Haematology · Haematology
Anaemia
Also known as Anaemia · Low haemoglobin · Iron deficiency anaemia · Megaloblastic anaemia · Nutritional anaemia
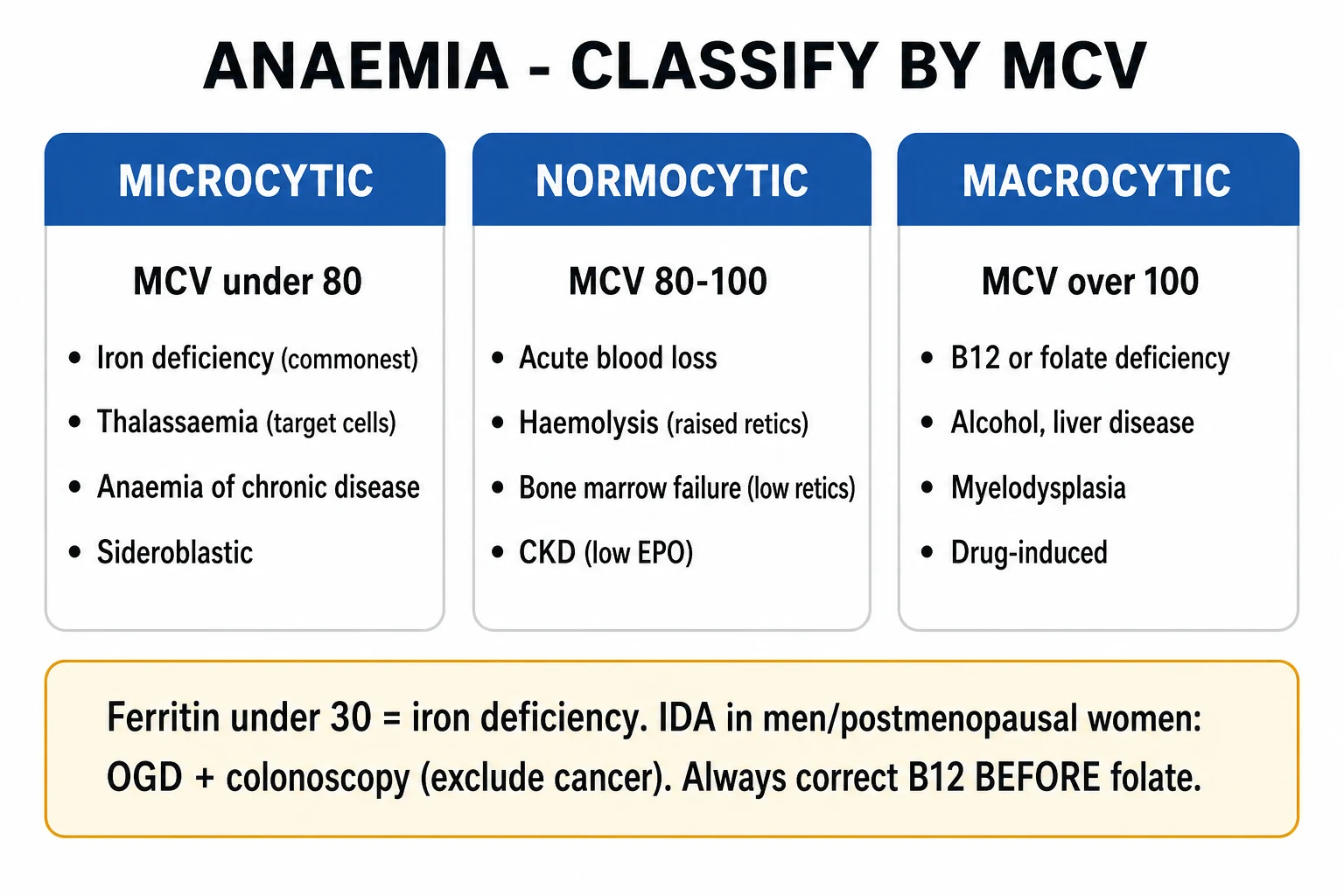
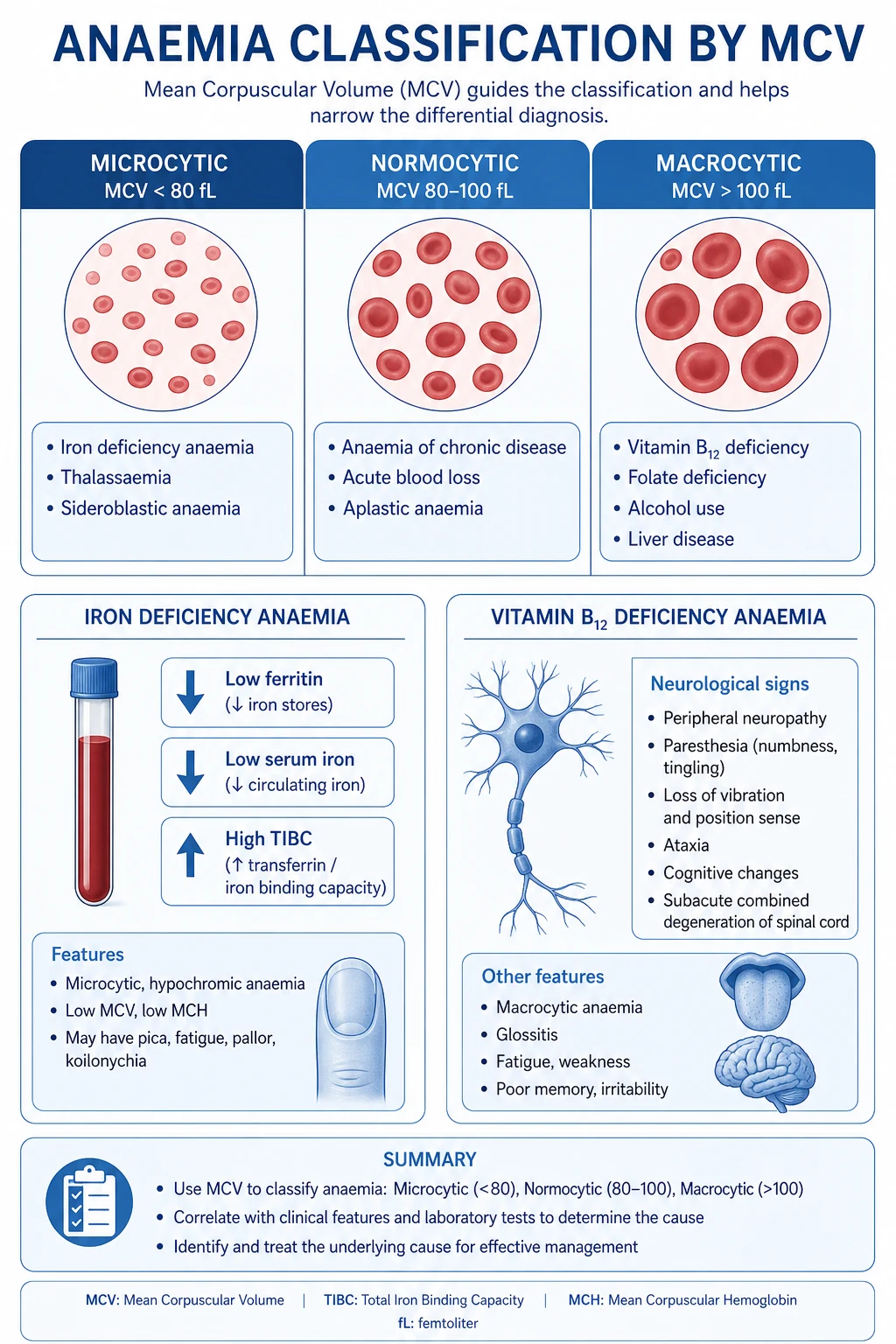
Anaemia (WHO: Hb under 130 g/L men, under 120 g/L non-pregnant women, under 110 g/L pregnant women and children 6 months to 5 years) is not a diagnosis but a sign of disease. The examinable skill is the MCV-based framework: microcytic (under 80 fL — iron deficiency, thalassaemia, anaemia of chronic disease, sideroblastic, lead), normocytic (80 to 100 fL — acute blood loss, anaemia of chronic disease, haemolysis, aplastic, mixed deficiency) and macrocytic (over 100 fL — megaloblastic B12/folate, alcohol, liver disease, hypothyroid, MDS, drugs). The reticulocyte count splits causes into underproduction vs destruction/loss. Iron deficiency (most common worldwide): low ferritin, low iron, high transferrin/TIBC, low % saturation, high sTfR. Megaloblastic: hypersegmented neutrophils, macro-ovalocytes, pancytopenia, raised LDH and indirect bilirubin, intrinsic factor antibodies (pernicious), neurological signs with B12. Treat the cause: oral ferrous sulphate 200 mg TDS ( elemental iron 65 mg per tablet) for 3 to 6 months after Hb normalises; IV ferric carboxymaltose if intolerant/malabsorbing; IM hydroxocobalamin loading (BSH regimen) for B12 deficiency; oral folic acid 5 mg daily for folate deficiency. NEVER give folate alone in B12 deficiency (precipitates subacute combined degeneration). Transfuse at Hb under 70 g/L, under 80 g/L if symptomatic/elderly/cardiac, with single-unit prescribing in older patients.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Exam tags
Red flags
Overview & Definition
Anaemia is defined by the World Health Organization as a haemoglobin concentration below the lower limit of the normal range for age, sex and physiological state.[1]
WHO haemoglobin thresholds (sea level)[1]
| Population | Anaemia (Hb, g/L) |
|---|---|
| Men (15+ years) | under 130 |
| Non-pregnant women (15+ years) | under 120 |
| Pregnant women | under 110 |
| Children 6 months to 5 years | under 110 |
| Children 5 to 11 years | under 115 |
| Children 12 to 14 years | under 120 |
Why "anaemia" is a sign, not a diagnosis
Haemoglobin is the final common pathway of erythropoiesis, iron homeostasis, haem synthesis, red-cell survival and blood loss. A low value tells you that something is wrong; the MCV, reticulocyte count and film tell you what. The single biggest cognitive error in anaemia is to chase the number with iron or transfusion before asking why — particularly dangerous in microcytic anaemia of a man or post-menopausal woman, where the assumption of iron deficiency must trigger a search for occult gastrointestinal blood loss until proven otherwise.[1]
Functional consequences
Haemoglobin carries ~1.34 mL of oxygen per gram. A fall in Hb reduces arterial oxygen content (CaO2). The body compensates by: (1) increasing cardiac output (tachycardia, hyperdynamic circulation, flow murmurs), (2) increasing 2,3-bisphosphoglycerate (2,3-BPG) in erythrocytes which right-shifts the oxyhaemoglobin dissociation curve (raised P50, easier O2 unloading to tissues), and (3) renal hypoxia driving erythropoietin (EPO) release from interstitial fibroblasts, stimulating marrow erythropoiesis. When compensation fails, symptoms of tissue hypoxia appear.[1]
Classification
There are two complementary classifications — every anaemic patient must be classified by both. [1]
Morphological classification (by MCV)
| MCV (fL) | Category | Principal causes |
|---|---|---|
| under 80 | Microcytic | Iron deficiency, thalassaemia, anaemia of chronic disease (some), sideroblastic, lead poisoning |
| 80 to 100 | Normocytic | Acute blood loss, early iron deficiency, anaemia of chronic disease, haemolysis, aplastic/marrow infiltration, mixed deficiency |
| over 100 | Macrocytic | Megaloblastic (B12, folate, drugs); non-megaloblastic (alcohol, liver disease, hypothyroid, MDS, reticulocytosis, artefact/cold agglutinins) |
Kinetic classification (by mechanism)
- Decreased production (reticulocytes inappropriately low for the degree of anaemia) — substrate/hormone deficiency (iron, B12, folate, EPO), marrow failure (aplastic, infiltration, myelofibrosis), chronic disease (hepcidin block).
- Increased destruction — haemolysis (reticulocytes high) — hereditary (membrane, enzyme, haemoglobinopathies) vs acquired (immune, microangiopathic, infections, drugs).
- Blood loss (reticulocytes high once marrow responds, ~5 to 7 days after acute bleed) — acute (trauma, GI, obstetric) or chronic (menorrhagia, GI, hookworm). [1]
Bedside three-step diagnostic algorithm
- Step 1 — Confirm anaemia (Hb below threshold); check MCV.
- Step 2 — Reticulocyte count (or reticulocyte production index, RPI): low = underproduction; high = haemolysis or bleeding.
- Step 3 — Targeted tests by MCV class (iron studies / haemolysis screen / B12-folate / marrow).[1]
Epidemiology & Risk Factors
Anaemia is the commonest haematological disorder worldwide, affecting an estimated 1.6 to 1.9 billion people (~25 to 30% of the global population); iron deficiency is responsible for about half of all cases.[1]
Demographic and risk-factor profile
- Pre-school children (under 5) — highest prevalence (~40 to 45% globally); rapid growth, low dietary iron, recurrent infection, hookworm (in endemic regions).
- Pregnant women — ~30 to 40% prevalence; iron demands of fetus and expanded maternal blood volume; folate demand rises sharply in the third trimester.
- Women of reproductive age — menstruation, repeated pregnancies, dietary deficiency.
- Older adults (>65 years) — prevalence rises again; causes are more often multifactorial (chronic disease, GI blood loss from cancer/NSAIDs, B12 deficiency, CKD).
- Patients with chronic disease — CKD (low EPO), inflammatory bowel disease, rheumatoid arthritis (ACD), heart failure, malignancy.
- Dietary/lifestyle — strict vegan/vegetarian (B12, iron), alcohol excess (folate, marrow toxicity, GI blood loss), pica.
- Geography/ethnicity — thalassaemia (Mediterranean, Middle East, South Asia, South-East Asia), sickle-cell trait/disease (sub-Saharan Africa, India, Middle East), G6PD deficiency (malarial belts), hookworm/malaria (tropics).
- Drugs — NSAIDs/aspirin/anticoagulants (GI blood loss), PPIs and H2 blockers (reduced acid → impaired iron), metformin (B12), methotrexate/trimethoprim/phenytoin (folate), chemotherapy, sulfasalazine.
- Postsurgical — gastrectomy, ileal resection, bariatric surgery (B12 and iron malabsorption).[1][1]
Anaemia — epidemiology at a glance
Pathophysiology
Erythropoiesis and red-cell lifespan
Erythroid precursors mature in the marrow over ~7 days under EPO drive, extruding the nucleus to become reticulocytes, then mature erythrocytes (lifespan ~120 days). A normal marrow replaces the ~1% of red cells lost daily and can increase output 6 to 8 fold under sustained EPO stimulation. A reticulocyte count above ~2% (corrected for anaemia, RPI over 2) therefore indicates the marrow is responding — pointing to haemolysis or blood loss, not underproduction.[1]
Iron homeostasis and the hepcidin axis
The body has no regulated mechanism to excrete iron (~1 to 2 mg lost daily in desquamated cells); balance is controlled at absorption (duodenal enterocytes via DMT1 and ferroportin). Iron is delivered to the marrow by transferrin, the iron transport protein; total iron-binding capacity (TIBC) measures circulating transferrin. Stored iron is held as ferritin (intracellular, soluble, the storage protein) and haemosiderin (insoluble, in macrophages). Serum ferritin reflects stores (1 ng/mL ~= 8 to 10 mg stored iron) but is an acute-phase reactant, so it is falsely elevated in inflammation, infection, malignancy and liver disease.[1]
Hepcidin, a peptide hormone produced by the liver, is the master regulator of iron. It binds ferroportin on enterocytes, macrophages and placenta, causing its internalisation and degradation — thereby blocking iron export into plasma. Conditions that raise hepcidin (inflammation via IL-6) trap iron in macrophages and enterocytes → functional iron deficiency = anaemia of chronic disease (low serum iron, low/normal TIBC, high ferritin). Conditions that lower hepcidin (iron deficiency, hypoxia, erythropoietic drive, pregnancy) increase iron absorption and release.[1]
Haem synthesis and the megaloblastic mechanism
Red cells are produced by repeated DNA synthesis, which requires vitamin B12 (cobalamin) and folate as coenzymes for thymidylate and purine synthesis. Deficiency of either impairs DNA replication while RNA (and hence protein) synthesis continues — producing nuclear-cytoplasmic asynchrony (large immature nuclei, abundant cytoplasm). The marrow shows megaloblastic change (giant metamyelocytes, large erythroblasts) and the blood shows macro-ovalocytes and hypersegmented neutrophils (5 or more lobes, or at least 5% with 6 lobes). Ineffective erythropoiesis causes intramedullary destruction → raised LDH, raised indirect bilirubin, low haptoglobin and a pancytopenia (white cells and platelets also affected).[1]
B12 vs folate — absorption and the neurological lesion
- Vitamin B12 (cobalamin) — daily requirement ~1 to 2 micrograms; body stores 2 to 5 mg (enough for 3 to 5 years). Bound in food to proteins; released by gastric acid and pepsin, then bound to R-binder (haptocorrin) in the stomach. In the duodenum, pancreatic enzymes degrade R-binder and B12 binds intrinsic factor (IF) secreted by gastric parietal cells. The B12-IF complex binds cubilin-amnionless receptor in the terminal ileum for absorption. Deficiency causes megaloblastic anaemia AND neurological damage — subacute combined degeneration of the spinal cord (demyelination of dorsal and lateral columns, with loss of proprioception/vibration, spasticity, extensor plantars), peripheral neuropathy, optic atrophy and cognitive/psychiatric change. The neurology relates to impaired methylation of myelin basic protein via methionine synthase (B12-dependent) and accumulation of methylmalonic acid.[1]
- Folate — daily requirement ~50 to 200 micrograms; body stores only 5 to 20 mg (enough for ~4 months). Absorbed mainly in the proximal jejunum (no IF required). Deficiency produces the same megaloblastic anaemia but NO neurological signs.[1]
Haemolysis mechanism
Red-cell destruction occurs intravascularly (free haemoglobin released; depleted haptoglobin; haemoglobinuria, methaemalbumin) or extravascularly (macrophages of spleen/liver; raised unconjugated bilirubin and LDH; spherocytes if antibody-coated). The marrow responds with reticulocytosis within 5 to 7 days. See the haemolytic-anaemia topic for the full mechanism (membrane, enzyme, haemoglobinopathy, immune, microangiopathic).
Clinical Presentation
Anaemia is often asymptomatic until Hb falls below ~80 to 90 g/L in previously healthy adults, but symptoms appear earlier in the elderly, those with cardiac/respiratory disease, or with rapid onset (the body has not had time to compensate).[1]
General symptoms of anaemia (any cause)
- Fatigue, weakness, lethargy, reduced exercise tolerance — reduced O2 delivery to muscle.
- Dyspnoea on exertion (progressing to dyspnoea at rest when severe).
- Palpitations, exertional chest pain, syncope or near-syncope.
- Light-headedness, headache, tinnitus, difficulty concentrating.
- Cold extremities (peripheral vasoconstriction).
General signs
- Pallor of conjunctivae, palmar creases, face, nail beds, oral mucosa — clinical but insensitive/specific only at severe Hb (under 70 to 80 g/L).
- Tachycardia, wide pulse pressure, hyperdynamic precordium — compensatory high-output state.
- Systolic flow murmur (ejection, pulmonary area; soft, no radiation) and occasionally a venous hum or carotid bruit.
- Tachypnoea; signs of high-output cardiac failure if severe/chronic (oedema, basal crackles, raised JVP).
- Koilonychia (spoon nails — brittle, concave) in chronic iron deficiency. [1]
Features pointing to a specific cause
- Iron deficiency — koilonychia, angular cheilitis/stomatitis, atrophic glossitis (smooth sore tongue), pica (craving for ice/earth/starch — pagophagia for ice is highly specific), Plummer-Vinson syndrome (dysphagia, oesophageal web, glossitis — risk of post-cricoid cancer), beeturia.
- B12 deficiency — glossitis (beefy red sore tongue), neurological: peripheral neuropathy (paraesthesia, numbness, loss of vibration and joint position sense in the lower limbs first), subacute combined degeneration (spastic paraparesis, extensor plantars, Romberg positive, sensory ataxia), optic atrophy, cognitive impairment/dementia, mood disturbance/psychosis ("megaloblastic madness"), autonomic and bladder/bowel dysfunction. Also mild jaundice (lemon-yellow) from ineffective erythropoiesis, and melanin pigmentation of knuckles.
- Folate deficiency — glossitis and megaloblastic anaemia as above, but no neurological signs; may cause infertility and is teratogenic (neural tube defects).
- Haemolysis — jaundice (lemon-yellow, pre-hepatic), dark urine (haemoglobinuria in intravascular), splenomegaly, gallstones (pigment), leg ulcers (sickle).
- Anaemia of chronic disease — signs of the underlying condition (RA, SLE, CKD, malignancy, chronic infection).
- Aplastic/marrow infiltration — features of pancytopenia: infection (low neutrophils), bleeding (low platelets), mucosal pallor; lymphadenopathy/hepatosplenomegaly suggest infiltration (leukaemia, lymphoma, myelofibrosis).
Atypical / under-recognised presentations
- Elderly — anaemia presents as heart failure, angina, falls, confusion, dementia-like decline rather than fatigue; thresholds to investigate and transfuse are lower (under 80 g/L).[1]
- Cardiac/respiratory disease — even modest anaemia worsens angina and heart failure; treat at a higher Hb.
- Diabetic — autonomic and peripheral neuropathy of B12 deficiency can mimic or be concealed by diabetic neuropathy; check B12 in diabetics on metformin with paraesthesia.
- Pregnant — symptoms of physiological anaemia (dyspnoea, fatigue) overlap with normal pregnancy; screen with Hb/iron studies at booking and 28 weeks.
- Immunocompromised / post-transplant / HIV — anaemia from chronic disease, drug marrow toxicity (zidovudine, ganciclovir), parvovirus B19 (pure red-cell aplasia), opportunistic infection.
- Children — irritability, failure to thrive, behavioural and cognitive impairment (iron deficiency impairs neurodevelopment), pallor; severe anaemia in malaria regions presents as breathlessness, heart failure.
- Chronic occult blood loss — may present only as iron-deficiency with no gastrointestinal symptoms; the absence of symptoms does not exclude colorectal cancer.
Differential Diagnosis
Microcytic anaemia (MCV under 80 fL) — distinguishing features
Iron deficiency anaemia
- Most common; low ferritin (under 30 in uncomplicated; under 70 with inflammation), low serum iron, **high TIBC/transferrin**, low % saturation (under 20%), **high soluble transferrin receptor**
- **High sTfR/ferritin ratio** distinguishes from ACD
- Blood film: **microcytic hypochromic**, anisocytosis, pencil (elliptical) cells, poikilocytes
- No family history; symptoms of cause (menorrhagia, GI loss); rapid response to iron therapy
- **Lead level normal**; no basophilic stippling
Thalassaemia trait (alpha or beta)
- **Normal or high ferritin, iron, % saturation**; normal TIBC
- **Mentzer index MCV/RBC count over 13 = IDA; under 13 = thalassaemia trait** (high RBC count)
- Film: **target cells, basophilic stippling**, microcytosis disproportionate to anaemia (Hb often near normal)
- **Raised HbA2 (>3.5%)** in beta-thalassaemia trait (electrophoresis); alpha requires genetic testing
- Ethnicity (Mediterranean, South Asian, Middle Eastern, South-East Asian); family history; **iron therapy does not help and is harmful**
Anaemia of chronic disease
- **Normal or high ferritin, low serum iron, LOW/normal TIBC, low % saturation**
- **High sTfR/ferritin ratio is normal** (sTfR not raised — iron access, not stores, is the problem)
- MCV usually normocytic; **microcytic only in long-standing disease**
- Underlying inflammation/infection/malignancy; raised CRP, ESR; **high hepcidin**
- Low reticulocytes (underproduction); does **not** respond to iron therapy
Sideroblastic anaemia
- **High ferritin, high serum iron, high % saturation (often over 50 to 80%)** — iron is present but cannot be incorporated into haem
- **Ring sideroblasts** on Prussian-blue marrow stain (iron-laden mitochondria around the nucleus)
- Hereditary (X-linked ALAS2), myelodysplastic (RARS/Ring sideroblasts), reversible causes (alcohol, lead, isoniazid, copper deficiency, chloramphenicol)
- Film: **dimorphic population** (microcytic and macrocytic cells), basophilic stippling (lead)
- **Lead poisoning overlap**: may coexist — high ferritin, % saturation and serum iron; ring sideroblasts on marrow if present
Lead poisoning (plumbism)
- Microcytic anaemia with **basophilic stippling**, high ferritin, high % saturation
- Inhibits **ferrochelatase** and **ALA dehydratase** — blocks haem synthesis
- **Abdominal pain, constipation, encephalopathy, peripheral neuropathy (wrist/foot drop), gingival blue line**, nephropathy
- Children with pica (paint, soil); adults (occupational — batteries, paint, plumbing, ammunition)
- **Raised blood lead; raised urinary ALA and coproporphyrin**
Normocytic anaemia (MCV 80 to 100 fL) — distinguishing features
Acute blood loss
- Normal MCV initially; reticulocytes rise at 5 to 7 days
- Hb and Hct may be normal immediately after acute bleed (plasma volume has not yet equilibrated); **falls over 24 to 72 hours** as fluid shifts in
- Clinical bleeding (trauma, GI, obstetric); **tachycardia, hypotension, postural drop**
- Film normal initially; **iron studies normal** then low ferritin if bleeding continues
Anaemia of chronic disease
- Most common cause of normocytic anaemia; **MCV 80 to 95**, low reticulocytes
- Iron studies: low iron, low TIBC, normal/high ferritin; raised CRP
- Underlying inflammatory/infective/malignant/CKD cause; raised hepcidin
Haemolytic anaemia
- **High reticulocyte count (RPI over 2)** — marrow is responding
- Raised LDH, raised indirect bilirubin, **low haptoglobin**, jaundice, splenomegaly
- Film: polychromasia (blue reticulocytes), specific morphology (spherocytes — AIHA/hereditary spherocytosis; sickle cells; schistocytes/helmet cells — MAHA; Heinz bodies — G6PD)
- **Direct Coombs (DAT) positive** in autoimmune haemolysis
Aplastic anaemia / marrow failure
- **Pancytopenia** with low reticulocytes; **aplastic marrow** (cellularity under 25%)
- Triad of anaemia + infections + bleeding; no organomegaly
- Idiopathic, drugs (chloramphenicol, NSAIDs, sulfonamides), viruses (parvovirus B19, hepatitis), radiation, inherited (Fanconi)
- Macrocytosis often present; high EPO
Marrow infiltration
- Leukaemia, lymphoma, myeloma, myelofibrosis, metastatic cancer (breast, prostate), miliary TB
- **Leukoerythroblastic film** (nucleated red cells, immature myeloid precursors, teardrop cells in myelofibrosis)
- Organomegaly (hepatosplenomegaly, lymphadenopathy); cytopenias
- Bone pain; dry tap on marrow; trephine biopsy diagnostic
Mixed deficiency
- Combined iron deficiency + B12/folate deficiency (common in elderly, post-gastrectomy)
- MCV may be normal (iron deficiency lowers MCV, B12 raises it — they cancel)
- Film shows **dimorphic population**; both iron studies and B12/folate abnormal
Macrocytic anaemia (MCV over 100 fL) — megaloblastic vs non-megaloblastic
Megaloblastic (B12/folate deficiency)
- **Macro-ovalocytes** (large oval red cells), **hypersegmented neutrophils** (over 5 lobes), pancytopenia
- **Raised LDH, raised indirect bilirubin, low haptoglobin** (ineffective erythropoiesis — intramedullary haemolysis)
- **Megaloblastic marrow** (giant metamyelocytes, nuclear-cytoplasmic asynchrony)
- **Low serum B12 and/or folate**; raised **homocysteine** and **methylmalonic acid (MMA)** (MMA raised only in B12, not folate)
- **Neurological signs only with B12 deficiency** (peripheral neuropathy, subacute combined degeneration)
- Causes of B12 deficiency: **pernicious anaemia** (anti-IF, anti-parietal cell antibodies), gastrectomy, terminal-ileum disease/resection (Crohn's), dietary (vegan), blind-loop syndrome, metformin, nitrous oxide, pancreatic insufficiency
- Causes of folate deficiency: poor intake, **increased demand (pregnancy, haemolysis, malignancy, dialysis)**, malabsorption (coeliac, tropical sprue), drugs (methotrexate, trimethoprim, phenytoin, sulfasalazine), alcohol
Non-megaloblastic macrocytosis
- **Round macrocytes**, NO hypersegmentation, NO pancytopenia
- **Alcohol excess** (most common; direct marrow toxicity, folate deficiency, liver disease)
- **Hypothyroidism**
- **Reticulocytosis** (young red cells are larger) — e.g. haemolysis, recovery from blood loss
- **Myelodysplastic syndrome (MDS)** and other marrow disorders
- **Drugs**: hydroxyurea, azathioprine, zidovudine, chemotherapy
- **Artefact**: cold agglutinins cause red-cell clumping → spuriously high MCV (raised MCHC clue)
Clinical & Bedside Assessment
History — structure the questioning around cause
- Symptoms of anaemia: onset (acute vs chronic), severity, progression, relation to exertion.
- Blood loss: overt (melaena, haematemesis, haematuria, menorrhagia — quantify pads/tampons/clots), occult (drug history — NSAIDs, aspirin, anticoagulants).
- Dietary: vegetarian/vegan, pica (ice/earth/starch — iron deficiency), alcohol, fad diets.
- GI symptoms: dyspepsia, reflux, change in bowel habit, weight loss, dysphagia — points to cancer, peptic ulcer, IBD, coeliac.
- Gynaecological: menstrual loss, pregnancies, menorrhagia.
- Drugs/toxins: NSAIDs, PPIs, metformin, methotrexate, phenytoin, trimethoprim, sulfasalazine, chemotherapy, lead exposure (occupation, hobbies).
- Past history: gastrectomy/bariatric, IBD, CKD, autoimmune disease (thyroid, vitiligo, Addison's — cluster with pernicious anaemia), malignancy, rheumatoid arthritis.
- Family history: thalassaemia, sickle cell, hereditary spherocytosis, G6PD, pernicious anaemia.
- Travel/exposure: malaria, hookworm, tuberculosis.
- Neurological: paraesthesia, numbness, weakness, unsteadiness, visual or cognitive change — B12 deficiency.
- Systems: fever, night sweats, weight loss (malignancy, infection), bone pain (myeloma, metastases).
Examination — bedside signs
General
- Pallor of conjunctiva (most reliable bedside sign — pallor of the lower lid conjunctiva with the patient looking up), palmar creases, nail beds, oral mucosa, face.
- Jaundice (scleral — haemolysis or ineffective erythropoiesis).
- Lymphadenopathy, hepatosplenomegaly (infiltration, haemolysis, infection).
- Stigmata of chronic disease: clubbing (IBD, malignancy, cyanotic heart disease), koilonychia (iron deficiency).
Specific cause signs
- Iron deficiency — koilonychia (spoon-shaped, brittle nails), angular cheilitis/stomatitis, atrophic glossitis (smooth, red, sore tongue), Plummer-Vinson triad (dysphagia + oesophageal web + glossitis).
- B12 deficiency — glossitis, neurological: impaired vibration and joint position sense (posterior columns) — test with 128 Hz tuning fork at the medial malleolus; spastic paraparesis, extensor plantars (lateral columns); Romberg positive; peripheral neuropathy; optic atrophy; cognitive impairment.
- Haemolysis — splenomegaly, jaundice, frontal bossing and maxillary hypertrophy in chronic congenital haemolysis (thalassaemia major — chipmunk facies), leg ulcers (sickle).
- Chronic disease/marrow failure — purpura, infection, organomegaly.
- Pernicious anaemia / autoimmune — vitiligo, thyroid goitre/scar, signs of Addison's (autoimmune polyglandular cluster).
- Lead — gingival blue line, wrist drop, abdominal tenderness.
Cardio-respiratory (severity)
- Tachycardia, wide pulse pressure, hyperdynamic apex, ejection systolic flow murmur (pulmonary area), venous hum.
- Signs of high-output cardiac failure (raised JVP, basal crackles, oedema, gallop) in severe/chronic anaemia.
Rectal (where appropriate)
- Melena (black tarry stools — upper GI bleed), fresh blood (lower GI bleed), mass (rectal cancer).
Investigations
The first-line panel is the FBC, reticulocyte count and peripheral film, supplemented by iron studies in virtually every adult.[1]
Step 1 — confirm and characterise
- Full blood count — Hb, MCV, MCH, MCHC, RDW (red-cell distribution width — raised RDW suggests a mixed/dimorphic population, e.g. iron deficiency developing or recovering, or combined deficiency).
- Reticulocyte count — expressed as % and as absolute count. Corrected reticulocyte count = retic% x (patient Hct / normal Hct). Reticulocyte production index (RPI) = corrected retic / 2 (maturation correction). RPI over 2 = adequate marrow response → haemolysis or blood loss. RPI under 2 = underproduction.
- Peripheral blood film — morphology dictates the next step (microcytic hypochromic / target cells / spherocytes / sickle cells / schistocytes / macro-ovalocytes / hypersegmented neutrophils / blasts / nucleated red cells).
Step 2 — iron studies
| Test | Iron deficiency | Anaemia of chronic disease | Thalassaemia | Sideroblastic |
|---|---|---|---|---|
| Serum ferritin | Low (under 30 in uncomplicated; under 70 with inflammation) | Normal or high | Normal/high | High |
| Serum iron | Low | Low | Normal/high | High |
| TIBC / transferrin | High (over 400) | Low/normal | Normal | Normal |
| % transferrin saturation | Low (under 20; under 15 in children) | Low | Normal | High (over 50 to 80%) |
| sTfR | High | Normal | Normal/high | Normal |
| sTfR/log ferritin ratio | High | Normal | — | — |
Diagnostic ferritin thresholds (BSH/British Society of Gastroenterology):[1]
- Ferritin under 30 micrograms/L — diagnostic of iron deficiency (sensitivity/specificity >90%) in primary care without inflammation.
- Ferritin under 70 in inflammatory states (CRP raised, infection, malignancy, CKD) — iron deficiency still likely; treat.
- Ferritin normal or high does NOT exclude iron deficiency in inflammation — measure soluble transferrin receptor (sTfR), sTfR/log ferritin ratio, or proceed to marrow iron stain (gold standard).
Step 3 — by MCV class
If microcytic:
- Ferritin, iron, TIBC, % saturation (iron studies).
- Hb electrophoresis / HPLC for thalassaemia (raised HbA2 over 3.5% in beta-thalassaemia trait) — send if iron studies normal or after a trial of iron shows no response.
- Blood lead if lead poisoning suspected (occupational, abdominal pain, basophilic stippling, encephalopathy in children).
- Marrow with Prussian-blue stain if sideroblastic suspected (ring sideroblasts) or to confirm iron stores.
If normocytic with high reticulocytes (haemolysis/loss):
- LDH (raised), haptoglobin (low — most sensitive for haemolysis), indirect (unconjugated) bilirubin (raised), AST (raised, from young red cells), urine haemosiderin/haemoglobin (intravascular haemolysis).
- Direct antiglobulin test (DAT / direct Coombs) — distinguishes immune (positive) from non-immune (negative) haemolysis.
- Osmotic fragility, G6PD assay (not during active haemolysis — reticulocytes have normal enzyme, giving a false-normal result; retest after recovery), flow cytometry for CD55/CD59 (PNH). [1]
If normocytic with low reticulocytes (underproduction):
- U&E, eGFR (CKD — low EPO), LFTs, TSH, CRP/ESR (chronic disease), HIV, viral hepatitis, parvovirus B19 IgM/PCR.
- Bone marrow aspirate and trephine biopsy if pancytopenia, blasts, organomegaly or unexplained anaemia — diagnosing aplastic, leukaemia, myelodysplasia, myelofibrosis, infiltration. [1]
If macrocytic:
- Serum B12 and serum and red-cell folate.
- If B12 borderline/normal but suspicion high — homocysteine (raised in both B12 and folate deficiency) and methylmalonic acid (MMA) (raised in B12 deficiency only) — the most sensitive markers of functional deficiency.
- Intrinsic factor antibodies (highly specific for pernicious anaemia — but sensitivity only 50%), anti-parietal cell antibodies (sensitive but less specific), gastrin (high in pernicious anaemia due to achlorhydria).
- Marrow if macrocytosis with pancytopenia and normal B12/folate (MDS, aplastic). [1]
Step 4 — find the cause of iron deficiency (mandatory in adults)
Iron deficiency in an adult man or post-menopausal woman is GI blood loss until proven otherwise.[1]
- Coeliac serology (anti-tissue transglutaminase IgA + total IgA) in all patients, especially the young.
- Faecal immunochemical test (FIT) / faecal occult blood.
- Upper GI endoscopy (oesophagogastroduodenoscopy) — oesophagitis, peptic ulcer, gastric/oesophageal cancer, duodenal biopsy for coeliac.
- Colonoscopy — colorectal cancer, polyps, IBD, angiodysplasia.
- Capsule endoscopy if OGD and colonoscopy negative — small-bowel causes (Crohn's, tumours, angiodysplasia).
- In premenopausal women with menorrhagia and otherwise well — gynaecological evaluation; endoscopic work-up reserved for symptoms or non-response to iron.
- Stool microscopy for hookworm in endemic areas; urinalysis (haematuria — schistosomiasis, GU cancer).
Named scores reproduced verbatim
Mentzer index (MCV in fL divided by RBC count in millions/microL):
- Over 13 = iron deficiency anaemia; under 13 = thalassaemia trait. [1]
Corrected reticulocyte count = reticulocyte % x (patient Hct / 45). [1]
Reticulocyte production index (RPI) = corrected reticulocyte count / maturation factor (maturation factor = 1.0 at Hct 45%, 1.5 at 35%, 2.0 at 25%). RPI over 2 = adequate marrow response (haemolysis/bleeding); under 2 = underproduction. [1]
WHO haemoglobin thresholds (above) — reproduced verbatim.[1]
Management — Resuscitation
Acute, severe or symptomatic anaemia — the time-critical bundle
The resuscitation priority is tissue oxygenation, not a number. Thresholds balance the benefit against transfusion risks (acute reactions, TACO — transfusion-associated circulatory overload; TRALI — transfusion-related acute lung injury; transfusion-transmitted infection; alloimmunisation; iron overload).[1]
- Assess ABC; oxygen by mask if hypoxic or shocked; two large-bore cannulae.
- Identify and control bleeding (trauma, GI — endoscopic/surgical; obstetric — see APH/PPH topics).
- Intravenous access and crystalloid (0.9% sodium chloride or balanced crystalloid) for volume if shocked.
- Group and save / crossmatch; transfuse if:
- Hb under 70 g/L in a stable adult (restrictive strategy — TRICC trial equivalence).[1]
- Hb under 80 g/L with symptoms (chest pain, orthopnoea, syncope, heart failure) or cardiac disease.
- Hb under 80 g/L in the elderly (>65) or perioperative.
- Hb under 100 g/L rarely, in acute coronary syndrome or severe sepsis (individualise).
- Single-unit transfusion in older/vulnerable patients, then reassess — never two units by default.[1]
- Group O negative for women of childbearing potential and O positive for men in life-threatening haemorrhage (massive transfusion protocol).
- Crossmatch 2 to 4 units for a controlled, slow transfusion (over 1 to 2 hours per unit; diuretic — oral furosemide 20 to 40 mg if at risk of circulatory overload); monitor vital signs, watch for fever, rash, dyspnoea, hypotension (transfusion reaction — stop, return unit to blood bank).
- Avoid transfusing to treat chronic iron-deficiency — it raises antibodies and loads iron; treat the deficiency with iron.
Specific resuscitation scenarios
- Acute upper GI bleed — see upper-GI-bleed topic; transfuse to Hb 70 to 90 g/L, give IV pantoprazole 80 mg bolus then 8 mg/hour, urgent OGD within 24 hours.
- Megaloblastic crisis / severe B12 deficiency with neurological signs — urgent IM hydroxocobalamin 1000 micrograms on alternate days for 2 weeks (see below); do NOT delay; folate must be given WITH B12 if both deficient, never folate alone.
- Severe haemolysis — transfuse if symptomatic/life-threatening; crossmatch may be difficult (auto-antibodies) — use least incompatible blood; treat the cause (see haemolytic-anaemia topic). [1]
Management — Definitive & Stepwise
Treat the cause, not the number. After resuscitation, definitive therapy is cause-specific. The four common examinable treatments are iron, vitamin B12, folate and erythropoiesis-stimulating agents.[1][1][1]
1. Iron deficiency anaemia
Principle — replace stores (not just correct Hb), and find and treat the cause.[1]
Oral iron — first line:
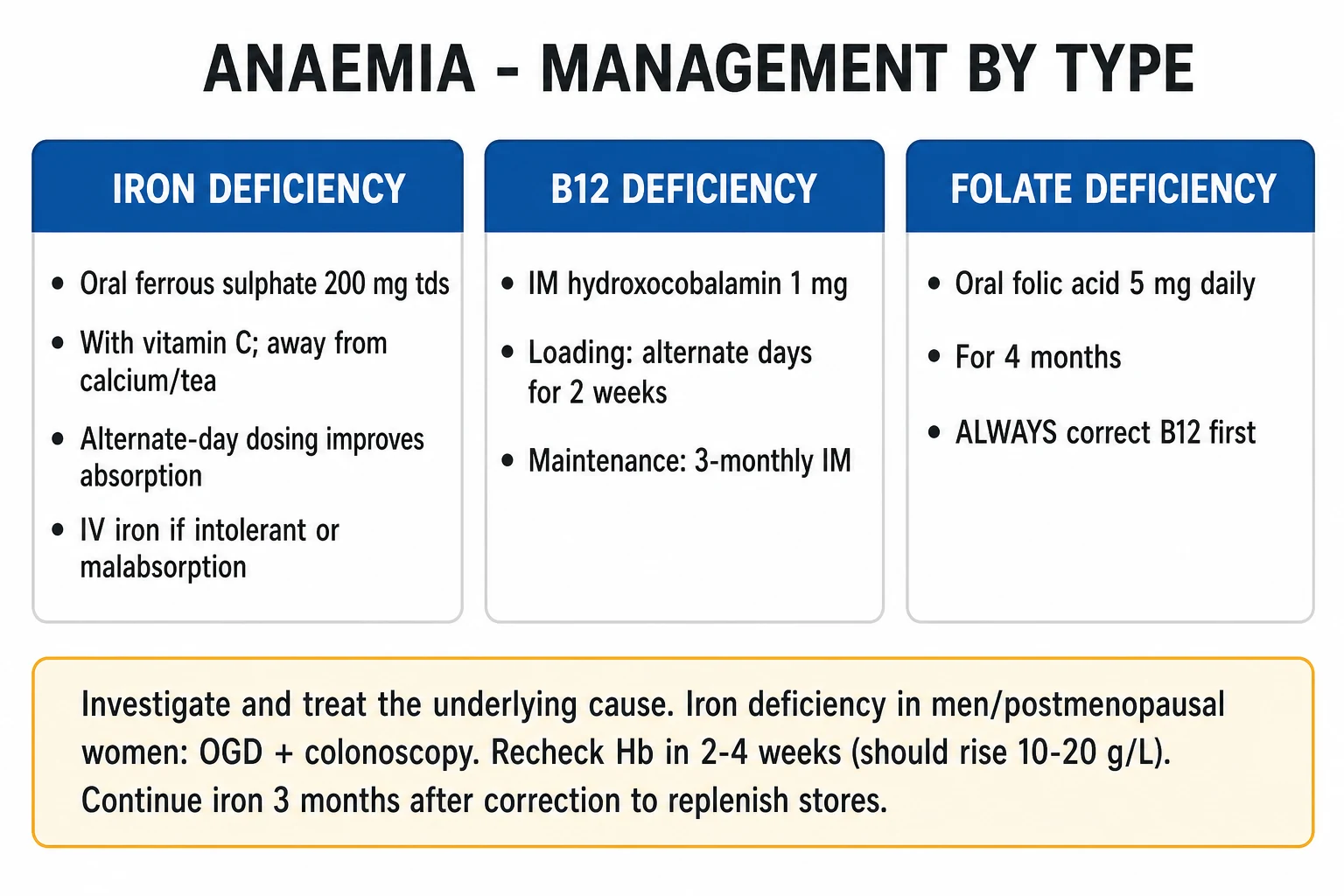
- Ferrous sulphate 200 mg orally three times daily (elemental iron ~65 mg per tablet; ~195 mg/day — exceeds the ~15 to 20% absorption ceiling, so the gut absorbs what it can).[1]
- Alternative salts: ferrous fumarate 322 mg (106 mg elemental), ferrous gluconate 300 mg (35 mg elemental) — similar efficacy, choose by tolerance/cost.
- Take on an empty stomach with vitamin C (orange juice) to maximise absorption; avoid within 2 hours of calcium, antacids, PPIs, tea, coffee, dairy, bran (reduce absorption).
- Duration: continue for 3 to 6 months AFTER haemoglobin normalises to replenish stores (typically 6 months total).[1]
- Expected response: reticulocyte rise in 7 to 10 days; Hb rise ~10 to 20 g/L per fortnight; normalisation of Hb in 6 to 8 weeks.
- Adverse effects (40 to 60%): constipation, dark stools, nausea, abdominal pain, metallic taste — manage by taking with food, reducing to once daily, switching salt, or using modified-release (NOT preferred — absorption worse).
- Special oral: liquid ferrous fumarate/ferric ammonium citrate for children and those unable to swallow tablets.
Intravenous iron — second line:
- Indications: intolerance to oral iron, malabsorption (coeliac, IBD, post-bariatric, atrophic gastritis, Helicobacter colonisation), non-adherence, ongoing blood loss exceeding oral replacement (IBD, hereditary haemorrhagic telangiectasia, dialysis), need for rapid correction (preoperative, late pregnancy, severe symptomatic anaemia), chronic kidney disease (with ESA), heart failure with iron deficiency.
- Agents and doses (BSH/British Society of Gastroenterology):[1][1]
- Ferric carboxymaltose (Ferinject) — 1000 mg IV over 15 minutes (up to 15 mg/kg in children); repeat weekly to total calculated dose (using the Ganzoni formula: dose (mg) = weight (kg) x (target Hb minus actual Hb) x 2.4 + iron stores (500 mg)); single doses up to 1000 mg, maximum 15 mg/kg per infusion.
- Ferric derisomaltose (Monofer) — up to 20 mg/kg in a single infusion (often 1000 to 2000 mg over 30 to 60 minutes).
- Low-molecular-weight iron dextran (CosmoFer) — total dose infusion over 4 to 6 hours (test dose first).
- Iron sucrose (Venofer) — 100 to 200 mg IV over 15 to 30 minutes, repeated (common in dialysis).
- Ferric derisomaltose and ferric carboxymaltose — preferred for high single-dose outpatient replacement (low risk of serious hypersensitivity).
- Cautions — hypersensitivity reactions (rare but serious; full resuscitation facilities required; observe 30 minutes post-infusion), hypophosphataemia (especially ferric carboxymaltose — FGF23-mediated; monitor phosphate, symptomatic myopathy possible), skin staining (extravasation; deep cannula, large vein), avoid in active infection (iron feeds bacteria).
- Indications for oral challenge before IV are no longer routinely required when oral therapy has failed or is inappropriate.
Find and treat the cause — GI workup mandatory in adults (see Investigations).[1]
Erythropoiesis-stimulating agents (ESAs) — reserved for CKD-associated anaemia (Hb under 100 to 110 g/L), cancer-treatment-related anaemia (with chemotherapy), and selected MDS. Epoetin alfa/beta SC, darbepoetin alfa (longer-acting). MUST ensure adequate iron stores (give IV iron with ESA). Target Hb 100 to 120 g/L (not normal — raises thrombosis/cardiovascular risk). [1]
2. Vitamin B12 deficiency
IM hydroxocobalamin is preferred (retained longer than cyanocobalamin).[1]
UK BSH regimen (British Society of Haematology / BNF):
- Initial loading: 1 mg (1000 micrograms) IM on alternate days for 2 weeks (up to 7 doses), or daily if neurological disease (use 1 mg IM daily while symptoms improve, continuing until no further improvement — minimum of 6 doses, often more).[1]
- Maintenance: 1 mg IM every 2 to 3 months for life (in pernicious anaemia, gastrectomy, ileal disease, dietary vegan who will not change diet).
- In dietary deficiency (reversible cause) — no maintenance needed once diet corrected.
- High-dose oral cyanocobalamin (1000 to 2000 micrograms daily) is increasingly used (1 to 2% passive absorption) for maintenance in adherent patients without malabsorption, but IM is standard for initial therapy and in any patient with malabsorption or neurological signs.
Response: reticulocytosis in 3 to 5 days; hypokalaemia in the first 48 hours (vigorous erythropoiesis consumes K+ — monitor and replace); Hb rises over weeks; neurological signs improve over months — early damage may not fully recover.[1]
3. Folate deficiency
- Oral folic acid 5 mg daily for 4 months (lifelong if malabsorption/chronic haemolysis).[1]
- CRITICAL: always exclude/treat coexisting B12 deficiency first or concurrently — giving folate alone to a B12-deficient patient precipitates or worsens subacute combined degeneration of the cord (folate drives erythropoiesis but not myelin synthesis, accelerating B12 depletion). If in doubt, give both.
- Prophylaxis: 400 micrograms daily pre-conception and in pregnancy (400 micrograms daily reduces neural tube defects; 5 mg daily in women with prior affected pregnancy, on antiepileptics, or with malabsorption).[1]
4. Other cause-specific treatments
- Anaemia of chronic disease — treat the underlying disease; IV iron if iron-restricted erythropoiesis (e.g. IBD, CKD with ESA); ESAs in CKD/cancer.
- Haemolytic anaemia — see topic (immune: corticosteroids — prednisolone 1 to 1.5 mg/kg/day; splenectomy; rituximab; folic acid 5 mg daily during active haemolysis).
- Aplastic anaemia — see topic (antithymocyte globulin + ciclosporin, allogeneic stem-cell transplant; supportive transfusions/antimicrobials).
- Thalassaemia — see topic (transfusion-chelation programme; curative HSCT; gene therapy).
- Anaemia of CKD — IV iron and ESA to Hb 100 to 120 g/L. [1]
Stepwise management ladder (escalation triggers)
- Confirm anaemia; classify by MCV and reticulocytes; find the cause.
- Resuscitate if severe/symptomatic (transfusion per thresholds above).
- Treat the cause with substrate (iron / B12 / folate) OR specific therapy (immunosuppression, ESA, chelation, transplant).
- Reassess response at 2 to 4 weeks — reticulocyte rise, Hb rise; if no response, re-evaluate the diagnosis and adherence.
- Escalate — IV iron for oral failure; specialist referral for refractory, pancytopenia, marrow disease, transfusion dependence.
- Replenish stores (iron 3 to 6 months post-Hb; B12 maintenance for life in pernicious).
- Prevent recurrence — treat the underlying cause; dietary advice; screening/prophylaxis in pregnancy and high-risk groups.
Specific Subtypes & Scenarios
Iron deficiency anaemia — in depth
- Most common cause of anaemia worldwide; dietary deficiency (low intake of haem/absorbable iron), blood loss (menorrhagia, GI — peptic ulcer, cancer, hookworm, IBD, angiodysplasia, NSAIDs), malabsorption (coeliac, atrophic gastritis, H. pylori, gastrectomy, bariatric), increased demand (growth, pregnancy, lactation, EPO/ESA therapy).
- Stages of depletion: (1) depleted stores (low ferritin, normal Hb) → (2) iron-deficient erythropoiesis (low ferritin, low % saturation, raised sTfR, normal Hb) → (3) iron deficiency anaemia (low Hb, microcytic).[1]
- Plummer-Vinson syndrome — iron deficiency + dysphagia + oesophageal web + glossitis; increased risk of post-cricoid squamous cell carcinoma.
- Pica — pagophagia (ice) is highly specific; also earth, starch.
- Treat the cause; respond to iron within 7 to 14 days.
Anaemia of chronic disease (ACD) — overview (see dedicated topic)
- Normocytic (occasionally microcytic) anaemia of inflammation, infection, malignancy, CKD; hepcidin-mediated iron trapping. Low serum iron, low/normal TIBC, normal/high ferritin. Treat the underlying disease; IV iron and/or ESA if iron-restricted erythropoiesis.
Megaloblastic anaemia — B12 deficiency in depth[1]
- Pernicious anaemia — autoimmune destruction of gastric parietal cells (anti-parietal cell antibodies) and/or neutralisation of intrinsic factor (anti-IF antibodies); achlorhydria and loss of IF prevent B12 absorption. Associated with other autoimmune disease (thyroid, Addison's, vitiligo, type 1 diabetes, premature ovarian failure) and a three-fold increased risk of gastric carcinoma (annual endoscopy recommended in some guidelines).[1]
- Post-gastrectomy — loss of IF and acid; deficiency takes 3 to 5 years to manifest.
- Terminal ileum disease — Crohn's, resection, blind-loop syndrome (bacterial utilisation of B12), fish tapeworm (Diphyllobothrium latum), pancreatic insufficiency (failure to degrade R-binder).
- Drugs — metformin (interferes with calcium-dependent IF-B12 absorption in the ileum; common in diabetics), nitrous oxide (inactivates methionine synthase — recreational or occupational, can cause acute severe deficiency), PPIs long-term, colchicine, neomycin.
- Dietary — strict vegan; breast-fed infants of vegan mothers.
- Clinical: megaloblastic anaemia + mild jaundice (lemon-yellow) + pancytopenia + glossitis + neurological (peripheral neuropathy, subacute combined degeneration, optic atrophy, dementia).
- Investigation: low serum B12; raised MMA and homocysteine (most sensitive); intrinsic factor antibodies (specific); anti-parietal cell antibodies (sensitive); Schilling test (historical, to localise the cause); gastroscopy if pernicious anaemia (atrophy, type A gastritis).
Folate deficiency in depth
- Reduced intake (poor diet — no body store beyond 4 months; alcoholics, elderly, refugees).
- Increased demand — pregnancy (neural tube defect risk), lactation, chronic haemolysis (give 5 mg daily prophylactically in sickle cell, thalassaemia, hereditary spherocytosis), malignancy, dialysis (folate lost).
- Malabsorption — coeliac, tropical sprue, IBD.
- Drugs — methotrexate (inhibits dihydrofolate reductase; rescue with folinic acid), trimethoprim, phenytoin, sulfasalazine, oral contraceptives. [1]
Acute blood loss
- Acute haemorrhage (trauma, GI, obstetric, surgical, ruptured ectopic/aortic aneurysm). Hb may be normal initially — resuscitate from shock (vital signs), not the Hb. Replace volume; transfuse if unstable or Hb under 70. Iron therapy to replenish stores lost in a major bleed.
Pregnancy-associated anaemia
- Physiological haemodilution lowers Hb; WHO defines anaemia in pregnancy as Hb under 110 g/L (under 105 in second trimester), severe under 70.[1]
- Iron demand rises from 1 mg/day (non-pregnant) to 5 to 6 mg/day (third trimester); folate demand rises three-fold.
- Consequences: maternal fatigue, infection, post-partum haemorrhage risk, pre-eclampsia, preterm delivery, low birth weight, perinatal mortality; the child of an iron-deficient mother has impaired cognition.
- Management: routine IFA supplementation (60 mg elemental iron + 0.4 mg folic acid daily) in pregnancy; screen at booking and 28 weeks; oral ferrous sulphate 200 mg TDS if iron deficient; IV ferric carboxymaltose in third trimester if oral fails or severe (avoid first trimester — limited safety data); never transfuse for iron deficiency in pregnancy unless haemodynamically unstable.[1]
- Folate 400 micrograms daily (5 mg if high-risk) pre-conception to at least 12 weeks.
Anaemia of prematurity
- Preterm infants; low EPO; treated with recombinant EPO and iron; minimise phlebotomy; transfuse at low Hb thresholds by postnatal age.
Anaemia in CKD
- Normocytic; underproduction (low EPO) + uraemic platelet dysfunction + iron deficiency (ESAs increase demand). IV iron + ESA to Hb 100 to 120 g/L. Withhold ESA if Hb over 115. [1]
Anaemia in the elderly
- Multifactorial: iron deficiency (GI cancer, NSAIDs), B12, folate, ACD, CKD, MDS. Lower thresholds to investigate and transfuse (under 80 g/L). Single-unit transfusions. Aim to find reversible cause — don't write off as "anaemia of ageing". [1]
Anaemia in malignancy
- ACD + marrow infiltration + chemotherapy + bleeding + haemolysis + iron deficiency. IV iron and ESA (caution in active malignancy; ESAs may accelerate tumour growth and increase thrombosis — only with curative-intent chemotherapy).
Complications & Pitfalls
Complications of untreated anaemia
- High-output cardiac failure (tachycardia, cardiomegaly, pulmonary oedema, peripheral oedema) — chronic severe anaemia.
- Angina and myocardial infarction in those with coronary disease.
- Cognitive impairment — especially iron deficiency in children (developmental delay; may be irreversible).
- Impaired immunity — increased infection risk.
- In pregnancy: preterm delivery, low birth weight, pre-eclampsia, postpartum haemorrhage, perinatal mortality.
- B12 deficiency neurological damage — permanent if untreated (subacute combined degeneration).
- Tissue hypoxia — syncope, falls (elderly).
Complications of transfusion
- Acute transfusion reactions — febrile non-haemolytic, allergic/anaphylactic, acute haemolytic (ABO mismatch), bacterial sepsis (platelets), TACO (transfusion-associated circulatory overload), TRALI (transfusion-related acute lung injury).
- Delayed — delayed haemolytic transfusion reaction (3 to 14 days, anamnestic alloantibodies), transfusion-transmitted infection (hepatitis B/C, HIV, malaria, prion — rare), iron overload (transfusion haemosiderosis — every unit ~200 mg iron; chelate after ~20 units or serum ferritin over 1000), alloimmunisation (anti-Rh/Kell — affects future transfusion and pregnancy), post-transfusion purpura, GVHD (irradiate cellular products for immunocompromised).[1]
Pitfalls
- Treating the number, not the cause — e.g. transfusing chronic iron deficiency, missing a colon cancer.
- Assuming iron deficiency without GI work-up in men/post-menopausal women — always investigate.
- Giving folate alone in B12 deficiency — precipitates/worsens subacute combined degeneration.
- Misreading ferritin as normal in inflammation — measure CRP, sTfR, or marrow iron.
- Missing a mixed deficiency (iron + B12) — MCV may be normal; check both.
- Over-transfusing the elderly or those with heart failure — risk TACO; single-unit prescribing.[1]
- Diagnosing G6PD deficiency during active haemolysis — false normal (young reticulocytes); retest after recovery.
- Treating beta-thalassaemia trait with iron — ineffective and causes overload.
- Confusing cold-agglutinin artefact with true macrocytosis — MCHC raised, MCV spuriously high.
- Failure to detect ongoing blood loss during iron therapy — Hb fails to rise; reassess for occult bleeding (GI, menorrhagia).
Prognosis & Disposition
- Nutritional deficiency (iron, B12, folate) — excellent with treatment; full recovery of Hb and (mostly) neurological function if caught early.
- Pernicious anaemia — needs lifelong B12; excellent for the anaemia; neurological recovery depends on duration; increased gastric cancer risk (surveillance).
- Anaemia of chronic disease — mirrors the prognosis of the underlying disease.
- Haemolytic anaemia — varies widely (autoimmune often responds; hereditary is chronic; transfusion-dependent haemoglobinopathies carry iron-overload and organ damage).
- Aplastic anaemia — high mortality untreated; HSCT curative in young fit patients.
- Marrow infiltration (leukaemia, myelofibrosis, MDS) — depends on the underlying disease.
- Severe anaemia (Hb under 50 g/L) — high mortality if untreated; transfusion and cause-directed therapy are urgent. [1]
Disposition
- Outpatient — most chronic stable anaemia (oral iron, B12, folate, follow-up).
- Inpatient (ward) — symptomatic anaemia needing transfusion, severe B12 with neurology, haemolysis requiring therapy, diagnostic uncertainty with pancytopenia.
- ICU — massive haemorrhage, severe symptomatic anaemia with cardiac failure, transfusion reaction.
- Specialist referral — haematology (marrow disease, transfusion dependence, haemolysis), gastroenterology (iron-deficiency work-up), nephrology (CKD/ESA), gynaecology (menorrhagia), obstetrics (pregnancy).
Special Populations
Pregnancy
- Lower thresholds: anaemia Hb under 110 g/L (under 105 in second trimester); severe under 70.[1]
- Routine IFA (60 mg elemental iron + 0.4 mg folic acid) from first antenatal contact to 3 months post-partum; screen at booking and 28 weeks.
- Oral iron first-line; IV ferric carboxymaltose in second/third trimester if oral fails or severe.
- Avoid transfusion for iron deficiency — only if haemodynamically unstable.
- Folate 400 micrograms (5 mg high-risk) pre-conception to 12 weeks for neural tube defect prevention.
- B12 deficiency in pregnancy — IM hydroxocobalamin; treat to prevent maternal and fetal deficiency.
Children
- WHO thresholds: under 110 g/L (6 months to 5 years), under 115 (5 to 11), under 120 (12 to 14).
- Iron deficiency — most common; risk in preterm, low birth weight, exclusive breast-feeding beyond 6 months, cow's-milk-heavy diet, pica. Causes developmental delay that may be irreversible — treat early.
- Iron prophylaxis: 1 mg/kg/day elemental iron for breast-fed preterm infants from 4 weeks; iron-fortified formula; introduce iron-rich solids by 6 months.
- Treatment: 3 to 6 mg/kg/day elemental iron in divided doses (e.g. ferrous sulphate; liquid ferrous fumarate in young children) for 3 months after Hb normalises.
- Megaloblastic anaemia — usually folate (maternal deficiency); B12 deficiency in breast-fed infants of vegan mothers or pernicious (rare juvenile pernicious).
- Transfusion thresholds are lower (children tolerate low Hb); transfuse for severe symptomatic anaemia or Hb under 50 to 70 g/L. [1]
Elderly
- Lower thresholds to investigate and transfuse (under 80 g/L); single-unit transfusion.
- Atypical presentations — heart failure, angina, falls, confusion.
- Multifactorial causes common; do not attribute to "ageing".
- Increased transfusion risk (TACO, TRALI) — slow infusion, diuretic cover (oral furosemide 20 to 40 mg), careful monitoring.
- Increased GI cancer risk — investigate iron deficiency rigorously. [1]
Immunocompromised / transplant / HIV
- Anaemia of chronic disease, drug marrow toxicity (zidovudine, ganciclovir, chemotherapy), parvovirus B19 pure red-cell aplasia (treat with IV immunoglobulin), opportunistic infection, malignancy.
- Irradiate cellular blood products to prevent transfusion-associated GVHD; CMV-negative products if CMV-seronegative transplant candidate.
- Leucodeplete all products.
Anticoagulated / antiplatelet patients
- Increased GI bleeding risk (warfarin, DOACs, aspirin, clopidogrel) — check INR, drug levels; reverse per protocol if life-threatening bleed; balance bleeding vs thrombotic risk during transfusion/investigation.
Evidence, Guidelines & Regional Differences
Landmark evidence
- TRICC trial (Hébert 1999, NEJM) — restrictive transfusion strategy (Hb under 70 g/L) was at least as safe as liberal (under 100) in critically ill adults, with fewer complications. Underpins modern restrictive transfusion.[1]
- TRIPICU (Lacroix 2007, JAMA) — restrictive strategy safe in paediatric ICU.
- FOCUS (Carson 2011, NEJM) — in hip-fracture surgery, Hb under 80 g/L threshold non-inferior to under 100 in patients with cardiovascular risk factors.
- FERRIC-HF, FAIR-HF, CONFIRM-HF, AFFIRM-HF, IRONOUT-HF — IV ferric carboxymaltose improves symptoms, exercise capacity and quality of life in heart failure with iron deficiency, independent of anaemia.
- PPI-Reflux, PREVENTT (2021, Lancet) — IV iron before major abdominal surgery did NOT reduce transfusion or improve outcome (challenges routine pre-op IV iron).
- Stabler (NEJM 2013) — authoritative review of B12 deficiency diagnosis and treatment.[1]
- Goddard et al (BSG 2011) — UK guideline for iron-deficiency anaemia management and GI work-up.[1]
- Pavord et al (BSH 2012) — UK guideline for iron deficiency in pregnancy.[1]
Regional differences
Controversies
- Oral vs IV iron first — oral remains first-line; IV iron first is increasingly advocated in IBD, heart failure, late pregnancy, dialysis and when rapid correction is needed.
- Duration of oral iron — once-daily alternate-day dosing may improve absorption (hepcidin-mediated) and reduce adverse effects vs TDS, but TDS remains standard practice and guideline.[1]
- IV iron and infection — caution in active infection; withheld during active bacteraemia.
- Hypophosphataemia after ferric carboxymaltose — increasingly recognised; monitor phosphate in symptomatic patients.
- ESA in cancer — restrict to chemotherapy-induced anaemia; risk of thrombosis and possible tumour progression.
- Transfusion in upper GI bleed — restrictive (Hb 70 to 90) improves outcome (over-transfusion worsens portal pressure and rebleeding).
- B12 oral vs IM — high-dose oral (1000 to 2000 micrograms daily) increasingly accepted as equivalent for maintenance and even initial therapy in selected patients; IM remains standard in malabsorption, neurological disease, and pernicious anaemia.
Exam Pearls
Microcytic anaemia — microcytosis causes
TAILS
trait (alpha or beta); normal/high ferritin, target cells, raised HbA2 in beta
low iron, LOW TIBC, high/normal ferritin; hepcidin block
low ferritin, HIGH TIBC; the commonest cause worldwide
inhibits ferrochelatase and ALA dehydratase; basophilic stippling; gingival blue line
ring sideroblasts in marrow; high ferritin; dimorphic film; hereditary, MDS, drugs (isoniazid)
Macrocytosis (MCV over 100) — megaloblastic vs non-megaloblastic
MACRO
macro-ovalocytes, hypersegmented neutrophils, pancytopenia, raised LDH; neurology if B12
non-megaloblastic round macrocytes; commonly with folate deficiency and liver disease
non-megaloblastic round macrocytes; target cells
young red cells are large; polychromasia on film; haemolysis or recovery from bleed
hypothyroid, MDS, drugs (hydroxyurea, AZT), artefact (cold agglutinins — high MCHC)
High-yield one-liners
- Most common cause of anaemia worldwide = iron deficiency.
- Iron deficiency in an adult man or post-menopausal woman = GI blood loss until proven otherwise.
- Ferritin is an acute-phase reactant — false normal/high in inflammation; use sTfR or marrow.
- TIBC rises in iron deficiency, falls in ACD — the single best discriminator.
- Macro-ovalocytes + hypersegmented neutrophils = megaloblastic anaemia (B12 or folate).
- NEVER give folate alone if B12 deficiency is possible — precipitates subacute combined degeneration of the cord.
- Subacute combined degeneration = B12 deficiency (dorsal + lateral columns; loss of vibration/proprioception, spastic paraparesis, extensor plantars).
- Methylmalonic acid raised in B12 but NOT folate deficiency — best discriminator.
- Reticulocyte count is the single most useful test to split anaemia into underproduction vs destruction/loss.
- RPI over 2 = haemolysis or blood loss; under 2 = underproduction.
- Pernicious anaemia = anti-intrinsic-factor antibodies; achlorhydria; increased gastric cancer risk.
- Transfuse at Hb under 70 g/L (under 80 if symptomatic/elderly/cardiac); single-unit prescribing.
- TRICC trial — restrictive (under 70) transfusion is non-inferior to liberal.
- Hypokalaemia can complicate B12/folate treatment (vigorous erythropoiesis).
- Ferrous sulphate 200 mg TDS for 3 to 6 months after Hb normalises to replenish iron stores.
- IM hydroxocobalamin 1 mg on alternate days for 2 weeks, then 1 mg every 2 to 3 months for life (pernicious anaemia).
- Pagophagia (ice pica) is highly specific for iron deficiency.
- Plummer-Vinson syndrome = iron deficiency + dysphagia + oesophageal web + glossitis; risk of post-cricoid carcinoma.
- MDS is the commonest cause of sideroblastic anaemia in older adults.
- Lead poisoning inhibits ferrochelatase and ALA dehydratase; basophilic stippling, abdominal pain, neuropathy, encephalopathy in children.
- Nitrous oxide inactivates methionine synthase — can cause rapid B12 deficiency in recreational users.
- Metformin causes B12 deficiency — check in long-term diabetics.
- Cold agglutinins spuriously raise MCV (and MCHC) — artefact.
- G6PD assay is unreliable during active haemolysis — retest after recovery.
- IV iron: ferric carboxymaltose 1000 mg — beware hypophosphataemia.
- Anaemia Mukt Bharat — IFA red tablet (60 mg iron + 0.4 mg folate) daily for 100 days in pregnancy. [1]
Exam application bank (NEET-PG / INICET)
One-line answer
Anaemia (WHO: Hb under 130 g/L men, under 120 g/L non-pregnant women, under 110 g/L pregnant women and children 6 months to 5 years) is not a diagnosis but a sign of disease. The examinable skill is the MCV-based framework: microcytic (under 80 fL — iron deficiency, thalassaemia, anaemia of chronic disease, sideroblastic, lead), normocytic (80 to 100 fL — acute blood loss, anaemia of chronic disease, haemolysis, aplastic, mixed deficiency) and macrocytic (over 100 fL — megaloblastic B12/folate, alcohol, liver disease, hypothyroid, MDS, drugs). The reticulocyte count splits causes into underproduction vs destruction/loss. Iron deficiency (most common worldwide): low ferritin, low iron, high transferrin/TIBC, low % saturation, high sTfR. Megaloblastic: hypersegmented neutrophils, macro-ovalocytes, pancytopenia, raised LDH and indirect bilirubin, intrinsic factor antibodies (pernicious), ne [1]
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Anaemia.
[1] [1]References
- [1]Pavord S, Myers B, Robinson S, Allard S, Strong J, Oppenheimer C; British Committee for Standards in Haematology. UK guidelines on the management of iron deficiency in pregnancy. Br J Haematol, 2012.PMID 22512001