Neurology · neurology
Delirium
Also known as Acute confusional state · Acute brain failure · Toxic/metabolic encephalopathy · Acute psycho-organic syndrome · Intensive care unit (ICU) psychosis
Delirium is an acute, fluctuating disturbance of attention and awareness caused by a medical condition, substance intoxication or withdrawal, medication, toxin exposure, or multiple factors (DSM-5). It is a medical emergency and a marker of acute brain dysfunction, carrying an in-hospital mortality that can reach 25 percent and a doubled 6-month mortality in older adults. The commonest precipitants in the elderly are infection (UTI, pneumonia), drugs (opioids, benzodiazepines, anticholinergics), dehydration, metabolic/electrolyte disturbance, hypoxia, uncontrolled pain, surgery, constipation and urinary retention. Diagnosis is clinical using the Confusion Assessment Method (CAM) — acute onset with fluctuation AND inattention AND (disorganised thinking OR altered level of consciousness). The overriding management principle is to find and treat the precipitant; non-pharmacological multi-component care is first-line (orientation, sensory aids, hydration, sleep, mobility, bowel/bladder care, pain control). Pharmacological sedation with low-dose haloperidol 0.5 to 1 mg orally or intramuscularly is reserved for severe agitation or aggression that risks the patient or others. Benzodiazepines worsen delirium and are AVOIDED except in alcohol/benzodiazepine withdrawal and seizures. Hypoactive delirium is commonly missed and carries the worst prognosis.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Exam tags
Red flags

Overview & Definition
Delirium (from the Latin delirare, "to deviate from the straight track") is an acute, transient, fluctuating disturbance of attention, awareness and cognition caused by a general medical condition, substance intoxication or withdrawal, a medication or toxin. It reflects acute, diffuse cerebral dysfunction and is a clinical diagnosis defined by DSM-5-TR criteria.[1]
DSM-5-TR diagnostic criteria for delirium (the canonical five elements — examiner favourite): [1]
- Disturbance in attention and awareness — reduced ability to direct, focus, sustain and shift attention (the core, mandatory feature).
- Acute onset (hours to days) with a fluctuating course (waxes and wanes through the day, characteristically worse at night — "sundowning").
- An additional disturbance in cognition (memory deficit, disorientation, language, perception, visuospatial disturbance).
- The disturbances in (1) and (3) are not better explained by a pre-existing neurocognitive disorder and do not occur in the context of a coma.
- There is evidence from history, examination or investigations that the disturbance is a direct physiological consequence of a medical condition, substance intoxication/withdrawal, or toxin exposure (i.e. delirium is a syndrome, never a final diagnosis). [1]
The single most important practical point: delirium is a syndrome, not a diagnosis. The task is never to "treat delirium" — it is to find and reverse the precipitant. The confusion, hallucinations and agitation are the brain screaming that something is wrong systemically. Treating them with sedatives without hunting for the cause is the cardinal error.[1]
Conceptual frame — delirium as "acute brain failure": just as acute kidney injury is the renal response to a systemic insult, delirium is the brain's acute organ-failure response to a stressor. It is therefore a powerful marker of illness severity, predicts worse outcomes independent of comorbidity, and is increasingly recognised as a harbinger of long-term cognitive decline — not merely a transient, reversible phenomenon.[1]
Classification
By psychomotor subtype (the classification that matters most clinically, because it changes recognition, prognosis and approach):[1]
Hyperactive delirium
- Restless, agitated, shouting, pulling out lines, wandering, hypervigilant
- Prominent hallucinations, illusions and delusions (usually visual)
- Easily recognised — staff notice it
- ~25 percent of inpatient delirium
- Better prognosis than hypoactive (because it is recognised and treated)
Hypoactive delirium
- Quiet, withdrawn, lethargic, drowsy, decreased mobility and appetite
- Minimal motor activity; paucity of speech
- Commonly MISSED — looks 'calm', may be mistaken for depression or fatigue
- ~25-50 percent of inpatient delirium; majority in ICU and palliative care
- WORST prognosis — highest mortality, longest stay, most cognitive decline
Mixed delirium
- Fluctuates between hyperactive and hypoactive features over hours-days
- Commonest pattern overall in many cohorts
- Recognised because the hyperactive phase brings it to attention
- Prognosis intermediate
No-subtype
- Normal psychomotor activity but attention/awareness disturbed
- Meets DSM-5 but no motoric subtype fits
- Easily missed on cursory exam
- Document subtype at every assessment — it changes prognosis
By aetiology (DSM-5 specifiers): [1]
- Substance intoxication — e.g. anticholinergics, opioids, benzodiazepines, antihistamines, alcohol, corticosteroids, dopaminergic drugs.
- Substance withdrawal — alcohol / benzodiazepine / barbiturate withdrawal (delirium tremens).
- Medication-induced — onset during exposure, attributable to a prescription drug.
- Due to another medical condition — infection (UTI, pneumonia, sepsis), metabolic (uraemia, hepatic failure, hyponatraemia, hypoglycaemia, hypercalcaemia, thyroid storm), hypoxia/hypercapnia (respiratory failure, CO2 retention), neurological (stroke, subdural haematoma, meningitis/encephalitis, post-ictal state).
- Multifactorial — the rule rather than the exception in the elderly; usually two or more precipitants converge on a vulnerable brain.
- Subsyndromal delirium — features of delirium that do not meet full criteria; still independently associated with longer stay and worse outcomes; a target for prevention. [1]
Epidemiology & Risk Factors
Delirium is one of the commonest complications of hospitalisation in older adults and one of the most under-recognised.[1]
Delirium — incidence by setting
Inouye's predisposing vs precipitating model (the frame every exam question on risk runs through): delirium emerges when a predisposed/vulnerable brain is hit by an external precipitant. The more vulnerable the brain, the smaller the insult needed; the bigger the insult, the less vulnerable the brain can be.[1]
Predisposing factors (host vulnerability): [1]
- Age (especially over 75) — the strongest single host factor.
- Pre-existing dementia or cognitive impairment — multiplies risk roughly two- to three-fold ("delirium superimposed on dementia").
- Male sex, depression, prior stroke, Parkinson's disease, dementia with Lewy bodies.
- Sensory impairment — uncorrected vision or hearing loss.
- Functional dependence, low mobility, recent falls.
- Multiple comorbidities, polypharmacy, high anticholinergic burden.
- Alcohol misuse, malnutrition, dehydration, electrolyte disturbance at baseline.
- Severe illness at presentation (APACHE-II), prior delirium episode, sleep deprivation. [1]
Precipitating factors (the insults — high-yield, examine in every case): [1]
- Infection — the commonest single precipitant in the elderly: urinary tract infection, pneumonia, cellulitis, bacteraemia, COVID-19.
- Drugs — initiate, withdraw or change: opioids, benzodiazepines, anticholinergics (oxybutynin, hyoscine, amitriptyline), antihistamines, corticosteroids, dopaminergics, anticonvulsants; withdrawal of long-term alcohol or benzodiazepines.
- Dehydration and electrolyte disturbance — hyponatraemia, hypernatraemia, hypokalaemia, hypocalcaemia, hypercalcaemia.
- Hypoxia / hypercapnia — respiratory failure, CO2 retention, anaemia.
- Metabolic — uraemia, hepatic encephalopathy, hypoglycaemia, hyperglycaemia, thyroid dysfunction.
- Uncontrolled pain — under-treated pain precipitates delirium as readily as over-sedation.
- Surgery and anaesthesia — especially hip fracture repair, cardiac surgery, prolonged procedures.
- Environmental / ICU — sleep deprivation, sensory deprivation, immobility, catheters/lines, transfer between wards, restraints.
- Constipation and urinary retention — both reversible and commonly forgotten.
- Neurological — stroke, subdural haematoma (esp. after a fall in an anticoagulated patient), post-ictal state, non-convulsive status epilepticus, meningoencephalitis. [1]
Anticholinergic burden is a recurring exam favourite and a modifiable risk. The Anticholinergic Cognitive Burden (ACB) scale scores drugs 0 (none) to 3 (strong); high cumulative burden independently predicts delirium. Common high-burden culprits: oxybutynin, amitriptyline, hyoscine, promethazine, codeine, furosemide, digoxin at higher doses, ipratropium, ranitidine-class. A medication review aimed at de-prescribing anticholinergics on admission is a core prevention strategy.[1]
Pathophysiology
Delirium is mechanistically multifactorial — no single pathway explains all cases. The current model integrates neurotransmitter imbalance, neuroinflammation, direct neuronal insult, and sleep-wake/HPA-axis dysregulation converging on a brain whose reserve is already compromised.[1]
1. Neurotransmitter imbalance — the cholinergic-dopaminergic seesaw (the exam-favourite mechanism): [1]
- Acetylcholine DEFICIENCY in the central nervous system is the most consistent finding. Cholinergic neurons in the basal forebrain project widely to cortex and are essential for attention and consciousness. The vulnerability of the cholinergic system explains two clinical facts: (i) anticholinergic drugs reliably precipitate delirium (they block muscarinic receptors and tip an already-marginal system into failure); and (ii) patients with dementia (especially Alzheimer's disease, where cholinergic neurons degenerate) are highly susceptible to delirium.
- Dopamine EXCESS is the counterpart. Dopaminergic hyperactivity produces the agitation, hallucinations and psychosis of hyperactive delirium. This explains why dopamine-D2-blocking antipsychotics (haloperidol) are effective symptomatic therapy for agitation — but they do not treat the underlying cause.
- Other transmitters: GABA-ergic excess (from benzodiazepines and alcohol) impairs attention and explains why benzodiazepines worsen most delirium; serotonin excess is implicated in serotonin syndrome; norepinephrine dysregulation underlies the autonomic signs of withdrawal. [1]
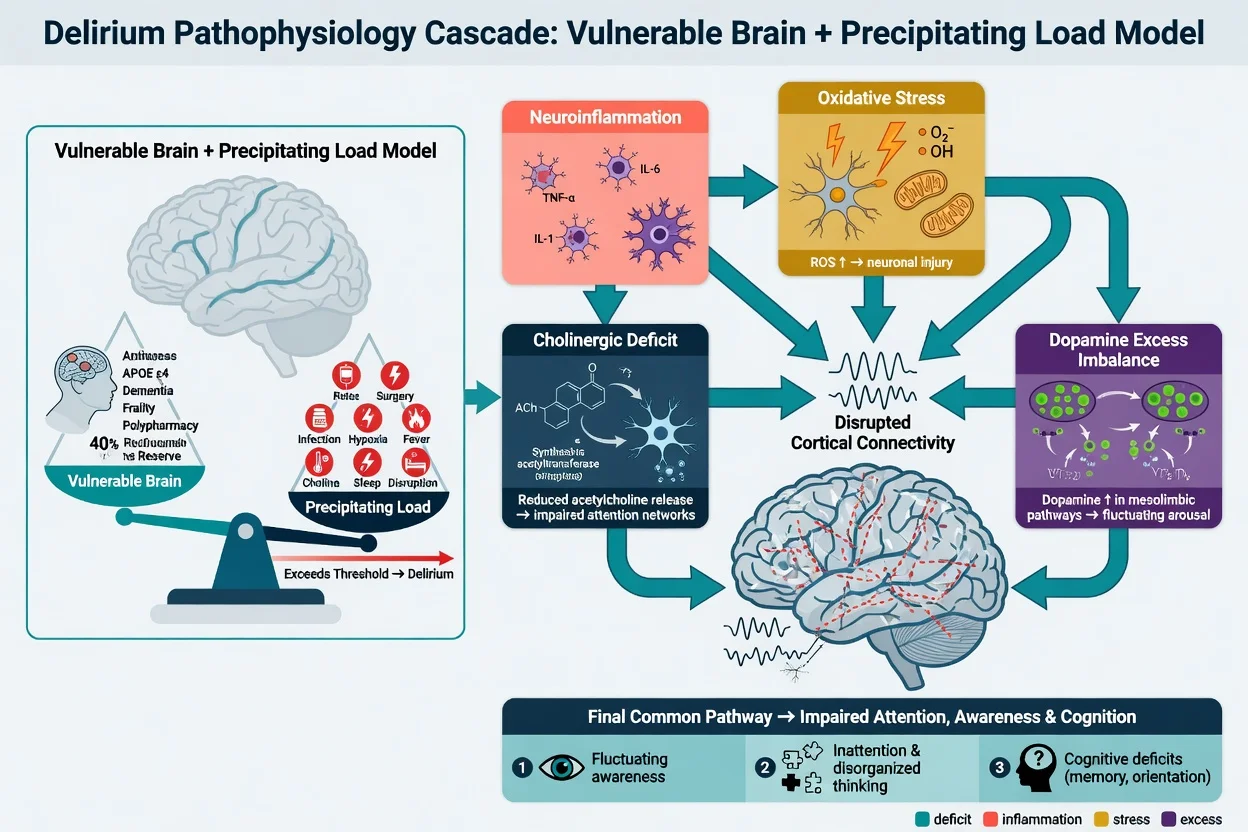
2. Neuroinflammation and microglial activation: infection, surgery and trauma trigger a peripheral cytokine surge (IL-1beta, IL-6, TNF-alpha). These cytokines cross the blood-brain barrier (active transport and leaky regions around the circumventricular organs) and activate microglia, which in turn release more cytokines, reactive oxygen species and glutamate, disrupting neuronal synaptic transmission and connectivity. In a brain with pre-existing microglial priming (ageing, dementia), the response is exaggerated — explaining the elderly vulnerability. [1]
3. Direct neuronal insult: focal or diffuse brain injury — stroke, traumatic brain injury, subdural haematoma, meningoencephalitis, hypoxia, hypoglycaemia — disrupts neuronal networks directly. [1]
4. Network disconnection: functional imaging shows disruption of higher-order cortical networks, particularly the default mode network and attentional networks, producing the global cognitive and attentional failure. [1]
5. Sleep-wake cycle disruption and HPA-axis dysregulation: melatonin dysregulation produces the characteristic sleep-wake inversion (drowsy by day, agitated at night — "sundowning"); cortisol excess from acute illness amplifies the inflammatory and cognitive disturbance. [1]
Why does delirium predict long-term cognitive decline? The "cognitive reserve" model: an episode of delirium may cause permanent neuronal injury (through sustained neuroinflammation, ischaemia, or unmasking a pre-clinical neurodegenerative process), accelerating the trajectory to dementia. Delirium is therefore both a consequence of, and a risk factor for, dementia — a two-way relationship central to modern geriatric medicine.[1]
Clinical Presentation
The core clinical features (memorise the cardinal triad — acute, fluctuating, inattentive):[1]
- Acute onset — developing over hours to days; the patient "wasn't like this yesterday." A collateral timeline from family or nursing staff is essential.
- Fluctuating course — severity waxes and wanes through the day; lucid intervals can mislead the assessor ("but they were fine this morning"). Classically worse at night (sundowning) when environmental cues and staffing reduce.
- Inattention — the defining core feature. The patient is distractible, cannot sustain or shift attention, cannot follow a conversation or commands, cannot do basic attention tasks (see Bedside Assessment).
- Altered level of consciousness — hyperalert, drowsy, stuporous or fluctuating between.
- Disorganised thinking — rambling, irrelevant, illogical speech; cannot follow a logical thread.
- Cognitive disturbance — disorientation (typically time first, then place, then person), recent-memory impairment, language disturbance (dysnomia, dysgraphia), visuospatial disturbance.
- Perceptual disturbance — visual illusions and hallucinations (more than auditory), poorly-formed paranoid delusions.
- Sleep-wake disturbance — reversal; insomnia at night, somnolence by day.
- Mood/affect — fear, anxiety, irritability, apathy, emotional lability. [1]
Hyperactive subtype — the patient is restless, agitated, hypervigilant, may shout, pull out lines and catheters, climb out of bed, strike staff, experience vivid visual hallucinations and paranoid delusions. Easily recognised — but commonly mislabelled as "agitation", "behavioural disturbance", or primary psychiatric illness. [1]
Hypoactive subtype — the patient is quiet, withdrawn, lethargic, drowsy, paucity of speech, decreased mobility and oral intake. Easily missed ("they're just tired / depressed / sleeping") — but carries the worst prognosis (highest mortality, longest stay, greatest cognitive decline) because it goes unrecognised and untreated. Always actively screen for it with attention testing in any elderly inpatient who is "quiet" or "off legs."[1]
Atypical presentation in the elderly — the "delirium masquerades": the classic fever/agitation may be ABSENT. Elderly patients with delirium may present with: [1]
- New, unexplained functional decline ("off legs", new inability to mobilise or self-care).
- Falls (the confused patient misjudges steps or forgets the bedrails).
- New urinary or faecal incontinence.
- Anorexia, refusal to eat or drink.
- Withdrawal and reduced interaction.
- A subtle but new worsening of baseline dementia. [1]
A lower threshold to screen for delirium in any deteriorating elderly inpatient is mandatory. [1]
Differential Diagnosis
An acutely confused patient is not always delirious, and delirium is not always the whole story. Distinguish:[1]
Delirium vs Dementia
- Onset: acute (hours-days) vs insidious (months-years)
- Course: fluctuating, worse at night vs progressive, steady decline
- Attention: GLOBALLY IMPAIRED (core feature) vs relatively preserved early
- Consciousness: clouded/reduced vs normal (clear until late)
- Hallucinations: usually VISUAL vs often absent (until late Lewy body)
- Reversibility: usually reversible vs progressive, irreversible
- Often COEXIST: delirium superimposed on dementia is common — acute worsening of dementia = delirium until proven otherwise
Delirium vs Depression
- Tempo: acute + fluctuating vs subacute (weeks) + sustained
- Core: attention/awareness vs MOOD (pervasive low mood, anhedonia)
- Attention: impaired vs intact (patient can attend if motivated)
- Responses: confabulation, disorganised vs 'I don't know', slow but coherent
- Sleep: fragmented/reversed vs early-morning wakening (characteristic)
- Diurnal: worse at night vs worse in morning
- Both can coexist — depression is a predisposing factor for delirium
Delirium vs Psychosis/Schizophrenia
- Consciousness: clouded in delirium vs CLEAR in primary psychosis
- Hallucinations: VISUAL, fleeting in delirium vs AUDITORY, systematised in schizophrenia
- Delusions: transient, poorly formed vs systematised, fixed, paranoid
- Onset: acute vs chronic (often insidious adolescence/young adult)
- Orientation: impaired vs intact
- Vital signs/autonomic: abnormal in delirium (fever, tachycardia) vs normal
- Acute psychosis in older person with no psychiatric history = presume delirium until excluded
Other differentials to actively exclude: [1]
- Mania — pressured speech, grandiosity, reduced sleep need; check consciousness and look for an organic trigger in any first-episode mania over 40.
- Generalised anxiety / panic — intact cognition, attention preserved, recognisable fear.
- Non-convulsive status epilepticus (NCSE) — subtle, fluctuating confusion, sometimes with subtle motor activity; EEG diagnostic (continuous spike-wave or rhythmic activity vs the generalised slowing of delirium). Suspect in any refractory or fluctuating confusion, especially with a seizure history.
- Post-ictal state — confusion after a witnessed or unwitnessed seizure; resolves over minutes to hours.
- Wernicke encephalopathy — the classic triad of confusion, ataxia and ophthalmoplegia/nystagmus; alcohol misuse or malnutrition; give IV thiamine BEFORE glucose.
- Alcohol withdrawal / delirium tremens — autonomic hyperactivity (tachycardia, hypertension, fever), coarse tremor, hallucinosis, seizures; onset 6-48 h after last drink, DTs at 48-72 h.
- Hepatic encephalopathy — liver disease, asterixis (flapping tremor), elevated ammonia (with caveats), constructional apraxia; precipitated by GI bleed, infection, constipation, electrolyte disturbance.
- Uraemic encephalopathy — chronic kidney disease, myoclonus, asterixis.
- Structural brain lesion — stroke, subdural haematoma (post-fall, anticoagulated), tumour, abscess — focal neurological signs, headache, asymmetric reflexes mandate imaging. [1]
Features suggesting a STRUCTURAL lesion rather than metabolic/toxic encephalopathy: focal neurological deficit, asymmetric tendon reflexes, new seizure, papilloedema (raised ICP), headache, sudden onset of a fixed deficit, history of head trauma or anticoagulation — these mandate urgent CT brain. [1]
Clinical & Bedside Assessment
History (collateral is ESSENTIAL): the patient cannot give a reliable history. Speak to the family, carer, nursing staff and GP. Specifically establish: [1]
- Baseline cognition and function — "What were they like two weeks ago? Could they manage money, dress, mobilise independently?" (to distinguish acute from chronic).
- Onset and course — when did it start? Is it worse at night? Has it fluctuated?
- Precipitants — new drugs (prescribed, OTC, herbal), drug withdrawal (alcohol, benzodiazepine), recent falls/heads, infections, surgery, constipation, urinary symptoms, pain.
- Full drug history including anticholinergic burden (ACB scale) and recent changes.
- Alcohol and substance use, sleep, sensory aids. [1]
Mental state examination and bedside attention testing (the core skill):[1]
- Digit span — ask the patient to repeat a string of digits forward then backward. Normal: at least 7 forward, 5 backward. Delirious patients fail below this.
- Months of the year backwards (December, November, October ...) — a sensitive, quick, language-independent test; failure is highly suggestive of inattention.
- Days of the week backwards.
- Serial sevens (subtract 7 from 100 repeatedly) — also tests concentration and calculation.
- The "A test" — read a short passage and ask the patient to squeeze your hand every time they hear the letter "A."
- Orientation — time (day, date, month, year), place (ward, hospital, city), person.
- Registration and short-term recall (name three objects, recall in 1 min and 5 min).
- Note speech, thought form, perception (ask directly about hallucinations) and mood. [1]
General examination — hunt the precipitant: [1]
- Vital signs: temperature (fever, hypothermia), pulse, blood pressure, respiratory rate (the most sensitive single sign of lower-respiratory infection), oxygen saturation, capillary glucose (immediately, in every confused patient).
- Hydration status (skin turgor, mucous membranes, axillary dryness), signs of sepsis.
- Infection sources: chest (crackles, consolidation), urine (dipstick — nitrites, leucocytes; consider retention — bladder scan), abdomen (tenderness, peritonism), skin (cellulitis, pressure sores), line sites, wounds.
- Abdomen: palpable bladder (retention), loaded rectum (constipation).
- Neurological: GCS, pupils, eye movements (Wernicke — nystagmus/ophthalmoplegia), focal deficit, meningism, asterixis, myoclonus, primitive reflexes.
- Cardiovascular: silent MI (ECG in every elderly confused patient), arrhythmia (atrial fibrillation), heart failure.
- Medication review: go through every drug, calculate anticholinergic burden, identify new/changed drugs. [1]
ABCDE primary survey in an agitated patient: secure the airway, give oxygen if hypoxic, establish IV access, check glucose, treat immediate life-threats (hypoxia, hypoglycaemia, hypotension), then calmly assess — with one-to-one nursing, in a quiet well-lit environment, with a familiar relative if possible. [1]
Investigations
Bedline bedside cognitive screens — reproduced verbatim:[1][4]
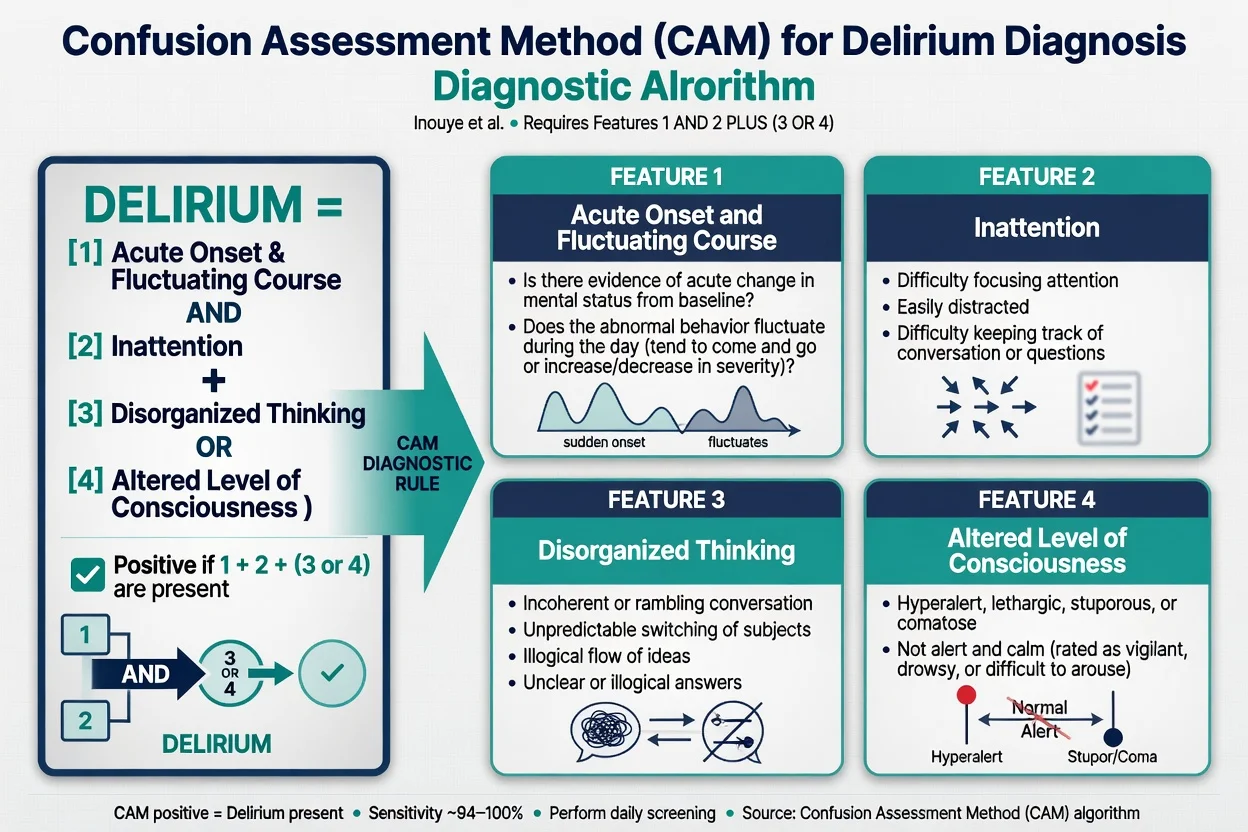
Confusion Assessment Method (CAM, Inouye 1990) — the most widely used bedside diagnostic instrument; sensitivity ~94 percent, specificity ~89 percent in trained hands. Diagnosis requires features 1 AND 2 AND (3 OR 4): [1]
- Acute onset and fluctuating course — information from family or staff; is there evidence of acute change from baseline, and does the abnormal behaviour fluctuate during the day?
- Inattention — difficulty focusing attention; easily distracted; difficulty keeping track of what was being said.
- Disorganised thinking — rambling, irrelevant, unclear or illogical flow of ideas; unpredictable switching from subject to subject.
- Altered level of consciousness — anything other than "alert" (i.e. vigilant/hyperalert, lethargic, stuporous or coma). [1]
4AT (Bellelli 2014) — a rapid, no-equipment screen used in wards and emergency departments; takes under two minutes. A score of 4 or more = delirium.[4]
- Alertness (0 = normal; 4 = markedly sleepy/unrousable).
- AMT-4 (age, date of birth, place, current year) — 0 errors = 0; 1-2 errors = 1; 3-4 errors = 2.
- Attention — months of the year backwards — 0 errors = 0; 1-2 errors = 1; more than 2 errors / cannot start = 2.
- Acute change or fluctuating course — yes = 4; no = 0. [1]
CAM-ICU (Ely 2001) — adapted for intubated/non-verbal ICU patients; combines the RASS (Richmond Agitation-Sedation Scale, −5 unrousable to +4 combative) with a structured attention (the letter "A" test with pictures) and organised-thinking checklist. Performed daily in ICU; validated in mechanically ventilated patients.[3]
Other useful scales (severity and screening): [1]
- Delirium Rating Scale-Revised-98 (DRS-R-98) — 13-item severity scale; distinguishes delirium from dementia and psychosis.
- Memorial Delirium Assessment Scale (MDAS) — 10-item severity scale, used widely in palliative care.
- Delirium Observation Screening (DOS) — nursing-observed 13-item screen.
- Nursing Delirium Screening Scale (Nu-DESC) — quick observational four-item screen.
- Cognitive test baseline — MMSE or MoCA (limited use during acute delirium because attention is impaired, but document the score to establish baseline). [1]
First-line laboratory panel to find the precipitant: [1]
- Capillary glucose (immediate — exclude hypoglycaemia first).
- Full blood count (infection — leucocytosis, leucopenia), CRP.
- Urea, electrolytes, creatinine (dehydration, uraemia, Na disturbance — hyponatraemia is a frequent precipitant), glucose.
- Liver function tests, albumin, calcium, magnesium, phosphate.
- TSH (thyroid storm or myxoedema coma).
- B12 and folate in the elderly/alcoholic.
- Urinalysis ± microscopy, culture and sensitivity — UTI is the commonest precipitant in the elderly.
- Chest X-ray — pneumonia, consolidation, heart failure.
- ECG — silent MI (especially in the elderly and diabetic), arrhythmia.
- Blood cultures if fever, sepsis or before antibiotics.
- Venous or arterial blood gas — hypoxia, hypercapnia (CO2 narcosis), acid-base disturbance.
- Troponin if chest pain or atypical presentation suggests acute coronary syndrome.
- Drug levels where relevant (digoxin, lithium, anticonvulsants); urine drug screen if suspected. [1]
Second-line / situation-specific: [1]
- CT or MRI brain — indicated with focal neurology, head trauma, anticoagulation with fall, suspected subdural/haemorrhage/stroke, no cause found on first-line, or failure to respond to treatment. CT is first-line; MRI for suspected encephalitis, small posterior strokes or Wernicke.
- Electroencephalogram (EEG) — not routine, but diagnostic when non-convulsive status epilepticus or Creutzfeldt-Jakob disease is suspected. Classic EEG of delirium = generalised slowing to theta/delta frequencies (vs normal alpha background); specific patterns: triphasic waves in metabolic encephalopathy (hepatic, uraemic), focal spikes/3-Hz spike-wave in NCSE, periodic lateralised epileptiform discharges (PLEDs) in herpes simplex encephalitis.
- Lumbar puncture — if meningitis, encephalitis (including HSV — send CSF PCR) or subarachnoid haemorrhage is suspected.
- Ammonia (hepatic encephalopathy), carboxyhaemoglobin (CO poisoning), blood alcohol and toxicology.
- Septic screen, COVID-19 PCR as indicated.
- Bladder scan (urinary retention) and abdominal X-ray (constipation) where clinically indicated. [1]
Prediction models: PREDELIRIC (PREdiction of DELIRium in ICu patients) — uses 10 predictors to estimate ICU delirium risk within 24 h of admission. AWOL (Age over 80, inability to spell "WORLD" backwards, Orientation deficit, illness severity) — a ward-based pre-op screen. Both identify patients for preventive bundles. [1]
Management — Resuscitation
ABCDE first. The agitated confused patient is a medical emergency until proven otherwise — treat as for any acutely deteriorating patient.[1]
Time-critical reversible causes to exclude IMMEDIATELY (the "WHIMP" of confusion that will kill if missed): [1]
- Hypoxia — give oxygen to target SpO2 94 to 98 percent (88 to 92 percent in COPD/CO2 retainers); respiratory failure is a leading and treatable cause.
- Hypoglycaemia — check capillary glucose immediately. If below 4 mmol/L, give 15-20 g rapid carbohydrate (e.g. 100 mL of Lucozade, 200 mL orange juice, or IV 75 mL of 20 percent glucose / 150 mL of 10 percent glucose; in unconscious patient, IV 25 g of 50 percent glucose via large vein or 1 mg IM glucagon).
- Hypotension / septic shock — apply the Surviving Sepsis hour-1 bundle: blood cultures, lactate, broad-spectrum antibiotics within 1 hour, balanced crystalloid 30 mL/kg, noradrenaline for fluid-refractory shock; reassess fluid responsiveness (passive leg raise) before further boluses. (The UK Sepsis Six = oxygen, IV antibiotics, IV fluids, blood cultures, lactate, hourly urine output.)
- Raised intracranial pressure / structural lesion — signs of raised ICP (papilloedema, unilateral dilated pupil, Cushing's triad), focal deficit or head trauma → urgent CT brain, neurosurgical referral; elevate head of bed 30 degrees, maintain perfusion pressure.
- Status epilepticus (including non-convulsive) — IV lorazepam 4 mg (repeated once), then IV levetiracetam or phenytoin; obtain EEG. [1]
Safety while the cause is being hunted: [1]
- One-to-one nursing in a calm, well-lit single room; remove hazards; consider low bed/floor mats.
- De-escalation — calm voice, reorientation, presence of a familiar relative/carer.
- Avoid physical restraints wherever possible — they increase agitation, injury, immobility and pressure sores, and are associated with longer delirium. Use only as a last resort for imminent harm.
- Treat pain — uncontrolled pain drives delirium; paracetamol 1 g QDS oral/IV as baseline, with opioid sparing (regional techniques where possible). [1]
Management — Definitive & Stepwise
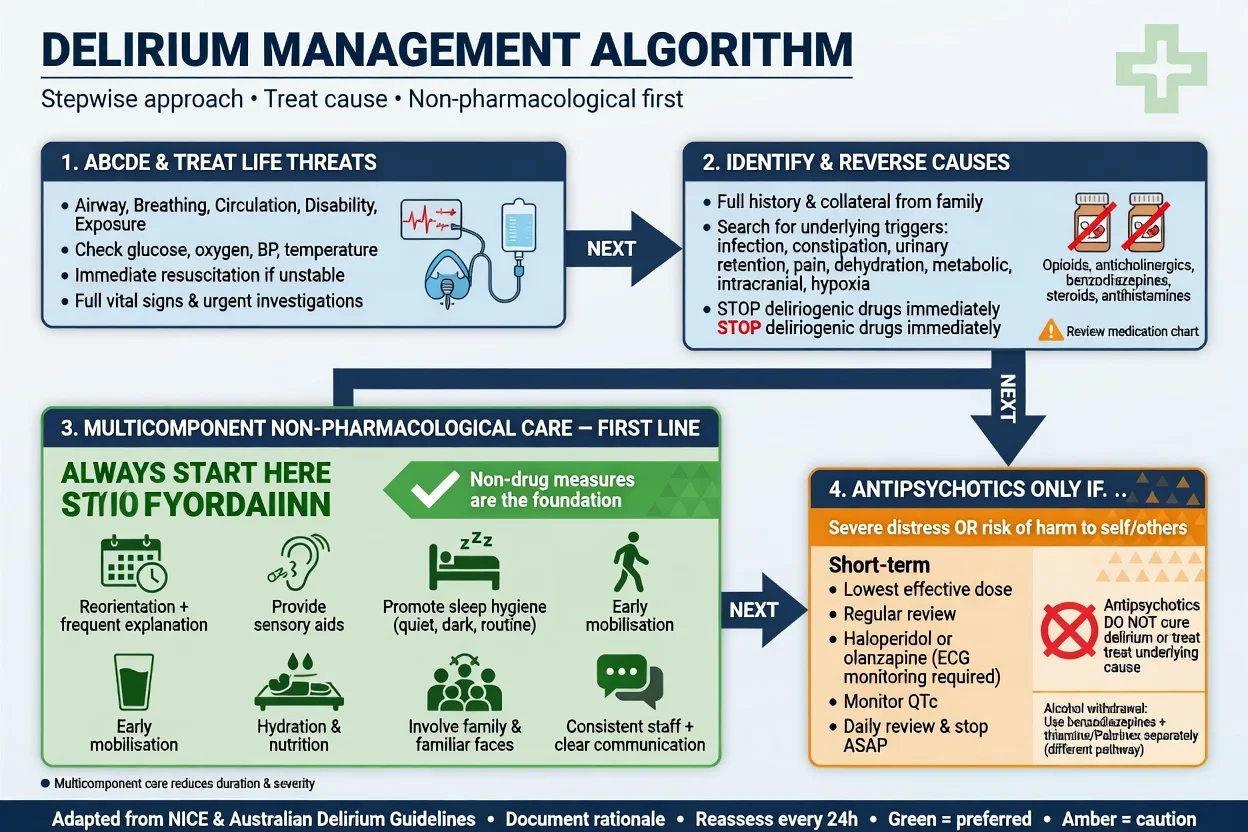
The overriding principle: delirium is a syndrome — find and treat every precipitant. Antipsychotics and sedatives are symptomatic and must never replace the search for the cause.[1]
Non-pharmacological care — FIRST-LINE for ALL patients
The Hospital Elder Life Program (HELP) multi-component bundle — the landmark evidence-based intervention (Inouye NEJM 1999) that reduced incident delirium by roughly 40 percent in hospitalised older adults. The core domains:[2]
Delirium prevention & treatment bundle
DELIRI
Review & deprescribe — stop anticholinergics, benzodiazepines, sedatives; minimise anticholinergic burden
Clock, calendar, familiar objects, photos; well-lit calm single room; family present; staff consistency
Encourage oral fluids; subcutaneous/IV if needed; monitor intake and dehydration
Treat UTI/pneumonia; remove catheter ASAP; bladder scan for retention; treat constipation
Repeated verbal reorientation; restore hearing aids and glasses (with working batteries!)
Early, frequent mobilisation; discourage daytime napping; preserve sleep-wake cycle
Additional first-line measures: [1]
- Pain control — regular paracetamol; opioid-sparing strategies; avoid as-needed-only analgesia.
- Oxygen if hypoxic.
- Sleep hygiene — minimise night-time observations/procedures, reduce noise and light at night, cluster care, treat pain and nocturia.
- Nutrition — assist with meals, dentures in, supplements if malnourished.
- Communication and family involvement — explain delirium, its fluctuating course and prognosis; family presence often calms the patient. [1]
Pharmacological therapy — RESERVED for severe agitation/distress
Pharmacological sedation is NOT routine. Reserve it for severe agitation, aggression or distress that endangers the patient (e.g. pulling at lines, falling out of bed) or others, AND that has not responded to non-pharmacological measures AND where the underlying cause is being actively sought and treated.[5][6]
Drug of choice — low-dose haloperidol: [1]
- Haloperidol 0.5 to 1 mg orally (or 0.5 mg intramuscularly in the elderly/agitated patient where oral route is not possible), repeated after 2 to 4 hours if required, titrated to the lowest effective dose.
- Maximum daily dose — caution in the elderly; typically do not exceed 5 mg/day in older adults without specialist input.
- IV route reserved for extreme emergency with ECG monitoring (QT-prolongation and torsade de pointes risk; IV haloperidol can prolong the QTc — avoid if QTc over 450 ms or with other QT-prolonging drugs).
- Mechanism — dopamine D2 receptor blockade; addresses the dopaminergic excess component.
- Cautions — extrapyramidal side effects, postural hypotension, anticholinergic effect of its own, QT prolongation and torsades, neuroleptic malignant syndrome, increased mortality in dementia (FDA black-box). [1]
Alternative atypical antipsychotics (when haloperidol contraindicated or for chronic use): [1]
- Risperidone 0.25 to 0.5 mg orally twice daily.
- Olanzapine 2.5 to 5 mg orally at night.
- Quetiapine 25 to 50 mg orally at night — preferred in Parkinson's disease or Lewy body dementia because it has the lowest dopaminergic blockade (see below).
- Note (MIND-USA trial, NEJM 2018): in critically ill ICU patients, antipsychotics (haloperidol, ziprasidone) did NOT improve delirium duration or outcomes vs placebo. This has reshaped practice: routine antipsychotic use for ICU delirium is not recommended; they remain symptomatic options for severe agitation only.[5]
Drugs to AVOID in delirium (memorise): [1]
- Benzodiazepines WORSEN delirium (GABA-ergic excess) — AVOID except: (i) alcohol or benzodiazepine withdrawal (lorazepam 1 to 2 mg PO/IM, or diazepam/chlordiazepoxide via symptom-triggered CIWA-Ar protocol); (ii) status epilepticus; (iii) specific toxin-related causes (e.g. anticholinergic overdose where physostigmine unavailable; cocaine/sympathomimetic toxicity).
- Anticholinergics — they precipitate and perpetuate delirium. [1]
Wernicke prophylaxis — give BEFORE glucose: in any patient with suspected alcohol misuse, malnutrition or ataxia/confusion of unclear cause, give IV thiamine (Pabrinex IV high-potency, 1 pair = thiamine 250 mg + other B vitamins) before any IV glucose. Glucose alone can precipitate Wernicke encephalopathy in a thiamine-deficient patient by accelerating thiamine depletion. Standard regimen: one pair IV OD for 3 to 5 days (high-risk: two pairs TDS for 2 days then one pair OD for 5 days), followed by oral thiamine. [1]
ICU-specific strategies — the PADIS 2018 ABCDEF bundle (Society of Critical Care Medicine):[6]
PADIS ABCDEF bundle for ICU delirium
ABCDEF
Use CPOT/BPS in non-verbal patients; treat pain adequately
Both spontaneous awakening trials AND spontaneous breathing trials (SAT + SBT) daily
Choice of analgesia and sedation — prefer analgesia-first, light sedation; minimise benzodiazepines
Delirium assessment and management — daily CAM-ICU; treat cause; mobilise
Early and progressive mobilisation/exercise — reduces delirium and weakness
Family engagement and empowerment — orient, reassure, involve in care
Dexmedetomidine — an alpha-2 agonist sedative that produces arousable sedation without significant respiratory depression and is associated with less ICU delirium than benzodiazepine-based regimens; recommended by PADIS as a preferred sedative in mechanically ventilated adults at risk of delirium.[6]
Specific Subtypes & Scenarios
-
Alcohol withdrawal and delirium tremens (DTs): tremulousness, anxiety, insomnia and autonomic hyperactivity (tachycardia, hypertension, fever) begin within 6 to 48 hours of cessation; generalised tonic-clonic seizures ("rum fits") at 6 to 48 h; delirium tremens at 48 to 72 h with vivid visual hallucinations, severe agitation, disorientation, marked autonomic storm — carries 5 to 15 percent mortality untreated. Management: benzodiazepines are first-line (the exception to the rule) — chlordiazepoxide or diazepam by symptom-triggered CIWA-Ar scale, or lorazepam in liver failure; thiamine (Pabrinex) before glucose; fluid and electrolyte correction (magnesium, potassium); treat in a quiet environment. This is the ONE delirium where benzodiazepines are the treatment. [1]
-
Postoperative delirium: affects 15 to 50 percent of older adults after major surgery (hip fracture, cardiac, vascular, prolonged procedures). Risk factors: age, baseline cognitive impairment, polypharmacy/anticholinergic burden, intraoperative hypotension/hypoxia, depth of anaesthesia, postoperative pain and opioids, infection, sleep disruption. Prevention is the most effective strategy (AGS 2015 best-practice): preoperative cognitive and medication review, avoid anticholinergics/benzodiazepines, regional anaesthesia/analgesia where possible, early mobilisation, orientation, family involvement, treat pain. No routine pharmacological prophylaxis is recommended.[7]
-
ICU delirium: the commonest — affects 50 to 80 percent of mechanically ventilated patients (detected with CAM-ICU daily). Independent predictor of longer ventilation, longer ICU/hospital stay, higher 6- and 12-month mortality, and long-term cognitive impairment ("post-intensive care syndrome"). PADIS 2018 strategies (ABCDEF bundle above) target prevention; dexmedetomidine-based sedation reduces incidence vs benzodiazepines. Routine antipsychotics do not improve outcomes (MIND-USA).[3][5][6]
-
Terminal / palliative delirium: very common in the last days of life; causes include hypoxia, metabolic failure, opioids, infection, dehydration. Reversible causes are still sought and treated; opioid rotation (e.g. morphine to fentanyl or methadone) reduces opioid-induced neurotoxicity (accumulating metabolites). Haloperidol is the symptomatic drug of choice for agitation/hallucinations. When delirium is irreversible in the actively dying patient, family communication and anticipatory symptom control are central. [1]
-
Drug-induced delirium — reversal by class:
- Opioid (miosis, sedation, respiratory depression) → naloxone 0.4-0.8 mg IV/IM titrated (caution in chronic users — avoid precipitating acute withdrawal/pain crisis).
- Benzodiazepine (sedation, ataxia) → flumazenil 0.2 mg IV over 15 s, repeated up to 1 mg total (caution: can precipitate seizures in chronic users/mixed overdose — use selectively, not routinely).
- Anticholinergic (dry, flushed, mydriasis, urinary retention, tachycardia) → supportive; physostigmine rarely used (risk of seizures/bradycardia), mainly in severe anticholinergic poisoning.
- Insulin/hypoglycaemic → glucose. [1]
-
Paediatric delirium: under-recognised; presents similarly with acute attention and awareness disturbance; common precipitants are infection, medication (opioids, benzodiazepines, anticholinergics), postoperative state, ICU admission. Screen with CAPD (Cornell Assessment of Pediatric Delirium). Same principles: find and treat cause; non-pharmacological first; low-dose antipsychotic for severe distress. [1]
Complications & Pitfalls
Direct complications of delirium:[1]
- Increased mortality — in-hospital mortality up to 25 percent in some series; doubled 6- and 12-month mortality in older adults; persistent increased risk for up to a year.
- Longer hospital and ICU stay, higher readmission rates, increased institutionalisation (care-home placement) at discharge.
- Persistent delirium at discharge in roughly 30 to 50 percent of patients; many take weeks to months to fully resolve, and some never do.
- Accelerated cognitive decline and increased risk of incident dementia — delirium is now understood as a two-way relationship with dementia.
- Falls, pressure sores, aspiration, malnutrition, dehydration, infections, venous thromboembolism from immobility and reduced intake.
- Psychological distress — patients often recall frightening hallucinations and experiences; post-traumatic stress symptoms are common, especially after ICU.
- Family distress, loss of confidence, caregiver burden. [1]
Iatrogenic complications of pharmacological sedation: [1]
- Falls and fractures from oversedation and postural hypotension.
- Aspiration pneumonia from depressed consciousness.
- Pressure sores and immobility-related complications.
- QT prolongation and torsade de pointes from haloperidol (especially IV and with other QT-prolonging drugs/electrolyte disturbance).
- Extrapyramidal side effects, akathisia, parkinsonism.
- Neuroleptic malignant syndrome (rare, life-threatening).
- Increased mortality in elderly patients with dementia (antipsychotics carry an FDA black-box warning). [1]
Classic pitfalls (examiner-favourite list): [1]
- Missing the diagnosis by labelling it "agitation", "confusion", "behavioural disturbance" or "dementia."
- Missing the HYPOACTIVE subtype — the quiet, withdrawn patient is overlooked until complications develop.
- Treating with sedatives without hunting for the cause — the single most dangerous error.
- Using a typical antipsychotic in Parkinson's disease or Lewy body dementia — risk of severe, sometimes fatal, neuroleptic sensitivity reaction (rigidity, hyperpyrexia, marked cognitive collapse). Use quetiapine or clozapine instead.
- Misattributing to alcohol withdrawal in a non-drinker, or missing alcohol withdrawal in a covert drinker.
- Missing Wernicke encephalopathy — always give thiamine before glucose in at-risk patients.
- Missing non-convulsive status epilepticus — obtain EEG in refractory or fluctuating confusion.
- Missing a structural lesion — subdural haematoma in an anticoagulated patient who has fallen.
- Giving IV haloperidol without ECG monitoring — QT prolongation can cause torsade.
- Over-reliance on sedatives, under-use of the HELP bundle. [1]
Prognosis & Disposition
Mortality: delirium is an independent predictor of death. In-hospital mortality is roughly 10 to 25 percent; 6-month mortality roughly doubles; risk persists for up to a year. ICU delirium predicts higher 6- and 12-month mortality even after adjusting for severity of illness.[1][3]
Cognitive trajectory: delirium does not always fully resolve. Roughly 30 to 50 percent have delirium at discharge; many take weeks to months to clear; a substantial minority never return to baseline. Delirium predicts accelerated decline in patients with dementia and new incident dementia in those without — it is both a marker and a driver of long-term cognitive loss. [1]
Predictors of poor outcome: older age, pre-existing dementia, hypoactive subtype, severity and duration of delirium, multiple precipitants, ICU admission, functional dependence, comorbidity, sensory deprivation, delayed recognition. [1]
Disposition: most delirium is managed on a general ward with a clear plan, one-to-one nursing if needed, and a daily review for resolution. Escalate to ICU if the patient has severe agitation unresponsive to measures and risks airway compromise, if the underlying precipitant requires critical care (septic shock, severe hypoxia, status epilepticus, raised ICP), or if monitoring/intensive nursing cannot be delivered on the ward. Discharge only when delirium has substantially resolved, the precipitant is treated, function is recovering, and a safe social and rehabilitation package is in place — premature discharge drives readmission and functional collapse. [1]
Special Populations
- Elderly — the highest-incidence group; presentation is often atypical (no fever, no agitation; falls, new incontinence, functional decline). Lower drug doses (start low, go slow — haloperidol 0.5 mg, not 5 mg); aggressive anticholinergic deprescribing; ensure sensory aids, hydration and mobility.
- Delirium superimposed on dementia — common, dangerous, and hard to diagnose. Any acute worsening of cognition or function in a dementia patient = delirium until proven otherwise; outcomes are worse than either alone.
- Parkinson's disease and dementia with Lewy bodies — typical antipsychotics are contraindicated (severe neuroleptic sensitivity with rigidity, hyperpyrexia, sometimes fatal). If pharmacological therapy is unavoidable, use quetiapine 25 to 50 mg orally (lowest D2 blockade) or clozapine under specialist supervision. Avoid haloperidol, risperidone and olanzapine.
- Postoperative / elective surgery — preoperative cognitive screening, medication review and anticholinergic deprescribing, regional anaesthesia and analgesia where possible, early mobilisation, family involvement.
- End-stage renal disease — uraemic encephalopathy (myoclonus, asterixis), dialysis disequilibrium, accumulation of renally cleared psychoactive drugs; dose-adjust all psychotropes.
- End-stage liver disease — hepatic encephalopathy (asterixis, constructional apraxia); precipitants (GI bleed, infection, constipation, electrolyte disturbance, sedatives); treat with lactulose (titrate to 2-3 soft stools/day) and rifaximin 550 mg BD.
- Pregnancy — delirium is rare but the same systematic search for precipitant applies; consider hypertensive encephalopathy (pre-eclampsia), sepsis, and thyrotoxicosis. Most psychotropes are relatively contraindicated — involve psychiatry and obstetric medicine. [1]
Evidence, Guidelines & Regional Differences
Landmark evidence (examiner-favourite): [1]
- Hospital Elder Life Program (HELP), Inouye NEJM 1999 (PMID 10053175) — a multicomponent targeted intervention (orientation, sensory aids, oral hydration, sleep enhancement, early mobilisation) reduced incident delirium by roughly 40 percent in hospitalised older adults; remains the cornerstone of prevention.[2]
- MIND-USA, Girard NEJM 2018 (PMID 30346242) — randomised trial of haloperidol, ziprasidone and placebo in critically ill ICU patients with delirium; no difference in delirium/coma-free days. Reshaped practice away from routine antipsychotic use for ICU delirium.[5]
- CAM-ICU validation, Ely JAMA 2001 (PMID 11730446) — established the validity and reliability of the CAM-ICU in mechanically ventilated patients, enabling routine daily delirium screening in ICU.[3]
- 4AT validation, Bellelli Age Ageing 2014 (PMID 24590568) — validated a rapid, no-equipment delirium screen suitable for ward and emergency department use.[4]
Guidelines: [1]
- SCCM PADIS 2018 (Devlin, Crit Care Med 2018, PMID 30113379) — the authoritative ICU guideline; recommends the ABCDEF bundle, light sedation, analgesia-first, dexmedetomidine over benzodiazepines, daily delirium screening, early mobility; recommends AGAINST routine antipsychotic prophylaxis or treatment of ICU delirium.[6]
- American Geriatrics Society 2015 Best Practice Statement (PMID 25535170) — postoperative delirium in older adults; endorses multicomponent non-pharmacological prevention; recommends AGAINST prophylactic antipsychotics.[7]
DSM-5-TR vs ICD-11: DSM-5-TR retains the five elements above; ICD-11 uses "Delirium" as a neurocognitive syndrome with essentially the same clinical features (disturbance of attention/awareness, acute onset, fluctuating, with cognitive impairment, due to a medical/substance cause), organised under "Delirium" with subcategories by cause. [1]
Controversies: (1) whether any pharmacological agent can prevent or shorten delirium — prophylactic antipsychotics are not recommended; dexmedetomidine shows promise in ICU prevention and treatment of hyperactive delirium. (2) Whether cholinesterase inhibitors help — not supported. (3) The exact causal relationship between delirium and long-term dementia (cause, unmasking, or shared substrate). [1]
Exam Pearls
- Acute + fluctuating + inattention = DELIRIUM. Chronic + progressive + intact attention = DEMENTIA. This one line answers half of all delirium MCQs.
- Commonest precipitant in the elderly = INFECTION (UTI and pneumonia); then drugs, dehydration, hypoxia, metabolic, surgery.
- Highest-yield drug precipitants = OPIOIDS, BENZODIAZEPINES, ANTICHOLINERGICS (+ corticosteroids, dopaminergics).
- CAM — features 1 AND 2 AND (3 OR 4): (1) acute onset + fluctuating, (2) inattention, (3) disorganised thinking, (4) altered consciousness.
- 4AT — score 4 or more = delirium.
- Core pathophysiology = central ACETYLCHOLINE DEFICIENCY + DOPAMINE EXCESS — explains anticholinergic precipitation AND antipsychotic response.
- Haloperidol 0.5 to 1 mg PO/IM for severe agitation; avoid IV without ECG (QT prolongation, torsades).
- BENZODIAZEPINES WORSEN DELIRIUM — except alcohol/benzodiazepine withdrawal and seizures. This is the most-tested exception.
- Hypoactive delirium is missed and carries the WORST prognosis.
- EEG of delirium = generalised theta/delta slowing; NCSE = focal/3-Hz spike-wave.
- Visual hallucinations predominate in delirium (vs auditory in schizophrenia).
- Wernicke triad = confusion + ataxia + ophthalmoplegia/nystagmus — give IV thiamine BEFORE glucose.
- NEVER give a typical antipsychotic in Parkinson's or Lewy body dementia — use quetiapine.
- MIND-USA (2018): antipsychotics do NOT improve outcomes in ICU delirium — do not use routinely.
- HELP (Inouye 1999): multi-component non-pharmacological bundle reduced delirium by ~40 percent.
- Mortality of delirium: up to 25 percent in-hospital; doubled at 6 months.
- Delirium is a SYNDROME — never a final diagnosis. Always find and treat the precipitant.
- Sundowning = worsening of confusion at night.
- Check capillary glucose FIRST in every confused patient.
- Disorientation order in delirium: time, then place, then person (person is last to go). [1]
Exam application bank (NEET-PG / INICET)
One-line answer
Delirium is an acute, fluctuating disturbance of attention and awareness caused by a medical condition, substance intoxication or withdrawal, medication, toxin exposure, or multiple factors (DSM-5). It is a medical emergency and a marker of acute brain dysfunction, carrying an in-hospital mortality that can reach 25 percent and a doubled 6-month mortality in older adults. The commonest precipitants in the elderly are infection (UTI, pneumonia), drugs (opioids, benzodiazepines, anticholinergics), dehydration, metabolic/electrolyte disturbance, hypoxia, uncontrolled pain, surgery, constipation and urinary retention. Diagnosis is clinical using the Confusion Assessment Method (CAM) — acute onset with fluctuation AND inattention AND (disorganised thinking OR altered level of consciousness). The overriding management principle is to find and treat the precipitant; non-pharmacological multi-co
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Delirium.
References
- [1]Inouye SK. Delirium in older persons N Engl J Med, 2006.PMID 16540616
- [2]Inouye SK, Bogardus ST, Charpentier PA, et al. A multicomponent intervention to prevent delirium in hospitalized older patients N Engl J Med, 1999.PMID 10053175
- [3]Ely EW, Inouye SK, Bernard GR, et al. Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU) JAMA, 2001.PMID 11730446
- [4]Bellelli G, Morandi A, Davis DHJ, et al. Validation of the 4AT, a new instrument for rapid delirium screening: a study in 234 hospitalised older people Age Ageing, 2014.PMID 24590568
- [5]Girard TD, Exline MC, Carson SS, et al. Haloperidol and Ziprasidone for Treatment of Delirium in Critical Illness N Engl J Med, 2018.PMID 30346242
- [6]Devlin JW, Skrobik Y, Gelinas C, et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU Crit Care Med, 2018.PMID 30113379
- [7]American Geriatrics Society Expert Panel on Postoperative Delirium in Older Adults. Postoperative delirium in older adults: best practice statement from the American Geriatrics Society J Am Coll Surg, 2015.PMID 25535170