Neurology · General Medicine
Raised Intracranial Pressure
Also known as Raised intracranial pressure · Intracranial hypertension · ICP · Idiopathic intracranial hypertension · IIH · Pseudotumour cerebri
Raised intracranial pressure (ICP) occurs when the volume of brain, blood or CSF exceeds the rigid skull's capacity (Monro-Kellie doctrine). Normal ICP is 5 to 15 mmHg in a supine adult; in traumatic brain injury, ICP over 22 mmHg defines raised ICP and warrants treatment. Causes include space-occupying lesions (tumour, haematoma, abscess), hydrocephalus (obstructive and communicating), cerebral oedema (vasogenic, cytotoxic, osmotic), traumatic brain injury, cerebral venous sinus thrombosis and idiopathic intracranial hypertension (IIH). Presentation: headache (worse on waking, coughing, bending), nausea and vomiting, papilloedema, altered consciousness, and the Cushing triad (bradycardia, hypertension, irregular respiration — a pre-terminal sign). The four herniation syndromes — uncal, central, tonsillar (coning), and subfalcine — are the feared complications. Cerebral perfusion pressure (CPP) = MAP minus ICP; target CPP 60 to 70 mmHg. Management: head up 30 degrees, normocapnia (PaCO2 4.0 to 5.0 kPa), mannitol 0.5 to 1 g/kg or 3 percent hypertonic saline, dexamethasone for vasogenic oedema, treat the cause; refractory: induced coma, decompressive craniectomy. IIH (young obese women; headache, papilloedema, visual loss; normal MRI/MRV; LP opening pressure over 25 cmH2O) is treated with weight loss, acetazolamide 1 to 2 g/day, and CSF shunting or optic nerve sheath fenestration if vision is threatened.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Overview & Definition
Raised intracranial pressure is a neurological emergency and one of the most high-yield topics in clinical medicine. The skull is a rigid, unyielding container, so any increase in the volume of its three contents — brain tissue, blood, and cerebrospinal fluid — raises the pressure inside. Normal intracranial pressure is 5 to 15 mmHg in a supine adult (equivalent to about 7 to 20 cmH2O). In children the normal range is lower, about 1.5 to 10 mmHg, and in infants under 5 mmHg because the open fontanelles and unfused sutures provide additional compliance. Raised ICP is generally defined as a sustained pressure over 20 mmHg in adults and over 15 mmHg in children; in traumatic brain injury the Brain Trauma Foundation 4th edition sets the treatment threshold at over 22 mmHg.[1][5]
As pressure climbs, cerebral perfusion pressure falls (CPP equals MAP minus ICP), the brain is starved of blood, and ultimately the brain substance is forced from one intracranial compartment to another — herniation. The most catastrophic form is tonsillar herniation (coning), in which the cerebellar tonsils are forced through the foramen magnum, compressing the medulla and causing respiratory arrest and death. The clinical discipline is to recognise the signs early (headache pattern, papilloedema, falling consciousness), image urgently with non-contrast CT, reduce the pressure (head elevation, osmotic agents, treat the cause), and prevent herniation. A single bedside error — performing a lumbar puncture before imaging, or missing a falling GCS — can convert a salvageable patient into a brainstem-dead one.[1]
Classification
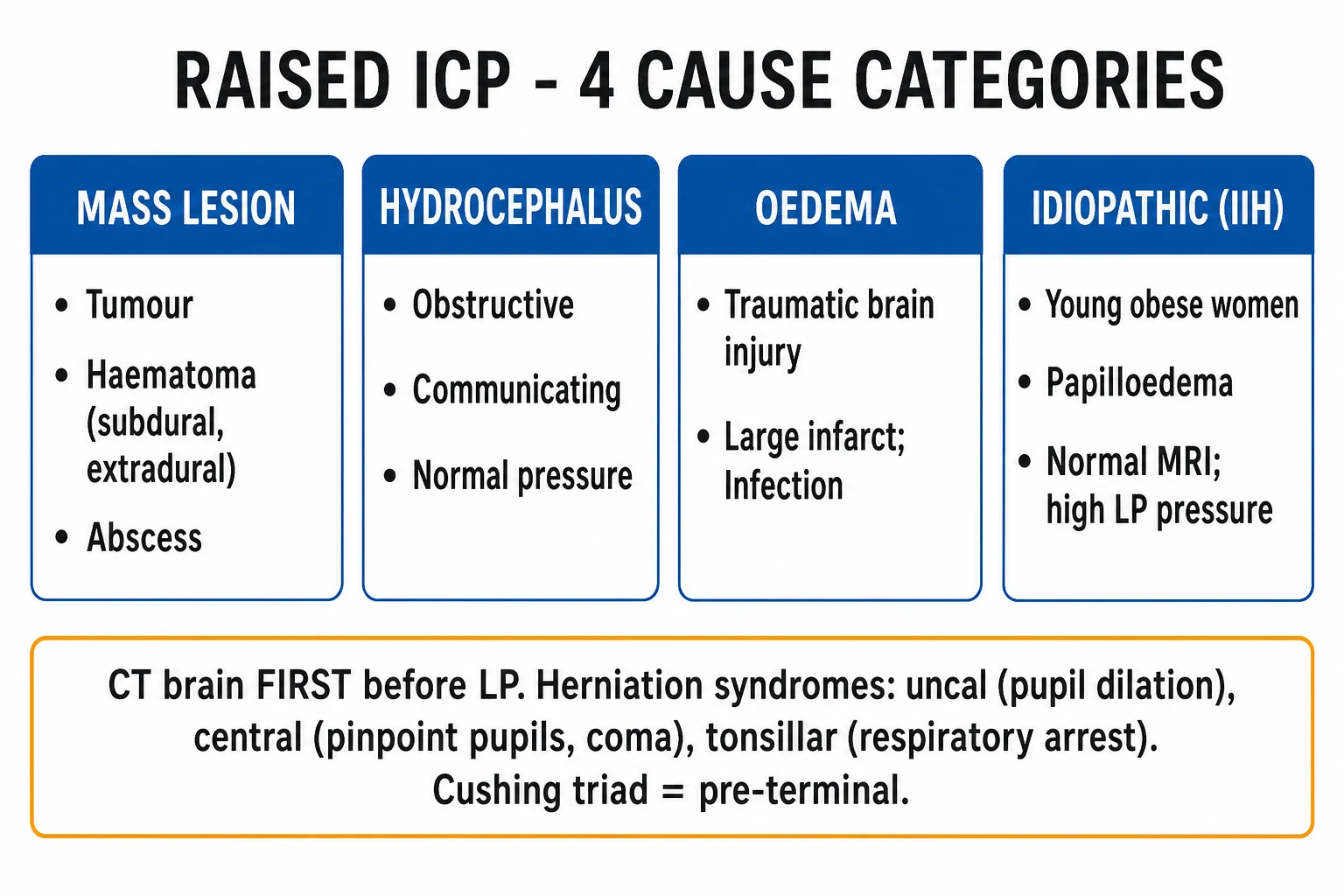
Raised ICP is classified by two axes: the mechanism that increases intracranial volume, and the anatomical herniation syndrome the raised pressure ultimately produces. The Monro-Kellie doctrine is the unifying principle — the skull's total volume is fixed, so an increase in one component (brain, blood, or CSF) must be offset by a decrease in another, until compensation is exhausted and pressure rises steeply. By mechanism, the causes fall into discrete groups: a space-occupying mass (tumour, haematoma, abscess) that adds volume directly; hydrocephalus (obstructive or communicating) where excess CSF accumulates; cerebral oedema (vasogenic, cytotoxic, osmotic, or interstitial) that swells the brain parenchyma; venous outflow obstruction (cerebral venous sinus thrombosis) that increases cerebral blood volume; and idiopathic intracranial hypertension, where no structural cause is found.[1][2]
Mass lesion
- Tumour (glioma, metastasis, meningioma), haematoma (extradural, subdural, intracerebral), abscess
- Focal neurological signs, midline shift on CT
- Definitive: evacuate or resect; dexamethasone for surrounding vasogenic oedema
Hydrocephalus
- Obstructive (aqueduct stenosis, posterior fossa tumour, fourth ventricle outflow) vs communicating (post-SAH, post-meningitis)
- Ventriculomegaly on imaging; gait disturbance, dementia, incontinence in chronic
- Definitive: EVD, VP shunt, or endoscopic third ventriculostomy
Oedema / vascular
- Vasogenic (tumour or abscess), cytotoxic (infarct or TBI), osmotic (hyponatraemia rapid correction), interstitial (hydrocephalus)
- Cerebral venous sinus thrombosis in young women
- Osmotherapy; dexamethasone for vasogenic only; anticoagulate venous thrombosis
Idiopathic (IIH)
- Young obese women of reproductive age, normal neuroimaging
- High LP opening pressure over 25 cmH2O, normal CSF composition
- Weight loss plus acetazolamide; surgery if vision threatened
Cerebral oedema subtypes
Cerebral oedema — excess fluid in brain tissue — is itself a major cause of raised ICP and comes in four pathophysiological varieties that the examiner distinguishes deliberately. Vasogenic oedema follows disruption of the blood-brain barrier: fluid and plasma proteins leak into the extracellular space, classically around a brain tumour, abscess, or metastasis, and it is steroid-responsive (dexamethasone tightens the barrier). Cytotoxic (cellular) oedema results from intracellular swelling after failure of the sodium-potassium pump — the hallmark of ischaemic stroke, hypoxia, and severe traumatic brain injury — and is not steroid-responsive. Osmotic oedema occurs when plasma osmolality drops rapidly (for example, severe hyponatraemia or rapid correction, dialysis disequilibrium) and water shifts into the brain along the osmotic gradient. Interstitial (hydrocephalic) oedema is the transependymal migration of CSF into the periventricular white matter in obstructive hydrocephalus, producing the classic "halo" or "transependymal ooze" on imaging.[1]
Epidemiology & Risk Factors
The epidemiology of raised ICP is the epidemiology of its causes, because raised ICP is a syndrome rather than a single disease. In emergency practice, traumatic brain injury is the commonest cause — severe TBI (GCS 3 to 8) produces raised ICP in over 50 percent of patients, and uncontrolled intracranial hypertension carries roughly 50 percent mortality. In neurosurgical series, brain tumours (glioblastoma, metastases) and hydrocephalus dominate; in paediatric practice, congenital hydrocephalus (aqueduct stenosis, Dandy-Walker malformation, myelomeningocele with Chiari II) and intraventricular haemorrhage of prematurity are the leading causes. [1]
Idiopathic intracranial hypertension has a striking demographic: the classical patient is a young, obese woman of reproductive age (the 20 to 45 year bracket). The incidence in the general population is about 1 per 100,000, but it rises to 19 per 100,000 in obese women of childbearing age and climbs further with increasing body mass index. Obesity is the dominant modifiable risk factor, and weight loss of 5 to 10 percent is the single most effective treatment. Drug precipitants of IIH include tetracyclines (doxycycline, minocycline), vitamin A and retinoids (isotretinoin, excess retinol, hypervitaminosis A), combined oral contraceptive pill, lithium, growth hormone, anabolic steroids, and steroid withdrawal. Secondary risk groups include patients with severe TBI, large middle cerebral artery infarct (which undergoes malignant swelling at 24 to 72 hours), intracerebral or subdural haematoma (especially in the anticoagulated and elderly), cerebral venous sinus thrombosis (young women, prothrombotic states), and severe meningitis or encephalitis.[1][2]
Age shapes the differential: in infants, hydrocephalus and congenital malformations predominate; in children, posterior fossa tumours (medulloblastoma, ependymoma, pilocytic astrocytoma); in young adults, IIH, venous sinus thrombosis, and trauma; in the elderly, subdural haematoma, metastases, and the secondary effects of stroke. [1]
Pathophysiology
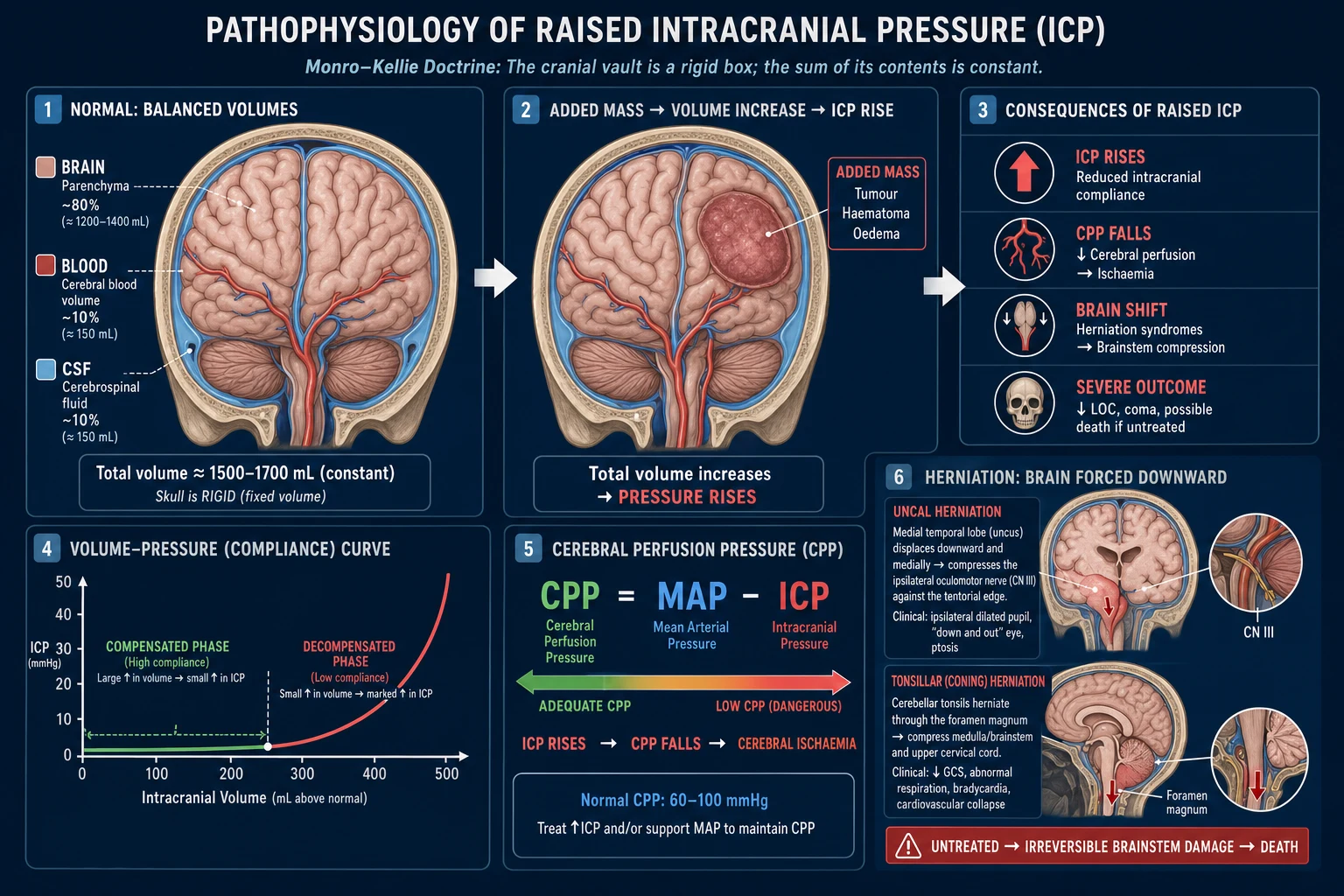
The Monro-Kellie doctrine, first articulated by Alexander Monro and George Kellie in the 18th century, is the conceptual key to everything that follows. The rigid, unyielding skull holds a fixed total volume made up of three incompressible components: brain parenchyma about 80 percent, intracranial blood about 10 percent, and cerebrospinal fluid about 10 percent. Because the total volume cannot change, any increase in one component must be offset by an equal decrease in another — or pressure must rise. Early on, a growing mass or accumulating oedema is buffered by displacement of CSF from the cranial vault into the spinal subarachnoid space and displacement of venous blood out of the cranium into the extracranial venous system. During this compensated phase the ICP stays nearly flat, which is why a patient with a slow-growing meningioma can have a massive tumour and a normal pressure.[1]
Once this compliance reserve is exhausted, the intracranial volume-pressure curve turns steep — small further volume increases now cause a dangerous, exponential pressure spike. This is the point of decompensation, and it explains the clinical tempo: a patient who was stable for weeks may deteriorate over hours once the curve's flat portion is spent. The curve also explains why anything that transiently increases intracranial blood volume (coughing, straining, hypercapnia, seizures, agitation) can tip a compensated patient into crisis. [1]
As ICP climbs, cerebral perfusion pressure falls — CPP equals MAP minus ICP — and once CPP drops below about 60 mmHg the brain becomes ischaemic. Cerebral autoregulation, which normally holds cerebral blood flow constant across a wide range of mean arterial pressures (MAP 50 to 150 mmHg) by adjusting arteriolar calibre, fails in the injured brain — perfusion then passively follows pressure, so hypotension becomes directly injurious. This is why maintaining CPP at 60 to 70 mmHg is a treatment target in neurocritical care: too low risks ischaemia, too high risks worsening oedema and haemorrhage.[1][5]
Several factors worsen raised ICP by increasing cerebral blood volume or metabolic demand: hypercapnia causes cerebral vasodilation; hypoxia and fever raise cerebral metabolic rate and blood flow; seizures massively increase metabolic demand; agitation and pain raise sympathetic tone and venous pressure. Each of these converts into a treatment principle — maintain normocapnia, normoxia, normothermia, give analgesia and sedation, and prophylax or treat seizures. [1]
Raised ICP — key numbers
The herniation syndromes — the end-game of uncontrolled ICP
Herniation is the displacement of brain tissue from one intracranial compartment to another through the rigid dural partitions (falx cerebri and tentorium cerebelli) or the foramen magnum. It is the mechanism by which raised ICP kills, and each syndrome produces a recognisable clinical pattern.[1]
Uncal herniation is the commonest and most examinable. The medial temporal lobe (uncus) is forced downward through the tentorial hiatus and compresses, in sequence, the ipsilateral oculomotor (third) nerve (causing a progressively dilating, then fixed and dilated, pupil on the same side) and the ipsilateral cerebral peduncle (causing contralateral hemiparesis). The combination of an ipsilateral fixed dilated pupil with contralateral hemiparesis is the classic bedside signature. Occasionally, the contralateral cerebral peduncle is compressed against the opposite tentorial edge, producing ipsilateral hemiparesis (Kernohan's notch phenomenon) — a false-localising sign that can mislead the unwary. Uncal herniation is a lateral mass phenomenon (typically a temporal lobe haematoma or tumour). [1]
Central (transtentorial) herniation is a more symmetrical, axial downward shift of the diencephalon and brainstem through the tentorial hiatus — the result of diffuse bilateral pressure (generalised oedema, large bilateral masses). It compresses the brainstem in stages: the diencephalon first (small reactive pupils, drowsiness), then the midbrain and pons (midposition fixed pupils 3 to 5 mm, decorticate then decerebrate posturing), then the medulla (irregular breathing, respiratory arrest). Diabetes insipidus may appear from hypothalamic-pituitary compression. [1]
Tonsillar herniation (coning) is the most feared: the cerebellar tonsils are forced downward through the foramen magnum and compress the medulla, producing respiratory arrest, loss of consciousness, and death within minutes. It is the mechanism by which a lumbar puncture performed in the presence of raised ICP can kill the patient — removing CSF pressure from below creates a cranial-to-spinal pressure gradient that sucks the tonsils down into the foramen. This is the rationale for CT before LP. [1]
Subfalcine (cingulate) herniation is the displacement of the cingulate gyrus under the falx cerebri, compressing the anterior cerebral artery against the rigid falx and producing contralateral leg weakness (an ACA-territory ischaemic deficit). It is often the earliest herniation syndrome with a frontal mass. [1]
Upward (cerebellar) herniation is upward displacement of the cerebellum through the tentorial hiatus, seen with posterior fossa masses; it compresses the midbrain and obstructs the cerebral aqueduct, and it can be precipitated by a ventricular shunt that drains the supratentorial ventricles faster than it relieves a posterior fossa mass. [1]
The Cushing triad (hypertension with widened pulse pressure, bradycardia, and irregular breathing) is the medullary response to critical brainstem ischaemia: sympathetic discharge raises blood pressure (the widened pulse pressure is the clue), the baroreceptor reflex produces a secondary vagal bradycardia, and direct brainstem compression produces irregular (Cheyne-Stokes or ataxic) respiration. It is a late, pre-terminal sign present in only a minority of cases — its absence never excludes raised ICP.[1]
The herniation syndromes — UCTS-U
UCTSU
temporal lobe under tentorium — ipsilateral fixed dilated pupil (CN III), contralateral hemiparesis
axial transtentorial — pinpoint to midposition pupils, posturing, coma, DI
coning through foramen magnum — medullary compression, respiratory arrest, death
cingulate under falx — ACA compression, contralateral leg weakness
cerebellar — posterior fossa mass compressing midbrain; shunt-induced
Clinical Presentation
The cardinal quartet of raised ICP is headache, vomiting, papilloedema, and altered consciousness — but the tempo, pattern, and individual signs vary with the cause and the patient's age, and the examiner tests the corners. [1]
Headache is the cardinal symptom and has a characteristic pattern: it is worse on waking (having been lying flat all night raises cerebral venous pressure), worsened by coughing, sneezing, bending forward or straining at stool (each transiently raises intrathoracic and hence intracranial venous pressure), and progressive over days to weeks rather than episodic. It may be relieved by vomiting (which briefly lowers pressure) and by standing up. The headache is often bifrontal or generalised. Contrast this with tension headache (bilateral, pressing, worse at the end of the day, no papilloedema), migraine (throbbing, photophobic, phonophobic, builds over hours with aura, relieved by sleep), and cluster headache (unilateral periorbital, excruciating, lacrimation and nasal congestion, in bouts lasting weeks). A sudden thunderclap headache reaching maximum intensity within seconds to one minute suggests subarachnoid haemorrhage, not gradual raised ICP.[1]
Vomiting in raised ICP is classically effortless and unexpected — not preceded by nausea — because it arises from direct compression of the vomiting centre in the medulla rather than from gastrointestinal stimulation. Projectile vomiting is a classic paediatric sign. [1]
Papilloedema is the most specific sign of raised ICP but is frequently absent in acute presentations (it takes hours to days to develop as axoplasmic flow is obstructed at the optic nerve head). Fundoscopy shows, in sequence, loss of spontaneous venous pulsations (the earliest sign), blurring of the disc margins (starting at the superior and inferior poles), elevation of the disc, and finally flame haemorrhages and cotton-wool spots in advanced chronic papilloedema. Acutely, the fundus may be entirely normal — a normal fundus never excludes raised ICP. [1]
Altered consciousness ranges from subtle cognitive slowing and irritability through drowsiness to deep coma. The Glasgow Coma Scale must be documented and trended serially — a falling score, especially a drop of two or more points, is an emergency demanding immediate imaging and escalation. [1]
The Cushing triad — hypertension with widened pulse pressure, bradycardia, and irregular respiration — is a late, pre-terminal sign of brainstem herniation. It is present in only about a third of cases of fatal raised ICP, so its absence never excludes raised ICP. It demands immediate action, not observation.[1]
At the bedside, uncal herniation declares itself with an ipsilateral fixed dilated pupil (third-nerve compression) and contralateral hemiparesis (cerebral peduncle compression). The asymmetry localises the lesion. Beware Kernohan's notch — compression of the contralateral peduncle producing ipsilateral hemiparesis, a false-localising sign. Subfalcine herniation presents with contralateral leg weakness from anterior cerebral artery compression. Central herniation produces bilateral pinpoint to midposition fixed pupils, posturing (decorticate then decerebrate), and coma. Tonsillar herniation (coning) presents with sudden respiratory arrest and loss of consciousness — the patient may have been talking moments before. [1]
Atypical presentations
The examiner tests atypical presentations deliberately. In the elderly, cerebral atrophy increases intracranial compliance, so a chronic subdural haematoma or slow-growing tumour may reach enormous size before producing symptoms — presentation is later and subtler, often as cognitive change, falls, anorexia, or a fluctuating conscious level rather than classical headache. In children, especially pre-verbal children, the signs are irritability, lethargy, head tilt (a compensatory posture to relieve pressure), vomiting, and in infants a bulging fontanelle and sunset sign (the eyes are driven downward, exposing the sclera above the iris, from pressure on the tectal plate). In pregnancy, IIH is commoner; the differential includes pre-eclampsia and eclampsia (hypertension, proteinuria, seizures) and cortical vein thrombosis.[2]
The IIH pattern is distinctive: a young obese woman with daily headache, transient visual obscurations (lasting seconds, often on bending forward, due to momentary optic nerve head ischaemia), pulsatile tinnitus (venous turbulence from raised venous pressure), diplopia from a sixth-nerve palsy (a false-localising sign from traction on the long, vulnerable sixth nerve as the brain shifts), and progressive visual field loss on perimetry. The main risk is permanent blindness from chronic optic atrophy. [1]
Differential Diagnosis
The differential diagnosis of a possible raised ICP presentation divides into other causes of headache, other causes of optic disc swelling, and other causes of acute coma. [1]
Migraine / tension / cluster / MOH
- No papilloedema, no progressive morning pattern
- Migraine: throbbing, photophobia, aura, hours; cluster: unilateral periorbital, lacrimation, bouts
- Medication-overuse: analgesic intake 15-plus days/month; improves on withdrawal
Meningitis / encephalitis
- Fever, meningism (neck stiffness, photophobia, Kernig sign)
- Raised ICP may coexist; CSF and systemic features dominate
- CT before LP if any focal sign, papilloedema, or reduced consciousness
Subarachnoid haemorrhage
- Sudden thunderclap maximum-intensity headache, worst of life
- Meningism, sentinel bleed on CT; CT sensitivity falls after 6 hours
- LP for xanthochromia if CT negative and over 6 hours
Other optic disc swelling
- Papillitis: pain on eye movement, EARLY visual loss
- CRVO: flame haemorrhages in all four quadrants
- Pseudopapilloedema (drusen): no vessel obscuration, spontaneous venous pulsations preserved
The distinction between IIH and a posterior fossa tumour causing obstructive hydrocephalus is critical and the reason MRI/MRV is mandatory before diagnosing IIH — a posterior fossa mass produces identical headache and papilloedema but imaging reveals the tumour and ventriculomegaly. Among causes of acute coma with a normal CT, consider hepatic or metabolic encephalopathy, post-ictal state (especially non-convulsive status epilepticus), intoxication (alcohol, opioids, benzodiazepines), sepsis, and hypertensive encephalopathy — each demands its own urgent pathway rather than neurosurgery.[1]
Clinical & Bedside Assessment
The focused neurological examination in suspected raised ICP has a single purpose: detect the dangerous signs that demand immediate imaging and escalation. [1]
- Glasgow Coma Scale — document and trend serially at least hourly. A falling score, especially a drop of two or more points, is an emergency. Reproduce the components: Eyes 1 to 4 (opens spontaneously, to speech, to pain, none), Verbal 1 to 5 (orientated, confused, inappropriate words, incomprehensible sounds, none), Motor 1 to 6 (obeys commands, localises pain, withdraws, abnormal flexion, abnormal extension, none); range 3 to 15. Intubate at GCS 8 or less (the airway is at risk).
- Fundoscopy — look for blurred disc margins (starting superiorly and inferiorly), loss of spontaneous venous pulsations, disc elevation, then flame haemorrhages. Acute raised ICP may have a normal fundus, so a normal fundus never rules it out.
- Pupils — size and reactivity. A unilateral fixed dilated pupil (over 4 mm and unresponsive to light) localises to uncal herniation on that side until proven otherwise. Bilateral midposition fixed pupils (3 to 5 mm) suggest central herniation; bilateral pinpoint pupils suggest pontine lesion or opiates.
- Motor and focal exam — assess for hemiparesis, Babinski sign, reflex asymmetry, and a focal deficit pointing to a mass lesion. Note that uncal herniation typically produces contralateral hemiparesis, but Kernohan's notch can produce ipsilateral hemiparesis.
- Vital signs — look for the Cushing triad: rising blood pressure with widened pulse pressure, falling pulse (bradycardia), and irregular breathing. Also document temperature (fever worsens ICP).
- Transorbital ultrasound — an optic nerve sheath diameter over 5.0 to 5.8 mm measured 3 mm behind the globe is a rapid, non-invasive bedside surrogate for raised ICP with reasonable sensitivity, useful in the emergency department or ICU when CT is being arranged.
- False-localising sixth-nerve palsy — the abducens nerve has a long intracranial course and is tethered at the petroclinoid ligament; as the brain shifts with raised ICP the nerve is stretched, producing a unilateral or bilateral lateral rectus palsy with horizontal diplopia. It does not localise the lesion — hence "false-localising" — and is one of the modified Dandy criteria allowed in IIH. [1]
Investigations
Non-contrast CT brain — the FIRST and urgent test
The non-contrast CT brain is the first investigation in any patient with suspected raised ICP. It is fast, widely available, and answers the critical questions: is there a mass lesion, a haematoma, hydrocephalus, midline shift, or effacement of the basal cisterns? Time is critical because the CT result determines the next action — neurosurgery, an LP (if safe), or further imaging. CT features of raised ICP and impending herniation include midline shift (over 5 mm is significant), effacement of the basal cisterns (the ambient, quadrigeminal, and suprasellar cisterns — effacement is a danger sign of impending herniation), loss of grey-white matter differentiation (a sign of cytotoxic oedema and ischaemia), compression of the ventricles (slit-like in diffuse swelling) or ventriculomegaly (in hydrocephalus), and a visible mass (tumour, haematoma, abscess).[1]
MRI brain with MRV
MRI is second-line for detail — posterior fossa lesions (better visualised without bone artefact than CT), small tumours, and cerebral venous sinus thrombosis on MR venography. In IIH workup, MRI/MRV is mandatory to exclude a venous sinus thrombosis or a posterior fossa mass before the diagnosis of idiopathic can be made. MRV shows absent or irregular venous sinus flow in thrombosis. [1]
Lumbar puncture — contraindicated before imaging
Lumbar puncture is contraindicated before imaging in any patient with suspected raised ICP because of the risk of tonsillar herniation (coning) — removing CSF pressure from below creates a cranial-to-spinal pressure gradient that can force the cerebellar tonsils through the foramen magnum. The exceptions to "CT before LP" are: suspected meningococcal disease in a febrile patient with a non-blanching rash (give antibiotics immediately, do not delay for imaging) and the immunocompromised patient where the threshold for imaging is even lower. [1]
In IIH, after a normal CT/MRI, the lumbar puncture is both diagnostic and therapeutic: measure the opening pressure (in the lateral decubitus position with legs relaxed, not flexed, to avoid falsely elevating pressure). Opening pressure over 25 cmH2O in adults (over 28 cmH2O in children) confirms raised ICP; the CSF composition must be normal (cells, protein, glucose). Removing 20 to 30 mL of CSF can relieve the headache temporarily.[2]
Modified Dandy criteria for IIH
The modified Dandy criteria establish the diagnosis of idiopathic intracranial hypertension and exclude mimics: (1) signs and symptoms of raised ICP (headache, papilloedema, visual obscurations); (2) no localising neurological signs except a unilateral or bilateral sixth-nerve palsy (false-localising); (3) raised CSF opening pressure over 25 cmH2O (adults) with normal CSF composition (no cells, normal protein and glucose); (4) normal neuroimaging — no mass, no hydrocephalus, no venous sinus thrombosis on MRI/MRV. All four must be satisfied; a posterior fossa tumour or venous thrombosis is a "secondary" cause, not IIH.[2]
Invasive ICP monitoring
Invasive ICP monitoring is indicated in severe traumatic brain injury (GCS 3 to 8) with an abnormal CT, or a normal CT with two or more of: age over 40, unilateral or bilateral motor posturing, systolic BP under 90 mmHg. The intraventricular catheter (external ventricular drain, EVD) is the gold standard — it measures pressure directly and also allows therapeutic CSF drainage; its disadvantages are invasiveness, infection risk (ventriculitis), and difficulty placing it in a small or compressed ventricle. The intraparenchymal fibre-optic probe (Camino, Codman) is easier to place, has lower infection risk, but cannot drain CSF and may drift. Modern multimodal monitoring adds brain tissue oxygenation (PbtO2), microdialysis (lactate-pyruvate ratio for ischaemia), and continuous EEG.[5]
Bloods
Routine bloods include glucose, urea and electrolytes, liver function, coagulation screen (before any neurosurgical procedure), full blood count and CRP (infection), and a drug or toxin screen if the cause of coma is unexplained. In the anticoagulated patient, check the INR or anti-Xa level urgently. [1]
Management — Resuscitation
The emergency bundle treats the secondary brain injury while the underlying cause is identified and definitively fixed. The guiding aim is to lower ICP and protect CPP — every intervention either reduces intracranial volume or supports cerebral perfusion. The targets are: avoid hypotension (keep systolic BP over 110 mmHg; maintain CPP 60 to 70 mmHg), avoid hypoxia (keep SpO2 over 94 percent and PaO2 over 60 mmHg), normocapnia, normoglycaemia, and normothermia.[1]
- Airway and Breathing — intubate and ventilate if GCS is 8 or less (the airway is at risk and ventilation must be controlled). Give supplemental oxygen to keep SpO2 over 94 percent — hypoxia raises ICP by causing cerebral vasodilation and is directly injurious.
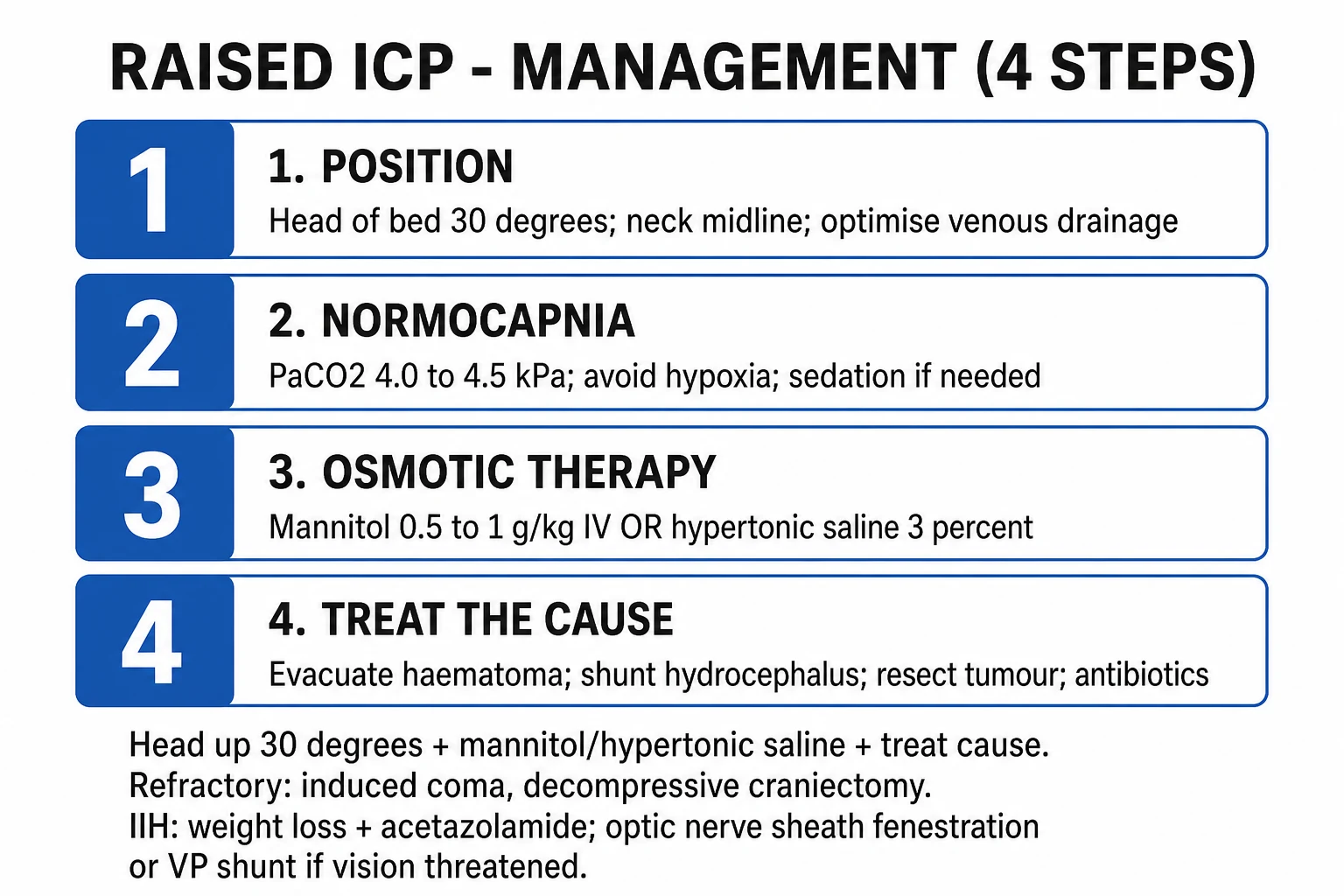
- Normocapnia — target PaCO2 4.0 to 5.0 kPa (35 to 40 mmHg). Brief, mild hyperventilation (PaCO2 4.0 to 4.5 kPa) is reserved for the actively herniating patient as a temporising measure only — it causes cerebral vasoconstriction, momentarily reducing cerebral blood volume and ICP. Prolonged hypocapnia (below 4.0 kPa) causes cerebral ischaemia and is harmful, so hyperventilation is never a sustained strategy.
- Position — head of bed up 30 degrees, neck midline to optimise venous drainage from the brain via the jugular veins. Avoid tight endotracheal-tube ties and any jugular venous compression; even turning the head to one side impedes venous return.
- Perfusion — avoid hypotension (a single episode of systolic BP under 90 mmHg doubles mortality in severe TBI). Maintain CPP 60 to 70 mmHg with isotonic fluids and vasopressors (noradrenaline) as needed.
- Normoglycaemia and normothermia — treat fever (paracetamol, cooling) and seizures (both raise cerebral metabolic demand and ICP). Tight glucose control is avoided because hypoglycaemia is injurious; aim for the normal range.
- Osmotherapy (first-line drugs) — mannitol 0.5 to 1 g/kg IV (typically 0.25 to 1 g/kg as a 20 percent solution over 10 to 15 minutes) draws water out of the brain into the intravascular space by osmosis and is excreted by the kidney. Check serum osmolality and stop if it exceeds 320 mOsm/L (risk of acute kidney injury from hyperosmolar injury). Alternatively, 3 percent hypertonic saline (about 250 mL bolus, or 5 mL/kg) achieves the same osmotic gradient and may be preferred in hypovolaemic patients or those with renal impairment. Both lower ICP within minutes.
- Clinical herniation (Cushing triad, or a unilateral fixed dilated pupil, or a sudden GCS drop) — give emergency mannitol or hypertonic saline, hyperventilate briefly, and arrange urgent CT and neurosurgical referral. This is a "load and go" moment.[1]
Exam application bank (NEET-PG / INICET)
One-line answer
Raised intracranial pressure (ICP) occurs when the volume of brain, blood or CSF exceeds the rigid skull's capacity (Monro-Kellie doctrine). Normal ICP is 5 to 15 mmHg in a supine adult; in traumatic brain injury, ICP over 22 mmHg defines raised ICP and warrants treatment. Causes include space-occupying lesions (tumour, haematoma, abscess), hydrocephalus (obstructive and communicating), cerebral oedema (vasogenic, cytotoxic, osmotic), traumatic brain injury, cerebral venous sinus thrombosis and idiopathic intracranial hypertension (IIH). Presentation: headache (worse on waking, coughing, bending), nausea and vomiting, papilloedema, altered consciousness, and the Cushing triad (bradycardia, hypertension, irregular respiration — a pre-terminal sign). The four herniation syndromes — uncal, central, tonsillar (coning), and subfalcine — are the feared complications. Cerebral perfusion pressur
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Raised Intracranial Pressure.
Management — Definitive & Stepwise
In neurocritical care, a tiered approach is used, escalating only when the lower tier fails. Each tier adds more aggressive intervention with more risk, so escalation is deliberate and guided by ICP and CPP monitoring.[1][5]
Tier 0 — basics
- Head up 30 degrees, neck midline to optimise venous drainage.
- Sedation and analgesia — propofol (titrated infusion) or midazolam with fentanyl; reduces cerebral metabolic demand, agitation, and the sympathetic response to the endotracheal tube. Propofol can cause hypotension; watch CPP.
- Normoxia, normocapnia, normoglycaemia, normothermia — the four normals that protect the injured brain.
- Seizure prophylaxis — phenytoin or levetiracetam for one week in severe TBI with intracranial haematoma or depressed skull fracture (does not reduce late seizures but lowers early ones).
- Treat fever with paracetamol and cooling; fever raises cerebral metabolic demand. [1]
Tier 1 — osmotic therapy
- Mannitol 0.25 to 1 g/kg IV bolus (20 percent solution), repeated guided by ICP and the osmolar gap (measured minus calculated osmolality over 20 mOsm/L signals a waning effect and renal risk). Check serum osmolality and renal function every 6 hours; stop over 320 mOsm/L.
- 3 percent hypertonic saline bolus (250 mL or 5 mL/kg) — useful in hypovolaemic patients and those on mannitol; monitor serum sodium (aim under 160 mmol/L).
- CSF drainage via an EVD — 5 to 10 mL aliquots can lower ICP immediately in a hydrocephalic patient. [1]
Tier 2 — metabolic suppression and surgery
- Barbiturate coma — thiopentone loading then infusion to suppress cerebral metabolic rate (the brain's metabolic demand falls in parallel with blood flow). Use continuous EEG to titrate to burst suppression. Risks: hypotension, immunosuppression, prolonged ICU stay.
- Decompressive craniectomy — removal of a large bone flap (frontotemporoparietal) to give the swollen brain room to expand outward, preventing downward herniation. Reserved for refractory intracranial hypertension unresponsive to tier 0 and tier 1. The RESCUEicp trial showed it lowers mortality and ICP but at the cost of higher rates of vegetative and severely disabled survival in younger patients — a shared-decision, last-tier option, not a first-line treatment.[4]
Treat the cause definitively
- Evacuate an extradural, subdural, or intracerebral haematoma (an extradural haematoma evacuated before coning is one of neurosurgery's most rewarding operations).
- EVD or shunt for hydrocephalus (see below).
- Resect or debulk a tumour; dexamethasone 4 to 8 mg QID (loading 8 to 16 mg) for vasogenic oedema around a tumour or abscess.
- Antibiotics for brain abscess or meningitis (empirical ceftriaxone plus metronidazole, guided by culture). [1]
A critical caveat: corticosteroids are HARMFUL in traumatic and ischaemic raised ICP. The landmark CRASH trial (MRC CRASH, over 10,000 patients randomised) showed that intravenous corticosteroids increased mortality in traumatic brain injury and must not be used for traumatic or haemorrhagic oedema. Reserve dexamethasone for vasogenic oedema (tumour or abscess) only — the mechanism is blood-brain barrier stabilisation, which does not apply to cytotoxic or traumatic oedema.[3]
Raised ICP acute management — HOMBT
HOMBT
neck midline to drain venous blood
mannitol 0.5 to 1 g/kg or 3 percent hypertonic saline 250 mL
keep CPP 60 to 70 mmHg; avoid hypotension and hypoxia
PaCO2 4.0 to 5.0 kPa; hyperventilate only briefly if herniating
evacuate, shunt, resect; dexamethasone for vasogenic oedema only
CSF shunts and diversion
For hydrocephalus, definitive treatment diverts CSF out of the cranial compartment. The ventriculoperitoneal (VP) shunt is the workhorse — a catheter from the lateral ventricle to the peritoneal cavity, with a one-way valve (programmable or fixed-pressure). It is used for both obstructive and communicating hydrocephalus. Endoscopic third ventriculostomy (ETV) is an alternative for obstructive hydrocephalus from aqueduct stenosis — a fenestration is made in the floor of the third ventricle, allowing CSF to bypass the obstruction and flow directly to the basal cisterns, avoiding a shunt and its lifelong complications. The EVD (external ventricular drain) is a temporary measure in acute hydrocephalus, allowing both pressure monitoring and therapeutic CSF drainage, and is the bridge between acute presentation and definitive shunting. [1]
Shunt complications are common and examinable: blockage (the commonest, presenting with headache, vomiting, drowsiness — shunt malfunction); infection (Staphylococcus epidermidis or aureus, presenting with fever, meningism, shunt-track redness — requires shunt removal and antibiotics); overdrainage (the ventricles collapse, causing slit-ventricle syndrome or intracranial hypotension with orthostatic headache); and underdrainage (persistent hydrocephalus). The syndrome of the trephined (sinking skin flap syndrome) is a delayed complication of decompressive craniectomy, where the brain sinks under the absent bone flap as atmospheric pressure exceeds intracranial, producing neurological deterioration corrected by cranioplasty. [1]
Specific Subtypes & Scenarios
Idiopathic intracranial hypertension (IIH)
IIH (pseudotumour cerebri) is raised ICP with no identifiable structural cause after thorough investigation. The classical patient is a young, obese woman of reproductive age. The presentation is daily progressive headache, transient visual obscurations (lasting seconds, often on bending), pulsatile tinnitus, papilloedema on fundoscopy, and a sixth-nerve palsy (false-localising). The main risk is permanent blindness from chronic optic atrophy — visual loss is the indication for surgery. Diagnosis uses the modified Dandy criteria: signs of raised ICP, no localising signs except a sixth-nerve palsy, opening pressure over 25 cmH2O with normal CSF, and normal MRI/MRV (excluding venous sinus thrombosis). Treatment is staged: weight loss of 5 to 10 percent (the single most effective intervention, often achieved with dietitian support or bariatric surgery in severe obesity); acetazolamide 1 to 2 g/day (up to 4 g/day), a carbonic anhydrase inhibitor that reduces CSF production; topiramate as an alternative (also aids weight loss). If vision is threatened despite maximal medical therapy, the options are optic nerve sheath fenestration (protects vision fastest by relieving pressure on the optic nerve head) or a VP or lumboperitoneal shunt (relieves the systemic ICP). Monitor vision with serial perimetry and optical coherence tomography (OCT) of the retinal nerve fibre layer — a falling field or thinning nerve fibre layer drives surgical timing.[2][6]
Severe traumatic brain injury
In severe TBI (GCS 3 to 8), the secondary brain injury — hypoxia, hypotension, raised ICP — determines outcome far more than the primary impact. The Brain Trauma Foundation 4th edition guidelines set the monitoring and treatment thresholds: ICP monitoring in GCS 3 to 8 with abnormal CT (or normal CT with two of: age over 40, motor posturing, systolic BP under 90); treat ICP over 22 mmHg; target CPP 60 to 70 mmHg; avoid prophylactic steroids (harmful — CRASH trial); use multimodal monitoring (ICP, PbtO2, microdialysis) in the most severe.[3][5]
Obstructive versus communicating hydrocephalus
Obstructive (non-communicating) hydrocephalus results from a block within the ventricular system — aqueduct stenosis, a posterior fossa tumour (medulloblastoma, ependymoma compressing the fourth ventricle), or fourth-ventricle outflow obstruction. Imaging shows ventriculomegaly proximal to the block (e.g. lateral and third ventricles dilated with a normal fourth ventricle in aqueduct stenosis). Treatment is EVD, VP shunt, or endoscopic third ventriculostomy (ETV, for aqueduct stenosis). Communicating hydrocephalus results from impaired CSF absorption at the arachnoid granulations — after subarachnoid haemorrhage (blood blocks the granulations), after meningitis (inflammatory debris), or with carcinomatous meningitis. All four ventricles are dilated; treatment is usually a VP shunt. Normal pressure hydrocephalus is a chronic communicating form in the elderly with the triad of gait apraxia, dementia, and urinary incontinence — treatable by shunting.[1]
Cerebral venous sinus thrombosis
Cerebral venous sinus thrombosis presents with headache, papilloedema, and seizures, mimicking IIH in young prothrombotic women, but may produce a venous infarct (often haemorrhagic) with focal deficits. Diagnose on MRV (absent or irregular venous sinus flow). Treat with anticoagulation (heparin then warfarin) even in the presence of haemorrhage — the haemorrhage is venous, caused by back-pressure, and anticoagulation relieves the obstruction. This is the key exam point: a haemorrhagic venous infarct is treated with anticoagulation, not withheld from it.[2]
The herniation syndromes — immediate management
Any herniation syndrome is an emergency: give immediate osmotherapy (mannitol or hypertonic saline), hyperventilate briefly, arrange urgent CT, and involve neurosurgery for decompression or evacuation. A unilateral fixed dilated pupil (uncal) in a patient with a temporal haematoma may reverse with emergency evacuation; a patient with tonsillar coning and respiratory arrest is often beyond salvage but deserves the full bundle. [1]
Complications & Pitfalls
Brain herniation (coning)
- Uncal, central, tonsillar, subfalcine — fatal if untreated
- Tonsillar causes respiratory arrest via medullary compression
- Prevent: CT before LP; osmotherapy early; never herniate
Visual loss in IIH
- Progressive optic atrophy and permanent blindness
- Serial perimetry and OCT are mandatory
- Visual obscurations predict risk; ONSF or shunt if threatened
Mannitol toxicity
- Hypovolaemia and hypotension, hyperosmolar acute kidney injury
- Stop if serum osmolality over 320 mOsm/L
- Rebound ICP rise on discontinuation; monitor electrolytes and renal function
Surgical complications
- Decompressive craniectomy: infection, subdural hygroma, syndrome of the trephined
- VP shunt: blockage, infection (Staph epidermidis), overdrainage (slit-ventricle)
- EVD: ventriculitis, haemorrhage on placement
The classic diagnostic pitfall is performing an LP before CT in a patient with a mass lesion — this can precipitate tonsillar herniation (coning) by releasing the spinal pressure gradient. Always image first if there is any focal sign, reduced consciousness, papilloedema, immunocompromise, new-onset seizure, abnormal fundus, or a history suggestive of a mass (progressive headache, vomiting). Another is giving corticosteroids in traumatic raised ICP — the CRASH trial proved this increases mortality; reserve dexamethasone for vasogenic oedema (tumour or abscess) only.[3] A third is prolonged hyperventilation — the initial reduction in ICP from hypocapnia is bought at the price of cerebral ischaemia, so hyperventilation is a bridge to definitive treatment, not a sustained therapy. A fourth is missing the slowly deteriorating GCS — a drop of two points is an emergency even if the patient is still "talking".
Prognosis & Disposition
Prognosis depends on the underlying cause and the speed of treatment. The prognostic factors in TBI-related raised ICP are age, initial GCS, pupillary response (bilaterally fixed dilated pupils carry 70 to 90 percent mortality), the degree of ICP control achieved, and the CPP maintained. Treatable causes — an extradural haematoma, hydrocephalus, a brain abscess — can have excellent outcomes if decompressed promptly before herniation. An extradural haematoma evacuated before coning is one of neurosurgery's most rewarding operations: the patient walks in with a headache and walks out neurologically intact. Severe TBI with uncontrolled ICP carries roughly 50 percent mortality. Malignant tumours with mass effect have a poor prognosis driven by the underlying disease. IIH is chronic and relapsing but usually vision-threatening rather than life-threatening — visual monitoring is the safety net that drives surgical decisions; the IIH Treatment Trial showed acetazolamide plus weight loss improves papilloedema and symptoms in mild disease.[6]
In devastating brain injury with uncontrollable ICP despite tier 0, tier 1, and decompressive craniectomy, the discussion moves to palliative care and withdrawal of life-sustaining treatment — a multidisciplinary decision involving neurosurgery, intensive care, and the family, guided by prognostic signs (bilaterally absent pupillary and corneal reflexes, absent motor response, sustained ICP over 40 mmHg).[4]
Disposition: any patient with reduced consciousness, papilloedema, a monitored ICP, or an evolving neurological deficit belongs in ICU or neurocritical care; any surgical lesion (haematoma, hydrocephalus, tumour with mass effect) goes to theatre; stable IIH with intact vision can go to the ward with close perimetry and OCT follow-up. [1]
Special Populations
- Infants — the open fontanelle and unfused sutures provide additional compliance, so the signs differ: bulging fontanelle (palpated when the infant is calm and upright), splayed sutures (separation of the cranial bones), rapidly increasing head circumference (plot on a centile chart — crossing centiles is a red flag), sunset sign (eyes driven downward, exposing sclera superiorly, from tectal plate compression), a high-pitched cry, irritability, and vomiting. Causes in infants: congenital hydrocephalus (aqueduct stenosis, Chiari II with myelomeningocele, Dandy-Walker malformation), intraventricular haemorrhage of prematurity, and congenital infections.
- Children — posterior fossa tumours (medulloblastoma, ependymoma, pilocytic astrocytoma) are the commonest cause, often presenting with ataxia, head tilt, vomiting, and obstructive hydrocephalus. Always image a child with a headache that is progressive, present on waking, or accompanied by vomiting or ataxia.
- Pregnancy — IIH is commoner in pregnancy (the hormonal and weight changes raise susceptibility). Differentiate from pre-eclampsia and eclampsia (hypertension, proteinuria, seizures, raised liver enzymes). Acetazolamide is generally avoided in the first trimester (theoretical teratogenicity) but is considered safe in the second and third; weight management is key. Cerebral venous sinus thrombosis is also commoner in pregnancy and the puerperium.
- The elderly — cerebral atrophy increases intracranial compliance, so presentation is later and subtler (cognitive change, falls, fluctuating consciousness) — a chronic subdural haematoma may reach enormous size before symptoms. Subdural haematoma after even minor trauma is common, especially when anticoagulated — present with a delayed, fluctuating conscious level weeks after the injury.
- The anticoagulated patient — any new headache or reduced consciousness demands urgent CT and immediate reversal of warfarin (vitamin K plus prothrombin complex concentrate) or a DOAC (idarucizumab for dabigatran, andexanet alfa for apixaban or rivaroxaban) before a bleed expands. Do not wait for the INR; reverse empirically if the clinical suspicion is high.
- The immunocompromised and HIV-positive patient — think toxoplasma abscess (ring-enhancing lesion on CT, treated with sulphadiazine plus pyrimethamine), primary CNS lymphoma (periventricular, EBV-driven, steroids cause dramatic shrinkage that confuses the biopsy — withhold steroids until biopsy if lymphoma is suspected), and cryptococcal meningitis (which raises ICP and may need repeat therapeutic LPs or a shunt to relieve pressure).[1][2]
Evidence, Guidelines & Regional Differences
CRASH trial — corticosteroids in TBI
Lancet 2005
PMID 15936423
Key finding
In over 10,000 adults with head injury, intravenous corticosteroids INCREASED 2-week mortality (risk ratio 1.18) and 6-month mortality. Steroids are HARMFUL in traumatic brain injury and must not be used for traumatic raised ICP. Reserve dexamethasone for vasogenic oedema (tumour, abscess) only.
RESCUEicp — decompressive craniectomy
NEJM 2016
PMID 27602507
Key finding
In 408 patients with refractory traumatic intracranial hypertension, decompressive craniectomy lowered mortality (26.9 percent vs 48.9 percent) compared with medical management, but survivors had higher rates of vegetative state and severe disability. A last-tier option: it trades death for disability in younger patients.
Brain Trauma Foundation 4th edition
Neurosurgery 2020
PMID 32761068
Key finding
Updated severe TBI guidelines: treat ICP over 22 mmHg; target CPP 60 to 70 mmHg; use multimodal monitoring (ICP, PbtO2, microdialysis); avoid prophylactic steroids; decompressive craniectomy is an option for refractory ICP.
IIH Treatment Trial
JAMA 2014
PMID 24756514
Key finding
In 165 patients with mild IIH, acetazolamide plus weight loss improved papilloedema and visual field function more than placebo plus weight loss. Acetazolamide is effective in mild-moderate IIH; surgery (ONSF or shunt) is reserved for vision-threatening disease.
Indian (AIIMS and ICMR neurocritical care protocols) apply the same ICP and CPP thresholds but, in resource-limited settings, rely more on clinical signs (GCS, pupils) and empirical osmotic therapy when invasive ICP monitoring is unavailable. The principles — head up, normocapnia, mannitol or hypertonic saline, treat the cause — are universal and cost-neutral; what varies is the monitoring infrastructure. The cerebral perfusion equation CPP equals MAP minus ICP is the single most reproduced fact across every guideline.[1]
Exam Pearls
- "Raised ICP: headache (worse on waking or coughing) plus vomiting plus papilloedema plus falling consciousness."[1]
- "Cushing triad equals bradycardia plus hypertension with wide pulse pressure plus irregular respirations equals pre-terminal brainstem herniation — its absence never excludes raised ICP."
- "CPP equals MAP minus ICP. Treat ICP over 22 mmHg (trauma); keep CPP 60 to 70 mmHg."[5]
- "CT FIRST before LP — risk of coning. Never do LP first in a possible mass."
- "Acute: head up 30 degrees, neck midline, normocapnia (PaCO2 4.0 to 5.0 kPa), mannitol 0.5 to 1 g/kg or 3 percent hypertonic saline 250 mL, treat the cause."
- "IIH equals young obese women, papilloedema, normal MRI/MRV, LP pressure over 25 cmH2O, normal CSF. Treat: weight loss plus acetazolamide 1 to 2 g/day; surgery if vision threatened."[2]
- "Herniation: uncal (ipsilateral fixed dilated pupil, contralateral hemiparesis) equals emergency. Tonsillar (coning) equals respiratory arrest and death. Central (pinpoint pupils, coma, DI). Subfalcine (ACA compression, contralateral leg weakness)."
- "Steroids for vasogenic oedema (tumour or abscess) ONLY — they are HARMFUL in traumatic raised ICP (CRASH trial)."[3]
- "Monro-Kellie: rigid skull, fixed volume — brain about 80 percent, blood about 10 percent, CSF about 10 percent. Exhaust compensation and pressure spikes exponentially."
- "False-localising sixth-nerve palsy: long nerve stretched at the petroclinoid ligament as the brain shifts; does not localise the lesion."
References
- [1]Kareemi H, Pratte M, English S, et al. Initial Diagnosis and Management of Acutely Elevated Intracranial Pressure J Intensive Care Med, 2023.PMID 36802976
- [2]Wang MTM, Bhatti MT, Danesh-Meyer HV. Idiopathic intracranial hypertension: Pathophysiology, diagnosis and management J Clin Neurosci, 2022.PMID 34929642
- [3]Edwards P, Arango M, Balica L, et al. Final results of MRC CRASH, a randomised placebo-controlled trial of intravenous corticosteroid in adults with head injury-outcomes at 6 months Lancet, 2005.PMID 15936423
- [4]Hutchinson PJ, Kolias AG, Timofeev IS, et al. Trial of Decompressive Craniectomy for Traumatic Intracranial Hypertension N Engl J Med, 2016.PMID 27602507
- [5]Hawryluk GWJ, Rubiano AM, Totten AM, et al. Guidelines for the Management of Severe Traumatic Brain Injury: 2020 Update of the Decompressive Craniectomy Recommendations Neurosurgery, 2020.PMID 32761068
- [6]Wall M, McDermott MP, Kieburtz KD, et al. Effect of acetazolamide on visual function in patients with idiopathic intracranial hypertension and mild visual loss: the idiopathic intracranial hypertension treatment trial JAMA, 2014.PMID 24756514