Neurology · General Medicine
CNS Infections — Meningitis, Encephalitis, Brain Abscess, TB, Cryptococcal, Neurocysticercosis
Also known as Central nervous system infections · Acute bacterial meningitis · Viral encephalitis · Brain abscess · Tuberculous meningitis · Cryptococcal meningitis · Neurocysticercosis
CNS infections span the meninges (meningitis), brain parenchyma (encephalitis, abscess), or both (meningoencephalitis). Acute bacterial meningitis is a time-critical emergency: fever, headache, neck stiffness and altered mental status (all four in about 44 percent of cases) demand empiric IV antibiotics within one hour — ceftriaxone 2 g IV BD plus vancomycin, adding ampicillin for Listeria in the over-50, pregnant, or immunocompromised — with dexamethasone 10 mg IV q6h for four days given before or with the first antibiotic dose. CSF analysis distinguishes bacterial (neutrophils, low glucose, high protein) from viral (lymphocytes, normal glucose), TB (low glucose, high lymphocytes, ADA raised), and fungal (cryptococcal antigen positive) patterns. HSV encephalitis needs IV aciclovir 10 mg/kg TDS for 14 to 21 days. Brain abscess shows a ring-enhancing lesion with restricted diffusion on MRI and is treated with ceftriaxone plus metronidazole and surgical aspiration. TB meningitis (basal exudates, cranial nerve palsies), cryptococcal meningitis (HIV, India ink, CRAG), and neurocysticercosis (Taenia solium, seizures, albendazole) complete the spectrum.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Exam tags
Red flags
Overview & Definition
Central nervous system infections are a heterogeneous family united by one clinical discipline: suspect them early, treat them fast, and never let imaging or a lumbar puncture delay life-saving antibiotics. The defining anatomical question is where the infection sits — in the subarachnoid space (meningitis), in the brain parenchyma (encephalitis or abscess), in both (meningoencephalitis), or in an extra-axial compartment (subdural empyema, epidural abscess). The defining therapeutic question is what the organism is — because the antibiotic ladder, the duration, and the adjuncts differ sharply between a pneumococcus, a herpesvirus, a mycobacterium, a cryptococcus, and a tapeworm larva.[1][12]
Meningitis is inflammation of the meninges with involvement of the subarachnoid space and CSF; the brain parenchyma is comparatively spared, so the dominant features are fever, headache, and meningismus. Encephalitis is parenchymal brain inflammation, dominated by altered mental status, seizures, and focal neurological signs; when meningeal and parenchymal features coexist, the term meningoencephalitis applies. A brain abscess is a localised collection of pus within the brain parenchyma, walled off by a collagen capsule over about two weeks; it behaves as both an infection and a mass lesion, which is why lumbar puncture is dangerous. Aseptic meningitis describes CSF pleocytosis with negative routine bacterial cultures — usually viral (enterovirus, HSV-2), but also TB, fungal, drug-induced (NSAIDs, co-trimoxazole, IVIG), or autoimmune.[1]
The unifying clinical imperative is the one-hour rule: in suspected community-acquired bacterial meningitis, empiric intravenous antibiotics and dexamethasone must be in the patient within one hour of presentation, ideally after blood cultures but before lumbar puncture or CT if either will cause delay. Outcome is time-dependent: mortality and neurological sequelae rise with every hour antibiotics are deferred.[2][3]

Classification
The most useful classification combines syndrome (where the infection is) with organism (what causes it) and tempo (how fast it evolved). The combination drives the empiric therapy decision at the bedside. [1]
Acute bacterial meningitis
Viral encephalitis
Brain abscess
Tuberculous meningitis
Cryptococcal meningitis
Neurocysticercosis
The classification matters because the empiric antibiotic, the decision to image before LP, and the role of steroids all pivot on it. A patient with the acute bacterial meningitis syndrome gets ceftriaxone and dexamethasone immediately; a patient with a focal deficit or papilloedema gets imaging first (suspecting abscess or mass); an immunocompromised host with subacute headache gets TB, cryptococcal, and toxoplasmosis pathways added from the outset.[1][2]
Epidemiology & Risk Factors
The single most exam-tested epidemiological fact is the organism-by-age ladder, because it determines empiric antibiotic choice. Conjugate vaccination has reshaped this ladder profoundly: Haemophilus influenzae type b (Hib) and pneumococcal conjugate vaccines (PCV13) have fallen in children wherever they are used, leaving Streptococcus pneumoniae and Neisseria meningitidis as the dominant community-acquired pathogens in older children and adults, with Listeria monocytogenes added in the over-50, pregnant, alcoholic, and immunocompromised host.[1][2]
Risk factors fall into three groups. First, defective clearance or architecture: asplenia, complement or terminal pathway deficiency (properdin, C5 to C9), eculizumab therapy, and sickle cell disease all predispose to encapsulated organisms, particularly pneumococcus and meningococcus — and mandate vaccination. Second, anatomical breaches: CSF leak (skull base fracture), cochlear implant, CSF shunt, recent neurosurgery, penetrating head injury, and chronic otitis, sinusitis, or dental infection. Third, immune compromise: HIV, alcohol misuse, malignancy, immunosuppressive therapy, diabetes, pregnancy, and extremes of age, each broadening the differential to include Listeria, TB, Cryptococcus, and Toxoplasma.[1][18]
Regional epidemiology is examined deliberately. The sub-Saharan meningitis belt experiences explosive meningococcal A and W epidemics in the dry season; mass MenAfriVac conjugate vaccination has dramatically reduced MenA. The Indian subcontinent carries a heavy burden of tuberculous meningitis and Japanese encephalitis (monsoon-season, rice-paddy transmission via Culex mosquitoes), both of which are uncommon in temperate regions. Cryptococcal meningitis tracks HIV prevalence, with the highest burden in sub-Saharan Africa.[12][14][18]
Pathophysiology
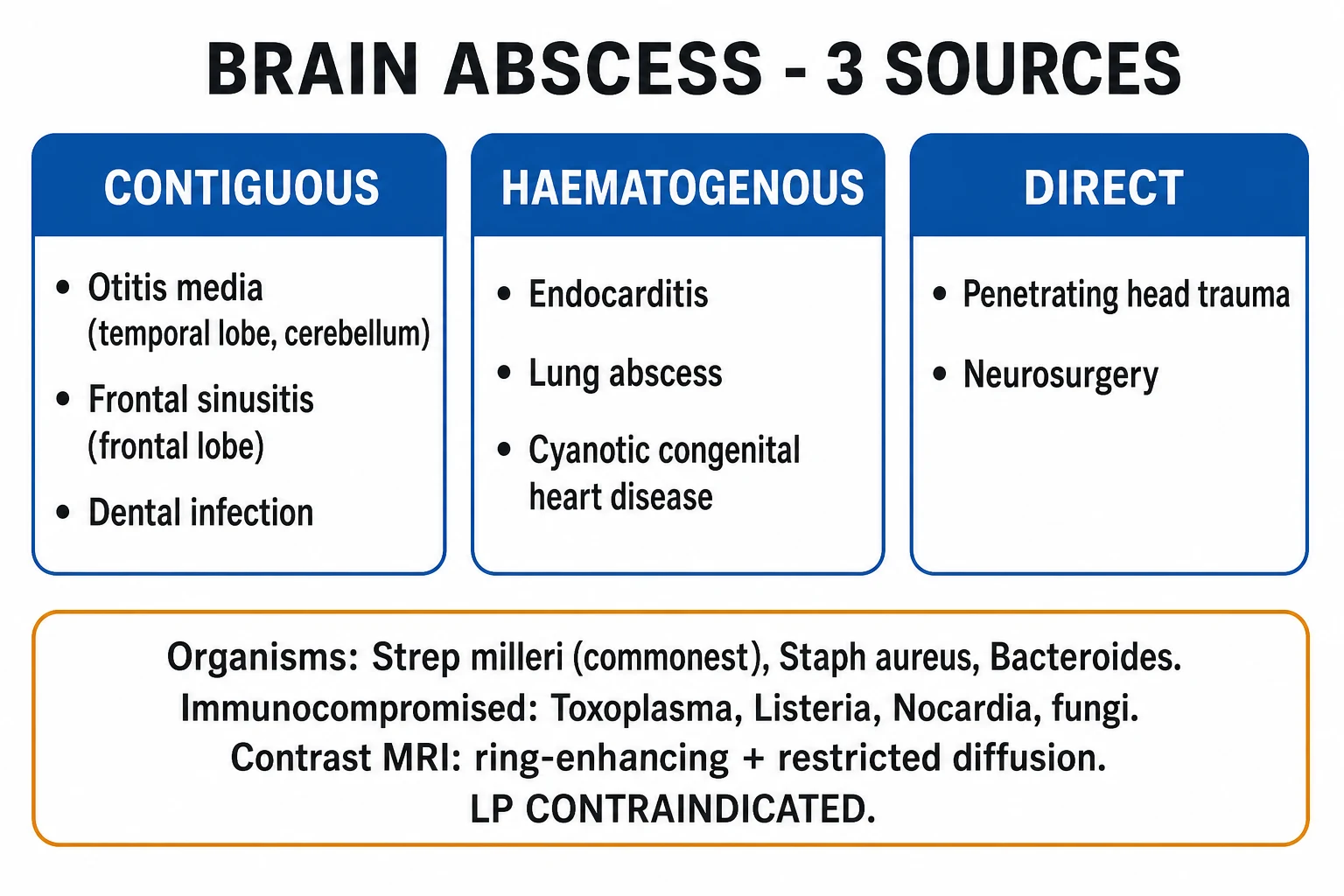
The common route for community-acquired bacterial meningitis is haematogenous: the organism colonises the nasopharynx (pneumococcus, meningococcus), gains bacteraemia, and crosses the blood-brain barrier at the choroid plexus or cerebral endothelium by transcellular transport or within loaded phagocytes (a Trojan horse mechanism for Listeria). Direct contiguous spread (otitis, mastoiditis, sinusitis, dental infection) explains many brain abscesses and a minority of meningitis cases; traumatic (skull base fracture with CSF leak) and iatrogenic (neurosurgery, shunt, rarely lumbar puncture) routes complete the picture.[1][12]
Why the central nervous system is vulnerable. CSF is an immunological sanctuary: it contains little complement, scant immunoglobulin, few phagocytes, and opsonisation is slow. Once organisms reach the subarachnoid space they multiply relatively unchecked. Their cell-wall components — pneumococcal cell wall, meningococcal lipopolysaccharide endotoxin — activate complement and the Toll-like receptors (TLR2, TLR4) on meningeal macrophages. The resulting cytokine storm (IL-1β, TNF-α, IL-6) drives a massive neutrophil influx into the CSF. This inflammation has three destructive consequences: it disrupts the blood-brain barrier producing vasogenic oedema, it impairs CSF outflow at the arachnoid villi producing communicating hydrocephalus, and it inflames the walls of subarachnoid arteries and veins producing vasculitis with ischaemic stroke. All three raise intracranial pressure, and the loss of cerebral autoregulation compounds the injury.[1][3]
This cascade explains both the disease and its treatment. Antibiotics kill bacteria but release more cell-wall components, transiently intensifying inflammation — which is exactly why dexamethasone, given just before or with the first antibiotic dose, reduces cochlear damage (sensorineural hearing loss) and, in pneumococcal meningitis, mortality.[3][4]
HSV encephalitis follows a different mechanism. Herpes simplex virus type 1 reaches the temporal lobe either by reactivation along the trigeminal or olfactory pathway or by primary infection, producing a characteristic haemorrhagic, necrotising inflammation of the medial temporal and frontal lobes — often asymmetric. This anatomy explains the clinical signature: behavioural change, memory disturbance, aphasia, complex partial seizures, and olfactory or gustatory hallucinations.[9][10]
Brain abscess evolves in two stages. The early cerebritis phase (days 1 to 14) is a poorly demarcated area of oedema, neutrophil influx, necrosis, and surrounding hyperaemia, with no capsule. Over the next two weeks a capsule forms — inner granulation tissue, a collagen wall laid down by fibroblasts, and an outer gliotic rind. The mature abscess behaves as a mass lesion (raised ICP, midline shift, herniation risk) and may rupture into the ventricular system, an event with catastrophic mortality.[6][7]
Tuberculous meningitis begins when a subpial or subependymal granuloma (a Rich focus) seeded during an earlier bacteraemia ruptures into the subarachnoid space. The resulting thick, gelatinous basal exudate wraps around the base of the brain, the circle of Willis, and the cranial nerves — explaining the III, VI, VII, and VIII nerve palsies, the hydrocephalus from basal cistern blockage, and the vasculitic infarcts (often in the internal capsule and basal ganglia, producing hemiparesis) that define the disease.[12][13]
Cryptococcal meningitis in advanced HIV results from reactivation of Cryptococcus neoformans; the yeast reaches the meninges haematogenously, replicates in the CSF, and sheds a polysaccharide capsule that migrates out through the arachnoid villi and obstructs CSF reabsorption — producing the characteristically very high opening pressures that drive papilloedema, cranial nerve palsies, and visual loss, and that demand repeated therapeutic lumbar punctures.[14]
Clinical Presentation
Acute bacterial meningitis
The classic presentation is the tetrad of fever, headache, neck stiffness, and altered mental status. All four coexist in only about 44 percent of patients, but virtually all (about 95 percent) have at least one, and most have two — usually fever and headache with meningismus. The headache is typically severe, generalized, and builds over hours to a day; photophobia and nausea or vomiting are common, and altered mental status ranges from mild confusion to coma.[1]
FEVER-M
Meningococcal disease has a distinctive signature: a rapidly evolving petechial or purpuric non-blanching rash, septicaemic shock, and disseminated intravascular coagulation with purpura fulminans and adrenal haemorrhage (Waterhouse-Friderichsen syndrome). A patient with meningococcaemia can deteriorate from febrile to shocked within hours, and the rash — checked on pressure with a glass — is the bedside signal to escalate immediately.[18]
Viral encephalitis
HSV encephalitis presents over a few days with fever, headache, and a change in behaviour or consciousness — confusion, agitation, personality change, aphasia, hallucinations (often olfactory or gustatory), and focal or secondarily generalised seizures. The temporal-lobe predominance produces the classic features of memory disturbance and complex partial seizures. A patient with fever and altered behaviour, rather than neck stiffness alone, should be assumed to have encephalitis until CSF PCR and MRI show otherwise.[8][9]
Brain abscess
Brain abscess presents as headache (the commonest symptom, in 70 to 90 percent), fever, focal neurological deficit, seizures, and altered consciousness — but the classic triad of headache, fever, and focal deficit is present in only about 20 percent, so most patients present with one or two features and the diagnosis hinges on imaging. Fever is absent in around half. A history of otitis, sinusitis, dental infection, endocarditis, or cyanotic congenital heart disease is the clue to the source.[6][7]
Tuberculous meningitis
TB meningitis declares itself more slowly, over one to three weeks, with a prodrome of malaise, low-grade fever (often evening), anorexia, and vague headache. This is followed by meningism, cranial nerve palsies (III causing ptosis and pupillary dilatation, VI causing lateral rectus palsy, VII facial weakness, VIII deafness), and focal deficits from vasculitic stroke. The Medical Research Council grades severity: Grade I (GCS 15, no focal deficit), Grade II (GCS 11 to 14 or focal deficit), Grade III (GCS 10 or below) — the grade predicts outcome and drives the steroid decision.[12][13]
Cryptococcal meningitis
In advanced HIV (CD4 count under 100 cells/μL), cryptococcal meningitis produces a subacute meningitis with prominent raised-ICP features — headache, papilloedema, and cranial nerve palsies — sometimes with comparatively modest meningismus. Classical features may be muted because the host inflammatory response is blunted; the opening pressure at lumbar puncture is frequently very high and is itself a treatable problem.[14]
Neurocysticercosis
Neurocysticercosis presents most often with new-onset seizures (parenchymal cysts, viable or calcified), with headache and raised ICP when cysts are intraventricular or subarachnoid (causing hydrocephalus). Onset is over months to years. A patient from an endemic region with adult-onset focal epilepsy and calcified brain lesions on imaging has neurocysticercosis until proven otherwise.[16][17]
Atypical presentations
Examiners test the atypical presentations deliberately. The elderly may have little or no fever, presenting as confusion or falls. The immunocompromised present subtly, with atypical organisms and muted signs. The neonate shows bulging fontanelle, irritability, high-pitched cry, poor feeding, and apnoea rather than neck stiffness. The neutropenic patient may have no CSF pleocytosis to point to infection. Recognising these prevents the catastrophic assumption that "no fever, no meningitis."[1][2]
Differential Diagnosis
The differential of the acute febrile headache with meningismus is wide, and several mimics are themselves emergencies. Subarachnoid haemorrhage produces thunderclap headache and meningismus but usually without fever at onset; CT and xanthochromia distinguish it. Encephalitis overlaps with meningitis but is dominated by altered mental status and seizures. Brain abscess adds focal deficit and is excluded only by imaging — which is why any focal sign mandates CT before LP. Cerebral malaria (in endemic regions) causes fever and impaired consciousness with a normal CSF. Septic encephalopathy — confusion in a septic but non-meningitic patient — has a near-normal CSF and resolves with treatment of the systemic sepsis. Drug-induced meningitis (NSAIDs, co-trimoxazole, IVIG) and autoimmune meningitis/encephalitis (NMDA receptor antibody encephalitis, neurosarcoid, lupus) complete the aseptic differential and must be considered when cultures are negative.[1][10]
The ring-enhancing lesion differential is its own exam topic: brain abscess, toxoplasmosis (HIV, multiple lesions, anti-Toxoplasma IgG), neurocysticercosis (cyst with scolex), tuberculoma, primary or metastatic tumour, tumefactive demyelination (multiple sclerosis), and a resolving haematoma. Diffusion-weighted MRI is the discriminator: abscess restricts diffusion (bright on DWI, dark on ADC), necrotic tumour does not.[6][7]
Clinical & Bedside Assessment
A focused examination in suspected CNS infection runs through five questions. Is the patient septic or shocked? Check airway, breathing, circulation, perfusion, capillary refill, and blood pressure — meningococcaemia can kill within hours. Is the meningeal irritation present? Test neck stiffness (flexion), Kernig sign (pain or resistance on extending the knee with the hip flexed at 90 degrees), and Brudzinski sign (involuntary hip flexion on passive neck flexion). These signs are highly specific but only moderately sensitive; their absence does not exclude meningitis. Is there a rash? Inspect the whole skin for petechiae and purpura, checking that they do not blanch under pressure from a glass. Is there a focal deficit, papilloedema, or depressed consciousness? These are red flags for a mass lesion and mandate imaging before LP. Where is the source? Otoscopy (otitis media), sinus tenderness, dental exam, skin for entry sites or signs of immunosuppression (oral candidiasis, Kaposi sarcoma), and a cardiac murmur (endocarditis) all narrow the differential.[1][2]
A simultaneous bedside capillary glucose should be drawn whenever meningitis is suspected, because CSF glucose is interpreted against the concurrent blood glucose (the CSF-to-blood glucose ratio under 0.4 is strongly suggestive of bacterial meningitis). [1]
Investigations
Lumbar puncture and CSF analysis
CSF analysis is the diagnostic cornerstone for meningitis and encephalitis, but it must be timed correctly and performed only when safe. The non-negotiable rule: antibiotics and dexamethasone come first, LP comes second — never delay empiric therapy to obtain CSF. LP provides opening pressure, cell count and differential, glucose (with a paired blood glucose), protein, Gram stain and culture, and targeted molecular tests. [1]
The CSF pattern usually points to the aetiology. Bacterial meningitis shows a cloudy or turbid CSF, a raised opening pressure (over 18 cmH₂O), a neutrophilic pleocytosis (often hundreds to thousands of cells per microlitre, predominantly polymorphs), glucose under 40 mg/dL or a CSF-to-blood ratio under 0.4, protein over 1 g/L, a Gram stain positive in 60 to 90 percent, and a positive culture (the gold standard). Viral meningitis or encephalitis shows a clear CSF with lymphocytic pleocytosis (10 to a few hundred cells per microlitre), a normal glucose, a mildly raised protein, and a positive PCR (HSV-1/2, VZV, enterovirus) — the PCR for HSV can be negative in the first 24 to 48 hours, so a negative early result with high suspicion warrants repeat LP after three to seven days.[1][8]

TB meningitis produces a cobweb or pellicle coagulum when CSF stands, a lymphocytic pleocytosis of 50 to 500 cells, a glucose markedly depressed (often under 1.0 mmol/L), protein of 1 to 5 g/L or higher, and an adenosine deaminase (ADA) above 10 U/L. Acid-fast bacilli on Ziehl-Neelsen stain are positive in only a minority; GeneXpert MTB/RIF and mycobacterial culture (the latter taking weeks) provide confirmation. Cryptococcal meningitis shows lymphocytes, low glucose, high protein, a strongly positive cryptococcal antigen (CRAG) in CSF and serum (sensitivity above 95 percent in HIV), and India ink positivity in about 50 to 75 percent of AIDS cases.[12][14]
Bacterial
Viral (HSV)
Tuberculous
Cryptococcal
Blood and other tests
Blood cultures (two sets) should be drawn before antibiotics if possible; they are positive in roughly half of bacterial meningitis cases and may be diagnostic when LP is deferred. Other bloods: full blood count (leucocytosis), urea and electrolytes (hyponatraemia from SIADH), liver function, glucose, coagulation screen, C-reactive protein and procalcitonin (the latter favouring bacterial over viral), and an HIV test in any atypical, subacute, or immunosuppressed presentation. Serum and urine CRAG screens for cryptococcal antigen in advanced HIV; Toxoplasma IgG stratifies the HIV patient with a ring-enhancing lesion.[1][14]
Imaging
Contrast MRI is the gold standard for encephalitis and abscess. In HSV encephalitis, T2/FLAIR sequences show hyperintensity and swelling of the medial temporal lobe and inferior frontal lobe, often bilateral but asymmetric, with restricted diffusion and sometimes petechial haemorrhage. In brain abscess, contrast MRI shows a ring-enhancing lesion with central restricted diffusion on DWI — the single feature that best distinguishes abscess from necrotic tumour. CT with contrast is used in the emergency department and to clear a patient for LP, but it is less sensitive than MRI for early encephalitis and for small posterior fossa lesions.[6][7]
In TB meningitis, contrast CT or MRI shows basal exudate enhancement, hydrocephalus, and sometimes tuberculomas; in neurocysticercosis, MRI shows the pathognomonic cyst with an internal scolex in viable parenchymal cysts, and calcified nodules on CT in the inactive stage.[12][16]
EEG
A periodic lateralised epileptiform discharge (PLED) pattern over a temporal lobe strongly supports HSV encephalitis and is one indication for empirical aciclovir while CSF PCR is awaited. EEG also detects non-convulsive status epilepticus, which can masquerade as reduced consciousness in any CNS infection.[8]
Management — Resuscitation

The first hour decides outcome. The resuscitation bundle for suspected bacterial meningitis has four time-critical components, run in parallel.[2][3]
- Airway, breathing, circulation — oxygen, two large-bore cannulae, intravenous fluids if hypotensive or shocked, and vasopressors (noradrenaline) for septic shock. Intubate if GCS is 8 or below, if the airway is threatened, or for status epilepticus refractory to first-line drugs.
- Blood cultures, then empiric IV antibiotics immediately — within one hour of presentation. Do not wait for LP or CT. Ceftriaxone 2 g IV twice daily plus vancomycin 15 to 20 mg/kg IV (to cover penicillin-resistant pneumococcus), adding ampicillin 2 g IV every four hours when Listeria is in the differential (over 50, pregnant, immunocompromised, alcoholic).
- Dexamethasone 10 mg IV every six hours for four days, given before or with the first antibiotic dose; continue only if pneumococcal meningitis is confirmed, since the benefit is concentrated there.[3][4]
- Lumbar puncture after stabilisation, provided no red flag mandates imaging first; CT before LP if immunocompromised, new seizures, papilloedema, reduced consciousness, or focal deficit.
Exam application bank (NEET-PG / INICET)
One-line answer
CNS infections span the meninges (meningitis), brain parenchyma (encephalitis, abscess), or both (meningoencephalitis). Acute bacterial meningitis is a time-critical emergency: fever, headache, neck stiffness and altered mental status (all four in about 44 percent of cases) demand empiric IV antibiotics within one hour — ceftriaxone 2 g IV BD plus vancomycin, adding ampicillin for Listeria in the over-50, pregnant, or immunocompromised — with dexamethasone 10 mg IV q6h for four days given before or with the first antibiotic dose. CSF analysis distinguishes bacterial (neutrophils, low glucose, high protein) from viral (lymphocytes, normal glucose), TB (low glucose, high lymphocytes, ADA raised), and fungal (cryptococcal antigen positive) patterns. HSV encephalitis needs IV aciclovir 10 mg/kg TDS for 14 to 21 days. Brain abscess shows a ring-enhancing lesion with restricted diffusion on MR [1]
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on CNS Infections — Meningitis, Encephalitis, Brain Abscess, TB, Cryptococcal, Neurocysticercosis.
For suspected viral encephalitis, the resuscitation reflex adds IV aciclovir 10 mg/kg three times daily (every eight hours), started empirically and early while CSF PCR and MRI are awaited — because HSV encephalitis outcome is time-dependent and the drug is far safer than a missed diagnosis.[8][11]
For brain abscess, the resuscitation priority is to recognise the mass lesion (no LP), control raised ICP (head of bed elevated 30 degrees, normocapnia, osmotherapy with mannitol 0.5 g/kg or hypertonic saline if herniating), and arrange urgent neurosurgical referral for drainage.[6]
The first-hour pathway in suspected bacterial meningitis
Management — Definitive & Stepwise
Acute bacterial meningitis — empiric and targeted therapy
Empiric therapy is selected by age, immune status, and the setting (community vs healthcare-associated). [1]
Neonate (under 1 month)
Child 1 mo to 5 yr / adult under 50 (community)
Over 50 / immunocompromised / pregnant / alcoholic
Post-neurosurgery / CSF shunt
Severe penicillin allergy (anaphylaxis)
Once an organism and sensitivities are known, therapy is de-escalated and the duration set by the organism: meningococcal meningitis seven days, pneumococcal and Hib ten to fourteen days, Listeria and gram-negative bacilli twenty-one days. Adjunctive dexamethasone 10 mg IV every six hours for four days reduces hearing loss and, in pneumococcal disease, mortality; it must be given before or with the first antibiotic dose to blunt the inflammatory surge of bacterial lysis, and is continued only if pneumococcus is confirmed.[2][3][4]
The classic landmark trial (de Gans and van de Beek, NEJM 2002) showed a mortality reduction from 25 to 15 percent in pneumococcal meningitis with dexamethasone; the individual-patient-data meta-analysis (van de Beek, Lancet Neurology 2010) and the Cochrane review (Brouwer 2015) confirm the benefit is concentrated in high-income settings and pneumococcal disease, and is weaker or absent in low-income, TB-endemic settings — a controversy worth knowing.[3][4][5]
Viral encephalitis (HSV)
IV aciclovir 10 mg/kg three times daily (every eight hours) for 14 to 21 days, dose-adjusted for renal function and given with adequate hydration to prevent crystalline nephropathy. Start it empirically in any patient with suspected encephalitis. CSF PCR confirms HSV, but an early negative PCR with high clinical suspicion should prompt a repeat lumbar puncture after three to seven days. Without treatment, HSV encephalitis mortality approaches 70 percent and survivors are left with severe temporal-lobe deficits; the Whitley/Sköldenberg trials in the 1980s established aciclovir over vidarabir as definitive therapy, halving mortality.[8][9][11]
Brain abscess
Treatment combines broad-spectrum antibiotics, surgical drainage, and source control. Empiric ceftriaxone 2 g IV twice daily plus metronidazole 500 mg IV every eight hours covers the streptococci (especially Streptococcus milleri group), anaerobes (Bacteroides), and Enterobacteriaceae that cause most community-acquired abscesses; add vancomycin when Staphylococcus aureus or resistant streptococci are suspected (trauma, endocarditis, neurosurgery). In the immunocompromised host, extend cover to Toxoplasma (pyrimethamine plus sulfadiazine), Nocardia (high-dose co-trimoxazole), and fungi (amphotericin-based). Stereotactic aspiration is both diagnostic (culture the pus) and therapeutic, and is preferred; surgical excision is reserved for multiloculated, persistent, fungal, or posterior-fossa abscesses. Antibiotics alone are an option only for small abscesses (under 2 cm), multiple abscesses, or surgically inaccessible lesions, and require serial MRI monitoring. Total antibiotic duration is four to six weeks intravenously.[6][7]
Tuberculous meningitis
Standard therapy is the four-drug RIPE regimen — rifampicin (usually 10 to 15 mg/kg or weight-banded), isoniazid (with pyridoxine 25 mg daily to prevent peripheral neuropathy), pyrazinamide, and ethambutol — for an intensive two months, followed by rifampicin plus isoniazid for a total of 9 to 12 months. Adjunctive corticosteroids improve survival (dexamethasone taper per the Thwaites regimen, or prednisolone in children) and are standard of care in all but the mildest disease; they reduce the inflammatory basal exudate, hydrocephalus, and vasculitic stroke. Hydrocephalus may require an external ventricular drain or shunt. Drug-resistant TB meningitis requires expert input and the addition of fluoroquinolones and other agents; treatment should follow WHO and national (ICMR) guidance.[12][13]
Cryptococcal meningitis
Treatment is divided into induction, consolidation, and maintenance phases. Induction uses amphotericin B deoxycholate 0.7 to 1.0 mg/kg/day plus flucytosine 100 mg/kg/day for two weeks; flucytosine clears the CSF faster and reduces relapse. The AMBITION-c trial (NEJM 2022) established that a single 10 mg/kg dose of liposomal amphotericin B combined with flucytosine and fluconazole is non-inferior to the two-week standard regimen and substantially safer — a major advance for resource-limited settings. Consolidation is fluconazole 800 to 1200 mg/day for eight weeks, then maintenance fluconazole 200 mg/day until immune reconstitution on antiretroviral therapy. Raised intracranial pressure is managed with daily therapeutic lumbar punctures or a shunt; antiretroviral therapy is deferred for four to six weeks to reduce the risk of immune reconstitution inflammatory syndrome (IRIS).[14][15]
Neurocysticercosis
Management is symptom-directed and subtype-specific. For viable parenchymal cysts, albendazole 15 mg/kg/day in two divided doses for 7 to 14 days (some regimens extend to 28 days) kills the parasite; praziquantel 50 mg/kg/day in three divided doses for 15 days is an alternative, and the two can be combined for subarachnoid disease. Corticosteroids (prednisolone 1 mg/kg/day, or higher for many cysts) are given before and during antiparasitic therapy to control the inflammatory response released by dying cysts, which can otherwise precipitate seizures, raised ICP, or stroke. Antiepileptic drugs control seizures; calcified (non-viable) cysts are treated with antiepileptics alone — no antiparasitic drug is needed. Hydrocephalus from intraventricular or subarachnoid cysts requires neurosurgical shunting, and intraventricular cysts may need endoscopic removal. These principles are codified in the 2017 IDSA/ASTMH guidelines.[16][17]
Specific Subtypes & Scenarios
Meningococcal disease and its prevention
N. meningitidis colonises the nasopharynx and is spread by respiratory droplets; invasive disease manifests as either meningitis, septicaemia, or both. The meningitis belt of sub-Saharan Africa suffers dry-season epidemics; mass MenA conjugate vaccination has transformed this epidemiology. Post-exposure chemoprophylaxis is given to household and kissing contacts within 24 hours of the index case: rifampicin 600 mg orally twice daily for two days, ciprofloxacin 500 mg orally as a single dose, or ceftriaxone 250 mg intramuscularly as a single dose. Healthcare workers exposed to respiratory secretions also need prophylaxis.[18]
HSV encephalitis — the temporal-lobe emergency
The combination of fever, altered behaviour, and seizures, with MRI showing medial temporal-lobe signal change and CSF PCR positive for HSV, is the signature. PLEDs on EEG support the diagnosis. Outcome depends on how early aciclovir is started: the morbidity (memory impairment, temporal-lobe epilepsy) is substantial even in treated patients, so the threshold to treat empirically is deliberately low.[8][11]
Subdural empyema and epidural abscess
These are surgical emergencies that arise by direct spread from sinusitis (frontal), otitis, or dental infection. Subdural empyema presents with fever, headache, focal deficit, and seizures, and progresses rapidly; epidural abscess (intracranial or spinal) presents with local pain followed by neurological deficit. Treatment is urgent surgical drainage plus antibiotics (ceftriaxone plus metronidazole plus vancomycin). Delay causes irreversible neurological injury.[6]
Toxoplasmosis in HIV
In an HIV patient with CD4 under 100 and multiple ring-enhancing lesions, cerebral toxoplasmosis is the leading diagnosis; anti-Toxoplasma IgG is usually positive. Treatment is pyrimethamine 200 mg loading then 50 to 75 mg/day plus sulfadiazine 1 to 1.5 g q6h, with folinic acid, for two to six weeks. If there is no radiographic response within two weeks, primary CNS lymphoma (EBV-driven) must be considered and biopsied.[7]
Complications & Pitfalls
The complications of CNS infection span the acute phase and the long term. Sensorineural hearing loss is the commonest long-term sequela of bacterial meningitis (10 to 30 percent) — hence the role of dexamethasone and the need for early audiological assessment on recovery. Seizures and post-meningitis epilepsy, hydrocephalus (communicating in bacterial and TB meningitis, obstructive in intraventricular neurocysticercosis and some abscesses), focal deficits and stroke (vasculitic infarct, especially in TB and pneumococcal meningitis), cranial nerve palsies, cognitive impairment, and the syndrome of inappropriate antidiuretic hormone with hyponatraemia all occur. Cerebral venous sinus thrombosis, subdural effusion or empyema, and brain abscess may complicate meningitis.[1][13]
In brain abscess, the catastrophic complication is rupture into the ventricular system — sudden deterioration, high mortality — and herniation from mass effect. In cryptococcal meningitis, uncontrolled raised ICP causes irreversible visual loss and is itself a major cause of death; in HIV patients starting ART, immune reconstitution inflammatory syndrome (IRIS) can worsen any CNS infection and is the reason ART is deferred.[6][14]
The classic pitfalls are procedural and cognitive. Lumbar puncture in the presence of a mass lesion or raised ICP can precipitate fatal herniation — image first if any red flag is present. Delaying antibiotics for CT or LP costs lives — give antibiotics first. Assuming "no fever excludes meningitis" is repeatedly disproved in the elderly, immunocompromised, and neutropenic. Forgetting ampicillin for Listeria in the over-50 or pregnant patient is a common, avoidable error. Missing HSV encephalitis by waiting for CSF PCR before starting aciclovir is indefensible. Stopping dexamethasone in non-pneumococcal meningitis (where it has no proven benefit) is correct practice.[2][8]
Prognosis & Disposition
Bacterial meningitis carries a mortality of 10 to 20 percent, higher for pneumococcal than meningococcal disease; up to a third of survivors have neurological sequelae, most often hearing loss, cognitive impairment, or epilepsy. Meningococcal septicaemia kills 5 to 15 percent, with limb loss and skin scarring from purpura fulminans in survivors. HSV encephalitis, untreated, kills about 70 percent; early aciclovir halves mortality but leaves many with temporal-lobe morbidity. TB meningitis kills 20 to 30 percent, with worse outcomes in grade III disease and HIV; many survivors are left disabled. Cryptococcal meningitis kills 10 to 30 percent depending on access to amphotericin, raised ICP management, and ART; brain abscess kills 5 to 15 percent, with 30 to 50 percent of survivors left with residual deficit or epilepsy.[1][6][13][14]
The decisive prognostic markers are Glasgow Coma Scale at presentation, time to antibiotics, the organism and its sensitivities, immune status, seizures, and comorbidity. Disposition: admit to ICU if the GCS is 8 or below, if the patient is intubated or in septic shock, has status epilepticus, or has uncontrolled raised ICP; otherwise to a neurology or infectious diseases ward with close observation; rehabilitation for those with residual neurological deficit. A safety-net follow-up must include audiology at six to eight weeks and neuropsychological review where cognition is affected.[1]
Special Populations
The neonate (under one month) is infected by group B streptococcus, E. coli K1, and Listeria; treat with cefotaxime plus ampicillin, and add IV aciclovir if HSV is suspected (a vesicular rash, maternal genital HSV, or a CSF picture with red cells and a low glucose). The signs are non-specific — bulging fontanelle, irritability, high-pitched cry, poor feeding, apnoea — and a septic work-up including LP is mandatory.[2]
In pregnancy, the Listeria risk rises (food-borne, third-trimester) and ampicillin is added to empiric therapy; certain drugs are avoided (tetracyclines; co-trimoxazole in the third trimester for kernicterus risk). The elderly present atypically — confusion, little or no fever — and carry a worse prognosis, with pneumococcus and Listeria both in the differential.[1]
In HIV with CD4 under 100, think Cryptococcus (screen with serum/urine CRAG and treat antigenaemia), Toxoplasma (multiple ring-enhancing lesions), TB, syphilis, and progressive multifocal leucoencephalopathy (JC virus). Defer ART after cryptococcal meningitis to reduce IRIS. The transplant, neutropenic, or heavily immunosuppressed patient is at risk from Listeria, Nocardia, Aspergillus, and gram-negatives, mandating broader empiric cover. After neurosurgery or with a CSF shunt, the differential shifts to coagulase-negative staphylococci, Staphylococcus aureus, and Pseudomonas; treat with vancomycin plus ceftazidime (or meropenem) and plan shunt removal.[2][14]
Evidence, Guidelines & Regional Differences
The evidence base is anchored by a handful of landmark studies. de Gans and van de Beek (NEJM 2002) established adjunctive dexamethasone in adults with bacterial meningitis, halving pneumococcal mortality; the individual-patient-data meta-analysis (van de Beek, Lancet Neurology 2010) and the Cochrane review (Brouwer 2015) refined this, showing the benefit is concentrated in high-income, pneumococcal settings — a controversy that limits dexamethasone recommendations in some low-income, TB-endemic regions. The IDSA bacterial meningitis guidelines (Tunkel, 2004), though older, still anchor empiric therapy choices, and the Brouwer Nature Reviews Disease Primers (2016) synthesises current understanding.[1][2][3][4][5]
In viral encephalitis, the Whitley and Sköldenberg trials (NEJM 1986) established aciclovir over vidarabine, and the UK ABN/British Infection Society guidelines (Solomon, 2012) operationalised the first-dose-within-six-hours aciclovir reflex. The Granerod encephalitis study (Lancet Infectious Diseases 2010) defined the contemporary aetiological spectrum.[8][10][11]
In TB meningitis, the Thwaites trials (and the Lancet Neurology 2022 review with Wilkinson's 2017 Nature Reviews Neurology primer) define RIPE-plus-steroids as standard. In cryptococcal meningitis, the AMBITION-c trial (NEJM 2022) has displaced the older two-week amphotericin regimen in many centres with a single high-dose liposomal amphotericin strategy, and the Rajasingham Nature Reviews Disease Primers (2023) integrates this into the modern paradigm.[12][13][14][15]
For neurocysticercosis, the 2017 IDSA/ASTMH guidelines (White et al.) define who gets antiparasitic therapy (viable parenchymal cysts) and who gets antiepileptics alone (calcified cysts).[17]
Regional deltas are real and examined. The meningitis belt drives MenA conjugate vaccine strategy; the Indian subcontinent carries TB meningitis and Japanese encephalitis (with JE vaccine in the national programme and Culex-vector control); sub-Saharan Africa carries the cryptococcal burden (CRAG screening at CD4 under 100). Vaccine schedules differ — MenB (Bexsero/Trumenba) is used in the UK and ANZ for adolescents and infants respectively, MenACWY in the US for pre-adolescents and college entrants, and PCV13 universally in childhood.[18]
Exam Pearls
DALEK
References
- [1]Brouwer MC, Tunkel AR, van de Beek D. Community-acquired bacterial meningitis Nat Rev Dis Primers, 2016.PMID 27808261
- [2]Tunkel AR, Hartman BJ, Kaplan SL, et al. Practice guidelines for the management of bacterial meningitis Clin Infect Dis, 2004.PMID 15494903
- [3]de Gans J, van de Beek D. Dexamethasone in adults with bacterial meningitis N Engl J Med, 2002.PMID 12432041
- [4]Brouwer MC, McIntyre P, Prasad K, van de Beek D. Corticosteroids for acute bacterial meningitis Cochrane Database Syst Rev, 2015.PMID 26362566
- [5]van de Beek D, Farrar JJ, de Gans J, et al. Adjunctive dexamethasone in bacterial meningitis: a meta-analysis of individual patient data Lancet Neurol, 2010.PMID 20138011
- [6]Corsini Campioli C, Castillo Almeida NE, O'Horo JC, et al. Bacterial Brain Abscess: An Outline for Diagnosis and Management Am J Med, 2021.PMID 34297973
- [7]Sonneville R, Ruimy R, Benzonana N, et al. An update on bacterial brain abscess in immunocompetent patients Clin Microbiol Infect, 2017.PMID 28501669
- [8]Solomon T, Michael BD, Smith PE, et al. Management of suspected viral encephalitis in adults--Association of British Neurologists and British Infection Association National Guidelines J Infect, 2012.PMID 22120595
- [9]Steiner I. Recent issues in herpes simplex encephalitis J Neurovirol, 2013.PMID 23775137
- [10]Granerod J, Ambrose HE, Davies NW, et al. Causes of encephalitis and differences in their clinical presentations in England: a multicentre, population-based prospective study Lancet Infect Dis, 2010.PMID 20952256
- [11]Whitley RJ, Alford CA, Hirsch MS, et al. Vidarabine versus acyclovir therapy in herpes simplex encephalitis N Engl J Med, 1986.PMID 3001520
- [12]Wilkinson RJ, Rohlwink U, Misra UK, et al. Tuberculous meningitis Nat Rev Neurol, 2017.PMID 28884751
- [13]Thwaites GE, van Toorn R, Schoeman J, et al. Tuberculous meningitis: progress and remaining questions Lancet Neurol, 2022.PMID 35429482
- [14]Rajasingham R, Govender NP, Jordan A, et al. Cryptococcal meningitis Nat Rev Dis Primers, 2023.PMID 37945681
- [15]Jarvis JN, Lawrence DS, Meya DB, et al. Single-Dose Liposomal Amphotericin B Treatment for Cryptococcal Meningitis N Engl J Med, 2022.PMID 35320642
- [16]Garcia HH, Nash TE, Del Brutto OH. Clinical symptoms, diagnosis, and treatment of neurocysticercosis Lancet Neurol, 2014.PMID 25453460
- [17]White AC Jr, Coyle CM, Rajshekhar V, et al. Diagnosis and Treatment of Neurocysticercosis: 2017 Clinical Practice Guidelines by the Infectious Diseases Society of America (IDSA) and the American Society of Tropical Medicine and Hygiene (ASTMH) Clin Infect Dis, 2018.PMID 29481580
- [18]Rosenstein NE, Perkins BA, Stephens DS, Popovic T, Hughes JM. Meningococcal disease N Engl J Med, 2001.PMID 11333996