Infectious Diseases · General Medicine
Tetanus
Also known as Tetanus · Lockjaw · Clostridium tetani infection
Tetanus is an acute, toxin-mediated neurological disease caused by Clostridium tetani tetanospasmin released from spores germinating in anaerobic, necrotic wounds. The toxin travels retrogradely in motor nerves to the spinal cord and brainstem, cleaves synaptobrevin (VAMP), and blocks release of the inhibitory neurotransmitters glycine and GABA, producing unopposed sustained muscle contraction and reflex spasms with a preserved sensorium. The classic phenotype is trismus (lockjaw), risus sardonicus, opisthotonos and stimulus-triggered spasms, progressing to autonomic instability and respiratory failure. Diagnosis is clinical — there is no useful laboratory test. Management rests on three pillars: neutralise unbound toxin (human tetanus immunoglobulin, HTIG), eradicate the organism (wound debridement plus metronidazole), and control spasms and support vital functions in ICU (benzodiazepines, magnesium sulphate, mechanical ventilation, autonomic control) — followed by active vaccination, because the disease does not confer immunity. Tetanus is entirely preventable by DTaP/Tdap vaccination every 10 years, wound prophylaxis, and maternal immunisation.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Overview & Definition
Tetanus is an acute, non-communicable, toxin-mediated neurological disease caused by the anaerobic, spore-forming, Gram-positive bacillus Clostridium tetani. The organism itself rarely causes invasive infection or tissue destruction; almost all the illness is the work of a single exotoxin — tetanospasmin (tetanus neurotoxin, TeNT) — that the bacillus releases after germinating in a necrotic, anaerobic wound. The toxin is carried retrogradely along motor nerves to the spinal cord and brainstem, where it cleaves synaptobrevin (VAMP, a SNARE protein) and prevents release of the inhibitory neurotransmitters glycine and GABA. Loss of inhibition produces the clinical signature of tetanus: sustained, severe muscle contraction (rigidity), reflex spasms provoked by any stimulus, and — in severe disease — autonomic instability, all with a fully preserved sensorium.[3][1]
Two facts dominate the clinical approach. First, the diagnosis is entirely clinical — there is no laboratory test that confirms or excludes tetanus in time to matter, and treatment must begin on recognition. Second, tetanus is entirely preventable by vaccination, yet it remains a disease of the unvaccinated in every country; the tetanus-prone wound in an under-immunised person is a public-health emergency, not a routine dressing change.[3][4]

Classification
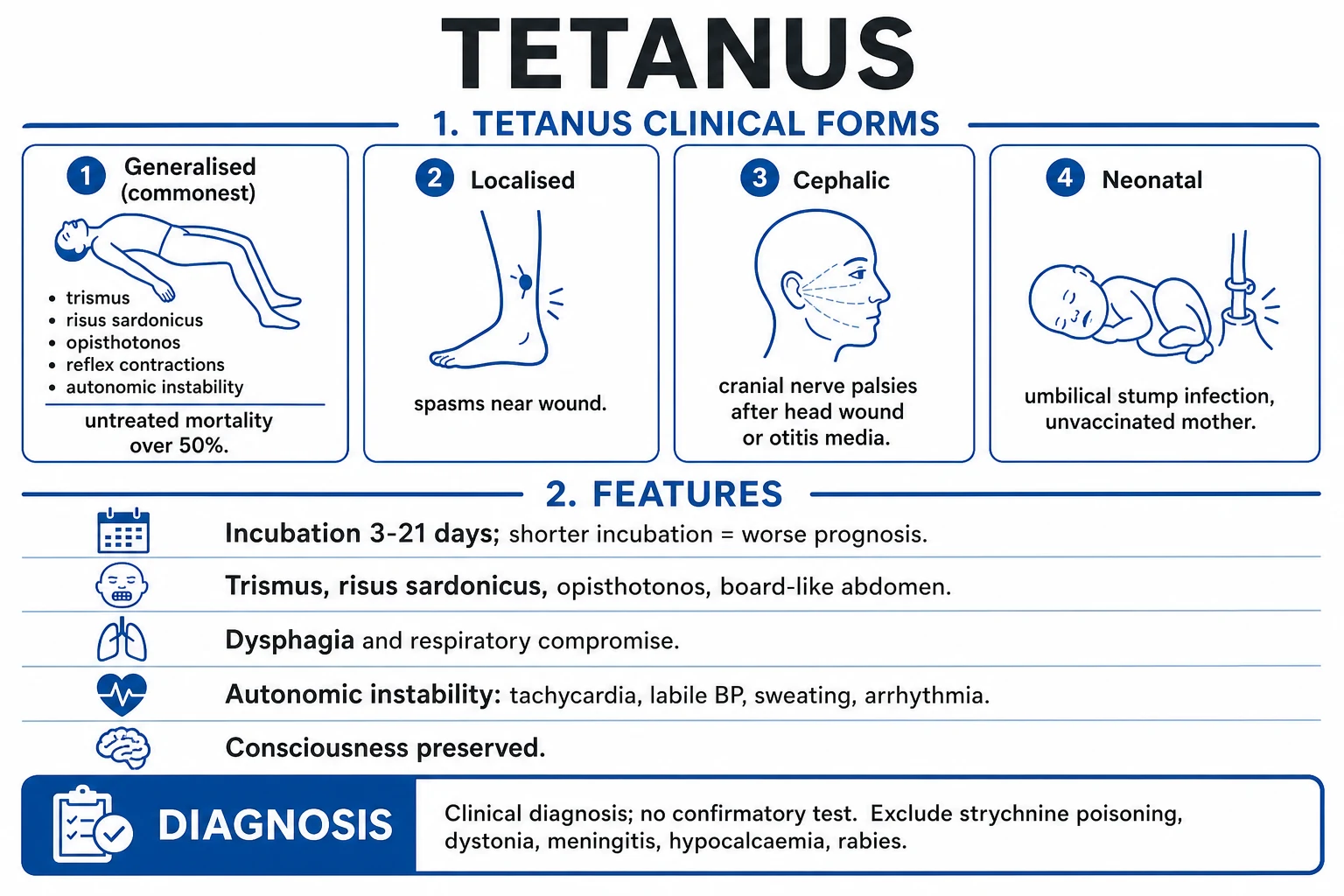
Tetanus is classified by its clinical form (the distribution of muscle involvement), because each form carries a different portal of entry, prognosis, and management emphasis.[3]
Generalised tetanus
- The commonest form (about 80% of cases)
- Descending pattern: trismus first, then risus sardonicus, neck stiffness, dysphagia, opisthotonos, board-like abdomen, then reflex spasms and autonomic instability
- Sensorium preserved throughout
- Mortality 10-40% even with ICU care; over 50% untreated
Localised tetanus
- Persistent rigidity/spasm confined to muscles near the causative wound (e.g. a single limb)
- Often precedes generalised tetanus by days
- Milder, favourable prognosis if it remains localised
- May occur in partially immune patients
Cephalic tetanus
- Rare; follows head/face wounds, otitis media, or dental infection
- Cranial nerve dysfunction (most often CN VII palsy) with trismus
- Can progress to generalised tetanus
- Particularly poor prognosis
Neonatal tetanus
- Generalised tetanus in a neonate, usually from umbilical stump infection in an infant of an unvaccinated mother
- Onset day 5-14 of life: poor sucking, rigidity, spasms, opisthotonos
- Case-fatality 50-90% without ICU; **eliminated by maternal vaccination**
- One of the WHO target diseases for elimination
Severity grading is essential for ICU triage and for comparing outcomes. The widely used Ablett classification (Ablett 1967, four grades) stratifies by the intensity of spasms, the presence of autonomic disturbance, and the need for ventilation:[5]
| Ablett grade | Clinical features | Management |
|---|---|---|
| Grade I (mild) | Mild to moderate trismus; generalised rigidity; no spasms, no dysphagia, no autonomic signs | Ward-level care; benzodiazepines; observe |
| Grade II (moderate) | Moderate trismus and rigidity; brief reflex spasms provoked by stimuli; no autonomic dysfunction; no respiratory compromise | Quiet room, benzodiazepines; usually ward/HDU |
| Grade III (severe) | Severe trismus, generalised rigidity; prolonged spasms, dysphagia, reflex spasms on minimal stimuli, tachycardia, beginning autonomic instability | ICU; consider paralysis and ventilation |
| Grade IV (very severe) | Grade III plus severe autonomic instability (labile or sustained hypertension/hypotension, marked tachycardia, arrhythmias) often requiring ventilation and vasoactive drugs | ICU, mechanical ventilation, magnesium, autonomic control |
Epidemiology & Risk Factors
C. tetani spores are ubiquitous in soil, dust and animal (especially horse) manure worldwide; they survive boiling for short periods and resist most disinfectants. The organism is therefore an environmental contaminant rather than a communicable pathogen, and every skin breach in an under-immunised person is a potential portal.[3]
Tetanus is now rare where immunisation programmes are robust, but it has not been eradicated — it remains a disease of the unvaccinated and under-vaccinated in every region. High-risk groups and exposures:[1][3]
Host at risk
- Never vaccinated / incomplete primary series
- Lapsed boosters (over 10 years since last dose, or over 5 years for a tetanus-prone wound)
- Elderly (waning immunity, lapsed boosters)
- Neonates of unvaccinated or under-vaccinated mothers
- Intravenous drug users (skin abscesses, heroin contaminants)
- People in remote/rural areas with poor vaccine access
Wound/exposure at risk
- Puncture wounds (nail, splinter, thorn)
- Contaminated wounds: soil, manure, rust
- Necrotic/avascular tissue, deep wounds, retained foreign body
- Burns, frostbite, crush injuries
- Umbilical stump (neonate) when instrument/cord-care is unclean
- Surgical wounds, dental infection, otitis media, chronic ulcers (diabetic foot), IM injections in drug users
- Tattooing/body piercing with unsterile technique
Neonatal tetanus — historically a major cause of neonatal death — has been eliminated (under 1 case per 1000 live births in every district) in most of the world through maternal tetanus toxoid vaccination and clean delivery/cord care. It persists where mothers are unvaccinated, as targeted by the WHO maternal and neonatal tetanus elimination (MNTE) initiative.[4]
Pathophysiology
The entire disease is the consequence of a single molecular cascade. Understanding it explains why consciousness is preserved, why the toxin is irreversible, why the incubation period predicts severity, and why magnesium works.[3][1]
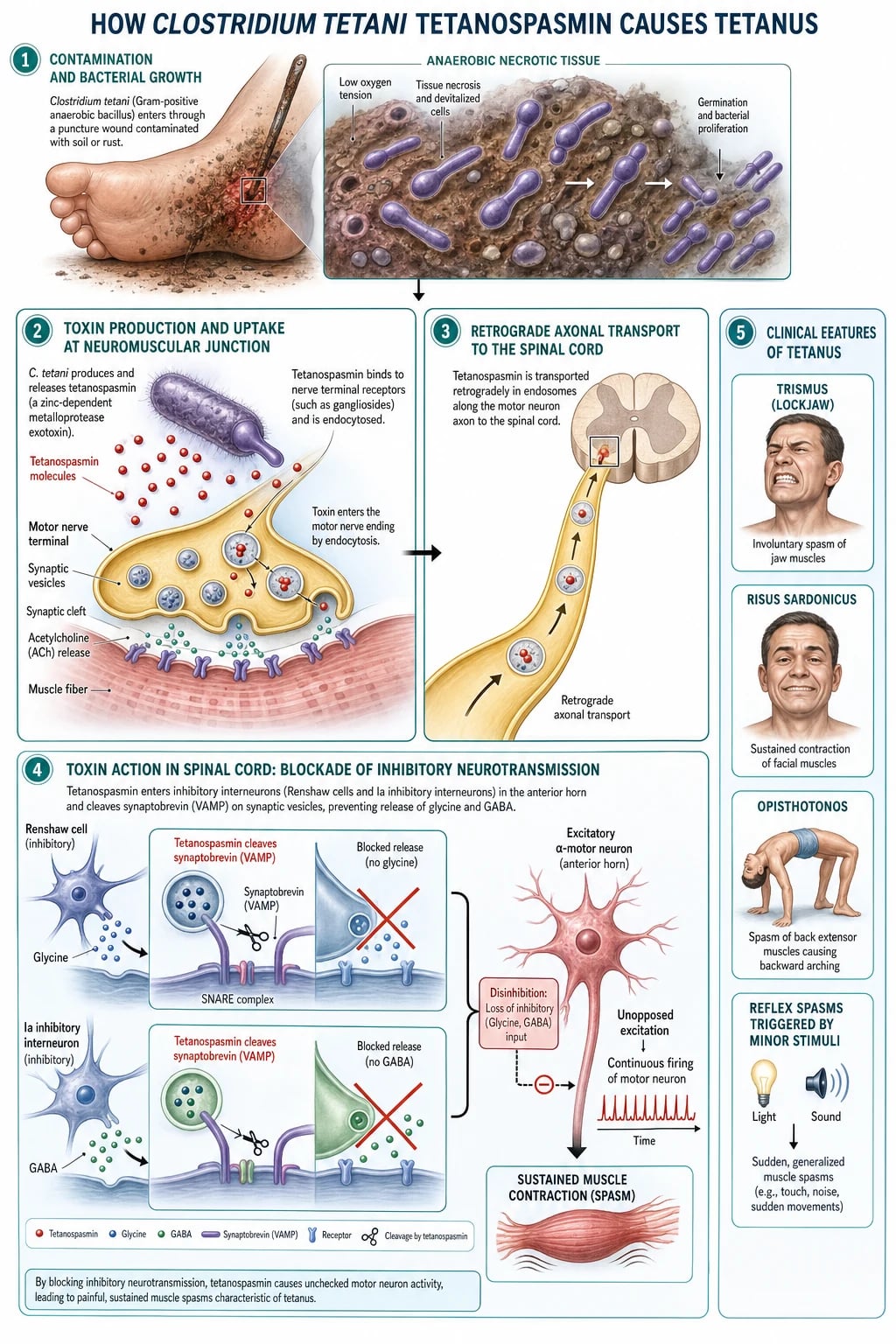
1. Inoculation and germination. C. tetani spores enter a wound. They germinate only under anaerobic, low-redox conditions — necrotic tissue, foreign body, crush injury, or a deep puncture that seals over. The bacilli multiply locally but rarely invade or cause local inflammation; in fact the wound may look trivial or have healed by the time symptoms begin.[3]
2. Toxin production and uptake. Germinating bacilli release tetanospasmin (TeNT), a 150-kDa zinc-endopeptidase neurotoxin (the same family as botulinum toxin). The toxin's heavy chain binds GD1b/GT1b gangliosides and a protein receptor (SV2/Niacetamide receptor) on the presynaptic membrane of motor neurones at the neuromuscular junction. Binding triggers endocytosis.[3]
3. Retrograde axonal transport. The endocytosed toxin travels retrogradely along the motor axon to the cell body in the anterior horn of the spinal cord (or the equivalent motor nucleus of a cranial nerve). Some toxin then crosses to inhibitory interneurons (Renshaw cells and other glycinergic/GABAergic interneurons) in the spinal cord and brainstem. This axonal journey is the basis of the incubation period — the longer the nerve the toxin must climb, the longer the incubation, and the shorter the incubation the heavier the toxin load and the worse the disease.[3]
4. SNARE cleavage and blockade of inhibition. Inside the inhibitory presynaptic terminal, the toxin's light chain — a zinc-dependent endopeptidase — cleaves synaptobrevin (VAMP, vesicle-associated membrane protein), one of the SNARE proteins required for synaptic-vesicle exocytosis. With the SNARE clipped, synaptic vesicles can no longer fuse and the neurone cannot release its neurotransmitter. For tetanospasmin the relevant transmitters are the inhibitory amino acids glycine (Renshaw-cell inhibition of the motor neurone) and GABA. Their loss removes recurrent and reciprocal inhibition of motor neurones and of autonomic pathways.[3][1]
5. Clinical translation. Loss of inhibition produces:[3]
- Sustained muscle contraction (rigidity) — tonic overactivity of antagonistic muscle groups: trismus (masseters close first), risus sardonicus (facial muscles), opisthotonos (paraspinal muscles arch the back), board-like abdominal rigidity, and nuchal rigidity.
- Reflex spasms — any sensory stimulus (light, sound, touch, suction) fires motor neurones that are no longer braked by inhibition, producing violent, painful, prolonged spasms that can cause laryngospasm, apnoea, fractures and rhabdomyolysis.
- Autonomic instability — loss of inhibition in the brainstem and sympathetic centres produces labile hypertension and hypotension, tachycardia and bradycardia, arrhythmias, profuse sweating and salivation, typically peaking in the second week.
- Preserved consciousness and sensation — because tetanospasmin acts on inhibitory motor interneurons and autonomic centres, not on sensory pathways or the cortex, the patient remains awake, aware and in agony throughout. This single fact distinguishes tetanus from almost every mimic.[3]
6. Irreversibility and recovery. Once the SNARE is cleaved the inhibition cannot be reversed; recovery requires the synthesis and transport of new synaptobrevin and the formation of new synaptic terminals — a process taking 4 to 6 weeks. This is why the disease runs its full course even when the toxin is neutralised and the organism eradicated, and why survivors need prolonged rehabilitation.[3]
TARGET
Tetanospasmin vs botulinum toxin — the mirror image (an exam favourite). Both are zinc-endopeptidase neurotoxins that cleave SNARE proteins and block neurotransmitter release; they differ in where they act.[3]
Tetanospasmin (tetanus)
- Enters motor nerve ending at the NMJ, travels retrogradely to the spinal cord
- Acts on inhibitory interneurons (Renshaw cells); blocks glycine and GABA
- Net effect: loss of inhibition → sustained excitation, rigidity and spasms
- Consciousness preserved; cranial nerves spared early (except cephalic form)
Botulinum toxin (botulism)
- Stays at the neuromuscular junction; does NOT travel centrally
- Acts on the motor nerve ending itself; blocks acetylcholine release
- Net effect: flaccid paralysis, descending, with cranial nerve palsies early
- No spasms; autonomic (parasympathetic) dysfunction is hypofunctional
Clinical Presentation
The classical picture is a descending sequence of increasing rigidity and spasm in a patient who is fully alert.[3][1]
Onset — trismus (lockjaw). The first symptom in about 50-75% of patients is trismus — painful spasm of the masseter muscles that prevents the patient from opening the mouth. This is also the first sign to be misattributed (to dental abscess, tonsillitis, or temporomandibular dysfunction). Trismus is followed within hours to days by dysphagia, neck stiffness and a feeling of generalised apprehension.[2]
Established disease — the classic triad.[3]
- Risus sardonicus — sustained spasm of the facial muscles producing a characteristic grinning grimace (eyebrows raised, corners of the mouth drawn back and up).
- Opisthotonos — extreme spasm of the paraspinal muscles arching the back so that the head and heels approach the bed and the body rests on the occiput and heels.
- Board-like abdominal rigidity — sustained contraction of the abdominal wall that may mimic an acute abdomen.[3]
Reflex spasms. Once rigidity is established, any stimulus — a sudden noise, a light switched on, a touch, an airway suction catheter, or even the patient's own cough — triggers a violent, painful, sustained spasm that may last seconds to minutes. Laryngospasm during a spasm is immediately life-threatening (sudden apnoea, hypoxic arrest); spasms of the respiratory muscles cause respiratory failure.[3]
Autonomic instability (severe disease, second week). Loss of inhibition in autonomic centres produces labile hypertension alternating with hypotension, tachycardia (occasionally bradycardia from vagal storms), arrhythmias, profuse sweating, salivation, and pyrexia. Autonomic failure is the leading cause of death in patients who survive the early spasms.[5]
Sensorium is preserved. The patient is awake, terrified and in severe pain throughout — a defining feature that helps separate tetanus from meningitis, encephalitis and status epilepticus, in which consciousness is impaired.[3]
Neonatal tetanus
- Onset day 5-14 of life in an infant of an unvaccinated mother
- First signs: poor sucking, excessive crying, clenched fists, refusal to feed
- Then generalised rigidity, opisthotonos, spasms triggered by touch/feeding, apnoea
- Umbilical stump often the portal (unclean instrument/cord care)
- High mortality; preventable by maternal tetanus toxoid during pregnancy
Cephalic tetanus
- Follows otitis media, head/face/scalp wounds, dental infection
- Cranial nerve palsy (CN VII most often; also III, IV, VI, IX, X, XII) with trismus
- Dysphagia, facial spasm; may evolve to generalised tetanus
- Carries a poor prognosis
Localised tetanus
- Rigidity/spasm confined to the muscles near the wound (often a limb)
- Mild, indolent course; can persist for weeks
- May precede generalisation by several days
Atypical / partially immune
- A patient with partial immunity may have only localised or mild disease
- Elderly patients may present with vague stiffness, dysphagia and falls before classic trismus
Differential Diagnosis
The combination of trismus, rigidity, stimulus-triggered spasms and a clear sensorium with a relevant wound is essentially diagnostic. The difficulty is the early case (isolated trismus) or the atypical case. Each mimic has a discriminating feature.[2][3]
Strychnine poisoning
- The closest mimic — same mechanism (glycine antagonist at the postsynaptic receptor), same spasms, same preserved consciousness
- Distinguishing features: no wound, no fever, **inter-spasm relaxation** (muscles flaccid between spasms), rapid onset after ingestion, history of exposure (pesticide, herbal remedy)
- Treat supportively; decontaminate GI tract
Drug-induced dystonia (e.g. metoclopramide, haloperidol)
- Acute onset trismus/oculogyric crisis/neck torticollis after a dopamine antagonist
- No opisthotonos, no autonomic storms, no wound
- **Rapidly resolves with IV benztropine or diphenhydramine** — a diagnostic and therapeutic test
Peritonsillar/retropharyngeal abscess or severe tonsillitis
- Trismus from local pain and inflammation; fever, sore throat, toxic appearance
- Asymmetric peritonsillar fullness, uvular deviation; CT confirms
- Sensorium may be impaired if sepsis; no generalised rigidity
Meningitis / encephalitis
- Fever, headache, altered sensorium, meningeal signs
- Sensorium usually impaired (unlike tetanus); no stimulus-triggered reflex spasms; CSF abnormal
- Seizures in encephalitis are not stimulus-provoked and are followed by a post-ictal state
Rabies
- Bite history; phobic spasms (hydrophobia, aerophobia), fluctuating consciousness, progressing to coma and death
- Spasms are pharyngeal/laryngeal on swallowing, not whole-body rigidity; no opisthotonos
- Almost universally fatal once symptomatic
Hypocalcaemic tetany
- Carpopedal spasm, perioral tingling, Trousseau and Chvostek signs
- Low serum ionised calcium; no stimulus-triggered generalised spasms; no preserved opisthotonos
- Resolves with IV calcium gluconate
Status epilepticus / subcontinuous seizures
- Impaired consciousness between seizures; post-ictal confusion; EEG diagnostic
- Not stimulus-triggered; no sustained inter-seizure rigidity
Stiff-person syndrome
- Chronic autoimmune (anti-GAD) rigidity and spasms over months; not acute
- Insidious, no wound, no fever
Clinical & Bedside Assessment
A focused assessment has three goals: confirm the clinical diagnosis, grade severity (Ablett), and identify the portal of entry.[3]
Confirming the diagnosis at the bedside.[3]
- Trismus — inability to open the mouth; the spatula test is a useful bedside manoeuvre. A spatula is touched against the posterior pharyngeal wall: a positive test is reflex spasm of the masseters biting down on the spatula (rather than the normal gag). It is highly suggestive of tetanus in the right context.
- Risus sardonicus and opisthotonos are pathognomonic in combination.
- Board-like abdominal rigidity (with the patient unable to relax the abdominal wall) is present even between spasms; it must not be mistaken for a surgical abdomen.[3]
Grading severity (Ablett) — re-applied through the illness, because a patient can deteriorate from grade II to grade IV over hours (see the Classification table). Grade III/IV mandates ICU for airway protection, paralysis/ventilation and autonomic control.[5]
Identifying the portal. Examine every skin break: punctures, lacerations, burns, ulcers (including the diabetic foot), the umbilicus in a neonate, recent injections in an IV drug user, otitis media, dental sepsis. Remember that in up to 15-25% of cases no portal is found — a normal-looking wound does not exclude tetanus.[3]
Monitoring in established disease. Continuous ECG, SpO2, BP (arterial line in severe disease), spasm frequency, temperature, urine output, and — when magnesium is used — serum magnesium levels and deep tendon reflexes (loss of the patellar reflex is the first sign of magnesium toxicity).[5]
Investigations
There is no diagnostic laboratory test for tetanus. The diagnosis is made clinically and the role of investigations is to exclude mimics and to support the critically ill patient.[3][1]
[1]Tests to exclude mimics:[1]
- Serum calcium and albumin (corrected or ionised) — exclude hypocalcaemic tetany.
- Serum creatine kinase — may be elevated from muscle spasm (and rhabdomyolysis with AKI), but is non-specific.
- Toxicology screen — strychnine, theophylline, antipsychotics (for dystonia).
- CSF analysis — in meningitis/encephalitis the CSF is abnormal; in tetanus it is normal.
- Neuroimaging (CT/MRI brain) — exclude space-occupying lesions and stroke where the picture is unclear.
- EEG — distinguish status epilepticus.[1]
Wound cultures for C. tetani are insensitive and slow; the organism is fastidious and may be absent by the time of presentation. They should not delay treatment.[1]
ICU monitoring in severe tetanus:[5]
- Continuous ECG and intra-arterial BP; telemetry for arrhythmias.
- SpO2 and (if ventilated) capnography and serial blood gases.
- Serum magnesium every 6-12 hours during magnesium infusion (target 2-4 mmol/L); check knee reflexes before each dose.
- U&E, creatinine, CK (for rhabdomyolysis/AKI), glucose, lactate; blood cultures if line infection/sepsis suspected.
- DVT prophylaxis status; pressure-area and nutrition assessment.[5]
Management — Resuscitation
Tetanus is a time-critical medical emergency. The resuscitation bundle is run concurrently with the diagnostic assessment and is aimed at preventing death from airway obstruction, respiratory failure and a violent spasm.[3][2]
ABCDE — with tetanus-specific priorities.[2]
- Airway/Breathing — place the patient in a quiet, dark, undisturbed room; minimise noise, light, suction and unnecessary handling. High-flow oxygen. Have suction and intubation equipment immediately at the bedside because laryngospasm may occur without warning. Early elective endotracheal intubation (or tracheostomy) is indicated for grade III/IV disease, recurrent laryngospasm, or worsening respiratory function — the threshold to intubate should be low.
- Circulation — IV access; treat hypotension with cautious fluids; prepare for autonomic storms (have labetalol, morphine, magnesium and vasopressors available).
- Disability — give a benzodiazepine immediately to control spasms and reduce anxiety. IV diazepam 10 mg (or 0.1-0.2 mg/kg) titrated to spasm control, repeated as required, is the standard first agent; midazolam is preferred for continuous infusion.
- Exposure — examine for the portal (every skin break); remove the source (see definitive management).[5]
The single most important nursing intervention is the dark, quiet room. Any sensory input can trigger a fatal spasm; in severe cases even a dropped instrument or a door slamming has precipitated fatal laryngospasm.[2]
Management — Definitive & Stepwise
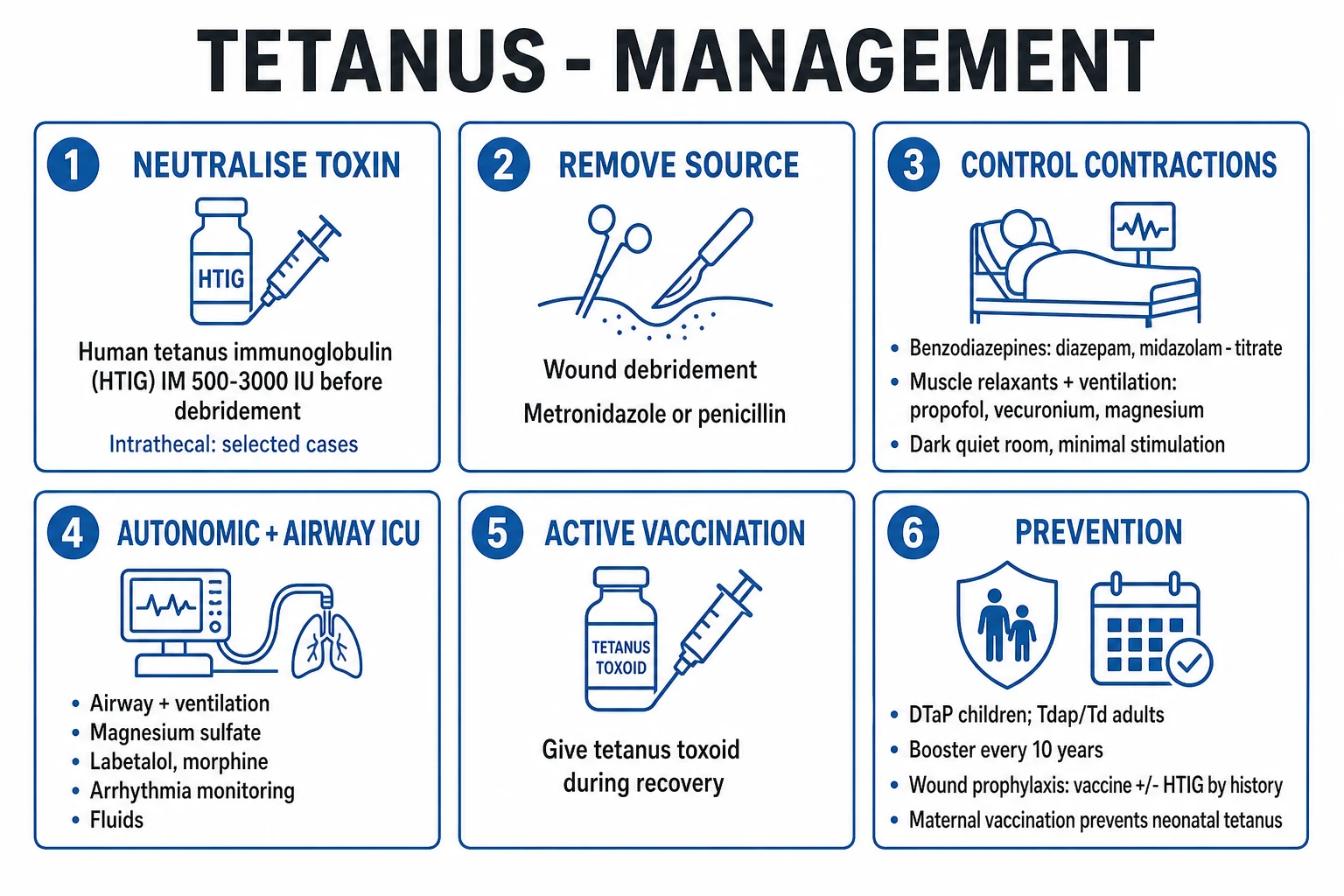
Definitive treatment is built on three pillars: neutralise unbound toxin, eradicate the organism and remove its anaerobic source, and control spasms with intensive support. To these is added a fourth, non-negotiable step — active vaccination of the survivor, because the toxin dose that produces disease is too small to induce immunity.[3]
Neutralise unbound toxin
Human tetanus immunoglobulin (HTIG) IM 500 IU (range 500-3000 IU), ideally BEFORE wound debridement so toxin released by manipulation is mopped up. Inactivates only free toxin — it cannot reverse toxin already bound to nerves.
Eradicate the organism
IV metronidazole 500 mg q8h (or 400 mg PO q12h for 7-10 days) is preferred; surgical wound debridement of necrotic tissue to remove the anaerobic source.
Control spasms and support
Benzodiazepines (diazepam or midazolam infusion) titrated; add IV magnesium sulphate in severe disease; paralysis + mechanical ventilation for grade IV or refractory spasms; treat autonomic instability; ICU nursing.
Active vaccination
Full tetanus toxoid primary series (or booster) — surviving tetanus does NOT confer immunity, because the toxin dose causing disease is sub-immunogenic. Give the first dose at discharge, complete the schedule.
Pillar 1 — Neutralise unbound toxin: human tetanus immunoglobulin (HTIG)
HTIG (human tetanus immune globulin) provides passive immunity by binding and neutralising circulating, unbound tetanospasmin. It does not reverse toxin already bound to nerve tissue (which is irreversible), so it limits disease progression but does not abolish existing symptoms.[3][6]
- Dose and route: 500 IU IM as soon as the diagnosis is made (some authorities use 3000-6000 IU; there is no strong evidence favouring higher doses, and 500 IU is the WHO-supported practical dose). A proportion is infiltrated around the wound before debridement; the rest is given IM at a site distant from the toxoid vaccination site (so the immunoglobulin does not blunt the active immune response).
- Timing: ideally before wound debridement, so that toxin released by surgical manipulation is neutralised.
- Equine antitoxin is used in many low-resource settings where HTIG is unavailable (10 000-20 000 U IV/IM after a test dose), but carries a significant risk of serum sickness and anaphylaxis; HTIG is preferred wherever available.[6]
Intrathecal HTIG has been studied as a way of delivering antitoxin directly to the CNS. A 2022 factorial randomised controlled trial (Van Hao et al., Lancet Global Health) compared human IM antitoxin versus equine IM antitoxin, each with or without intrathecal human antitoxin. Human IM antitoxin was superior to equine IM antitoxin (less disease progression, lower mortality), and adding intrathecal antitoxin did not improve outcome — supporting the use of HTIG by the IM route without intrathecal administration.[6]
Pillar 2 — Eradicate the organism and remove its anaerobic source
- Metronidazole is the antibiotic of choice. IV metronidazole 500 mg every 8 hours for 7-10 days (or oral 400 mg every 12 hours where appropriate) eradicates the bacillus.[3]
- Avoid high-dose penicillin G. Penicillin is bactericidal against C. tetani but is structurally a GABA antagonist; high doses can worsen spasms. Metronidazole avoids this and is at least as effective. Where neither is available, macrolides (erythromycin) or doxycycline are alternatives.
- Surgical wound debridement — remove all necrotic tissue, foreign bodies and sealed-over scabs that create the anaerobic environment, ideally after HTIG has been given so that toxin released by manipulation is neutralised. Even a trivial-appearing wound should be opened and cleaned.[2]
Pillar 3 — Control spasms and support vital functions
Benzodiazepines are the cornerstone: they bind the GABA-A receptor and enhance inhibitory tone, partially countering the loss of GABA/glycine. Diazepam has been traditional (large doses, e.g. 10-40 mg IV, repeated, or 100-300 mg/24 h by infusion); midazolam is preferred for continuous infusion because of its shorter half-life and predictable kinetics (e.g. 0.05-0.2 mg/kg/h).[3]
Magnesium sulphate — in severe (grade III/IV) tetanus — inhibits presynaptic catecholamine release and competes with calcium at the neuromuscular junction, controlling both spasms and autonomic storms and reducing the need for sedation and ventilation. The Thwaites 2006 randomised controlled trial established its role: IV magnesium sulphate loading 40 mg/kg over 30 min, then infusion 1-3 g/h (or 0.5-2 g/h) titrated to abolish spasms while preserving the knee jerk (target serum magnesium 2-4 mmol/L). It reduced the need for mechanical ventilation and for verapamil, but did not reduce overall mortality — magnesium is an adjunct, not a replacement for ICU care.[5]
Magnesium sulphate (severe tetanus)
Spasm and autonomic control in Ablett III/IV tetanus
Dose
Load 40 mg/kg IV over 30 min (max ~5 g adult); then 1-3 g/h IV infusion titrated to spasm frequency and the patellar reflex
Neuromuscular blockade and mechanical ventilation are required when spasms cannot be controlled, when there is recurrent laryngospasm, or in grade IV disease with autonomic storms. Vecuronium or rocuronium infusion with propofol/midazolam/fentanyl sedation and lung-protective ventilation provides complete spasm control. A tracheostomy is performed early in the ventilated course because the duration of paralysis is usually weeks.[3]
Autonomic instability — treated with morphine infusion (0.05-0.2 mg/kg/h, blunts sympathetic surges), magnesium (above), beta-blockers (esmolol or labetalol for hypertension/tachycardia — avoid long-acting propranolol which can precipitate sudden cardiac death from unopposed vagal surges), and vasopressors/inotropes for hypotensive episodes. Swings of BP and heart rate can be extreme; titrate carefully.[5]
General supportive care — nasogastric or parenteral nutrition (the metabolic demand of constant muscle activity is high), DVT prophylaxis, pressure-area care, stress-ulcer prophylaxis, careful fluid/electrolyte balance, and prevention of nosocomial infection. The course is long (weeks of ICU), and complications are the rule rather than the exception.[3]
Pillar 4 — Active vaccination of the survivor
Survivors of tetanus must be actively vaccinated. The quantity of toxin that causes clinical disease is too small to provoke a protective antibody response, so a single episode of tetanus confers no immunity. Give a full primary course of tetanus toxoid (3 doses) or, if previously partially vaccinated, complete the series, and reinforce every 10 years. Plan the first dose before or at discharge.[3][7]
Specific Subtypes & Scenarios
Neonatal tetanus
Generalised tetanus in the neonate, almost always from infection of the umbilical stump (unclean instrument or cord care, application of animal dung or ash) in an infant of a mother without protective antitoxin antibody. Onset is between day 5 and day 14 of life with poor sucking, irritability and excessive crying, progressing to generalised rigidity, opisthotonos and spasms triggered by handling or feeding, then apnoea. Case-fatality is high (50-90%) without ICU, and elimination (under 1 case per 1000 live births in every district) is achieved by maternal tetanus toxoid immunisation and clean delivery/cord care.[4]
Cephalic tetanus
Rare; follows otitis media, head/face/scalp lacerations, or dental infection. The toxin acts on cranial nerve nuclei producing a lower-motor-neurone cranial nerve palsy (most often CN VII) together with trismus. It may progress to generalised tetanus and carries a poor prognosis.[3]
Localised tetanus
Persistent rigidity/spasm of muscles near the wound (often a single limb), sometimes persisting for weeks. It may herald generalised tetanus. It is milder and occurs more often in partially immune patients.[1]
Tetanus in special exposures
- IV drug users — skin abscesses, contaminated heroin (which may contain C. tetani spores); often unvaccinated.
- Diabetic foot ulcers and chronic wounds — a portal in the elderly with waning immunity.
- Post-surgical / post-partum / intra-abdominal — rare, often severe, sometimes with no obvious wound; tetanus has been described after abdominal surgery and septic abortion.
- Immunisation omission — a survivor of an incomplete primary series remains at risk of a further episode.[3]
Complications & Pitfalls
Complications of the disease:[3][5]
Respiratory
- Laryngospasm and sudden apnoea (an immediate killer)
- Respiratory failure from spasm of respiratory muscles
- Aspiration pneumonia
- Ventilator-associated pneumonia in prolonged ICU stays
Autonomic / cardiovascular
- Labile hypertension and hypotension
- Arrhythmias and sudden cardiac death (the leading late cause of death)
- Myocarditis and shock
Musculoskeletal / metabolic
- Vertebral and long-bone fractures from violent spasms
- Rhabdomyolysis with acute kidney injury
- Hyperthermia from sustained muscle activity
Critical-illness complications
- Deep vein thrombosis and pulmonary embolism
- Decubitus ulcers, contractures
- Critical-illness polyneuropathy/myopathy
- Nosocomial and line infections
Classic pitfalls (each costs lives):[3]
- Diagnosing something else — attributing trismus to a dental abscess and missing early tetanus.
- Delaying or omitting HTIG because the diagnosis is "not yet confirmed" — there is no confirmatory test.
- Using high-dose penicillin G alone — GABA-antagonist effect worsens spasms; use metronidazole.[3]
- Nursing in a normal bright ward — any stimulus can trigger fatal laryngospasm; the patient must be in a quiet, dark room.
- Forgetting to vaccinate the survivor — tetanus recurs; the disease does not immunise.[3]
- Underestimating autonomic instability — the patient who survives the spasms can still die of arrhythmia in the second week.
Prognosis & Disposition
Mortality is determined by the severity grade, the tempo of onset, the access to ICU, and the patient's age and comorbidity.[3][5]
Adverse prognostic factors: incubation period under 7 days; onset-to-spasm interval under 48 hours; severe (Ablett III/IV) presentation; autonomic instability; cephalic tetanus; neonatal tetanus; IV drug use; extremes of age; delayed presentation; and lack of access to ICU, HTIG and mechanical ventilation.[3]
Recovery and rehabilitation. Because the toxin-nerve binding is irreversible, recovery requires regeneration of new synapses over 4-6 weeks; rigidity and spasms gradually subside. Rehabilitation addresses deconditioning, contractures, swallowing, and psychological sequelae. Survivors must complete active vaccination.[3]
Disposition. Grade I-II may be managed on a quiet ward/HDU; grade III/IV, autonomic instability, recurrent laryngospasm or respiratory compromise mandate ICU. Isolate the patient from stimuli; plan tracheostomy for the prolonged ventilated course; arrange vaccination before discharge.[5]
Special Populations
Pregnancy — preventing neonatal tetanus
Maternal vaccination is the cornerstone of neonatal-tetanus elimination. Protective antitoxin antibody is transferred transplacentally and protects the neonate at birth and through the umbilical-healing period. The WHO 5-dose schedule of tetanus toxoid (TT) or tetanus-diphtheria (Td) in women of childbearing age and during pregnancy eliminates neonatal tetanus in the community:[4][7]
5-DOSES
In India, the schedule is incorporated into the universal immunisation programme: 2 doses of tetanus toxoid in pregnancy (Tdap/Td), 4 weeks apart, for primigravidae; a single booster in subsequent pregnancies within 5 years.[4]
Neonate
Recognise early (day 5-14, poor feeding, rigidity, spasms); treat as severe tetanus with HTIG (50-200 IU/kg IM), benzodiazepines and meticulous ICU support. The decisive intervention is maternal vaccination.[4]
Elderly
Waning immunity and lapsed boosters; a lower threshold for prophylaxis and a higher threshold for ICU survival. Atypical early symptoms (stiffness, dysphagia, falls) must not be dismissed.[1]
Immunocompromised / HIV
Vaccinate with toxoid (it is a toxoid, not a live vaccine, and is safe); antibody response may be blunted, so check titres and boost as needed after severe immunosuppression.[7]
Wound prophylaxis — the CDC/ACIP table (reproduced verbatim)
Every wound in every patient should trigger a check of the immunisation history. The decision to give toxoid alone versus toxoid plus immunoglobulin depends on the wound type and the number of prior toxoid doses.[7]
| Prior tetanus toxoid doses | Clean, minor wound | Tetanus-prone (dirty) wound |
|---|---|---|
| Under 3, or unknown | Give Td/Tdap; start primary series | Give Td/Tdap AND HTIG 250 IU IM |
| 3 or more | Booster only if last dose over 10 years ago | Booster only if last dose over 5 years ago; HTIG not needed |
Tetanus-prone wounds include those contaminated with dirt/soil/faeces/saliva; puncture wounds; wounds containing necrotic or devitalised tissue; burns, frostbite, crush and avulsion injuries; wounds from missiles; and wounds delayed over 6 hours before treatment.[7]
HTIG prophylaxis dose: 250 IU IM (some references use 250-500 IU); give at a site separate from the toxoid.[7]
Evidence, Guidelines & Regional Differences
WHO position paper on tetanus vaccines (February 2017). Recommends 6 doses of tetanus-toxoid-containing vaccine across the life course: a 3-dose primary series in infancy (as DTaP/DTP, combined in pentavalent DTP-HepB-Hib in many countries including India), 3 booster doses (in the second year, at 4-7 years, and at 9-15 years), and a tetanus-diphtheria booster every 10 years through adult life. Women of childbearing age should receive 5 doses to eliminate maternal and neonatal tetanus. The 2017 paper reaffirmed the 10-year booster interval for adults.[7]
Landmark trials and what they changed.[7]
Magnesium sulphate for severe tetanus (Thwaites et al.)
Lancet
Double-blind, randomised, placebo-controlled trial; 256 Vietnamese adults with severe tetanus.
Key finding
IV magnesium sulphate (load 40 mg/kg, infusion 1-3 g/h titrated to patellar reflex) reduced the requirement for mechanical ventilation and for verapamil; did NOT reduce overall mortality.
Practice change
Magnesium is now a standard adjunct in severe (Ablett III/IV) tetanus for spasm and autonomic control, but does not replace ICU care and ventilation.
Human vs equine intramuscular antitoxin, with or without human intrathecal antitoxin (Van Hao et al.)
Lancet Global Health
Factorial, randomised controlled trial in Vietnamese adults with tetanus.
Key finding
Human IM antitoxin was superior to equine IM antitoxin (less disease progression, lower mortality); adding intrathecal human antitoxin did NOT improve outcome.
Practice change
Use human tetanus immunoglobulin (HTIG) by the intramuscular route; intrathecal administration is not recommended.
Where the evidence is weak. The optimum dose of HTIG (500 vs 3000-6000 IU) is uncertain; the choice of autonomic agent (labetalol vs esmolol vs morphine vs magnesium) is largely empirical; the role of intrathecal antitoxin is now not supported; and there are no high-quality trials of early elective intubation versus delayed intubation, although expert consensus favours early airway control in grade III/IV disease.[3][6]
Exam Pearls
- Tetanus = toxin-mediated, NOT invasive infection — the organism stays local; the disease is all toxin.
- Mechanism in one line: tetanospasmin → retrograde axonal transport to spinal cord → cleaves synaptobrevin (VAMP) → blocks glycine and GABA → unopposed excitation → rigidity, spasms, autonomic storms.
- Consciousness and sensation are PRESERVED — the single best discriminator from meningitis/encephalitis/status epilepticus.
- The tetanus triad: trismus → risus sardonicus → opisthotonos, with stimulus-triggered reflex spasms.
- Incubation 3-21 days; onset-to-spasm interval under 48 h or incubation under 7 days = severe disease and high mortality.
- Diagnosis is clinical — no useful test; normal CSF, calcium and CK do not exclude it; a positive wound culture does not prove it.
- Treatment — four pillars: HTIG (neutralise toxin) + metronidazole and debridement (remove source) + benzodiazepines/magnesium/ventilation/ICU (control spasms, support autonomic) + active vaccination (the disease does not immunise).
- Avoid high-dose penicillin G — GABA antagonist; worsens spasms. Use metronidazole.
- Magnesium sulphate (Thwaites 2006) reduces ventilation need in severe tetanus; does not reduce mortality. Monitor serum magnesium and the knee jerk.
- HTIG route: intramuscular (not intrathecal, per the 2022 factorial RCT).
- Strychnine is the closest mimic — same mechanism, same spasms, but flaccid between spasms and no wound.
- Botulism vs tetanus: botulinum toxin stays at the NMJ and blocks acetylcholine → descending flaccid paralysis with early cranial nerve palsies; tetanospasmin travels centrally and blocks glycine/GABA → rigidity.
- Neonatal tetanus = day 5-14, umbilical stump, unvaccinated mother; eliminated by maternal TT.
- Prevention: DTaP/Tdap primary + booster every 10 years; wound prophylaxis per CDC/ACIP table (toxoid ± HTIG); maternal vaccination.[6]
Exam application bank (NEET-PG / INICET)
One-line answer
Tetanus is an acute, toxin-mediated neurological disease caused by Clostridium tetani tetanospasmin released from spores germinating in anaerobic, necrotic wounds. The toxin travels retrogradely in motor nerves to the spinal cord and brainstem, cleaves synaptobrevin (VAMP), and blocks release of the inhibitory neurotransmitters glycine and GABA, producing unopposed sustained muscle contraction and reflex spasms with a preserved sensorium. The classic phenotype is trismus (lockjaw), risus sardonicus, opisthotonos and stimulus-triggered spasms, progressing to autonomic instability and respiratory failure. Diagnosis is clinical — there is no useful laboratory test. Management rests on three pillars: neutralise unbound toxin (human tetanus immunoglobulin, HTIG), eradicate the organism (wound debridement plus metronidazole), and control spasms and support vital functions in ICU (benzodiazep
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard.[3]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes.[2]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change.[2]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each.[2]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory.[2]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Tetanus.
References
- [1]Bhatia R, Prabhakar S, Grover VK. Tetanus. Neurology India, 2002.PMID 12577086
- [2]Fields B, Guerin CS, Justice SB. Don't Be a Stiff: A Review Article on the Management of Tetanus. Advances in Emergency Nursing Journal, 2021.PMID 33952870
- [3]Yen LM, Thwaites CL. Tetanus. Lancet, 2019.PMID 30935736
- [4]Thwaites CL, Beeching NJ, Newton CR. Maternal and neonatal tetanus. Lancet, 2015.PMID 25149223
- [5]Thwaites CL, Yen LM, Loan HT, et al. Magnesium sulphate for treatment of severe tetanus: a randomised controlled trial. Lancet, 2006.PMID 17055945
- [6]Van Hao N, Binh ND, Truong AH, et al. Human versus equine intramuscular antitoxin, with or without human intrathecal antitoxin, in tetanus: a factorial, randomised, controlled trial. Lancet Global Health, 2022.PMID 35561721
- [7]World Health Organization. Tetanus vaccines: WHO position paper - February 2017. Weekly Epidemiological Record, 2017.PMID 28185446