrate, alcohol advice, sick-day rules, driving rules (do not drive for at least 45 min after recovery from a moderate episode).
- Continuous glucose monitoring (CGM) with low-glucose alarms — especially for nocturnal hypoglycaemia, hypoglycaemia unawareness, and pregnancy. Real-time CGM reduces severe hypoglycaemia by about 30 per cent in T1DM.[4]
- Glucagon rescue kit prescribed to patients at risk and their carers (intranasal or intramuscular). The newer ready-to-use nasal glucagon (3 mg) and stable liquid glucagon pens are easier for lay use than the older powder-and-diluent kits.
- Driving: in the UK, DVLA requires Group 1 drivers to have had no more than ONE severe episode in the past 12 months (no severe episode while driving in the past 12 months for Group 2 / commercial); impaired awareness of hypoglycaemia is a notifiable condition.[2]
- Screen for HAAF (Clarke or Gold questionnaires); structured hypoglycaemia avoidance programmes (e.g. Blood Glucose Awareness Training, BGAT) reduce severe events.
Specific Subtypes & Scenarios
A handful of presentations are examined so predictably that they deserve their own treatment. [1]
Insulinoma — the exam-favourite non-diabetic cause
A rare (1-3 per million per year) neuroendocrine tumour of pancreatic beta-cells; usually solitary, small (under 2 cm), benign (over 90 per cent), and occurs in the body and tail of the pancreas. Part of MEN1 in 5-10 per cent (screen prolactin, calcium, parathyroid hormone). The classic history is Whipple's triad with fasting neuroglycopenic symptoms that the patient learns to avert by frequent eating — leading to weight gain.[3][8]
- Diagnosis: biochemical first (insulin high, C-peptide high, proinsulin high, β-hydroxybutyrate low, sulfonylurea screen negative during supervised fast); then localise (CT/MRI pancreas → EUS → GLP-1 receptor PET → ASVS).
- Treatment: surgical enucleation (laparoscopic for superficial lesions) or partial pancreatectomy for deep lesions. Pre-operative diazoxide for symptom control. Everolimus or chemoembolisation for malignant/metastatic disease.
- Prognosis: surgical cure in 90-95 per cent of sporadic benign cases; long-term follow-up for MEN1. [1]
Sulfonylurea-induced hypoglycaemia — the dangerous drug
The commonest cause of severe hypoglycaemia in older T2DM. Glibenclamide (glyburide) is the most dangerous due to its long half-life and active hepatic metabolites; glipizlide, gliclazide, glimepiride are safer. Risk factors: age over 65, renal impairment, poor oral intake, alcohol, interacting drugs (fluconazole, sulfonamides, warfarin). Prolonged hypoglycaemia (24-48 h) is characteristic; treatment is octreotide + dextrose infusion, not glucagon.[2]
Alcohol-induced hypoglycaemia
Caused by inhibition of hepatic gluconeogenesis (the NADH/NAD+ shift drives pyruvate to lactate instead of to glucose); typically occurs 6-24 hours after binge drinking, often in a malnourished alcoholic or a child. Treat with thiamine before dextrose (avoid Wernicke). Lactic acidosis and alcoholic ketoacidosis may coexist. Mortality is high if untreated. [1]
Adrenal crisis presenting as hypoglycaemia
In primary adrenal insufficiency (Addison's) cortisol deficiency impairs gluconeogenesis; secondary adrenal insufficiency (pituitary failure, abrupt cessation of chronic steroids) is also a cause. Features: hypotension, hyponatraemia, hyperkalaemia (only in primary), hyperpigmentation, abdominal pain. Treat empirically with IV hydrocortisone 100 mg before confirmatory tests; do not delay for a Synacthen test in the sick patient.[11]
Non-islet cell tumour hypoglycaemia (NICTH)
Caused by tumours (typically solitary fibrous tumour of pleura, hepatocellular carcinoma, retroperitoneal sarcoma, gastrointestinal stromal tumour) that secrete incompletely processed 'big IGF-II', which binds poorly to IGF-binding proteins, leading to elevated free IGF-II and insulin-like effects. The diagnostic clue is HYPOglycaemia with LOW insulin, LOW C-peptide, LOW IGF-I but a high IGF-II/IGF-I ratio (over 10). Treatment is tumour debulking and glucocorticoids (suppress big IGF-II).[9]
Post-gastric-bypass hypoglycaemia
Occurs months to years after Roux-en-Y. Mechanism is exaggerated postprandial GLP-1 and incretin response driving endogenous hyperinsulinaemia (sometimes true beta-cell hyperplasia, historically called nesidioblastosis). Workup is a mixed-meal test. Treatment is small frequent low-glycaemic meals, acarbose, diazoxide, octreotide; rarely partial pancreatectomy. [1]
Autoimmune insulin syndrome (Hirata syndrome)
Insulin autoantibodies (often triggered by sulfhydryl drugs — methimazole, captopril — or by viral illness in HLA-DR4 individuals) bind postprandial insulin, then release it hours later, producing late postprandial hypoglycaemia. Diagnostic: high total insulin, low free insulin, positive insulin antibodies, low C-peptide at the time of release. Often self-limiting; low-carbohydrate diet, glucocorticoids, plasmapheresis for severe cases. [1]
Factitious / surreptitious hypoglycaemia
Suspect in healthcare workers, patients with diabetes in the family, or those with psychiatric history. The workup is identical to insulinoma; the discriminator is:
- Self-injected insulin → high insulin, LOW C-peptide.
- Sulfonylurea ingestion → high insulin, high C-peptide, POSITIVE sulfonylurea screen.
- A careful history, a search for injection marks, and review of the patient's access to insulin and oral hypoglycaemics are crucial. [1]
Neonatal and paediatric hypoglycaemia
- Neonate of a diabetic mother — fetal hyperinsulinaemia from maternal hyperglycaemia; transient hypoglycaemia within hours of birth.
- Premature / IUGR / SGA infants — limited glycogen and fat stores.
- Inborn errors — galactosaemia, hereditary fructose intolerance, glycogen storage disease types I and III, fatty-acid oxidation defects (MCAD), organic acidaemias.
- Idiopathic ketotic hypoglycaemia — the commonest cause after age 1 year; fasting hypoglycaemia with ketonuria; treats with avoidance of prolonged fasting and uncooked cornstarch at bedtime.
- Congenital hyperinsulinism — ABCC8/KCNJ11 mutations; severe persistent neonatal hypoglycaemia with suppressed ketones; diazoxide, glucagon infusion, near-total pancreatectomy if refractory.
- Beckwith-Wiedemann syndrome — macrosomia, macroglossia, omphalocele, hemihypertrophy, neonatal hypoglycaemia. [1]
Complications & Pitfalls
Complications
- Acute: seizures, coma, arrhythmia (QT prolongation, torsades), cardiac arrest, falls and injury (especially in the elderly), aspiration.
- Cerebral oedema — particularly in children given large glucose boluses; use 10% not 50% in children.
- Permanent neurological injury — if coma is prolonged (over 30-60 min); cortical blindness, persistent vegetative state.
- Hypoglycaemia-associated autonomic failure (HAAF) and unawareness — recurrent hypoglycaemia shifts the threshold; reversible with 2-3 weeks of strict avoidance.
- Mortality — sudden death (dead-in-bed syndrome, presumed arrhythmia); about 6-10 per cent of T1DM deaths.[4]
- Vascular events — the ADVANCE trial showed severe hypoglycaemia doubled the risk of major macrovascular events and death; the mechanism involves endothelial dysfunction, inflammation, platelet activation, and QT prolongation.[6]
- Dextrose extravasation injury — 50% dextrose causes severe tissue necrosis if extravasated; use 10-20% where possible.
- Wernicke encephalopathy — precipitated by IV dextrose in thiamine-deficient patients; always give thiamine first.
- Octreotide side-effects — abdominal cramps, steatorrhoea, gallstones, bradycardia.
- Diazoxide side-effects — fluid retention, hirsutism, hyperglycaemia, nausea, hyperuricaemia.
Classic pitfalls
- Not checking glucose in a 'drunk' or 'seizing' patient — the cardinal error; hypoglycaemia is rapidly fatal if missed.
- Treating with glucagon in sulfonylurea overdose — it stimulates insulin release and worsens rebound.
- Giving 50% dextrose — irritant, extravasation injury; 10-20% preferred.
- Forgetting thiamine in the alcoholic — precipitates Wernicke.
- Not drawing the critical sample during a non-diabetic episode — once glucose is given, insulin, C-peptide, β-hydroxybutyrate are uninterpretable.
- Stopping the fast at 48 hours and concluding 'not insulinoma' — 5-10 per cent of insulinomas need the full 72 hours; the Endocrine Society protocol is 72 h.[3]
- Misdiagnosing NICTH as insulinoma — insulin and C-peptide are LOW in NICTH; missing the tumour delays potentially life-saving resection.
- Assuming an unconscious diabetic is hyperglycaemic — they are more often hypoglycaemic; check the glucose.
- Not relaxing glucose targets after a severe episode — failure to reverse HAAF guarantees recurrence.
- Letting the patient drive home after recovery — DVLA prohibits driving for at least 45 min after a moderate episode and for some time after any severe episode.
Prognosis & Disposition
Mild hypoglycaemia in a well patient, corrected by 15 g carbohydrate, with a clear precipitant (skipped meal, exercise) and a normal regimen thereafter, may be managed at home with education and review. [1]
Severe hypoglycaemia mandates admission — for cause investigation (especially in non-diabetics), for observation after sulfonylurea or long-acting insulin overdose (24-48 h), and for regimen adjustment. The prognostic determinants are: [1]
- Underlying cause — reversible (skipped meal) versus persistent (insulinoma, NICTH).
- Duration and depth of hypoglycaemia — prolonged coma carries a risk of permanent neurological injury.
- HAAF/unawareness — predicts recurrence; relaxation of targets and CGM are mandatory.
- Comorbidity — renal, hepatic, cardiac, cognitive impairment all worsen prognosis.
- Adherence to follow-up — clinic review within 1-2 weeks; structured diabetes education; consider Diabetes Technology service. [1]
After recovery, the disposition decision:[2]
- Discharge in 4-6 hours if: episode was mild, fully reversed, the cause is clear and reversible (e.g. missed meal), the patient is neurologically intact, social situation is safe, no sulfonylurea/long-acting insulin involved.
- Admit if: severe episode, ongoing risk (sulfonylurea or long-acting insulin), recurrent, no clear cause, non-diabetic presentation, cognitive impairment, social isolation, or DVLA-relevant circumstance. [1]
Special Populations
Pregnancy
- Tighter glucose targets increase hypoglycaemia risk in T1DM and T2DM in pregnancy (especially first trimester and peripartum).
- Severe hypoglycaemia in pregnancy is common in T1DM — educate partners in IM glucagon; CGM mandatory.
- Gestational diabetes is rarely treated with insulin in doses high enough to cause severe hypoglycaemia.
- During labour, maintain glucose with a sliding-scale dextrose-insulin infusion; check glucose hourly.
- Intrapartum glucagon crosses the placenta but is preferred over prolonged hypoglycaemia. [1]
The elderly
- Atypical presentation (confusion, falls, focal signs mimicking stroke); always check glucose.
- Higher risk because of renal impairment, polypharmacy, cognitive impairment, irregular meals.
- Avoid glibenclamide in over-65s; prefer agents with low hypoglycaemia risk (metformin, DPP-4i, SGLT2i, GLP-1 RA).
- HbA1c targets relaxed (e.g. 58-64 mmol/mol / 7.5-8 per cent) in frailty. [1]
Children
- Idiopathic ketotic hypoglycaemia — commonest after age 1 year; treat with cornstarch and avoid prolonged fasting.
- Congenital hyperinsulinism — diazoxide, glucagon, surgery.
- Inborn errors — dietary management with metabolic team.
- Children with T1DM — HAAF develops rapidly; CGM and structured education of the family. [1]
Renal impairment
- Reduced clearance of insulin and sulfonylureas; gluconeogenesis impaired.
- Avoid glibenclamide (eGFR under 30); choose gliclazide, glipizide with caution; insulin doses usually reduced.
- Pre-dialysis patients are at particular risk of nocturnal hypoglycaemia. [1]
Driving
- DVLA Group 1 (car/motorcycle): no more than one severe episode in 12 months; no severe episode while driving; impaired awareness of hypoglycaemia requires notification and likely licence suspension until resolved.
- DVLA Group 2 (lorry/bus): must have no severe hypoglycaemia in the past 12 months and intact awareness; if insulin-treated, must demonstrate blood glucose monitoring at least twice daily and at relevant times.
- Patients are advised not to drive for at least 45 minutes after recovery from a moderate hypoglycaemic episode (long enough for cognitive recovery). [1]
Evidence, Guidelines & Regional Differences
Landmark trials
- ACCORD (2008-2011, NEJM) — randomised intensive glucose lowering (HbA1c target under 6 per cent / 42 mmol/mol) versus standard therapy in T2DM; the intensive arm was stopped early for excess all-cause mortality (14 deaths per 1000 patient-years higher); severe hypoglycaemia was significantly more common and a strong predictor of death.[7]
- ADVANCE (NEJM 2010) — severe hypoglycaemia in T2DM was independently associated with doubled risk of major macrovascular events and death (HR 2.9 for cardiovascular death within 5 years after a severe event); the direction of causality is debated but the association is robust.[6]
- VADT, UKPDS, DCCT — collectively show that intensive glucose lowering reduces microvascular complications but at the cost of more hypoglycaemia; macrovascular benefit is modest and offset by harm if hypoglycaemia is severe.
The "glucose paradox"
Tight glycaemic control prevents long-term complications but causes short-term hypoglycaemic harm — the glucose paradox. The lesson of ACCORD/ADVANCE is that glucose targets must be individualised, with more lenient targets (HbA1c up to 64 mmol/mol / 8 per cent) for those at risk of hypoglycaemia (elderly, comorbidities, hypoglycaemia unawareness, renal impairment).[4][7]
Guideline deltas
- Endocrine Society (2009) — the canonical evaluation-and-management guideline for adult hypoglycaemic disorders; Whipple's triad, the 72-hour supervised fast, the critical sample, the diagnostic algorithm reproduced above.[1]
- ADA / Endocrine Society Workgroup (2013) — the three-level severity classification (Level 1, 2, 3); introduced the alert value of under 3.0 mmol/L (54 mg/dL) as the threshold for clinically important hypoglycaemia to be reported in trials.[2]
- NICE NG28 (UK, 2022) — type 2 diabetes in adults; minimise hypoglycaemia by avoiding sulfonylureas in older/frail patients and prefer agents with low hypoglycaemia risk; '4 is the floor' for treating hypoglycaemia in hospitalised patients.
- JBDS-IP (UK, 2023) — hospital management of hypoglycaemia in adults with diabetes; 15-15 rule, IV 10-20% dextrose or IM glucagon, low-glucose threshold of 4.0 mmol/L in inpatients; recommends avoiding 50% dextrose where possible.
- Indian (RSSDI 2022, ICMR) — Indian guidelines mirror ADA with regional drug-availability adjustments; gliclazide preferred over glibenclamide; increasing CGM access.
Controversies
- The definition of clinical hypoglycaemia (3.0 vs 3.9 mmol/L) — the levels system reconciles the two (3.0 is the report threshold; 3.9 is the action threshold in diabetes).
- Self-monitoring vs CGM — CGM is now preferred in T1DM and insulin-treated T2DM with hypoglycaemia unawareness.
- Closed-loop insulin delivery ('artificial pancreas') — reduces both hypoglycaemia and HbA1c; the standard of care for many T1DM patients.
- Glucagon formulations — the move from powder-and-diluent to ready-to-use nasal spray and stable liquid pens increases lay-use adoption. [1]
Exam Pearls
- Whipple's triad — symptoms + documented low glucose + relief with glucose. Without all three, do not investigate for organic causes.
- Severity levels (ADA 2013): Level 1 (under 3.9), Level 2 (under 3.0), Level 3 (severe — needs another's help).[2]
- The 15-15 rule — 15 g fast carbohydrate, recheck at 15 min, repeat if under 4.
- Severe hypoglycaemia — IV 10-20% dextrose (avoid 50%) OR IM/SC glucagon 1 mg.
- Glucagon is INEFFECTIVE in sulfonylurea overdose, glycogen depletion, alcohol, anorexia, adrenal insufficiency — give dextrose, and octreotide 50-100 mcg SC q8h for sulfonylurea.
- Always give thiamine before dextrose in alcoholics or the malnourished (Wernicke prevention).
- The 5 questions to ask in any unconscious/seizing patient — glucose, oxygen, opioids, intracranial event, sepsis.
- Insulinoma — Whipple's triad + weight gain; insulin HIGH, C-peptide HIGH, proinsulin HIGH, β-hydroxybutyrate LOW, sulfonylurea screen NEGATIVE.
- Exogenous insulin abuse — insulin HIGH, C-peptide LOW, proinsulin LOW.
- Sulfonylurea ingestion (factitious) — insulin HIGH, C-peptide HIGH, sulfonylurea screen POSITIVE.
- Non-islet cell tumour hypoglycaemia (NICTH) — insulin LOW, C-peptide LOW, IGF-II/IGF-I ratio over 10; big tumour (solitary fibrous, hepatoma).
- HAAF — recurrent hypoglycaemia shifts the autonomic and glucagon thresholds to LOWER glucose; reversible with 2-3 weeks strict avoidance; relax HbA1c target.
- The "dead-in-bed" syndrome — sudden nocturnal death in young T1DM, presumed arrhythmia from silent hypoglycaemia; 2-6 per cent of T1DM deaths.[4]
- ACCORD stopped early for excess mortality in intensive glucose-lowering arm.[7]
- ADVANCE showed severe hypoglycaemia doubled the risk of macrovascular events and death.[6]
- β-hydroxybutyrate is the single best bedside discriminator of endogenous hyperinsulinaemic hypoglycaemia (it is suppressed under 2.7 mmol/L when insulin is high).
- Octreotide is the antidote to sulfonylurea-induced hypoglycaemia (suppresses insulin secretion).
- Pregnancy + T1DM — high hypoglycaemia risk in first trimester; CGM mandatory.
- DVLA — impaired awareness of hypoglycaemia is notifiable; one severe episode in 12 months (Group 1) or any severe episode (Group 2) is reportable.
- Acarbose patients — use pure glucose (dextrose), not sucrose (sucrose digestion blocked by acarbose).
EXPLAIN
the 15-15 rule, meal planning, exercise, alcohol, sick-day rules
in non-diabetic or recurrent cases — the critical sample, supervised fast
relax targets, CGM, switch agents, glucagon rescue kit
Clarke or Gold questionnaire; structured avoidance
no glucagon in sulfonylurea; thiamine before dextrose; no 50% in children
patient, GP, DVLA where relevant
structured review in 1-2 weeks; diabetes technology assessment
Exam application bank (NEET-PG / INICET)
One-line answer
Hypoglycaemia is plasma glucose low enough to cause symptoms (typically under 3.0 mmol/L / 54 mg/dL). It produces a biphasic clinical syndrome: first autonomic / sympathetic activation (sweating, tremor, palpitations, hunger, anxiety) at glucose roughly 3.3 to 3.7 mmol/L, then neuroglycopenia (confusion, drowsiness, seizures, coma, and at its extreme, death) as glucose falls below 3.0 mmol/L. In adults in the community the dominant cause is glucose-lowering therapy in diabetes (insulin, sulfonylureas, glinides); in non-diabetics, insulinoma, non-islet cell tumour hypoglycaemia (IGF-II), adrenal insufficiency, alcohol, sepsis/critical illness, and autoimmune insulin syndrome must each be excluded. The diagnostic cornerstone is Whipple's triad (symptoms + low documented glucose + relief with glucose). Treatment is layered: mild — 15 g fast-acting oral carbohydrate, recheck at 15 minutes; s [1]
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Hypoglycaemia.
References
- [1]Cryer PE, Axelrod L, Grossman AB, Heller SR, Montori VM, Seaquist ER, Service FJ. Evaluation and management of adult hypoglycemic disorders: an Endocrine Society Clinical Practice Guideline J Clin Endocrinol Metab, 2009.PMID 19088155
- [2]Seaquist ER, Anderson J, Childs B, Cryer P, Dagogo-Jack S, Fish L, Heller SR, Rodriguez H, Rosenzweig T, Vigersky R. Hypoglycemia and diabetes: a report of a workgroup of the American Diabetes Association and the Endocrine Society Diabetes Care, 2013.PMID 23589542
- [3]Service FJ. Hypoglycemic disorders N Engl J Med, 1995.PMID 7700289
- [4]Cryer PE. The barrier of hypoglycemia in diabetes Diabetes, 2008.PMID 19033403
- [5]Cryer PE. Hypoglycemia: still the limiting factor in the glycemic management of diabetes Endocr Pract, 2008.PMID 18996798
- [6]Zoungas S, Patel A, Chalmers J, de Galan BE, Li Q, Billot L, Woodward M, Ninomiya T, Neal B, MacMahon S, Grobbee DE, Kengne AP, Marre M, Heller SR, on behalf of the ADVANCE Collaborative Group. Severe hypoglycemia and risks of vascular events and death N Engl J Med, 2010.PMID 20925543
- [7]ACCORD Study Group, Gerstein HC, Miller ME, Genuth S, Ismail-Beigi F, Buse JB, Goff DC Jr, Probstfield JL, Cushman WC, Ginsberg HN, Bigger JT, Grimm RH Jr, Byington RP, Rosenberg YD, Friedewald WT. Long-term effects of intensive glucose lowering on cardiovascular outcomes N Engl J Med, 2011.PMID 21366473
- [8]Placzkowski KA, Vella A, Thompson GB, Grant CS, Reading CC, Charboneau JW, Andrews JC, Lloyd RV, Service FJ. Secular trends in the presentation and management of functioning insulinoma at the Mayo Clinic, 1987-2007 J Clin Endocrinol Metab, 2009.PMID 19141587
- [9]Ata F, Al Hommosi MM, Ahmed F, Al Mansouri A, Alkhoder L, Mahmood A, Sufyan M, Islam MA, Yasin J, Khan RR. A systematic review of literature on Insulin-like growth factor-2-mediated hypoglycaemia in non-islet cell tumours Endocrinol Diabetes Metab, 2024.PMID 38411039
- [10]Cryer PE. Hypoglycemia in diabetes Diabetes Care, 2003.PMID 12766131
- [11]Feingold KR. Hypoglycemia 2000.PMID 25905360