Nephrology · General Medicine
Haematuria (Evaluation)
Also known as Haematuria · Hematuria · Blood in urine · Microscopic haematuria · Macroscopic haematuria
Haematuria (red blood cells in the urine) is a sign, not a diagnosis. It is divided into visible (macroscopic/gross) and non-visible (microscopic, defined as more than 3 RBCs per high-power field on microscopy). The pivotal diagnostic distinction is glomerular vs urological source: glomerular bleeding shows dysmorphic red cells, red-cell casts and proteinuria and is managed by nephrology; urological bleeding shows isomorphic (intact) red cells and needs cystoscopy and CT urogram. Painless visible haematuria is cancer until proven otherwise and warrants an urgent suspected-cancer referral. Evaluation first excludes infection and transient causes, then uses urine microscopy to direct either a urological or nephrological work-up.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Overview & Definition
Haematuria is the presence of red blood cells (RBCs) in the urine. It is a sign, not a diagnosis — the clinician's task is not merely to detect it but to triage its source and seriousness. Two thresholds matter at the bedside.[1]
First, visible (macroscopic, gross) haematuria — urine that is red, pink, brown or cola-coloured to the naked eye. Second, non-visible (microscopic) haematuria — urine of normal colour that contains blood only on dipstick and is confirmed by more than 3 RBCs per high-power field on microscopy of a centrifuged midstream specimen.[6]
The single most important diagnostic judgement is whether bleeding is glomerular (driving a nephrology work-up and renal biopsy) or urological (driving cancer exclusion with CT urogram and cystoscopy). This is settled by urine microscopy: the morphology of the red cells (dysmorphic with casts vs isomorphic and intact) is the deciding clue. Because painless visible haematuria in an adult is so frequently a presentation of urological malignancy, it is treated as cancer until proven otherwise and triggers an urgent suspected-cancer referral.[1][2]
Why the dipstick alone is not enough
The urine dipstick detects haem peroxidase activity, which is present in intact RBCs, free haemoglobin and myoglobin. It is therefore positive in true haematuria, haemoglobinuria and myoglobinuria, and cannot distinguish between them. A positive dipstick therefore must be confirmed by microscopy before the label of haematuria is applied.[5]
False positives on dipstick include myoglobinuria (rhabdomyolysis — very high creatine kinase), haemoglobinuria (intravascular haemolysis — low haptoglobin, raised LDH), concentrated urine, oxidative contaminants (e.g. povidone-iodine, bleach), and recent beetroot or drugs such as phenazopyridine (which can also turn the urine orange).[6]
False negatives occur when the urine is dilute or when ascorbic acid (vitamin C) in the urine interferes with the peroxidase reaction; in this situation a patient can have true haematuria with a negative dipstick, underlining the importance of microscopy.
[1]Classification
Haematuria is classified along three axes that each change the clinical approach: visibility, source (glomerular vs urological) and symptom context.[1][6]
By visibility
- Visible (macroscopic / gross) — the patient sees blood. Always warrants investigation. The colour is informative: bright red suggests fresh lower-tract (bladder/urethral) bleeding; brown, tea or cola-coloured suggests blood that has dwelt in acidic urine (typically glomerular, where RBCs lyse) or bleeding from the upper urinary tract.
- Non-visible (microscopic) — found on dipstick, confirmed by microscopy (more than 3 RBC/HPF). Divided into symptomatic (with dysuria, urgency, frequency, flank pain) and asymptomatic. The threshold of clinical concern and the intensity of work-up depend on the symptom context and the patient's cancer risk.[6]
By source — glomerular vs urological (the pivotal split)
Glomerular (nephrology)
- Dysmorphic RBCs (blebs, vesicles), acanthocytes over 5%
- Red-cell casts (pathognomonic of glomerular bleeding)
- Proteinuria (UACR over 30 mg/g), often over 500 mg/g
- Brown / tea / cola urine
- Causes: IgA nephropathy, thin basement membrane disease, post-infectious GN, Alport syndrome, lupus nephritis
- Work-up: UACR, eGFR, C3/C4, ANA, ANCA, anti-GBM, hepatitis/HIV serology; renal biopsy
- Refer to nephrology
Urological (urology)
- Isomorphic (intact, uniform-biconcave) RBCs
- No casts; little or no proteinuria
- Bright-red or pink urine, plus or minus clots
- Causes: bladder/renal/urothelial cancer, stones, BPH, trauma, infection, prostatitis
- Work-up: CT urogram (upper tract) + cystoscopy (bladder); urine cytology if high risk
- Refer to urology — cancer exclusion
By symptom context (drives urgency)
- Painless visible haematuria — cancer until proven otherwise; urgent cystoscopy + CT urogram.[1]
- Painful visible haematuria — stone (colic, loin-to-groin pain) or infection (dysuria, frequency, fever); cancer still must be excluded once the acute event resolves.
- Symptomatic microscopic haematuria — investigate the cause (UTI, stone); re-check after treatment.
- Asymptomatic microscopic haematuria — risk-stratify by age, sex, smoking and RBC count (see Investigations).[6]
Pseudohematuria and pigmenturia — the red herrings
Non-haematuria causes of red/brown urine that must be excluded before labelling haematuria: beetroot (beeturia), rifampicin, phenazopyridine, sulfasalazine, myoglobin (rhabdomyolysis), haemoglobin (intravascular haemolysis), porphyrins (acute intermittent porphyria), food dyes, anthocyanins. Dipstick-positive urine with microscopy showing no RBCs = myoglobinuria, haemoglobinuria, or lysed cells — measure creatine kinase and plasma free haemoglobin/haptoglobin.
[1]Epidemiology & Risk Factors
Asymptomatic microscopic haematuria is found in roughly 2–20% of the adult population, the wide range reflecting age, sex, definition and the number of samples tested. Prevalence rises with age and is higher in men, smokers, and those with occupational dye/rubber exposure. Most cases are benign, but a small minority — particularly older smokers with visible haematuria — harbour malignancy.[3]
Cancer risk in haematuria — the headline numbers drive the entire work-up:
[1]Cancer yield of haematuria by type
Bladder cancer is the commonest urological malignancy and the commonest cancer diagnosis made on haematuria work-up. It is three to four times more common in men than women, has a peak age over 60, and is strongly linked to tobacco smoking (the single biggest modifiable risk factor, accounting for about half of cases).[2]
Risk factors for urological malignancy presenting as haematuria (must be elicited in every history):
[2]| Risk factor | Why it matters |
|---|---|
| Smoking (tobacco) | Carcinogenic amines excreted in urine; about half of bladder cancer |
| Age over 40–45 | Cancer yield rises sharply with age |
| Male sex | 3–4 times higher bladder cancer incidence |
| Occupational exposure | Aromatic amines — dye, rubber, paint, textile, leather industries; hairdressers |
| Cyclophosphamide | Acrolein metabolite; up to 10 times bladder cancer risk |
| Pelvic radiotherapy | Radiation cystitis and late urothelial malignancy |
| Schistosoma haematobium | Chronic bladder inflammation → squamous-cell carcinoma (endemic regions: sub-Saharan Africa, Egypt, Middle East) |
| Arsenic in drinking water | Transitional- and squamous-cell carcinoma |
| Chronic indwelling catheter / recurrent UTI | Chronic inflammation → squamous metaplasia/cancer |
Causes of glomerular haematuria in young adults (the nephrology arm): IgA nephropathy (commonest primary glomerulonephritis worldwide), thin basement membrane disease (benign familial haematuria), post-infectious (post-streptococcal) glomerulonephritis (children, 1–3 weeks after a streptococcal throat or skin infection), Alport syndrome (X-linked, sensorineural deafness + ocular signs + progressive renal failure), lupus nephritis, and ANCA-associated vasculitis.[5]
Pathophysiology
Why does blood appear in the urine — and why does the shape of the red cell betray its origin? The answer lies in the glomerular filtration barrier.[5]
The normal glomerular filtration barrier
The normal glomerular filtration barrier has three layers, each of which normally excludes red blood cells: (1) the fenestrated glomerular endothelium, (2) the glomerular basement membrane (GBM) with its negatively-charged type-IV collagen network, and (3) the podocyte foot processes with their slit diaphragms (nephrin, podocin). Together these normally hold back all blood cells and most proteins. When this barrier is damaged — by immune-complex deposition (IgA nephropathy, lupus), inflammation (post-infectious GN), genetic thinning/alteration of the collagen network (thin basement membrane disease, Alport syndrome), or podocyte effacement — red cells squeeze through the disrupted membrane.[5]
Mechanical deformation as RBCs traverse a damaged barrier produces dysmorphic cells. As an RBC is forced through rents in the GBM and then the slit diaphragm, the cell membrane is stressed and stretched; it emerges distorted, with blebs, vesicles, and the characteristic ring-shaped acanthocytes (annular cells with one or more bleb-like protrusions). RBCs that then lodge and aggregate in the tubular lumen — enmeshed by Tamm-Horsfall protein — become red-cell casts, which are pathognomonic of glomerular bleeding. Acanthocytes over 5% of urinary RBCs strongly suggest a glomerular source.[5]
By contrast, urological bleeding occurs below the glomerulus — from the renal pelvis, ureter, bladder, prostate or urethra — where blood leaks from capillaries and venules directly into the urinary space without traversing the filtration barrier. These red cells suffer no mechanical deformation and appear isomorphic (intact, biconcave, uniform in size). There is no opportunity for cast formation in the renal tubule.
[8]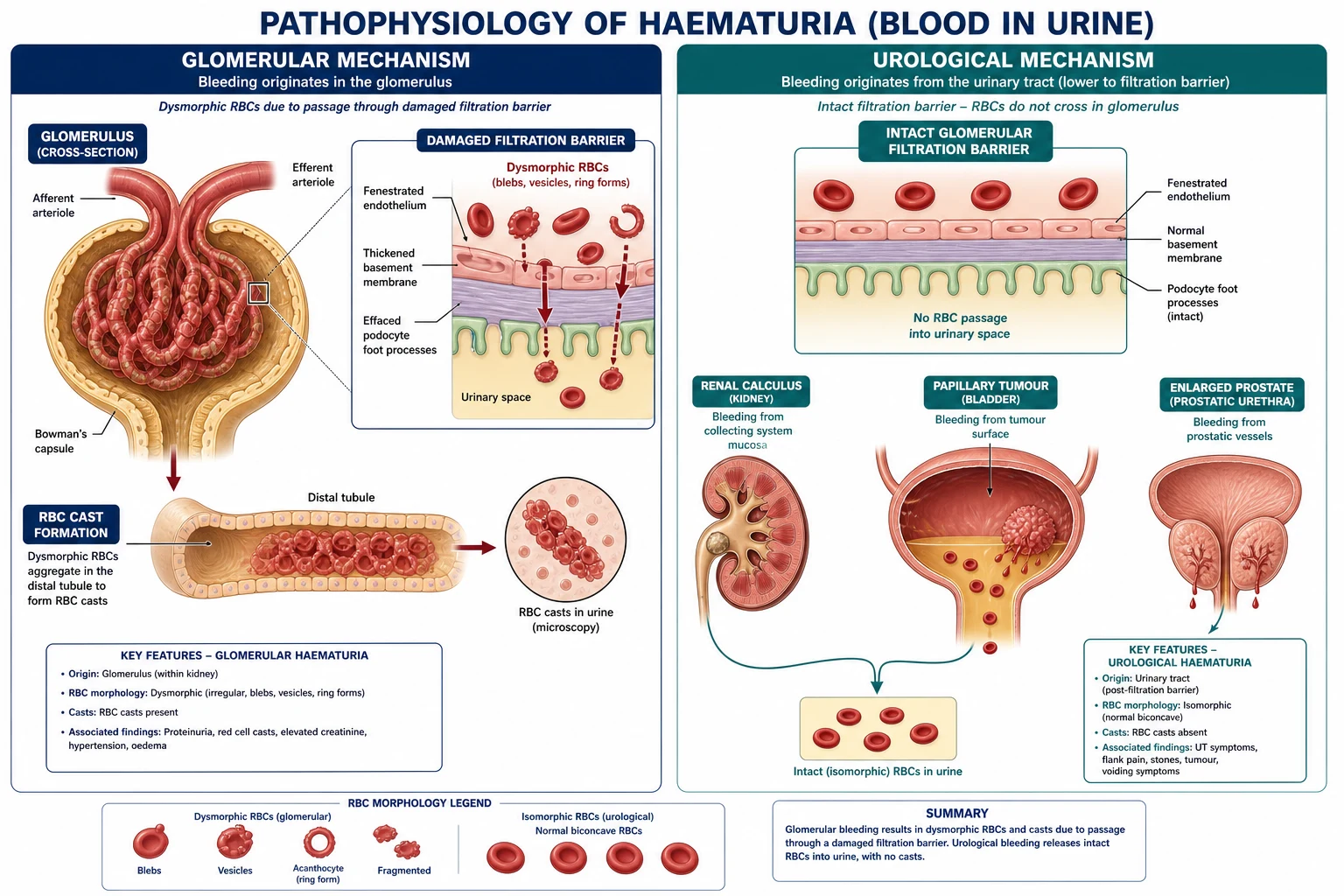
Mechanisms of the major urological causes
- Urinary stones — the crystalline calculus abrades the fragile transitional (urothelial) lining, with secondary inflammation and microvascular tearing; the bleeding is typically painful (colic) and may be visible or microscopic.
- Urinary tract infection — urothelial inflammation, hyperaemia and mucosal ulceration release RBCs; typically accompanied by dysuria, frequency, urgency (and positive culture).
- Benign prostatic hyperplasia — androgen-driven stromal and glandular hyperplasia with neovascularisation produces fragile, friable prostatic veins that bleed easily, classically as initial-haematuria or terminal haematuria and sometimes heavy post-TURP.
- Bladder / urothelial cancer — transitional-cell (urothelial) carcinoma (and squamous-cell where schistosomiasis) grows as a papillary, friable mass that bleeds on its surface, often painlessly; high-grade lesions and carcinoma in situ bleed more.
- Renal-cell carcinoma — invasion of the renal collecting system by tumour, or erosion of renal vasculature.
- Haemorrhagic cystitis — bacterial infection (E. coli), radiation (late effect, months to years after pelvic radiotherapy), cyclophosphamide (acrolein metabolite irritant), viral (BK virus, adenovirus in transplant patients).
- Trauma — blunt/penetrating renal injury, urethral catheterisation, contact sports.
Detailed disease mechanisms
IgA nephropathy is the commonest primary glomerulonephritis globally. Pathogenesis involves galactose-deficient IgA1 (Gd-IgA1) that is recognised by autoantibodies, forming immune complexes that deposit in the glomerular mesangium. Mesangial proliferation and complement activation damage the filtration barrier, allowing RBCs to escape. The synpharyngitic macroscopic haematuria reflects mucosal IgA production during upper respiratory infection with simultaneous mesangial IgA deposition.
[5]Thin basement membrane disease is caused by mutations in COL4A3 or COL4A4 (type IV collagen alpha chains), producing a thinned but structurally intact GBM. It is autosomal dominant, presents with isolated microscopic haematuria, and has a benign course. The key distinction from Alport syndrome is the absence of hearing loss, ocular defects and progressive renal failure.
[5]Post-streptococcal glomerulonephritis follows infection with nephritogenic strains of group A beta-haemolytic Streptococcus (throat or skin). Circulating immune complexes deposit subepithelially, producing the classic "lumpy-bumpy" basement membrane and low complement C3. The disease is self-limiting in children; adults have a more variable course.
[5]Alport syndrome arises from mutations in COL4A5 (X-linked), or less commonly COL4A3/COL4A4 (autosomal recessive). The abnormal type IV collagen cannot maintain the GBM architecture, leading to progressive splitting, proteinuria and renal failure. Associated sensorineural deafness and anterior lenticonus are pathognomonic.
[5]Lupus nephritis produces immune-complex deposition at multiple sites (subendothelial, subepithelial, mesangial), causing a pleomorphic urinary sediment with both dysmorphic RBCs and casts. Hypocomplementaemia (low C3 and C4) and positive anti-dsDNA are diagnostic clues.
[5]ANCA-associated vasculitis and anti-GBM disease cause pauci-immune or linear IgG deposition along the GBM, producing crescentic glomerulonephritis with severe haematuria, proteinuria and rapidly declining eGFR. Anti-GBM disease may coexist with pulmonary haemorrhage (Goodpasture syndrome).
[5]Urological mechanisms in detail
Bladder cancer most commonly arises from urothelial cells. Low-grade papillary tumours have a frond-like surface that bleeds on contact; high-grade tumours and carcinoma in situ bleed more diffusely. The bleeding is typically painless because the tumour is not invasive at the mucosal surface. Squamous-cell carcinoma develops in schistosomiasis-endemic regions due to chronic egg deposition and squamous metaplasia.
[7]Renal-cell carcinoma (clear cell, papillary, chromophobe) bleeds when tumour invades the collecting system or when necrotic tumour erodes into a vessel. The classic triad of flank pain, haematuria and palpable mass is now uncommon because most RCCs are detected incidentally on imaging.
[4]Upper-tract urothelial carcinoma (renal pelvis, ureter) presents with painless haematuria and may cause ureteric obstruction. CT urogram shows an intraluminal filling defect; ureteroscopy allows direct visualisation and biopsy.
[11]Nephrolithiasis causes haematuria through mechanical abrasion of the urothelium. The degree of bleeding does not correlate with stone size; even tiny stones can cause visible haematuria when they migrate. Microscopic haematuria is common in stone formers, but absence of RBCs does not exclude a stone (up to 20% of ureteric stones have no haematuria on dipstick).
[11]BPH causes bleeding from dilated, fragile veins in the prostatic urethra and bladder neck. The classic pattern is terminal haematuria because the bladder neck compresses the prostate at the end of voiding. Acute urinary retention with catheterisation can precipitate heavy bleeding.
[8]Prostatitis causes haematuria through inflamed prostatic ducts and urethra; it is often accompanied by dysuria, perineal pain and fever. Vigorous prostate massage or DRE can worsen bacteraemic spread and should be avoided in acute bacterial prostatitis.
[8]Radiation cystitis reflects late-onset microvascular injury and urothelial ischaemia months to years after pelvic radiotherapy. The bladder mucosa becomes friable, telangiectatic and prone to bleeding that may be refractory to conservative measures.
[4]Cyclophosphamide/ifosfamide-induced haemorrhagic cystitis is caused by the urothelial toxic metabolite acrolein. The risk is dose-dependent and is reduced by mesna (sodium 2-mercaptoethanesulfonate), which binds acrolein in the urine. Haematuria can occur during therapy or years later.
[7]Why colour matters
Bright-red fresh blood implies a lower-tract source with short transit time; brown, tea or cola-coloured urine implies older, haemolysed blood (often glomerular, where RBCs lyse in acidic urine) or upper-tract bleeding with longer dwell time. The colour therefore provides a clue, but it is not definitive — microscopy remains the pivotal investigation.
[5]Clinical Presentation
The history is the single most informative step — it localises the likely site and flags cancer risk. A focused history should establish visibility, colour, pain, timing in the stream, clots, associated symptoms, and risk factors. The combination of these elements often points toward the correct diagnosis well before any formal investigation is ever even ordered in most cases.[1]
Visibility and colour
Ask whether the blood is seen with the naked eye (visible/macroscopic) or found only on testing (microscopic). Note the colour: bright red (fresh, lower tract), pink (small-volume lower-tract), brown / tea / cola / smoky (old blood, glomerular or upper tract).
[5]Pain
Painless visible haematuria raises the suspicion of malignancy and is the cardinal red flag. Painful haematuria points to stone (ureteric colic — sudden, severe, loin-to-groin, nausea/vomiting), infection (dysuria, frequency, urgency, suprapubic pain, fever, and sometimes rigors in pyelonephritis), or clot colic (a clot passing down the ureter causing ureteric-spasm pain).
[10]Timing in the stream (the urological triad of site)
| Mnemonic | Timing in stream | Anatomical site |
|---|---|---|
| Initial haematuria | Blood only at the start of the stream | Anterior urethra (urethritis, urethral stricture, meatal cause) |
| Total haematuria | Blood throughout the stream | Bladder or upper tract (bladder cancer, renal/ureteric lesion) |
| Terminal haematuria | Blood only at the end of the stream | Bladder neck / prostate / trigone (BPH, bladder-base tumour, schistosomiasis) |
Clots and clot retention
Ask about clots — their presence implies heavier, lower-tract bleeding; vermiform (worm-like) clots suggest upper-tract (ureteric) moulding of clots; clot retention (inability to void, painful palpable bladder) is a urological emergency.
[11]Associated symptoms — glomerular pattern
Brown/cola urine + oedema + hypertension + oliguria suggests the nephritic syndrome (IgA nephropathy, post-infectious GN). Ask about a recent sore throat or skin infection (post-streptococcal GN, 1–3 weeks after; synpharyngitic in IgA nephropathy — bleeding concurrent with the pharyngitis). Systemic features of lupus (rash, arthralgia), vasculitis (sinusitis, haemoptysis), and Alport syndrome (family history of deafness/renal failure) should be sought.
[5]Urological/urothelial risk history
Document smoking (the single biggest risk factor), occupational exposure (dye, rubber, paint, textile, leather), cyclophosphamide, pelvic radiotherapy, recurrent UTI/indwelling catheter, and travel/residence in schistosomiasis-endemic regions (sub-Saharan Africa, Egypt, Middle East).[2]
Drug history
Anticoagulants (warfarin, DOACs, antiplatelets) — bleeding from any cause is amplified, but cancer must still be excluded (do not attribute haematuria to anticoagulation alone). Rifampicin, phenazopyridine, sulfasalazine colour urine red but are not true haematuria.
[1]Atypical presentations
- Elderly — may present with clot retention, anaemia, or weight loss; the threshold for cystoscopy and CT urogram is at its lowest.
- Anticoagulated — bleeding is more dramatic but the underlying cause still demands a full work-up.
- Pregnancy — common causes are UTI and stones; ultrasound is the first-line imaging to avoid radiation.
- Children — commonest causes are post-infectious GN and Henoch-Schönlein purpura (IgA vasculitis); refer to paediatric nephrology.
- Menstruating women — exclude contamination; repeat the urinalysis mid-cycle with a midstream catch.
- Exercise-induced (march) haematuria — benign, reproducible after strenuous exertion, resolves within 48–72 hours of rest.
- Immunocompromised / transplant — broaden the differential to BK polyomavirus nephropathy, adenovirus, opportunistic infection, and post-transplant lymphoproliferative disorder.
- Schistosomiasis-endemic regions — terminal-stream visible haematuria in children and young adults, with chronic bladder inflammation and late squamous-cell carcinoma.
Differential Diagnosis
The differential is best organised by the glomerular vs urological split, then by the symptom context.[1][3]
Glomerular causes (nephritic / nephrology)
| Cause | Distinguishing features |
|---|---|
| IgA nephropathy (Berger) | Commonest primary GN. Synpharyngitic macroscopic haematuria (concurrent with URTI, no latency); persistent microscopic haematuria between episodes; variable proteinuria; raised serum IgA in 30–50% |
| Thin basement membrane disease | Familial (autosomal dominant), isolated microscopic haematuria, normal renal function and BP, no proteinuria/hearing loss; diffuse GBM thinning on biopsy; benign prognosis |
| Post-infectious GN | Children, 1–3 weeks after streptococcal pharyngitis or impetigo; low C3 (normalises in 6–8 weeks); oedema, hypertension, oliguria, cola urine; ASO/anti-DNase B raised |
| Alport syndrome | X-linked; haematuria + sensorineural deafness + ocular signs (anterior lenticonus, macular flecks) + progressive renal failure; family history |
| Lupus nephritis | Young women; rash, arthralgia; low C3 and C4; positive ANA, anti-dsDNA |
| ANCA-associated vasculitis / anti-GBM | Pulmonary haemorrhage, sinusitis, rapidly progressive GN; positive ANCA / anti-GBM |
Urological causes (cancer exclusion / urology)
| Cause | Distinguishing features |
|---|---|
| Bladder cancer | Painless visible haematuria; smoker/occupational history; cystoscopy (gold standard); urothelial/transitional greater than squamous (schistosomiasis) |
| Renal-cell carcinoma | Painless haematuria + flank mass + weight loss (classic triad, now rare); CT shows enhancing renal mass |
| Upper-tract urothelial cancer | Painless visible haematuria; CT urogram shows filling defect; urine cytology often positive |
| Renal / ureteric stones | Colic (loin-to-groin), haematuria microscopic or visible; non-contrast CT (CT urogram in haematuria protocol) |
| Benign prostatic hyperplasia | Older men, LUTS, initial or terminal haematuria; enlarged prostate on DRE; diagnosis of exclusion after cancer excluded |
| UTI / prostatitis | Dysuria, frequency, urgency, fever; positive urine culture; haematuria resolves after treatment |
| Trauma (including catheterisation, contact sport) | Clear temporal relationship; resolves |
| Haemorrhagic cystitis | Radiation history, cyclophosphamide, or viral (BK/adenovirus in transplant) |
| Schistosoma haematobium (bilharzia) | Endemic regions; terminal-stream haematuria; squamous-cell bladder cancer |
Non-RBC causes of red/brown urine (must be excluded)
Beetroot (beeturia), rifampicin, phenazopyridine, sulfasalazine, myoglobin (rhabdomyolysis — raised CK), haemoglobin (haemolysis — raised LDH, low haptoglobin), porphyrins, food dyes. Dipstick-positive but microscopy-negative urine = myoglobinuria, haemoglobinuria, or lysed cells.
[1]Cannot-miss mimics: a UTI/stone in an older smoker does not exclude cancer — complete the work-up once the acute event settles, because synchronous cancers and post-obstructive tumours exist.
[10]Clinical & Bedside Assessment
Vital signs — blood pressure (hypertension points to a glomerular process), temperature (infection), heart rate and postural measurements (anaemia from heavy bleeding).
[5]Abdomen — palpate for a palpable bladder (clot retention), renal mass (renal-cell carcinoma, polycystic kidneys), and loin tenderness (pyelonephritis, stone).
[10]Digital rectal examination (men) — enlarged, smooth prostate (BPH), nodular hard prostate (cancer), tender boggy prostate (prostatitis).
[8]Genital examination — exclude a local penile/urethral/vaginal source of bleeding (which can contaminate the urine sample) and a testicular/epididymal cause.
[1]Bedside tests
- Urinalysis / dipstick — blood, leucocyte esterase, nitrite (infection), protein (glomerular), glucose, specific gravity. A positive dipstick for blood must be confirmed by microscopy.
- Urine microscopy — the pivotal test. Look for dysmorphic RBCs and acanthocytes (glomerular), RBC casts (pathognomonic glomerular), isomorphic RBCs (urological), WBCs/bacteria (infection), crystals (stones).
- Phase-contrast microscopy (where available) — quantifies dysmorphic RBCs (a dysmorphic count over 30% or acanthocytes over 5% favours a glomerular source).[5]
- Blood pressure measurement at every visit.
Named signs and manoeuvres
- Costovertebral angle (CVA) tenderness — suggests pyelonephritis or stone.
- Suprapubic dullness / palpable bladder — clot retention or chronic retention from BPH.
- Bimanual renal palpation — renal mass, polycystic kidneys, hydronephrosis.
- Prostate consistency on DRE — smooth and enlarged (BPH), nodular and hard (cancer), tender and boggy (prostatitis).
- Skin rash / arthritis — lupus, vasculitis, Henoch-Schönlein purpura.
- Hearing test — sensorineural deafness in Alport syndrome.
Investigations
The investigation strategy is two-branched and decided by the urine-microscopy pattern and the cancer-risk profile.[3][4]
Step 1 — confirm and exclude transient causes (every patient)
- Repeat urinalysis and microscopy on a clean-catch midstream specimen (menstruating women: repeat mid-cycle). A single positive dipstick that is microscopy-negative is not haematuria.
- Exclude infection — urine culture; treat UTI and re-check urinalysis 4–6 weeks after treatment (transient post-infective haematuria resolves, persistent haematuria does not).
- Exclude transient causes — heavy exercise (re-check after 48 h of rest), trauma (catheterisation, contact sport), menstruation.
- Document the visibility, the timing in the stream, the presence of clots, and the cancer-risk history.
Step 2 — first-line bloods (all)
U&E and eGFR, UACR (urine albumin-to-creatinine ratio) or PCR, FBC (anaemia from bleeding, eosinophilia), coagulation (PT/INR, APTT), CRP/ESR (infection/inflammation), and blood pressure.
[5]Step 3 — branch by urine microscopy pattern
Branch A — glomerular pattern (dysmorphic RBCs, casts, proteinuria) → nephrology work-up
- UACR/PCR, eGFR (baseline and to stratify).
- Complement C3 and C4 (low in post-infectious GN, lupus, membranoproliferative GN; C3 low with C4 normal in post-infectious; both low in lupus/MPGN).
- Serology — ANA, anti-dsDNA (lupus); ANCA, anti-MPO, anti-PR3 (ANCA-associated vasculitis); anti-GBM (Goodpasture).
- Hepatitis B, hepatitis C, HIV (cryoglobulinaemia, membranous, HIV-associated nephropathy).
- Serum IgA (raised in 30–50% of IgA nephropathy), ASO and anti-DNase B (post-streptococcal).
- Renal biopsy — indicated for nephritic syndrome, nephrotic-range proteinuria, rapidly progressive GN, declining eGFR, or when the serology is diagnostic-inconclusive; it provides the definitive diagnosis and prognosis.[5]
Branch B — urological pattern (isomorphic RBCs) or any visible haematuria → urology work-up
- CT urogram (CT of abdomen and pelvis with unenhanced, nephrographic and excretory/delayed phases) — the investigation of choice for the upper urinary tract. The unenhanced phase detects calcified stones; the nephrographic phase detects renal parenchymal masses; the excretory phase detects upper-tract urothelial tumours (filling defects in the enhanced collecting system). It is the single most comprehensive upper-tract study but carries radiation and a contrast-nephropathy risk — check eGFR first, hydrate, and use low-osmolar contrast with caution in CKD.[4]
- Cystoscopy — the gold standard for the lower tract; the only test that can directly visualise, biopsy and resect a bladder lesion. Mandatory for any visible haematuria, and for microscopic haematuria in intermediate/high-risk patients. Flexible cystoscopy is a well-tolerated outpatient procedure. A systematic review found sensitivity 87–100% and specificity 64–100% for detecting bladder cancer in adults presenting with haematuria.[7]
- Urine cytology — high sensitivity for high-grade tumours and carcinoma in situ, low sensitivity for low-grade tumours; useful as an adjunct in high-risk patients and for upper-tract surveillance. Negative cytology does not exclude cancer.
- Renal and bladder ultrasound — a reasonable first-line or alternative in pregnancy, young low-risk patients, and where CT is contraindicated (contrast allergy, CKD); less sensitive than CT for upper-tract urothelial lesions and small renal masses.[4]
- MRI/MR urogram — useful when radiation or iodinated contrast is contraindicated (pregnancy, severe contrast allergy, gadolinium not contraindicated); excellent for renal mass characterisation but less available and more costly.
Imaging findings to remember
| Finding | Interpretation |
|---|---|
| Filling defect in the renal pelvis/ureter on excretory CT | Upper-tract urothelial carcinoma, blood clot, stone, sloughed papilla |
| Enhancing renal parenchymal mass | Renal-cell carcinoma, angiomyolipoma, oncocytoma, metastasis |
| Bladder mass on ultrasound | Bladder cancer, blood clot, trabeculated bladder (BPH) |
| Non-obstructing calcification | Stone, vascular calcification |
| Hydronephrosis without stone | Obstructing tumour, clot, stricture, extrinsic compression |
AUA/SUFU risk-stratification of asymptomatic microscopic haematuria (reproduced)
The American Urological Association (AUA/SUFU) 2020 guideline risk-stratifies asymptomatic microhaematuria into low, intermediate and high risk, which then drives the intensity of work-up.[6]
Low risk — all of: age under 40 (women) / under 50 (men); never-smoker or under 10 pack-years; 10 or fewer RBC/HPF; no risk factors for urothelial cancer. Work-up: shared decision — repeat urinalysis or optional cystoscopy/renal ultrasound.
[4]Intermediate risk — any of: age 40–59 (women) / 50–59 (men); 11–25 RBC/HPF; light/moderate smoker (10–30 pack-years); low-to-moderation additional risk factors. Work-up: cystoscopy and renal ultrasound (CT urogram if prior US negative/symptoms progress).
[4]High risk — any of: age 60 or older; more than 25 RBC/HPF; heavy smoker (more than 30 pack-years); prior visible haematuria; occupational exposure; cyclophosphamide, pelvic radiotherapy, gross/persistent haematuria; CIS risk. Work-up: cystoscopy and CT urogram.[6]
Symptomatic or visible haematuria bypasses risk stratification — all such patients get cystoscopy and CT urogram, regardless of risk band.[1]
NICE NG12 suspected-cancer referral (UK) — reproduced thresholds
- Visible haematuria at any age — 2-week-wait suspected-cancer referral for urological assessment.[1]
- Aged 45 and over with unexplained non-visible haematuria — 2-week-wait referral.
- Aged 60 and over with unexplained non-visible haematuria and either dysuria or raised WBC — 2-week-wait referral.
Management — Resuscitation
Most haematuria is painless and not acutely life-threatening, but visible haematuria with clots and retention is a urological emergency.[1]
ABCDE for the haemodynamically compromised patient
- Airway / Breathing — oxygen if hypoxic; assess for associated sepsis (pyelonephritis).
- Circulation — IV access, fluid resuscitation for hypovolaemia, group-and-save and crossmatch; transfuse for significant anaemia/haemodynamic instability; correct coagulopathy (reverse warfarin with vitamin K/PCC per INR; hold DOAC; platelets if thrombocytopenic).
- Clot retention — pass a large (three-way) Foley catheter and begin continuous bladder irrigation with normal saline; if clots cannot be cleared by hand irrigation, cystoscopic clot evacuation under anaesthesia is required, with diathermy or laser to bleeding lesions.
- Exclude upper-tract obstruction (rising creatinine, hydronephrosis on ultrasound) — JJ stent or nephrostomy if obstructed by clots or tumour.
Refractory haemorrhagic cystitis
Haemorrhagic cystitis (radiation / cyclophosphamide) refractory to catheter/irrigation: intravesical alum, formalin instillation (under anaesthesia, caustic), hyperbaric oxygen (radiation), and selective internal iliac artery embolisation as escalation options.
[5]Management — Definitive & Stepwise
The definitive plan is cause-specific, but the diagnostic pathway is common to all (see Investigations). The cardinal organisational principle: exclude infection and transient causes → urine microscopy → branch to urology (cancer) or nephrology (glomerular) work-up.[1][6]
Painless visible haematuria (cancer pathway)
Urgent cystoscopy + CT urogram (within 2 weeks per NICE NG12 suspected-cancer pathway). Do not delay for infection treatment if cancer is the leading concern — investigate in parallel.[1]
Glomerular haematuria — cause-specific management
| Cause | Management |
|---|---|
| IgA nephropathy | ACE inhibitor or ARB for proteinuria/hypertension (e.g. ramipril 2.5–10 mg PO daily; losartan 50–100 mg PO daily) — slows progression; fish oil (omega-3) for proteinuria; systemic corticosteroids (prednisolone 0.5–1 mg/kg/day tapering) for progressive proteinuria/declining eGFR per KDIGO; tonsillectomy in selected recurrent synpharyngitic disease |
| Thin basement membrane disease | Reassurance — benign; long-term monitoring of BP, renal function and proteinuria; ACEi/ARB if hypertensive/proteinuric |
| Post-infectious GN | Supportive — control BP and fluid overload (fluid restriction, loop diuretic furosemide 20–40 mg PO daily); treat the infection (penicillin for streptococcus); dialysis for severe AKI/hyperkalaemia/overload; usually self-limiting in children |
| Alport syndrome | ACE inhibitor (e.g. ramipril) early to slow progression; renal replacement therapy for ESRD; genetic counselling |
| Lupus / vasculitis / anti-GBM | Immunosuppression — corticosteroids + cyclophosphamide or rituximab; plasmapheresis for anti-GBM/severe crescentic GN |
Urological haematuria — cause-specific management
| Cause | Management |
|---|---|
| Bladder cancer | Transurethral resection of bladder tumour (TURBT) for staging and resection; intravesical BCG for high-grade/CIS; radical cystectomy + urinary diversion for muscle-invasive disease |
| Renal-cell carcinoma | Partial or radical nephrectomy (laparoscopic/robotic); ablation for small lesions; targeted/immunotherapy (tyrosine-kinase inhibitors, checkpoint inhibitors) for advanced disease |
| Upper-tract urothelial cancer | Nephroureterectomy with bladder-cuff excision for high-grade/invasive; conservative endoscopic resection for low-grade |
| Stones | ESWL (shock-wave lithotripsy), ureteroscopy with laser lithotripsy, or PCNL (percutaneous nephrolithotomy) depending on stone size, site, composition |
| BPH | Alpha-blocker (tamsulosin 0.4 mg PO daily) ± 5-alpha-reductase inhibitor (finasteride 5 mg PO daily); TURP or laser prostatectomy for refractory bleeding/obstruction |
| UTI | Antibiotic by culture — nitrofurantoin 100 mg PO modified-release twice daily for 3 days (lower UTI), or IV co-amoxiclav / ceftriaxone for pyelonephritis; re-check urinalysis 4–6 weeks after |
| Schistosomiasis | Praziquantel 40 mg/kg PO in two divided doses; treat early to prevent squamous-cell carcinoma |
| Haemorrhagic cystitis | Stop offending drug (switch cyclophosphamide for ifosfamide with mesna protection); catheter/irrigation; intravesical alum/formalin; hyperbaric oxygen for radiation-induced |
Drug-dose detail for common causes
Lower UTI with haematuria. First-line: nitrofurantoin 100 mg modified-release PO twice daily for 3 days (if eGFR 45 mL/min or higher). Alternatives: trimethoprim 200 mg PO twice daily for 3 days if low local resistance and not used in the past 3 months; pivmecillinam 400 mg PO three times daily for 3 days; fosfomycin 3 g PO single dose. Re-check urinalysis 4–6 weeks after treatment because persistent haematuria after infection needs the full cancer work-up.[6]
Pyelonephritis. Outpatient if well: ciprofloxacin 500 mg PO twice daily for 7 days or co-amoxiclav 625 mg PO three times daily for 7 days. Severe or septic: IV ceftriaxone 1–2 g daily or co-amoxiclav 1.2 g IV three times daily; adjust to culture; imaging (ultrasound/CT) to exclude obstruction or abscess.
[10]Acute prostatitis. Ciprofloxacin 500 mg PO twice daily for 4 weeks or trimethoprim 200 mg PO twice daily for 4 weeks; for severe infection, IV ceftriaxone 1 g daily or co-amoxiclav. Add tamsulosin 0.4 mg PO daily for bladder-outlet symptoms; avoid vigorous DRE or prostate massage (risk of sepsis).
[8]Renal colic with haematuria. Analgesia: NSAIDs (diclofenac 50 mg PO three times daily or ketorolac 10 mg IV/IM) if no CKD/ulcer/bleeding risk; paracetamol 1 g PO; antiemetic (ondansetron 4–8 mg IV/PO). Medical expulsive therapy for distal ureteric stones under 10 mm: tamsulosin 0.4 mg PO daily for up to 4 weeks. Definitive: ESWL for stones under 10 mm in renal pelvis/proximal ureter; ureteroscopy for distal ureteric stones; PCNL for stones over 20 mm or staghorn.[6]
BPH-related haematuria (after cancer excluded). Tamsulosin 0.4 mg PO daily ± finasteride 5 mg PO daily (6-month trial for prostate volume over 30 mL); TURP or HoLEP for refractory bleeding or retention.
[8]Conservative management / repeat testing is appropriate for: transient causes (exercise, menstruation, single contaminated specimen), low-risk young patients with a single microscopic episode and negative work-up, and persistent low-risk microhaematuria with a shared decision to forego invasive tests — but the default is to complete the work-up.[6]
Detailed management algorithms by scenario
Scenario 1: painless visible haematuria in an adult. This is the cancer pathway. Immediate actions: confirm true haematuria (microscopy), secure IV access, check FBC/coagulation/eGFR, and urgently refer for cystoscopy and CT urogram within the suspected-cancer 2-week window. Do not delay for UTI treatment if the presentation is otherwise consistent with malignancy — investigate in parallel. If clots are present, place a three-way catheter and begin bladder irrigation. If clot retention occurs, perform cystoscopic clot evacuation.
[10]Scenario 2: painful visible haematuria with colic. Treat as renal colic and possible stone: analgesia, antiemetic, imaging with CT KUB or CT urogram. Once the acute stone episode is controlled, if the patient is older than 45 or has risk factors, complete the cancer work-up because a stone does not exclude synchronous malignancy.
[11]Scenario 3: painful visible haematuria with dysuria/fever. Treat as UTI/pyelonephritis: urine culture, empiric antibiotics, hydration. Re-check urinalysis 4–6 weeks after treatment. Persistent haematuria requires cystoscopy and CT urogram.
[10]Scenario 4: glomerular-pattern haematuria. Refer to nephrology. Baseline work-up includes UACR, eGFR, C3/C4, ANA, anti-dsDNA, ANCA, anti-GBM, hepatitis/HIV serology, serum IgA, ASO/anti-DNase B. Indications for renal biopsy: nephritic syndrome, nephrotic-range proteinuria, rapidly progressive GN, declining eGFR, diagnostic uncertainty. Management: ACE inhibitor/ARB for proteinuria and blood pressure control; immunosuppression for progressive IgA nephropathy, lupus nephritis, vasculitis or anti-GBM disease.
[9]Scenario 5: haematuria in pregnancy. First-line imaging is renal ultrasound; avoid CT. If stones are suspected and ultrasound is non-diagnostic, MR urogram (without gadolinium) is the safest cross-sectional option. Treat UTIs with pregnancy-safe antibiotics (cephalexin, nitrofurantoin — avoid near term, amoxicillin). Persistent or heavy haematuria requires combined obstetric/urology input.
[10]Scenario 6: anticoagulated patient with painless visible haematuria. Do NOT attribute to anticoagulation alone. Investigate for cancer in parallel with any necessary coagulation correction. Hold warfarin and give vitamin K/PCC if bleeding is heavy; hold DOACs; reverse heparin with protamine if applicable. Complete the cancer work-up once the patient is stabilised.
[5]Urology escalation ladder for refractory bleeding
Step 1 — bedside: large three-way catheter and continuous bladder irrigation with normal saline; manual irrigation to evacuate clots; correct coagulopathy and transfuse if indicated.
[5]Step 2 — cystoscopy: clot evacuation, diathermy or laser fulguration of bleeding points, resection of bladder tumour (TURBT), bladder wash with alum.
[7]Step 3 — intravesical therapy: 1% alum solution (astringent, temporary), formalin 1–4% (under anaesthesia, permanent mucosal fixation, risk of reflux), silver nitrate, prostaglandin E1 or tranexamic acid bladder instillation in selected cases.
[10]Step 4 — radiological/surgical: bilateral internal iliac artery embolisation (or selective superior vesical artery embolisation) for arterial bleeding refractory to endoscopic control; percutaneous nephrostomy or JJ stent for upper-tract obstruction; cystectomy with urinary diversion as last resort for life-threatening radiation cystitis.
[4]Step 5 — adjuvant: hyperbaric oxygen for radiation-induced haemorrhagic cystitis (improves tissue oxygenation and angiogenesis); sodium pentosan polysulfate for interstitial cystitis/bladder pain syndrome.
[4]Specific Subtypes & Scenarios
- Painless visible haematuria in the adult — the cancer pathway. Urgent cystoscopy + CT urogram. The yield is highest here (about 17% pooled); the commonest diagnosis is bladder cancer, followed by renal and upper-tract urothelial tumours.[1][7]
- Glomerular haematuria (IgA nephropathy, thin basement membrane disease, post-infectious GN, Alport) — distinguished by serology, family history, latency from infection, hearing/ocular exam; managed by nephrology with ACEi/ARB and selective immunosuppression.[5]
- Loin pain haematuria syndrome — a diagnosis of exclusion (after stones, tumour, obstruction, glomerular disease all excluded); characterised by recurrent flank pain with microscopic haematuria in young women; managed with analgesia, hydration, ACEi; favourable long-term renal prognosis.
- Exercise-induced (march) haematuria — benign, reproducible after strenuous exertion (running, contact sport), resolves within 48–72 h of rest; re-check off-exercise.
- Haematuria in schistosomiasis (Schistosoma haematobium) — terminal-stream visible haematuria in endemic regions (sub-Saharan Africa, Egypt, Middle East); chronic bladder inflammation drives squamous-cell bladder cancer; treat with praziquantel.[2]
- Anticoagulant-related haematuria — bleeding is amplified but the underlying cause (often cancer) must still be excluded with full imaging and cystoscopy; never attribute haematuria to warfarin/DOACs alone.
- Radiation / cyclophosphamide cystitis — late effect (months to years after pelvic radiotherapy or high-dose cyclophosphamide); refractory bleeding needs intravesical therapy or hyperbaric oxygen.
- Haematuria after catheterisation — common and usually self-limiting; persistent haematuria, especially in older patients, still needs urological work-up.
- Haematuria with trauma — imaging by CT with contrast (or ultrasound for initial screen in stable blunt trauma); grade renal injury; angioembolisation for active extravasation.
Persistent or isolated microscopic haematuria
If haematuria persists on two of three properly collected midstream urine specimens (AUA/SUFU recommendation), proceed to risk-stratification. Young, low-risk patients with a single episode may be observed with repeat testing, but persistent haematuria in any risk band warrants imaging. In low-risk patients under 40, a renal ultrasound plus cystoscopy or shared-decision surveillance is reasonable; in intermediate and high risk, cystoscopy and CT urogram are indicated. A normal work-up does not eliminate the need for follow-up — patients should have repeat urinalysis annually, and any development of visible haematuria or new symptoms triggers urgent re-evaluation.
[4]Follow-up after a negative cancer work-up
For low-risk asymptomatic microscopic haematuria with a negative cystoscopy and CT urogram, options include: annual urinalysis, with repeat cystoscopy/CT urogram if haematuria persists, becomes visible, or new risk factors appear. Smoking cessation is strongly advised because ongoing tobacco exposure is the single biggest modifiable risk factor for missed or interval urothelial cancer. Shared decision-making is central — the patient should understand the small residual risk of malignancy, the radiation and contrast burden of repeated CT, and the limitations of ultrasound.
[4]Complications & Pitfalls
Complications of inadequate investigation
- Missed early malignancy — the principal and most dangerous failure; delayed bladder/renal cancer diagnosis worsens survival.
- Progressive CKD from untreated glomerular disease (IgA nephropathy with heavy proteinuria, vasculitis).
- Obstructive uropathy / AKI from clot retention or papillary/tumour obstruction of the upper tract.
Complications of clot retention
Obstructive uropathy and AKI, bladder rupture (rare), secondary infection. Manage with three-way catheter + irrigation, cystoscopic clot evacuation and diathermy.[1]
Classic diagnostic errors
- Attributing visible haematuria to UTI/BPH/anticoagulation without CT urogram + cystoscopy — the cardinal pitfall.
- Treating a glomerular disease as urological — a patient with IgA nephropathy referred for cystoscopy instead of nephrology/biopsy.
- Missing schistosomiasis in an endemic-region patient.
- Not repeating a transient (exercise, UTI, menstruation) haematuria before labelling it pathological.
- Over-investigating a young, low-risk patient with a single transient microscopic episode.
- Forgetting cytology in high-risk patients with carcinoma in situ (which may be invisible on imaging and even on white-light cystoscopy).
- Accepting a therapeutic INR as the cause of painless visible haematuria without cancer work-up.
- Missing urinary TB in a patient with sterile pyuria and haematuria from an endemic region.
Procedure complications
Cystoscopy (UTI, bleeding, urethral trauma, rare bladder perforation); CT urogram (contrast nephropathy, allergy, radiation dose); renal biopsy (bleeding, arteriovenous fistula, infection, rarely nephrectomy).
[9]Medicolegal and documentation issues
Document the exact description of the urine (colour, clots, timing in stream), all risk factors (smoking, occupational exposure, family history, travel), medication list (anticoagulants, cyclophosphamide, phenazopyridine, rifampicin), and the microscopy result. Any decision to defer cystoscopy or CT urogram in a low-risk patient must be a shared decision recorded in the notes, with a clear safety-net and follow-up plan. Painless visible haematuria in an adult should never be managed with "watch and wait" without imaging. Failure to refer appropriately is a leading cause of delayed cancer diagnosis and litigation in urological practice.
[5]Quality improvement pearls
Use a structured proforma for haematuria referrals to ensure microscopy results, risk factors, medication and prior imaging are communicated. Multidisciplinary team discussion of complex cases (young patients with possible glomerular disease, pregnant patients, immunocompromised patients) improves outcomes. Audit the time from referral to cystoscopy and CT urogram — delays beyond the 2-week suspected-cancer window worsen cancer-stage at diagnosis.
[5]Prognosis & Disposition
Prognosis depends entirely on the underlying cause.[1][2]
- Urological malignancy caught early through haematuria work-up is often localised and treatable: localised bladder cancer has a 5-year survival over 80–90%, falling dramatically once muscle-invasive or metastatic. Early cystoscopy and CT urogram save lives.
- Glomerular causes span a spectrum: thin basement membrane disease is benign (normal life expectancy); IgA nephropathy is variable (20–40% progress to ESRD over 20–25 years, predicted by proteinuria, hypertension, eGFR at diagnosis and biopsy lesions — the MEST-C score); post-infectious GN in children usually resolves completely; Alport syndrome progresses to ESRD (timing by genotype).
- Transient causes (infection, exercise, menstruation) resolve fully.
Disposition
- Painful visible haematuria with clot retention — admit for catheter/irrigation, urgent urology.
- Painless visible haematuria — urgent suspected-cancer referral (within 2 weeks per NICE NG12) for cystoscopy + CT urogram.
- Glomerular-pattern haematuria with nephritic syndrome/declining eGFR — urgent nephrology referral and consider biopsy.
- Low-risk asymptomatic microhaematuria with negative work-up — repeat urinalysis annually; shared decision on further imaging.[6]
Prognosis by cause
- Urological malignancy caught early through haematuria work-up is often localised and treatable: localised bladder cancer has a 5-year survival over 80–90%, falling dramatically once muscle-invasive or metastatic. Early cystoscopy and CT urogram save lives. Upper-tract urothelial carcinoma and renal-cell carcinoma also have markedly better survival when detected at an early stage.
- Glomerular causes span a spectrum: thin basement membrane disease is benign (normal life expectancy); IgA nephropathy is variable (20–40% progress to ESRD over 20–25 years, predicted by proteinuria, hypertension, eGFR at diagnosis and biopsy lesions — the MEST-C score); post-infectious GN in children usually resolves completely; Alport syndrome progresses to ESRD (timing by genotype); lupus nephritis prognosis depends on class and response to immunosuppression; ANCA-associated vasculitis and anti-GBM disease can cause rapid progression without treatment.
- Transient causes (infection, exercise, menstruation, catheter trauma) resolve fully once the trigger is removed.
- Loin pain haematuria syndrome has an excellent renal prognosis despite recurrent pain, provided malignancy, stone and glomerular disease are excluded.
- Sickle cell trait/disease renal papillary necrosis can recur but is usually manageable with hydration; the underlying sickle disease determines long-term renal outcomes.
Disposition
- Painful visible haematuria with clot retention — admit for catheter/irrigation, urgent urology.
- Painless visible haematuria — urgent suspected-cancer referral (within 2 weeks per NICE NG12) for cystoscopy + CT urogram.
- Glomerular-pattern haematuria with nephritic syndrome/declining eGFR — urgent nephrology referral and consider biopsy.
- Low-risk asymptomatic microhaematuria with negative work-up — repeat urinalysis annually; shared decision on further imaging.[6]
- Anticoagulated patient with visible haematuria — admit if haemodynamically unstable or unable to void; otherwise urgent outpatient urology work-up with coagulation correction in parallel.
- Pregnant patient with haematuria — manage with obstetrics and urology/nephrology; disposition depends on infection control, stone obstruction, and fetal well-being.
Special Populations
- Pregnancy — common causes are UTI and stones; ultrasound is the first-line imaging (avoid radiation); MR urogram if cross-sectional imaging is essential. Use pregnancy-safe antibiotics (nitrofurantoin at term caution, beta-lactams). Persistent haematuria in pregnancy needs urology/nephrology input. Physiological hydronephrosis of pregnancy can mimic obstruction; the presence of fever, persistent pain or infection indicates intervention. Vaginal contamination must be excluded by clean-catch midstream technique or catheter specimen.
- Children — commonest causes are post-infectious GN, IgA nephropathy, Henoch-Schönlein purpura (IgA vasculitis), hypercalciuria and structural anomalies; refer to paediatric nephrology/urology. Cystoscopy/CT are rarely indicated in isolated microscopic haematuria unless there is visible haematuria, significant trauma or a suspicious mass. Vigilance for abuse/trauma and congenital anomalies (e.g. duplicated collecting system, ureterocele).
- Anticoagulated — bleeding is amplified but cancer must still be excluded; investigate in parallel with reversing the anticoagulant where indicated. A therapeutic INR is never an acceptable sole explanation. Coordinate with haematology/anticoagulation clinic for peri-procedural bridging (e.g. DOAC hold 24–48 h, warfarin hold 5 days with bridging low-molecular-weight heparin if high thrombotic risk).
- Elderly / very high cancer risk — lowest threshold for cystoscopy and CT urogram; the cancer yield is at its highest. Age over 60, smoking history, occupational exposure, and heavy RBCs on microscopy all place the patient in the AUA/SUFU high-risk category. Even transient haematuria in this group should be evaluated.
- Immunocompromised / transplant — broaden the differential to BK polyomavirus nephropathy, adenovirus, cytomegalovirus, opportunistic infection (fungal, mycobacterial), and post-transplant lymphoproliferative disorder. Immunosuppression may mask fever and inflammation; maintain a low threshold for biopsy and targeted PCR testing (BK viral load, adenovirus PCR).
- Post-renal transplant — haematuria may indicate ureteric stricture, BK nephropathy, T-cell-mediated rejection, transplant renal-cell carcinoma or viral cystitis; low threshold for transplant-nephrology review and ultrasound. Ureteric obstruction from clot or stricture requires urgent percutaneous nephrostomy.
- Sickle cell disease / trait — renal papillary necrosis causes haematuria due to ischaemic injury of the renal medulla; manage with hydration, analgesia and avoid NSAIDs if possible. Papillary necrosis can also be seen in diabetes, analgesic nephropathy and tuberculosis.
- Long-distance runners / athletes — exercise-induced haematuria is benign, usually microscopic, resolves within 48–72 hours of rest and is thought to reflect bladder-wall trauma from repetitive impact. Re-check off-exercise; if persistent, complete the standard work-up.
- Patients with indwelling catheter — catheter-related haematuria is common from mechanical trauma and urethral irritation; exclude bladder cancer and clots; ensure adequate catheter size and balloon volume; consider bladder irrigation for persistent bleeding.
Evidence, Guidelines & Regional Differences
The major guidelines converge on the cardinal principle — visible haematuria mandates cystoscopy and CT urogram — but differ in the threshold work-up for asymptomatic microscopic haematuria.[3][4]
AUA/SUFU 2020 Microhematuria Guideline (US) — risk-stratifies (low/intermediate/high) and recommends a risk-adapted intensity of work-up; low-risk patients may forego cystoscopy/CT urogram in a shared decision, while high-risk patients get both. This risk-adapted approach recognises the radiation and contrast cost of universal CT urogram. The guideline also recommends using two of three properly collected urine specimens to confirm microscopic haematuria before further work-up, to reduce transient false positives.[6]
NICE NG12 (UK) — suspected-cancer referral: visible haematuria at any age and age 45 and over with unexplained non-visible haematuria trigger a 2-week-wait urology referral. The UK favours a low threshold for cancer-exclusion imaging. The threshold of 45 years is lower than the AUA/SUFU age-based intermediate-risk band, reflecting the UK strategy of earlier cancer exclusion.
[4]EAU (Europe) — Guidelines on Bladder Cancer: recommend cystoscopy + CT urogram for visible haematuria; supports ultrasound as a reasonable upper-tract screening tool in lower-risk patients. The EAU guidelines also emphasise that urine cytology has high specificity and is most useful in high-risk patients and for surveillance of upper-tract urothelial carcinoma.[4]
India / ICMR / Indian urology practice: empirical practice mirrors the EAU — ultrasound + cystoscopy for visible haematuria, with CT urogram where ultrasound is non-diagnostic or in high-risk patients, reflecting resource and contrast considerations; schistosomiasis and tuberculosis of the urinary tract are important differentials in endemic regions. TB can cause sterile pyuria, haematuria, and "coral ring" calcifications in the renal tract; diagnosis requires urine AFB smear/culture, PCR and imaging.
[4] [1] [4]Controversies
- Screening for microscopic haematuria in asymptomatic adults is not recommended population-wide — the yield is low and the cost/radiation of universal work-up is high. Opportunistic detection during routine medical evaluation is acceptable, but mass screening is not supported.
- Radiation/contrast cost of universal CT urogram in low-risk young patients — balanced against the small but real risk of missed cancer; the AUA risk-stratified approach and ultrasound-first strategies address this.[4]
- Microhaematuria in women — historically under-investigated (often dismissed as contamination), yet women with visible haematuria often present later with more advanced cancer. The AUA/SUFU guideline explicitly includes women and does not dismiss menstrual contamination without repeat testing.
- Routine urine cytology — high specificity but variable sensitivity; its role is mainly in high-risk patients and upper-tract surveillance, not as a universal screening test. Some centres use urinary biomarkers (UroVysion FISH, NMP22, BTA) but these are not first-line for routine evaluation.
- The role of MR urogram — increasingly used as an alternative to CT urogram in pregnancy and contrast allergy, but access and cost limit routine use. Gadolinium should be avoided in pregnancy unless essential.
- Anticoagulation and haematuria — there is controversy about whether anticoagulants unmask underlying cancer or directly cause bleeding. The current consensus is that anticoagulants do not cause de novo haematuria; they reveal underlying pathology. Therefore, cancer work-up must proceed.
Exam Pearls
- Cardinal rule: painless visible haematuria in an adult is cancer until proven otherwise → urgent cystoscopy + CT urogram.[1]
- Red-cell casts = glomerular disease (pathognomonic); acanthocytes over 5% strongly suggest glomerular bleeding.
- Dysmorphic RBCs + proteinuria → nephrology/biopsy; isomorphic RBCs → urology (CT urogram + cystoscopy).
- Microscopic haematuria = more than 3 RBCs per high-power field on microscopy (NOT dipstick alone — dipstick detects haem peroxidase and is positive in myoglobinuria/haemoglobinuria).[6]
- Synpharyngitic haematuria = IgA nephropathy (concurrent with URTI, no latency); latency 1–3 weeks after pharyngitis = post-streptococcal GN.
- Schistosoma haematobium → squamous-cell bladder cancer; the commonest cause of bladder cancer in endemic regions.[2]
- Initial-stream blood = anterior urethra; total = bladder/upper tract; terminal = bladder neck/prostate.
- Exclude infection, menstruation, exercise, trauma BEFORE labelling true haematuria; repeat the urinalysis.
- Do NOT attribute haematuria to anticoagulants without a full work-up — investigate cancer in parallel.
- CT urogram for upper tract; cystoscopy for bladder (gold standard for the lower tract).
- AUA/SUFU risk stratification: low risk = shared decision; intermediate = cystoscopy + renal ultrasound; high risk = cystoscopy + CT urogram.
- NICE NG12: visible haematuria at any age = 2-week-wait; age 45+ with unexplained non-visible haematuria = 2-week-wait.
- The classic triad of renal-cell carcinoma (flank pain, haematuria, palpable mass) is now rare; most RCCs are detected incidentally on imaging.
- Post-streptococcal GN: low C3 with normal C4, ASO/anti-DNase B raised, C3 normalises in 6–8 weeks; if C3 remains low beyond 8 weeks, consider lupus nephritis or membranoproliferative GN.
- Loin pain haematuria syndrome is a diagnosis of exclusion; recurrent flank pain + microscopic haematuria in young women, normal work-up, good prognosis.
- Thin basement membrane disease is benign; Alport syndrome is progressive — differentiate by hearing, ocular findings and family history.
- Painless visible haematuria in an anticoagulated patient is still cancer until proven otherwise.
- Cystoscopy sensitivity is high (87–100%) but specificity varies; a normal cystoscopy does not exclude upper-tract cancer — CT urogram is still needed.[7]
- Urine cytology is most sensitive for high-grade tumours and carcinoma in situ; negative cytology does not rule out low-grade bladder cancer.
- Menstrual contamination should be excluded by repeating the urinalysis mid-cycle with a clean midstream specimen.
- Exercise-induced haematuria resolves within 48–72 hours of rest; persistent haematuria requires full work-up.
- Radiation cystitis can present years after pelvic radiotherapy; hyperbaric oxygen is a disease-modifying option for refractory cases.
- Cyclophosphamide causes acrolein-mediated haemorrhagic cystitis; mesna prophylaxis reduces risk.
- Terminal-stream haematuria in an Egyptian or sub-Saharan African patient should raise Schistosoma haematobium and squamous-cell bladder cancer.
Causes of haematuria — RBC URINE
RBC-URINE
IgA, thin BM, post-infectious GN, Alport, RCC
Cancer (urothelial, squamous), haemorrhagic cystitis
Stones anywhere in the urinary tract
Urethritis, urethral stricture, benign prostatic hyperplasia
UTI, tuberculosis, schistosomiasis
Trauma, catheterisation, exercise (march)
Urothelial (renal pelvis, ureter)
Cyclophosphamide, anticoagulants, radiation
References
- [1]Dulku G, Shivananda A, Chakera A. Painless Visible Haematuria in Adults: An Algorithmic Approach Guiding Management. Cureus, 2019.PMID 31886075
- [2]Griffiths TR, Action on Bladder Cancer. Current perspectives in bladder cancer management. International Journal of Clinical Practice, 2013.PMID 23137019
- [3]Linder BJ, Bass EJ, Mostafid H, Boorjian SA. Guideline of guidelines: asymptomatic microscopic haematuria. BJU International, 2018.PMID 28921833
- [4]Taylor JI, Tipples D, Cuthbert G, et al. Diagnostic Imaging in the Evaluation of Asymptomatic Microhematuria: Systematic Review. The Journal of Urology, 2023.PMID 36883858
- [5]Saha MK, Agarwal N, Al-Busaidi S, Chopra S, Shirazi P, Carrier M, Karpman E, Rege K, Sheth S, Srivastava A. Glomerular Hematuria and the Utility of Urine Microscopy: A Review. American Journal of Kidney Diseases, 2022.PMID 35777984
- [6]Barocas DA, Boorjian SA, Alvarez RD, et al. Microhematuria: AUA/SUFU Guideline. The Journal of Urology, 2020.PMID 32698717
- [7]Devlies W, Todesco LV, Necchi A, et al. The Diagnostic Accuracy of Cystoscopy for Detecting Bladder Cancer in Adults Presenting with Haematuria: A Systematic Review from the European Association of Urology Guidelines Office. European Urology Focus, 2024.PMID 37633791
- [8]Sandhu JS, Bixler BR, Dahm P, et al. Management of Lower Urinary Tract Symptoms Attributed to Benign Prostatic Hyperplasia: AUA Guideline Amendment 2023. The Journal of Urology, 2024.PMID 37706750
- [9]Rovin BH, Adler SG, Barratt J, et al. KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney International, 2021.PMID 34556256
- [10]Gupta K, Hooton TM, Naber KG, et al. International Clinical Practice Guidelines for the Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Women: A 2010 Update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clinical Infectious Diseases, 2011.PMID 21292654
- [11]Skolarikos A, Geraghty R, Somani B, et al. European Association of Urology Guidelines on the Diagnosis and Treatment of Urolithiasis. European Urology, 2025.PMID 40268592