Infectious Diseases · General Medicine
Bacterial Meningitis & Acute Meningoencephalitis
Also known as Meningitis · Bacterial meningitis · Acute meningitis · Meningococcal meningitis · Meningoencephalitis · Aseptic meningitis
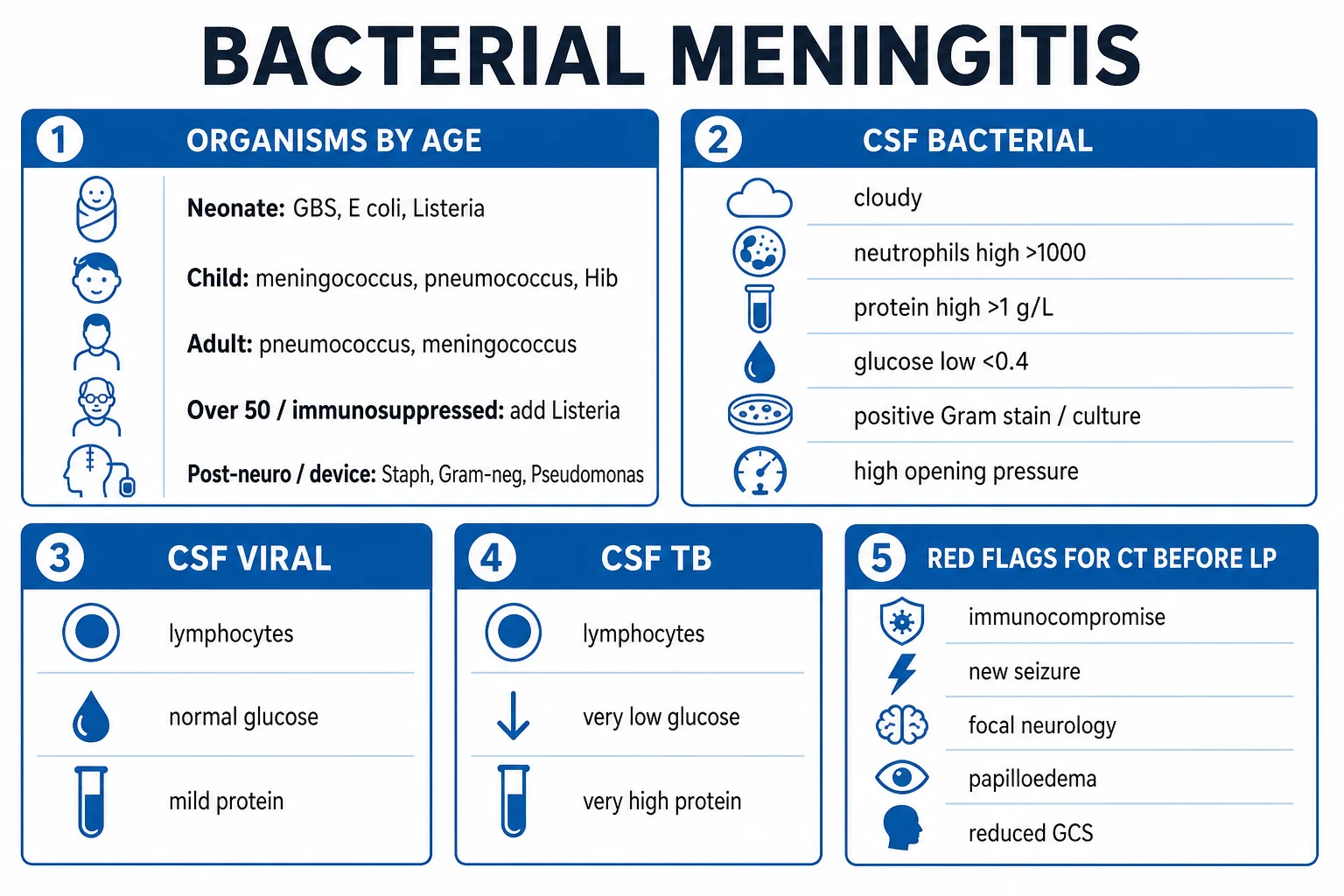
Bacterial meningitis is a life-threatening medical emergency — acute inflammation of the meninges and subarachnoid space, most often from haematogenous spread of Streptococcus pneumoniae or Neisseria meningitidis. Classic triad: fever, headache, neck stiffness plus photophobia, vomiting, altered mental status and seizures; meningococcal disease adds a rapidly evolving petechial/purpuric rash and septicaemia. Organisms by age: neonate — Group B strep, E. coli, Listeria; child — meningococcus, pneumococcus, Hib; adult — pneumococcus, meningococcus; over 50 / immunocompromised / pregnant — add Listeria. Diagnosis rests on lumbar puncture CSF (cloudy, neutrophils over 1000, protein over 1 g/L, glucose under 40 mg/dL or under 40% of serum, positive Gram stain/culture) — but CT head first when red flags are present, and empirical IV antibiotics must never be delayed for the LP or CT. Treatment: ceftriaxone + vancomycin + ampicillin (Listeria) + aciclovir (HSV) plus adjunctive dexamethasone with the first antibiotic dose. Mortality 10-30%; sensorineural hearing loss is the commonest sequel.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Overview & Definition
Meningitis is inflammation of the meninges — the membranes (dura mater, arachnoid mater, pia mater) that surround the brain and spinal cord — most often due to infection of the subarachnoid space and the cerebrospinal fluid (CSF) within it.[1]
The clinical skill in suspected meningitis is not the diagnosis (it is clinical, then confirmed by LP) but three time-critical decisions taken in parallel:[1]
- Recognise the syndrome — fever with headache and neck stiffness (plus photophobia, vomiting, altered mentation, or a petechial rash) is bacterial meningitis (or meningococcal septicaemia) until proven otherwise.
- Give empirical IV antibiotics immediately on suspicion — before lumbar puncture, before blood cultures, before CT. Every hour of delay increases mortality and neurological disability.[1][2]
- Decide whether CT is needed before LP — and add adjunctive dexamethasone, Listeria cover (ampicillin), and HSV cover (aciclovir) where appropriate.
Meningitis vs encephalitis vs meningoencephalitis vs aseptic meningitis
- Meningitis — inflammation predominantly of the meninges; brain parenchyma spared. Classic fever + headache + neck stiffness; cognition usually preserved until late.
- Encephalitis — inflammation predominantly of the brain parenchyma; diffuse brain dysfunction dominates (confusion, behaviour change, seizures, focal deficits, coma). Herpes simplex encephalitis is the treatable archetype (temporal lobe changes on MRI/EEG).
- Meningoencephalitis — both meninges and parenchyma inflamed; a combined clinical picture (meningeal signs PLUS encephalopathy). Common with HSV, enterovirus, arboviruses (Japanese encephalitis, West Nile), tuberculous and fungal disease.
- Aseptic meningitis — CSF pleocytosis with negative routine bacterial cultures; the commonest cause is viral (enterovirus, HSV-2, mumps), but the term also encompasses TB, fungal, drug-induced (NSAIDs, trimethoprim, IVIG), and autoimmune causes. "Aseptic" does not mean benign — always exclude the treatable bacterial and viral causes first.[1]
The depth standard for this chapter is the community-acquired acute bacterial meningitis of adults and children, with subtypes (viral, tuberculous, fungal, neonatal, post-neurosurgical) covered in Specific Subtypes.[1]
Classification
Meningitis is classified along three axes that the examiner will probe — aetiology, host, and tempo — because each changes the organism, the CSF picture, and the empirical antibiotic choice.[1]
By aetiology (the axis that drives treatment):[1]
Bacterial (purulent)
- Emergency. Neutrophilic CSF, low glucose, high protein
- Adult: S. pneumoniae, N. meningitidis; over 50/immunocompromised add Listeria
- Empirical IV ceftriaxone + vancomycin + ampicillin + dexamethasone
Viral (aseptic)
- Commonest overall; usually self-limiting
- Enterovirus (commonest), HSV-2, mumps, HIV seroconversion
- Lymphocytic CSF, normal glucose; aciclovir if HSV encephalitis suspected
Tuberculous
- Subacute-chronic; basal exudate, cranial nerve palsies, stroke
- Mycobacterium tuberculosis; very low CSF glucose, cobweb coagulum
- RHZE + ethionamide + corticosteroids; 9-12 months
Fungal
- Immunosuppressed (HIV/AIDS). Cryptococcus neoformans is the archetype
- Lymphocytic CSF, low glucose, positive India ink and CrAg, very high opening pressure
- Liposomal amphotericin B + flucytosine; therapeutic LP for raised pressure
By host / setting:[1]
- Community-acquired — the archetype; organisms dictated by age and vaccination history.
- Post-neurosurgical / CSF-shunt / external ventricular drain — Staphylococcus aureus, coagulase-negative staphylococci, Gram-negative bacilli (including Pseudomonas), and Propionibacterium acnes; empirical therapy is vancomycin + ceftazidime or cefepime (anti-pseudomonal), and infected hardware must be removed or externalised.[1]
- Recurrent meningitis — suspect a CSF leak (cribriform plate, skull-base fracture), complement / properdin deficiency or eculizumab (recurrent meningococcal), anatomical defect (dermal sinus, midline cleft), or Mollaret meningitis (recurrent HSV-2).
By tempo:[1]
- Acute (hours-days) — bacterial, viral, early HSV encephalitis.
- Subacute-chronic (days-weeks) — tuberculous, fungal, carcinomatous, partially-treated bacterial.[1]
Epidemiology & Risk Factors
Bacterial meningitis is uncommon but uniformly life-threatening — incidence roughly 3 per 100 000 per year in high-income countries after the vaccine era, with case-fatality of 10-30% even with optimal care, and permanent neurological sequel in a further 20-30%.[1] The epidemiology has been transformed by conjugate vaccination (Hib, pneumococcal PCV, meningococcal MenACWY/MenB), which is now the single most powerful public-health lever.
Organisms by age — the question most often asked in MCQs:[1]
| Age band | Commonest organisms |
|---|---|
| Neonate (0-1 month) | Group B strep (S. agalactiae), E. coli (K1 capsule), Listeria monocytogenes |
| Infant / child (1 month-15 yr) | N. meningitidis, S. pneumoniae, H. influenzae type b (where unvaccinated) |
| Young adult (16-50 yr) | S. pneumoniae (commonest), N. meningitidis |
| Over 50 / alcoholic / immunocompromised | S. pneumoniae, N. meningitidis, plus Listeria monocytogenes |
| Post-neurosurgery / CSF shunt | S. aureus, coagulase-negative staph, Gram-negatives, Pseudomonas |
Risk factors and the organism they favour (high-yield):[1]
| Host / risk factor | Organism to add or suspect |
|---|---|
| Asplenia, sickle-cell, haematological malignancy | Encapsulated organisms — S. pneumoniae, N. meningitidis, H. influenzae (overwhelming post-splenectomy infection) |
| Complement (C5-C9) / properdin deficiency; eculizumab / ravulizumab | Recurrent meningococcal disease — vaccinate AND give prophylaxis on exposure |
| HIV / CD4 under 200 | Cryptococcus, Listeria, TB, Salmonella, syphilis |
| Pregnancy | Listeria (impaired cell-mediated immunity) |
| Skull-base fracture, CSF leak (rhinorrhoea/otorrhoea) | S. pneumoniae (recurrent) |
| Otitis media, mastoiditis, sinusitis | S. pneumoniae, H. influenzae, anaerobes; rarely brain abscess |
| CSF shunt / VP shunt / external drain | Coag-neg staph (S. epidermidis), S. aureus, Pseudomonas |
| Alcohol misuse, chronic liver disease | S. pneumoniae, Listeria |
| Terminal complement pathway deficiency | Recurrent meningococcal (otherwise benign course) |
Meningococcal epidemiology — peaks at two ages: infants (declining maternal antibody) and adolescents/young adults (colonisation, dormitory/college residence, military barracks). Epidemics occur in the sub-Saharan African "meningitis belt" and during mass gatherings (Hajj). Serogroups B, C, W, Y predominate in high-income countries; serogroup A historically drove the African belt and is now curtailed by MenAfriVac.[1]
Pathophysiology
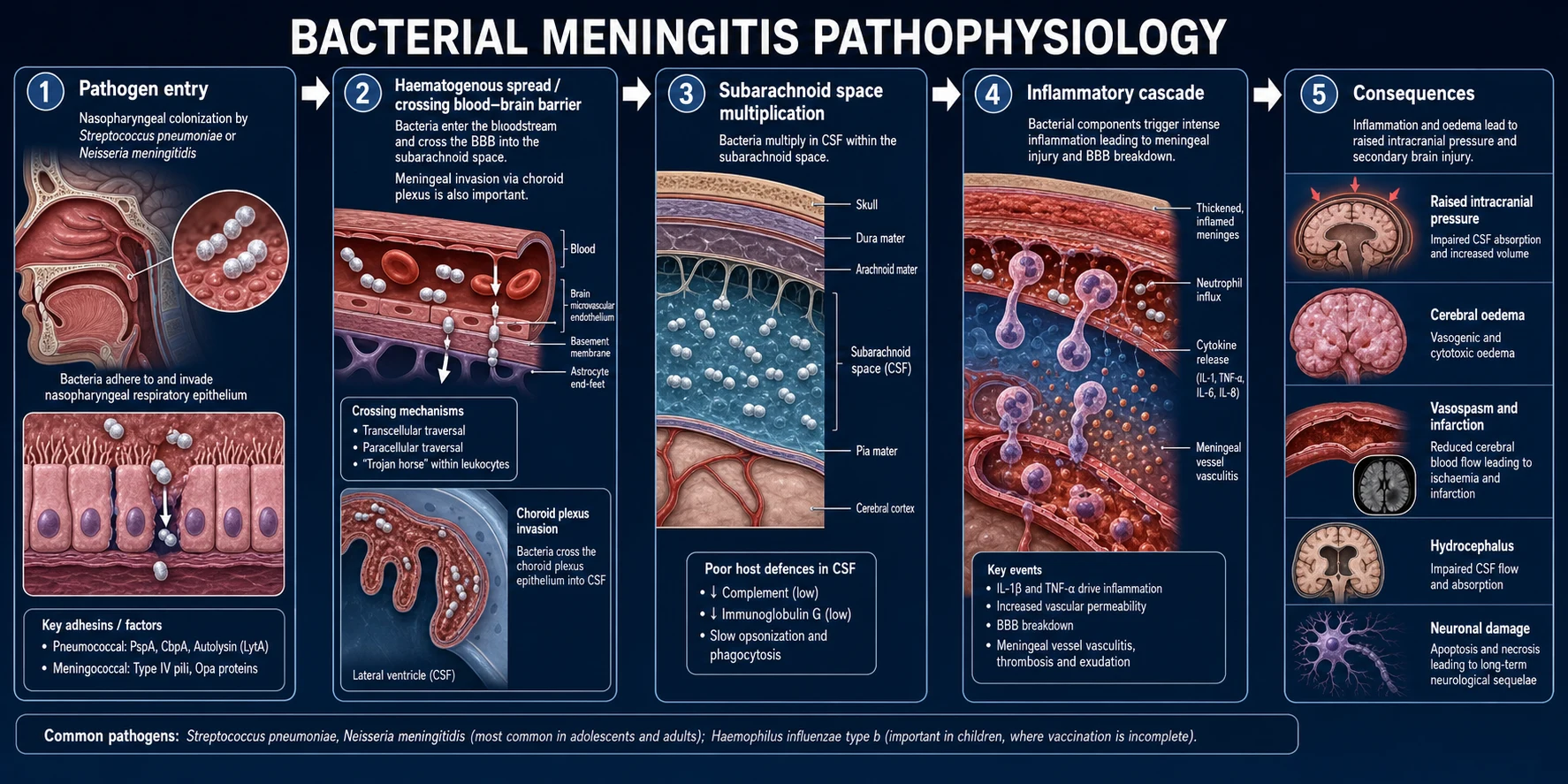
The pathogenesis of bacterial meningitis is a five-stage cascade from nasopharyngeal colonisation to neuronal injury. Understanding it explains why dexamethasone works, why the CSF glucose falls, and why hearing is lost.[1]
Stage 1 — Mucosal colonisation and invasion. S. pneumoniae and N. meningitidis colonise the nasopharynx (meningococcal carriage is common and usually asymptomatic). Meningococcal pili and IgA1 protease, and the pneumococcal polysaccharide capsule and pneumolysin, allow the organism to evade mucosal defences and invade the epithelium.[1]
Stage 2 — Bacteraemia and crossing the blood-brain barrier. The organism enters the bloodstream (bacteraemia — the cause of the petechial rash and septicaemia in meningococcal disease) and reaches the choroid plexus and cerebral capillaries. It crosses the blood-brain barrier by transcytosis across endothelial cells, by surviving within phagocytes ("Trojan horse", especially Listeria and Mycobacterium tuberculosis), or by direct invasion of the choroid plexus epithelium. Less commonly the organism reaches the CSF by contiguous spread (otitis, mastoiditis, sinusitis), by traumatic breach (skull-base fracture, CSF leak), or iatrogenically (neurosurgery, CSF shunt).[1]
Stage 3 — Multiplication in the CSF. The subarachnoid space is a uniquely permissive site for bacterial growth: it contains low complement, low immunoglobulin, and few phagocytes, with slow opsonisation and turnover. Bacteria multiply rapidly, fuelled by their capsule (resists non-immune phagocytosis) and by available nutrients.[1]
Stage 4 — The inflammatory cascade (the key to the whole clinical picture). Bacterial cell-wall components — pneumococcal peptidoglycan/teichoic acid and meningococcal endotoxin (lipopolysaccharide) — activate complement and toll-like receptors (TLR2, TLR4) on meningeal macrophages and endothelial cells, releasing a cytokine storm (IL-1 beta, TNF-alpha, IL-6, CXCL8/IL-8). This recruits a massive neutrophil influx into the CSF (causing the cloudy, purulent fluid and the neutrophilic pleocytosis). Neutrophils and cytokines together:[1]
- Increase blood-brain barrier permeability → vasogenic oedema (protein leaks into CSF → the high CSF protein).
- Damage the glucose transporter (GLUT-1) and increase glucose consumption by neutrophils and bacteria → low CSF glucose.
- Induce vasospasm and vasculitis of the subarachnoid vessels → cerebral ischaemia and infarction (the cause of strokes and cranial-nerve palsies).
- Impair CSF resorption at the arachnoid granulations (blocked by inflammatory debris) → communicating hydrocephalus and raised intracranial pressure.[1]
Stage 5 — Raised intracranial pressure and neuronal injury. The combination of vasogenic + cytotoxic oedema, hydrocephalus, and impaired autoregulation raises intracranial pressure; combined with vasculitic ischaemia and direct bacterial toxicity, this produces neuronal injury — seizures, focal deficits, decreased conscious level and, if unchecked, transtentorial herniation and death. The cochlea is uniquely vulnerable (its aqueduct allows direct bacterial and inflammatory ingress), which is why sensorineural hearing loss is the commonest long-term complication.[1]
Why dexamethasone works — when bacteria are killed by antibiotics, cell-wall fragments are released in large quantities, amplifying the inflammatory cascade (the Jarisch-Herxheimer-like worsening). Dexamethasone, given with or just before the first antibiotic dose, down-regulates the cytokine/chemokine response, reduces BBB disruption, oedema and neuronal injury, and specifically reduces sensorineural hearing loss in pneumococcal meningitis — hence the timing rule (with/before the first dose).[3]
Clinical Presentation
The classic adult triad — fever + neck stiffness + altered mental status — is fully present in only about two-thirds of patients, but almost all have at least two of the three; a patient with fever and headache and any sign of meningeal irritation warrants action.[1]
The full classic picture:[1]
- Fever (often high, with rigors) — present in over 95%.
- Severe, diffuse headache — the commonest single symptom.
- Neck stiffness (meningism, nuchal rigidity) — over 70%; develops over hours.
- Photophobia and eye pain on movement.
- Nausea and vomiting.
- Altered mental status — confusion, drowsiness, agitation; coma is a poor prognostic sign.
- Myalgia, arthralgia, malaise.
- Seizures (focal or generalised) — about 15-30%; a marker of parenchymal involvement.[1]
Meningococcal disease adds the rapidly evolving petechial/purpuric rash — classically non-blanching on the glass test — distributed over the trunk, limbs and mucous membranes, that may progress to purpura fulminans (large confluent purpuric areas with skin necrosis) and septic shock with Waterhouse-Friderichsen syndrome (bilateral adrenal haemorrhage, profound shock, hyponatraemia, hyperkalaemia). Meningococcaemia can progress from a febrile, well-looking patient to shock and death within hours.[1]
Raised intracranial pressure features: decreasing GCS, new seizures, focal neurology, Cushing's triad (hypertension, bradycardia, irregular respiration — a pre-terminal sign), and papilloedema (late). These — plus unilateral pupil dilatation and decerebrate posturing — herald transtentorial herniation.[3]
Atypical presentations (always examined):[1]
- Elderly — confusion, falls, functional decline, anorexia; fever may be absent and neck stiffness subtle. A lower threshold to investigate and treat is essential; Listeria must be covered.
- Immunocompromised — presentation is subtle or indolent; consider Listeria, Cryptococcus, TB. Listeria may produce rhombencephalitis (cranial-nerve palsies, cerebellar signs, hydrocephalus).
- Diabetic / uraemic — fever and confusion may be attributed to the chronic disease; meningeal signs blunted.
- Pregnant — Listeria risk; symptoms overlap with hyperemesis or sepsis of another source.
- Neonate — non-specific: poor feeding, lethargy, irritability, fever or hypothermia, apnoea, seizures (often subtle — cycling movements, lip-smacking), high-pitched cry, bulging fontanelle (late). Neck stiffness is often absent. The threshold to investigate a febrile or non-specifically unwell neonate is very low.[1]
Bacterial meningitis — key numbers
Differential Diagnosis
An acute febrile illness with headache and meningeal signs is not always bacterial meningitis. Distinguish:[1][2]
- Viral (aseptic) meningitis — usually milder, self-limiting, with normal glucose and a lymphocytic CSF. Enterovirus is the commonest cause (summer/autumn, concomitant rash or GI symptoms). Prognosis is excellent; treat HSV if suspected.
- Encephalitis / meningoencephalitis (HSV) — confusion, behaviour change and seizures dominate over meningeal signs; temporal-lobe changes on MRI and periodic lateralised epileptiform discharges (PLEDs) on EEG. Untreated HSV encephalitis has 70% mortality — give IV aciclovir empirically whenever it is possible. CSF: lymphocytes, often red cells (haemorrhagic), normal/mildly low glucose, HSV PCR positive.
- Subarachnoid haemorrhage — thunderclap ("worst ever") headache at onset; blood in the basal cisterns/sulci on CT; xanthochromia and uniform red cells (no clearing) in CSF. May have low-grade fever but is not a febrile-septic illness.
- Tuberculous meningitis — subacute onset (days to weeks), basal meningitis with cranial-nerve palsies (III, VI, VII, VIII), stroke, and hydrocephalus; very low CSF glucose (often under 20-40 mg/dL), lymphocytes, cobweb coagulum, AFB/GeneXpert. HIV co-infection common.
- Cryptococcal meningitis — HIV/AIDS or other immunosuppression; subacute/chronic; CSF shows lymphocytes, low glucose, positive India ink and cryptococcal antigen (CrAg), and often a very high opening pressure requiring therapeutic LPs.
- Brain abscess / subdural empyema — focal neurology predominates; ring-enhancing lesion on imaging; may arise from contiguous otitis/sinusitis/endocarditis or haematogenous (cyanotic heart disease).
- Migraine — severe headache and photophobia but no fever, no septic picture, no meningeal signs.
- Cervical dystonia / mechanical neck pain — no fever, no systemic upset; movement-related.
- Drug-induced aseptic meningitis — NSAIDs, trimethoprim (especially in lupus), IVIG, OKT3; eosinophils may be present in CSF.
- Systemic infection with meningoencephalopathic features — malaria, enteric fever, leptospirosis, rickettsial fever, dengue; CSF usually near-normal but the patient is encephalopathic.
- Autoimmune / neoplastic meningitis — lupus cerebritis, Behcet, carcinomatous/lymphomatous meningitis (cytology positive).[5]
Always specifically consider HSV encephalitis and tuberculous meningitis when the picture is not a straightforward acute bacterial meningitis — both are eminently treatable but missed at great cost.[1]
Clinical & Bedside Assessment
Vital signs and conscious level drive triage. Record temperature, respiratory rate, oxygen saturation, blood pressure, capillary refill, GCS, and blood glucose. Assess for sepsis (qSOFA), shock, and raised ICP.[1]
Meningeal irritation — the named signs (reproduced exactly):[1]
- Kernig sign — with the patient supine and the hip flexed to 90 degrees, passive extension of the knee produces pain or resistance in the back/hamstrings (stretch of the inflamed meninges and nerve roots). Specificity high but sensitivity low (~5%).
- Brudzinski signs:
- Neck (nuchal) sign — passive flexion of the neck produces involuntary flexion of the hips and knees.
- Brudzinski of the cheek — pressure on the cheek produces forearm flexion.
- Contralateral leg sign — passive flexion of one hip and knee produces flexion of the contralateral leg.
- Jolt accentuation of headache — the baseline headache worsens with horizontal rotation of the head two to three times per second; higher sensitivity than Kernig/Brudzinski for meningitis in the alert patient.[1]
Examine the skin for the petechial/purpuric rash of meningococcal disease (perform the glass test — press a glass tumbler against the rash; petechiae/purpura do not blanch), and for purpura fulminans and peripheral gangrene.[1]
Look for the source and the host:[1]
- Ears (otitis media, mastoiditis), nose and throat (sinus tenderness, meningococcal/pharyngeal carriage), skin (cellulitis, infected shunt site), heart (murmur of endocarditis), chest (pneumonia).
- Cranial nerves (III, IV, VI, VII, VIII palsies — VI palsy is a false-localising sign of raised ICP), papilloedema (fundoscopy), and focal motor/sensory deficits.
- CSF shunt / ventricular reservoir — palpate the tubing, look for erythema along the track.
- Stigmata of immunocompromise (oral candidiasis, lymphadenopathy) and head trauma / basal-skull fracture (Battle sign, raccoon eyes, haemotympanum, CSF rhinorrhoea/otorrhoea).[1]
Take blood cultures and a throat swab (for meningococcus) — but do not delay antibiotics if these cannot be obtained instantly.[1]
Investigations
Lumbar puncture (LP) is the diagnostic cornerstone — but the rule of thumb is: antibiotics first, LP when safe. The CSF analysis answers the aetiological question and confirms the diagnosis.[2][4]
Before the LP (and during, in parallel):[2]
- Blood cultures (two sets) — ideally before antibiotics, but never delay antibiotics for them.
- Blood glucose — taken at the same time as the CSF glucose so a CSF-to-serum ratio can be calculated.
- FBC, U&E (watch for SIADH/hyponatraemia), LFT, coagulation, CRP, lactate, and blood gas (acidosis of sepsis).
- Throat swab / EDTA blood for meningococcal/pneumococcal PCR (especially after antibiotics).
- HIV test (cryptococcal and TB risk).
- Coagulation and platelets before LP (correct coagulopathy/thrombocytopenia; platelet count over 50 is generally safe).[5]
When to obtain CT head BEFORE lumbar puncture
Do NOT delay antibiotics. Obtain CT before LP when any of the following are present (the universally cited indications):[2][4]
- Immunocompromise (HIV, transplant, chemotherapy, immunosuppressants).
- New-onset seizures (within 1 week).
- Papilloedema or other signs of raised ICP.
- Abnormal level of consciousness (decreased GCS / confused).
- Focal neurological deficit (including III, IV, VI, VII, VIII palsies).
- History of CNS disease (mass lesion, stroke, infection).
- Head trauma within the past 1 week.
- Prolonged or unresponsive coma.[5]
A normal CT does not fully exclude raised pressure, and a contrast-enhanced CT adds sensitivity for abscess/empyema. If LP must be deferred, start empirical antibiotics immediately and reconsider LP once the patient is stabilised (a delayed LP still helps with aetiology even after antibiotics — PCR and cellular pattern persist for days).[2]
The CSF analysis (reproduced verbatim)
Bacterial
- Cloudy/turbid; opening pressure raised
- Neutrophils 100-5000 (PMN predominance)
- Protein over 1 g/L (100 mg/dL)
- Glucose under 40 mg/dL OR under 40% of serum
- Gram stain and culture positive; PCR if pretreated
Viral
- Clear; opening pressure normal/mildly raised
- Lymphocytes 10-500 (neutrophils early, then lymphs)
- Protein normal or mildly raised (under 1 g/L)
- Glucose normal (usually over 40% of serum)
- Enterovirus/HSV PCR; culture rarely needed
Tuberculous
- Fibrin web/cobweb coagulum; pressure raised
- Lymphocytes (PMNs early); 50-500 cells
- Protein markedly raised (1-5 g/L)
- Glucose VERY LOW (under 20-40 mg/dL)
- AFB stain (low yield), GeneXpert/NAAT, culture (slow)
Fungal (Crypto)
- Clear/slightly cloudy; OPENING PRESSURE OFTEN VERY HIGH
- Lymphocytes (may be paucicellular in advanced HIV)
- Protein mildly-moderately raised
- Glucose low to normal
- India ink positive; cryptococcal antigen (CrAg) highly sensitive
CSF thresholds — high-yield:[2]
- CSF glucose under 40 mg/dL, OR CSF-to-serum glucose ratio under 0.4 (under 0.31 strongly favours bacterial) → bacterial.
- CSF protein over 1 g/L (100 mg/dL) → bacterial; over 1.5 g/L with a very low glucose and lymphocytes → TB.
- CSF white-cell count over 1000/mm3, neutrophilic → bacterial.
- CSF lactate — over 4 mmol/L favours bacterial; under 3 mmol/L favours viral (where available).[2]
Special tests when indicated: multiplex PCR panels (e.g. FilmArray ME — simultaneous detection of the common bacterial, viral and fungal targets within about an hour), CSF cryptococcal antigen, AFB smear and GeneXpert MTB/RIF / Xpert Ultra, enterovirus and HSV-1/2 PCR, meningococcal and pneumococcal PCR (especially valuable after antibiotics have sterilised the culture), VDPR/RPR (syphilis), cytology (malignant), oligoclonal bands (autoimmune). Repeat LP is reserved for patients who fail to improve.[2]
Imaging beyond CT: MRI brain with contrast if abscess, subdural empyema, ventriculitis, cerebral oedema, or basal-exudate of TB meningitis is suspected. MRI temporal-lobe changes (T2/FLAIR hyperintensity, often bilateral but asymmetric) → HSV encephalitis. EEG if seizures or encephalopathy.[2]
Management — Resuscitation
ABCDE first. Secure the airway; give oxygen to keep SpO2 at 94-98% (or 88-92% in chronic CO2 retainers); gain IV access; treat shock, seizures and raised ICP.[2][4]
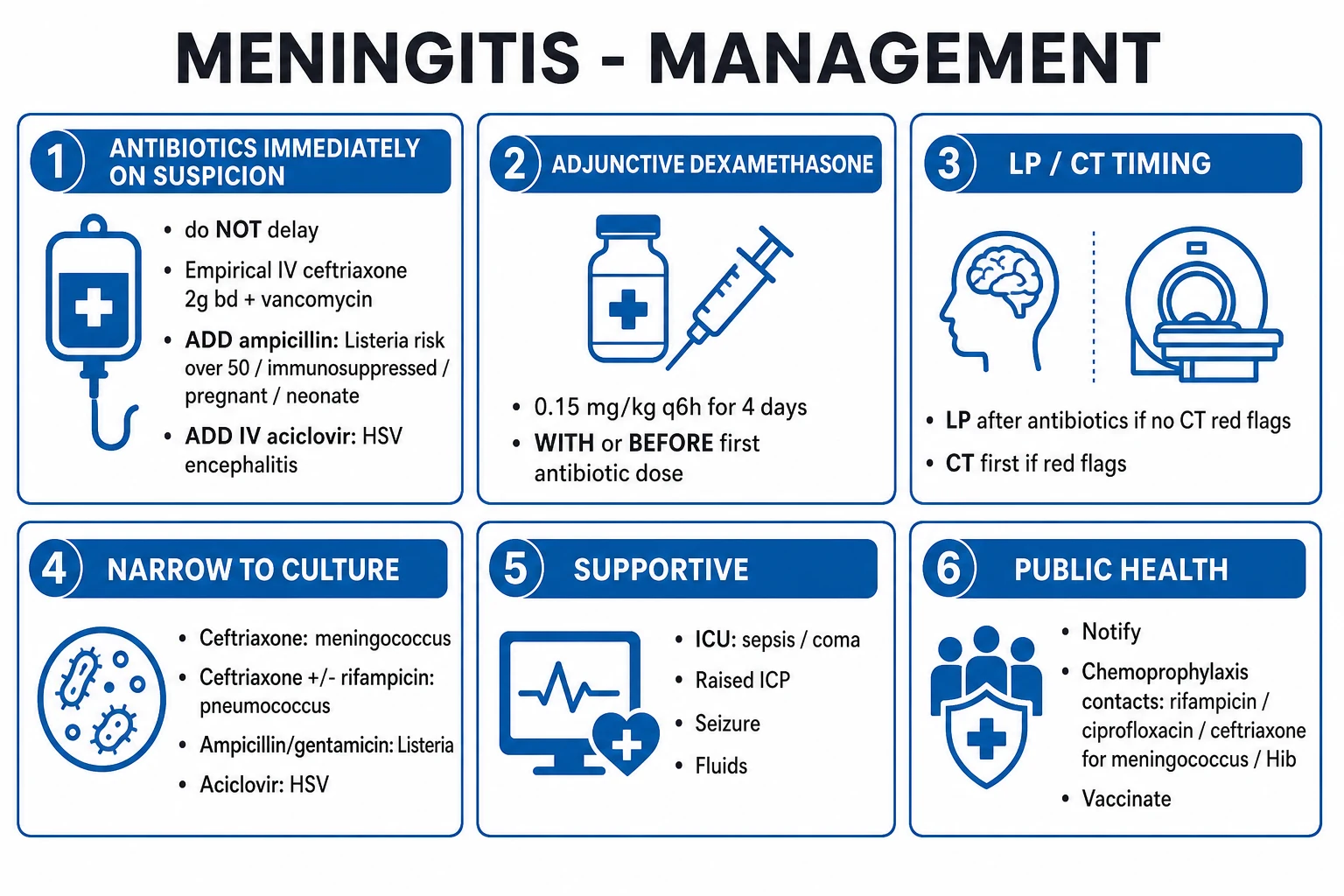
The non-negotiable rule: give empirical IV antibiotics IMMEDIATELY on suspicion of bacterial meningitis — do NOT delay for blood cultures, LP, or CT. A useful model: if you suspect bacterial meningitis, the antibiotic is given before the patient leaves the bedside.[1][2]
Adjunctive dexamethasone — give IV dexamethasone 0.15 mg/kg (adult ~10 mg) every 6 hours for 4 days, with or 15-20 minutes before the first antibiotic dose, in suspected pneumococcal meningitis. Continue only if pneumococcal is confirmed; do not give in neonatal or clearly meningococcal disease. The landmark trial (de Gans and van de Beek) showed reduced mortality in pneumococcal meningitis and reduced hearing loss overall.[3]
Empirical antibiotic regimen — adult community-acquired (with drug, dose, route):[1]
- IV ceftriaxone 2 g every 12 hours (covers S. pneumoniae incl. many penicillin-resistant strains, N. meningitidis, H. influenzae).
- PLUS IV vancomycin (load 15-20 mg/kg, then 15-20 mg/kg every 8-12 h to trough 15-20 mg/L) — for penicillin-resistant pneumococcus and MRSA cover. (Where beta-lactam allergy or high-resistance, vancomycin + a respiratory fluoroquinolone such as moxifloxacin is an alternative.)
- PLUS IV ampicillin 2 g every 4 hours (or amoxicillin 2 g 4-hourly) if Listeria is possible — age over 50, immunocompromised, pregnant, neonate, alcoholic.
- PLUS IV aciclovir 10 mg/kg every 8 hours (over 1 h infusion) if HSV encephalitis is possible (confusion, seizures, temporal changes) — until HSV PCR is negative.[2]
Meningococcal septicaemia in shock: apply the Surviving Sepsis hour-1 bundle — oxygen, blood cultures, lactate, broad-spectrum antibiotics within 1 hour, balanced crystalloid 30 mL/kg for hypotension or lactate over 4, noradrenaline for fluid-refractory shock, and reassess fluid responsiveness. Give empirical ceftriaxone 2 g IV immediately (do not wait for the full bundle). Isolate the patient with droplet precautions until 24 hours of antibiotics have been given. Notify public health.[2]
Raised ICP management (if signs of herniation): elevate the head of the bed to 30 degrees, maintain normoxia, normocapnia (PaCO2 4.5-5.0 kPa — avoid prophylactic hyperventilation), and normoglycaemia; give IV mannitol 0.25-1 g/kg or hypertonic saline (3%) 250 mL; treat seizures aggressively (IV lorazepam 4 mg, then IV levetiracetam 60 mg/kg or phenytoin 20 mg/kg); obtain urgent CT and involve neurosurgery if there is obstructive hydrocephalus (external ventricular drain) or a surgical mass lesion.[2]
Management — Definitive & Stepwise
Once the organism and susceptibility are known, de-escalate to directed therapy. The regimens below (drug + dose + route + duration) are the standard adult doses; neonatal and paediatric doses are weight-based (see Special Populations).[2][4]
Directed antimicrobial therapy — common organisms
| Organism | Drug (adult) | Route & dose | Duration |
|---|---|---|---|
| S. pneumoniae (penicillin-susceptible) | Benzylpenicillin (or ceftriaxone) | Penicillin 2.4 g IV 4-hourly; ceftriaxone 2 g IV BD | 10-14 days |
| S. pneumoniae (penicillin-resistant) | Ceftriaxone + vancomycin (+/- rifampicin) | As above; vanco to trough 15-20 mg/L | 14 days |
| N. meningitidis | Ceftriaxone (or penicillin) | 2 g IV BD | 7 days |
| H. influenzae type b | Ceftriaxone | 2 g IV BD | 7 days |
| Listeria monocytogenes | Ampicillin + gentamicin | Ampicillin 2 g IV 4-hourly; gentamicin 5 mg/kg OD (stop gent after 1 week) | 21 days |
| Group B strep | Benzylpenicillin (or ampicillin) | Penicillin 2.4 g IV 4-hourly | 14-21 days |
| Gram-negative bacilli | Cefotaxime / ceftazidime / cefepime (or meropenem) | 2 g IV 6-8-hourly | 21 days |
| Post-neurosurgical / shunt | Vancomycin + ceftazidime or cefepime (+/- rifampicin) | Plus remove/externalise infected shunt | 10-14 days after shunt removal; intraventricular therapy if retained |
| HSV encephalitis | Aciclovir | 10 mg/kg IV TDS (over 1 h) | 14-21 days |
Dexamethasone — 0.15 mg/kg IV every 6 hours for 4 days; start with or 15-20 min before the first antibiotic dose; continue only if pneumococcal is confirmed (no benefit — and possible harm — in meningococcal or neonatal). If dexamethasone was not given with the first dose, it may still be given with the next dose if the LP confirms a gram stain consistent with pneumococcus, but the benefit is greatest when started before antibiotics.[3]
Step-down and oral switch — most meningitis therapy is IV throughout (CSF penetration of oral agents is usually inadequate); oral step-down is reserved for selected, fast-responding patients with susceptible organisms and good bioavailability (e.g. fluoroquinolone for fully sensitive meningococcal disease after clinical response).[3]
Escalation triggers to ICU
Transfer to intensive care if any of: GCS under 8 (intubate and ventilate), seizures or status epilepticus, septic shock, raised intracranial pressure or signs of herniation, respiratory failure, hyponatraemia from SIADH with seizures, or rapidly deteriorating conscious level.[3]
Meningococcal public-health measures (the question that always comes up)
- Isolate the index case with droplet precautions until 24 hours of effective antibiotics.
- Notify public health (statutory notification of suspected meningococcal disease).
- Chemoprophylaxis of close contacts within 24 hours (ideally): oral ciprofloxacin 500 mg single dose (adult; preferred — single dose, well tolerated) OR rifampicin 600 mg every 12 hours for 2 days (4 doses); in pregnancy, give IM ceftriaxone 250 mg single dose (avoid ciprofloxacin/rifampicin if possible). Paediatric doses are weight-banded.
- Vaccinate close contacts if the strain is vaccine-preventable; consider benzylpenicillin prophylaxis for GPs/delay — but the index case also needs chemoprophylaxis if treated with ceftriaxone for under 7 days (ceftriaxone eradicates carriage, but a 1-dose fluoroquinolone is belt-and-braces in some guidance).[1]
Adjunctive and disease-specific therapy
- Hearing assessment — all survivors should have a formal audiology assessment before discharge and at 6-8 weeks; early cochlear implantation for profound loss.
- Vaccination history — give missing vaccines before discharge; the index case may need MenACWY/MenB boosters.
- Thromboprophylaxis (LMWH) per VTE risk once bleeding risk is acceptable.[5]
Specific Subtypes & Scenarios
Viral meningitis — most cases are enterovirus (echo, coxsackie; summer/autumn, often with a rash or GI illness), HSV-2 (primary genital herpes), mumps (parotitis, orchitis; where unvaccinated), HIV (seroconversion illness — send HIV test), and arboviruses (Japanese encephalitis, West Nile — regional). Management is supportive (analgesia, hydration, antiemetics); give IV aciclovir empirically whenever HSV encephalitis is possible until HSV PCR is negative. Prognosis is excellent in most immunocompetent adults; recovery within days to weeks.[1]
HSV encephalitis — the treatable archetype of viral encephalitis; HSV-1 in adults, often with temporal-lobe features (behaviour change, aphasia, complex partial seizures, anosmia). CSF: lymphocytes, often red cells (haemorrhagic), mildly raised protein; HSV PCR (sensitive after 24-48 h). MRI shows T2/FLAIR hyperintensity in the temporal lobes (often bilateral, asymmetric); EEG shows PLEDs. Treat with IV aciclovir 10 mg/kg TDS for 14-21 days; start empirically in any suspected encephalitis. Untreated mortality is ~70%; with aciclovir ~15-30% but high residual morbidity (memory, behaviour, seizures).[2]
Tuberculous meningitis — subacute-chronic, with prodrome (malaise, low-grade fever, headache) for 1-3 weeks then meningism, cranial-nerve palsies (especially VI), stroke (basal-ganglia infarct from vasculitis of the lenticulostriate vessels), and hydrocephalus. CSF: very low glucose, lymphocytes, high protein, cobweb coagulum; AFB stain yield is low (~10-20%), GeneXpert/Xpert Ultra improves it; culture is slow (weeks). Treat with RIPE (Rifampicin, Isoniazid, Pyrazinamide, Ethambutol) + a 5th agent (ethionamide or aminoglycoside) for 2 months, then Rifampicin + Isoniazid for 7-10 months (total 9-12 months); ADD corticosteroids (dexamethasone or prednisolone taper) — mortality benefit (in HIV-negative; benefit in HIV-positive is not confirmed by the 2023 ACT HIV trial).[5]
Cryptococcal meningitis — Cryptococcus neoformans / gattii, classically in HIV/AIDS with CD4 under 100, transplant recipients, and other T-cell-deficient states. Subacute/chronic presentation; CSF is often paucicellular in advanced HIV (poor host response) with a markedly raised opening pressure, lymphocytes, low glucose, high protein. India ink (sensitivity ~50-70%), cryptococcal antigen (CrAg) in CSF and serum (highly sensitive), and culture. Treat with liposomal amphotericin B 3-4 mg/kg/day + flucytosine 25 mg/kg QDS for 2 weeks (induction), then high-dose fluconazole 800 mg/day for 8 weeks (consolidation), then 200 mg/day maintenance until immune reconstitution. Therapeutic lumbar punctles (daily if needed) for raised opening pressure are a key adjunct; acetazolamide and shunting may be needed.[5]
Neonatal meningitis — see Special Populations; organisms GBS, E. coli K1, Listeria; empirical IV ampicillin + cefotaxime (or an aminoglycoside); avoid ceftriaxone in the neonate (biliary sludging, kernicterus — displaces bilirubin).[1]
Post-neurosurgical / CSF-shunt — coagulase-negative staph (S. epidermidis), S. aureus, Gram-negatives including Pseudomonas, and Cutibacterium (Propionibacterium) acnes. Empirical IV vancomycin + ceftazidime or cefepime (anti-pseudomonal); remove or externalise the infected shunt (it is a foreign body — antibiotics alone rarely cure); intraventricular therapy (vancomycin) may be needed if the shunt is retained. CSF from a shunt tap shows the organism.[1]
Recurrent meningitis — every patient with a second episode needs a hunt for a correctable predisposition: CSF leak (high-resolution CT/MRI cisternography, beta-2 transferrin in nasal fluid), complement pathway deficiency (CH50, AP50, individual complement components), asplenia, humoral immunodeficiency, anatomical defect (dermal sinus tract, midline cleft), or Mollaret meningitis (HSV-2). Vaccinate (pneumococcal, meningococcal ACWY + B, Hib) and consider lifelong prophylaxis where appropriate (e.g. eculizumab-receiving patients).[1]
Complications & Pitfalls
Acute / early:[1]
- Septic shock and multi-organ failure (especially meningococcal); DIC and purpura fulminans with peripheral and skin necrosis requiring skin/limb grafting; Waterhouse-Friderichsen (bilateral adrenal haemorrhage — give stress-dose hydrocortisone).
- Seizures (early and late) and status epilepticus.
- Raised intracranial pressure with cerebral oedema and transtentorial herniation — the commonest cause of early death.
- Stroke (arterial vasculitis or venous sinus thrombosis), subdural empyema/effusion, cerebral abscess, ventriculitis.
- Hyponatraemia from SIADH — common; can cause seizures; correct slowly with hypertonic saline if severe.
- Cranial-nerve palsies — III, IV, VI (false-localising), VII, VIII (hearing).[1]
Long-term:[1]
- Sensorineural hearing loss — the commonest long-term complication (~10%, higher in children and pneumococcal disease); reason for dexamethasone and audiology follow-up.
- Cognitive impairment, behavioural change, focal neurological deficits, epilepsy, visual loss.
- Hydrocephalus (communicating or obstructive — may need a shunt).
- Ataxia, developmental delay (children).[3]
Classic pitfalls (the examiner's favourites):[1]
- Delaying antibiotics for LP, blood cultures, or CT — the single most dangerous and most common error.
- Not covering Listeria in the over-50, pregnant, immunocompromised, or neonatal patient (add ampicillin).
- Not adding aciclovir when HSV encephalitis is possible (a treatable, lethal disease).
- Giving dexamethasone too late — the benefit is with/before the first antibiotic dose.
- Missing TB or Cryptococcus in the subacute/immunosuppressed patient.
- Forgetting chemoprophylaxis of meningococcal contacts within 24 hours.
- Over-relying on a normal CT to exclude raised ICP before LP (clinical criteria decide).
- Using ceftriaxone in the neonate (use cefotaxime + ampicillin).
- Not doing an audiology follow-up.
- Attributing confusion in the elderly to dementia or sepsis of another source.[3]
Prognosis & Disposition
Mortality and morbidity — adult community-acquired bacterial meningitis has a case-fatality of 10-30% (pneumococcal highest, up to 20-30%; meningococcal ~5-10% for meningitis but 10-40% with septicaemia); 20-30% of survivors have permanent neurological sequel (deafness, cognitive impairment, epilepsy, focal deficits). HSV encephalitis has ~70% mortality untreated and ~15-30% even with aciclovir, with high residual morbidity. Tuberculous meningitis prognosis is stage-dependent (MRC grade I ~80-90% good outcome, grade III ~50% mortality); permanent deficit is common.[1]
Poor prognostic factors: very young or old age, immunocompromise, delay in antibiotics, coma (low GCS) at presentation, seizures, bacteraemia/pneumococcal aetiology, thrombocytopenia, high CSF bacterial load, low CSF leucocyte count relative to bacterial load (poor host response), and septic shock.[1]
Disposition:[1]
- ICU if GCS under 8, seizures/status, shock, raised ICP, or respiratory failure.
- Ward (with close observation) once stable, neurologically improving, and on directed therapy.
- Discharge when afebrile, neurologically stable, with a plan for IV therapy completion (inpatient or OPAT) and audiology at 6-8 weeks.
- Follow-up with audiology, neuropsychology if cognitive impairment, and review of vaccination status.[1]
Special Populations
[1]Neonate (0-28 days) — presentation is non-specific (poor feeding, lethargy, irritability, fever or hypothermia, apnoea, seizures, bulging fontanelle late); neck stiffness is often absent. Organisms: GBS (early-onset under 7 days, late-onset 7-90 days), E. coli K1, Listeria, Klebsiella. Empirical: IV ampicillin 100 mg/kg + cefotaxime 50 mg/kg (or an aminoglycoside such as gentamicin); avoid ceftriaxone (bilirubin displacement, biliary sludging). Duration: GBS 14-21 days, Gram-negative 21 days, Listeria 14-21 days (ampicillin + aminoglycoside). Low threshold to LP in any febrile or non-specifically unwell neonate; NICE sepsis guidance applies.[1]
Pregnancy — physiological immunosuppression of cell-mediated immunity increases Listeria risk; empirical regimen adds ampicillin. Safe antibiotics: ceftriaxone, ampicillin, aciclovir. Avoid ciprofloxacin in pregnancy if alternatives exist (theoretical cartilage effects); for meningococcal prophylaxis in pregnancy use ceftriaxone 250 mg IM single dose. Meningitis in pregnancy increases the risk of preterm labour and fetal loss; involve obstetrics early.[1]
Elderly (over 50) — atypical/blunted presentation (confusion, falls, no fever, subtle neck stiffness); Listeria and pneumococcus predominate; always add ampicillin; lower threshold to admit, image (CT before LP), and treat; beware polypharmacy (renal dosing, drug interactions) and aspiration.[1]
Immunocompromised (HIV, transplant, anti-TNF, chemotherapy, complement blockade) — broaden empirically: cover Listeria (ampicillin), HSV (aciclovir), and consider TB, Cryptococcus, Gram-negatives; CT before LP (mass lesions common); if cryptococcal is suspected, send CSF and serum CrAg and measure opening pressure (often very high — therapeutic LPs). Complement deficiency or eculizumab/ravulizumab → recurrent meningococcal disease: vaccinate with MenACWY + MenB (4CMenB) AND give meningococcal prophylaxis on any exposure.[1]
Post-neurosurgery / CSF shunt — empirical vancomycin + ceftazidime or cefepime (cover staph including MRSA and Pseudomonas); remove or externalise the infected shunt (foreign body); consider intraventricular vancomycin (5-20 mg/day) if the shunt is retained or ventriculitis is severe; duration 10-14 days after hardware removal.[1]
Anticoagulated patient — warfarin/DOAC is a relative contraindication to LP; reverse (vitamin K + PCC for warfarin; specific reversal agents for DOACs) and confirm normal coagulation before LP. Do not delay antibiotics for reversal.[1]
Evidence, Guidelines & Regional Differences
Landmark trial — dexamethasone (de Gans & van de Beek, NEJM 2002). A multicentre, randomised, double-blind, placebo-controlled European trial of adjunctive dexamethasone (10 mg every 6 h for 4 days, given with or just before the first antibiotic dose) in adults with acute bacterial meningitis. It reduced mortality overall (from 25% to 15%) — driven by the pneumococcal subgroup — and reduced hearing loss (especially in H. influenzae and pneumococcal disease), without an increase in gastrointestinal bleeding. Subsequent meta-analyses and the ESCMID/IDSA guidelines endorse dexamethasone for suspected or proven pneumococcal meningitis, given with/before the first antibiotic dose, and not for meningococcal or neonatal disease.[3]
[3]India (ICMR/NCDC, NTEP) and the developing world: community resistance to penicillin and rising cephalosporin resistance in S. pneumoniae; TB and Cryptococcus are far more common (HIV burden); Japanese encephalitis, enterovirus, and mumps are regionally important viral causes; scrub typhus and leptospirosis can mimic meningitis. Empirical therapy commonly ceftriaxone 2 g BD + vancomycin + ampicillin (high Listeria and resistant-pneumococcus burden); GeneXpert/Xpert Ultra for CSF TB is widely available under the National TB Elimination Programme (NTEP); dexamethasone benefit in bacterial meningitis has been harder to demonstrate in low-income settings (possibly because of late presentation, malnutrition, HIV co-infection, and high rates of pretreatment). Vaccination coverage is expanding under the Universal Immunisation Programme (Hib as pentavalent, PCV, MenA in outbreaks); meningococcal Hajj vaccination is mandatory for pilgrims.
Key guideline sources:[2]
- ESCMID 2016 (van de Beek et al.) — diagnosis and treatment of acute bacterial meningitis: empirical regimens, LP timing, dexamethasone indications.[2]
- IDSA / Tunkel 2004 — practice guidelines for the management of bacterial meningitis (adults and children, including shunt infection).[4]
- Surviving Sepsis Campaign (SSC) hour-1 bundle — applies to meningococcal septicaemia.
- NICE CG102 / NG51 (UK) — bacterial meningitis and meningococcal septicaemia in children; NICE CKS for adults.
- WHO — integrated management of childhood illness (IMCI); TB and HIV-associated meningitis guidance.
Controversies:[2]
- Dexamethasone in low-income settings and in antibiotic-pretreated patients — benefit attenuated; some guidelines are selective.
- Routine CT before LP — Auburtin (2006) showed clinical criteria predict the unsafe LP better than CT findings; overuse of CT delays LP and antibiotics.
- PCR replacing culture — multiplex panels are fast but expensive; culture still needed for susceptibility.
- ACT HIV 2023 (Donovan et al.) — adjunctive dexamethasone did not improve survival in HIV-positive tuberculous meningitis, refining the long-held assumption that steroids always help TBM.[5]
- Adjunctive glycerol, immunoglobulin, and hypothermia — not routine; investigational.
Vaccination (the prevention that examiners reward):[5]
- Hib conjugate — near-elimination of H. influenzae type b meningitis.
- Pneumococcal conjugate (PCV10/13/15/20) — dramatic fall in vaccine-serotype pneumococcal meningitis; non-vaccine serotypes and the 23-valent polysaccharide (PPSV23) in older adults.
- Meningococcal — MenACWY (conjugate) and MenB (4CMenB / Trumenba) — adolescent boosters, complement deficiency, asplenia, Hajj, outbreaks.
- MMR — mumps meningitis prevention.
- Japanese encephalitis, rabies (post-exposure) — regional / risk-based.[5]
Exam Pearls
Meningitis — empirical antibiotic regimen by LAMP
LAMP
add ampicillin if over 50, pregnant, immunocompromised, or neonate
add if HSV encephalitis possible (confusion, seizures, temporal changes)
ceftriaxone 2 g BD + vancomycin (cover penicillin-resistant pneumococcus)
0.15 mg/kg with/before the first antibiotic dose (pneumococcal benefit)
- Classic triad: FEVER + NECK STIFFNESS + ALTERED MENTAL STATUS — but two of three is enough to act.
- Meningococcal: NON-BLANCHING PETECHIAL/PURPURAR RASH; antibiotics within 1 hour; isolate 24 h; chemoprophylax contacts.
- Empirical IV antibiotics IMMEDIATELY on suspicion — do NOT delay for LP/CT/blood cultures.
- CSF bacterial: cloudy, NEUTROPHILS high, PROTEIN high, GLUCOSE LOW (under 40 mg/dL or under 40% of serum), high opening pressure.
- CSF viral: lymphocytes, NORMAL glucose, mildly raised protein. CSF TB: very low glucose + cobweb coagulum. CSF Cryptococcus: India ink + CrAg, very high opening pressure.
- Add AMPICILLIN for Listeria (over 50, pregnant, immunocompromised, neonate).
- Add ACICLOVIR if HSV encephalitis suspected (temporal changes, seizures, confusion).
- DEXAMETHASONE 0.15 mg/kg q6h x 4 days, with/before first antibiotic dose — pneumococcal benefit; reduces deafness.
- CT before LP: immunocompromise, new seizures, papilloedema, altered GCS, focal neurology, trauma, prolonged coma, CNS disease.
- Hearing loss is the commonest complication → dexamethasone + audiology follow-up.
- Organisms by age: neonate GBS/E. coli/Listeria; child pneumo/meningo/Hib; adult pneumo/meningo; over 50 add Listeria.
- Chemoprophylaxis of contacts: ciprofloxacin 500 mg PO STAT (or rifampicin/ceftriaxone in pregnancy).
- Kernig & Brudzinski signs; jolt accentuation.
- Post-neurosurgery/shunt: vancomycin + ceftazidime/cefepime; remove the shunt.
- Complement/properdin deficiency + eculizumab → recurrent meningococcal disease.
- Neonate: avoid ceftriaxone (use ampicillin + cefotaxime).
- Listeria rhombencephalitis; TB basal meningitis + cranial-nerve palsies; HSV temporal-lobe changes.
- Waterhouse-Friderichsen = bilateral adrenal haemorrhage in meningococcal septicaemia → give stress-dose steroids.[3]
Exam application bank (NEET-PG / INICET)
One-line answer
Bacterial meningitis is a life-threatening medical emergency — acute inflammation of the meninges and subarachnoid space, most often from haematogenous spread of Streptococcus pneumoniae or Neisseria meningitidis. Classic triad: fever, headache, neck stiffness plus photophobia, vomiting, altered mental status and seizures; meningococcal disease adds a rapidly evolving petechial/purpuric rash and septicaemia. Organisms by age: neonate — Group B strep, E. coli, Listeria; child — meningococcus, pneumococcus, Hib; adult — pneumococcus, meningococcus; over 50 / immunocompromised / pregnant — add Listeria. Diagnosis rests on lumbar puncture CSF (cloudy, neutrophils over 1000, protein over 1 g/L, glucose under 40 mg/dL or under 40% of serum, positive Gram stain/culture) — but CT head first when red flags are present, and empirical IV antibiotics must never be delayed for the LP or CT. Treat[1]
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard.[1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes.[1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change.[1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each.[1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory.[1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Bacterial Meningitis & Acute Meningoencephalitis.
References
- [1]van de Beek D, Brouwer M, Hasbun R, Koedel U, Whitney CG, Wijdicks E. Community-acquired bacterial meningitis. Nature Reviews Disease Primers, 2016.PMID 27808261
- [2]van de Beek D, Cabellos C, Dzupova O, et al. ESCMID guideline: diagnosis and treatment of acute bacterial meningitis. Clinical Microbiology and Infection, 2016.PMID 27062097
- [3]de Gans J, van de Beek D. Dexamethasone in adults with bacterial meningitis. New England Journal of Medicine, 2002.PMID 12432041
- [4]Tunkel AR, Hartman BJ, Kaplan SL, et al. Practice guidelines for the management of bacterial meningitis. Clinical Infectious Diseases, 2004.PMID 15494903
- [5]Donovan J, Bang ND, Imran D, et al. Adjunctive dexamethasone for tuberculous meningitis in HIV-positive adults. New England Journal of Medicine, 2023.PMID 37819954