General Surgery · General Surgery
Abdominal Wall Hernias
Also known as Inguinal hernia · Femoral hernia · Incisional hernia · Umbilical hernia · Strangulated hernia
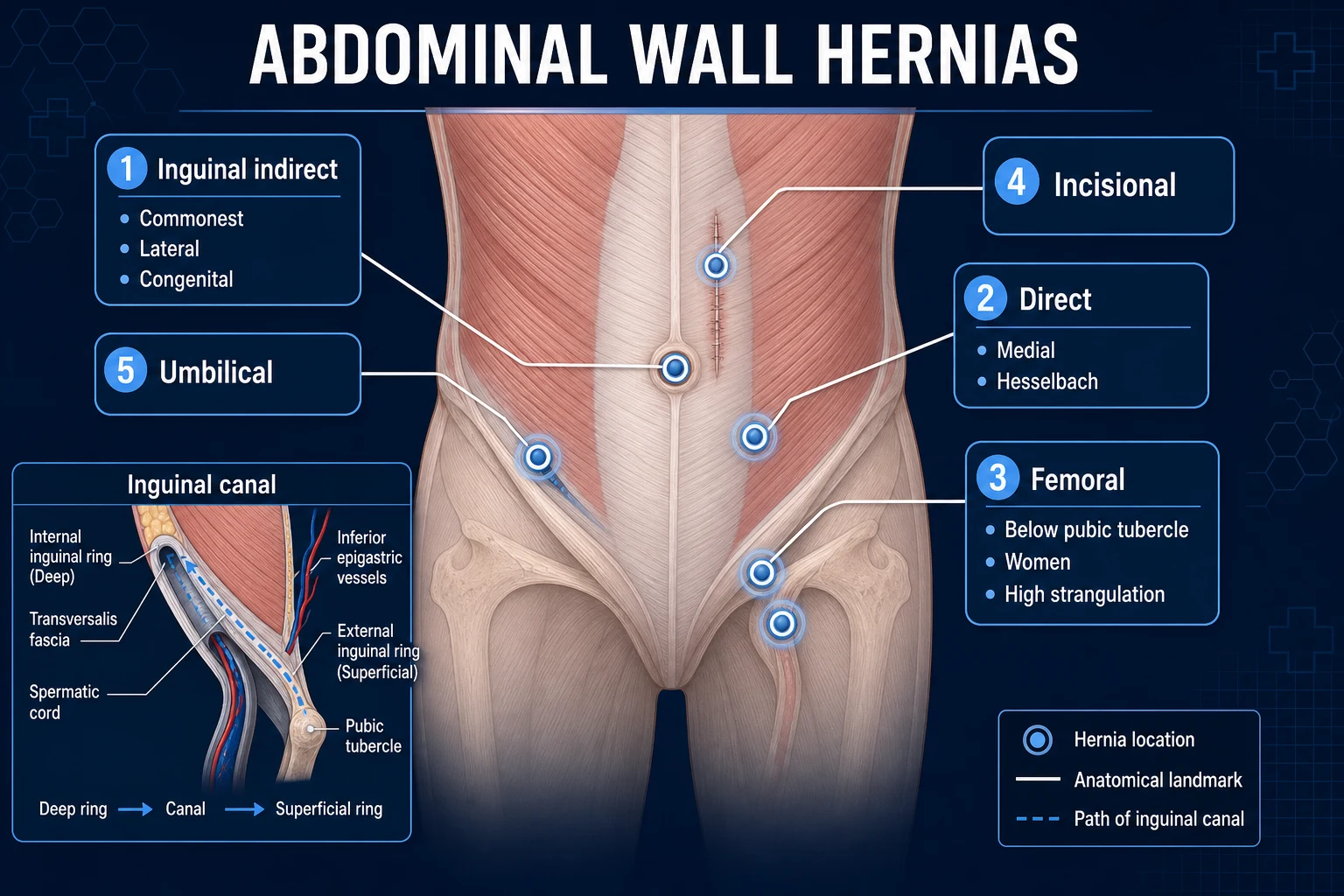
Hernia = abnormal protrusion of a viscus (or part of a viscus) through a defect in the wall of its containing cavity. Inguinal hernias are commonest (75%, above and medial to the pubic tubercle): indirect (through the deep ring, lateral to the inferior epigastric, congenital) versus direct (through Hesselbach's triangle, medial, acquired). Femoral hernias lie below and lateral to the pubic tubercle and carry the highest strangulation risk. Lichtenstein tension-free mesh repair is the open gold standard for inguinal hernia; strangulation (irreducible plus tender plus obstructive signs) is a surgical emergency. Always check the hernial orifices in any unexplained small-bowel obstruction.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Exam tags
Red flags
Overview & Definition
A hernia is defined as an abnormal protrusion of a viscus, or part of a viscus, through a defect in the wall of its containing cavity. The vast majority of clinically important hernias involve abdominal contents protruding through a congenital or acquired weakness in the abdominal wall, and the groin is by far the commonest site.[2]
Every hernia has three anatomical components:[2]
- The sac: a pouch of peritoneum (parietal) that lines the hernia. A true hernia always has a peritoneal sac — this distinguishes it from a divarication or eventration where the wall bulges but no sac forms.
- The coverings: the layers of abdominal wall that the sac pushes ahead of itself as it expands. The number and identity of these coverings depend on where the sac originates and how far it travels — for example, an indirect inguinal sac acquires internal oblique and external oblique layers as it traverses the canal.
- The contents: whatever abdominal viscus enters the sac — most commonly small bowel (ileum) or omentum, but occasionally large bowel, appendix, bladder, or ovary.[2]
The clinical life-history of a hernia follows a predictable and examinable cascade: reducible (contents return spontaneously to the abdomen) progresses to irreducible / incarcerated (contents are stuck, but still viable) and finally to strangulated (the blood supply is compromised, leading to venous congestion, arterial occlusion, ischaemia, gangrene and perforation).[2] Incarceration simply means irreducibility with a narrow neck; strangulation adds ischaemia and is a surgical emergency. A clinically silent but dangerous variant is the Richter's hernia, in which only the anti-mesenteric border of bowel is trapped within a small, rigid orifice — it strangulates and gangrenes without ever producing intestinal obstruction, because the lumen is never fully occluded.
Hernias are common — a groin hernia is the commonest surgical condition of men — and they are examined in every surgical short-answer, viva and long-case format because they test anatomy, clinical reasoning and decision-making simultaneously.[2]
Classification
Hernias are classified by anatomical site, by aetiology (congenital versus acquired), and by their clinical state (reducible, irreducible, obstructed, strangulated). The anatomical classification is the one examiners expect.[2]
Inguinal (75%)
above + medial to pubic tubercle
- **Indirect (about 2 of every 3 inguinal hernias):** through the deep ring, LATERAL to the inferior epigastric, congenital (patent processus vaginalis), all ages, M-to-F about 2:1, can enter the scrotum
- **Direct (about 1 in 3):** through HESSELBACH'S triangle, MEDIAL to the inferior epigastric, acquired, elderly males, rarely enters the scrotum, rarely strangulates
- **Pantaloon:** combined direct + indirect straddling the inferior epigastric on both sides of it
- Treatment: **Lichtenstein tension-free mesh repair** (open) or TEP/TAPP (laparoscopic)
Femoral (about 3%)
below + lateral to pubic tubercle
- Through the **femoral canal**, below the inguinal ligament and medial to the femoral vein
- F-to-M about 4-to-1, classic patient is an elderly woman
- **Highest strangulation risk** of any hernia — narrow, unyielding, rigid margins — up to 40% present already strangulated
- Always repaired; emergency surgery if strangulated
Anterior abdominal wall
midline and lateral wall
- **Umbilical / paraumbilical (10 to 15%):** congenital in children (usually closes by age 5) and acquired in multiparous or obese adults
- **Epigastric:** through the linea alba between the umbilicus and the xiphoid, small, often painful
- **Incisional (5 to 10%):** through a previous surgical scar; risk factors are wound infection, obesity, smoking
- **Spigelian:** through the linea semilunaris (the aponeurotic edge of the rectus) just lateral to the rectus, often interparietal and easily missed clinically
Rare / pelvic hernias
internal and atypical
- **Obturator:** through the obturator canal, elderly females, the **Howship-Romberg sign** (pain radiating from the inner thigh to the knee, worsened by extension, relieved by flexion)
- **Richter's:** only the anti-mesenteric border of bowel enters the sac — strangulates WITHOUT obstruction
- **Sliding (sliding hernia):** a viscus (caecum on the right, sigmoid on the left, or bladder) forms part of the wall of the sac
- **Parastomal:** beside a colostomy or ileostomy; internal (paraduodenal, foramen of Winslow) hernias present as obstruction without an external lump
By clinical state, the same hernia moves through reducible, irreducible (incarcerated), obstructed (lumen blocked but blood supply intact) and strangulated (blood supply cut off). The distinction between obstructed and strangulated is one of timing and viability — obstructed bowel is still salvageable, strangulated bowel is dying or dead.[2]
The Nyhus classification of inguinal hernia
The Nyhus classification (Nyhus, 1993) stratifies inguinal hernias by anatomical type, integrity of the posterior wall (transversalis fascia) and size of the internal ring, and is widely used to guide the choice between tissue and mesh repair:[8]
Type I
Indirect, normal ring
- Indirect inguinal hernia
- Internal (deep) ring of normal size and structure
- Posterior wall (transversalis fascia) intact
- Typical of infants, children and young adults
- Treatment: simple herniotomy / high sac ligation — NO mesh
Type II
Indirect, dilated ring
- Indirect inguinal hernia
- Internal ring enlarged but posterior wall intact (no true defect)
- Sac does not extend into the scrotum
- Treatment: herniotomy with ring narrowing or mesh reinforcement
Type III — posterior wall defect
IIIA direct / IIIB large indirect / IIIC femoral
- **IIIA — direct inguinal hernia** through Hesselbach's triangle
- **IIIB — large or complicated indirect** (pantaloon, sliding, scrotal) with destruction of the posterior wall and ring over 4 cm
- **IIIC — femoral hernia**
- Treatment: mesh repair mandatory (Lichtenstein / TEP / TAPP)
Type IV — recurrent
previous repair failed
- **IVA — direct recurrent**
- **IVB — indirect recurrent**
- **IVC — femoral recurrent**
- **IVD — combined / other**
- Treatment: prefer a different anatomical plane (laparoscopic) to avoid scar tissue
The Gilbert classification of inguinal hernia
The Gilbert classification (Gilbert, 1989) is an office-based, pre-operative classification based on the integrity of the internal ring and the posterior wall, designed to be used by the surgeon at the time of open repair:[9]
The five-type Gilbert classification of inguinal hernia
The Gilbert system was later expanded by Rutkow and Robbins (1993, 1998) to include Type 6 (pantaloon, combined direct + indirect) and Type 7 (femoral). Both Nyhus and Gilbert schemas serve the same purpose — to translate anatomy into a surgical decision — and examiners will accept either.[9]
Anatomy of the Groin — the Dimensions Examiners Test
No hernia question is answerable without a precise mental map of groin anatomy. The inguinal canal is an oblique passage about 4 cm long running parallel to and just above the inguinal ligament, from the deep ring to the superficial ring.[2]
The structural boundaries of the inguinal canal
The deep (internal) inguinal ring is an opening in the transversalis fascia at the midpoint of the inguinal ligament (midway between the anterior superior iliac spine and the pubic tubercle). The superficial (external) ring is a triangular opening in the external oblique aponeurosis, above and medial to the pubic tubercle. Because the rings do not lie opposite each other, increases in intra-abdominal pressure actually close the canal (a shutter mechanism) — which is why a normal canal does not herniate under load.[2]
The contents of the canal in the male are the spermatic cord (ductus deferens, testicular artery and vein, pampiniform plexus, cremasteric artery, vasal vessels, genital branch of the genitofemoral nerve and ilioinguinal nerve), and in the female the round ligament of the uterus.[2]
Hesselbach's (inguinal) triangle — the site of direct hernias — has three boundaries that examiners insist on reciting verbatim:[2]
- Medial: the lateral border of the rectus abdominis.
- Inferior: the inguinal ligament.
- Lateral: the inferior epigastric artery.[4]
A hernia lateral to the inferior epigastric is indirect; a hernia medial to it is direct. This single relationship is the cornerstone of the indirect-versus-direct distinction.[2]
The femoral canal lies below the inguinal ligament and is the medial-most compartment of the femoral sheath. Its boundaries are:[2]
- Anterior: the inguinal ligament.
- Posterior: the pectineal (Cooper's) ligament on the pubic ramus.
- Medial: the sharp, crescentic edge of the lacunar (Gimbernat's) ligament.
- Lateral: the femoral vein.[2]
The femoral canal is short (about 1.25 cm), narrow, and bounded by unyielding ligamentous walls — this anatomy is precisely why femoral hernias strangulate so often. The named ligaments of the floor — Poupart's (the inguinal ligament), Gimbernat's (the lacunar ligament, often incised to reduce a strangulated femoral hernia) and Cooper's (the pectineal ligament, the anchor point for many mesh repairs) — are tested repeatedly.[2]
Epidemiology & Risk Factors
Groin hernia repair is among the most frequently performed of all elective operations. Lifetime risk of undergoing inguinal hernia repair is about 27% in men and 3% in women. Inguinal hernias dominate (around 75% of all abdominal wall hernias); femoral hernias make up only about 3% but punch far above their weight in emergency work because of their strangulation rate.[2]
Headline numbers for abdominal wall hernias
The risk factors for any hernia reduce to two forces: a weakness in the abdominal wall and a sustained rise in intra-abdominal pressure. Wall weakness is congenital (a patent processus vaginalis, collagen disorders such as Ehlers-Danlos, or surgical scarring) or acquired (ageing, malnutrition, previous wound infection). Raised intra-abdominal pressure is produced by:[5]
- Chronic cough (COPD, smoking, tuberculosis).
- Chronic constipation and straining at stool.
- Prostatic outflow obstruction with straining to micturate.
- Heavy manual labour and weightlifting.
- Ascites, obesity, pregnancy.
- Peritoneal dialysis.[2]
Smoking is doubly dangerous: it produces chronic cough and it damages collagen cross-linking, which is why smokers have both more incisional and more recurrent hernias.[2][5] Specific risk factors worth knowing by name and condition:[2]
- Age. The prevalence of inguinal hernia rises steeply after 50, because of collagen degeneration in the transversalis fascia and a lifetime of mechanical loading.
- Family history. A first-degree relative with an inguinal hernia roughly doubles personal risk — a useful viva one-liner.
- Collagen disorders. Ehlers-Danlos syndrome, Marfan syndrome, osteogenesis imperfecta, and the rare Snyder-Robinson syndrome (an X-linked connective-tissue disorder with severe inguinal hernias in children) all predispose to hernia formation and recurrence because of defective collagen cross-linking.
- Abdominal aortic aneurysm (AAA). Inguinal hernia is more common in patients with AAA (and vice-versa) — a long-recognised association that reflects shared connective-tissue weakness. Always examine the groins in a patient with AAA and vice-versa.
- Obesity. Increases intra-abdominal pressure and stretches the linea alba, predisposing to incisional and umbilical hernias — and paradoxically masks the diagnosis clinically.
- Low birth weight and prematurity. The commonest single risk factor for congenital indirect inguinal hernia in children; the patent processus vaginalis is more frequent in low-birth-weight and preterm infants and the hernia presents in the first year of life in about 5% of ex-premature babies.
- Smoking and COPD. Both the chronic cough and the impaired collagen metabolism contribute.
- Chronic constipation and prostatism — straining raises intra-abdominal pressure.
- Ascites (cirrhosis, peritoneal dialysis). Umbilical and incisional hernias are common; spontaneous rupture is a recognised catastrophe.
- Pregnancy. Midline (diastasis-related) and incisional hernias are most affected; groin hernias are usually managed conservatively until the second trimester or post-partum.
- Chronic ambulatory peritoneal dialysis (CAPD). Long-term dialysis fluid raises intra-abdominal pressure and weakens the abdominal wall; prophylactic mesh at catheter removal is increasingly considered.[2]
India and low-resource settings: heavy manual labour in agriculture and construction is the dominant risk factor. Chronic cough from pulmonary tuberculosis still contributes. Malnutrition weakens the abdominal wall musculature. Where mesh access or training is limited, tissue repairs (Bassini, Shouldice) remain in use, with correspondingly higher recurrence. Femoral hernias in elderly rural women often present late with strangulation because of distance to surgical care, and incisional hernias after open laparotomy are more common because of higher wound-infection rates and non-mesh repairs.[2]
Pathophysiology
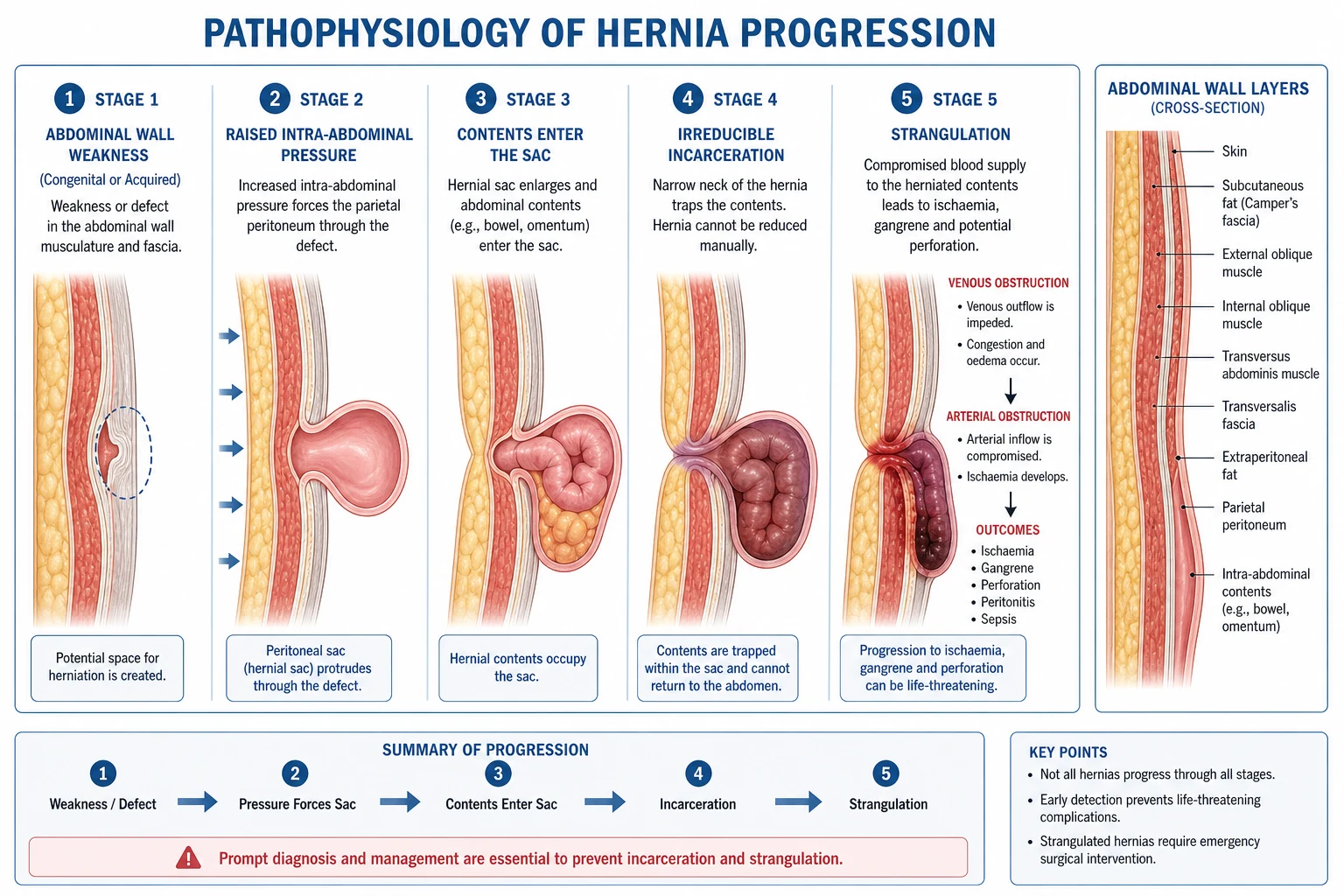
The mechanical narrative is straightforward, but the biology behind it is what examiners reward when distinguishing a strong answer from a rote one.[2]
- Predisposition. The wall defect is either pre-formed (a congenital patent processus vaginalis, an open umbilical ring, a weak transversalis fascia in Hesselbach's triangle) or acquired (collagen degeneration with age, surgical division of abdominal-wall fibres, wound infection with tissue loss).
- Pressure loading. Anything that repeatedly raises intra-abdominal pressure then drives peritoneum (the sac) through the defect. Over time the defect enlarges, the sac lengthens, and contents begin to enter it.
- Entrapment at the neck. A narrow, rigid neck is the dangerous feature. Contents enter the sac but cannot return. Venous return is occluded first (low-pressure system), the bowel and sac become congested and oedematous, swelling further occludes the arterial supply, and the bowel becomes ischaemic — this is strangulation. Untreated, the bowel infarcts, perforates, and the patient develops peritonitis and systemic sepsis.[2]
The processus vaginalis is the embryological key to indirect hernias. As the testis descends from the posterior abdominal wall to the scrotum in the seventh to ninth month of gestation, it carries a diverticulum of peritoneum — the processus vaginalis — through the inguinal canal ahead of it. Normally this tube obliterates, leaving only the tunica vaginalis around the testis. If it fails to obliterate (patent processus vaginalis, present in up to 20% of adults at autopsy), a pre-formed sac exists through which bowel can herniate at any time of life — explaining why indirect inguinal hernias are congenital in origin even when they present in adult life, and why they can extend into the scrotum along the line of testicular descent. The direct hernia, by contrast, pushes through a weakened Hesselbach's triangle as the transversalis fascia thins with age — it is genuinely acquired and rarely enters the scrotum because it does not traverse the canal's full length.[2]
Clinical Presentation
The classical story is unmistakable: a patient notices a groin (or scrotal) lump that appears on standing, coughing or straining and disappears on lying down. As the hernia enlarges it produces an aching discomfort, worse with exertion and relieved by lying down, and may become harder to reduce over months.[2]
Typical features of a reducible hernia:[2]
- A lump that appears or enlarges on standing, coughing, straining or heavy lifting.
- Reduces spontaneously on lying down, or with gentle pressure.
- A positive cough impulse (an expansile impulse felt on the lump when the patient coughs).
- Aching or dragging discomfort, rarely severe.
- Possible extension into the scrotum (indirect inguinal).[2]
Atypical presentations examiners test deliberately:[2]
- Elderly woman with a small, tender groin lump and vomiting — a strangulated femoral hernia masquerading as bowel obstruction.
- Repeated episodes of small-bowel obstruction with no abdominal scar — an occult incarcerated femoral or obturator hernia.
- Intermittent inner-thigh pain in an elderly woman, no visible lump — an obturator hernia producing the Howship-Romberg sign (pain along the adductor surface of the thigh to the knee, relieved by flexion, caused by obturator nerve compression).
- A non-obstructing tender groin mass with systemic toxicity — a Richter's hernia (the anti-mesenteric border is strangulated without obstructing the lumen).[4]
Incarceration versus strangulation — the distinction that drives disposition:[2]
Incarcerated (irreducible)
stuck but viable
- Cannot be reduced back into the abdomen
- Mildly tender or non-tender
- Patient is systemically well, no fever
- No signs of bowel obstruction
- Treatment: urgent (not emergency) surgical repair
Strangulated
ischaemic — emergency
- Irreducible AND locally very tender AND tense
- Overlying skin may be red or dusky
- Systemically toxic: tachycardia, fever, leucocytosis
- Signs of small-bowel obstruction (vomiting, distension, constipation)
- Treatment: EMERGENCY surgery, with bowel resection if gangrenous
When a hernia contains bowel and that bowel becomes obstructed, the patient develops the classical small-bowel-obstruction picture — colicky central abdominal pain, distension, vomiting and absolute constipation — plus a tender irreducible hernia. The hernial orifices must therefore be examined in every patient presenting with bowel obstruction.[2]
Differential Diagnosis
A groin lump has a wide differential, and distinguishing each from a hernia is a viva staple. The most useful single discriminator is the position relative to the pubic tubercle and the behaviour on coughing and lying down.[2]
- Inguinal hernia — above and medial to the pubic tubercle; cough impulse; reduces on lying down.
- Femoral hernia — below and lateral to the pubic tubercle; high strangulation risk; classic in elderly women.
- Saphena varix — cough impulse that empties on lying down; disappears completely; blue, soft, with varicose veins below.
- Femoral artery aneurysm — pulsatile (expansile) with a bruit; does not reduce; usually in a patient with vascular disease.
- Inguinal lymphadenopathy — multiple, often matted lumps; no cough impulse; does not reduce; look for a distal focus of infection or malignancy.
- Lipoma of the cord — soft, lobulated, non-reducible; mimics a hernia at operation; cough impulse absent.
- Hydrocele — fluctuant, transilluminates; surrounds the testis; you can get above the swelling (palpate the cord above it); no cough impulse.
- Varicocele — bag-of-worms feel above the testis; left side in about 90%; decompresses on lying down; no expansile cough impulse.
- Undescended testis — empty scrotum; palpable mass along the line of descent; no separate testis in the scrotum.
- Psoas abscess — lump in the femoral triangle; fluctuant; associated with lumbar spine tuberculosis (Pott's); hip held in flexion.
- Sebaceous cyst or lipoma of skin — superficial, fixed to skin; no cough impulse; does not change with posture.[2]
Clinical & Bedside Assessment
Examination is performed with the patient standing and then lying supine, both groins exposed.[2]
Inspection (standing first): look for a visible lump, its relationship to the pubic tubercle, scrotal extension, and any previous surgical scars. Ask the patient to cough — a hernia produces a visible bulge.[2]
Palpation: confirm the cough impulse by placing a fingertip on the suspected deep ring (midpoint of the inguinal ligament). An expansile impulse suggests an indirect inguinal hernia. Determine the relationship to the pubic tubercle:[2]
[2]The deep-ring occlusion test distinguishes indirect from direct hernias. After reducing the hernia fully, occlude the deep ring with a fingertip and ask the patient to cough or strain. If the hernia is controlled (no bulge appears), it is indirect — it exits through the occluded deep ring. If the hernia bulges medial to your occluding finger, it is direct — it pushes through Hesselbach's triangle, medial to the ring.[2]
Completing the examination: examine both groins (bilateral inguinal hernias are common), palpate the opposite testis and cord, perform a digital rectal examination (prostatic enlargement contributing to raised intra-abdominal pressure), and auscultate the hernia for bowel sounds if it is large. Always examine the abdomen for signs of obstruction if the hernia is irreducible.[2]
Investigations
The diagnosis of a hernia is clinical — a confident history and examination are sufficient in the great majority of cases, and no imaging is required before elective repair.[2]
- Ultrasound of the groin is the first-line investigation when there is genuine doubt: it can distinguish a hernia from a lymph node, a saphena varix, a lipoma of the cord or a hydrocele, and it can demonstrate a small femoral hernia that is hard to feel in an obese patient.
- CT of the abdomen and pelvis is used for complex, recurrent or large incisional hernias, for suspected internal hernias (paraduodenal), and in the emergency setting to confirm the cause of obstruction and to assess bowel viability. CT is the modality of choice for the rare pelvic hernias — obturator, sciatic, perineal — where clinical detection is poor.
- MRI is reserved for sportsman's hernia / Gilmore's groin (chronic groin pain in athletes with suspected posterior-wall injury) and for distinguishing a true hernia from musculoskeletal causes of groin pain.
- Herniography (injecting contrast into the peritoneum and fluoroscoping for a sac) is of historical interest only and is rarely used today, having been supplanted by ultrasound.
- Routine blood tests are not needed for elective repair, but a full blood count, group-and-save, urea and electrolytes and ECG form the standard pre-operative work-up. In the emergency presentation, an elevated lactate or white-cell count supports the diagnosis of strangulation.[4]
Management — Resuscitation
A strangulated hernia with bowel obstruction is a surgical emergency. The immediate priority is resuscitation, not the operating room.[2]
- NBM (nil by mouth) immediately.
- Nasogastric tube on free drainage to decompress the stomach and reduce the risk of aspiration.
- Intravenous fluids — start with isotonic crystalloid (for example 0.9% sodium chloride with a potassium supplement) to correct the dehydration and electrolyte disturbance of small-bowel obstruction; insert a urinary catheter to monitor response.
- Analgesia — opioid analgesia (for example morphine 0.1 mg/kg intravenously, titrated) plus an antiemetic.
- Broad-spectrum antibiotics — for example co-amoxiclav 1.2 g intravenously or a second-generation cephalosporin plus metronidazole, given before surgery for strangulation.
- Emergency surgery once the patient is resuscitated — do not delay operating to "settle" a confirmed strangulated hernia.[2]
Taxis (gentle reduction): should be attempted only when there are no signs of strangulation (no fever, no peritonism, the hernia is not tense and the overlying skin is normal). Give adequate analgesia, place the patient head-down (Trendelenburg), and apply gentle sustained pressure. If unsuccessful, abandon and operate. The danger of taxis in a strangulated hernia is reduction en masse — reducing the bowel and its strangulated, ischaemic segment back into the abdomen, where it is then hidden but still gangrenous.[2]
Management — Definitive and Stepwise
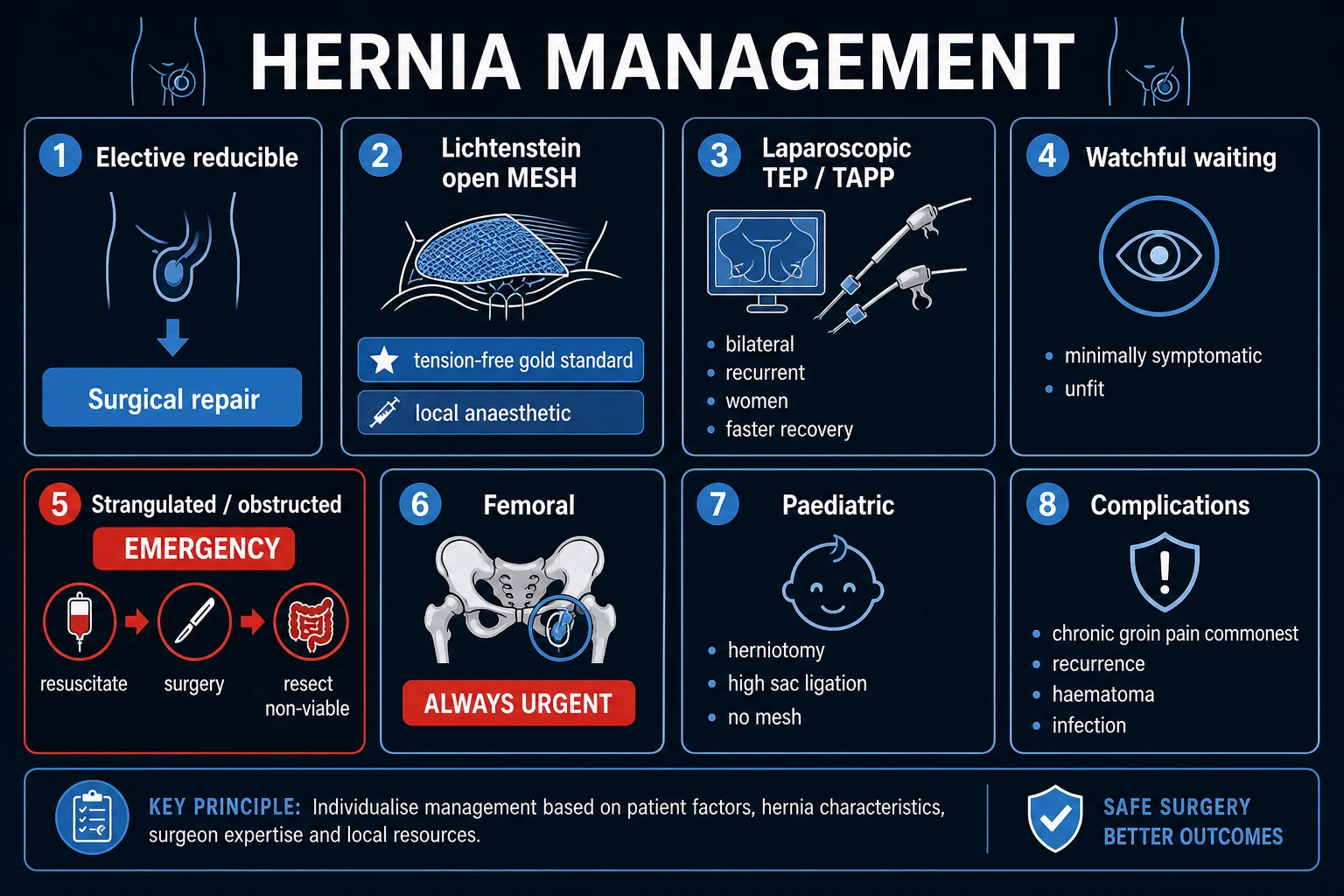
The aim of hernia repair is to close the defect, restore anatomy and prevent recurrence — using either a tension-free mesh (modern standard) or a tissue repair where mesh is contraindicated. The principle of tension-free repair, introduced by Lichtenstein, transformed recurrence rates from 10 to 15% (older tissue repairs) to under 3%.[2]
Elective inguinal hernia repair
Open — Lichtenstein tension-free mesh repair is the open gold standard for primary unilateral inguinal hernia.[2][2]
- A synthetic non-absorbable mesh (polypropylene, e.g. Prolene) is placed on the posterior wall of the canal, on top of (anatomically anterior to) the transversalis fascia.
- The mesh is sutured to the pubic tubercle, the inguinal ligament and the conjoint tendon, with a slit for the spermatic cord to pass through.
- Crucially the repair is tension-free — no attempt is made to pull tissues tightly together. This is the reason for the low recurrence rate (about 1 to 3%).
- Performed under local, regional or general anaesthesia; commonly as a day-case procedure.[2]
Laparoscopic repair (TEP or TAPP) places the mesh in the pre-peritoneal space (posterior to the defect, where intra-abdominal pressure actually pushes the mesh against the wall to seal it).[2][6]
- TEP (totally extraperitoneal): the pre-peritoneal space is entered and developed without opening the peritoneum.
- TAPP (transabdominal pre-peritoneal): the peritoneal cavity is entered, the peritoneum over the defect is incised, the mesh is placed in the pre-peritoneal plane, and the peritoneum is closed over it.
- Indications: bilateral inguinal hernias (one set of ports instead of two open incisions), recurrent hernias after a previous anterior open repair (the dissection enters virgin tissue), and patient preference for a minimally invasive approach.
- The VA Cooperative trial (Neumayer et al.) showed that laparoscopic repair, in less-experienced hands, had a higher recurrence rate than open Lichtenstein — so laparoscopic repair is operator-dependent and should be done by experienced surgeons.[6]
Tissue repairs (no mesh) are reserved for contaminated fields, mesh-allergy (rare), or centres without mesh access:[2]
- Shouldice repair (the "Canadian" repair) — overlapping repair of the transversalis fascia in four layers; the best of the tissue repairs, with recurrence under 5% at experienced centres.
- Bassini repair — non-tension-free approximation of the conjoint tendon to the inguinal ligament behind the cord; historically important but high recurrence (10 to 15%), now largely abandoned except in resource-limited settings.[2]
Paediatric inguinal hernia: the defect is a patent processus vaginalis — the wall itself is normal, so the only treatment needed is herniotomy (high ligation and excision of the sac at the deep ring). No mesh is used. Bilateral in about 10%; premature infants have a higher incidence.[2]
Preperitoneal and open-mesh alternatives for groin hernia
Several other repair options are tested in the operating theatre and the viva:[2]
- Kugel repair (open preperitoneal). A small transverse incision is made 2 to 3 cm above the inguinal ligament, the preperitoneal space is developed bluntly between the transversus abdominis and the peritoneum, and a self-expanding polypropylene patch with a "memory recoil ring" is placed to cover the entire myopectineal orifice (direct, indirect and femoral spaces) from behind. It aims to combine the low recurrence of laparoscopic preperitoneal mesh with the avoidance of general anaesthesia and pneumoperitoneum, and is especially useful for recurrent hernia after an anterior repair.[12]
- Read-Rives preperitoneal repair. A posterior approach through the space of Bogros places a wide Dacron or polyester mesh in the preperitoneal plane without fixation, relying on intra-abdominal pressure to hold it against the abdominal wall. The principle — Pascal's hydrostatic paradox applied to hernia — is the same as the modern Stoppa "giant prosthetic reinforcement of the visceral sac" (GPRVS) for bilateral or recurrent groin hernias, in which a single large sheet of mesh lines both myopectineal orifices through a midline preperitoneal incision.[13]
- Robotic TAPP. A platform-assisted variant of TAPP using the da Vinci system; it offers three-dimensional magnified vision, wristed instrumentation and easier intracorporeal suturing, so that complex primary and recurrent inguinal hernias (and many ventral hernias) can be repaired with a preperitoneal or transabdominal mesh with reduced surgeon fatigue. Outcomes are at least equivalent to laparoscopic TEP/TAPP and may be lower recurrence for recurrent and complex hernias, but cost and console-time remain constraints.
Ventral and incisional hernia — how the mesh sits
Ventral and incisional hernia repair depends critically on where the mesh is placed. The four classical planes (anterior to posterior) are:[4][5]
- Onlay: mesh laid on the anterior rectus sheath, anterior to the defect. Easy to place, but high recurrence (mesh lifts off as the repair is under tension) and a high rate of seroma and wound complications.
- Inlay (bridging): mesh sutured to the edges of the defect with no overlap — almost always abandoned because of unacceptable recurrence.
- Sublay (retrorectus, Rives-Stoppa): mesh placed in the retrorectus space between the rectus muscle and the posterior rectus sheath. The mesh is under the muscle, supported by the abdominal wall and held in place by intra-abdominal pressure. This is the gold-standard open repair for medium and large incisional hernias with low recurrence and few mesh-related complications.
- Underlay (intraperitoneal onlay mesh, IPOM): mesh placed inside the peritoneal cavity and fixed to the abdominal wall with tackers or sutures. A composite mesh (polypropylene + an anti-adhesion barrier on the visceral side, e.g. ePTFE or oxidized regenerated cellulose) is mandatory here because the mesh is in direct contact with bowel. Laparoscopic IPOM is the commonest minimally invasive approach for ventral and incisional hernia.[4]
Component separation (Ramirez) for massive defects
When the defect is large or the abdominal wall has lost domain (the viscera can no longer be returned to the abdomen without respiratory compromise), component separation allows the midline to be closed without tension. The original technique was described by Ramirez, Ruas and Dellon (1990):[10]
- Anterior component separation releases the external oblique aponeurosis about 1 to 2 cm lateral to the rectus, allowing the rectus complex to advance medially by 5 to 10 cm on each side (10 to 20 cm total) at the level of the umbilicus.
- The posterior component separation (also called transversus abdominis release, TAR) releases the transversus abdominis medial to the linea semilunaris and develops the retrorectus and preperitoneal planes widely, allowing even larger medialisation and providing an excellent sublay pocket for mesh.
- These techniques can be combined with a sublay (Rives-Stoppa) mesh or with perforator-sparing ("perforator-preserving") modifications to reduce skin-flap complications.[10]
Mesh in contaminated and dirty wounds
Mesh in a contaminated (e.g. concurrent bowel resection) or dirty (established infection) field is contentious. Synthetic permanent polypropylene or polyester mesh is generally avoided because the infection rate approaches 30% and mesh removal may be required. The choices are:[2]
- Primary tissue repair with delayed mesh in 6 to 12 months if recurrence occurs.
- Biological mesh (porcine dermis, bovine pericardium, small-intestinal submucosa) — used in contaminated fields because it is resorbable, becomes incorporated and is more resistant to infection; long-term recurrence rates are similar to synthetic mesh in clean cases and may be higher in contaminated cases.
- Absorbable synthetic mesh (e.g. polyglycolic or polylactic acid) as a temporising bridge with planned definitive repair later.[2]
Femoral hernia repair
A femoral hernia is always repaired — watchful waiting is not appropriate because of the high strangulation rate (up to 40% at presentation).[2]
The classical approaches are described by their incision:[2]
- Lockwood (low) approach — infra-inguinal incision, used for elective repair.
- McEvedy (high) approach — oblique incision above and parallel to the inguinal ligament, used for strangulated femoral hernias because it allows access to the abdomen for bowel resection if needed.
- Lotheissen (trans-inguinal) approach — opens the inguinal canal, retracts the cord, and repairs from above; the modern preference is often to combine this with a Cooper's ligament (McVay) repair.[2]
The defect is closed with non-absorbable sutures approximating the inguinal ligament to Cooper's (pectineal) ligament (a McVay / Cooper's ligament repair), or by mesh. In strangulation, the rigid Gimbernat's (lacunar) ligament is frequently incised to release and reduce the hernia, but care must be taken because of an abnormal obturator artery (a coronaria mortis) crossing it in up to 30% of patients.[2]
Umbilical and paraumbilical hernia
- Children: the vast majority close spontaneously by age 5. Repair is indicated if the hernia persists beyond age 4, becomes symptomatic, or strangulates. Herniotomy with a small Mayo repair is typical.
- Adults: do not close spontaneously and should be repaired. The classical Mayo repair uses a vest-over-pants overlapping closure of the rectus sheath, but modern practice favours a small mesh for larger defects (over 2 cm) to reduce recurrence.[5]
Incisional hernia
Incisional hernias follow 10 to 15% of midline laparotomies; risk factors include wound infection, obesity, smoking, type of incision (midline higher than transverse) and surgical technique.[5]
- Small defects (under 4 cm): primary closure with non-absorbable sutures may suffice.
- Larger defects (over 4 cm) or recurrent: mesh repair — onlay (anterior to the anterior rectus sheath), sublay (in the retrorectus space, generally preferred), or underlay (intraperitoneal). Laparoscopic mesh repair is increasingly used for smaller incisional hernias.
- Massive defects with loss of domain: a component separation technique releases the external oblique aponeurosis to allow midline closure.
- The European Hernia Society classification stratifies incisional hernias by size (W1 under 4 cm, W2 4 to 10 cm, W3 over 10 cm) and recurrence (primary versus recurrent) and guides mesh choice.[4]
Robson-Hunt classification (strangulated hernia)
For the strangulated hernia at laparotomy, the Robson-Hunt classification describes the operative findings and guides whether resection is needed:[5]
- Bowel viable — reduce and repair.
- Bowel of doubtful viability — warm packs, re-assess; if it recovers, reduce and repair.
- Bowel gangrenous — resection and anastomosis, then repair.[2]
Mesh is generally avoided in a contaminated field (gangrenous bowel), but a biological mesh or primary tissue repair may be used.[2]
Truss and watchful waiting
- Truss: a mechanical device that holds the hernia reduced. Useful only as a temporising measure in patients unfit or unwilling for surgery. It does not cure the hernia, and pressure from the pad may injure the contents or the cord. It is not a substitute for repair.
- Watchful waiting: Fitzgibbons et al. randomised minimally symptomatic men to watchful waiting versus repair and found that watchful waiting was safe in the short term, but crossover to surgery was common (about 25% at 2 years, mainly for pain) and the long-term risk of acute presentation remained. Watchful waiting is therefore a reasonable option for the elderly, asymptomatic patient with significant comorbidity, but definitive treatment remains surgical repair.[3]
Specific Hernia Subtypes and Scenarios
Pantaloon hernia: a combined direct and indirect hernia straddling the inferior epigastric vessels on both sides, like a pair of pantaloons. Easily missed at open repair unless the cord structures are inspected carefully.[2]
Sliding hernia (hernia en glissade): a viscus forms part of the wall of the sac — the caecum on the right, the sigmoid colon on the left, or the bladder medially. The danger at operation is injury to the viscus when the sac is mobilised. The sac should be reduced rather than dissected off the viscus, and a mesh placed to reinforce the posterior wall.[2]
Richter's hernia: only the anti-mesenteric border of bowel enters the sac. Because the lumen is never fully occluded, the patient does not develop classical bowel obstruction — yet the trapped wall strangulates and gangrenes. This is the classic trap of the femoral hernia, and the reason a small femoral hernia can present with systemic sepsis and a tender groin lump but no obstructive symptoms.[2]
Obturator hernia: through the obturator canal in the pelvic floor. Classically an elderly, emaciated woman with no visible lump. The hallmark is the Howship-Romberg sign — pain radiating from the inner thigh down to the knee, worsened by extension and external rotation of the hip, relieved by flexion, caused by compression of the obturator nerve. Up to 90% present with obstruction; mortality is high because of delayed diagnosis.[2]
Spigelian hernia: through the linea semilunaris (the aponeurotic edge of the lateral border of the rectus abdominis), usually just below the arcuate line. Often interparietal (between muscle layers), so it is easily missed clinically and frequently diagnosed on CT or ultrasound. Strangulation is common because of the narrow neck.[2]
Epigastric hernia: a small defect in the linea alba between the umbilicus and the xiphoid process. Often presents with a small, painful, non-reducible lump of pre-peritoneal fat. Repair is by simple closure of the defect; small defects do not always need mesh.[2]
Parastomal hernia: beside a colostomy or ileostomy. Common (up to 50% of stomas over time). Repair is by stomal relocation or mesh reinforcement around the stoma. Prophylactic mesh at stoma formation is increasingly recommended.[2]
Sportsman's hernia (Gilmore's groin / athletic pubalgia): not a true anatomical hernia but a chronic disruption of the common aponeurosis of the rectus abdominis and the adductor longus (or a tear of the posterior inguinal wall) in athletes. The patient has exercise-related groin pain, often after a sudden change-of-direction sport (football, rugby, hockey), but no palpable lump and no cough impulse. MRI is the imaging investigation of choice, and definitive treatment is physiotherapy with selective laparoscopic mesh reinforcement of the posterior wall; a missed athletic pubalgia is a common cause of failed inguinal hernia repair in young athletes.[2]
Rectus diastasis (divarication of the recti): a thinning and widening of the linea alba above or below the umbilicus, most often after pregnancy or major weight loss. There is no true fascial defect and no peritoneal sac, so it is not a hernia in the strict sense — but it is a common source of an abdominal bulge that mimics a ventral hernia. Repair is usually cosmetic (plication of the linea alba, sometimes combined with abdominoplasty); symptomatic cases benefit from a TRS-style endoscopic-assisted plication.[4]
Lumbar hernia: a rare posterolateral abdominal wall hernia through one of two triangles:[4]
- Superior lumbar triangle of Grynfeltt-Lesshaft (bounded by the 12th rib, the erector spinae and the posterior border of the internal oblique) — the commoner site.
- Inferior lumbar triangle of Petit (bounded by the iliac crest, the latissimus dorsi and the external oblique) — usually smaller and more obvious clinically.[4]
Primary lumbar hernias are spontaneous and more common in elderly, thin women; secondary lumbar hernias follow trauma, flank surgery (nephrectomy, iliac-bone harvest) or infection. Incarceration and strangulation are common because of the narrow, rigid bony edges. CT confirms the diagnosis; open mesh repair (transabdominal or extra-peritoneal) is the standard, with laparoscopic repair increasingly used for small defects.[4]
Sciatic hernia: an extremely rare pelvic floor hernia through the greater or lesser sciatic foramen. It is almost never diagnosed clinically and usually presents as an unexplained pelvic mass, sciatica (sciatic nerve compression), or bowel obstruction in an elderly woman. CT or MRI is required. Treatment is operative reduction and closure of the sciatic foramen with mesh or a transabdominal approach — but the diagnosis is so often missed that the patient may present with strangulation or gluteal sepsis first.[2]
Perineal hernia: a herniation through a defect in the pelvic floor, most often after abdominoperineal resection (APR) for low rectal cancer (incidence up to 26% after APR), pelvic exenteration, or perineal trauma. Women are at higher risk because of the wider pelvic outlet. Small asymptomatic perineal hernias can be observed; larger or symptomatic ones are repaired by a combined abdominal and perineal approach with mesh (transabdominal, perineal, or a combination), with recurrence rates of 30 to 50% historically and falling with modern biologic and synthetic mesh reinforcement of the pelvic floor.[4]
Complications and Pitfalls
Of the disease (untreated hernia):[2]
- Incarceration — irreducible but viable; risk of progression to strangulation.
- Obstruction — bowel in the sac is kinked; small-bowel obstruction with its complications.
- Strangulation — ischaemia, gangrene, perforation, faecal peritonitis, sepsis, death. Mortality is 5 to 15% when bowel resection is required.[2]
Of surgery:[2]
- Recurrence: open Lichtenstein 1 to 3%; laparoscopic 2 to 5% (higher in inexperienced hands); tissue repairs (Bassini) 10 to 15%.[2]
- Chronic groin pain (inguinodynia / chronic post-herniorrhaphy pain): affects up to 10 to 12% of patients and is the most important quality-of-life complication. Caused by neuropathy of the ilioinguinal, iliohypogastric or genitofemoral nerves (often at the mesh), or by neuroma. Identification and proactive management of all three nerves during surgery (and mesh fixation that avoids them) reduces incidence.[2]
- Wound infection: 1 to 5%; deep mesh infection is a serious complication requiring mesh removal in some cases.
- Seroma and haematoma: common, usually self-limiting; aspiration risks infection.
- Ischaemic orchitis: thrombosis of the pampiniform plexus, usually from cord dissection at redo surgery, leading to testicular atrophy. Risk is highest after repair of recurrent hernias.
- Urinary retention: common post-operatively, especially in elderly men with prostatism; short-term catheterisation may be needed.
- Injury to cord structures: vas deferens (rare infertility), testicular artery (testicular atrophy), ilioinguinal nerve (numbness of the medial thigh and scrotum).[2]
Pitfalls examiners trap candidates with:[2]
-
Missing a femoral hernia. Always palpate below and lateral to the pubic tubercle, not just the inguinal canal. A small femoral hernia in an obese woman is the classic missed diagnosis that becomes a fatal strangulation.
-
Forgetting to check the hernial orifices in small-bowel obstruction. An incarcerated femoral hernia is the commonest cause of obstruction in the patient with no previous surgery.
-
Attempting taxis in a strangulated hernia. The danger is reduction en masse — the ischaemic bowel is reduced into the abdomen and the catastrophe is hidden.
-
Injuring an abnormal obturator artery (coronaria mortis) when incising Gimbernat's ligament to release a strangulated femoral hernia.
-
Treating an obstructed femoral hernia as a simple obstruction by nasogastric decompression alone — only surgery will relieve the obstruction.
-
Using mesh in a contaminated field (gangrenous bowel resection) — risk of mesh infection; consider biological mesh or tissue repair.[2] Other recognised operative complications worth naming:[2]
-
Mesh infection — 1 to 3% in clean cases, up to 30% in contaminated or dirty cases. Superficial wound infection usually responds to antibiotics and drainage; deep prosthetic infection is far more serious — the mesh may need to be removed entirely, with a staged re-repair several months later. Biological meshes are preferred in contaminated cases.
-
Mesh erosion and migration. Erosion into adjacent viscera (bowel, bladder) is rare but serious and well-documented with intraperitoneal onlay mesh. Presents late with fistula, sepsis, recurrent urinary tract infection (bladder erosion) or chronic pain. Laparoscopic or open mesh removal is required; small-bowel fistula from eroded polypropylene mesh is the most dramatic presentation.
-
Vascular injury. Damage to the inferior epigastric vessels, the external iliac or femoral vessels, or an aberrant obturator artery (coronaria mortis) is a recognised laparoscopic and open complication, particularly during tack placement in TEP/TAPP and during dissection in recurrent femoral hernia repair. Major vascular injury may need conversion to open repair and vascular surgical repair.
-
Visceral injury. Bowel, bladder and, rarely, stomach or liver laceration can occur during adhesiolysis at laparoscopic repair, during peritoneal closure in TAPP, or during repair of a sliding hernia containing caecum, sigmoid or bladder.
-
Bladder injury — a specific concern in laparoscopic repair of direct and femoral hernias, where the bladder forms part of the medial preperitoneal space; recognised by intra-operative gas or urine in the field, repaired immediately with absorbable sutures and catheter drainage for 7 to 10 days.
-
Recurrence — depends on the technique. The EU Hernia Trialists Collaboration meta-analysis of 4005 patients in 15 trials showed open mesh repair cut recurrence from 4.4% to 1.4% compared with non-mesh tissue repair (OR 0.39, 95% CI 0.25 to 0.59), and the VA Cooperative trial of open vs laparoscopic mesh showed open Lichtenstein recurrence 4.9% versus 10.1% laparoscopic in less-experienced hands.[11][6]
-
Chronic post-herniorrhaphy pain (CPIP / inguinodynia) — the most important patient-centred complication. Reported in 10 to 15% of patients after open mesh repair, lower (~6 to 8%) after laparoscopic repair, and severe enough to limit daily activity in 1 to 3%. Best prevented by careful nerve handling (identification and preservation of the ilioinguinal, iliohypogastric and genital branch of the genitofemoral nerve), avoiding heavy-weight polypropylene close to the nerves, and using light-weight macroporous mesh where possible. Established CPIP is managed with neuropathic analgesia (gabapentin or duloxetine), targeted nerve blocks, and surgical neurectomy for refractory cases.
Mortality — emergency versus elective
The clearest summary statistic a candidate should know: emergency hernia repair carries a 4 to 5-fold higher mortality than the same operation performed electively, and bowel resection at the emergency operation roughly doubles mortality again. For strangulated femoral hernia specifically, post-operative mortality is 5 to 15% in older series and remains substantially higher than the near-zero mortality of elective femoral repair. The take-home message for the viva: a femoral hernia is best repaired when it is asymptomatic.[2]
Prognosis and Disposition
- Elective inguinal repair: excellent outcomes. Recurrence under 3%; return to work and normal activity in 1 to 2 weeks (longer for heavy manual work). Day-case surgery is the norm.[2]
- Patients on peritoneal dialysis (CAPD). Umbilical, ventral and inguinal hernias are all more common in patients on long-term continuous ambulatory peritoneal dialysis. Hernia repair should ideally be performed after a period of haemodialysis (with the abdomen dry for at least 24 to 48 hours before surgery) and with a switch back to haemodialysis for 2 to 4 weeks post-operatively to allow mesh incorporation without the mechanical and inflammatory load of dialysate. Prophylactic mesh at the time of catheter insertion is increasingly used in high-risk patients.
- Recurrent hernias. A hernia that recurs after an anterior open mesh repair is best approached from a different anatomical plane (laparoscopic TEP/TAPP, robotic TAPP, or open preperitoneal Kugel) so that the surgeon operates in virgin territory rather than scar tissue; conversely, a hernia that recurs after a posterior (preperitoneal) repair is usually best re-repaired from the front. The overall re-recurrence rate is about 5 to 10% after a properly selected redo approach.
- Femoral hernia: outcomes depend on presentation. Elective repair carries low morbidity; emergency repair with strangulation and bowel resection carries a mortality of 5 to 15%.[2]
- Incisional hernia: recurrence is higher (10 to 20%), particularly with large defects, obesity and smoking. Mesh repair halves recurrence compared with primary suture.[4]
- Strangulated hernia with gangrenous bowel: prognosis worsens with delay; the safety-net is the recognition of strangulation and the prompt decision to operate.
The disposition is straightforward: elective symptomatic hernias are referred for outpatient repair; an irreducible hernia warrants same-day surgical admission; a strangulated hernia needs immediate resuscitation and emergency theatre.[2]
Special Populations
- Children. Congenital indirect inguinal hernia from a patent processus vaginalis. Repair is by herniotomy (high ligation of the sac at the deep ring), not mesh. Bilateral in about 10%; premature infants have a much higher incidence and a higher risk of incarceration. The contralateral side is examined routinely; some surgeons explore the contralateral side in young infants.[2]
- Elderly women. Femoral hernias are over-represented and frequently present strangulated. A high index of suspicion, low threshold for ultrasound and a low threshold for surgery are essential.[2]
- Pregnancy. Groin hernias are uncommon in pregnancy. Asymptomatic hernias are managed conservatively; symptomatic hernias are repaired electively in the second trimester or post-partum. Strangulation warrants emergency surgery at any stage.[2]
- Ascites and cirrhosis. Umbilical and incisional hernias are common in cirrhosis with ascites. Rupture of an umbilical hernia is a catastrophic event with high mortality. Repair (often with pre-operative ascites control and a TIPSS) is preferred once liver function allows.[2]
- Patients on anticoagulation. Continue anticoagulation where the indication is strong; bridge peri-operatively. Open inguinal repair is well-tolerated but inguinal haematoma is a recognised complication.[2]
Evidence, Guidelines and Regional Differences
[3] [6] [11] [10] [12]European Hernia Society / HerniaSurge guidelines (2018, updated 2023).[2][7] Key recommendations:
- Open Lichtenstein repair is recommended for primary unilateral inguinal hernia in adults; laparoscopic (TEP or TAPP) is recommended for bilateral and for recurrent hernias after a previous anterior repair.
- Watchful watching is an acceptable alternative in minimally symptomatic men, with informed discussion of the high crossover rate.
- Truss is not recommended as definitive treatment.
- Day-case surgery should be the default; mesh-based repair should be the default; tissue repairs are reserved for contaminated fields.
- Antibiotic prophylaxis is not routinely required for elective open repair in low-risk patients but may be used selectively.
- The 2023 update (Stabilini et al.) reaffirms Lichtenstein and laparoscopic repair as complementary, with decision-making guided by surgeon expertise, hernia characteristics and patient factors.[7]
Closure of abdominal wall incisions (EHS 2015, Muysoms et al.).[5] Mass closure with a continuous, slowly absorbable monofilament suture (e.g. PDS loop) at a suture-to-wound-length ratio of at least 4:1, with small bites (5 to 8 mm), reduces incisional hernia incidence. These principles — the "small-bites" technique — have become the standard for laparotomy closure.
United Kingdom (NICE). NICE recognises open mesh repair as the standard for inguinal hernia; laparoscopic repair is recommended for recurrent and bilateral hernias and for patients who prefer it and are fit for general anaesthesia. Day-case surgery is the default. USA. Open Lichtenstein and laparoscopic repair (TEP/TAPP) are both endorsed by the SAGES and Americas Hernia Society guidelines; watchful waiting is an accepted option. Europe. The HerniaSurge guidelines (EHS) are the dominant standard, with the 2023 update the current reference.[2][7]
Prevention
Because hernias arise from a combination of wall weakness and raised intra-abdominal pressure, prevention targets the modifiable contributors:[2]
- Smoking cessation — reduces chronic cough and improves collagen quality, lowering both primary incisional and recurrent hernia rates.
- Weight loss in the obese.
- Treatment of chronic cough (COPD, asthma, tuberculosis).
- Treatment of constipation (dietary fibre, hydration, laxatives).
- Treatment of bladder outflow obstruction (prostatic hyperplasia).
- Optimal surgical technique for any laparotomy — small-bites mass closure with slowly absorbable monofilament suture, prophylactic antibiotics, meticulous wound care, and consideration of prophylactic mesh for high-risk closures (obese, smokers, aortic aneurysm, midline incision in contaminated field).[5]
Exam Pearls and High-Yield Minutiae
- Inguinal hernia: ABOVE and MEDIAL to the pubic tubercle. Femoral hernia: BELOW and LATERAL. This single relationship is the most frequently examined fact in groin hernia.[2]
- Indirect: LATERAL to the inferior epigastric (through the deep ring). Direct: MEDIAL to the inferior epigastric (through Hesselbach's triangle).
- Hesselbach's triangle: rectus abdominis (medial), inguinal ligament (inferior), inferior epigastric (lateral).
- Deep ring = midpoint of the inguinal ligament. Superficial ring = above and medial to the pubic tubercle.
- Indirect inguinal hernia can enter the scrotum. Direct rarely does.
- Femoral hernia: highest strangulation risk of any hernia (up to 40% at presentation). Always repaired.
- Lichtenstein mesh repair: tension-free, open, gold standard.
- Paediatric inguinal hernia: herniotomy (high ligation of the sac). No mesh.
- Strangulated hernia = irreducible AND tender AND signs of obstruction. Emergency surgery.
- Always check hernial orifices in any unexplained small-bowel obstruction.
- Richter's hernia: anti-mesenteric border strangulates WITHOUT obstruction. Classic femoral hernia trap.
- Howship-Romberg sign: obturator hernia — inner-thigh pain radiating to the knee, relieved by hip flexion.
- Sliding hernia: caecum (right) or sigmoid (left) forms part of the wall of the sac.
- Ligaments of the floor: Poupart's (inguinal), Gimbernat's (lacunar), Cooper's (pectineal).
- Coronaria mortis: an abnormal obturator artery crosses Gimbernat's ligament — danger when incising it.
- Taxis is contraindicated in strangulation (risk of reduction en masse).
- McEvedy approach for strangulated femoral hernia; Lotheissen (trans-inguinal) approach for elective; McVay / Cooper's ligament repair for closure.
Inguinal canal boundaries — anterior to posterior
AEIOU
External oblique aponeurosis (reinforced by internal oblique in the lateral one-third)
Inguinal ligament (Poupart's) — the rolled-under lower edge of external oblique
Spermatic cord (M) / round ligament (F), ilioinguinal nerve
Deep ring (lateral, midpoint of inguinal lig.) + superficial ring (medial, above pubic tubercle)
Transversalis fascia (reinforced medially by the conjoint tendon)
The four boundaries of Hesselbach's triangle — MDIL
MDIL
Lateral border of the rectus abdominis forms the medial boundary
Direct inguinal hernia passes through this triangle
Inguinal ligament (Poupart's) is the floor of the triangle
Inferior epigastric artery is the lateral boundary
Quick self-test: a 78-year-old woman presents with small-bowel obstruction, no previous surgery, and a 2 cm tender lump below and lateral to the pubic tubercle. What is the diagnosis and the immediate management?
Diagnosis: strangulated femoral hernia (Howship-Romberg not present here, but the position below and lateral to the pubic tubercle in an elderly woman with obstruction is classical). Immediate management: NBM, nasogastric tube, intravenous fluids, analgesia, broad-spectrum antibiotics, and emergency surgery (McEvedy approach) with bowel resection if gangrenous. Do NOT attempt taxis.
References
- [2]HerniaSurge Group. International guidelines for groin hernia management. Hernia, 2018.PMID 29330835
- [3]Fitzgibbons RJ Jr, Giobbie-Hurder A, Gibbs JO, et al. Watchful waiting vs repair of inguinal hernia in minimally symptomatic men: a randomized clinical trial. JAMA, 2006.PMID 16418463
- [4]Muysoms FE, Miserez M, Berrevoet F, et al. Classification of primary and incisional abdominal wall hernias. Hernia, 2009.PMID 19495920
- [5]Muysoms FE, Antoniou SA, Bury K, et al. European Hernia Society guidelines on the closure of abdominal wall incisions. Hernia, 2015.PMID 25618025
- [6]Neumayer L, Giobbie-Hurder A, Jonasson O, et al. (VA Cooperative Studies Program 456). Open mesh versus laparoscopic mesh repair of inguinal hernia. N Engl J Med, 2004.PMID 15107485
- [7]Stabilini C, van Veenendaal N, Aasvang E, et al. Update of the international HerniaSurge guidelines for groin hernia management. BJS Open, 2023.PMID 37862616
- [8]Nyhus LM. Individualization of hernia repair: a new era. Surgery, 1993.PMID 8356511
- [9]Gilbert AI. An anatomic and functional classification for the diagnosis and treatment of inguinal hernia. Am J Surg, 1989.PMID 2919740
- [10]Ramirez OM, Ruas E, Dellon AL. "Components separation" method for closure of abdominal-wall defects: an anatomic and clinical study. Plast Reconstr Surg, 1990.PMID 2143588
- [11]EU Hernia Trialists Collaboration. Mesh compared with non-mesh methods of open groin hernia repair: systematic review of randomized controlled trials. Br J Surg, 2000.PMID 10931018
- [12]Kugel RD. The Kugel repair for groin hernias. Surg Clin North Am, 2003.PMID 14533907
- [13]Wantz GE. Giant prosthetic reinforcement of the visceral sac. Surg Gynecol Obstet, 1989.PMID 2814751