General Surgery · General Surgery
Portal Hypertension
Also known as Portal HTN · Variceal bleeding · Portosystemic hypertension · Oesophageal varices
Portal hypertension is sustained elevation of the portal venous pressure gradient (HVPG over 5 mmHg). Commonest cause worldwide is cirrhosis (sinusoidal); the commonest pre-sinusoidal cause globally is schistosomiasis. Four consequences: varices (oesophageal and gastric), ascites, splenomegaly with hypersplenism, and hepatic encephalopathy. Acute variceal bleed: resuscitate with restrictive transfusion (Hb target 70 to 80), terlipressin 2 mg IV every 4 h, ceftriaxone 1 g IV daily (mandatory antibiotic prophylaxis), and endoscopic band ligation within 12 h. Refractory bleeding: balloon tamponade (Sengstaken-Blakemore) as a bridge, then TIPSS. Primary prophylaxis: non-selective beta-blocker (propranolol, nadolol, carvedilol) or EVL. Secondary prophylaxis: beta-blocker plus serial EVL. HVPG over 10 = clinically significant; over 12 = bleeding risk; over 16 = high mortality.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Exam tags
Red flags
Overview & Definition
Portal hypertension is sustained elevation of the pressure gradient between the portal vein and the inferior vena cava, measured clinically as the hepatic venous pressure gradient (HVPG). The HVPG is the difference between the wedged (or balloon-occluded) hepatic venous pressure, which reflects sinusoidal pressure, and the free hepatic venous pressure, which reflects intra-abdominal inferior vena cava pressure. A normal HVPG is 3 to 5 mmHg. Portal hypertension is defined as an HVPG over 5 mmHg, but the clinically important thresholds are higher: an HVPG over 10 mmHg is clinically significant portal hypertension (CSPH) — the point at which varices form and ascites may develop; an HVPG over 12 mmHg is the threshold for variceal bleeding; and an HVPG over 16 mmHg predicts high mortality from a bleed. A fall in HVPG to under 12 mmHg, or by over 20 percent of baseline on medical therapy, identifies a responder with a markedly reduced risk of first or recurrent bleeding.[2]
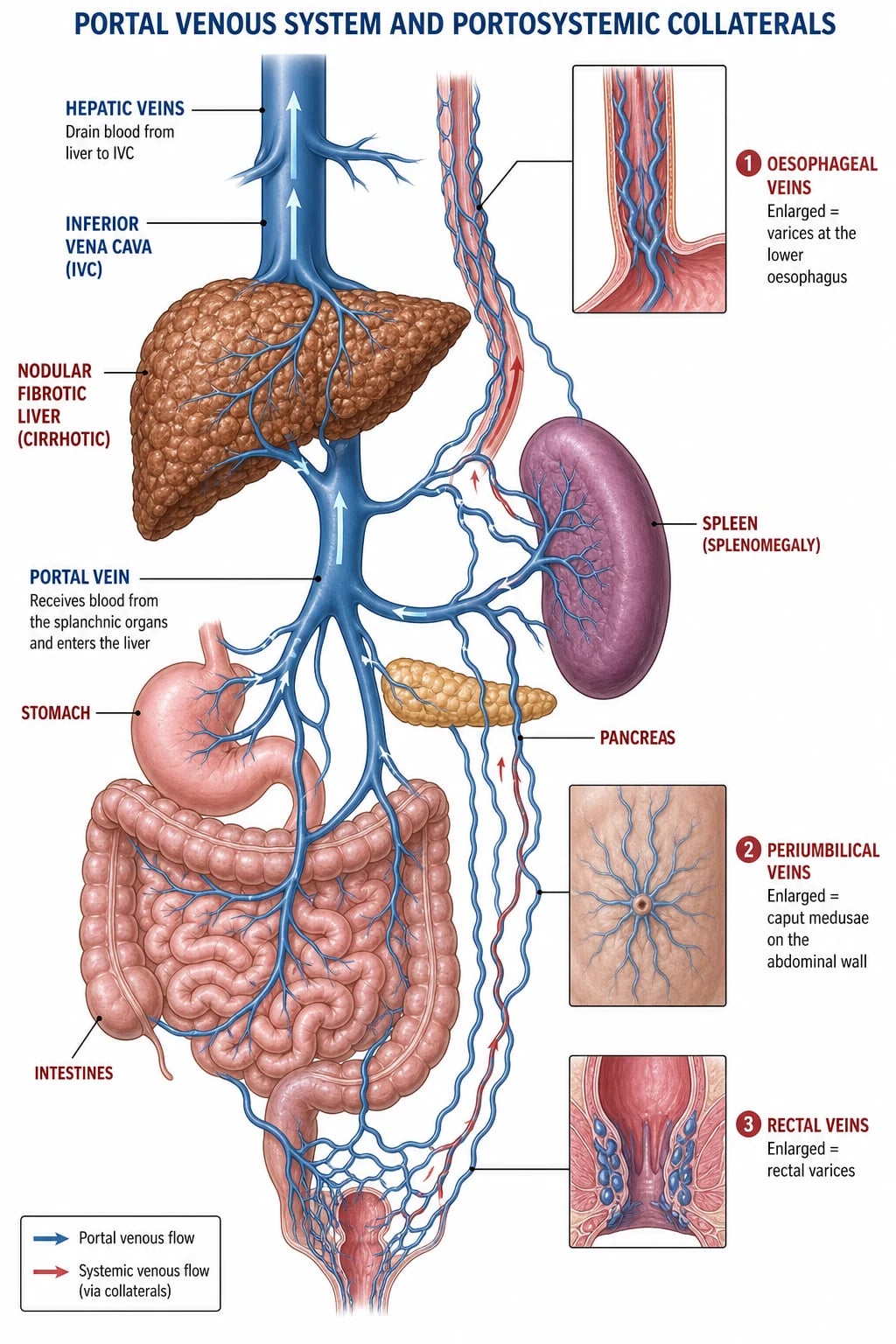
The portal vein is formed behind the neck of the pancreas by the union of the superior mesenteric vein (draining the midgut) and the splenic vein (draining the spleen and foregut via the left gastric and short gastric veins). It delivers nutrient-rich but partially deoxygenated blood to the liver, contributing roughly 75 percent of hepatic inflow; the hepatic artery supplies the remaining 25 percent. Because the portal circulation is interposed between two capillary beds (splanchnic and hepatic sinusoids) and has no valves, any obstruction to flow — before, within, or after the liver — transmits pressure backwards into the splanchnic bed and opens the embryonic portosystemic anastomoses. [1]
Portal-systemic anastomoses (where collaterals open)
When portal pressure rises, blood is decompressed through four classic sites of portosystemic communication, plus the bare areas of the liver:[1]
- Oesophago-gastric junction — the left gastric (coronary) vein (portal) anastomoses with the oesophageal veins draining to the azygos and hemi-azygos (systemic). These dilate into oesophageal and gastric varices, the commonest source of life-threatening haemorrhage.
- Rectum / anal canal — the superior rectal vein (portal, via inferior mesenteric) meets the middle and inferior rectal veins (systemic, internal iliac), producing rectal varices (which are not haemorrhoids — they lie above the dentate line and are portosystemic collaterals).
- Periumbilical region — the paraumbilical veins running in the falciform ligament (portal, ligamentum teres) anastomose with superficial epigastric and thoraco-epigastric veins (systemic), producing a radiating caput medusae and the audible Cruveilhier-Baumgarten murmur.
- Retroperitoneum — veins of the second part of the duodenum, pancreas, and bare areas of the liver and right kidney (e.g., retroduodenal, retroperitoneal, lumbar) dilate; these are typically silent but bleed at surgery.
- Bare areas of the liver — diaphragmatic and retroperitoneal venous communications. [1]
The five portosystemic anastomosis sites — OPERA
OPERA
left gastric (coronary) vein to azygos — varices, the lethal site
paraumbilical veins in falciform ligament to superficial epigastric — caput medusae and Cruveilhier-Baumgarten murmur
superior rectal (portal) to middle and inferior rectal (systemic) — rectal varices, NOT haemorrhoids
duodenal, pancreatic, bare-area veins — silent collaterals that bleed at surgery
diaphragmatic and retroperitoneal communications
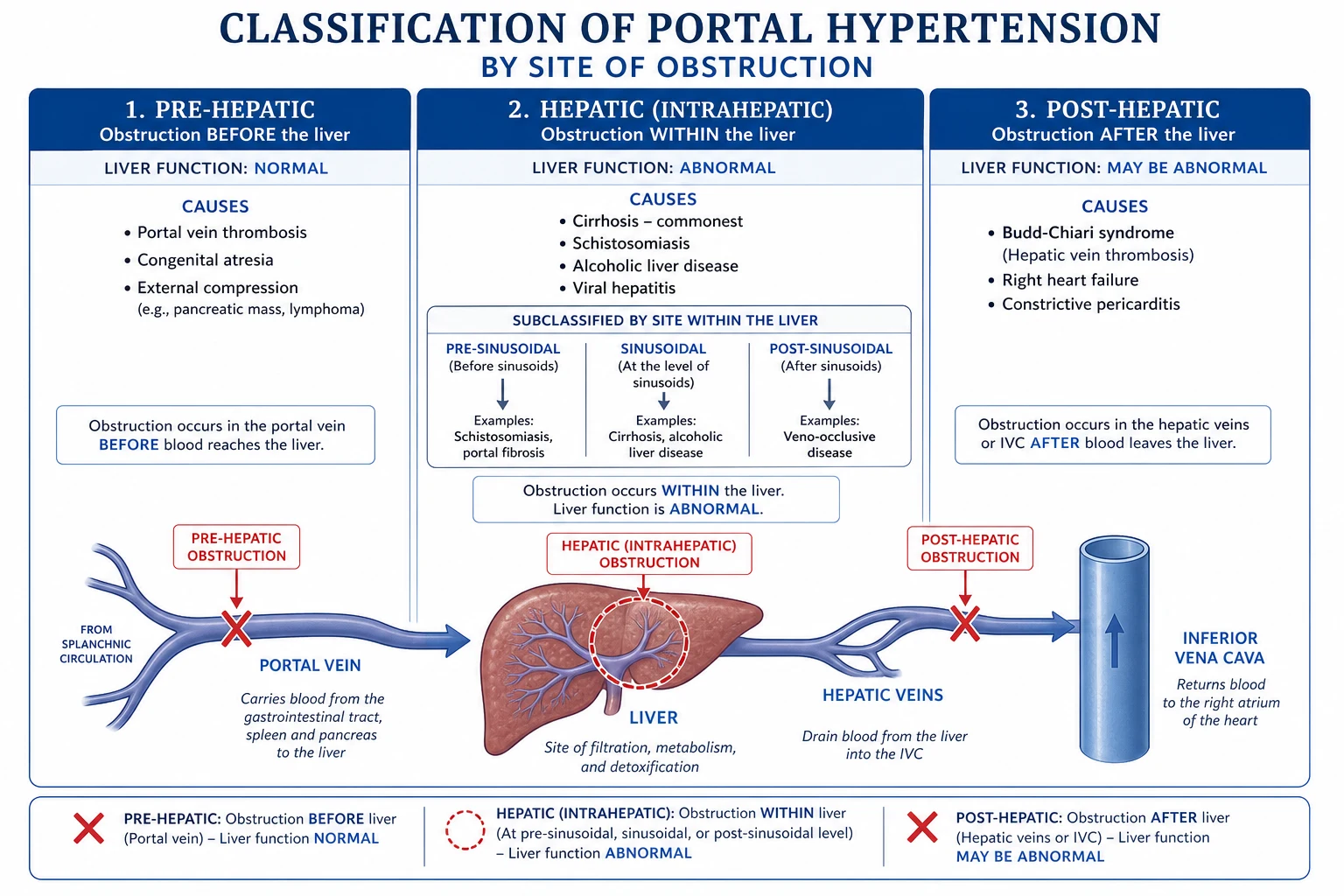
Classification
Portal hypertension is classified by the site of obstruction to portal flow into pre-hepatic, intra-hepatic, and post-hepatic. The intra-hepatic group is further split anatomically into pre-sinusoidal, sinusoidal, and post-sinusoidal, because the level of obstruction predicts whether liver function (and therefore synthetic function and coagulation) is preserved. [1]
Pre-hepatic
obstruction before the liver sinusoids
- Portal vein thrombosis (adults); cavernous transformation when chronic
- Splenic vein thrombosis (isolated, e.g. pancreatitis) — left-sided portal HTN
- Congenital portal vein atresia / stenosis
- External compression (pancreatic cancer, nodes, post-surgery)
- **Liver synthetic function is NORMAL**
Intra-hepatic (sinusoidal)
COMMONEST in the West
- **Cirrhosis** (alcohol, hepatitis B and C, NAFLD/NASH) — the dominant cause
- Sinusoidal obstruction from regenerative nodules and fibrosis
- **Liver function ABNORMAL** (low albumin, raised INR, bilirubin)
- HVPG rises because the obstruction is at the sinusoid
Intra-hepatic (pre-sinusoidal)
commonest worldwide
- **Schistosomiasis** (Schistosoma mansoni / japonicum eggs in portal venules) — the commonest cause globally
- Congenital hepatic fibrosis
- Nodular regenerative hyperplasia
- Sarcoidosis, granulomatous disease
- **Liver function often PRESERVED** — hepatocytes are intact
Post-hepatic
obstruction after the sinusoids
- **Budd-Chiari syndrome** — hepatic vein / IVC thrombosis
- Right-sided heart failure / tricuspid regurgitation
- **Constrictive pericarditis**
- Liver function may be abnormal; presents with painful hepatomegaly and ascites
Epidemiology & Risk Factors
Portal hypertension is, in most of the world, a complication of cirrhosis, and cirrhosis itself is among the top ten causes of death in the middle-aged. The global aetiological burden of cirrhosis is shifting: alcohol remains dominant in Europe and the Americas; chronic hepatitis B drives disease in sub-Saharan Africa, East and South-East Asia; hepatitis C is declining where direct-acting antivirals are available but persists where access is limited; and metabolic dysfunction-associated steatohepatitis (MASH, formerly NASH) tied to obesity and type 2 diabetes is the fastest-rising cause in the West.[1] Once cirrhosis is established, varices develop at roughly 6 to 8 percent per year, and about one-third of patients with varices will bleed. Each variceal haemorrhage carries 15 to 25 percent six-week mortality in modern series, and untreated survivors face a 60 percent one-year rebleed rate.
Portal hypertension — the numbers that matter
Schistosomiasis is the commonest cause of portal hypertension worldwide by absolute patient numbers. Schistosoma mansoni and S. japonicum eggs embolise to the pre-sinusoidal portal venules, where a granulomatous reaction obstructs flow before the sinusoid. Because hepatocytes remain intact, synthetic liver function is preserved (normal albumin and INR) and patients classically present with well-tolerated variceal bleeds and prominent splenomegaly but without the stigmata of chronic liver disease. Treatment is praziquantel 40 mg per kg as a single oral dose to kill the adult worm, plus variceal prophylaxis and eradication as for cirrhotic portal hypertension. India has small endemic pockets (Gujarat, Maharashtra) and larger burdens exist in sub-Saharan Africa, Egypt, Brazil, and China.[1]
Pathophysiology
Portal pressure is governed by Ohm's-law analogy: portal pressure equals portal venous blood flow multiplied by hepatic vascular resistance. Portal hypertension therefore arises from a rise in resistance, a rise in flow, or both — and in cirrhosis both occur.[2]
1. Increased intrahepatic resistance
The structural component is obvious: fibrous septa, regenerative nodules, and sinusoidal capillarisation physically distort and compress the vascular bed. But there is also a dynamic, reversible component. Injured hepatocytes and sinusoidal endothelial cells activate hepatic stellate cells, which trans-differentiate into contractile myofibroblast-like cells wrapped around the sinusoids. These cells constrict the sinusoid in response to vasoconstrictors (endothelin-1, angiotensin II, thromboxane) and relax in response to nitric oxide (NO). In cirrhosis the balance shifts toward vasoconstriction because intrahepatic NO bioavailability falls, even though systemic NO is high. This dynamic element is therapeutically important: it is why drugs that reduce portal inflow (beta-blockers) and procedures that decompress the system (TIPSS) work. [1]
2. Increased portal venous inflow (splanchnic vasodilation)
As portal pressure rises, the splanchnic circulation paradoxically vasodilates, driven by excess nitric oxide, glucagon, prostacyclin, and other vasodilators released from a hyperdynamic splanchnic endothelium. Vasodilation increases the volume of blood delivered to the portal system, perpetuating and amplifying the hypertension and producing the hyperdynamic circulation of cirrhosis — a bounding pulse, warm peripheries, low systemic vascular resistance, and a high cardiac output that ultimately decompensates into cardiomyopathy and hepatorenal failure. This is the rationale for non-selective beta-blockers, which reverse the splanchnic vasodilation (unopposed alpha-mediated vasoconstriction) and reduce inflow. [1]
Variceal rupture — Laplace's law
A varix behaves like a pressurised tube. Wall tension is proportional to the transmural pressure multiplied by vessel radius, divided by wall thickness (Laplace). A varix therefore ruptures when portal pressure (transmural pressure) is high, the varix is large, and its wall is thin — the basis of endoscopic grading by size and the presence of red wale signs and cherry-red spots, which mark areas of wall thinning. This is also why band ligation works: it obliterates the thin-walled varix and replaces it with a fibrotic nodule. [1]
Clinical Presentation
Portal hypertension declares itself through its four complications — variceal bleeding, ascites, splenomegaly, and encephalopathy — overlaid on the stigmata of chronic liver disease when the cause is cirrhosis. [1]
Variceal bleeding
oesophageal and gastric
- **Massive, painless haematemesis** or melaena; may precipitate hypovolaemic shock
- Oesophageal varices at the GOJ (left gastric to azygos) are the commonest source
- Gastric varices (short gastric / left gastric) bleed less often but harder to control
- Each episode carries 15 to 25 percent six-week mortality
- Bleeding risk rises with variceal size, red wale signs, and Child-Pugh class
Ascites
sinusoidal portal HTN plus hypoalbuminaemia
- Driven by sinusoidal hypertension (Starling shift), low albumin, and splanchnic vasodilation
- **Serum-to-ascites albumin gradient (SAAG) over 11 g/L** confirms a portal hypertensive cause
- Risk of spontaneous bacterial peritonitis (SBP)
- Refractory ascites signal advanced disease and hepatorenal risk
Splenomegaly and hypersplenism
venous congestion
- Enlarged spleen from chronic venous congestion — often the first physical sign
- **Thrombocytopaenia** (platelets under 100) from sequestration is a non-invasive marker of CSPH
- Leucopaenia and anaemia may coexist
- Isolated splenic vein thrombosis causes left-sided (sinistral) portal HTN with gastric varices
Hepatic encephalopathy
portosystemic shunting
- Nitrogenous toxins (ammonia) bypass the liver through collaterals to the brain
- Asterixis (flapping tremor), constructional apraxia, confusion progressing to coma
- Grade with West Haven criteria; minimal HE detectable on psychometric testing
- Precipitants: bleed, infection, constipation, sedatives, electrolyte disturbance, TIPSS
Signs of chronic liver disease (point to a cirrhotic cause)
When portal hypertension arises from cirrhosis, the examination also reveals the stigmata of hepatocellular failure: palmar erythema, spider naevi (in the distribution of the superior vena cava), gynaecomastia and testicular atrophy from impaired oestrogen metabolism, parotid enlargement, Dupuytren contracture, jaundice, fetor hepaticus, and asterixis. Caput medusae — a crown of dilated periumbilical veins radiating from a recanalised umbilical vein — with a venous hum and thrill over the umbilicus is the Cruveilhier-Baumgarten sign, virtually pathognomonic of portal hypertension.[1]
Atypical presentations
Examiners test the corners. Consider portal hypertension in a child with painless haematemesis (extrahepatic portal vein obstruction), in a young woman with sudden hepatomegaly and ascites (Budd-Chiari, often post-partum or in a myeloproliferative disorder), in a patient with a known pancreatic mass and isolated gastric varices (splenic vein thrombosis), and in chronic constrictive pericarditis presenting with ascites out of proportion to leg oedema. A patient who bleeds from varices with entirely normal liver synthetic function should prompt a search for a pre-sinusoidal (schistosomiasis) or pre-hepatic (portal vein thrombosis) cause. [1]
Differential Diagnosis
The acute presentation — upper gastrointestinal haemorrhage — generates a wide differential, of which varices are one cause. The chronic presentation — ascites with splenomegaly — generates another. [1]
| Condition | Key distinguishing feature |
|---|---|
| Oesophageal/gastric varices | Known chronic liver disease; massive painless haematemesis; signs of portal HTN; SAAG over 11 g/L if ascites present |
| Peptic ulcer (gastric/duodenal) | Epigastric pain, melena more than haematemesis, normal liver function, NSAID or H. pylori history |
| Mallory-Weiss tear | Post-emesis haematemesis after initial non-bloody vomit; normal liver usually |
| Gastric / oesophageal malignancy | Weight loss, dysphagia, anaemia; mass on endoscopy |
| Aorto-enteric fistula | Prior aortic graft, sentinel bleed then catastrophic haematemesis; urgent CT angiography |
| Dieulafoy lesion / angiodysplasia | Painless bleed, normal liver, diagnosis at endoscopy |
| Budd-Chiari syndrome | Acute painful hepatomegaly, ascites, tender liver; hepatic vein thrombosis on imaging |
| Right heart failure / constrictive pericarditis | Raised JVP, hepatomegaly, ascites; echocardiography diagnostic |
| Intra-abdominal malignancy with peritoneal deposits | SAAG under 11 g/L (exudate), cytology positive, fixed pelvic mass |
Clinical & Bedside Assessment
Begin with a focused general examination for the stigmata of chronic liver disease: pallor, jaundice, scratch marks, spider naevi, palmar erythema, gynaecomastia, testicular atrophy, parotid enlargement, Dupuytren contracture, clubbing. Smell for fetor hepaticus (sweet, musty, mercaptan breath). Assess hydration and the signs of shock (tachycardia, hypotension, cold peripheries, oliguria, confusion) in any bleeder. [1]
Abdominal examination looks for hepatosplenomegaly, ascites (shifting dullness, fluid thrill), caput medusae, and superficial abdominal wall collaterals. A venous hum over the umbilicus (Cruveilhier-Baumgarten) is pathognomonic. Test for asterixis (flapping tremor with wrists dorsiflexed) and constructional apraxia (Reitan trail, clock drawing) for encephalopathy. A digital rectal examination may reveal melaena, and anoscopy distinguishes true rectal varices (above the dentate line, blanching bluish) from haemorrhoids. [1]
Bedside pearl: what does a platelet count of 70 with splenomegaly tell you?
In a cirrhotic patient, thrombocytopaenia under 150 with splenomegaly is a robust non-invasive marker of clinically significant portal hypertension (CSPH) — Baveno VII endorses platelet count plus liver stiffness as a rule-out test for high-risk varices, sparing endoscopy when both are reassuring.[2]
Investigations
Investigation serves three purposes: confirm portal hypertension, define its cause and site, and grade severity for prognosis and transplant listing. [1]
Bloods. A full blood count shows thrombocytopaenia (hypersplenism), anaemia (blood loss, alcohol, folate deficiency, haemodilution), and leucopaenia. Liver function tests show a cholestatic or hepatocellular pattern depending on aetiology. Coagulation (INR) and albumin gauge synthetic function and feed the Child-Pugh and MELD scores. Renal function and electrolytes screen for hepatorenal syndrome and hyponatraemia. Send viral serology (HBsAg, anti-HCV), autoimmune and metabolic markers (ferritin, caeruloplasmin, alpha-1-antitrypsin, immunoglobulins, anti-mitochondrial antibody), and alpha-fetoprotein for hepatocellular carcinoma surveillance. [1]
Endoscopy (oesophago-gastro-duodenoscopy, OGD). The cornerstone for diagnosis and therapy. Varices are graded by size (small, medium, large) and inspected for red signs (red wale marks, cherry-red spots, haematocystic spots) that predict bleeding. Gastric varices are classified (Sarin: GOV1, GOV2, IGV1, IGV2). At the same session, band ligation or glue injection delivers therapy. [1]
Ultrasound with Doppler. First-line imaging. It shows liver nodularity and echotexture, portal vein patency and flow direction (hepatofugal, away from the liver, in advanced disease), splenomegaly, ascites, and screens for hepatocellular carcinoma. Portal vein thrombosis appears as an echogenic clot or absence of flow with cavernous transformation when chronic. Splenic vein patency should be specifically checked when isolated gastric varices are found. [1]
Cross-sectional imaging — CT and MR portography, contrast-enhanced ultrasound. Define vascular anatomy, confirm thrombosis, plan TIPSS or surgery, screen for hepatocellular carcinoma, and quantify collaterals. MR elastography and transient elastography (FibroScan) estimate liver stiffness, which — combined with platelet count — stratifies the probability of CSPH and high-risk varices non-invasively (Baveno VII).[2]
Hepatic venous pressure gradient (HVPG). The gold standard for diagnosing and grading portal hypertension. A balloon-tipped catheter is passed under fluoroscopy via the internal jugular vein to a hepatic vein; the wedged pressure reflects sinusoidal pressure and the free pressure the IVP. The difference is the HVPG. It is reproducible and prognostic and is the metric by which beta-blocker response is judged — but it is invasive and requires expertise, so it is reserved for diagnostic uncertainty, research, and assessing treatment response in specialised centres. [1]
Severity scores
Child-Pugh and MELD — the two prognostic scores
Child-Pugh combines bilirubin, albumin, INR, encephalopathy, and ascites to give a 5 to 15 score (A/B/C). MELD (Model for End-stage Liver Disease) uses bilirubin, INR, and creatinine (and sodium in MELD-Na); it predicts three-month mortality and drives transplant allocation — a MELD over 15 generally warrants transplant assessment. Both are reproduced verbatim in the references.[2]
Management — Resuscitation
Acute variceal bleeding is a medical emergency managed by a resuscitation bundle started before endoscopy and continued through it. The four pillars — airway, restrictive transfusion, vasoactive drug, and antibiotic — are delivered simultaneously, not sequentially, alongside plans for urgent endoscopy and a defined rescue pathway.[1][2]
Acute variceal bleed — the bundle (ABC plus TAB)
ABC-TAB
protect the airway; intubate early if encephalopathic or uncontrolled haemorrhage to prevent aspiration
high-flow oxygen; monitor SpO2
two large-bore cannulae, crossmatch 4 to 6 units, RESTRICTIVE transfusion — Hb target 70 to 80 g/L (over-transfusion raises portal pressure)
2 mg IV every 4 hours (splanchnic vasoconstriction; reduces portal pressure). Reduce to 1 mg q4h after 48 h; stop by day 5
ceftriaxone 1 g IV daily for up to 7 days — MANDATORY; reduces mortality and rebleeding by treating and preventing bacterial infection
urgent OGD within 12 hours for endoscopic variceal ligation (EVL) — the definitive first-line therapy
Two principles are examiner-favourite traps. First, transfusion is restrictive — a target haemoglobin of 70 to 80 g/L (liberal in active bleeding but not driven higher), because over-transfusion raises central venous and portal pressure, worsens bleeding, and impairs coagulation. Second, antibiotics are mandatory in every variceal bleed, independent of aspiration risk or ascites: infection (often bacteraemia or spontaneous bacterial peritonitis) accompanies up to half of bleeds, drives rebleeding, and short-term antibiotic prophylaxis (ceftriaxone 1 g IV daily for up to seven days) reduces mortality by roughly a third.[2]
Vasoactive drugs. Terlipressin, a synthetic vasopressin analogue, is the preferred agent in most of the world: 2 mg IV every four hours for the first 48 hours, then 1 mg every four hours, discontinued by day five. It causes splanchnic vasoconstriction and reduces portal inflow. A systematic review and meta-analysis of vasoactive agents (terlipressin or vasopressin versus octreotide or somatostatin) found similar control of bleeding and mortality between the two classes, with more adverse events (ischaemia, hyponatraemia) in the terlipressin group; octreotide (50 microgram bolus then 50 microgram per hour infusion) or somatostatin are acceptable alternatives where terlipressin is contraindicated (ischaemic heart disease, peripheral vascular disease, pregnancy).[4]
Self-test: name the four drugs and their doses in the acute variceal bleed bundle
The four pillars delivered simultaneously are (1) restrictive transfusion to a haemoglobin target of 70 to 80 g/L; (2) terlipressin 2 mg IV every 4 hours (or octreotide 50 mcg per hour infusion) for splanchnic vasoconstriction; (3) ceftriaxone 1 g IV daily (mandatory antibiotic prophylaxis for up to 7 days); and (4) endoscopic variceal ligation within 12 hours. Refractory bleeding escalates to balloon tamponade as a bridge then TIPSS.[1][2]
Refractory bleeding — the rescue ladder
If bleeding continues despite vasoactive drug and endoscopic therapy: [1]
- Balloon tamponade (Sengstaken-Blakemore or Minnesota tube, or the self-expanding Cook tube). The gastric balloon is inflated to tamponade the varix at the gastro-oesophageal junction. Use only as a bridge for a maximum of 24 hours while arranging definitive treatment; risks include aspiration, oesophageal ulceration and perforation, and pressure necrosis. Endotracheal protection should be in place.
- Self-expanding covered oesophageal metal stent — an alternative bridge that is easier to place and carries a lower perforation risk.
- Transjugular intrahepatic portosystemic shunt (TIPSS) — the definitive rescue therapy, decompressing the portal system by stenting a tract between the portal and hepatic veins. [1]
Management — Definitive and Stepwise
Primary prophylaxis (prevent the first bleed)
All patients with cirrhosis should be screened for varices. The aim of primary prophylaxis is to prevent the first variceal haemorrhage in those found to have medium or large varices, or small varices with red signs or Child-Pugh B/C disease. Baveno VII endorses a non-invasive rule-out (liver stiffness under 25 kPa and platelet count over 150) to spare endoscopy in low-risk patients.[2]
- Non-selective beta-blocker (NSBB). Propranolol 20 to 40 mg twice daily, titrated to reduce resting heart rate by about 25 percent to 55 to 60 bpm; nadolol 40 mg once daily (longer half-life, less CNS penetration); or carvedilol 6.25 mg once daily (additive alpha-1 blockade, greater portal-pressure reduction — now the preferred agent where tolerated). Mechanism: beta-2 blockade removes splanchnic vasodilatory tone, leaving unopposed alpha-mediated vasoconstriction, which cuts portal inflow and pressure; carvedilol also lowers intrahepatic resistance. Side effects: fatigue, hypotension, bronchospasm, erectile dysfunction; contraindicated in asthma, second-degree heart block, bradycardia.
- Endoscopic variceal ligation (EVL). First-line for large varices, or where NSBB are contraindicated or not tolerated. Bands are applied at two- to eight-week intervals until variceal eradication (typically two to four sessions). [1]
Secondary prophylaxis (prevent rebleed)
Every patient who survives a variceal bleed needs secondary prophylaxis — without it, 60 percent rebleed within a year. The evidence-based standard is combination therapy: NSBB plus serial EVL, which is superior to either modality alone.[2]
Transjugular intrahepatic portosystemic shunt (TIPSS)
TIPSS places a covered stent between an intrahepatic portal vein branch and a hepatic vein under fluoroscopic guidance via the internal jugular vein, decompressing the portal system. It controls refractory bleeding, refractory ascites, hepatic hydrothorax, and Budd-Chiari syndrome, and is the bridge to transplant. It controls bleeding in over 90 percent but causes new or worsening encephalopathy in 30 to 50 percent (by shunting nitrogenous toxins straight to the systemic circulation), and stenosis or thrombosis requires surveillance Doppler. Contraindications include severe heart failure, severe liver failure, polycystic liver disease, uncontrolled encephalopathy, and active sepsis. [1]
Pre-emptive (early) TIPSS — Baveno VII. For patients at high risk of treatment failure after an acute variceal bleed — Child-Pugh B with active bleeding at endoscopy, or Child-Pugh C scoring 10 to 13 — a TIPSS placed within 72 hours of admission reduces treatment failure, rebleeding, and mortality. This recommendation rests on the landmark Early TIPS trial (Garcia-Pagan 2010): in 63 high-risk patients randomised within 24 hours, early covered-stent TIPS within 72 hours gave a 97 percent one-year probability of remaining free of the composite endpoint (failure to control bleeding or rebleeding) versus 50 percent with pharmacotherapy plus EVL, and improved one-year survival (86 percent versus 61 percent).[3]
Surgical shunts (now rarely used)
Historically the mainstay of portal decompression, surgical shunts are now largely supplanted by TIPSS (less invasive, lower peri-procedural mortality) and are reserved for failed TIPSS, TIPSS not technically feasible, or specialised centres with surgical expertise: [1]
- Distal splenorenal (Warren) shunt — selectively decompresses gastro-oesophageal varices into the left renal vein while preserving mesenteric-portal perfusion; lowest encephalopathy rate of the surgical shunts.
- Mesocaval shunt — jugular or prosthetic graft between SMV and IVC.
- Portocaval shunt — side-to-side or end-to-side; the most effective decompression but the highest encephalopathy rate. [1]
Devascularisation procedures (oesophageal transection, Sugiura-Futagawa) are historical salvage options now virtually obsolete in centres with TIPSS. [1]
Liver transplant
The only definitive cure for portal hypertension arising from cirrhosis. Reserved for decompensated cirrhosis (Child-Pugh C, MELD over 15, or a decompensating event such as refractory ascites, recurrent encephalopathy, or hepatorenal syndrome). Allocation is by MELD/MELD-Na score. Portal hypertension from pre-hepatic or pre-sinusoidal causes (portal vein thrombosis, schistosomiasis) does not require transplant — the liver is structurally preserved. [1]
Management of ascites
Ascites is managed in a stepwise ladder keyed to severity:[2]
- Sodium restriction to under 88 mmol (2 g) per day and fluid restriction only if hyponatraemic (sodium under 120 to 125).
- Diuretics — spironolactone plus furosemide in a 100:40 ratio (e.g. spironolactone 100 mg and furosemide 40 mg each morning), titrated upward to a maximum of 400 mg and 160 mg respectively, targeting 0.5 kg per day weight loss (up to 1 kg per day if peripheral oedema). The ratio maintains normokalaemia.
- Large-volume paracentesis (LVP) for tense or refractory ascites — drain over 5 litres in one sitting, with 6 to 8 g of intravenous albumin per litre removed if over 5 litres, to prevent post-paracentesis circulatory dysfunction and hepatorenal syndrome.
- TIPSS for refractory ascites (diuretic-resistant or diuretic-intractable) in selected patients.
- Liver transplant for refractory ascites as a decompensating event. [1]
Management of hepatic encephalopathy
Treatment combines precipitant removal with ammonia-lowering therapy:[2]
- Identify and treat the precipitant — infection (including SBP), gastrointestinal bleeding, constipation, dehydration, electrolyte disturbance (hypokalaemia), sedatives/opioids, TIPSS, and worsening liver failure. This alone resolves many episodes.
- Lactulose 15 to 30 mL orally two to three times daily, titrated to two to three soft stools per day. The disaccharide is fermented by colonic bacteria to organic acids that lower colonic pH, convert absorbable ammonia to non-absorbable ammonium, and have a cathartic effect.
- Rifaximin 550 mg twice daily — a minimally absorbed antibiotic that reduces ammonia-producing gut flora; add to lactulose for recurrent or persistent encephalopathy and for secondary prevention.
- Supportive care — airway protection in grade III to IV encephalopathy, nutrition with adequate protein (do not restrict protein), correction of electrolytes. [1]
Specific Subtypes and Scenarios
Portal vein thrombosis (pre-hepatic). Acute portal vein thrombosis presents with abdominal pain or is found incidentally; anticoagulation (low-molecular-weight heparin transitioning to warfarin or a direct oral anticoagulant for at least six months) aims for recanalisation and prevents extension. Chronic thrombosis produces cavernous transformation (a tangle of periportal collaterals) and portal hypertension with varices but normal liver synthetic function; management focuses on variceal prophylaxis and eradication. Anticoagulation is safe and beneficial even in cirrhotic portal vein thrombosis when varices are adequately treated. [1]
Budd-Chiari syndrome (post-hepatic). Hepatic vein or IVC thrombosis, classically in a young woman with a myeloproliferative disorder (JAK2 mutation), on oral contraceptives, or post-partum. The classic triad is abdominal pain, hepatomegaly, and ascites. Diagnosis is by Doppler and CT/MR venography showing hepatic vein occlusion. Treatment is anticoagulation, angioplasty or stenting of short stenoses, TIPSS as the default decompressive procedure, and liver transplant for fulminant or end-stage disease. [1]
Splenic vein thrombosis (sinistral, left-sided portal hypertension). Usually a complication of pancreatitis or pancreatic cancer. Isolated gastric (fundal) varices develop with normal liver function. Splenectomy is curative. [1]
Gastric varices. Bleed less often but more severely than oesophageal varices and are harder to band. GOV2 and IGV1 (fundal varices) are treated with cyanoacrylate (glue) injection as first-line endoscopic therapy; TIPSS is the preferred rescue and is used earlier than for oesophageal varices. Balloon-occluded retrograde transvenous obliteration (BRTO) is an alternative where there is a spontaneous gastrorenal shunt. [1]
Schistosomiasis (pre-sinusoidal). Covered above — preserved liver function, prominent splenomegaly, well-tolerated bleeds. Treat the parasite with praziquantel and manage varices as for cirrhosis; surgical shunts (distal splenorenal) remain a reasonable option where TIPSS is unavailable because the liver tolerates shunting well. [1]
Complications and Pitfalls
Variceal bleeding. Despite modern therapy, 15 to 25 percent six-week mortality per episode. Sixty percent rebleed within a year without secondary prophylaxis. Bleeding precipitates encephalopathy, infection, and hepatorenal syndrome.[1]
Hepatic encephalopathy. May follow a bleed (protein load), infection, TIPSS (30 to 50 percent incidence), or arise spontaneously in decompensation. Managed as above. Recurrent encephalopathy post-TIPSS may require shunt reduction. [1]
Spontaneous bacterial peritonitis (SBP). Infection of ascitic fluid without an obvious source. Presents with fever, abdominal pain, worsening encephalopathy, or simply deterioration. Diagnostic tap: an ascitic polymorphonuclear count over 250 cells per cubic millimetre defines SBP. Treat with cefotaxime 2 g IV every eight hours (or ceftriaxone 2 g IV daily) for five to seven days, with albumin 1.5 g per kg on day one and 1 g per kg on day three to prevent hepatorenal syndrome. Secondary prophylaxis with oral norfloxacin 400 mg daily or ciprofloxacin 500 mg daily; primary prophylaxis is given to high-risk groups (low ascitic protein, prior SBP, acute GI bleed). [1]
Hepatorenal syndrome (HRS-AKI). Functional renal failure from intense splanchnic vasodilation reducing effective circulating volume and renal perfusion; the kidneys are histologically normal. Diagnosed by the ICA criteria (rise in creatinine, no response to albumin challenge, exclusion of other causes). HRS-AKI (formerly type 1) is rapid and fatal untreated; treated with terlipressin plus albumin (or noradrenaline in ICU). HRS with refractory ascites (formerly type 2) is indolent. Definitive treatment is liver transplant. [1]
Other. Hepatopulmonary syndrome (intrapulmonary shunting, hypoxaemia, orthodeoxia) and portopulmonary hypertension (pulmonary arterial hypertension from portosystemic shunting) are pulmonary vascular complications. Hepatic hydrothorax (usually right-sided) and umbilical hernia with risk of rupture are mechanical complications of ascites. Gastric antral vascular ectasia and portal hypertensive gastropathy cause chronic occult bleeding. [1]
Classic pitfalls
- Over-transfusing a variceal bleed — raises portal pressure and worsens bleeding.
- Forgetting antibiotics — a mortality-reducing, evidence-mandated component of the bundle.
- Mistaking rectal varices for haemorrhoids — varices lie above the dentate line, are portosystemic collaterals, and bleed into the portal system.
- Misattributing ascites with a low SAAG to portal hypertension — a SAAG under 11 g/L is peritoneal (malignancy, TB), not portal.
- Delaying TIPSS in a high-risk Child-Pugh B/C bleeder who qualifies for pre-emptive TIPSS within 72 hours.
- Restricting protein in encephalopathy — protein restriction is obsolete and worsens sarcopenia; treat the precipitant instead. [1]
Prognosis and Disposition
Variceal bleeding. Six-week mortality of 15 to 25 percent per episode in modern series, lower with adherence to the full bundle (restrictive transfusion, vasoactive drug, antibiotic, EVL, and pre-emptive TIPSS where indicated). Survivors need structured secondary prophylaxis and surveillance endoscopy. [1]
Cirrhosis by Child-Pugh class (approximate one- and two-year survival): A 100 percent then 85 percent; B 80 percent then 60 percent; C 45 percent then 35 percent. MELD predicts three-month mortality more precisely and drives transplant allocation. [1]
TIPSS. Controls bleeding in over 90 percent and refractory ascites in the majority; one-year survival is 60 to 80 percent, limited by the underlying liver disease. Thirty to 50 percent develop encephalopathy. [1]
Pre-hepatic and pre-sinusoidal causes (portal vein thrombosis, schistosomiasis, congenital hepatic fibrosis) carry a far better prognosis because hepatocellular function is preserved; patients tolerate bleeds well and live normal spans with variceal control. [1]
Disposition. Every acute variceal bleed is admitted to a unit with 24-hour endoscopy and interventional radiology. High-risk patients (Child-Pugh B active bleed, Child-Pugh C 10 to 13) are flagged early for pre-emptive TIPSS. Survivors are enrolled in a surveillance and secondary prophylaxis programme, with transplant referral when MELD exceeds 15 or a decompensating event occurs. [1]
Special Populations
Children (extrahepatic portal vein obstruction). The commonest cause of portal hypertension in children, usually from neonatal portal vein thrombosis (cannulation, sepsis). Liver function is normal; presentation is with variceal bleeding, often well tolerated. Managed conservatively (EVL, beta-blockers). The Meso-Rex bypass (mesenteric-to-left-portal-vein autologous jugular vein graft) restores physiological portal inflow and is the definitive treatment for refractory bleeding in expert centres. [1]
Pregnancy. Portal hypertension in pregnancy carries a higher risk of variceal bleeding because of increased blood volume and intra-abdominal pressure. Varices should be screened and eradicated before conception where possible. Terlipressin is avoided (uterine vasospasm); octreotide or endoscopic therapy are preferred in pregnancy. TIPSS and surgery are deferred where possible. Vaginal delivery is acceptable with good pain control; caesarean is for obstetric indications. [1]
The anticoagulated patient. Anticoagulation is not contraindicated in cirrhosis once varices are treated; portal vein thrombosis on anticoagulation should be managed jointly with hepatology. Reverse warfarin with vitamin K and prothrombin complex concentrate for an acute bleed; direct oral anticoagulants have specific reversal strategies. [1]
The elderly and comorbid. Frail, elderly patients tolerate bleeds poorly; beta-blocker dosing should start low and titrate slowly; pre-emptive TIPSS decisions weigh encephalopathy risk against bleeding risk. [1]
Evidence, Guidelines and Regional Differences
Baveno VII consensus (2022). The current international standard for portal hypertension, "Personalized Care for Portal Hypertension", supersedes Baveno VI. Key recommendations: CSPH is defined non-invasively by liver stiffness over 25 kPa (rule-in) or under 15 kPa with platelets over 150 (rule-out); NSBBs (preferably carvedilol) are first-line for CSPH; EVL for large varices or NSBB intolerance; the acute bleed bundle includes vasoactive drug, antibiotic, and EVL with pre-emptive TIPSS for high-risk patients; secondary prophylaxis combines NSBB and EVL; and aetiological cure (antivirals, alcohol abstinence, weight loss) can reverse portal hypertension in early disease.[2] A 2025 review traces the evolution of the Baveno guidelines from invasive HVPG measurement toward non-invasive elastography and personalised surveillance, confirming endoscopic band ligation and NSBB as the cornerstones and early TIPSS as the rescue standard.[1]
The Early TIPS trial (Garcia-Pagan, NEJM 2010). The pivotal randomised trial establishing pre-emptive TIPSS: 63 high-risk cirrhotic patients (Child-Pugh C under 14, or Child-Pugh B with active bleeding) randomised within 24 hours to covered-stent TIPSS within 72 hours versus pharmacotherapy plus EVL. Early TIPSS gave a 97 percent versus 50 percent one-year freedom from failure-to-control-bleeding-or-rebleeding and improved one-year survival (86 percent versus 61 percent), without excess serious adverse events.[3]
Vasoactive agent meta-analysis (Huaringa-Marcelo 2021). Twenty-one RCTs comparing terlipressin/vasopressin with octreotide/somatostatin found no difference in mortality, bleeding control, rebleeding, transfusion, or length of stay; the terlipressin group had more adverse events. The choice of vasoactive agent is therefore often driven by availability, cost, and contraindications rather than efficacy.[4]
Regional differences. In India and across the tropics, schistosomiasis and viral hepatitis B and C are major drivers of portal hypertension, and alcohol is rising. Access to TIPSS is limited to major tertiary centres, so EVL and beta-blockers are the most widely available interventions and the Sengstaken-Blakemore tube may be the only temporising option in resource-limited settings. Public-health programmes — hepatitis B vaccination, praziquantel mass treatment for schistosomiasis, and harm reduction for alcohol — are reducing the burden at population level. Nodular regenerative hyperplasia and congenital hepatic fibrosis are uncommon intra-hepatic pre-sinusoidal causes that, like schistosomiasis, preserve liver function and present with variceal bleeding.[1]
Exam Pearls
- HVPG: over 5 = portal HTN; over 10 = clinically significant; over 12 = bleed risk; over 16 = high mortality. A fall to under 12 or by over 20 percent on a beta-blocker defines a responder.[1]
- Acute variceal bleed bundle: restrictive transfusion (Hb 70 to 80) plus terlipressin plus mandatory antibiotics plus EVL within 12 hours; refractory bleed escalates to balloon tamponade bridge then TIPSS.[2]
- Antibiotics (ceftriaxone 1 g IV daily) are mandatory in every variceal bleed — they reduce mortality by about a third by treating and preventing infection.[2]
- Pre-emptive TIPSS within 72 hours for Child-Pugh B with active bleed or Child-Pugh C scoring 10 to 13 — the Early TIPS trial showed improved survival.[3]
- NSBB mechanism: beta-2 blockade leaves unopposed alpha-mediated splanchnic vasoconstriction, cutting portal inflow; carvedilol adds alpha-1 blockade and lowers intrahepatic resistance.
- Sengstaken-Blakemore tube is a BRIDGE only — maximum 24 hours; risks aspiration, oesophageal perforation, pressure necrosis.[1]
- Ascites: sodium restriction, then spironolactone plus furosemide 100:40, then large-volume paracentesis with albumin (6 to 8 g per litre over 5 L), then TIPSS for refractory.
- Encephalopathy: treat the precipitant, lactulose titrated to two to three stools, rifaximin 550 mg BD for prevention.[2]
- SBP: ascitic PMN over 250 — cefotaxime plus albumin; secondary prophylaxis with norfloxacin.
- Schistosomiasis is the commonest cause worldwide; pre-sinusoidal, liver function preserved, praziquantel 40 mg/kg.[1]
- Rectal varices are NOT haemorrhoids — they lie above the dentate line and are portosystemic collaterals.
- SAAG over 11 g/L = portal hypertensive ascites; under 11 g/L = peritoneal (malignancy, TB).
- Portal vein = superior mesenteric vein plus splenic vein, behind the neck of the pancreas.
Exam application bank (NEET-PG / INICET)
One-line answer
Portal hypertension is sustained elevation of the portal venous pressure gradient (HVPG over 5 mmHg). Commonest cause worldwide is cirrhosis (sinusoidal); the commonest pre-sinusoidal cause globally is schistosomiasis. Four consequences: varices (oesophageal and gastric), ascites, splenomegaly with hypersplenism, and hepatic encephalopathy. Acute variceal bleed: resuscitate with restrictive transfusion (Hb target 70 to 80), terlipressin 2 mg IV every 4 h, ceftriaxone 1 g IV daily (mandatory antibiotic prophylaxis), and endoscopic band ligation within 12 h. Refractory bleeding: balloon tamponade (Sengstaken-Blakemore) as a bridge, then TIPSS. Primary prophylaxis: non-selective beta-blocker (propranolol, nadolol, carvedilol) or EVL. Secondary prophylaxis: beta-blocker plus serial EVL. HVPG over 10 = clinically significant; over 12 = bleeding risk; over 16 = high mortality. [1]
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Portal Hypertension.
References
- [1]Brzdek M, Dobrowolska K, Janczura J, et al. Advances in portal hypertension management: Evolution of the Baveno guidelines World J Gastroenterol, 2025.PMID 41024757
- [2]de Franchis R, Bosch J, Garcia-Tsao G, Reiberger T, Ripoll C; Baveno VII Faculty. Baveno VII - Renewing consensus in portal hypertension J Hepatol, 2022.PMID 35120736
- [3]Garcia-Pagan JC, Caca K, Bureau C, et al. Early use of TIPS in patients with cirrhosis and variceal bleeding N Engl J Med, 2010.PMID 20573925
- [4]Huaringa-Marcelo J, Huaman MR, Branez-Condorena A, et al. Vasoactive Agents for the Management of Acute Variceal Bleeding: A Systematic Review and Meta-analysis J Gastrointestin Liver Dis, 2021.PMID 33723542