General Surgery · General Surgery
Acute Cholecystitis
Also known as Acute calculus cholecystitis · Gallbladder inflammation · Biliary inflammation · Murphy positive
Acute cholecystitis is acute inflammation of the gallbladder, 90% caused by a gallstone impacting the cystic duct. Classic: right upper quadrant pain + Murphy sign (inspiratory arrest on RUQ palpation) + fever. Ultrasound is first-line: gallbladder wall thickening, pericholecystic fluid, stones, sonographic Murphy sign. Management: early laparoscopic cholecystectomy within 72 hours (Tokyo Guidelines 2018). If unfit: percutaneous cholecystostomy. Complications: gangrene, perforation, empyema, emphysematous cholecystitis. Acalculous cholecystitis (10%): ICU patients, high mortality.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Exam tags
Red flags

Overview & Definition
Acute cholecystitis is acute inflammation of the gallbladder wall, almost always triggered by obstruction of the cystic duct. In approximately 90% of cases, a gallstone impacts in the cystic duct or Hartmann pouch, producing the syndrome of constant right upper quadrant pain, fever, and a positive Murphy sign — the recognised hallmark of acute calculous cholecystitis.[1][2]
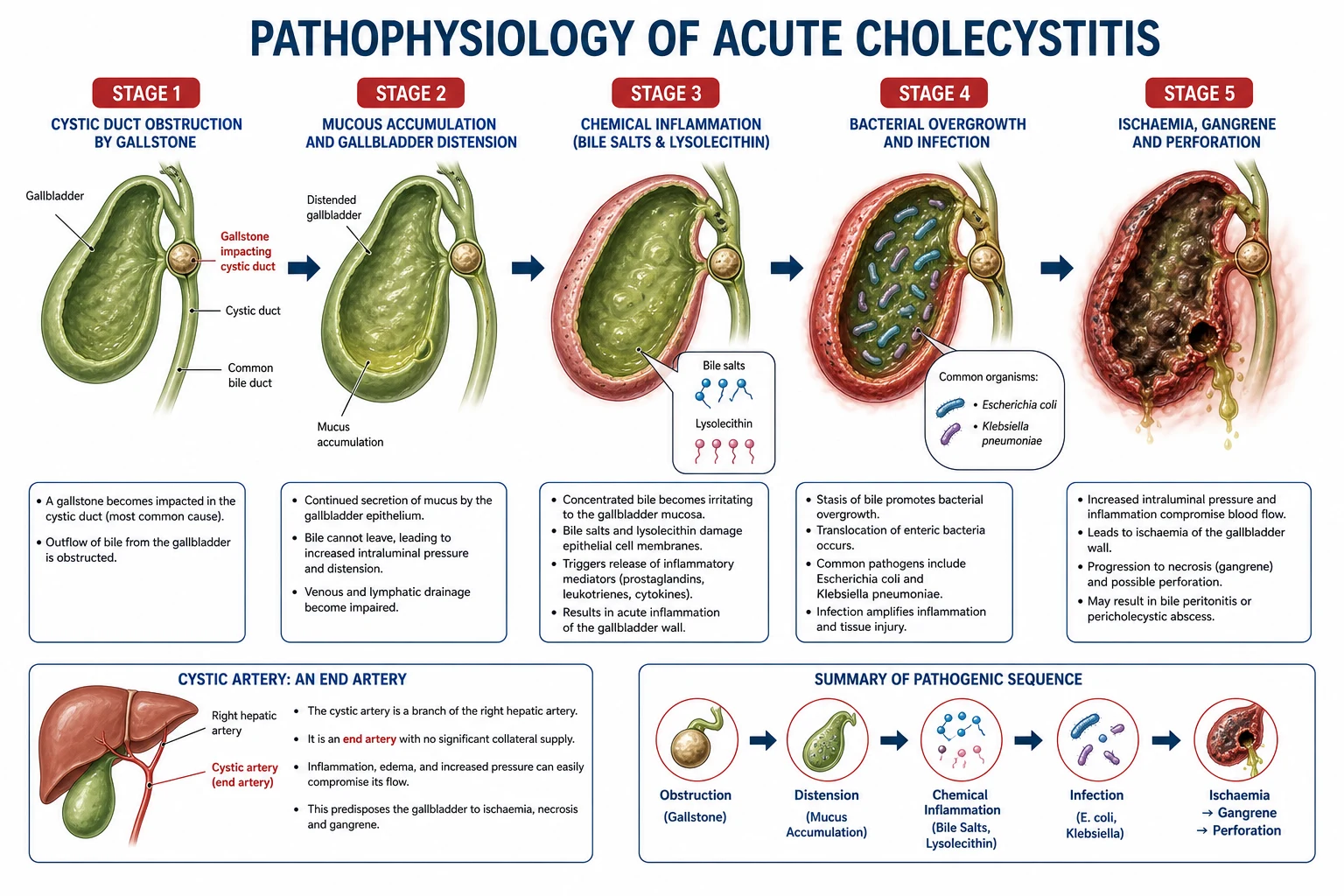
The obstructed gallbladder cannot empty, yet it continues to absorb water and secrete mucus, so it progressively distends. Stagnant bile becomes chemically toxic and then secondarily infected, the wall becomes oedematous and ischaemic, and the disease may advance from a sterile inflammatory process to suppuration, gangrene, or perforation. The clinical problem is therefore not merely "an inflamed gallbladder" but a time-dependent condition in which delay escalates the risk of gangrene and sepsis — the central justification for early surgery.[2][3]
In the remaining 10% of cases, no stone is present: this is acute acalculous cholecystitis, a disease of the critically ill (ICU sepsis, major burns, trauma, prolonged fasting, total parenteral nutrition) with a disproportionate mortality of 30 to 50%. The distinction between calculous and acalculous disease matters because the patient, the timing, and the first-line treatment differ.[2]
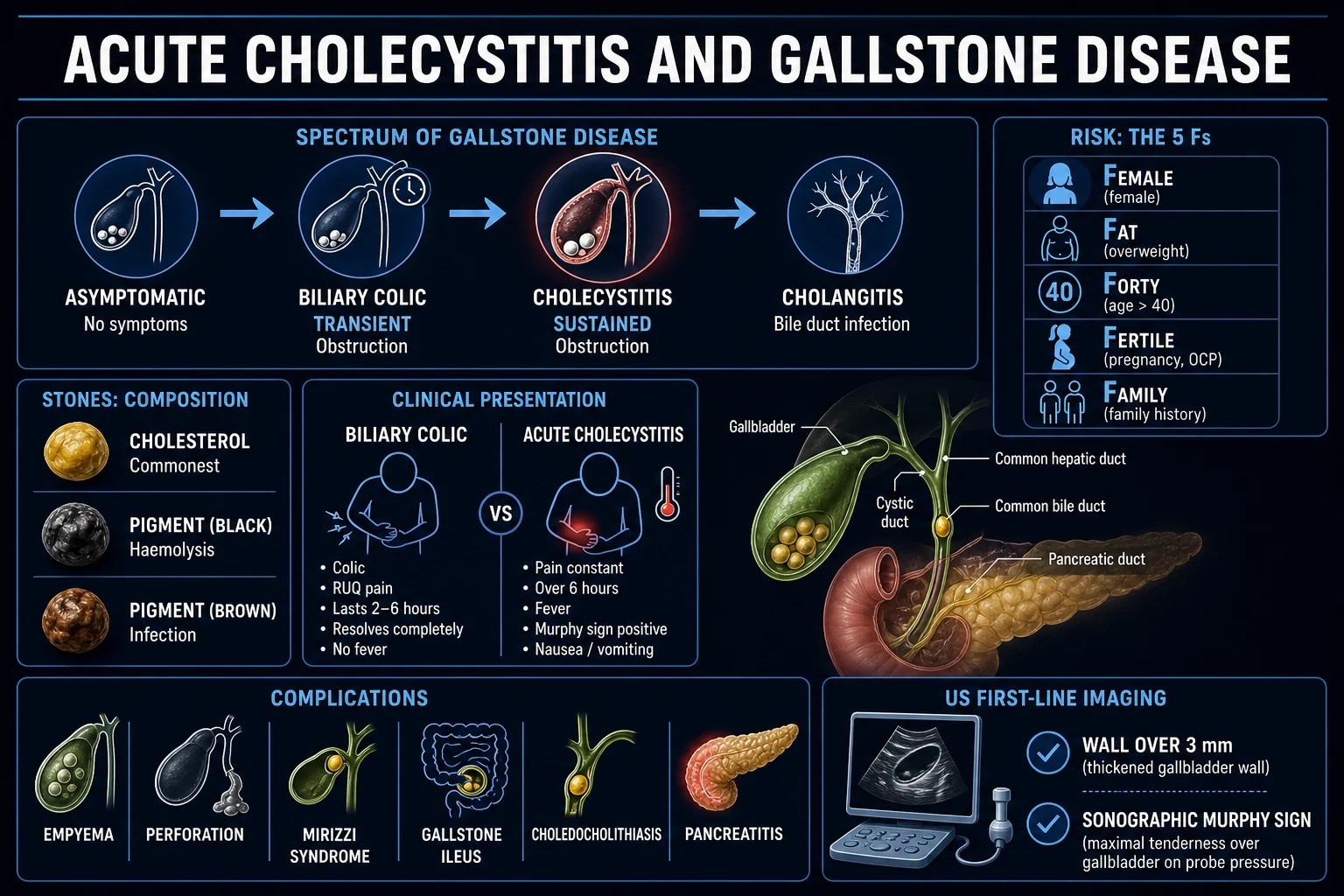
The single most important clinical distinction at the bedside is acute cholecystitis versus biliary colic. Biliary colic is transient cystic duct obstruction that resolves spontaneously within 6 hours, with no fever, no leucocytosis, and no persistent tenderness; it is managed electively. Acute cholecystitis is persistent inflammation requiring admission, antibiotics, and usually inpatient surgery.[1]
Biliary Anatomy & the Biliary Colic–Cholecystitis Boundary
A secure understanding of biliary anatomy is the foundation for both diagnosis and safe surgery. The gallbladder lies in the gallbladder fossa on the undersurface of the right liver lobe, between the right and left hepatic lobes. It is divided into the fundus (the rounded blind end projecting beyond the liver edge), the body, and the infundibulum (the tapered neck that joins the cystic duct). The Hartmann pouch is a small outpouching at the junction of the gallbladder neck and the cystic duct; it is the most common site for a stone to lodge and cause obstruction.[2]
The cystic duct is usually 2 to 4 cm long and 1 to 3 mm in diameter, and it joins the common hepatic duct to form the common bile duct (CBD). The triangle of Calot is bounded by the cystic duct, the common hepatic duct, and the inferior surface of the liver; the cystic artery runs within this triangle. Safe laparoscopic cholecystectomy demands a clear critical view of safety (CVS): the triangle of Calot is cleared so that only the cystic duct and cystic artery enter the gallbladder, and no other structures are divided until this view is achieved.[2]
The arterial supply of the gallbladder is almost exclusively from the cystic artery, a branch of the right hepatic artery in the majority of people. The cystic artery divides into anterior and posterior branches at the gallbladder wall; because the fundus is the most distal from the inflow, it is the first part to become ischaemic when intraluminal pressure rises. Venous drainage is via small cystic veins into the portal vein, and lymphatic drainage goes to the cystic lymph node near the neck of the gallbladder and then to the porta hepatis nodes. This explains why inflammation is rarely limited to the mucosa and why the disease can spread quickly to the peritoneum and adjacent liver bed.[2]
Biliary colic
transient cystic-duct obstruction
- Pain is colicky and typically resolves within **4 to 6 hours**
- No systemic inflammation: no fever, normal WCC, normal CRP
- Murphy sign is absent or non-specific
- US may show stones but **no wall thickening or pericholecystic fluid**
- Managed as day-case or elective cholecystectomy
Acute cholecystitis
persistent cystic-duct obstruction with inflammation
- Pain is constant and lasts **more than 6 hours**
- Fever, leucocytosis, and raised CRP are typical
- **Murphy sign is positive**
- US shows wall thickening greater than 3 to 4 mm, pericholecystic fluid, sonographic Murphy sign
- Requires admission, antibiotics, and usually early surgery
The distinction matters because biliary colic can be managed electively, whereas acute cholecystitis is a time-dependent disease in which delayed treatment allows progression to gangrene, perforation, or sepsis. A patient whose pain has lasted more than 6 hours, or who has fever or a positive Murphy sign, should be treated as acute cholecystitis until proven otherwise.[1][2]
Classification
Acute cholecystitis is classified by (a) the presence of a stone, (b) the severity grade using the Tokyo Guidelines 2018 (TG18), and (c) the presence of a complication. All three axes drive management.[1]
Calculous (90%)
gallstone obstruction
- Stone impacts in the **cystic duct** or Hartmann pouch
- Women aged 40 to 60 (the 5 Fs); cholesterol stones dominate
- Classic RUQ pain + **Murphy sign** + fever + leucocytosis
- Definitive treatment: **early laparoscopic cholecystectomy within 72 hours**
Acalculous (10%)
no stone; critically ill host
- ICU patients: sepsis, major burns, trauma, prolonged fasting, TPN
- Mechanism: bile stasis + gallbladder ischaemia + bacteraemia
- Diagnosis difficult (intubated, no pain history); low threshold to scan
- **Mortality 30 to 50%**; percutaneous cholecystostomy first-line
Complicated
gangrene / perforation / empyema
- **Gangrenous:** necrotic wall — the fundus ischaemic first (end artery)
- **Perforated:** localised pericholecystic abscess or free peritonitis (2 to 11%)
- **Empyema:** gallbladder filled with pus — clinically toxic
- **Emphysematous:** gas-forming organisms in the wall (diabetic, emergency)
The Tokyo Guidelines 2018 severity grading is the internationally accepted framework and is the schema examiners expect:[1]
Tokyo Guidelines 2018 — severity grading of acute cholecystitis
Acute versus chronic cholecystitis. Repeated episodes of cystic duct obstruction, or persistent low-grade inflammation, produce chronic cholecystitis — a thickened, fibrotic gallbladder wall with recurrent bouts of biliary colic, often with a contracted, shrunken gallbladder at surgery. Acute cholecystitis is the florid, single-episode inflammatory event. The two coexist: most patients who present acutely have an underlying chronic cholecystitis, and an elective cholecystectomy specimen typically shows both. Cholecystitis glandularis proliferans (Rokitansky-Aschoff sinuses) and a porcelain gallbladder (calcified wall, up to a 5 to 25% cancer risk in some series) are chronic sequelae that examiners ask about.[2]
Epidemiology & Risk Factors
Gallstones are extraordinarily common — present in roughly 10 to 15% of adults in Western populations — but most are silent. Of patients with known gallstones, around 1 to 3% per year develop biliary complications, and acute cholecystitis is the most common of these. Among patients presenting with acute cholecystitis, roughly 10 to 20% have or will develop a complication such as gangrene or perforation.[2][6]
Headline epidemiology
The classical risk-factor mnemonic for cholesterol gallstones is the 5 Fs. It is simplistic (the "Fair" component is the weakest) but examiners still expect it:[2]
The 5 Fs — gallstone risk factors
5 Fs
oestrogen increases cholesterol saturation of bile; progesterone impairs gallbladder emptying
increased hepatic cholesterol secretion into bile
cumulative cholesterol exposure and bile stasis
repeated pregnancy-induced biliary stasis
demographic association; weakest of the five
Beyond the 5 Fs, the clinically important risk factors are the non-cholesterol causes that examiners test:[2]
- Rapid weight loss and bariatric surgery — mobilises cholesterol, contracts the gallbladder against concentrated bile; prophylactic cholecystectomy is sometimes performed at bariatric surgery.
- Total parenteral nutrition (TPN) and prolonged fasting — bile stasis; a leading cause of acalculous cholecystitis in ICU.
- Ileal disease or resection (Crohn disease) and ileal bypass — loss of the enterohepatic bile-salt circulation depletes the bile-acid pool, favouring cholesterol supersaturation.
- Cirrhosis and haemolysis — pigment (black) stones; sickle cell disease, thalassaemia, hereditary spherocytosis.
- Diabetes mellitus — predisposes to emphysematous cholecystitis and gangrene via vascular disease and immunopathy.
- Drugs — oral contraceptive pill, fibrates, octreotide, cephalosporins (biliary sludge).
Other clinically relevant associations include metabolic syndrome and non-alcoholic fatty liver disease (NAFLD), which increase cholesterol secretion into bile; cholesterol-lowering drugs such as clofibrate; ceftriaxone (calcium–ceftriaxone sludge); thiazide diuretics; and erythropoietic protoporphyria. A positive family history and certain ethnic groups (for example Native American and Chilean Mapuche populations) have a markedly higher prevalence of cholesterol stones. Conversely, vitamin C, unsaturated fat, coffee, and moderate alcohol intake appear to be protective, partly by enhancing gallbladder contractility or reducing cholesterol saturation.[2]
Gallstone type matters. The two main types are cholesterol stones (most common in the West, yellow-green, faceted) and pigment stones (black, from haemolysis, or brown, associated with infection and biliary stasis). Cholesterol stones form when bile becomes supersaturated with cholesterol; pigment stones form when unconjugated bilirubin precipitates in the setting of haemolysis or bacterial deconjugation. The proportion of pigment stones is higher in Asia and Africa, and in regions with chronic Salmonella carriage or haemolytic disease. This affects the differential diagnosis: a young patient with pigment stones and jaundice should be screened for haemolysis, and a patient with recurrent cholangitis in Asia may harbour brown pigment stones in the bile ducts.[2]
India: Gallstone disease is common across all regions. Haemolytic disorders (sickle cell disease, thalassaemia) cause pigment stones (black stones) in certain populations. Vegetarian diet and rapid weight loss are additional contributors. Access to laparoscopic surgery may be limited in rural areas, so open cholecystectomy is still practised and many patients present late with complications (gangrene, empyema, gallstone ileus). Chronic Salmonella typhi carriage in the gallbladder is a recognised risk factor for gallbladder carcinoma (endemic in the Gangetic belt) and for chronic cholecystitis. Gallbladder cancer is far more common in north India than in the West, and a porcelain gallbladder in this setting warrants urgent prophylactic cholecystectomy.[6]
Pathophysiology
The pathophysiology of acute calculous cholecystitis is a predictable cascade that unfolds after cystic duct obstruction; understanding the steps explains both the symptoms and the urgency.[2]
The four-step cascade: obstruction to chemical injury to infection to ischaemia
Why constant (not colicky) pain? In biliary colic the obstructing stone dislodges, so the pain resolves within hours. In acute cholecystitis the stone stays impacted and the gallbladder wall becomes inflamed and then infected, so the pain is constant and progressive, eased only by analgesia and resolution of the inflammation.[2]
Why the right shoulder tip? Inflammation of the diaphragmatic peritoneum is referred via the phrenic nerve (C3, 4, 5) to the supraclavicular and right shoulder-tip dermatomes (Boas sign territory, T8 to T9 referred hyperaesthesia).[2]
Why does gangrene start at the fundus? The cystic artery is the sole nutrient supply and the fundus is the most distal point from the inflow, so it becomes ischaemic first ("fundus-first" gangrene) — a classic viva answer.[2]
Acalculous mechanism. In the critically ill patient the gallbladder is not emptied (no food in the gut, no cholecystokinin stimulus), bile becomes inspissated, and gallbladder-wall ischaemia from shock and microvascular disease permits bacterial translocation. The combination of stasis, ischaemia, and bacteraemia drives a fulminant inflammation without a stone.[2]
The inflammatory cascade is amplified by tumour necrosis factor-alpha (TNF-alpha), interleukin-1 (IL-1), and platelet-activating factor, which increase vascular permeability and leukocyte recruitment. As intraluminal pressure rises, venous outflow and arterial inflow are compromised; the wall becomes tense, greyish, and ultimately necrotic. Because the cystic artery is an end-artery and the fundus is its most distal territory, ischaemia begins at the fundus and progresses proximally, explaining the "fundus-first" pattern of gangrene. Once the wall necroses, perforation follows — either contained by the omentum as a pericholecystic abscess or free into the peritoneal cavity.[2]
Clinical Presentation
The classic triad is constant right upper quadrant pain, fever, and a positive Murphy sign. A careful history and a deliberate Murphy manoeuvre will identify most cases before any imaging.[1][2]
Other examination findings:[2]
- Boas sign: hyperaesthesia (increased skin sensitivity) in the right infrascapular area (referred pain via T8 to T9) — a classical but infrequently elicited sign.
- Palpable RUQ mass: a distended, inflamed, omentum-wrapped gallbladder; in a thin patient this may be a true phlegmon.
- Generalised peritonism (guarding, rigidity, rebound) indicates perforation or gangrene with spillage — a surgical emergency.
- Courvoisier's law: in a jaundiced patient, a palpable, distended gallbladder is unlikely to be due to gallstones (chronic stone disease causes fibrosis and a contracted gallbladder); suspect a malignant obstruction (pancreatic head, periampullary, cholangiocarcinoma) of a non-fibrosed duct.
Atypical presentations — deliberately examined:[2]
- Elderly and diabetic patients may report only mild discomfort, no fever, and have a normal WCC yet harbour advanced disease (autonomic neuropathy dulls pain; immune senescence blunts inflammation). Maintain a low threshold for ultrasound.
- Pregnant women can present with epigastric or right-flank pain mistaken for reflux or round-ligament pain; ultrasound is safe at any gestation.
- ICU patients (acalculous) cannot give a history; the clue is unexplained sepsis, leucocytosis, or a distended gallbladder on a routine scan.
- Post-cholecystectomy or in chronic cholecystitis the picture can be smouldering rather than florid.
Charcot triad and Reynolds pentad. A crucial distinction in the jaundiced patient is between cholecystitis and ascending cholangitis. Charcot triad consists of fever, jaundice, and right upper quadrant pain; it is highly specific for ascending cholangitis. If the patient also develops hypotension and confusion, the picture becomes Reynolds pentad, indicating suppurative cholangitis and impending sepsis. Reynolds pentad is a surgical emergency: the priority is urgent biliary drainage by ERCP plus antibiotics, not simply cholecystectomy.[3][2]
Charcot triad — fever, jaundice, RUQ pain
Charcot
bacterial infection of the biliary tree
jaundice from obstructed bile flow
biliary obstruction and ductal distension
Differential Diagnosis
Acute cholecystitis is one of several causes of right upper quadrant pain; the discriminator is the combination of persistent local tenderness with systemic inflammation.[2][6]
Biliary colic
the key exclusion
- Pain **resolves within 6 h**, no fever, no Murphy sign, normal WCC and CRP
- Self-limiting cystic duct obstruction that dislodges
- Managed as day-case or elective cholecystectomy, not admission
Acute ascending cholangitis
must-not-miss
- **Charcot triad:** fever + jaundice + RUQ pain
- **Reynolds pentad:** adds hypotension and confusion (suppurative cholangitis)
- Emergency bile-duct drainage (ERCP) — not just antibiotics
Acute pancreatitis
may coexist (gallstone pancreatitis)
- Epigastric pain radiating straight through to the back
- **Raised amylase and lipase** (lipase more specific)
- Gallstones are a common cause — check LFTs and consider urgent ERCP if cholangitis features
Perforated peptic ulcer
surgical mimic
- Sudden-onset epigastric pain, then generalised peritonitis, **rigid abdomen**
- **Free intraperitoneal air** on erect chest X-ray or CT
- Needs emergency laparoscopy or laparotomy and closure
Acute appendicitis in pregnancy
displaced by gravid uterus
- Pain may be RUQ in 2nd or 3rd trimester
- Migration of pain, anorexia, leucocytosis
- Ultrasound first, then MRI if needed; do not delay surgery
The wider differential includes several conditions that examiners deliberately place in MCQ stems:[2]
- Peptic ulcer disease / perforation: epigastric or RUQ pain, often with a history of NSAID use or Helicobacter pylori; perforation gives sudden-onset pain, rigid abdomen, and free air under the diaphragm on erect chest X-ray.
- Acute pancreatitis: epigastric pain radiating through to the back, vomiting, and elevated serum lipase (more specific than amylase). Remember that gallstones are the most common cause of pancreatitis in many populations, so a patient may have both cholecystitis and pancreatitis.
- Acute viral hepatitis: prodromal malaise, anorexia, and very high transaminases (AST and ALT in the thousands) with a modest rise in bilirubin; ultrasound shows a normal gallbladder wall.
- Acute appendicitis: in pregnancy the appendix can be displaced to the RUQ by the gravid uterus; the pain migrates and is associated with anorexia and leucocytosis.
- Myocardial infarction: inferior-wall MI can present with epigastric or RUQ discomfort, especially in elderly diabetic patients; an ECG and troponin are essential.
- Right basal pneumonia / pleurisy: pleuritic pain referred to the RUQ, fever, cough, and consolidation on chest X-ray.
- Hepatic abscess: swinging fever, tender hepatomegaly, and a hypoechoic or low-attenuation collection on imaging.
- Right renal colic: loin-to-groin pain, haematuria, and a ureteric stone on CT KUB.
- Herpes zoster: dermatal vesicular rash preceding or accompanying pain, with a normal abdominal examination.
- Fitz-Hugh-Curtis syndrome: perihepatitis from pelvic infection causing RUQ pain, often in young women with vaginal discharge.
Clinical & Bedside Assessment
The bedside assessment is built around confirming a true Murphy sign and grading the systemic response, then excluding the surgical mimics.[2]
- Vital signs and sepsis screen: temperature (low-grade fever), heart rate (tachycardia with sepsis), blood pressure (hypotension suggests Grade III disease or perforation), respiratory rate, oxygen saturation, and mental status. Hypotension with confusion is a red flag for cholangitis or perforation.
- Inspection: reduced abdominal movement with respiration on the right; visible distension only with ileus or peritonitis.
- Palpation: localise tenderness to the right upper quadrant under the costal margin; assess for guarding, rigidity, rebound (peritonism). Attempt the Murphy manoeuvre deliberately — the single most specific bedside test.
- Auscultation: bowel sounds (reduced in ileus secondary to inflammation; absent in established peritonitis).
- General examination: sclera for jaundice, stigmata of chronic liver disease, signs of chronic haemolysis (pallor, splenomegaly), and lymphadenopathy.
- Rectal and hernial-orifice examination to exclude other causes of sepsis or pain, and to complete a systematic acute abdomen assessment.
Bedside Diagnostic Algorithm
A practical approach to the patient with RUQ pain is to ask three questions, then use the answer to select investigations. [1][2]
Three-step bedside triage for suspected acute cholecystitis
This algorithm prevents two common errors: missing cholangitis by assuming every RUQ patient has cholecystitis, and delaying surgery by over-investigating a clear-cut case. It also reminds the clinician that elderly, diabetic, and pregnant patients may not show the classic triad, so a low threshold for imaging is essential.
[2]Investigations
Investigation serves three purposes: to confirm cholecystitis (local inflammation plus systemic response), to exclude mimics and duct stones, and to grade severity for operative planning.[1][2]
Laboratory tests:[2]
- Full blood count: leucocytosis (WBC greater than 10 times ten to the power of nine per litre) with neutrophilia; a WBC greater than 18,000 is itself a Tokyo Grade II marker.[1]
- CRP: elevated (greater than 10 mg per litre); rising CRP over 24 to 48 h suggests progression to gangrene or empyema.
- Liver function tests: bilirubin, ALP, and GGT may be mildly abnormal from reactive inflammation; a bilirubin greater than 50 micromol per litre, or a dilated duct on ultrasound, suggests a common bile duct stone and warrants MRCP or ERCP.[2]
- Amylase and lipase: to exclude pancreatitis (which may coexist with gallstones).
- Urea and electrolytes: baseline before surgery; renal dysfunction is a Grade III marker.
- Blood cultures: if fever, rigors, or signs of sepsis — to guide antibiotic de-escalation.
- Group and save / crossmatch: before surgery (transfusion rarely needed for elective chole but routine for acute/emergency cases).
- Coagulation screen: PT or INR before any surgical or radiological drainage; clotting derangement suggests established sepsis or obstructive jaundice (vitamin K malabsorption).
Imaging — ultrasound is first-line:[2]
Ultrasound criteria for acute cholecystitis (sensitivity about 81%, specificity near 100% when combined with Murphy sign)
Hepatobiliary scintigraphy (HIDA / cholescintigraphy): used when ultrasound is inconclusive. A technetium-99 m-labelled iminodiacetic-acid analogue is injected and excreted into bile. Non-visualisation of the gallbladder within 60 minutes indicates cystic duct obstruction; sensitivity is high (greater than 95%, even in acalculous disease where stones may be absent) and a normal HIDA effectively excludes acute cholecystitis. False-positives occur in prolonged fasting, severe hepatocellular disease, and chronic cholecystitis.[2]
CT abdomen: second-line; preferred when complications are suspected (gangrene, perforation, pericholecystic abscess, emphysematous cholecystitis with gas in the wall) or when ultrasound is technically limited (obesity, overlying bowel gas). It is more sensitive than ultrasound for perforation and for alternative diagnoses.[2]
MRCP (magnetic resonance cholangiopancreatography): the non-invasive gold standard to image the biliary tree for common bile duct stones when LFTs are abnormal or the duct is dilated on ultrasound, without exposing the patient to ERCP's pancreatitis risk.[2]
ERCP (endoscopic retrograde cholangiopancreatography): both diagnostic and therapeutic — used pre-operatively in patients with confirmed choledocholithiasis to extract the stone and perform sphincterotomy, before laparoscopic cholecystectomy.[3]
Erect chest X-ray: to exclude free air from a perforated peptic ulcer and to identify right basal pneumonia; rarely shows pneumobilia (gallstone ileus).[2]
Tokyo Guidelines 2018 — Diagnostic Criteria
TG18 formalises the diagnosis of acute cholecystitis by requiring one local sign, one systemic sign, and imaging confirmation.[1]
Tokyo Guidelines 2018 diagnostic criteria
A diagnosis is suspected when A and B are present, and confirmed when C is also present. The criteria are deliberately constructed to mirror the clinical impression that good clinicians already form: a patient with RUQ pain, fever, leucocytosis, and ultrasound evidence of gallstones plus wall thickening has acute cholecystitis. Imaging is therefore not an optional add-on; it is the third essential pillar of the diagnosis.[1][2]
Management — Resuscitation
Every patient with acute cholecystitis receives the same initial bundle — the TG18 management bundle is the framework:[3][5]
Initial management bundle (all patients, on admission)
Rationale for the bundle. NBM reduces gallbladder contraction and prepares the patient for surgery. IV crystalloid corrects the hypovolaemia and third-space losses caused by vomiting, fever, and reduced oral intake, and maintains urine output above 0.5 mL per kg per hour. Analgesia is not a luxury: NSAIDs inhibit prostaglandin synthesis and may reduce inflammation directly, while opioids treat the severe visceral pain. Antibiotics are empirical because the most common organisms are gram-negative enteric bacilli and anaerobes; therapy is narrowed once culture results are available. The choice of agent should be adjusted for local resistance, drug allergy, renal function, and severity of sepsis.[4]
Management — Definitive & Stepwise
The Tokyo Guidelines 2018 commit to a severity-directed strategy: Grade I and II disease are managed by early laparoscopic cholecystectomy; Grade III disease is stabilised first, then drained.[1][3]
Grade I and II — early laparoscopic cholecystectomy
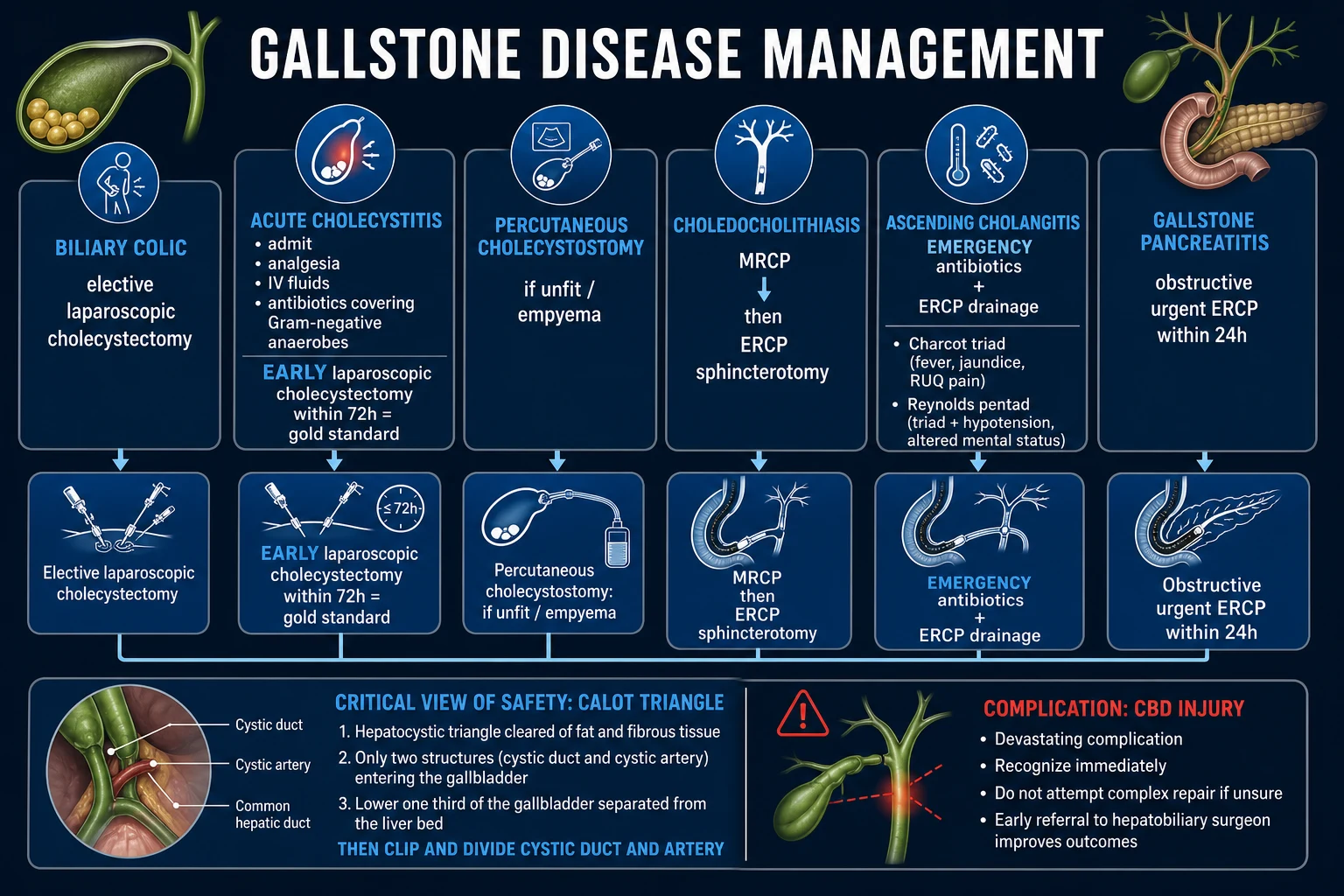
Early laparoscopic cholecystectomy within 72 hours of symptom onset is the gold standard. Multiple randomised trials and meta-analyses show that early surgery — compared with an initial conservative policy followed by delayed (interval) cholecystectomy 6 to 8 weeks later — reduces total hospital stay, complication rates, and readmission with recurrent attacks, with no increase in conversion rate or bile-duct injury.[3][6]
What if the patient presents after 72 hours? In real-world practice, many patients present late. Data from the Tokyo Guidelines and subsequent cohorts suggest that early cholecystectomy is still preferable even if the 72-hour window is exceeded, provided the patient is fit, the anatomy is favourable, and there is no severe sepsis. Delayed or interval cholecystectomy is reserved for patients who fail initial conservative management, those who are unfit for surgery, or those with severe inflammation that makes early dissection unsafe. The key principle is not to let the calendar drive the decision: fitness for surgery, severity of disease, and local expertise determine timing.[2]
Surgical technique points:[2]
- Laparoscopic approach (4 ports): camera port at or above the umbilicus, epigastric working port, and two right-sided retraction ports.
- Critical view of safety (CVS): the single most important safety step. The triangle of Calot is cleared of fat and fibrous tissue so that the cystic duct, the cystic artery, and the lower one-third of the gallbladder attached to the cystic duct are the only two structures entering the gallbladder; only then are duct and artery clipped and divided. Achieving CVS is the principal means of avoiding bile-duct injury.[2]
- Intra-operative cholangiography (IOC): selective use to confirm biliary anatomy and detect common duct stones; routine IOC is debated but reduces unrecognised bile-duct injuries.
- Conversion to open cholecystectomy in approximately 5 to 10% of acute cases — dense adhesions, unclear anatomy, uncontrolled bleeding, suspected bile-duct injury. A low threshold for conversion is itself a safety behaviour, not a failure.[2]
Subtotal cholecystectomy
When the gallbladder is densely adherent to the liver bed, the Calot triangle is frozen, or the anatomy is obscured by severe inflammation, a subtotal (fenestrating) cholecystectomy is a safe bail-out procedure. The anterior wall of the gallbladder is excised, the mucosa is curetted or ablated, and the posterior wall is left attached to the liver. The cystic duct is identified and closed if possible, or the remnant is drained. Subtotal cholecystectomy converts a high-risk total dissection into a controlled decompression, reducing the risk of bile-duct and vascular injury. The trade-off is a small risk of retained stones or a bile leak from the gallbladder remnant, but in carefully selected patients it is safer than persisting with a dangerous total cholecystectomy.[2]
High-risk surgical candidates and Grade III disease
For patients unfit for general anaesthesia, with severe comorbidity, or in Grade III disease with organ dysfunction, the source is controlled by percutaneous cholecystostomy — a pigtail catheter placed into the gallbladder lumen under ultrasound and fluoroscopic guidance, under local anaesthetic and sedation. This decompresses the septic focus, allows culture of bile, and bridges the patient to definitive care. If the patient recovers, an interval cholecystectomy (often laparoscopic) is performed after 6 to 8 weeks. Some elderly, comorbid patients are managed by cholecystostomy alone without cholecystectomy.[3][5]
Practical points for cholecystostomy. The procedure is usually performed under local anaesthesia with intravenous sedation; the transhepatic route is preferred because it reduces the risk of bile leak. The catheter is left to gravity or low-pressure suction drainage, and flushed regularly to maintain patency. Bile is sent for culture, and antibiotics are tailored to sensitivities. About 80 to 90% of patients improve clinically after drainage; complications include catheter dislodgement, leakage around the tract, bleeding, and delayed perforation. Once the patient has recovered, the catheter is clamped and removed when a trackogram confirms a mature tract, usually after 2 to 4 weeks. If stones remain in the gallbladder, interval cholecystectomy is recommended to prevent recurrence.[2]
Managing common bile duct stones
If MRCP, raised bilirubin, or a dilated duct suggests choledocholithiasis, two pathways exist:[3]
- Pre-operative ERCP with sphincterotomy and stone extraction, followed by laparoscopic cholecystectomy during the same admission — the commonest approach.
- Single-stage laparoscopic common bile duct exploration with IOC and choledochoscopy at the time of cholecystectomy — feasible in experienced centres.
Acalculous cholecystitis
In the critically ill patient the gallbladder is rarely fit for surgical resection in the acute phase. Percutaneous cholecystostomy is first-line, combined with broad-spectrum IV antibiotics covering gram-negatives, anaerobes, and enterococci. Interval cholecystectomy is considered only if the patient recovers fully; many are managed by drainage alone.[2]
Post-operative care and discharge
After laparoscopic cholecystectomy the patient is encouraged to mobilise on the day of surgery and to drink oral fluids; a planned overnight stay is usual for an acute (rather than elective) case, and same-day discharge is possible in selected fit patients. Analgesia is stepwise — regular paracetamol 1 g four times daily, with a short-acting opioid (for example oxycodone 5 mg every 4 to 6 hours) for breakthrough; NSAIDs are limited to patients without renal impairment or peptic-ulcer risk. Post-operative antibiotics are stopped within 24 hours for uncomplicated Grade I disease but continued for 4 to 7 days for gangrene, empyema, or cholangitis, per the TG18 antimicrobial guidance.[4] Thromboprophylaxis with low-molecular-weight heparin (for example enoxaparin 40 mg subcutaneously once daily) and anti-embolism stockings continues until the patient is fully mobile. Histology of the gallbladder is reviewed at the multidisciplinary meeting to exclude an incidental carcinoma. Discharge safety-net: the patient is warned to return urgently with new jaundice, persistent fever, severe abdominal pain, or bile-coloured wound drainage — the cardinal signs of a bile leak, collection, or retained stone.[2]
Managing Choledocholithiasis & Cholangitis
Choledocholithiasis is present in 8 to 15% of patients with gallstones, and a subset of patients with acute cholecystitis also have a common bile duct (CBD) stone. The risk of a CBD stone is higher when the patient is jaundiced, the CBD is dilated on ultrasound, or there is a history of gallstone pancreatitis.[2]
Ascending cholangitis is bacterial infection of an obstructed biliary tree. The classic Charcot triad is fever, jaundice, and RUQ pain; Reynolds pentad adds hypotension and confusion and indicates suppurative cholangitis. The management priorities are urgent biliary drainage and broad-spectrum antibiotics:[2]
- Resuscitation as for cholecystitis: NBM, IV fluids, IV analgesia.
- IV antibiotics covering gram-negatives and anaerobes; piperacillin-tazobactam, or a third-generation cephalosporin plus metronidazole, are commonly used, adjusted to local resistance and renal function.[4]
- Biliary drainage is the definitive step. ERCP with sphincterotomy is the first-line approach; if ERCP fails or is unavailable, percutaneous transhepatic biliary drainage (PTBD) or surgical drainage is used.
- Laparoscopic cholecystectomy should be performed once cholangitis has resolved, often during the same admission to prevent recurrence.[3]
For patients with a known CBD stone but no cholangitis, options include pre-operative ERCP followed by laparoscopic cholecystectomy, or single-stage laparoscopic CBD exploration at the time of cholecystectomy in experienced centres. The choice depends on local expertise, duct diameter, and stone burden.[2]
Specific Subtypes & Scenarios
Emphysematous cholecystitis. Gas-forming organisms (Clostridium perfringens, E coli, Klebsiella) infect the gallbladder wall; air is visible in the wall or lumen on X-ray, ultrasound, or CT. Risk factors: diabetes mellitus (around half of cases) and elderly men. Perforation and gangrene are commoner than in ordinary calculous disease, and emergency cholecystectomy (often open) with broad-spectrum antibiotics is the rule; mortality is 15 to 25%.[2]
Mirizzi syndrome. A stone impacted in the Hartmann pouch (cystic duct-gallbladder neck) externally compresses the adjacent common hepatic duct, producing obstructive jaundice despite a gallbladder aetiology. McSherry classification: Type I = external compression only; Type II = cholecysto-biliary fistula from erosion of the stone into the duct (and the further Csendes sub-typing II to V grades the size of the fistula). Diagnosis is by MRCP. Treatment is open cholecystectomy with bile-duct repair (sub-hepaticojejunostomy for large fistulae); laparoscopic dissection is hazardous and frequently converted.[2]
Gallstone ileus. A large stone (often over 2.5 cm) erodes through the gallbladder into the duodenum (cholecystoduodenal fistula), passes distally, and obstructs the terminal ileum (the narrowest point of the adult bowel). The classic Rigler triad on imaging is small-bowel obstruction + pneumobilia + an ectopic gallstone (often in the right iliac fossa). Treatment is enterolithotomy — a longitudinal enterotomy proximal to the stone to milk it out, with closure transversely; the fistula usually closes spontaneously, and cholecystectomy is deferred unless symptoms persist. Surgery is directed at the obstruction; cholecystectomy and fistula repair are reserved for patients with ongoing biliary symptoms or a persistent leak, because the inflamed gallbladder often makes one-stage repair hazardous. Mortality remains significant, especially in elderly patients with delayed diagnosis, so a high index of suspicion in a patient with small-bowel obstruction and pneumobilia is essential.[2]
Gangrenous and empyematous cholecystitis. In gangrene the wall is frankly necrotic (often at the fundus), with a high risk of perforation; at laparoscopy the gallbladder is friable and may disintegrate during dissection, requiring conversion. In empyema the lumen is filled with pus — the patient is toxic with high fever and rigors; percutaneous drainage plus antibiotics, then cholecystectomy, is safest.[2]
Xanthogranulomatous cholecystitis. A rare, locally destructive inflammatory variant that mimics gallbladder carcinoma on imaging (a thickened, nodular wall) and is often diagnosed only on histology after a difficult cholecystectomy. Awareness prevents unnecessary radical resection.[6]
Gallbladder carcinoma and porcelain gallbladder. Long-standing gallstones, especially stones greater than 3 cm, and a porcelain gallbladder (calcification of the wall) are associated with an increased risk of gallbladder adenocarcinoma. The risk reported for porcelain gallbladder has been variable, but the combination of chronic cholecystitis and wall calcification is an indication for prophylactic cholecystectomy in fit patients, particularly in regions with a high background incidence of gallbladder cancer such as north India.[2][6]
A porcelain gallbladder is detected on plain abdominal X-ray or CT as a calcified rim in the RUQ. Because the risk of malignancy is highest when the calcification is mural rather than mucosal, incidentally discovered porcelain gallbladder should be referred for cholecystectomy. If gallbladder carcinoma is found on histology, management depends on T-stage: pT1a (limited to mucosa) may need no further surgery, whereas pT1b or beyond requires radical re-resection including liver-bed excision and regional lymphadenectomy.[2]
Complications & Pitfalls
Complications of the disease:[2]
- Gangrene (around 10%): necrotic wall, often clinically silent until perforation.
- Perforation (2 to 11%): may be localised (pericholecystic abscess) or free (generalised biliary peritonitis, mortality up to 30%).
- Empyema: pus-filled gallbladder — a surgical-emergency equivalent.
- Cholecystoenteric fistula: most often into the duodenum (leading to gallstone ileus); rarely into the colon or stomach.
- Mirizzi syndrome and secondary biliary obstruction.
- Gallstone pancreatitis and ascending cholangitis when stones migrate into the common duct.
- Emphysematous cholecystitis (diabetic, gas in wall).
- Chronic cholecystitis and, in the long term, gallbladder carcinoma.
Complications of surgery:[2]
- Bile-duct injury (0.2 to 0.5%): the most feared complication. Prevented by meticulous critical view of safety dissection; recognised by post-operative bile leak, jaundice, or sepsis; managed by referral to an HPB surgeon for hepaticojejunostomy (Roux-en-Y).
- Bile leak from the cystic-duct stump or liver bed (duct of Luschka): managed by ERCP with sphincterotomy and stent to lower duct pressure.
- Bleeding from the cystic artery or liver bed.
- Conversion to open in 5 to 10% of acute cases.
- Post-cholecystectomy syndrome: recurrent biliary-type pain after cholecystitis — caused by retained stones, sphincter of Oddi dysfunction, or functional pain. It is reported in 5 to 10% of patients after cholecystectomy and can present weeks to months after surgery. The first step in evaluation is to repeat LFTs and imaging to look for retained CBD stones, bile-duct stricture, or a bile collection. If imaging is normal, endoscopic assessment of the sphincter of Oddi or functional testing may be needed. Treatment is directed at the underlying cause: ERCP for retained stones, sphincterotomy for sphincter of Oddi dysfunction, and multidisciplinary pain management for functional pain.
- Incidental gallbladder carcinoma found on histology — may need radical re-resection (liver-bed excision plus lymphadenectomy) if the tumour breaches the muscularis.
- Missing common duct stones — always check LFTs; if bilirubin is elevated, image the duct (MRCP or ERCP) before or at surgery.
- Not recognising emphysematous cholecystitis in a diabetic — gas in the wall changes the urgency and the antibiotic cover.
- Operating on acalculous cholecystitis in a critically ill patient when percutaneous drainage is safer.
- Bile-duct injury from inadequate CVS — "loss of plane" is the warning sign; convert if unsure.
- Underestimating Grade III disease — operating on a patient with organ dysfunction without prior resuscitation and drainage.
- Delaying surgery beyond 72 hours in a fit patient when early cholecystectomy is feasible and superior.
Prognosis & Disposition
- Uncomplicated acute cholecystitis treated by early laparoscopic cholecystectomy: mortality under 1%, hospital stay 2 to 4 days, return to normal activities in 1 to 2 weeks.[2]
- Elderly and diabetic patients: morbidity and mortality rise to around 10% from gangrene, perforation, and sepsis; atypical presentation drives delayed diagnosis.[2]
- Emphysematous cholecystitis: mortality 15 to 25%.
- Acalculous cholecystitis: mortality 30 to 50%, dominated by the underlying critical illness.
- Perforation with generalised peritonitis: mortality up to 30%.
- Early laparoscopic cholecystectomy within 72 hours reduces complications, total hospital stay, and readmission compared with delayed surgery — the central evidence-based message.[3][6]
Disposition: most patients are admitted under general surgery, undergo early laparoscopic cholecystectomy during the index admission, and are discharged within days. High-risk or Grade III patients go via cholecystostomy to a planned interval procedure. Discharge advice emphasises wound care, signs of bile leak or collections (jaundice, fever, pain), and a clear safety-net for return.[2]
Special Populations
- Diabetics — higher risk of emphysematous cholecystitis and gangrene; atypical presentation from autonomic neuropathy; more aggressive management and a low threshold for imaging.[2]
- Elderly — atypical and delayed presentation, higher complication rates; lower threshold for ultrasound and a higher index of suspicion for gangrene and carcinoma.[2]
- Pregnancy — acute cholecystitis is the second most common non-obstetric surgical emergency (after appendicitis). The hormonal environment of pregnancy (progesterone-mediated gallbladder hypomotility, increased cholesterol saturation) predisposes to stone formation. Conservative management risks recurrent attacks, preterm labour, and pancreatitis. Laparoscopic cholecystectomy is safe in all trimesters for acute disease when performed by an experienced surgeon; the first trimester raises concern for teratogenicity of anaesthesia and the third trimester increases technical difficulty from the gravid uterus. Open cholecystectomy is reserved for cases where laparoscopy is unsafe. Pregnant patients should receive pregnancy-appropriate antibiotics, NSAIDs are avoided (especially in the third trimester), and paracetamol and short-acting opioids are preferred. Fetal monitoring is required perioperatively.[6]
- ICU patients (acalculous cholecystitis) — diagnosis is opportunistic on a sepsis scan; percutaneous cholecystostomy is first-line; broad-spectrum antibiotics covering gram-negatives, anaerobes, and enterococci.[2]
- Children — gallstones are uncommon and usually pigment stones from haemolysis (sickle cell, spherocytosis); a haemolysis screen is mandatory. Paediatric dosing of analgesia and antibiotics is weight-based. Surgery is indicated for symptomatic or complicated disease.[2]
- Cirrhosis and portal hypertension — cholecystectomy in cirrhotic patients carries higher bleeding and infection risk; Child-Pugh class C patients have a prohibitive risk for elective surgery. In acute cholecystitis, cholecystostomy is often preferred as a bridge, and surgery is undertaken only after optimisation of coagulopathy, ascites, and encephalopathy.[2]
- Anticoagulated patients — anticoagulation must be managed perioperatively. Warfarin is usually bridged or stopped depending on thromboembolic risk; direct oral anticoagulants are omitted on the day of surgery. The risk of bleeding must be balanced against the urgency of source control.[2]
- Immunocompromised — atypical organisms (including fungi and cytomegalovirus) and an aggressive course; early imaging and a low threshold for drainage. Corticosteroid use may mask fever and tenderness, so a high index of suspicion is required.[2]
Evidence, Guidelines & Regional Differences
Tokyo Guidelines 2018 (TG18). The internationally adopted consensus, published as a series in the Journal of Hepato-Biliary-Pancreatic Sciences. The four papers cited here cover the diagnostic criteria and severity grading,[1] the initial-management flowchart,[3] the antimicrobial-therapy recommendations,[4] and the management bundles.[5] TG18 commit to early laparoscopic cholecystectomy for Grade I and II disease and to percutaneous cholecystostomy plus delayed surgery for Grade III.[1][3]
Early versus delayed laparoscopic cholecystectomy. Randomised trials and meta-analyses consistently favour early surgery (within 72 hours) over an initial conservative policy followed by interval cholecystectomy, with shorter total hospital stay, fewer readmissions with recurrent disease, and no increase in conversion or bile-duct-injury rates. The Cochrane review of early versus delayed laparoscopic cholecystectomy for biliary colic and related syndromes is the most cited summary of the evidence.[6]
Percutaneous cholecystostomy versus early surgery. In high-risk surgical candidates and in Grade III disease, cholecystostomy is a safe bridge; whether elderly, comorbid patients are best served by drainage alone or by subsequent cholecystectomy remains a topic of trial debate, and the 2024 EClinicalMedicine review highlights this as a continuing grey area.[6]
Antibiotic duration. TG18 antimicrobial guidance tailors duration to severity — short courses (4 to 7 days) for uncomplicated disease after cholecystectomy, longer courses for gangrene, empyema, or cholangitis. Routine prophylactic antibiotics at induction are standard.[4]
ACR Appropriateness Criteria. For suspected acute cholecystitis, right upper quadrant ultrasound is the most appropriate initial study. CT is reserved for suspected complications or non-diagnostic ultrasound, and MRCP or HIDA scintigraphy is used when duct stones or cystic duct obstruction remain uncertain.[2]
NICE / UK guidance. NICE recommends laparoscopic cholecystectomy as the definitive treatment for acute cholecystitis, ideally during the initial admission and within one week of diagnosis; percutaneous cholecystostomy is reserved for patients unfit for surgery. First-line empirical antibiotic regimens include co-amoxiclav or a cephalosporin plus metronidazole, aligned with TG18 antimicrobial advice.[2]
Landmark evidence. Early versus delayed laparoscopic cholecystectomy was clarified by randomised trials and meta-analyses: early surgery within 72 hours of symptom onset reduces total hospital stay, readmissions, and complication rates without increasing conversion or bile-duct injury. The Cochrane review summarising this evidence remains a standard reference. The CHOCOLATE trial and subsequent observational data in high-risk patients suggest that even in elderly or comorbid populations, early cholecystectomy often outperforms percutaneous cholecystostomy, although cholecystostomy remains an essential bridge for unstable patients.[6]
UK (NICE / AUGIS): early laparoscopic cholecystectomy within one week of diagnosis for acute cholecystitis; cholecystostomy reserved for those unfit for surgery. Co-amoxiclav or a cephalosporin plus metronidazole as first-line empirical cover.[3] US (SAGES, Tokyo-consistent practice): early laparoscopic cholecystectomy within 72 hours of presentation for Grade I and II; critical view of safety is the benchmark for safe dissection; selective IOC.[2] ANZ: aligned with TG18; cholecystostomy increasingly used in the elderly comorbid population, with registry data informing outcomes.[6]
India: pigment stones from haemolysis and gallbladder carcinoma (north India, especially the Gangetic belt) shift the differential; a porcelain gallbladder or a long-standing stone over 3 cm warrants prophylactic cholecystectomy. Laparoscopic surgery is standard in cities but open cholecystectomy persists in rural centres, and late presentation with gangrene or gallstone ileus is commoner. Chronic Salmonella typhi carriage in the gallbladder is endemic and is a recognised co-carcinogen for gallbladder cancer. Antibiotic resistance patterns (extended-spectrum beta-lactamase producers) increasingly drive empirical choice toward piperacillin-tazobactam in severe disease.[6]
Exam Pearls
When an examiner asks about acute cholecystitis, they are usually testing one of four discriminations: cholecystitis versus biliary colic, cholecystitis versus cholangitis, the timing of surgery, and the safe approach to a difficult gallbladder. Frame every answer around these axes, and use the Tokyo Guidelines severity grade to explain why the same disease may be treated by early laparoscopic cholecystectomy in one patient and by cholecystostomy in another.[1][2]
- Murphy sign = inspiratory arrest on RUQ palpation; reproducible only on the right; high specificity for acute cholecystitis.[1]
- 90% of acute cholecystitis is calculous. The other 10% (acalculous) occurs in ICU patients and carries high mortality.[2]
- Ultrasound first-line: wall thickening greater than 3 to 4 mm, pericholecystic fluid, stones, sonographic Murphy sign; CBD greater than 6 mm suggests choledocholithiasis.[2]
- HIDA = non-filling of the gallbladder = cystic duct obstruction; high sensitivity, useful when ultrasound is equivocal.[2]
- Early laparoscopic cholecystectomy within 72 hours is the gold standard for Grade I and II disease (Tokyo Guidelines 2018).[1][3]
- Courvoisier's law: palpable gallbladder plus jaundice is not due to gallstones — think malignancy.[2]
- Mirizzi syndrome: stone in Hartmann pouch compresses the common hepatic duct, producing jaundice; Type I compression, Type II onwards cholecysto-biliary fistula.[2]
- Emphysematous cholecystitis: diabetic or elderly, gas in the gallbladder wall, emergency surgery, 15 to 25% mortality.[2]
- Gallstone ileus: small-bowel obstruction plus pneumobilia plus ectopic gallstone (Rigler triad); treat by enterolithotomy.[2]
- Critical view of safety prevents bile-duct injury in laparoscopic cholecystectomy — the most-tested surgical safety concept.[2]
- Charcot triad (fever plus jaundice plus RUQ pain) and Reynolds pentad (adds hypotension and confusion) = ascending cholangitis, not cholecystitis — needs urgent ERCP drainage.[2]
- Tokyo Grade II marker = WBC greater than 18,000, RUQ mass, symptom duration over 72 h, or marked inflammation (gangrene, abscess, empyema, emphysematous).[1]
- Tokyo Grade III = organ dysfunction (cardiovascular, neurological, respiratory, renal, hepatic, haematological) — ICU plus cholecystostomy, not immediate surgery.[1]
- Subtotal cholecystectomy is the safe bail-out when the Calot triangle is frozen or the gallbladder is stuck to the liver bed.[2]
- Gas in the gallbladder wall in a diabetic patient = emphysematous cholecystitis: emergency surgery and broad-spectrum antibiotics.[2]
- Acalculous cholecystitis in the ICU: look for unexplained sepsis and a distended gallbladder; percutaneous cholecystostomy first-line.[2]
Self-test: which ultrasound finding most strongly supports acute cholecystitis over biliary colic?
A combined picture of wall thickening (greater than 3 to 4 mm), pericholecystic fluid, gallstones, and a positive sonographic Murphy sign. Pericholecystic fluid and wall thickening reflect inflammation; stones alone (without wall change) indicate uncomplicated gallstone disease. A sonographic Murphy sign (maximal tenderness as the probe compresses the gallbladder) has a high specificity for acute cholecystitis.[2]
References
- [1]Yokoe M, Hata J, Takada T, Strasberg SM, et al. Tokyo Guidelines 2018: diagnostic criteria and severity grading of acute cholecystitis (with videos). Journal of Hepato-Biliary-Pancreatic Sciences, 2018.PMID 29032636
- [2]Pisano M, Allievi N, Gurusamy K, et al. 2020 World Society of Emergency Surgery updated guidelines for the diagnosis and treatment of acute calculus cholecystitis. World Journal of Emergency Surgery, 2020.PMID 33153472
- [3]Miura F, Okamoto K, Takada T, Strasberg SM, et al. Tokyo Guidelines 2018: initial management of acute biliary infection and flowchart for acute cholangitis. Journal of Hepato-Biliary-Pancreatic Sciences, 2018.PMID 28941329
- [4]Gomi H, Solomkin JS, Takada T, et al. Tokyo Guidelines 2018: antimicrobial therapy for acute cholangitis and cholecystitis. Journal of Hepato-Biliary-Pancreatic Sciences, 2018.PMID 29090866
- [5]Mayumi T, Okamoto K, Takada T, et al. Tokyo Guidelines 2018: management bundles for acute cholangitis and cholecystitis. Journal of Hepato-Biliary-Pancreatic Sciences, 2018.PMID 29090868
- [6]Fugazzola P, Coccolini F, Tomasoni M, et al. Clinical update on acute cholecystitis and biliary pancreatitis: between certainties and grey areas. EClinicalMedicine, 2024.PMID 39469538