General Surgery · General Surgery
Breast Cancer
Also known as Carcinoma of the breast · Breast carcinoma · Mammary carcinoma · Ductal carcinoma · Paget disease of nipple
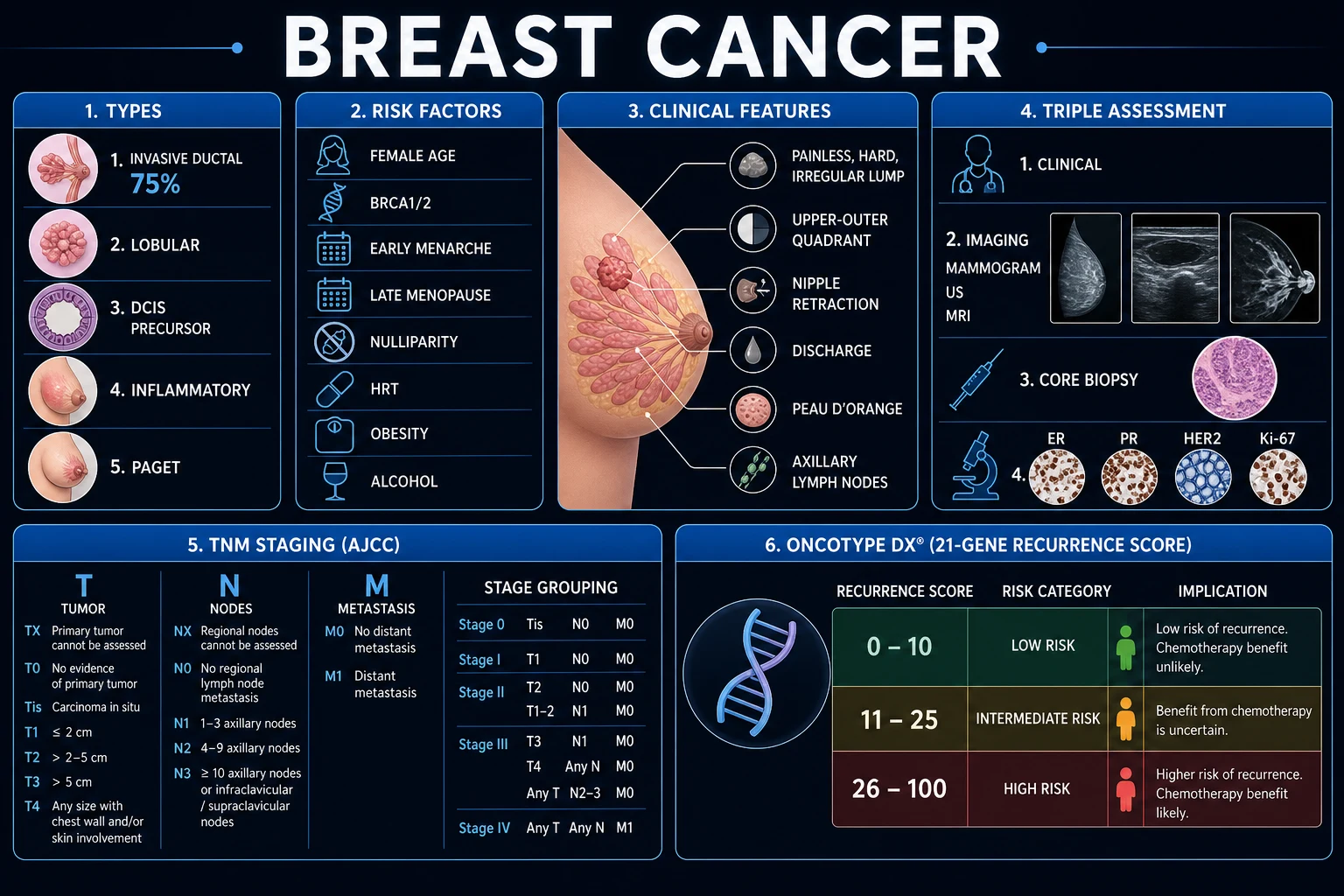
Breast cancer is the most common cancer in women worldwide (about 24% of all female cancers, lifetime risk roughly 1 in 8). Classic presentation: painless, hard, irregular, fixed breast lump. Diagnosis via triple assessment (clinical + imaging + biopsy, about 98% accurate). Molecular subtypes drive treatment: ER/PR+ (endocrine therapy), HER2+ (trastuzumab), triple-negative (chemotherapy). Surgery: wide local excision + radiotherapy (breast-conserving) or mastectomy. Sentinel lymph node biopsy for axillary staging. Commonest metastasis: bone (about 70%). BRCA1/2 mutations in about 5 to 10%.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Exam tags
Red flags

Overview & Definition
Breast cancer is a malignant neoplasm arising from the epithelial lining of the breast ducts or lobules. It is the most frequently diagnosed cancer in women worldwide, accounting for roughly a quarter of all female cancers, and is the second leading cause of cancer death in women after lung cancer. One in eight women in developed countries will develop breast cancer in her lifetime, reflecting the convergence of hormonal exposure, reproductive patterns, increasing longevity and screening activity.[3]
The mature breast is a modified sweat gland composed of 15 to 20 lobes, each subdivided into 20 to 40 lobules that contain the milk-producing acini. Each lobe drains through a branching ductal tree that converges on a lactiferous duct opening at the nipple. The ducts and lobules are the two anatomical sites of origin that define the two great histogenetic families of breast cancer — ductal (the great majority) and lobular. Cancers most often arise in the upper outer quadrant, which contains a disproportionate share of glandular tissue; this single quadrant accounts for about 40% of tumours. The breast's rich lymphatic network drains principally to the axillary nodes (levels I to III), then to the supraclavicular and internal mammary chains — and the axillary nodal status remains one of the most powerful prognostic indicators in the disease.[3]
The clinical importance of breast cancer at MBBS level is that it is common, screenable, and treatable when caught early, yet lethal when neglected. Almost every exam question — MCQ, SAQ, viva or long case — turns on five discriminating facts: the triple assessment, the TNM stage, the molecular subtype (ER/PR/HER2), the sentinel lymph node biopsy, and the endocrine-therapy-by-menopausal-status rule. This topic is built so that any one of these can be answered from first principles.[3]
Classification
Breast cancer is classified along three independent axes — anatomical extent (in situ versus invasive), histological type (ductal versus lobular and special subtypes), and molecular subtype (defined by ER, PR, HER2 and proliferation). All three must be stated on every histopathology report because each drives a different treatment decision.[3]
In situ (non-invasive)
contained by basement membrane; cannot metastasise
- **DCIS** (ductal carcinoma in situ): about 20% of new diagnoses, almost all screening-detected; microcalcifications on mammography
- **LCIS** (lobular carcinoma in situ): not cancer — a **risk marker** (6 to 10x risk of subsequent invasive cancer), often bilateral and ER+
- Treated by WLE + radiotherapy (DCIS) or active surveillance/endocrine prevention (LCIS); no axillary surgery needed
Invasive (infiltrating)
breaches basement membrane; can metastasise
- **Invasive ductal carcinoma (IDC), no special type**: about 75 to 80% of all breast cancers
- **Invasive lobular carcinoma (ILC)**: about 10 to 15%, loss of E-cadherin (CDH1), discohesive single-file growth, often multifocal and bilateral
- Spread: lymphatic to axillary nodes; haematogenous to bone (about 70%), lung, liver, brain
Special clinicopathological entities
distinctive biology and management
- **Inflammatory breast cancer (T4d)**: dermal lymphatic invasion, peau d'orange, erythema, warmth; aggressive, always neoadjuvant chemotherapy first
- **Paget disease of the nipple**: eczematous erosion of the nipple-areola complex with underlying DCIS or invasive carcinoma in 50 to 90%
- **Phyllodes tumour**: stromal origin, benign/borderline/malignant; wide excision; rarely nodal (haematogenous spread)
- **Male breast cancer**: about 1%, nearly always ductal and ER+; treated with mastectomy + tamoxifen; all offered BRCA testing
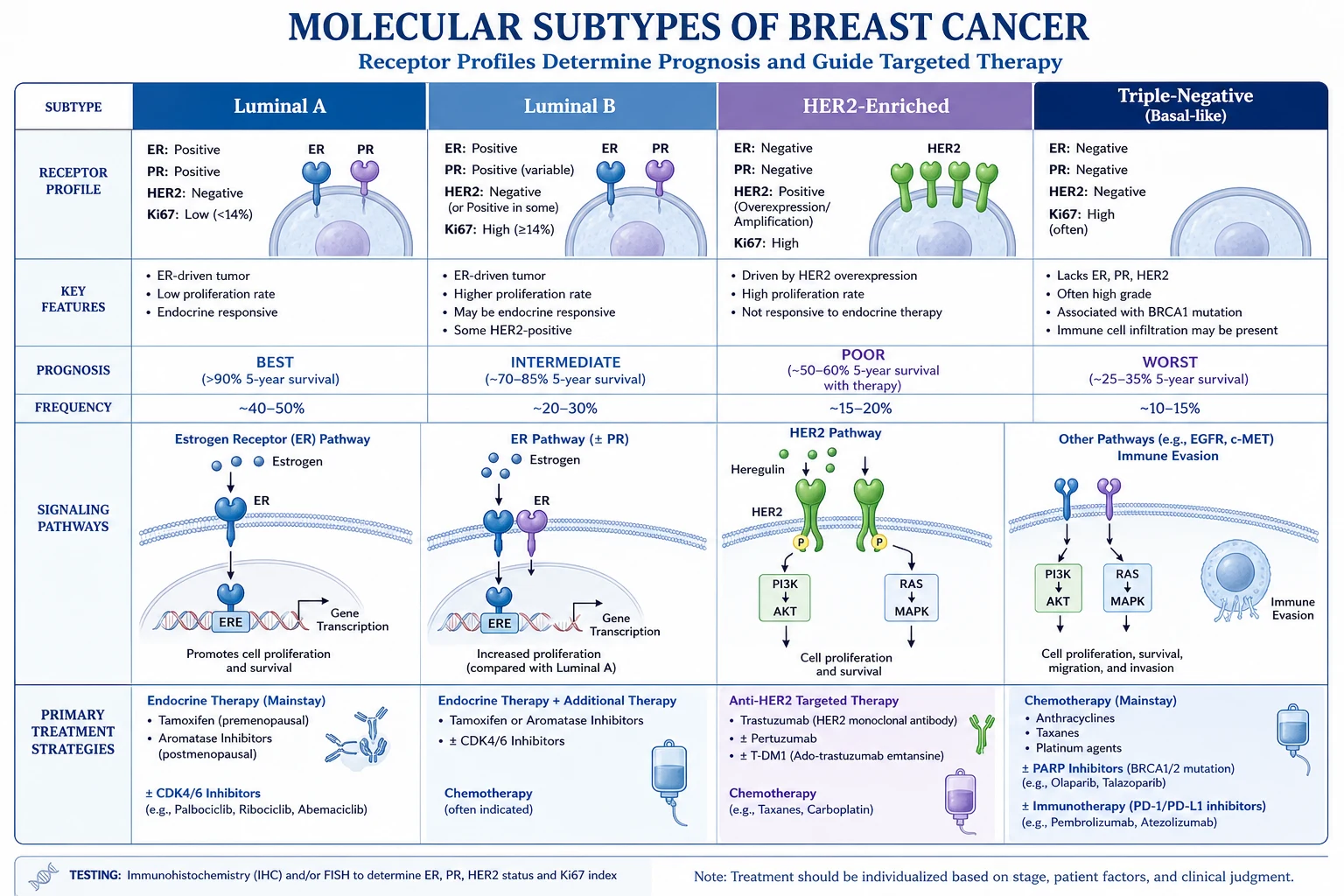
The molecular subtype is the most important modern classification because it determines the entire systemic therapy plan. It is derived from immunohistochemistry for ER, PR and HER2 (with HER2 confirmed by in-situ hybridisation when equivocal) and a proliferation marker, usually Ki-67.[1]
| Molecular subtype | ER/PR | HER2 | Ki-67 / grade | Typical treatment | Prognosis |
|---|---|---|---|---|---|
| Luminal A | Positive (high) | Negative | Low Ki-67, low grade | Endocrine alone ± chemo | Best |
| Luminal B | Positive (lower) | Negative or positive | High Ki-67, high grade | Endocrine + chemotherapy (+ anti-HER2 if HER2+) | Intermediate |
| HER2-enriched | Negative | Positive (amplified) | High | Chemotherapy + trastuzumab ± pertuzumab | Intermediate (much improved with anti-HER2) |
| Triple-negative / basal-like | Negative | Negative | High; often BRCA1-related | Chemotherapy (± platinum, immunotherapy) | Worst (recurrence concentrated in first 3 years) |
Epidemiology & Risk Factors
Breast cancer by the numbers
Breast cancer is the most common cancer in women globally and the leading cause of cancer death in women in many low- and middle-income countries. The peak incidence in Western populations sits between 50 and 70 years, the median age at diagnosis is around 62, and incidence rises steeply after 40. Mortality has fallen over the last three decades in high-income countries — a combined effect of organised mammographic screening, earlier presentation, and the introduction of effective adjuvant endocrine, anti-HER2 and chemotherapy regimens.[3]
The risk factors cluster into three groups. Genetic and familial risk is the most exam-relevant: germline BRCA1 (chromosome 17q21) and BRCA2 (chromosome 13q12) mutations account for 5 to 10% of all breast cancers and confer a 55 to 72% (BRCA1) and 45 to 69% (BRCA2) lifetime risk. BRCA1 tumours are characteristically high-grade, triple-negative and basal-like; BRCA2 tumours are more often ER-positive. The rarer syndromes — Li-Fraumeni (TP53), Cowden (PTEN), Peutz-Jeghers (STK11) and hereditary diffuse gastric cancer (CDH1) — each carry their own breast cancer risk. A first-degree relative with breast cancer roughly doubles personal risk, and this rises further if the relative was diagnosed before 50 or had bilateral disease.[3]
Hormonal and reproductive risk factors all share a common thread — cumulative lifetime oestrogen exposure to the breast epithelium. The classical list is early menarche (before age 12), late menopause (after 55), nulliparity, late age at first full-term pregnancy (after 30), short duration of breastfeeding, and exogenous hormones (combined oral contraceptives give a small transient increase; combined hormone replacement therapy increases risk and the excess falls after stopping). Obesity in postmenopausal women is a major and modifiable driver, because adipose tissue aromatises androgens to oestrogen; it also raises insulin and inflammatory signalling. Alcohol intake (roughly 7 to 10% increase per unit per day) and smoking are independent lifestyle risks.[3]
Prior breast disease and iatrogenic exposure form the third group: a personal history of breast cancer, atypical ductal or lobular hyperplasia, LCIS, and previous chest-wall radiotherapy (most classically for Hodgkin lymphoma in adolescence) all substantially raise risk. Dense breast tissue is both a risk factor and a confounder of mammographic detection — it roughly doubles risk and obscures small tumours, which is one rationale for MRI or tomosynthesis in dense breasts.[3]
India and South Asia. Breast cancer has now surpassed cervical cancer as the commonest cancer in Indian women in urban centres. The age-standardised incidence is rising at about 1 to 2% per year, and the peak age is 5 to 10 years younger than in Western series (40 to 50 years rather than 50 to 70). A majority present with locally advanced or metastatic disease (Stage III/IV in 50 to 70%), driven by low screening uptake, delayed referral, and limited access to mammography; most tumours are still found by self-examination or clinical breast examination. Triple-negative and locally advanced subtypes are over-represented. Founder BRCA mutations cluster in particular communities (e.g. Agarwal, Parsi). Tuberculosis of the breast is an important mimic in endemic regions and must be considered before committing to cancer therapy.[3]
Pathophysiology
Breast carcinogenesis is a multistep accumulation of genetic and epigenetic alterations that progressively liberates ductal or lobular epithelium from normal growth control. The classical morphological progression is normal epithelium → usual ductal hyperplasia → atypical ductal hyperplasia → ductal carcinoma in situ → invasive ductal carcinoma. Each step reflects additional hits: loss of cell-cycle checkpoints, escape from apoptosis, acquisition of replicative immortality, angiogenesis, and finally the capacity to degrade the basement membrane and survive in a foreign stroma or distant organ.[3]
The decisive molecular lesion determines both behaviour and treatment. ER-positive, HER2-negative tumours are driven by oestrogen signalling through the oestrogen receptor, which acts as a ligand-activated transcription factor turning on proliferative genes; starving them of oestrogen (aromatase inhibition, ovarian suppression) or blocking the receptor (tamoxifen) is therefore the backbone of therapy. HER2-amplified tumours overexpress the HER2 receptor tyrosine kinase, driving constitutive MAPK and PI3K signalling; they are biologically aggressive but uniquely sensitive to anti-HER2 monoclonal antibodies and antibody-drug conjugates. Triple-negative tumours are a heterogeneous group unified by absence of the two druggable receptors — many are basal-like and overlap with BRCA1-deficient biology, relying on homologous-recombination repair defects that make them vulnerable to platinum salts and PARP inhibitors.[1]
The mechanisms of spread explain the clinical phenotype. Direct extension produces the tethered, fixed lump and skin involvement. Lymphatic spread runs first to the axillary nodes (level I lateral, level II central/behind pectoralis minor, level III apical), then to supraclavicular and internal mammary nodes; nodal tumour burden is a dominant prognostic factor. Haematogenous spread seeds the characteristic distant sites — bone (about 70%, osteolytic or osteoblastic), lung, liver, and brain — and lobular carcinoma has a curious predilection for the peritoneum, retroperitoneum and gastrointestinal serosa. Dermal lymphatic invasion by tumour emboli is the pathological signature of inflammatory breast cancer, producing the peau d'orange, erythema and warmth.[3]
Clinical Presentation
The dominant lump is characterised at the bedside by its site (quadrant and clock position), size, consistency (hard, firm or soft), surface (irregular or smooth), edge (ill-defined or circumscribed) and mobility (mobile, tethered to skin, or fixed to chest wall). Malignant lumps are classically hard, irregular, ill-defined and tethered; they do not transilluminate. Bilateral, multiple, soft, mobile and tender lumps favour a benign process.[3]
Nipple changes are the next most common presentation. Recent unilateral nipple retraction or inversion in an older woman is caused by tumour tethering and shortening of the lactiferous ducts, and is a red flag. Nipple discharge is significant when it is spontaneous, unilateral, single-duct, persistent, and bloodstained or serosanguineous — these features point to an intraductal papilloma or carcinoma and mandate triple assessment with ductography or duct excision if no lump is palpable. Milky, multicoloured, bilateral, non-spontaneous discharge is almost always benign.[3]
Skin changes reflect tumour involvement of dermal structures and lymphatics. Dimpling (tethering to skin or Cooper ligaments) and skin retraction are subtle but important. Peau d'orange (orange-peel skin) — thickened, oedematous skin pitted by hair follicles — signals dermal lymphatic obstruction and is the cutaneous hallmark of inflammatory breast cancer. Erythema, warmth and rapid breast enlargement complete the inflammatory tetrad. Eczematous, crusting, weeping erosion of the nipple-areola complex that fails to settle with topical treatment is Paget disease and is almost always accompanied by underlying DCIS or invasive carcinoma.[3]
Axillary lymphadenopathy may be the first sign: a hard, fixed, matted axillary mass with or without a detectable breast primary. Distant metastatic symptoms bring a small fraction of patients to diagnosis — bone pain or pathological fracture (bone), dyspnoea and pleuritic pain (lung or pleural effusion), jaundice and right upper quadrant pain (liver), headache, seizures or focal deficit (brain), and behavioural change (leptomeningeal disease). Constitutional symptoms (weight loss, anorexia) indicate advanced disease.[3]
Atypical presentations are deliberately tested by examiners. Inflammatory breast cancer in a young woman is frequently misdiagnosed as mastitis or cellulitis — any "mastitis" not settling on antibiotics within two weeks, especially if not lactating, must be biopsied. Male breast cancer presents late with a unilateral retroareolar lump, nipple ulceration or discharge. Pregnancy-associated breast cancer hides within nodular lactating breast tissue and is therefore diagnosed at a later stage. Occult breast cancer may present as axillary nodal metastases with an impalpable, mammographically occult primary found only on MRI.[3]
Differential Diagnosis
A breast lump is a finding, not a diagnosis — the differential is wide and the features that separate benign from malignant are what the triple assessment is designed to resolve.[3]
Benign — stromal / epithelial
young women, mobile
- **Fibroadenoma** (15 to 30y): smooth, firm, highly mobile ('breast mouse'), rubbery, painless; benign stromal-epithelial proliferation
- **Phyllodes tumour**: usually older, large, rapidly growing smooth mass; stromal origin; benign/borderline/malignant; wide excision, no SLNB
- **Intraductal papilloma**: small subareolar lesion causing bloodstained single-duct nipple discharge
Benign — cystic / inflammatory
tender or fluctuant
- **Breast cyst** (30 to 50y): discrete, fluctuant, may transilluminate, tender, appears rapidly; aspirate to clear
- **Fibrocystic change**: cyclical (premenstrual), bilateral, multiple, tender nodularity; physiological, not premalignant
- **Galactocele**: lactating woman, cystic, milky contents
- **Breast abscess** (lactational) or **periductal mastitis**: tender, erythematous, fluctuant, fever; periductal type in smokers
Other / malignant mimics
trap doors
- **Fat necrosis**: prior trauma or surgery; firm, irregular, can closely mimic cancer and even calcify
- **Duct ectasia**: periareolar, thick non-bloody discharge, periductal inflammation, nipple retraction
- **Tuberculosis of the breast** (endemic regions): chronic sinus, granulomatous; mimics cancer
- **Skin cancers (e.g. basal cell, melanoma) and skin metastases**: rare, biopsied as for any lesion
The single rule that protects against error: any new, discrete, persistent breast lump in a woman over 35, or any lump with suspicious imaging, must be sampled by core needle biopsy — no benign label is assigned on clinical grounds alone.[3]
Clinical & Bedside Assessment
The triple assessment is the cornerstone of breast lump evaluation and combines clinical examination, imaging, and tissue sampling. When all three components agree, the triple assessment is about 98% accurate, and any disagreement mandates excision biopsy or repeat sampling. It is the single most tested concept in breast surgery examinations.[3]
- Clinical examination — inspection and palpation of both breasts, regional nodes and a focused systemic look.[3]
- Imaging — mammography and/or ultrasound guided by age and density; MRI in selected cases.
- Tissue sampling — core needle biopsy (gold standard), fine-needle aspiration cytology, or excision biopsy.
Clinical breast examination begins with the patient sitting, exposed to the waist, inspected in four positions — arms by the side, hands pressed onto hips (to tense pectoralis), arms raised above the head, and leaning forward. The examiner looks for asymmetry, contour change, skin changes (dimpling, peau d'orange, erythema, ulceration), nipple changes (retraction, eczema, discharge), and visible masses. Palpation is performed supine, with the ipsilateral arm raised above the head to spread the breast over the chest wall. All four quadrants, the central areolar area, and the axillary tail of Spence are palpated systematically with the flat of the fingers. Each lump is documented by site (clock position and distance from nipple), size, consistency, surface, edge and fixity to skin and chest wall. The axilla is examined for the five nodal groups (anterior, posterior, lateral, central, apical), and the supraclavicular fossae and the other breast are always checked.[3]
Triple assessment — the standard diagnostic approach
Investigations
Imaging is the second arm of triple assessment and the modality is chosen by age and breast density. Mammography is first-line for women over 35 (denser breasts in younger women obscure lesions and radiate glandular tissue unnecessarily). The malignant mammographic signs are clustered pleomorphic microcalcifications, a spiculated (star-like) mass, architectural distortion, and an asymmetric density that persists on spot compression. Mammographic findings are graded by the BI-RADS (Breast Imaging Reporting and Data System) score from 0 to 6: BI-RADS 0 incomplete (recall), 1 negative, 2 benign, 3 probably benign (short-interval follow-up), 4 suspicious (biopsy), 5 highly suggestive of malignancy (biopsy), and 6 known biopsy-proven malignancy. BI-RADS 4 and 5 mandate core biopsy.[3]
Ultrasound is first-line for women under 35 and is complementary at any age. It distinguishes solid from cystic lesions, characterises benign versus malignant morphology (malignant masses are hypoechoic, taller-than-wide, with indistinct margins and posterior shadowing; simple cysts are anechoic with posterior enhancement), and guides needle biopsy. Breast MRI is reserved for screening high-risk women (BRCA carriers, lifetime risk above 20 to 25%), assessing the extent of disease in dense breasts, evaluating response to neoadjuvant chemotherapy, imaging the augmented breast, and finding an occult primary in node-positive cancer with negative mammography and ultrasound.[3]
Tissue sampling completes the assessment. The 14-gauge core needle biopsy, taken under ultrasound or stereotactic guidance and yielding multiple cores, is the gold standard because it provides histological type, grade, ER, PR, HER2 and Ki-67 — the four pieces of information that determine systemic therapy. Fine-needle aspiration cytology is quick and minimally invasive but cannot assess invasion or receptors; it retains a role in cyst aspiration and sampling suspicious axillary nodes. Excision (open) biopsy is reserved for non-diagnostic cores or image-pathology discordance, and must always be performed as a definitive lumpectomy with curative intent when cancer is confirmed.[3]
Receptor and molecular testing on the core biopsy defines the molecular subtype (ER, PR, HER2 by immunohistochemistry; HER2 equivocation confirmed by in-situ hybridisation) and, increasingly, genomic assays such as Oncotype DX or MammaPrint to guide chemotherapy in ER-positive node-negative disease. Ki-67 proliferation index separates Luminal A (low) from Luminal B (high).[1]
Staging investigations for confirmed invasive cancer include CT chest/abdomen/pelvis, bone scan, and (where indicated) FDG-PET/CT — used selectively, typically for locally advanced disease, suspicious symptoms, or triple-negative/HER2-positive biology. Sentinel lymph node biopsy stages the axilla intraoperatively (see Management). BRCA genetic testing is offered when criteria are met: young age (under 45 to 50), triple-negative breast cancer under 60, bilateral disease, male breast cancer, ovarian cancer in the patient or family, or a strong family history — and is now increasingly performed with multigene panel testing.[3]
Screening
Screening is distinct from the triple assessment of a symptomatic woman: it is the invitation of asymptomatic women to a structural test on the basis of age or risk. Two organised programmes dominate MBBS examinations.[3]
The NHS Breast Screening Programme (NHSBSP) invites women aged 50 to 70 years for two-view mammography every three years; the programme is being progressively extended to cover ages 47 to 73. Mammography detects microcalcifications and small masses years before they become palpable, shifting the stage distribution toward DCIS and small node-negative invasive cancers and reducing breast-cancer mortality by about 20% in the invited population. Recall for assessment, biopsy and one-stop clinics flow directly from a positive screen. Self-referral is possible for older women. The principal harms of screening — overdiagnosis (detection of indolent cancers that would never have surfaced clinically), false-positive recalls, radiation exposure and biopsies — are openly weighed against benefit in the consent process.[3]
High-risk women are screened differently. BRCA1/2 carriers and women with a lifetime breast-cancer risk above about 20 to 25% are offered annual breast MRI from age 30 to 50 (more sensitive than mammography in dense, young breasts), with annual mammography added from age 40; MRI may be replaced or supplemented by tomosynthesis as women age and breast density falls. Women previously treated with mantle radiotherapy for Hodgkin lymphoma between ages 10 and 30 are also offered MRI-based screening beginning 8 to 10 years after radiation. Clinical breast examination and breast self-awareness are promoted as adjuncts, though neither alone reduces mortality.[3]
Chemoprevention complements screening in high-risk women: tamoxifen 20mg OD for 5 years (pre- or postmenopausal) or raloxifene (postmenopausal) reduces the incidence of ER-positive breast cancer in high-risk women, and is endorsed by NICE for women at moderate or greater risk.[3]
Management — Resuscitation
Breast cancer is not usually a surgical emergency, and the diagnostic and staging work-up is completed electively over days to weeks. A handful of oncological emergencies must be recognised and treated immediately, however:[3]
- Malignant spinal cord compression from vertebral metastases is the most urgent. Give dexamethasone 16mg IV immediately (loading), arrange urgent whole-spine MRI, and refer for emergency radiotherapy or surgical decompression within 24 hours — delay beyond 48 hours of paraplegia is rarely reversible.
- Hypercalcaemia of malignancy from widespread bone metastases presents with confusion, polyuria, constipation and thirst. Treat with aggressive IV normal saline rehydration, a bisphosphonate (zoledronic acid 4mg IV infusion) or denosumab 120mg subcutaneously, and treat the underlying cancer.
- Neutropenic sepsis on chemotherapy is a time-critical medical emergency — take cultures and give empirical broad-spectrum antibiotics within one hour of presentation, per local protocol.
- A fungating, ulcerated or bleeding local tumour needs palliative radiotherapy, topical haemostatic dressings and dedicated wound-care nursing.[3]
These aside, the priority is to stage the patient, determine the molecular subtype, present the case at a multidisciplinary team (MDT) meeting, and plan definitive locoregional and systemic therapy.[3]
Management — Definitive & Stepwise
Definitive treatment is multimodal and multidisciplinary, planned by surgery, medical oncology, radiation oncology, radiology and pathology together. The three pillars — surgery, radiotherapy, and systemic therapy — are combined differently for early, locally advanced, and metastatic disease, and the molecular subtype dictates the systemic arm.[3]
Surgery of the breast
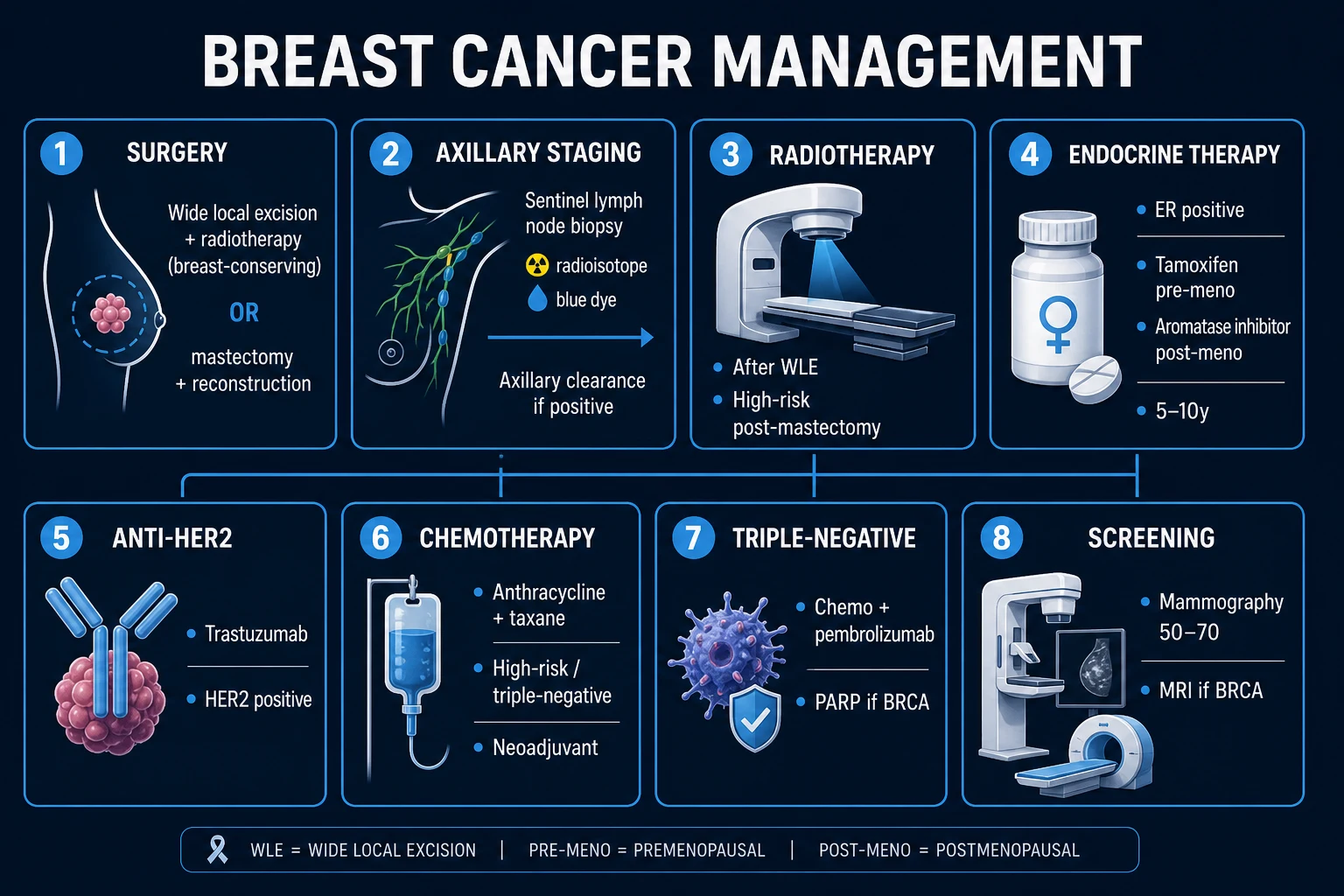
Wide local excision (WLE) plus whole-breast radiotherapy constitutes breast-conserving therapy (BCT) and is the standard of care for most unifocal tumours up to about 4 to 5cm. The landmark NSABP B-06 and Milan trials, and the EBCTCG meta-analysis, established that BCT produces survival identical to mastectomy provided clear margins are achieved and radiotherapy is delivered — omitting radiotherapy after WLE roughly doubles local recurrence and increases breast-cancer mortality.[4]
Mastectomy (simple or total) is preferred when the tumour is large relative to the breast, multicentric, inflammatory, when margins cannot be cleared by WLE, when radiotherapy is contraindicated (pregnancy, prior chest irradiation, severe connective tissue disease), or by patient choice. Skin-sparing and nipple-sparing mastectomy improve the cosmetic result when immediate reconstruction is planned. Immediate or delayed reconstruction — with an implant, a tissue expander, or an autologous flap (DIEP, TRAM or latissimus dorsi) — should be discussed with every patient facing mastectomy; it does not compromise oncological control when margins and radiotherapy are properly managed.[3]
Surgery of the axilla
The status of the axillary nodes is the single most powerful prognostic factor, and management has shifted from routine clearance to a staged, less-invasive philosophy. Sentinel lymph node biopsy (SLNB) is the standard for the clinically and radiologically node-negative axilla. A blue dye (methylene blue or patent blue V) and/or a radioisotope (technetium-99-labelled colloid) is injected at the tumour, areola or periareolar skin; the first draining node(s) — the sentinel node(s) — are identified and excised. If the sentinel node is negative, no further axillary surgery is needed (NSABP B-32 showed this is safe). If one to two nodes are positive and the patient is having breast-conserving therapy with adjuvant whole-breast radiotherapy and appropriate systemic therapy, ACOSOG Z0011 showed that completing axillary clearance adds no survival benefit — these patients can be observed. Three or more positive nodes, extranodal extension, or mastectomy without radiotherapy generally trigger axillary lymph node clearance (levels I to III) or axillary radiotherapy. SLNB has reduced the incidence of disabling arm lymphoedema from 25 to 40% after full clearance down to 5 to 8%.[3]
Radiotherapy
Whole-breast radiotherapy after WLE reduces local recurrence by about half and reduces 15-year breast-cancer mortality by about a sixth — roughly one breast cancer death avoided for every four recurrences prevented. A tumour-bed boost is given to high-risk patients. Post-mastectomy radiotherapy is offered for tumours over 5cm, four or more positive nodes, T4 disease, or positive margins, and reduces locoregional recurrence and improves survival. Modern techniques (breath-hold, intensity-modulated radiotherapy, prone positioning) minimise cardiac and pulmonary dose — an important consideration because older regimens measurably increased ischaemic heart disease and second lung cancers, particularly in smokers and after left-sided treatment.[4][7]
Systemic therapy — adjuvant and neoadjuvant
Systemic therapy is dictated by the molecular subtype, nodal status, tumour size, grade, Ki-67 and genomic risk score. It is given either adjuvant (after surgery) or neoadjuvant (before surgery).[3]
Endocrine therapy by menopausal status
TAPI
PREmenopausal — a SERM that blocks ER on the breast but stimulates the ovaries. Standard dose 20mg orally once daily for 5 to 10 years
POSTmenopausal — letrozole 2.5mg OD, anastrozole 1mg OD, or exemestane 25mg OD; block peripheral conversion of androgens to oestrogen in adipose
if a premenopausal woman takes an AI, add ovarian suppression with goserelin 3.6mg subcutaneously monthly (or 10.8mg 3-monthly)
Duration 5 to 10 years depending on recurrence risk — extended therapy reduces late relapse
Endocrine therapy is given to all ER-positive disease, regardless of menopausal status. In premenopausal women, tamoxifen 20mg orally once daily for 5 to 10 years remains the standard; it is a selective oestrogen receptor modulator that antagonises oestrogen at the breast but acts as a partial agonist at the endometrium and on coagulation, producing its signature side effects of venous thromboembolism (2 to 3x), endometrial cancer (2 to 3x), hot flushes and menstrual irregularity. In postmenopausal women, aromatase inhibitors — letrozole 2.5mg OD, anastrozole 1mg OD, or exemestane 25mg OD — are preferred, as the ATAC trial confirmed superiority over tamoxifen; their characteristic toxicities are osteoporosis and arthralgia rather than thrombosis. Adding ovarian function suppression (goserelin 3.6mg subcutaneously monthly) lets premenopausal women benefit from aromatase inhibitors and is recommended for higher-risk premenopausal disease (SOFT/TEXT trials).[3]
HER2-directed therapy has transformed the prognosis of HER2-positive breast cancer. Trastuzumab (Herceptin), a monoclonal antibody against the HER2 receptor external domain, is given at a loading dose of 8mg/kg IV then 6mg/kg every 3 weeks for one year with chemotherapy; the HERA trial confirmed its survival benefit. It is combined with pertuzumab (loading 840mg then 420mg every 3 weeks) in dual-blockade regimens for higher-risk and neoadjuvant settings. Trastuzumab's key toxicity is cardiotoxicity — asymptomatic drop in left ventricular ejection fraction and occasionally heart failure — so echocardiographic monitoring before and during treatment is mandatory.[5]
Chemotherapy is given for node-positive disease, large or high-grade tumours, HER2-positive disease (with trastuzumab), triple-negative disease, and younger premenopausal women with higher-risk biology. The backbone is the anthracycline-taxane sequence — typically doxorubicin 60mg/m2 plus cyclophosphamide 600mg/m2 every 3 weeks for four cycles (AC), followed by paclitaxel 175mg/m2 every 3 weeks or weekly paclitaxel 80mg/m2 for 12 weeks (AC-T) — or the dose-dense variant. For those in whom anthracyclines are contraindicated, docetaxel plus cyclophosphamide (TC) is an alternative. Anthracyclines carry a dose-dependent cardiotoxicity (monitor LVEF) and a small risk of secondary leukaemia; taxanes cause alopecia, neuropathy and neutropenia.[1]
Triple-negative breast cancer has no targetable receptor, so chemotherapy is the only systemic option — but it is increasingly individualised. Neoadjuvant platinum (carboplatin) improves pathological complete response in basal-like disease, and pembrolizumab (an anti-PD-1 antibody, 200mg IV every 3 weeks) added to chemotherapy and continued adjuvantly is now standard for PD-L1-positive early and metastatic triple-negative disease. For BRCA1/2-mutated triple-negative or HER2-negative metastatic cancer, the PARP inhibitor olaparib 300mg orally twice daily improved progression-free survival in the OlympiAD trial (7.0 versus 4.2 months; hazard ratio 0.58).[1][6]
Neoadjuvant therapy (given before surgery) is used to downsize a large tumour to enable breast conservation, to treat inflammatory breast cancer, to assess in-vivo chemosensitivity (a pathological complete response, pCR, predicts an excellent prognosis and can guide escalation or de-escalation), and to treat locally advanced disease. The same regimens that work adjuvantly are used neoadjuvantly.[3]
Palliative and metastatic therapy (Stage IV)
Metastatic breast cancer is incurable but treatable, with median survivals now measured in years for many subtypes. Bone metastases are managed with antiresorptive therapy — zoledronic acid 4mg IV monthly or denosumab 120mg subcutaneously every 4 weeks — which reduces skeletal events and pain, plus palliative radiotherapy for painful or weight-bearing deposits and orthopaedic fixation of impending pathological fractures. ER-positive metastatic disease is treated with endocrine therapy plus a CDK4/6 inhibitor (palbociclib 125mg OD, ribociclib, or abemaciclib), which roughly doubles progression-free survival. HER2-positive metastatic disease is treated with trastuzumab + pertuzumab, then trastuzumab emtansine (T-DM1) and, for HER2-low disease (immunohistochemistry 1+ or 2+/ISH-negative), trastuzumab deruxtecan, which nearly doubled survival versus chemotherapy in DESTINY-Breast04 (overall survival 23.4 versus 16.8 months) — at the cost of interstitial lung disease, which demands vigilance. Triple-negative metastatic disease is treated with chemotherapy (with pembrolizumab if PD-L1-positive), olaparib or talazoparib if BRCA-mutated, and antibody-drug conjugates such as sacituzumab govitecan.[1][5][6]
Specific Subtypes & Scenarios
Inflammatory breast cancer (T4d). The most aggressive breast cancer subtype, defined pathologically by dermal lymphatic invasion by tumour emboli. Clinically the breast is rapidly enlarged, warm, erythematous, indurated and tender, with peau d'orange skin and often a spectrum of confluent changes rather than a discrete lump; it is frequently misdiagnosed as mastitis or cellulitis. Standard treatment is primary systemic therapy — anthracycline- and taxane-based chemotherapy, with anti-HER2 therapy if HER2-positive — followed by mastectomy and axillary clearance, then chest-wall and nodal radiotherapy. Prognosis remains poor.[3]
Paget disease of the nipple. An eczematous, scaling, weeping, often itchy erosion of the nipple-areola complex, caused by intraepidermal spread of malignant Paget cells (large, clear, pale cells) from an underlying ductal carcinoma. About 50 to 90% have associated DCIS or invasive carcinoma. Any unilateral nipple eczema that fails to settle with topical treatment in two to three weeks must be biopsied. Treatment is that of the underlying cancer — mastectomy or WLE + radiotherapy — with systemic therapy by subtype.[3]
Phyllodes tumour. A fibroepithelial neoplasm of stromal origin (not epithelial), classified as benign, borderline or malignant based on stromal cellularity, mitoses, margins and stromal overgrowth. Presents as a rapidly growing, large, smooth, well-circumscribed mass, often in women 40 to 50 years. Treatment is wide local excision with at least 1cm margins. Sentinel node biopsy is NOT indicated — spread is haematogenous and nodal involvement is rare. Malignant phyllodes can metastasise to lung.[3]
Male breast cancer. Accounts for about 1% of all breast cancers. Presents late (delayed diagnosis) with a unilateral retroareolar lump, nipple retraction, ulceration or discharge. Histology is nearly always ductal and ER-positive, so mastectomy (rather than WLE) is the surgical standard, and tamoxifen 20mg OD is the endocrine therapy of choice even in men — the ASCO guideline confirms tamoxifen first-line, with a GnRH agonist plus aromatase inhibitor only for those who cannot tolerate tamoxifen. All men with breast cancer should be offered genetic testing, as the BRCA2 (and to a lesser extent BRCA1) carriage rate is high.[2]
Ductal carcinoma in situ (DCIS). Non-invasive, contained by the basement membrane, and therefore cannot metastasise — but if untreated about 30 to 50% progress to invasive cancer. Usually detected as microcalcifications on screening mammography. Treatment is WLE + whole-breast radiotherapy, with mastectomy for large or multicentric disease. Endocrine therapy (tamoxifen) may be added for ER-positive DCIS. The axilla does not require staging in pure DCIS, though SLNB may be considered at mastectomy.[3]
Complications & Pitfalls
Complications of the disease include local recurrence in the conserved breast or chest wall, distant metastases (bone about 70%, then lung, liver and brain), pathological fracture, spinal cord compression, hypercalcaemia, malignant pleural effusion, and the psychological burden of a cancer diagnosis — body image, anxiety and depression.[3]
Complications of surgery include seroma (the commonest, managed by aspiration), haematoma, wound infection, lymphoedema of the arm (5 to 8% after SLNB, 25 to 40% after full axillary clearance), shoulder stiffness, chronic pain, and sensory change from intercostobrachial nerve injury (numbness of the medial upper arm). Immediate versus delayed reconstruction has its own set of complications — implant capsular contracture, flap loss, donor-site morbidity.[3]
Complications of radiotherapy include acute skin erythema and desquamation, fatigue and breast oedema; and late effects of fibrosis, cardiac toxicity (ischaemic heart disease, more pronounced for left-sided tumours), pneumonitis, brachial plexopathy, and a small excess of secondary angiosarcoma in the irradiated field decades later. Modern radiotherapy minimises cardiac dose, and smoking cessation substantially lowers the radiation-related lung cancer risk.[7]
Complications of systemic therapy include chemotherapy-induced alopecia, nausea, neutropenia and sepsis, anthracycline and trastuzumab cardiotoxicity (the former dose-dependent and often permanent, the latter frequently reversible on stopping), taxane neuropathy, tamoxifen-related VTE and endometrial cancer, and aromatase-inhibitor osteoporosis and arthralgia.[1][3]
Classic pitfalls. Treating inflammatory cancer as mastitis; assigning a benign diagnosis on clinical grounds alone without triple assessment; failing to check receptor status before planning therapy; using tamoxifen in a postmenopausal woman without considering aromatase-inhibitor superiority; omitting genetic testing in a man with breast cancer or a young woman with triple-negative disease; missing a second primary in the contralateral breast; and forgetting to counsel about lymphoedema and arrange a compression sleeve before axillary surgery.[3]
Prognosis & Disposition
Prognosis is driven by the TNM stage, nodal burden, tumour grade, and molecular subtype. The 8th edition of the TNM classification (TNM-8) measures the invasive tumour size in millimetres, includes the clinical and pathological nodal categories, and incorporates biological factors through prognostic staging groups rather than anatomical staging alone. The anatomical T categories are: T1 — tumour up to 20mm (subdivided T1mi, T1a, T1b, T1c); T2 — tumour more than 20mm up to 50mm; T3 — tumour more than 50mm; T4 — extension to chest wall (T4a), skin (T4b), both (T4c), or inflammatory (T4d). Nodal categories run N0 (no regional metastasis) through N3 (infraclavicular or supraclavicular disease), and M0/M1 denote absence or presence of distant metastasis.[3]
Approximate five-year relative survival by stage (modern era):[3]
| Stage | Description | 5-year relative survival |[3] |---|---|---| | Stage I | Localised (T1N0M0) | about 99% | | Stage II | Regional, limited node involvement | about 85 to 86% | | Stage III | Locally advanced (large primary, extensive nodes, T4) | about 60% | | Stage IV | Distant metastasis (M1) | about 28 to 31% (improving) |
Molecular subtype heavily modifies these figures. Luminal A has the best prognosis; HER2-enriched was once the worst but has been transformed by trastuzumab; triple-negative now carries the worst prognosis, with recurrence concentrated in the first three years after diagnosis and a predilection for visceral and brain metastases. Achieving a pathological complete response to neoadjuvant chemotherapy — commonest in HER2-positive and triple-negative disease — confers an excellent prognosis and is increasingly used to escalate (for residual disease, e.g. T-DM1 in HER2+ or capecitabine in triple-negative) or de-escalate subsequent therapy.[1]
Disposition after treatment is to a multidisciplinary breast cancer follow-up programme — regular clinical examination and annual mammography, endocrine-therapy adherence and bone-density monitoring where relevant, cardiotoxicity surveillance after anthracycline/trastuzumab, lymphoedema and shoulder rehabilitation, and psychological support. Most recurrences occur within the first five years for triple-negative disease but can emerge over ten or more years in ER-positive disease, which is the rationale for extended endocrine therapy.[3]
Special Populations
Pregnancy-associated breast cancer (diagnosed during pregnancy or in the first postpartum year) is difficult to assess because the lactating breast is nodular and dense, so diagnosis is delayed and stage at presentation is more advanced. Ultrasound is the imaging modality of choice (mammography is safe with abdominal shielding; gadolinium MRI is avoided in the first trimester). Core biopsy is safe. Surgery is safe in any trimester; radiotherapy is deferred until after delivery; chemotherapy is safe in the second and third trimesters (anthracycline-based) but avoided in the first; tamoxifen is absolutely contraindicated (teratogenic). Termination of pregnancy is not routinely advised.[3]
BRCA1/2 carriers have a 55 to 72% and 45 to 69% lifetime breast cancer risk respectively, and a markedly elevated ovarian cancer risk. Management combines enhanced surveillance (annual breast MRI from age 25, mammography from 30), chemoprevention with tamoxifen or raloxifene in selected women, and risk-reducing surgery — bilateral risk-reducing mastectomy lowers breast cancer risk by about 90 to 95%, and bilateral salpingo-oophorectomy around age 35 to 40 (after childbearing) dramatically lowers ovarian cancer risk and, when performed premenopausally, also lowers breast cancer risk.[3]
Older and frail patients may not tolerate full-dose chemotherapy; decisions are individualised using a combination of chronologic age, comorbidity (e.g. Charlson score), functional status and patient preference. Standard endocrine therapy (often with an aromatase inhibitor) is well tolerated and under-used, and breast-conserving therapy with radiotherapy remains feasible for many.[3]
Male breast cancer is addressed in the subtypes section; tamoxifen is the endocrine standard, all men should be offered genetic testing, and mastectomy is the usual operation.[2]
Evidence, Guidelines & Regional Differences
The modern management of breast cancer is one of the most evidence-rich areas of medicine, built on landmark randomised trials and serial meta-analyses by the Early Breast Cancer Trialists' Collaborative Group (EBCTCG).[4]
- NSABP B-04 and B-06 established that breast-conserving therapy (WLE + radiotherapy) is equivalent to mastectomy for survival, provided margins are clear and radiotherapy given.
- EBCTCG radiotherapy meta-analysis (2011) showed that radiotherapy after breast-conserving surgery roughly halves local recurrence and reduces 15-year breast-cancer mortality by about a sixth — one death avoided for every four recurrences prevented.[4]
- EBCTCG radiotherapy risk analysis (2017) quantified the long-term cardiac and lung risks of modern radiotherapy, and showed that smoking determines the net effect of radiotherapy on mortality — for most non-smokers the benefits far outweigh the risks.[7]
- NSABP B-32 showed that sentinel lymph node biopsy is safe and accurate for node-negative disease, sparing women the morbidity of full axillary clearance.
- ACOSOG Z0011 showed that completing axillary clearance after one or two positive sentinel nodes adds no survival benefit in selected women having breast-conserving therapy.
- ATAC trial established the superiority of aromatase inhibitors over tamoxifen in postmenopausal ER-positive disease; SOFT/TEXT refined ovarian-function suppression in higher-risk premenopausal disease.
- HERA trial established one year of adjuvant trastuzumab as standard for HER2-positive disease.
- OlympiAD (2017) showed that the PARP inhibitor olaparib 300mg twice daily improved progression-free survival in HER2-negative metastatic breast cancer with a germline BRCA mutation.[6]
- DESTINY-Breast04 (2022) established trastuzumab deruxtecan for HER2-low metastatic breast cancer, nearly doubling overall survival versus chemotherapy, and created a new HER2-low clinical category.[5]
Exam Pearls
- Triple assessment = clinical examination + imaging (mammography/ultrasound) + tissue (core needle biopsy). About 98% accurate when all three agree.[3]
- Most common histology: invasive ductal carcinoma (75 to 80%). Most common site: upper outer quadrant (about 40%).[3]
- BRCA1 (chromosome 17q21) → triple-negative, basal-like. BRCA2 (chromosome 13q12) → often ER-positive. Both account for 5 to 10% of all breast cancers.[3]
- Peau d'orange = dermal lymphatic obstruction by tumour (inflammatory cancer, T4d). Paget disease = eczematous nipple + underlying carcinoma.[3]
- Sentinel lymph node biopsy: blue dye + radioisotope. If negative, no axillary clearance (NSABP B-32). ACOSOG Z0011: no clearance needed for 1 to 2 positive nodes in selected BCT patients.
- Tamoxifen = PREmenopausal (20mg OD, 5 to 10 years). Aromatase inhibitors = POSTmenopausal (letrozole 2.5mg / anastrozole 1mg / exemestane 25mg OD).[3]
- Tamoxifen side effects: VTE, endometrial cancer, hot flushes. Aromatase inhibitor side effects: osteoporosis, arthralgia.
- Trastuzumab: 8mg/kg loading then 6mg/kg q3w for 1 year for HER2+ disease; monitor LVEF (cardiotoxicity).[5]
- Commonest metastasis: BONE (about 70%) — then lung, liver, brain. Triple-negative: worst prognosis.[1]
- Phyllodes tumour: stromal origin, wide local excision, NO sentinel node biopsy (haematogenous spread).[3]
- Male breast cancer: mastectomy + tamoxifen. All men offered genetic testing.[2]
- Inflammatory breast cancer: always neoadjuvant chemotherapy first, then mastectomy, then radiotherapy.[3]
- Radiotherapy halves local recurrence and lowers 15-year breast-cancer mortality by about a sixth after breast-conserving surgery.[4]
- Olaparib 300mg BD for BRCA-mutated HER2-negative metastatic disease (OlympiAD). Trastuzumab deruxtecan for HER2-low metastatic disease (DESTINY-Breast04).[6][5]
References
- [1]Leon-Ferre RA, Goetz MP. Advances in systemic therapies for triple negative breast cancer. BMJ, 2023.PMID 37253507
- [2]Hassett MJ, Somerfield MR, Baker ER, et al. Management of Male Breast Cancer: ASCO Guideline. Journal of Clinical Oncology, 2020.PMID 32058842
- [3]Waks AG, Winer EP. Breast Cancer Treatment: A Review. JAMA, 2019.PMID 30667505
- [4]Early Breast Cancer Trialists' Collaborative Group (EBCTCG), Darby S, McGale P, Correa C, et al. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet, 2011.PMID 22019144
- [5]Modi S, Jacot W, Yamashita T, et al.; DESTINY-Breast04 Trial Investigators. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. New England Journal of Medicine, 2022.PMID 35665782
- [6]Robson M, Im SA, Senkus E, et al. Olaparib for Metastatic Breast Cancer in Patients with a Germline BRCA Mutation. New England Journal of Medicine, 2017.PMID 28578601
- [7]Taylor C, Correa C, Duane FK, et al.; EBCTCG. Estimating the Risks of Breast Cancer Radiotherapy: Evidence From Modern Radiation Doses to the Lungs and Heart and From Previous Randomized Trials. Journal of Clinical Oncology, 2017.PMID 28319436