Gastroenterology · General Surgery
Pancreatic Cancer
Also known as Pancreatic ductal adenocarcinoma · Pancreatic adenocarcinoma · Carcinoma pancreas · Exocrine pancreatic cancer
Pancreatic ductal adenocarcinoma (PDAC) is a highly lethal malignancy of the pancreatic exocrine cells, driven by an obligate KRAS mutation in over 90 percent of tumours followed by CDKN2A, TP53 and SMAD4 loss, and by a dense desmoplastic stroma that shields it from drugs and the immune system. It is the third to fourth leading cause of cancer death in developed countries, with an overall five-year survival of about 10 to 12 percent because over 80 percent are unresectable at presentation. Risk factors are smoking (the biggest modifiable risk), chronic pancreatitis, obesity, new-onset diabetes, advancing age, and hereditary syndromes (BRCA2/PALB2, Peutz-Jeghers, Lynch, hereditary pancreatitis, FAMMM). Site defines the picture: a head tumour (60 to 70 percent) causes painless obstructive jaundice with pale stools, dark urine and pruritus, and Courvoisier sign (a palpable non-tender gallbladder), while a body or tail tumour presents late with epigastric pain radiating to the back, weight loss and new-onset diabetes. Trousseau migratory thrombophlebitis is a paraneoplastic clue. Diagnosis rests on CT pancreas protocol, endoscopic ultrasound with FNA biopsy for tissue, and CA 19-9 for monitoring. Only a minority are resectable: pancreaticoduodenectomy (Whipple) for the head, distal pancreatectomy with splenectomy for body or tail, followed by adjuvant modified FOLFIRINOX (PRODIGE 24). Borderline resectable and locally advanced disease receive neoadjuvant FOLFIRINOX or gemcitabine plus nab-paclitaxel then reassessment; metastatic disease is treated with FOLFIRINOX (fit patients) or gemcitabine plus nab-paclitaxel, with olaparib maintenance for germline BRCA-mutated tumours (POLO), plus palliative biliary and duodenal stenting, coeliac plexus neurolysis and early palliative care.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Overview & Definition
Pancreatic ductal adenocarcinoma (PDAC) is a malignant epithelial neoplasm arising from the exocrine ductal epithelium of the pancreas, defined histologically by infiltrating gland-forming cells embedded in a dense, collagen-rich desmoplastic stroma. It accounts for over 90 percent of all pancreatic malignancies and is the prototype of an almost uniformly lethal solid cancer: most patients are incurable at presentation because the tumour has already invaded locally or spread before it produces symptoms.[1][3]
The central clinical challenge is early recognition of the small, still-resectable minority. The pancreas sits retroperitoneally behind the stomach and in front of the great vessels, so tumours grow silently for months. A head tumour is luckier for the patient in one sense: by compressing the distal common bile duct it produces painless obstructive jaundice early enough that the disease may still be local. A body or tail tumour grows without obstructing any duct, so it presents late with pain and weight loss and is almost never resectable. This anatomical asymmetry — not any special biological aggressiveness — is why the overall outcome is so poor.[1]
Although PDAC dominates, several other exocrine and endocrine pancreatic neoplasms exist (see Specific Subtypes) and behave very differently, with much better prognosis — a distinction examiners reward.[2]
Classification
Pancreatic cancer is classified by histology and by anatomical site. Both matter for prognosis. [1]
Histological classification
| Type | Frequency | Behaviour |
|---|---|---|
| Ductal adenocarcinoma (PDAC) | Over 90 percent | Highly lethal; the topic of this chapter |
| Acinar cell carcinoma | 1 to 2 percent | Older men; large tumour; may secrete lipase causing subcutaneous fat necrosis and polyarthritis |
| Pancreatic neuroendocrine tumour (pNET) | 2 to 5 percent | Often functional (insulinoma, gastrinoma, glucagonoma, VIPoma, somatostatinoma); slower-growing; better prognosis |
| Intraductal papillary mucinous neoplasm (IPMN) | Precursor | Main-duct IPMN carries a 40 to 70 percent malignancy risk; branch-duct much lower |
| Mucinous cystic neoplasm (MCN) | Premalignant | Women in 40s; ovarian-type stroma; resect if symptomatic or over 3 cm |
| Solid pseudopapillary neoplasm | Rare | Young women; low-grade malignant; resectable |
| Ampullary carcinoma | Periampullary | Arises at ampulla of Vater; presents early with jaundice; much better prognosis than PDAC |
Anatomical classification (the clinical one)
| Site | Proportion | Why it matters |
|---|---|---|
| Head (including uncinate) | 60 to 70 percent | Compresses distal CBD and ampulla, causing painless obstructive jaundice while still resectable |
| Body | 15 to 20 percent | Silent; presents with back pain and weight loss; usually advanced |
| Tail | 5 to 10 percent | Most silent; often found at metastatic stage |
| Diffuse | 5 to 10 percent | Whole-gland infiltration; worst prognosis |
Ductal adenocarcinoma
- Over 90 percent of pancreatic cancer
- Derived from ductal epithelium; PanIN precursor
- KRAS in over 90 percent; dense desmoplasia
- Five-year survival about 10 to 12 percent
Pancreatic neuroendocrine
- Two to five percent; islet-cell origin
- Often functional (insulinoma, gastrinoma)
- Slower; can metastasise but resectable
- Five-year survival 50 to 80 percent
Ampullary carcinoma
- Periampullary, at ampulla of Vater
- Obstructs bile duct EARLY (jaundice)
- Resectable in most; much better prognosis
- Five-year survival 40 to 50 percent after Whipple
Main-duct IPMN
- Cystic precursor; dilated main duct
- Malignancy risk 40 to 70 percent
- Resect regardless of symptoms
- Branch-duct IPMN has far lower risk
Epidemiology & Risk Factors
Pancreatic cancer is the fourteenth most commonly diagnosed cancer worldwide but the seventh leading cause of cancer death, an unusually lethal ratio (incidence roughly equals mortality). It is projected to become the second leading cause of cancer death in the United States by around 2030, overtaking breast, prostate and colorectal cancer as those improve.[2][4]
Pancreatic cancer - the numbers
Non-hereditary risk factors
- Tobacco smoking - the single biggest modifiable risk, conferring a two-fold increased risk and accounting for 20 to 25 percent of cases. Risk falls toward baseline after ten years of abstinence.
- Chronic pancreatitis of any cause confers a five- to fifteen-fold increased risk; the risk is highest with hereditary and tropical calcific pancreatitis and accumulates over decades.
- Obesity and physical inactivity - a body mass index over 30 raises risk by about 20 percent; central adiposity and adult-onset weight gain matter most.
- Diabetes mellitus - a complex bidirectional relationship. Long-standing type 2 diabetes modestly raises risk, but the examinable point is the opposite: new-onset diabetes after age 50, especially with weight loss, is a paraneoplastic marker of pancreatic cancer in up to 1 percent of cases, sometimes preceding the diagnosis by months.
- Heavy alcohol intake - acts largely through chronic pancreatitis; an independent effect is debated.
- Non-O ABO blood group (A, B, AB) and Helicobacter pylori carriage carry small excess risks.
- Advancing age - rare under 40; median age at diagnosis around 70.[1][4]
Hereditary and familial risk (about 10 percent of cases)
About one in ten pancreatic cancers cluster in families, and the hereditary syndromes carry defined surveillance obligations.[14]
| Syndrome | Gene | Lifetime PDAC risk | Surveillance |
|---|---|---|---|
| Hereditary pancreatitis | PRSS1 (AD) | Up to 40 percent by age 70 | From age 40, or 20 years after onset |
| Peutz-Jeghers | STK11 (LKB1) | 11 to 36 percent | From age 30-35 |
| Lynch syndrome | MLH1, MSH2, MSH6, PMS2 | 4 to 9 percent (about 9-fold) | From age 40-50 |
| Familial atypical multiple mole melanoma (FAMMM) | CDKN2A (p16) | 10 to 17 percent | From age 40 |
| Hereditary breast and ovarian cancer | BRCA1, BRCA2, PALB2 | 5 to 10 percent (BRCA2 highest) | From age 45-50, or 10 years before youngest affected relative |
| Ataxia-telangiectasia (carriers) | ATM | Modest excess | Individualised |
Familial pancreatic cancer is defined by two or more first-degree relatives with PDAC and no identifiable syndrome, conferring a two- to six-fold risk that scales with the number of affected relatives. All high-risk kindreds should be referred for surveillance with magnetic resonance cholangiopancreatography and endoscopic ultrasound, starting at the ages above and continued indefinitely, because detecting small T1N0 resectable tumours is the only realistic cure strategy in this population.[13][14]
Pathophysiology
PDAC develops through a defined histological precursor-to-carcinoma sequence (PanIN) overlaid on a genetic mutation cascade and shaped by a hostile tumour microenvironment. Understanding the cascade is high-yield for viva and MCQ. [1]
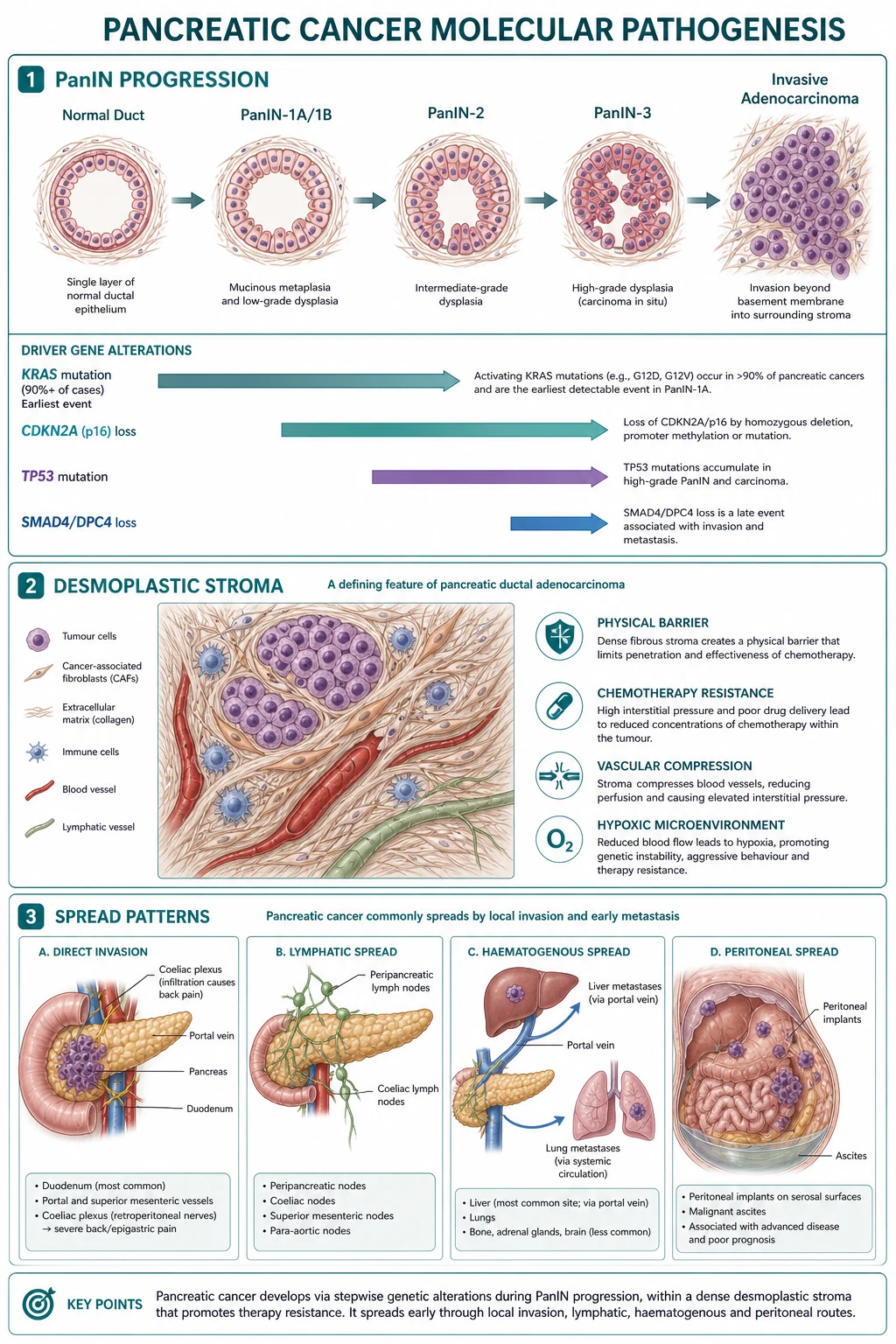
The precursor: pancreatic intraepithelial neoplasia (PanIN)
PDAC arises from microscopic pancreatic intraepithelial neoplasia (PanIN) lesions in the small intralobular ducts, progressing through histological grades: [1]
- PanIN-1A / 1B - flat or papillary mucinous epithelium, no atypia; common with age.
- PanIN-2 - mild architectural and cytological atypia.
- PanIN-3 (carcinoma in situ) - marked atypia, cribriforming, loss of polarity; the immediate precursor of invasive carcinoma. [1]
This progression parallels a stepwise accumulation of driver mutations, mirroring the adenoma-carcinoma sequence in colon cancer.[1][3]
The genetic mutation cascade (the four canonical drivers)
Whole-genome sequencing has refined the classical model. Four genes dominate, and the order and pattern of their loss is examinable.[5]
- KRAS (over 90 percent of PDAC) - the earliest and most frequent driver, found even in low-grade PanIN. The most common activating mutation is KRAS G12D. Mutant KRAS locks RAS-RAF-MEK-ERK signalling in the active, GTP-bound state, driving uncontrolled proliferation, survival and metabolic reprogramming. PDAC has the highest KRAS frequency of any solid tumour.
- CDKN2A (p16) (~90 percent of PDAC) - the second hit; loss disables the p16-CDK4-RB cell-cycle checkpoint, allowing uncontrolled G1-S transition. Inactivated in familial melanoma-pancreatic cancer (FAMMM).
- TP53 (50 to 75 percent) - a later event; loss disables DNA-damage-induced apoptosis and cell-cycle arrest.
- SMAD4 (DPC4) (~55 percent) - a later event, lost by deletion in chromosome 18q; loss of SMAD4 function (downstream of TGF-beta signalling) is strongly associated with widely metastatic disease and a worse prognosis. [1]
The remaining 5 to 10 percent are KRAS-wild-type tumours, more likely to harbour actionable alterations such as BRCA1/2, PALB2, ATM, mismatch-repair deficiency (Lynch), NRG1, ALK, ROS1 or NTRK fusions - all worth testing because they open targeted or immunotherapy doors.[5]
The tumour microenvironment - the desmoplastic stroma
A striking and clinically dominant feature of PDAC is its dense desmoplastic (fibrotic) stroma, which can make up most of the tumour volume. The stroma is produced by activated pancreatic stellate cells (quiescent vitamin-A-storing cells, akin to hepatic stellate cells) that, on activation by TGF-beta, PDGF, IL-6 and sonic hedgehog, transdifferentiate into collagen-secreting myofibroblasts. The stroma has several consequences: [1]
- It creates a high interstitial fluid pressure that collapses tumour vasculature and limits drug delivery, contributing to chemoresistance.
- It is hypoxic and avascular, which is exactly why PDAC appears as a hypoenhancing mass relative to the bright normal pancreas on the arterial phase of CT.
- It sequesters immune cells into an immunosuppressive (T-reg-rich, myeloid-derived-suppressor-cell-rich) phenotype, explaining why PDAC is refractory to checkpoint immunotherapy.[1][2]
Molecular subtypes (transcriptional)
Two dominant transcriptional subtypes - classical (epithelial) and basal-like (squamous or quasimesenchymal) - have reproducible prognostic and predictive value. Basal-like tumours carry a markedly worse prognosis and may respond preferentially to FOLFIRINOX, while classical tumours are chemotherapy-sensitive with a better outcome. Although not yet routine in clinic, this classification underpins current biomarker research.[2]
Anatomical basis of presentation
The pancreas is retroperitoneal, lying transversely across L1-L2 behind the stomach and in front of the superior mesenteric artery (SMA), superior mesenteric vein (SMV) and portal vein (PV), and the coeliac axis. The head sits within the C-loop of the duodenum, embracing the distal common bile duct as it joins the ampulla of Vater. This anatomy explains everything: [1]
- A head tumour compresses the distal CBD early, producing obstructive jaundice at a smaller size and so at an earlier stage.
- A body or tail tumour has no duct to obstruct; it grows until it invades the coeliac plexus (back pain) or metastasises (liver, peritoneum).
- Local invasion of the SMA, coeliac axis or SMV-PV confluence is what makes a tumour unresectable (locally advanced), even without distant spread.[1]
The dominant routes of spread are: (1) local into retroperitoneum, duodenum, stomach and peripancreatic fat with encasement of vessels; (2) lymphatic to pancreaticoduodenal, coeliac, superior mesenteric and porta hepatis nodes; (3) peritoneal causing malignant ascites; (4) haematogenous to liver (first and commonest) and lung.[1]
Clinical Presentation
PDAC is famous for presenting late and subtly. The dominant clues are site-dependent, and a handful of paraneoplastic phenomena are classic exam stems. [1]
Head tumour - the painless jaundice presentation
- Painless obstructive jaundice - the single most common presentation, in over 60 percent of patients. The skin and sclera become yellow, with dark urine, pale (clay-coloured) stools and pruritus.
- Courvoisier sign - a palpable, non-tender, distended gallbladder felt in the right upper quadrant in a jaundiced patient. Courvoisier's law states: in the presence of jaundice and a palpable gallbladder, the cause is unlikely to be gallstones. Gallstones cause repeated bouts of chronic cholecystitis that scar and contract the gallbladder; a distended, thin-walled gallbladder implies a progressive malignant obstruction (pancreatic head, cholangiocarcinoma, ampullary carcinoma) that has built up gradually without inflammation.
- Weight loss, anorexia and fatigue - usually marked, often preceding the jaundice. [1]
Body or tail tumour - the silent, late presentation
- Dull epigastric pain radiating through to the back, often worse at night and relieved by leaning forward - pain is from coeliac plexus and retroperitoneal invasion.
- Marked weight loss and cachexia.
- New-onset diabetes - sometimes the only clue, weeks to months before the cancer is found.
- Often no jaundice (no bile-duct obstruction), so diagnosis is delayed until the tumour is locally advanced or metastatic.[1][3]
Less common and atypical presentations
- Acute pancreatitis - a tumour obstructing the pancreatic duct can trigger an attack; any older patient with unexplained pancreatitis should be investigated for an underlying mass.
- Upper gastrointestinal bleeding - from duodenal invasion or variceal bleeding due to splenic vein thrombosis (a body or tail tumour compressing the splenic vein, causing left-sided, sinistral portal hypertension with isolated gastric fundal varices - a splenectomy is curative).
- Migratory thrombophlebitis (Trousseau syndrome) - recurrent, migrating, sterile venous thromboses in unusual sites (subclavian, portal, jugular, superficial) driven by tumour mucins and tissue factor; a paraneoplastic hallmark of PDAC and a poor prognostic sign.
- Malignant ascites or palpable Virchow's node (Troisier's sign) - peritoneal or nodal metastasis.
- Depression of recent onset, occasionally the first symptom (a debated association).
- Asymptomatic incidental finding on imaging done for another reason. [1]
Differential Diagnosis
Painless obstructive jaundice and an epigastric mass or pancreatic lesion have a focused differential. The key is to separate malignant distal obstruction (PDAC and its mimics) from benign causes, because each changes management entirely.[1]
Choledocholithiasis
- Usually PAINFUL colic with fever (cholangitis)
- Prior biliary colic, gallstones on ultrasound
- Dilated CBD with an echogenic stone
- Contracted, thick-walled gallbladder (NOT Courvoisier)
Cholangiocarcinoma
- Arises in bile duct, often at hilum (Klatskin)
- Mass centred on the duct, not the pancreas
- Progressive painless jaundice (mimics PDAC)
- Distinguished by MRCP and EUS-FNA cytology
Chronic pancreatitis
- Longstanding alcohol, recurrent pain
- Calcification, ductal changes on imaging
- Mass-forming focal pancreatitis mimics cancer
- CA 19-9 may be elevated; biopsy often needed
Autoimmune pancreatitis (IgG4)
- Painless jaundice in an older man (mimics PDAC)
- 'Sausage-shaped' full pancreas, capsule-like rim
- Raised serum IgG4; other organ involvement
- DRAMATIC steroid response (prednisolone 40 mg)
Ampullary carcinoma
- Obstructs bile duct EARLY at ampulla
- Painless jaundice, but intermittent and fluctuating
- Visible at endoscopy as a periampullary mass
- Far better prognosis than PDAC after Whipple
Pancreatic neuroendocrine tumour
- Often functional syndrome (hypoglycaemia, ZES)
- Hypervascular on CT (PDAC is hypovascular)
- Slower growth; often resectable at diagnosis
- Different biology, different chemotherapy
The two must-not-miss mimics are autoimmune pancreatitis (steroid-responsive and curable - never operate without a tissue diagnosis and IgG4 if the picture is atypical) and ampullary or cholangiocarcinoma (better prognosis, often confused with PDAC on imaging).[1]
Clinical & Bedside Assessment
The focused bedside assessment has four aims: (1) confirm obstructive jaundice, (2) assess Courvoisier sign and cachexia, (3) look for metastases and complications, and (4) assess fitness for major surgery. [1]
- General - cachexia, temporal wasting, muscle wasting (sarcopenia), conjunctival pallor (anaemia of chronic disease).
- Hands - finger clubbing is occasionally seen; look for clues to hereditary syndromes (mucocutaneous pigmentation of Peutz-Jeghers, multiple atypical naevi of FAMMM).
- Skin - jaundice, excoriations from pruritus, migratory thrombophlebitis (Trousseau), subcutaneous fat necrosis (acinar cell carcinoma).
- Abdomen - palpable gallbladder (Courvoisier sign) in the right upper quadrant; hepatomegaly from metastases or biliary congestion; epigastric mass (late); ascites (peritoneal); left supraclavicular lymphadenopathy (Virchow's node, Troisier's sign); periumbilical nodule (Sister Mary Joseph) - all indicate advanced disease.
- Examination for thrombosis - tender cord-like superficial veins in unusual sites.
- Cardiopulmonary and functional assessment for major surgery - exercise tolerance, frailty scores (Clinical Frailty Scale), nutritional status (must be optimised pre-operatively). [1]
Investigations
Investigation proceeds in a staged, goal-directed fashion: first confirm the mass and stage (CT pancreas protocol), then obtain tissue (endoscopic ultrasound with FNA), then complete staging (staging laparoscopy if proceeding to resection), and use tumour markers for adjunct and monitoring.[1][3]
Blood tests
- Liver function tests - the obstructive pattern of raised bilirubin, alkaline phosphatase and gamma-GT with relatively preserved transaminases (or a mixed picture); hypoalbuminaemia and anaemia of chronic disease in advanced disease.
- Coagulation - raised INR from vitamin-K malabsorption due to biliary obstruction (correct with intravenous or oral vitamin K 10 mg daily for three days); always check before any invasive procedure.
- CA 19-9 (carbohydrate antigen 19-9) - the principal tumour marker. Cut-off 37 U per mL; sensitivity about 80 percent and specificity about 80 percent for PDAC in jaundiced patients. Key caveats: (1) it is falsely elevated in any cholestasis (benign or malignant), (2) it is undetectable in the 5 to 10 percent of patients who are Lewis-antigen-negative (so a normal CA 19-9 does not exclude cancer), (3) it is not a screening test but is invaluable for diagnosis adjunct, baseline, monitoring response and detecting recurrence.[12]
- CEA - less sensitive, occasionally adjunctive.
- Glucose and HbA1c - new-onset diabetes.
- Renal function and full blood count - baseline before chemotherapy.
Imaging - the cornerstone
- Multiphase CT pancreas protocol (triphasic) - the single most important test. Performed as non-contrast, late arterial (pancreatic) phase (around 35 to 45 seconds) and portal venous phase, with thin slices. PDAC appears as a focal hypoenhancing mass against a brightly enhancing normal pancreas. Look for: dilation of both the pancreatic duct and the common bile duct (the double-duct sign) when a head tumour obstructs both; vascular involvement (abutment, encasement or occlusion of the SMA, coeliac axis, hepatic artery and SMV-PV confluence, measured in degrees of circumference); distant metastases (hypovascular liver lesions, peritoneal deposits); and regional adenopathy. CT has a sensitivity of about 90 percent for lesions over 2 cm and accurately predicts resectability in most cases.[3]
- Magnetic resonance cholangiopancreatography (MRCP) - best non-invasive ductal anatomy map; preferred when CT is indeterminate, in iodine-allergic patients, and to characterise small or isoattenuating tumours and cystic lesions.
- Endoscopic ultrasound (EUS) with fine-needle aspiration (FNA) or fine-needle biopsy (FNB) - the definitive tissue-sampling test, especially for small tumours missed on CT, for nodal staging, and for sampling cystic lesions. Sensitivity for tissue diagnosis over 90 percent.
- Endoscopic retrograde cholangiopancreatography (ERCP) - now mainly therapeutic (biliary stent placement, brush cytology), not diagnostic; reserved for obstructive jaundice requiring drainage or cholangitis.
- 18F-FDG PET-CT - useful for detecting occult metastases before planned resection and for restaging after neoadjuvant therapy, particularly in high CA 19-9 with normal CT.
- Staging laparoscopy - performed immediately before laparotomy to detect occult peritoneal or small superficial liver metastases not seen on CT; upstages about 10 to 15 percent of patients planned for resection, sparing them an unnecessary laparotomy.[1]
Histology and staging tissue
Tissue diagnosis is mandatory before neoadjuvant therapy or palliative chemotherapy, but not always required before upfront resection when imaging is characteristic (resection itself provides the diagnosis). EUS-FNA yields gland-forming adenocarcinoma cells in a desmoplastic stroma. For first-line metastatic disease, molecular profiling for KRAS, BRCA1/2, PALB2, ATM and mismatch-repair is now standard.[5]
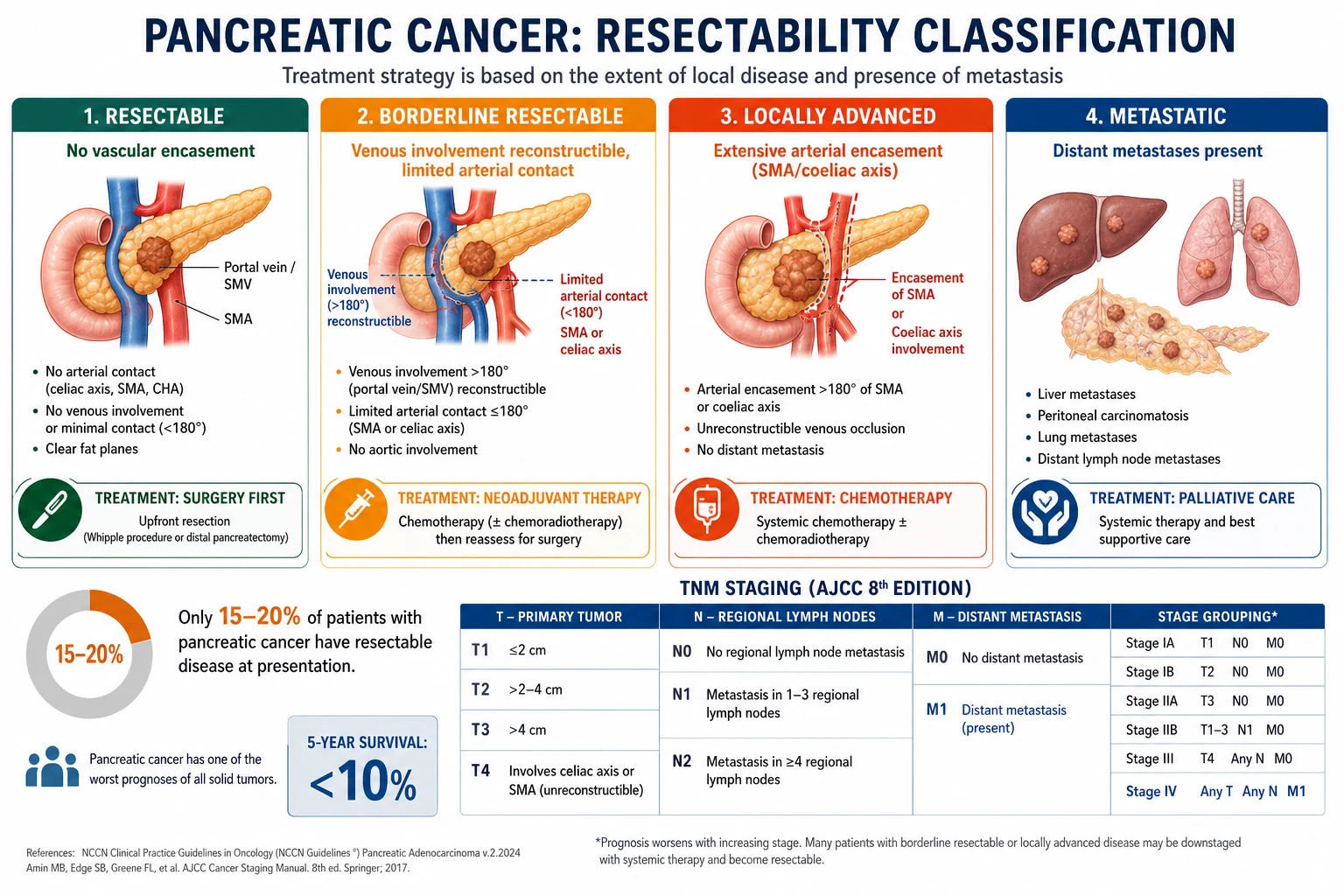
AJCC TNM staging (8th edition - reproduced)
| Stage | T (tumour) | N (nodes) | M (metastasis) | Meaning |
|---|---|---|---|---|
| 0 | Tis (carcinoma in situ) | N0 | M0 | PanIN-3, pre-invasive |
| IA | T1 (under or equal to 2 cm, confined) | N0 | M0 | Small, localised |
| IB | T2 (over 2 to 4 cm) | N0 | M0 | Larger, still localised |
| IIA | T3 (over 4 cm) | N0 | M0 | Large but resectable |
| IIB | T1-3 | N1 (1 to 3 regional nodes) | M0 | Limited nodal disease |
| III | Any T | N2 (4 or more nodes) OR T4 | M0 | T4 = involves coeliac, SMA or common hepatic artery = unresectable |
| IV | Any T | Any N | M1 | Distant metastasis (liver, peritoneum, lung) |
T4 (involvement of the coeliac axis, superior mesenteric artery or common hepatic artery) defines locally advanced, unresectable disease. M1 defines metastatic disease. Both are surgically incurable.[1]
Resectability criteria (NCCN)
| Category | Arterial | Venous | Strategy |
|---|---|---|---|
| Resectable | No contact with coeliac, SMA or common hepatic artery | No SMV-PV contact or under 180 degrees | Upfront surgery then adjuvant |
| Borderline resectable | Solid tumour contact under or equal to 180 degrees with SMA or coeliac, or reconstructable common hepatic artery involvement | Over 180 degrees SMV-PV contact or thrombosis but reconstructable | Neoadjuvant then reassess |
| Locally advanced (unresectable) | Over 180 degrees SMA or coeliac encasement; unreconstructable aortic involvement | Unreconstructable SMV-PV occlusion | Systemic chemotherapy, selected chemoradiotherapy, never curative surgery |
| Metastatic | Any | Any | M1 disease - palliative systemic therapy |
Resectability spectrum at presentation
T4 - encases SMA or coeliac
About 30 percent. Incurable by surgery; FOLFIRINOX plus or minus chemoradiotherapy; palliative biliary drainage.
Management - Resuscitation
PDAC rarely presents as an acute emergency, but several acute, time-critical presentations demand immediate action while staging proceeds.[1][3]
Acute presentations requiring resuscitation
Acute cholangitis (fever, jaundice, pain - Charcot triad; with shock - Reynolds pentad)
Resuscitate with IV fluids and start broad-spectrum antibiotics (e.g. piperacillin-tazobactam 4.5 g IV every eight hours, or ceftriaxone 2 g IV daily plus metronidazole 500 mg IV every eight hours). The DEFINITIVE treatment is urgent biliary decompression by ERCP with sphincterotomy and biliary stent (plastic or self-expandable metal stent). Percutaneous transhepatic biliary drainage (PTBD) if ERCP fails.
Severe coagulopathy of obstructive jaundice
Raised INR from vitamin K malabsorption. Give vitamin K 10 mg IV slowly (or orally) daily for three days; correct to INR under 1.5 before any invasive procedure or surgery. Fresh-frozen plasma only if actively bleeding or urgent procedure needed.
Gastric outlet obstruction (intractable vomiting)
Pass a nasogastric tube for decompression, correct dehydration and electrolytes, then arrange a palliative duodenal self-expandable metal stent (first-line, less invasive) or a palliative gastrojejunostomy (surgical double-bypass) at laparoscopy or laparotomy.
Symptomatic VTE or Trousseau thrombophlebitis
PDAC carries one of the highest thrombotic risks of any cancer. Therapeutic anticoagulation with low-molecular-weight heparin (e.g. enoxaparin 1.5 mg per kg subcutaneously once daily, or 1 mg per kg twice daily). All hospitalised PDAC patients should receive pharmacological VTE prophylaxis (enoxaparin 40 mg SC daily) unless contraindicated.
Severe pain emergency
Begin the WHO analgesic ladder (paracetamol, then weak then strong opioids - oral morphine 5 to 10 mg every four hours, titrated). For intractable retroperitoneal pain arrange an early coeliac plexus block or neurolysis (EUS-guided injection of bupivacaine and absolute alcohol or steroid).
Management - Definitive & Stepwise
Definitive management is decided entirely by resectability stage and is delivered by a specialised hepatopancreatobiliary multidisciplinary team. The overriding principle: the only chance of cure is a complete (R0) surgical resection combined with modern adjuvant chemotherapy; everything else is palliative.[1][3]
Stage 1 - Resectable disease (15 to 20 percent): surgery first
Surgical resection is the only potentially curative treatment. The operation depends on the site. [1]
Pancreaticoduodenectomy (Whipple procedure) is used for tumours of the pancreatic head, uncinate process, duodenum, distal bile duct and ampulla. It is one of the largest abdominal operations and the most examined procedure in GI oncology.[1]
- Resection (what is removed en bloc): the head of the pancreas (to the right of the portal vein), the duodenum (second, third and proximal fourth parts), the distal common bile duct and gallbladder, and either the distal stomach (classical Whipple) or pylorus preserved (pylorus-preserving pancreaticoduodenectomy, preferred where possible to preserve gastric function). Regional lymphadenectomy (pancreaticoduodenal, coeliac, SMA, porta hepatis nodes) is performed.
- Reconstruction (the three anastomoses - the exam answer):
- Pancreaticojejunostomy - the remnant pancreatic duct to a limb of jejunum (the anastomosis most prone to leak - the pancreatic fistula).
- Hepaticojejunostomy - the proximal bile duct to the same jejunal limb.
- Gastrojejunostomy (or duodenojejunostomy if pylorus-preserving) - to restore intestinal continuity.
- Outcomes: operative mortality is now under 5 percent in high-volume centres but morbidity remains 30 to 40 percent. [1]
Distal pancreatectomy with splenectomy is used for body and tail tumours. The spleen is removed with the tumour en bloc because the splenic artery and vein run along the upper border of the body and tail and are sacrificed; draining lymph nodes are taken. A spleen-preserving distal pancreatectomy is reserved for benign or low-grade lesions, not for PDAC. [1]
Total pancreatectomy is rarely used (multifocal disease, positive margin after Whipple, or hereditary IPMN) because it produces brittle diabetes and exocrine insufficiency. [1]
Adjuvant chemotherapy after R0 or R1 resection improves survival and is now standard:[8][9]
- Modified FOLFIRINOX (mFOLFIRINOX) - the preferred regimen for fit patients (ECOG 0-1) since the PRODIGE 24 / ACCORD 24 trial (Conroy 2018, NEJM). Regimen: oxaliplatin 85 mg per square metre, leucovorin 400 mg per square metre, irinotecan 150 mg per square metre (reduced from the metastatic 180 mg dose), all on day 1, then 5-fluorouracil 2400 mg per square metre as a 46-hour continuous infusion, repeated every two weeks for 12 cycles. Result: median overall survival 54.4 months versus 35.0 months for gemcitabine - the largest survival gain ever seen in the adjuvant setting.[8]
- Gemcitabine plus capecitabine - the ESPAC-4 trial (Neoptolemos 2017, Lancet) alternative. Regimen: gemcitabine 1000 mg per square metre on days 1, 8 and 15, plus capecitabine 830 mg per square metre orally twice daily on days 1 to 21, every four weeks for six cycles. Result: median OS 28.0 months versus 25.5 months for gemcitabine alone.[9]
- Gemcitabine monotherapy (1000 mg per square metre weekly for three of four weeks, six cycles) - older standard, now used only for less fit patients.
PRODIGE 24 / ACCORD 24 - adjuvant mFOLFIRINOX
Conroy T et al. N Engl J Med 2018
Phase III RCT, 493 patients with resected PDAC, ECOG 0-1: mFOLFIRINOX for 12 cycles vs gemcitabine for 6 cycles
Key finding
Median overall survival 54.4 months (mFOLFIRINOX) vs 35.0 months (gemcitabine); 3-year disease-free survival 57% vs 35%
Practice change
mFOLFIRINOX is the preferred adjuvant regimen for fit patients after R0 or R1 resection
Stage 2 - Borderline resectable disease (about 15 percent): neoadjuvant first
Borderline resectable tumours (venous reconstruction needed, or limited arterial contact) are best managed with neoadjuvant chemotherapy for two to four months - usually FOLFIRINOX (preferred if fit) or gemcitabine plus nab-paclitaxel - followed by restaging CT and resection if there is no progression. The rationale is threefold: (1) treat occult micrometastases early, (2) downsize the tumour to achieve an R0 margin, (3) spare non-responders a futile major operation. The PREOPANC Dutch trial and the Murphy total-neoadjuvant FOLFIRINOX-plus-losartan regimen (losartan to disrupt the stroma and improve drug delivery) are key evidence.[11]
Murphy total neoadjuvant FOLFIRINOX + losartan
Murphy JE et al. JAMA Oncol 2019
Single-arm phase II, 102 patients with locally advanced PDAC: FOLFIRINOX + losartan (an angiotensin-receptor blocker that softens the desmoplastic stroma) then chemoradiotherapy
Key finding
Resection rate 61% (previously thought unresectable); median overall survival 21.1 months; 2-year survival 48%
Practice change
Total neoadjuvant therapy including losartan to disrupt the stroma converted many locally advanced tumours to resectable
Stage 3 - Locally advanced disease (about 30 percent): systemic, never curative
These T4 tumours encase the SMA, coeliac axis or common hepatic artery and are not surgically curable. Treatment is systemic chemotherapy with FOLFIRINOX (fit patients) or gemcitabine plus nab-paclitaxel (less fit). Selected patients with stable or responding disease receive consolidative chemoradiotherapy. Biliary obstruction is managed with endoscopic or percutaneous biliary stenting (a self-expandable metal stent if life expectancy exceeds three to six months).[1]
Stage 4 - Metastatic disease (about 40 percent): palliative systemic therapy
Fit patients (ECOG 0-1) receive one of two first-line regimens, chosen on fitness and toxicity profile:[6][7]
- FOLFIRINOX - Conroy 2011, PRODIGE 4 / ACCORD 11 (NEJM). Regimen: oxaliplatin 85 mg per square metre, leucovorin 400 mg per square metre, irinotecan 180 mg per square metre, all day 1, then 5-fluorouracil 400 mg per square metre bolus then 2400 mg per square metre over 46 hours, every two weeks. Result: median OS 11.1 months versus 6.8 months for gemcitabine - the largest survival gain in metastatic PDAC. Toxicity is significant (neutropenia, diarrhoea, neuropathy, alopecia) - reserve for fit patients.[6]
- Gemcitabine plus nab-paclitaxel - Von Hoff 2013, MPACT (NEJM). Regimen: nab-paclitaxel 125 mg per square metre followed by gemcitabine 1000 mg per square metre on days 1, 8 and 15, every four weeks. Result: median OS 8.5 months versus 6.7 months for gemcitabine alone. Better tolerated than FOLFIRINOX; preferred for older or less fit patients.[7]
Less fit patients (ECOG 2) receive single-agent gemcitabine 1000 mg per square metre weekly for three of four weeks. Nanoparticle albumin-bound (nab) paclitaxel is the alternative. [1]
Targeted and biomarker-driven therapy: [1]
- Maintenance olaparib for germline BRCA1 or BRCA2-mutated metastatic PDAC - Golan 2019, POLO (NEJM). Olaparib 300 mg orally twice daily as maintenance after at least 16 weeks of disease control on platinum-based chemotherapy (e.g. FOLFIRINOX) more than doubled progression-free survival (7.4 versus 3.8 months). All metastatic PDAC patients should be germline BRCA-tested.[10]
- Mismatch-repair-deficient (dMMR) / microsatellite-instability-high (MSI-H) tumours - rare in PDAC (under 1 percent) - may respond to pembrolizumab (immune checkpoint inhibitor).
- NRG1, ALK, NTRK fusions (KRAS-wild-type tumours) - targeted by erlotinib, larotrectinib or entrectinib in selected cases.[5]
POLO - maintenance olaparib for germline BRCA PDAC
Golan T et al. N Engl J Med 2019
Phase III RCT, 154 patients with germline BRCA-mutated metastatic PDAC whose disease had not progressed on >=16 weeks of platinum chemotherapy: olaparib 300 mg BD maintenance vs placebo
Key finding
Median progression-free survival 7.4 months (olaparib) vs 3.8 months (placebo); first biomarker-driven therapy in PDAC
Practice change
Germline BRCA testing recommended for all metastatic PDAC; olaparib maintenance for BRCA carriers after platinum response
Palliative and supportive care (essential, early)
For the 80 percent who are unresectable, early specialist palliative care improves quality of life and survival. Key interventions:[1]
- Biliary decompression - ERCP with self-expandable metal stent (preferred for malignant obstruction) or plastic stent; PTBD if endoscopic access fails.
- Duodenal obstruction - endoscopic duodenal self-expandable metal stent, or surgical gastrojejunostomy as part of a palliative double-bypass (hepaticojejunostomy plus gastrojejunostomy, with biliary-enteric bypass) at laparoscopy when stenting fails.
- Pain - WHO ladder up to strong opioids; EUS-guided or CT-guided coeliac plexus neurolysis (injection of absolute alcohol to destroy the coeliac plexus) for intractable retroperitoneal pain.
- Nutrition - pancreatic enzyme replacement (PERT: pancreatin 25,000 to 40,000 units lipase with each meal, with a PPI), oral nutritional supplements, nasojejunal or PEG feeding in selected patients.
- VTE prophylaxis - high thrombotic risk; ambulatory metastatic PDAC patients on chemotherapy should be considered for primary prophylactic low-molecular-weight heparin (e.g. enoxaparin 40 mg SC daily) per guidelines, balancing bleed risk.
- Psychosocial support, advance care planning and end-of-life care - delivered in parallel, not deferred to the terminal phase. [1]
Specific Subtypes & Scenarios
- Ampullary carcinoma arises at the ampulla of Vater, obstructs the bile duct EARLY and presents with painless jaundice (often fluctuating, with anaemia from occult GI blood loss). It is resected by Whipple and carries a five-year survival of 40 to 50 percent - far better than PDAC - because it is found early.[2]
- Main-duct IPMN - a cystic precursor with a 40 to 70 percent malignancy risk; resect regardless of symptoms. Branch-duct IPMN is far lower risk and observed unless over 3 cm, with mural nodules, or symptomatic.[2]
- Mucinous cystic neoplasm (MCN) - a premalignant cystic tumour of women in their 40s, with characteristic ovarian-type stroma; resect if symptomatic or over 3 cm.
- Pancreatic neuroendocrine tumour (pNET) - separate biology, often functional (insulinoma = Whipple triad of fasting hypoglycaemia, low plasma glucose, symptom relief with glucose; gastrinoma = Zollinger-Ellison). Hypervascular on CT, slower-growing, often resectable; five-year survival 50 to 80 percent.
- Acinar cell carcinoma - older men, large tumour; may secrete lipase causing subcutaneous fat necrosis, polyarthritis and eosinophilia.
- Cystic lesions found incidentally - differentiate mucinous (IPMN, MCN - potentially malignant) from serous cystadenoma (benign, 'honeycomb' or 'sunburst' calcification) and pseudocyst (post-pancreatitis, high amylase fluid). EUS morphology and fluid CEA, amylase and cytology guide management.
- Hereditary / germline BRCA PDAC - test all metastatic patients; offer germline testing to resected patients with a family history; olaparib for BRCA carriers (POLO).[10][14]
Complications & Pitfalls
Disease-related complications
- Obstructive jaundice - pruritus, malabsorption of fat-soluble vitamins, coagulopathy; relieved by stenting.
- Cholangitis - bacterial infection of obstructed bile; emergency ERCP and stent.
- Duodenal obstruction - palliative duodenal stent or gastrojejunostomy.
- Pain - often severe, retroperitoneal; coeliac plexus neurolysis.
- Venous thromboembolism - one of the highest risks of any malignancy (Trousseau); therapeutic and prophylactic anticoagulation.
- Malnutrition, cachexia and exocrine insufficiency - PERT and nutritional support.
- Diabetes - often worsened by treatment; insulin.
- Liver, peritoneal and lung metastases - the cause of death in most. [1]
Procedure-related complications (Whipple)
- Postoperative pancreatic fistula (POPF) - the most feared complication (10 to 20 percent); leakage of enzyme-rich pancreatic fluid from the pancreaticojejunal anastomosis, causing abscess, pseudoaneurysm and sepsis. Risk factors: soft pancreas, small duct, high drain amylase.
- Delayed gastric emptying - the commonest complication (20 to 30 percent); prolonged ileus requiring nasogastric drainage and prokinetics; resolves over weeks.
- Post-pancreatectomy haemorrhage - early (anastomotic) or late (pseudoaneurysm erosion into the gastroduodenal artery stump). A sentinel bleed (small haematemesis) is a warning - urgent mesenteric angiography and embolisation; do not dismiss it.
- Intra-abdominal abscess, wound infection, anastomotic leak.
- Mortality under 5 percent in high-volume centres but much higher in low-volume centres - one reason centralisation matters.[1]
Classic pitfalls
- Mistaking autoimmune pancreatitis (IgG4) for PDAC and resecting - always check IgG4 and obtain tissue in an atypical case; AIP is steroid-responsive and curable.
- Missing ampullary carcinoma (much better prognosis) by assuming any periampullary mass is PDAC.
- Operating on a T4 locally advanced tumour that encases the SMA - it is unresectable; check the CT carefully.
- Forgetting Lewis-negative CA 19-9 - a normal CA 19-9 does not exclude PDAC.
- Ignoring a sentinel post-Whipple bleed - it heralds a pseudoaneurysm and death if untreated.
- Failing to germline-test metastatic PDAC - misses the small but important BRCA subgroup eligible for olaparib. [1]
Prognosis & Disposition
Prognosis is grim and dominated by stage at presentation.[1][2]
- Overall five-year survival about 10 to 12 percent - barely improved over decades, though adjuvant mFOLFIRINOX (PRODIGE 24) is changing this for the resected subgroup.
- After R0 resection plus adjuvant mFOLFIRINOX - median overall survival now exceeds 54 months and five-year survival reaches 30 to 40 percent in the best series.
- After R0 plus gemcitabine or no adjuvant - five-year survival 20 to 25 percent.
- Borderline resectable, downstaged and resected - five-year survival 15 to 30 percent.
- Locally advanced (T4) - median overall survival 15 to 20 months with FOLFIRINOX.
- Metastatic - median overall survival 8 to 11 months (FOLFIRINOX), 6 to 7 months (gemcitabine plus nab-paclitaxel), 6 months (gemcitabine alone); under three months with best supportive care alone.
- Untreated - median survival 3 to 6 months. [1]
Poor prognostic factors: advanced stage at diagnosis, caechoxia and low performance status (ECOG over 1), liver or peritoneal metastases, raised CA 19-9 baseline, SMAD4 loss / basal-like molecular subtype, positive resection margin (R1 or R2), node-positive disease, vascular invasion, and new-onset diabetes (a poor prognostic marker even after resection). [1]
Disposition is to a specialised hepatopancreatobiliary (HPB) multidisciplinary team for all resectable and borderline disease; to a medical oncology and palliative care team for locally advanced and metastatic disease; and to HPB cancer surveillance (EUS and MRCP) for hereditary high-risk kindreds. Patients are followed clinically and with CA 19-9 and CT every three to six months for two to three years after resection. [1]
Special Populations
- Hereditary high-risk kindreds (Peutz-Jeghers, hereditary pancreatitis, BRCA2, FAMMM, Lynch, familial PDAC) - lifelong surveillance with MRCP and EUS from age 40 to 50, or 10 years before the youngest affected relative. The goal is to find small T1N0 resectable tumours.[13][14]
- New-onset diabetes after age 50 with weight loss - index of suspicion for PDAC; imaging is reasonable if no other cause.
- Elderly and frail - dose-reduced gemcitabine or gemcitabine plus nab-paclitaxel rather than FOLFIRINOX; palliative focus; aggressive surgery only in the very fit.
- Anticoagulated patients - bridge or switch to low-molecular-weight heparin peri-operatively; PDAC itself carries a high VTE risk so therapeutic anticoagulation is usually continued long-term.
- Pregnancy - extremely rare; resection deferred to the postpartum period unless the tumour is obstructing; case-by-case multidisciplinary decisions.
- Renal or hepatic impairment - dose modifications of irinotecan and gemcitabine; FOLFIRINOX contraindicated in significant organ failure.
Evidence, Guidelines & Regional Differences
Landmark trials and what they changed
| Trial | Year | Setting | Key result | Practice change |
|---|---|---|---|---|
| PRODIGE 4 / ACCORD 11 (Conroy) | 2011 | Metastatic, fit | FOLFIRINOX median OS 11.1 vs 6.8 mo | FOLFIRINOX = first-line for fit metastatic |
| MPACT (Von Hoff) | 2013 | Metastatic | Gem-nab-paclitaxel OS 8.5 vs 6.7 mo | Alternative first-line, better tolerated |
| ESPAC-4 (Neoptolemos) | 2017 | Adjuvant | Gem-capecitabine OS 28.0 vs 25.5 mo | Adjuvant dual chemotherapy standard |
| PRODIGE 24 (Conroy) | 2018 | Adjuvant | mFOLFIRINOX OS 54.4 vs 35.0 mo | mFOLFIRINOX = preferred adjuvant for fit |
| POLO (Golan) | 2019 | BRCA metastatic maintenance | Olaparib PFS 7.4 vs 3.8 mo | Biomarker-driven maintenance therapy |
| Murphy | 2019 | Locally advanced, neoadjuvant | FOLFIRINOX + losartan resection rate 61% | Total neoadjuvant therapy expanded |
Controversies
- Surgery-first versus neoadjuvant for resectable disease - the PREOPANC and ongoing Alliance trials are testing whether all patients should receive neoadjuvant therapy; surgery-first remains standard for clearly resectable tumours, but neoadjuvant is gaining ground.
- Radiotherapy's role - declining in metastatic disease; consolidative chemoradiotherapy is selective in locally advanced disease.
- Immunotherapy - PDAC is refractory to checkpoint inhibitors because of its immunosuppressive, poorly antigenic stroma; responses only in the rare dMMR / MSI-H subgroup.
- Stromal depletion - hedgehog-pathway inhibitors failed to improve survival in trials, refuting the simple 'more stroma = worse' model.[2]
Regional guideline differences
[1] [1] [1]Exam Pearls
- Courvoisier's law: jaundice with a palpable, non-tender gallbladder is unlikely to be gallstones (stones scar and contract it); think malignant distal obstruction - pancreatic head cancer, cholangiocarcinoma, ampullary. The sign itself is Courvoisier sign.[1]
- KRAS mutation in over 90 percent of PDAC - the highest of any solid tumour. The four-gene cascade: KRAS, then CDKN2A (p16), then TP53, then SMAD4 (DPC4). SMAD4 loss = metastatic-prone.
- Trousseau migratory thrombophlebitis is a paraneoplastic hallmark; also consider pancreatic cancer in any older adult with unprovoked portal, splenic or cerebral vein thrombosis.
- Only 15 to 20 percent are resectable at presentation; the third to fourth leading cause of cancer death.
- Whipple has three anastomoses: pancreaticojejunostomy, hepaticojejunostomy, gastrojejunostomy (or duodenojejunostomy if pylorus-preserving). Removed: head of pancreas, duodenum (2nd-4th parts), distal CBD, gallbladder, ± distal stomach.
- Double-duct sign on CT (dilated CBD AND pancreatic duct) = head tumour until proven otherwise.
- CA 19-9 is undetectable in Lewis-negative patients (5 to 10 percent) - a normal value never excludes PDAC; it is for monitoring, not screening.
- Hypoenhancing mass on arterial-phase CT = PDAC (desmoplastic, avascular); hypervascular mass = think pNET or neuroendocrine.
- Distal pancreatectomy for body or tail removes the spleen because the splenic vessels are sacrificed; this matters for pneumococcal, meningococcal, Haemophilus and influenza vaccination pre- and post-operatively.
- PRODIGE 24 (adjuvant mFOLFIRINOX) and MPACT / PRODIGE 4 (metastatic) are the high-yield trial names.
- POLO = olaparib for germline BRCA metastatic PDAC after platinum response; the first biomarker-driven therapy in PDAC.
- New-onset diabetes after 50 with weight loss = think pancreatic cancer.
- Sentinel bleed after Whipple = pseudoaneurysm until proven otherwise - urgent angiography and embolisation.
- Ampullary carcinoma has a much better prognosis (early jaundice) - do not lump it with PDAC.
Exam application bank (NEET-PG / INICET)
One-line answer
Pancreatic ductal adenocarcinoma (PDAC) is a highly lethal malignancy of the pancreatic exocrine cells, driven by an obligate KRAS mutation in over 90 percent of tumours followed by CDKN2A, TP53 and SMAD4 loss, and by a dense desmoplastic stroma that shields it from drugs and the immune system. It is the third to fourth leading cause of cancer death in developed countries, with an overall five-year survival of about 10 to 12 percent because over 80 percent are unresectable at presentation. Risk factors are smoking (the biggest modifiable risk), chronic pancreatitis, obesity, new-onset diabetes, advancing age, and hereditary syndromes (BRCA2/PALB2, Peutz-Jeghers, Lynch, hereditary pancreatitis, FAMMM). Site defines the picture: a head tumour (60 to 70 percent) causes painless obstructive jaundice with pale stools, dark urine and pruritus, and Courvoisier sign (a palpable non-tender gallbl
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Pancreatic Cancer.
References
- [1]Kamisawa T, Wood LD, Itoi T, Takaori K, Hruban RH, Ye Y, et al. Pancreatic cancer Lancet, 2016.PMID 26830752
- [2]Kleeff J, Korc M, Apte M, La Vecchia C, Johnson CD, Biankin AV, et al. Pancreatic cancer Nat Rev Dis Primers, 2016.PMID 27158978
- [3]Ryan DP, Hong TS, Bardeesy N. Pancreatic adenocarcinoma N Engl J Med, 2014.PMID 25207767
- [4]Rawla P, Sunkara T, Gaduputi V. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors World J Oncol, 2019.PMID 30834048
- [5]Waddell N, Pajic M, Patch AM, Chang DK, Kassahn KS, Bailey P, et al. Whole genomes redefine the mutational landscape of pancreatic cancer Nature, 2015.PMID 25719666
- [6]Conroy T, Desseigne F, Ychou M, Bouche O, Guimbaud R, Becouarn Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer N Engl J Med, 2011.PMID 21561347
- [7]Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine N Engl J Med, 2013.PMID 24131140
- [8]Conroy T, Hammel P, Hebbar M, Ben Abdelghani M, Wei AC, Raoul JL, et al. FOLFIRINOX or Gemcitabine as Adjuvant Therapy for Pancreatic Cancer N Engl J Med, 2018.PMID 30575490
- [9]Neoptolemos JP, Palmer DH, Ghaneh P, Psarelli EE, Valle JW, Halloran CM, et al. Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): a multicentre, open-label, randomised, phase 3 trial Lancet, 2017.PMID 28129987
- [10]Golan T, Hammel P, Reni M, Van Cutsem E, Krarup-Hansen A, Bodoky G, et al. Maintenance Olaparib for Germline BRCA-Mutated Metastatic Pancreatic Cancer N Engl J Med, 2019.PMID 31157963
- [11]Murphy JE, Wo JY, Ryan DP, Jiang W, Yeap BY, Drapek LC, et al. Total Neoadjuvant Therapy With FOLFIRINOX in Combination With Losartan Followed by Chemoradiotherapy for Locally Advanced Pancreatic Cancer: A Phase 2 Clinical Trial JAMA Oncol, 2019.PMID 31145418
- [12]Ballehaninna UK, Chamberlain RS. Biomarkers for pancreatic cancer: promising new markers and options beyond CA 19-9 Tumour Biol, 2013.PMID 23949878
- [13]Wang Y, Cuggia A, Chen YI, Squire N, Moyser KH, Yilmaz AS, et al. Is Biannual Surveillance for Pancreatic Cancer Sufficient in Individuals With Genetic Syndromes or Familial Pancreatic Cancer? J Natl Compr Canc Netw, 2022.PMID 35714671
- [14]Syngal S, Brand RE, Church JM, Giardiello FM, Hampel HL, Burt RW, et al. ACG clinical guideline: Genetic testing and management of hereditary gastrointestinal cancer syndromes Am J Gastroenterol, 2015.PMID 25645574