General Surgery · General Surgery
Anorectal Disorders
Also known as Haemorrhoids · Anal fissure · Fistula-in-ano · Perianal abscess · Pilonidal sinus · Anal cancer · Rectal prolapse · Pruritus ani
Anorectal disorders span haemorrhoids (Grade I–IV; rubber band ligation first-line for II–III), anal fissure (posterior midline 90%; topical GTN 0.4% or diltiazem 2%; chronic = lateral internal sphincterotomy), anorectal abscess/fistula (cryptoglandular origin; Goodsall rule: anterior = straight, posterior = curved to midline; fistulotomy for low, seton/LIFT/advancement flap for high), pilonidal sinus (natal cleft, hirsute young males; excision ± Limberg flap), anal cancer (HPV 16/18; Nigro protocol 5-FU + mitomycin C chemoradiation), rectal prolapse (elderly women; rectopexy/Delorme/Altemeier) and pruritus ani.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Exam tags
Red flags
Overview & Definition
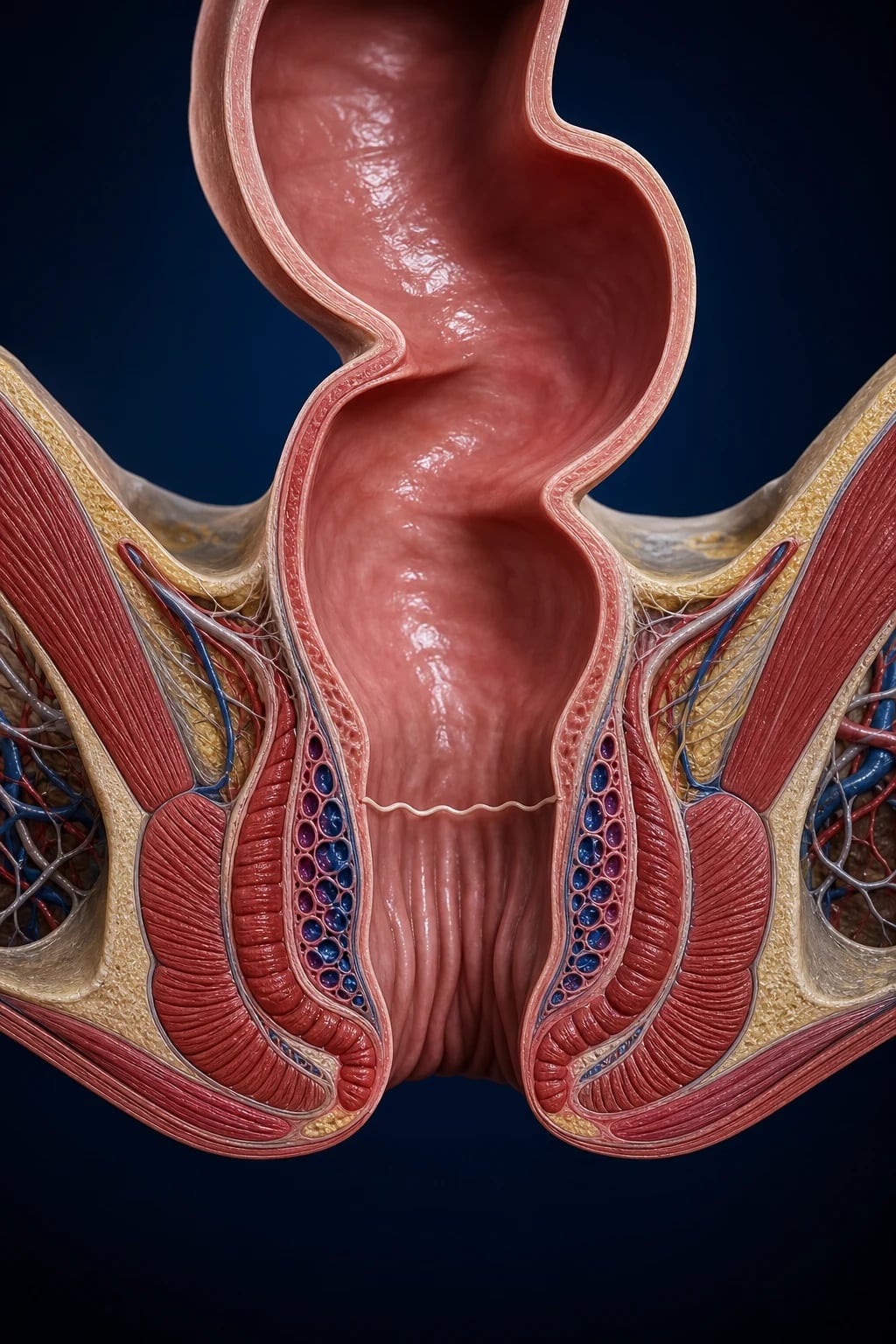
The anorectal region is a complex anatomical junction where the hindgut-derived columnar epithelium of the rectum transitions to the ectoderm-derived squamous epithelium of the perianal skin at the dentate (pectinate) line. This line — embryologically the union of the hindgut with the proctodeum — is the single most important landmark in anorectal medicine: structures above it are visceral (autonomic, painless) and drain to inferior mesenteric nodes, while those below are somatic (somatic pain, voluntary control) and drain to superficial inguinal nodes. Almost every clinical feature of an anorectal condition — pain versus painlessness, lymphatic spread, line of surgical excision — is dictated by its relationship to the dentate line.[3]
Anorectal disorders are a clinically heterogeneous group of seven conditions sharing this anatomical region. They present to the surgeon in three common ways: with pain (fissure, abscess, thrombosed external haemorrhoid), with bleeding (haemorrhoids, fissure, cancer), or with a lump/discharge (prolapse, fistula, pilonidal sinus, cancer). This topic integrates all seven — haemorrhoids, anal fissure, anorectal abscess and fistula-in-ano, pilonidal sinus, anal cancer, rectal prolapse, and pruritus ani — so that a candidate can answer any examiner question across MCQ, SAQ, viva, and long-case formats.[3]
Classification
Anorectal conditions are best classified by the primary disease process, because each condition has its own management ladder. The components below contrast the seven conditions and their key subtypes.[3]
Haemorrhoids
engorged anal cushions above dentate line
- **Grade I** — bleed, do not prolapse
- **Grade II** — prolapse on straining, reduce spontaneously
- **Grade III** — prolapse, require manual reduction
- **Grade IV** — permanently prolapsed, irreducible
- External haemorrhoids: below dentate line; thrombosed = painful perianal lump
Anal fissure
posterior midline tear (90%)
- **Acute** (under 6 weeks): superficial linear tear
- **Chronic** (over 6 weeks): sentinel pile, hypertrophied anal papilla, exposed internal sphincter fibres
- **Atypical** (multiple, lateral, painless): Crohn, HIV, syphilis, TB, anal cancer
- Internal sphincter hypertonia is the unifying mechanism
Anorectal abscess
by anatomical space
- **Perianal 60%** — between internal sphincter and anoderm
- **Ischiorectal 20%** — spreads into ischiorectal fossa
- **Intersphincteric 5%** — between internal and external sphincter
- **Supralevator 2.5%** — above levator ani (pararectal)
- **Submucosal** — under anorectal mucosa
Fistula-in-ano
cryptoglandular track
- **Simple (low)** — below puborectalis; fistulotomy safe
- **Complex (high)** — involves more than 30% of external sphincter; seton/LIFT/advancement flap
- **Goodsall rule** guides internal opening site
- Park classification: intersphincteric (commonest 70%), transsphincteric (25%), suprasphincteric, extrasphincteric
Pilonidal sinus
natal cleft hair sinus
- Acute pilonidal abscess vs chronic sinus
- **Primary midline pits** with secondary lateral openings
- **Sinus tracts** with hair and granulation tissue
- Recurrent disease common after primary closure
Anal cancer
squamous cell (HPV 16/18)
- Squamous cell carcinoma 85% (above dentate = cloacogenic, below = basaloid/SCC)
- Adenocarcinoma 10–15% (lower rectum, rare anal gland)
- TNM staging drives therapy
- **Nigro chemoradiation** is first-line curative
Rectal prolapse
elderly women
- **Partial (mucosal)** — mimics prolapsing haemorrhoids
- **Complete (full-thickness)** — rectal intussusception through anus
- **Internal intussusception** — rectal wall telescopes without exteriorisation
- Surgery choice driven by fitness and approach (abdominal vs perineal)
Epidemiology & Risk Factors
Headline numbers across the seven conditions
Haemorrhoids affect roughly 4–5% of the general population at any time, with a lifetime prevalence approaching 75% for some degree of symptom. Peak age is 45–65 years. Risk factors are anything that raises intra-abdominal venous pressure: chronic constipation, prolonged straining at stool, pregnancy, chronic cough, heavy lifting, obesity, and a low-fibre Western diet. Portal hypertension does not cause haemorrhoids (it causes anorectal varices — a separate, painless entity that should not be banded).[3]
Anal fissure is most common in young adults aged 20–40 with M ≈ F. Constipation with passage of a hard stool is the classic precipitant; pregnancy, inflammatory bowel disease (Crohn in particular), and prior anorectal surgery are additional risks. Multiple or atypical fissures raise Crohn disease, HIV, syphilis, TB or malignancy.[6]
Anorectal abscess and fistula predominantly affect males (2:1) aged 30–50. Cryptoglandular obstruction is the cause in 90%; the remainder are associated with Crohn disease, immunosuppression, malignancy, tuberculosis, actinomycosis, or prior anorectal surgery. Diabetes, HIV, and inflammatory bowel disease all predispose to complex, recurrent, or atypical disease. 30–50% of drained abscesses go on to develop a fistula, particularly with inadequate drainage.[8]
Pilonidal sinus disease is a disease of young (15–30 years), hirsute, often obese males in sedentary occupations — drivers, barbers, desk workers, military recruits. Family history, deep natal cleft, and poor personal hygiene all raise risk. Females are less often affected and when affected tend to have less hirsute disease.[15]
Anal cancer is uncommon (annual incidence ≈ 1–2 per 100,000) but rising, driven by HPV. Risk factors are HPV 16/18 infection, HIV/AIDS (relative risk ~30, especially with CD4 under 200), receptive anal intercourse, high lifetime number of sexual partners, smoking, solid-organ transplant immunosuppression, and cervical/vulvar/vaginal intraepithelial neoplasia.[12]
Rectal prolapse is overwhelmingly a disease of elderly women (F:M 6:1) — typically frail, multiparous, with chronic constipation, pelvic floor weakness, and often dementia or neurological comorbidity. Complete rectal prolapse in a child, by contrast, suggests cystic fibrosis, malnutrition, or chronic diarrhoea.[14]
Pruritus ani is common (1–5% population), M>F, peak 40–60s. Idiopathic in 25–75% of cases; secondary causes include anorectal disease (fissure, fistula, haemorrhoids, faecal soiling), infections (Candida, dermatophytes, pinworm, STIs), dermatoses (psoriasis, eczema, lichen sclerosus), and contact dermatitis from over-the-counter creams or wet wipes.[3]
India-specific points. Squatting defecation posture and prolonged straining contribute to perianal disease; pilonidal sinus is seen in young sedentary men and is also associated with long-distance train and truck travel. Tuberculosis is an important cause of atypical perianal fistula in endemic regions — caseating granulomata on biopsy, often coexisting with pulmonary or intestinal TB, demands antitubercular therapy before any surgical intervention. Late presentation of rectal prolapse in rural elderly women is common. Chigurupalli's excision with primary closure is an Indian modification of pilonidal surgery. In HIV-endemic populations, atypical perianal ulcers, complex fistulas and anal cancer are over-represented and biopsy is mandatory.[8]
Pathophysiology
Haemorrhoids
Haemorrhoids are engorged, displaced anal vascular cushions (not varicose veins) — three normal structures (left lateral, right posterior, right anterior) that contribute 15–20% of resting anal pressure and aid continence. When the supporting connective tissue (Treitz muscle and Parks's ligament) degenerates with age, straining and chronic constipation push the cushions distally. Venous outflow obstruction, arteriovenous communication dilation, and prolapse follow. Bleeding is bright red (arterial, from the arteriovenous communications). Above the dentate line they are painless; thrombosis of an external component below the dentate line is intensely painful.[3]
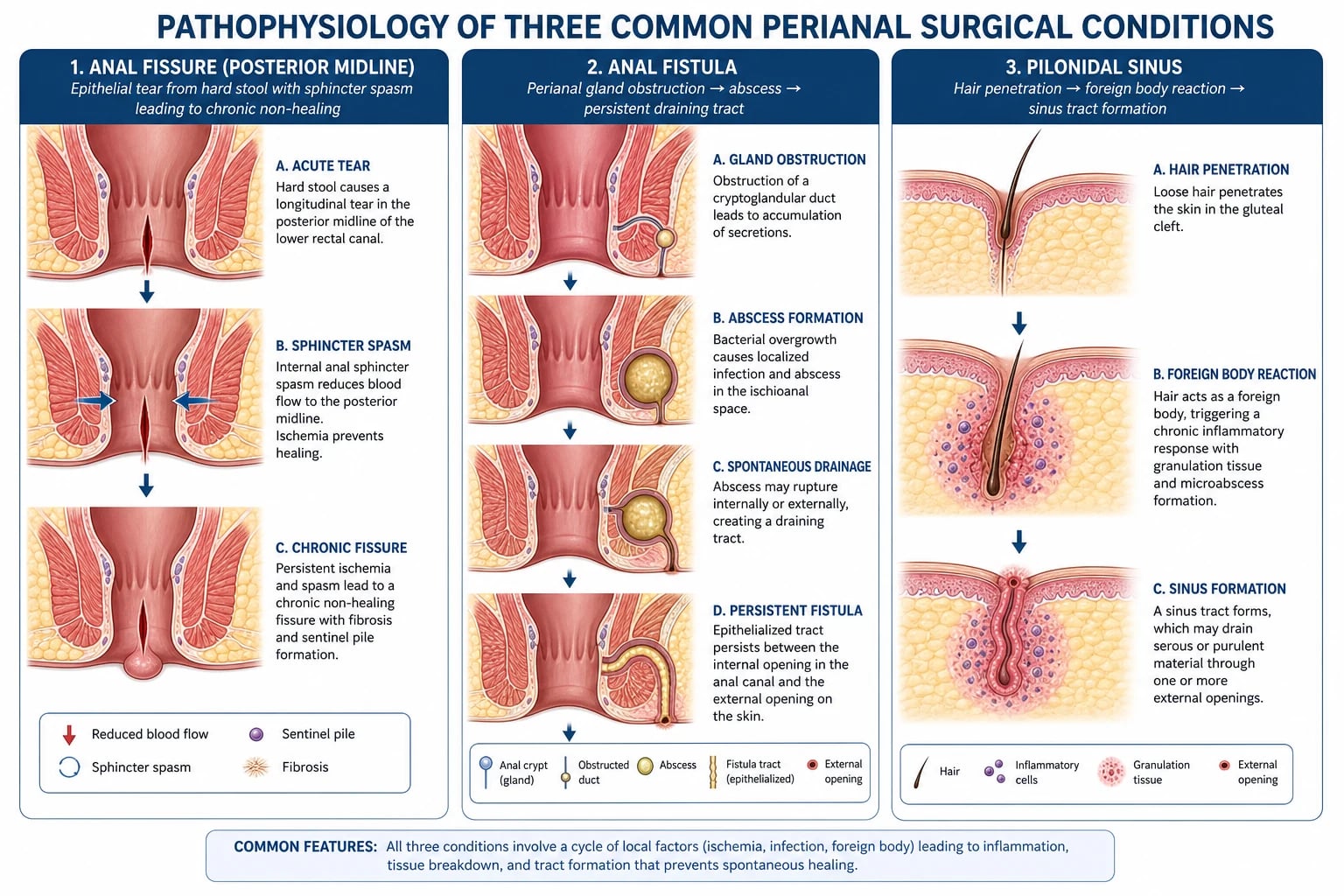
Anal fissure — the ischaemia cycle
A hard stool tears the sensitive squamous epithelium of the anoderm at the posterior midline (90%) — a watershed area with the poorest perfusion of the anal canal. The tear exposes the underlying internal anal sphincter, which reacts with sustained hypertonia. Maximum resting pressure rises, and the already-poor posterior midline perfusion falls further (the inferior rectal artery's posterior branches are anatomically deficient in 85%). The result is local ischaemia: the fissure cannot heal, hypertonia deepens, and the cycle self-perpetuates. Every effective fissure treatment — GTN, diltiazem, botulinum toxin, lateral internal sphincterotomy — works by lowering internal sphincter pressure and restoring perfusion.[4][6] This is why a "tight sphincter" is both the cause and the therapeutic target.
Anorectal abscess and fistula — the cryptoglandular theory
The anal glands of Hermann and Desfosses lie in the crypts of Morgagni at the dentate line, with ducts draining into the anal canal. Obstruction of a duct (typically by faecal material or oedema) → stasis → infection → pus accumulates in the gland and spreads along the path of least resistance into the perianal, ischiorectal, intersphincteric, or supralevator spaces. The abscess either points through the skin (spontaneous rupture) or is drained surgically; in 30–50% of cases a persistent epithelialised track remains between the internal opening at the diseased crypt and the external opening at the skin — this is a fistula-in-ano. The track does not heal because it is continuously bathed in faecal organisms. The Goodsall rule describes the typical course of these tracks.[8]
Pilonidal sinus — hair as a foreign body
The Bascom theory is now widely accepted: shed hair from the back of the head or the natal cleft itself is drawn by the suction effect of the deep natal cleft (especially during sitting/rising) into the midline pits, which are stretched hair follicles or skin defects. Hair acts as a foreign body → granulomatous inflammatory response → sinus with chronic discharge and recurrent abscess. The midline pits are the source; lateral openings are secondary. The condition is intensely linked to hirsute individuals with a deep natal cleft and friction from sedentary work.[15]
Anal cancer — HPV-driven carcinogenesis
Anal squamous cell carcinoma is etiologically linked to high-risk HPV (16 in ~75%, 18 in ~10%). The E6 and E7 oncoproteins inactivate p53 and Rb, permitting clonal expansion of dysplastic cells through anal intraepithelial neoplasia (AIN) to invasive carcinoma. Immunosuppression (HIV, transplant) impairs HPV clearance, accelerating this cascade. Most SCCs arise in the anal canal (transformation zone at the dentate line); lower-third tumours behave like skin SCC. The principal lymphatic spread is to inguinal nodes for tumours below the dentate line, and to inferior mesenteric and internal iliac nodes for tumours above.[12]
Rectal prolapse — intussusception
Complete (full-thickness) rectal prolapse is a true intussusception of the rectum through the anal canal. Predisposing factors are pelvic floor weakness (multiparity, chronic straining), a deep pouch of Douglas, redundant sigmoid, weak anal sphincters, and neurological disease. Constant straining telescopes the rectal wall downward; eventually it exteriorises through the anus, with progressive denervation of the external sphincter and faecal incontinence. Mucosal (partial) prolapse, by contrast, is radial rather than circumferential and is the pathophysiological cousin of prolapsing haemorrhoids.[14]
Pruritus ani
A final common pathway of perianal itch arising from cutaneous nerve endings: idiopathic (subclinical faecal soiling, anxiety) or secondary to local disease (fissure, fistula, haemorrhoids causing discharge), infection (Candida in moist or diabetic skin, dermatophytes, pinworm especially nocturnal in children), dermatoses (psoriasis, lichen sclerosus, atopic eczema), and contact/irritant dermatitis (over-washing, scented soaps, baby wipes, topical anaesthetics). The itch–scratch–lichenification cycle perpetuates and thickens the skin.[3]
Clinical Presentation
Haemorrhoids present with painless bright-red bleeding (on toilet paper, dripping into the pan), prolapse (the patient describes "something coming down" that may or may not reduce), and mucus discharge with pruritus. Grade IV prolapse is irreducible and may strangulate (severe pain, purple oedematous mass). External haemorrhoids below the dentate line are usually asymptomatic until they thrombose, producing an acutely tender, firm, bluish perianal lump.[3]
Anal fissure presents with the triad of severe sharp pain on defecation, bright-red bleeding on toilet paper, and constipation. The pain is characteristically described as "like passing glass" and may last for hours, causing the patient to dread defecation — the resulting avoidance worsens constipation, harder stool, and deeper tearing in a vicious cycle. A sentinel pile (skin tag at the distal end of a chronic fissure) and hypertrophied anal papilla (at the proximal end, above the dentate line) are stigmata of chronicity. Atypical presentations — painless fissure, lateral or multiple fissures, non-healing ulcer — demand search for Crohn, HIV, syphilis, TB, or cancer.[6]
Anorectal abscess presents with severe, throbbing perianal pain, a tender swelling, fever, and malaise. The pain is continuous (unlike fissure), worse on sitting or walking, and may prevent digital rectal examination. Ischiorectal abscesses are larger, less acutely tender initially, and can present with systemic upset. Supralevator abscesses may produce minimal external signs and present with deep pelvic pain, fever, and urinary symptoms. Diabetic or immunocompromised patients can deteriorate rapidly — crepitus, rapidly spreading erythema, and systemic sepsis herald Fournier gangrene (necrotising fasciitis).[8]
Fistula-in-ano presents with intermittent or continuous discharge of pus, blood, or faeculent material from a perianal opening, recurrent perianal pain when the opening temporarily occludes, and recurrent abscess. The opening is visible as a small red papule or pit, often with surrounding skin excoriation.[8]
Pilonidal sinus presents in a young hirsute male with acute abscess (painful, fluctuant swelling in the natal cleft, fever) or as a chronic sinus (one or more midline pits with recurrent discharge of pus, sometimes extruding hair). Recurrence is the rule without definitive surgery.[15]
Anal cancer presents with bleeding (often attributed to haemorrhoids), perianal pain, an anal mass, pruritus, or a change in bowel habit. A substantial minority present with enlarged inguinal lymph nodes from metastatic spread. The diagnosis is often delayed because symptoms are attributed to benign disease — any non-healing ulcer or atypical mass must be biopsied.[12]
Rectal prolapse presents with a mass protruding through the anus on straining that initially reduces spontaneously and later requires manual reduction. Associated symptoms: mucus discharge, faecal soiling, and faecal incontinence (sphincter denervation from chronic stretching). The prolapse is concentric, circumferential, and shows concentric mucosal folds (vs the radial folds of prolapsing haemorrhoids).[14]
Pruritus ani is perianal itch, classically worse at night, often with skin excoriation, lichenification, and secondary infection from chronic scratching. A focused history of cleansing products, topical agents, diabetes, sexual exposure, and bowel pattern is essential.[3]
Differential Diagnosis
Differential diagnosis of common anorectal presentations
The key discriminator for haemorrhoids versus fissure is pain: haemorrhoids bleed painlessly (unless thrombosed); fissures cause severe pain on defecation followed by a small amount of blood. For pruritus ani, exclude Candida, dermatophyte infection, pinworm, lichen sclerosus, and perianal Crohn; the latter two change management entirely.[6]
Clinical & Bedside Assessment
Examination is performed in the left lateral (Sims) or knee–chest (jack-knife) position with a chaperone and good lighting. The steps are inspect, palpate (PR), proctoscopy/sigmoidoscopy.[3]
Inspection — gently separate the buttocks. Look for:
- Posterior midline linear tear (anal fissure, 90%). Chronic fissure shows a sentinel pile (skin tag at the anal verge, distal end of the fissure) and may show exposed white internal sphincter fibres at its base.
- External opening of fistula (a small red papule or pit, often with discharge and surrounding excoriation). Apply the Goodsall rule.
- Thrombosed external haemorrhoid — a firm, tender, bluish lump at the anal verge.
- Pilonidal pits in the midline of the natal cleft, sometimes extruding hair.
- Prolapse — ask the patient to strain; complete rectal prolapse shows concentric mucosal folds, unlike the radial folds of prolapsing haemorrhoids.
- Anal ulcer or mass — atypical position or non-healing: biopsy.[12]
Goodsall rule (Goodsall–Miles, 1900): draw an imaginary transverse line through the centre of the anus.[8]
- External opening anterior to the line → the internal opening lies on a straight (radial) line directly to the anal canal at the corresponding clock position.
- External opening posterior to the line → the track is curved and opens into the posterior midline of the anal canal (6 o'clock).
- Exception: an anterior external opening more than 3 cm from the anal verge usually follows the posterior (curved) rule.
Palpation / PR exam — assess sphincter tone (hypertonic in chronic fissure), palpate for an indurated fistula track, a rectal mass, prostate, or a high-riding abscess. Defer PR if examination is too painful in acute fissure — examination under anaesthesia (EUA) is the safer route. A tender, boggy, fluctuant mass indicates an abscess needing drainage.[8]
Proctoscopy/sigmoidoscopy — directly visualise internal haemorrhoids (above the dentate line), the internal opening of a fistula, fissure, or tumour; exclude proximal rectal pathology.[3]
Investigations
Most anorectal conditions are clinical diagnoses confirmed at the bedside or under anaesthesia. Investigations are reserved for atypical, complex, or malignant presentations.[8]
- Proctoscopy / rigid sigmoidoscopy: first-line for haemorrhoids, fissure, internal opening of fistula; also excludes rectal tumour or proctitis. Perform gently in fissure or under anaesthesia.
- Endoanal ultrasound (EAUS): maps the fistula track and the extent of sphincter involvement; essential before surgery for any complex or recurrent fistula and to look for occult sphincter defects.
- MRI pelvis: the gold standard for complex, recurrent, or Crohn-related fistulas — defines secondary tracks, supralevator extension, and abscess cavities that EUA/EAUS may miss.
- Examination under anaesthesia (EUA): for painful conditions (acute fissure), for abscess drainage, and for definitive fistula mapping (with dye injection, hydrogen peroxide, or probe).
- Biopsy: any atypical, multiple, or non-healing ulcer or fissure (exclude anal cancer, AIN, Crohn, TB, HSV, syphilis). Pilonidal sinus biopsy in long-standing disease to exclude rare squamous carcinoma arising in chronic sinus ("Marjolin").
- FBC, CRP, blood glucose, HIV serology: in abscess with systemic sepsis or atypical/complex disease; diabetes and HIV must be excluded.
- Colonoscopy: if Crohn disease is suspected (multiple fissures, complex fistula, diarrhoea), or in patients over 45 with new bleeding to exclude colorectal cancer.[3]
Management — Resuscitation
Most anorectal conditions are not resuscitation emergencies. The two time-critical scenarios are anorectal sepsis and strangulated/torsed entities.[8]
For abscess with systemic features: admit, IV fluids, IV analgesia, IV antibiotics (co-amoxiclav 1.2 g IV TDS or metronidazole 500 mg IV TDS + cephalosporin), correct electrolytes and glucose, and take the patient to theatre for incision and drainage — antibiotics alone will not cure an abscess.[8]
For strangulated Grade IV haemorrhoid or acute thrombosed external haemorrhoid (within 72 hours of onset): urgent assessment; excision under local anaesthesia may be appropriate for thrombosed external haemorrhoid.[3]
Management — Definitive & Stepwise

Haemorrhoids
Management is dictated by grade and symptom severity. Always start with lifestyle (high-fibre diet 25–30 g/day, adequate fluids 2 L/day, avoid straining, bulk-forming laxatives such as ispaghula husk, sitz baths).[1][3]
[1] [2] [3]Rubber band ligation (RBL) technique
The MacRae meta-analyses established RBL as the most efficacious office procedure for Grade II–III disease, with comparable efficacy to surgical haemorrhoidectomy but far less pain — RBL is therefore first-line for Grade II–III haemorrhoids.[1][2]
Anal fissure
Treat acute fissure (under 6 weeks) conservatively first; escalate only if chronic or non-healing. The therapeutic principle is lowering internal sphincter pressure to restore perfusion.[4][5][6]
[4] [5] [6]Chronic fissure (over 6 weeks, or failed 6–8 weeks of topical therapy, with sentinel pile and exposed sphincter fibres):[7]
- Lateral internal sphincterotomy (LIS) — the gold standard. Through a small lateral (3 or 9 o'clock) incision, the lower one-third of the internal anal sphincter is divided (open or closed technique). Relieves hypertonia permanently. Heals 90–95%. Risk of incontinence to flatus ~5% (gas, occasionally liquid stool). Avoid LIS in Crohn disease, elderly with weak sphincters, or those with prior sphincter injury.[7]
- Fissurectomy + Botox — alternative in patients in whom sphincterotomy is contraindicated (Crohn, weak sphincter, primiparous women).[7]
- Advancement flap — for non-healing fissure after LIS or in atypical fissure with low resting pressure.
Anorectal abscess
Abscess management sequence
Cruciate incision and drainage (I&D) under general anaesthesia is the definitive treatment of anorectal abscess.[8] Antibiotics alone do not cure an abscess. Reserve antibiotics for: cellulitis extending beyond the abscess, immunocompromise, diabetes, valvular heart disease, or systemic sepsis — and never as a substitute for drainage.
Fistula-in-ano
The Goodsall rule guides surgical planning. The strategy is dictated by the amount of sphincter involved: low fistulas (subcutaneous, low intersphincteric, low transsphincteric) can be laid open without compromising continence; high fistulas must be managed by sphincter-sparing techniques.[8]
Fistula management — by height
The LIFT (ligation of intersphincteric fistula tract) procedure, first described by Rojanasakul, has become a workhorse sphincter-sparing option for transsphincteric fistulas, with success rates of 70–95% and minimal incontinence.[8][9][10]
Pilonidal sinus
[15] [16]The Cochrane review of pilonidal wound closure demonstrates that off-midline closure (Karydakis, Bascom, Limberg flap) is superior to midline closure in both healing time and recurrence — the natal cleft is best obliterated.[16] The systematic review by Wiinblad confirms that no single technique is universally superior, but flap-based off-midline reconstructions dominate for recurrent disease.[15] Lifelong depilation of the natal cleft reduces recurrence after any procedure.
Anal cancer
Squamous cell carcinoma of the anal canal is treated first-line with the Nigro protocol — concurrent chemoradiation. Radical surgery (abdominoperineal resection, APR) is reserved for local failure after chemoradiation or for patients who cannot tolerate chemoradiation. Diagnosis requires examination under anaesthesia with biopsy. Staging is by pelvic MRI, inguinal node assessment, and CT chest/abdomen/pelvis.[12]
[11] [12]The Nigro protocol (first described 1974) revolutionised anal cancer treatment, transforming it from a surgical disease treated by APR to a radiocurable disease treated by chemoradiation with sphincter preservation in 70–80%.[11] The ACT II randomised trial confirmed mitomycin C-based chemoradiation as standard, and showed no benefit to maintenance chemotherapy.[12] Colostomy-free survival at 5 years exceeds 70%, and overall survival approaches 75%. APR is reserved for local failure (persistent or recurrent disease after chemoradiation).[13]
Rectal prolapse
Surgical strategy is dictated by fitness for abdominal surgery and by continence status. The two routes are abdominal (for fit patients, lower recurrence) and perineal (for frail patients, lower morbidity).[14]
Rectal prolapse operations
The Cochrane review found no clear winner between abdominal and perineal approaches on aggregate, but abdominal rectopexy has the lowest recurrence and is preferred for fit patients; perineal procedures are reserved for the frail and elderly.[14]
Pruritus ani
A stepped approach: (1) exclude and treat any cause (Candida — topical clotrimazole 1% BD; dermatophyte — terbinafine 1% OD; pinworm — mebendazole 100 mg PO single dose repeated at 2 weeks; lichen sclerosus — ultra-potent topical steroid clobetasol 0.05% OD short course; perianal Crohn — treat underlying disease); (2) eliminate irritants — stop scented soaps, wet wipes, over-the-counter anaesthetic creams, excessive wiping (use water or moist cotton wool); (3) perianal hygiene — gentle washing with water and patting dry, dry with hairdryer on cool setting, cotton underwear; (4) symptom relief — topical hydrocortisone 1% for short course only (chronic steroid thins skin), oral antihistamine at night (hydroxyzine 25 mg) for sedation and itch cycle interruption; (5) intradermal methylene blue for refractory idiopathic pruritus ani (chemical denervation of perianal skin nerve endings — specialist centre).[3]
Specific Subtypes & Scenarios
Quick-fire scenarios — hide and self-test
- HIV patient with non-healing anal ulcer — biopsy for AIN/SCC; anal cancer is AIDS-defining.[12]
- Painless bright-red bleeding in a 50-year-old — exclude colorectal cancer by colonoscopy before attributing to haemorrhoids.
- Multiple atypical fissures in a young man — HIV test, syphilis serology, swab for HSV, biopsy.
- Complex recurrent fistula — MRI pelvis, EUA, consider Crohn (colonoscopy + biopsy), anti-TNF if confirmed.
- Acute thrombosed external haemorrhoid under 72 h — excision under local anaesthesia; over 72 h — conservative (warm baths, analgesia, stool softener).
- Diabetic with perianal sepsis — admit, IV antibiotics, urgent drainage, watch for Fournier gangrene.
- Strangulated Grade IV haemorrhoid — urgent excisional haemorrhoidectomy within 72 h (or conservative with later elective surgery).
- Pregnant with fissure — diltiazem 2% (avoid GTN — hypotension); avoid Botox and LIS; defer surgery post-partum.
- Elderly frail woman with complete rectal prolapse — perineal Delorme or Altemeier, not abdominal.
- HIV patient with non-healing anal ulcer — biopsy for AIN/SCC; anal cancer is AIDS-defining.
- Child with rectal prolapse — sweat chloride test for cystic fibrosis; usually managed by reduction, manual pressure, treating constipation.
Perianal Crohn disease deserves special attention. Fistulas and fissures in Crohn may be the presenting feature of intestinal disease. The principles: avoid sphincterotomy (high incontinence risk), preserve sphincter with loose setons, treat the underlying bowel disease (azathioprine, anti-TNF — infliximab 5 mg/kg at weeks 0, 2, 6, then 8-weekly; adalimumab 160 mg then 80 mg, then 40 mg every other week). Infliximab can close perianal Crohn fistulas in 50–70%. Surgery is for drainage of sepsis and seton placement, not cure.[8]
Hidradenitis suppurativa is an important mimic of complex fistula-in-ano and pilonidal sinus — affects axilla, groin, buttocks, perineum; chronic recurrent sinuses and scars; managed by dermatology and wide local excision rather than fistula surgery.[8]
HIV-related perianal disease spans the full spectrum: anal intraepithelial neoplasia (AIN), SCC, atypical ulceration (HSV, syphilis, CMV), large condylomata (HPV), and complex fistulas. Biopsy is mandatory for any chronic lesion; the threshold for EUA and biopsy in HIV patients with perianal disease is low.[12]
Complications & Pitfalls
Disease-related complications:[3]
- Untreated abscess → spontaneous rupture, recurrent abscess, fistula formation, septicaemia, Fournier gangrene (in diabetic/immunosuppressed), anal stenosis from chronic fibrosis.
- Strangulated Grade IV haemorrhoid → thrombosis, ulceration, gangrene.
- Chronic fissure → sentinel pile, hypertrophied papilla, anal stenosis from chronic spasm.
- Untreated anal cancer → inguinal and pelvic node metastasis, obstruction, fistulation.
- Chronic pilonidal sinus → squamous cell carcinoma (Marjolin ulcer, rare), chronic recurrent sepsis, sinus extension into the sacrum.
- Complete rectal prolapse → faecal incontinence (sphincter denervation), rectal ulceration, bleeding, incarceration.
Procedure-related complications:[3]
- Rubber band ligation: severe pain (band too low — remove immediately), secondary haemorrhage 7–10 days post-op, vasovagal, rare pelvic sepsis (report any fever/dysuria after banding).
- Haemorrhoidectomy: post-op pain (significant — main driver of stapled/THD adoption), urinary retention, anal stenosis (avoid excising more than the three primary cushions; preserve anoderm bridges), incontinence (injudicious sphincter division), recurrence.
- Lateral internal sphincterotomy: flatus incontinence ~5%, rare solid-stool incontinence; recurrence if insufficient division.
- Fistulotomy of a high fistula: incontinence (the cardinal sin — never divide more than 30% of the external sphincter in one stage).
- Seton: pain, drainage, cutting seton → incontinence.
- Pilonidal excision: wound infection, dehiscence (especially midline closure), recurrence 5–50% depending on technique.
- Chemoradiation for anal cancer: perianal skin desquamation, diarrhoea, cytopenias (mitomycin causes haemolytic–uraemic syndrome rarely), late anal stenosis, vaginal stenosis in women, small-bowel obstruction.
Pitfalls to actively avoid:[3]
- Misattributing bleeding to haemorrhoids without examining — the classic error that delays anal and rectal cancer diagnosis.
- Not biopsying a non-healing or atypical ulcer/fissure — missing anal cancer, AIN, or perianal Crohn.
- Fistulotomising a high fistula — dividing too much sphincter → incontinence. Always map with EUA + EAUS/MRI first; if in doubt, seton.
- Treating abscess with antibiotics alone — drains must be made; antibiotics are adjuncts only.
- Missing diabetes or immunosuppression in a septic perianal presentation — risk of catastrophic necrotising infection.
- Performing lateral sphincterotomy in Crohn disease — high risk of non-healing and incontinence.
- Midline closure after pilonidal excision — higher recurrence than off-midline.
Prognosis & Disposition
Outcomes at a glance
Acute anal fissure: 50–70% heal on topical GTN or diltiazem; recurrence 15–40% over 5 years. Chronic fissure heals in 90–95% after lateral sphincterotomy, with 5% minor incontinence.[6][7]
Anorectal abscess: drain; 30–50% develop a fistula requiring definitive surgery. Diabetic/immunocompromised patients need admission and aggressive management.[8]
Fistula-in-ano (low): 70–90% cure with fistulotomy. High/complex fistula: lower cure rates; LIFT, advancement flap, and seton give 60–95% healing; recurrence 10–30% per procedure.[8][9][10]
Pilonidal sinus: recurrence 10–50% after excision; lowest with off-midline flap reconstruction. Lifelong depilation reduces recurrence.[15][16]
Anal cancer (SCC): with Nigro chemoradiation, complete response in 80–90%, 5-year overall survival ~75%, colostomy-free survival 70–80%. Prognosis is stage-dependent — T1N0 5-year survival 90%, node-positive 50–60%, distant metastatic 20%. HIV does not by itself worsen outcome provided CD4 is maintained.[12][13]
Rectal prolapse: recurrence 5–15% (lowest after abdominal rectopexy); faecal incontinence improves in ~50% but not all. Perineal procedures have higher recurrence but acceptable for the frail.[14]
Pruritus ani: idiopathic 80% improve with hygiene measures; secondary resolves with treatment of the underlying cause; chronic lichenified cases may be refractory.[3]
Special Populations
- Pregnancy: haemorrhoids and fissures are common (constipation, venous engorgement, progesterone slowing gut). Conservative management first. Diltiazem 2% is preferred over GTN (hypotension concern). Defer Botox and LIS to post-partum. Most fissures and haemorrhoids improve after delivery.[6]
- Paediatrics: rectal prolapse in a child requires sweat chloride test for cystic fibrosis (the can't-miss diagnosis); also consider malnutrition, chronic diarrhoea, pertussis. Paediatric fissure is usually managed conservatively. Pilonidal sinus is rare before puberty.
- Elderly: rectal prolapse (perineal Delorme/Altemeier preferred for frail); faecal incontinence frequently coexists; avoid lateral sphincterotomy in weak sphincters; exclude colorectal cancer in any new bleeding.
- Crohn disease: perianal involvement is common and disabling. Never perform sphincterotomy. Use loose setons, anti-TNF, and treat underlying disease. Refer to a specialist IBD unit.
- HIV/AIDS: perianal SCC risk is greatly increased; AIN screening by anoscopy and biopsy is essential; biopsy all chronic ulcers; refer to a colorectal surgeon with HIV expertise.
- Immunosuppressed / transplant: high-risk for atypical infections (HSV, CMV, fungal, TB) and anal cancer; low threshold for biopsy.
- Anticoagulated: do not band or operate without reversing or bridging; injection sclerotherapy is safer than RBL for bleeding haemorrhoids in this group.
- Diabetic: perianal sepsis can be catastrophic — admit, urgent drainage, IV antibiotics, aggressive glucose control, and watch for Fournier gangrene.
Evidence, Guidelines & Regional Differences
Indian context: high burden of TB-related perianal fistula (caseating granulomata on biopsy — give anti-tubercular therapy before any surgery); cost constraints favour RBL and open Milligan–Morgan haemorrhoidectomy over stapled/THD; squatting defecation may worsen perianal disease. HPV vaccination uptake is low and anal cancer is under-recognised; HIV coinfection is an increasing driver. Tropical fistulas (amoebic, filarial, actinomycotic) must be considered in atypical presentations.[8]
Exam Pearls
Goodsall rule: APC
APC
external opening **anterior** to a transverse line through the anus → **straight (radial) track** to internal opening at the corresponding clock position
external opening **posterior** to that line → **curved track** opening into the **posterior midline** (6 o'clock)
draw the **transverse anal line** to apply the rule. **Exception**: anterior openings **more than 3 cm** from the verge behave as posterior (curved)
Anal fissure triad: PIE
PIE
**severe sharp pain** on defecation, lasting hours — unlike painless haemorrhoids
small bright-red blood on toilet paper (Iron in stool/TP) — never massive
**constipation** (avoidance) → harder stool → worse fissure (vicious cycle)
- Anal fissure: 90% posterior midline. Multiple or atypical = Crohn, HIV, syphilis, TB, cancer — biopsy.
- Goodsall: anterior fistula = straight track; posterior = curved to posterior midline.
- Lateral internal sphincterotomy — divide the lower one-third of the internal sphincter at 3 or 9 o'clock; gold standard for chronic fissure (90–95% heal, 5% flatus incontinence).
- Fistulotomy for LOW fistula; seton/LIFT for HIGH fistula. Never divide more than 30% of external sphincter in one stage.
- RBL is first-line for Grade II–III haemorrhoids (MacRae meta-analysis).[1][2] Never band below the dentate line (severe pain).
- Haemorrhoid grades: I (bleed only), II (prolapse, reduce spontaneously), III (prolapse, manual reduction), IV (irreducible).
- Nigro protocol = 5-FU + mitomycin C + radiotherapy — first-line curative for anal SCC; APR is salvage only.[11][12]
- ACT II: mitomycin C is non-inferior to cisplatin; maintenance chemotherapy adds nothing.[12]
- Pilonidal sinus: natal cleft, hirsute young males, hair foreign body; off-midline closure (Limberg/Karydakis) superior to midline.[15][16]
- LIFT (Rojanasakul) — sphincter-sparing option for transsphincteric fistula; 70–95% success.[8][10]
- Rectal prolapse: elderly women, 6:1. Rectopexy (abdominal, fit) vs Delorme/Altemeier (perineal, frail).[14]
- Sentinel pile = skin tag at distal end of chronic fissure (anal verge); hypertrophied anal papilla = at proximal end (above dentate line).
- GTN 0.4% ointment BD for 6–8 weeks — heals ~50%; headache is the limiting side effect; diltiazem 2% is the headache-free alternative.[4][5]
- Abscess always needs drainage; antibiotics alone do not cure. Always culture pus.
- Pain on defecation + bright blood = fissure; painless bleeding = haemorrhoids/cancer.
- Rectal prolapse = concentric circumferential folds; Grade IV haemorrhoids = radial folds.
- Biopsy any non-healing or atypical ulcer/fissure — exclude cancer, Crohn, TB.
- Pinworm — nocturnal perianal pruritus in children; mebendazole 100 mg PO stat, repeat at 2 weeks.
References
- [1]MacRae HM, McLeod RS. Comparison of hemorrhoidal treatment modalities. A meta-analysis. Dis Colon Rectum, 1995.PMID 7607026
- [2]MacRae HM, McLeod RS. Comparison of hemorrhoidal treatments: a meta-analysis. Dis Colon Rectum, 1997.PMID 9030078
- [3]Arezzo A, Podzemny V, Pescatori M. Surgical management of hemorrhoids. State of the art. Ann Ital Chir, 2011.PMID 21682110
- [4]Lund JN, Scholefield JH. Follow-up of patients with chronic anal fissure treated with topical glyceryl trinitrate. Lancet, 1998.PMID 9853449
- [5]Jonas M, Lund JN, Scholefield JH. Topical 0.2% glyceryl trinitrate ointment for anal fissures: long-term efficacy in routine clinical practice. Colorectal Dis, 2002.PMID 12780574
- [6]Nelson RL, Thomas K, Morgan J, Jones A. Non surgical therapy for anal fissure. Cochrane Database Syst Rev, 2012.PMID 22336789
- [7]Nelson RL, Manuel D, Gumienny C, et al. Efficacy of Fissurectomy and Botox for Chronic Anal Fissure. Dis Colon Rectum, 2016.PMID 27050610
- [8]Alasari S, Kim NK. Overview of anal fistula and systematic review of ligation of the intersphincteric fistula tract (LIFT). Tech Coloproctol, 2014.PMID 23893217
- [9]Zirak-Schmidt S, Perdawood SK. Management of anal fistula by ligation of the intersphincteric fistula tract — a systematic review. Colorectal Dis, 2014.PMID 25441733
- [10]Lange EO, Shubeck SS, Tejirian T, et al. Ligation of intersphincteric fistula tract: a sphincter-sparing option for complex fistula-in-ano. J Surg Res, 2016.PMID 26394877
- [11]Nigro ND, Vaitkevicius VK, Considine B Jr. Combined therapy for cancer of the anal canal: a preliminary report. Dis Colon Rectum, 1974.PMID 4830803
- [12]James RD, Glynne-Jones R, Meadows HM, et al. Mitomycin or cisplatin chemoradiation with or without maintenance chemotherapy for treatment of squamous-cell carcinoma of the anus (ACT II): a randomised, phase 3, open-label, 2 × 2 factorial trial. Lancet Oncol, 2013.PMID 23578724
- [13]Glynne-Jones R, Kadalayil L, Meadows HM, et al. Tumour- and treatment-related colostomy rates following mitomycin C or cisplatin chemoradiation with or without maintenance chemotherapy for treatment of squamous-cell carcinoma of the anus (ACT II). Eur J Cancer, 2014.PMID 24827136
- [14]Tou S, Brown SR, Malik AI, Nelson RL. Surgery for complete (full-thickness) rectal prolapse in adults. Cochrane Database Syst Rev, 2015.PMID 26599079
- [15]Wiinblad IM, Ulrichsen J, Nerup N, et al. Outcome after surgical treatment for chronic pilonidal sinus disease: a systematic review of common surgical techniques. Dis Colon Rectum, 2025.PMID 39982788
- [16]Cai Z, Zhao Z, Yang X, et al. Midline and off-midline wound closure methods after surgical treatment for pilonidal sinus. Cochrane Database Syst Rev, 2024.PMID 38226663