Neurology · General Medicine
Status Epilepticus
Also known as Status epilepticus · SE · Convulsive status · Non-convulsive status · Refractory status epilepticus
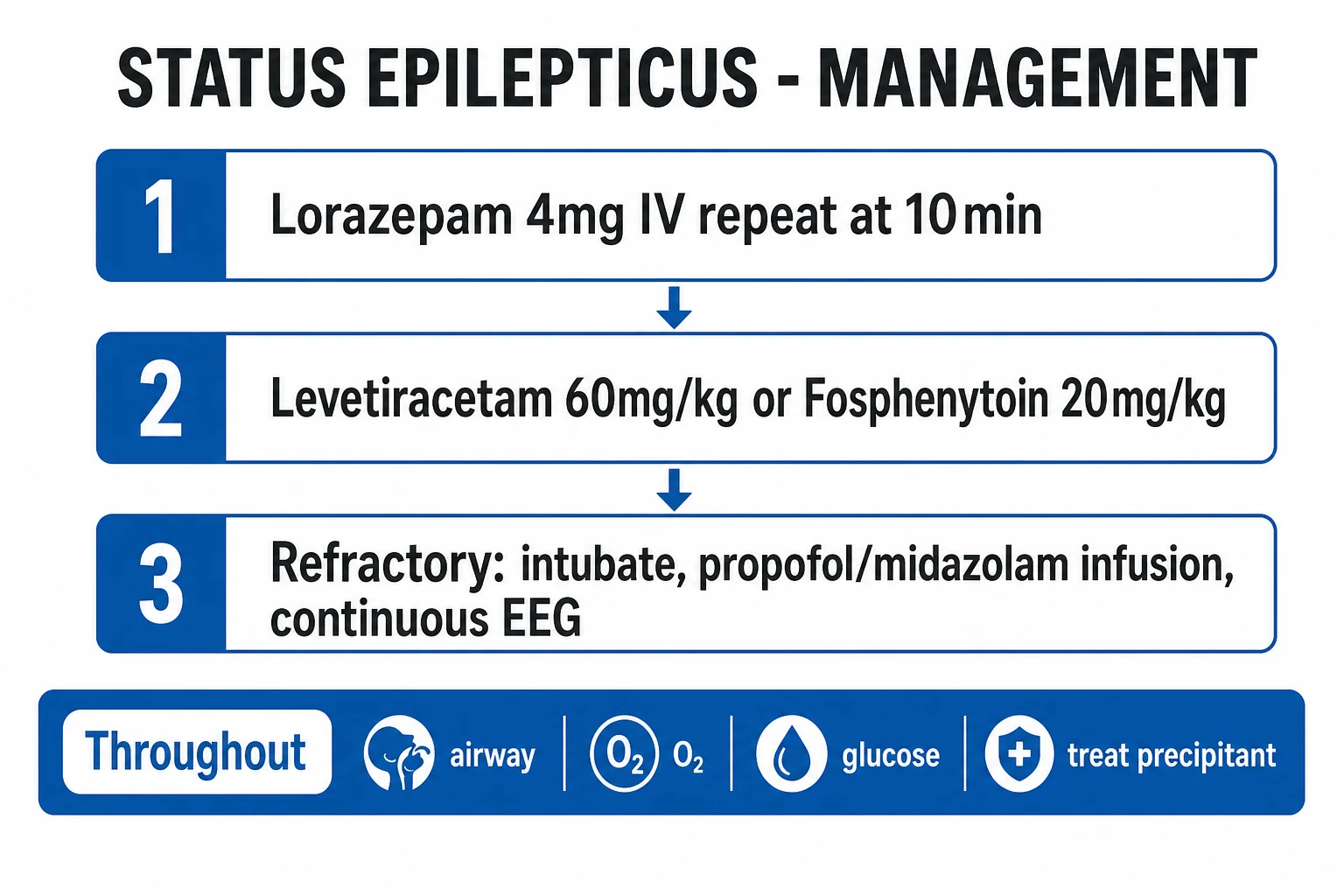
Status epilepticus (SE) is a continuous seizure lasting over 5 minutes, or recurrent seizures without recovery between them — a neurological emergency with mortality over 20 percent. The protocol is staged and time-critical: (1) IV lorazepam 4 mg (repeat once at 10 min); (2) IV levetiracetam 60 mg/kg or fosphenytoin 20 mg PE/kg or valproate 40 mg/kg; (3) refractory — ICU, intubation, anaesthetic infusion (propofol or midazolam) with continuous EEG. Always secure the airway, give oxygen, check and treat glucose and electrolytes, and find and treat the precipitant (AED non-adherence, infection, alcohol withdrawal, metabolic disturbance, stroke, tumour).
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Exam tags
Red flags
Overview & Definition
Status epilepticus (SE) is the most severe manifestation of epilepsy — a continuous or rapidly recurring seizure that does not self-terminate. It is a time-critical neurological emergency: every minute untreated increases neuronal injury and mortality, and reduces the chance that treatment will work. Across most emergency departments a single SE call mobilises the same urgency as a cardiac arrest, because the harm compounds every minute the brain keeps firing. [1]
The ILAE 2015 operational definition frames SE around two time points that the examiner rewards precisely.[1] t1 is the time beyond which a seizure should be treated as continuous — the point at which the brain's intrinsic seizure-terminating mechanisms have failed and active treatment must begin. t2 is the time beyond which there is a risk of long-term consequences — neuronal injury, pharmacoresistance and ongoing structural damage. For generalised convulsive SE the values are t1 equals 5 minutes and t2 equals 30 minutes; for focal SE t1 is 10 minutes; for absence SE t1 is 10 to 15 minutes; for myoclonic SE t1 is 10 to 15 minutes. The practical consequence is decisive: start treatment at 5 minutes, not 30. The window between t1 and t2 is the therapeutic window in which the seizure is most likely to respond to a benzodiazepine, before time-dependent pharmacoresistance takes hold.
A second, older operational definition still appears in older textbooks and exam stems: a continuous clinical or electrical seizure lasting at least 5 minutes, or two or more seizures without full recovery of consciousness between them. Both are correct and complementary — the first is the ILAE 2015 formulation; the second is the working "two seizures without recovery" rule used by most emergency and pre-hospital protocols. The protocolised, staged approach — benzodiazepine, then a second-line antiseizure drug, then anaesthesia — is among the most evidence-based treatments in neurology, resting on three large multicentre randomised trials.[2][4]

Classification
SE is classified along three independent axes — by semiology, by response to therapy, and by aetiology — because each axis changes the immediate management, the prognostic estimate, and the later work-up. An examiner will often ask for all three in the same breath. [1]
Convulsive SE
- Generalised convulsive SE (GCSE) — overt bilateral tonic-clonic; the classic emergency, most predictable on EEG
- Focal motor SE / epilepsia partialis continua — continuous clonic jerking of one body part, consciousness preserved
- Subtle SE — minimal twitching of face, hands or eyes, coma, ongoing electrographic seizure after prolonged GCSE (electromechanical dissociation)
Non-convulsive SE
- Altered consciousness, confusion or coma without overt convulsions — easily missed without EEG
- Often follows a controlled convulsion that has stopped motorically but not electrically
- Absence status (spike-wave stupor) — prolonged confusion, 3-Hz or atypical spike-wave on EEG
By therapy response
- Established SE — ongoing despite adequate benzodiazepine (around the 20–40 min mark)
- Refractory SE (RSE) — ongoing despite benzodiazepine plus one adequate second-line agent
- Super-refractory SE (SRSE) — ongoing or recurring for over 24 h after onset of anaesthetic infusion
By aetiology, SE uses the SAME framework — Structural, Autoimmune (immune), Metabolic, Infectious, genetic, unknown — and is further divided into acute symptomatic (stroke, infection, metabolic, hypoxia — prognosis driven largely by the cause) versus remote or progressive (old glial scar, tumour, neurodegeneration), and known epilepsy (non-adherence, withdrawal) versus new-onset SE. The aetiological axis matters most at the bedside because an untreated precipitant will defeat any amount of benzodiazepine: the patient in status from profound hyponatraemia or an occult intracranial bleed keeps seizing until the sodium is corrected or the haematoma is evacuated.[4]
A fourth, often-tested distinction is convulsive versus non-convulsive, because non-convulsive SE (NCSE) is the form most often missed. Subtle SE — minimal motor activity with ongoing electrographic seizure in a comatose patient, classically after prolonged GCSE — sits at the borderland and is a frequent cause of unexplained coma in intensive care.[5]
Epidemiology & Risk Factors
SE has an annual incidence of roughly 10 to 40 per 100,000 (some population studies report higher figures, up to 60 to 65 per 100,000 per year in adults and over 150 in young children), with a characteristic bimodal age distribution — peaking in early childhood (under 5 years, often febrile or infectious) and again in the elderly (over 60 years, driven by stroke, dementia and metabolic causes).[4][5] Overall short-term case fatality is over 20 percent, rising to 30 to 40 percent in refractory SE and higher still in the elderly and in anoxic aetiology. About a third of patients presenting in SE have no prior history of epilepsy — a first seizure that does not stop can be the debut of a brain tumour, an intracranial haemorrhage or severe metabolic disturbance, and the index of suspicion for a serious cause must be correspondingly high.
The commonest precipitants, in roughly descending order of frequency, are antiseizure-drug (AED) non-adherence or withdrawal (the single most frequent cause in known epilepsy and the most readily reversible), CNS infection (meningitis, encephalitis — and in India, neurocysticercosis and CNS tuberculosis are over-represented), metabolic disturbance (hyponatraemia, hypoglycaemia, hypocalcaemia, hepatic and renal failure), stroke (ischaemic or haemorrhagic), hypoxic-ischaemic encephalopathy after cardiac arrest, alcohol withdrawal, brain tumour (primary or metastatic), head trauma and drug toxicity (tricyclics, isoniazid, theophylline, tramadol, cocaine).[4]
Status epilepticus — the numbers that decide an answer
Risk factors that predict refractory SE and poor outcome include longer duration before treatment, age over 65, an acute symptomatic cause (especially anoxic encephalopathy), low presenting GCS, non-convulsive or subtle SE at onset, and prior epilepsy with non-adherence. In the developing world, additional contributors are inadequate AED supply and follow-up, neurocysticercosis and CNS tuberculosis, and a higher background prevalence of traumatic brain injury.[4]
Pathophysiology
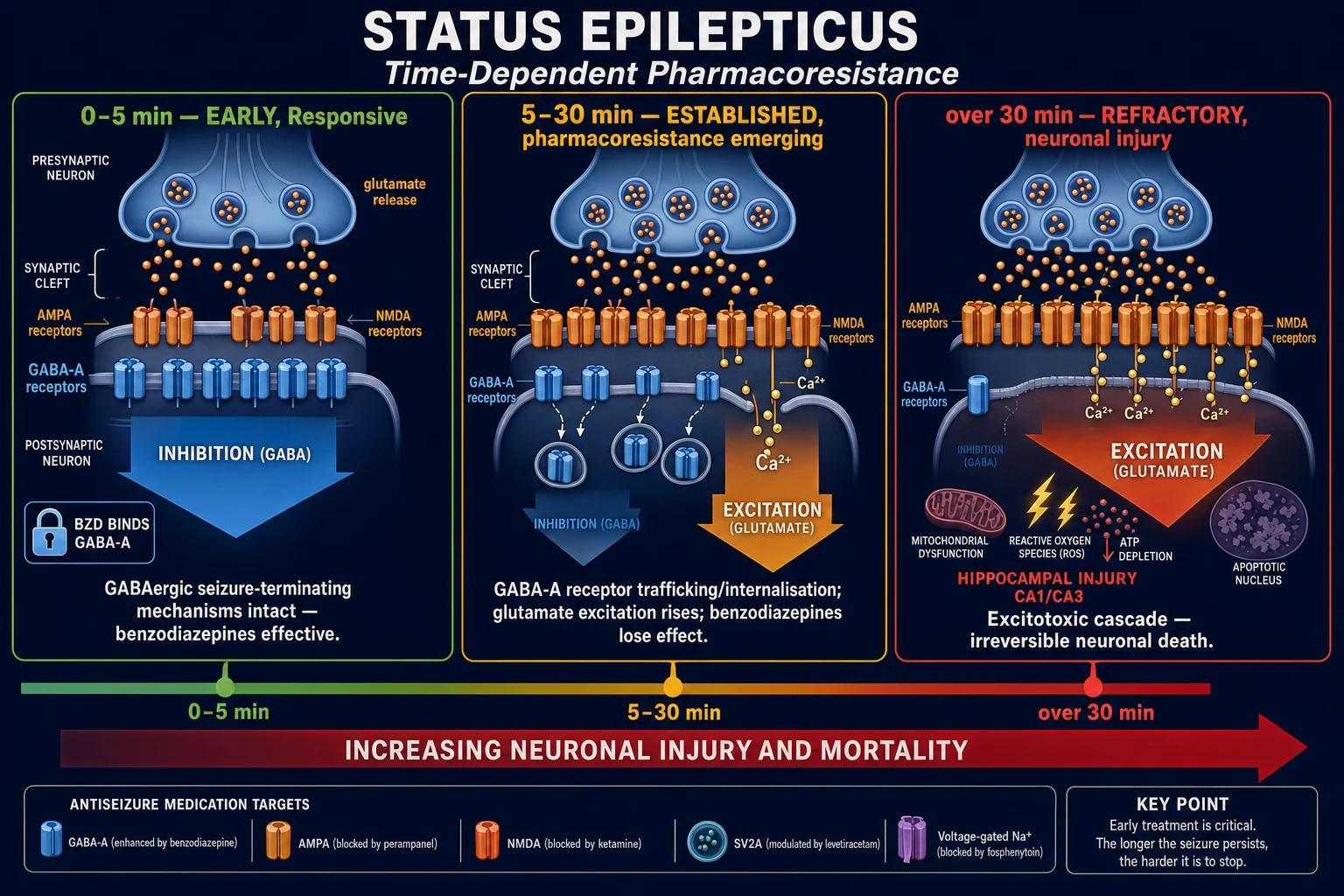
At its core, SE is a failure of the brain's intrinsic seizure-terminating mechanisms, with a progressive, self-reinforcing shift from inhibitory (GABAergic) dominance to excitatory (glutamatergic) dominance. Early on, GABA-A receptors are abundantly expressed on the neuronal surface, fast inhibitory neurotransmission is intact, and benzodiazepines work well. As the seizure continues, two molecular events produce the phenomenon that governs the entire protocol — time-dependent pharmacoresistance:[4][5]
- GABA-A receptors are internalised — they are trafficked off the synaptic membrane into clathrin-coated vesicles, so the surface density of the benzodiazepine's target falls, inhibition wanes, and a dose that worked at 5 minutes may fail at 30.
- NMDA and AMPA glutamate receptors are recruited and upregulated to the synapse, so excitation rises, calcium floods the neuron, and the seizure becomes self-sustaining and harder to abort. [1]
The downstream excitotoxic cascade — sustained NMDA-mediated calcium influx, mitochondrial dysfunction, oxidative stress, nitric-oxide-mediated injury and ATP depletion — drives neuronal necrosis and apoptosis. The hippocampus (CA1 and CA3 pyramidal cells) is the most vulnerable region, followed by the amygdala, piriform cortex and thalamus; the long-term consequence of prolonged SE is mesial temporal sclerosis, lasting cognitive impairment, and a substantially increased risk of future epilepsy. This is the molecular reason the t2 threshold sits at 30 minutes — beyond that point, structural injury is accumulating and the seizure is increasingly pharmacoresistant.[5]
The systemic consequences of prolonged convulsive SE compound the brain injury and themselves become life-threatening: hypoxia and aspiration, lactic acidosis from sustained muscle activity, hyperpyrexia, rhabdomyolysis (myoglobinuria, acute kidney injury and compartment syndrome), an autonomic surge (hypertension then hypotension), hyperkalaemia, disseminated intravascular coagulation, neurogenic pulmonary oedema, and cardiac ischaemia or arrhythmia from catecholamine excess. These systemic effects explain why a patient can die of SE without the brain being the immediate cause of death.[4]
Clinical Presentation
Generalised convulsive SE (GCSE) presents as continuous or rapidly recurrent tonic-clonic activity without recovery of consciousness between convulsions. The patient is unconscious, often cyanosed, with laboured breathing, excess oral secretions, and incontinence. As GCSE prolongs, the motor activity may become subtle — twitching of the face, hands or eyes, nystagmoid eye movements, or rhythmic blinking — while the patient remains comatose and the electrographic seizure continues (subtle SE, also called electromechanical dissociation). Recognising this transition is critical: the absence of dramatic convulsions does not mean the seizure has ended.[5]
Non-convulsive SE (NCSE) presents as altered consciousness, confusion or coma without overt convulsions — classically after a controlled convulsion that has stopped motorically but not electrically, or in the elderly as fluctuating confusion that is mistaken for delirium or dementia. There may be subtle automatisms (lip-smacking, picking at sheets), eye deviation, or minor myoclonic twitching. NCSE is frequently missed without a low threshold to request EEG, and it accounts for a substantial fraction of unexplained coma in ICU.[5]
Focal motor SE (epilepsia partialis continua) is continuous clonic jerking of one body region — a hand, a corner of the mouth, a foot — with consciousness preserved; causes include Rasmussen encephalitis (in children), a focal structural lesion (stroke, tumour, abscess), and metabolic disturbance. Absence status (spike-wave stupor) presents as prolonged confusion in children or the elderly — the patient is responsive but slow and "switched off" — with 3-Hz (typical) or atypical spike-wave on EEG. It can run for days before being recognised.[4]
Atypical presentations are high-yield and deliberately tested: the elderly patient with fluctuating confusion or coma (NCSE masquerading as delirium), the post-anoxic coma patient after cardiac arrest (myoclonic or non-convulsive SE), the patient with periodic lateralised epileptiform discharges (PLEDs / LPDs) who may be in focal SE in the right clinical context, and the ** ICU patient with unexplained depressed consciousness** after a convulsion that "looked controlled". For all of these, the unifying rule is the same: a patient who has stopped overtly convulsing but remains comatose after GCSE is in non-convulsive SE until proven otherwise — request an urgent EEG.[5]
Differential Diagnosis
Distinguishing true SE from its mimics is essential — escalating a mimic to anaesthesia is dangerous, and missing true SE is fatal. The examiner expects at least three mimics, each with a discriminating feature. [1]
Psychogenic non-epileptic seizure (PNES)
- Variable, out-of-phase motor activity; eyes forcibly closed (active resistance to opening)
- Preserved reflexes, no postictal confusion, no cyanosis; normal lactate, CK, prolactin
- EEG shows no electrographic seizure — the decisive test
Convulsive syncope / arrhythmia
- Brief (seconds), pallor precedes, rapid full recovery; may have a few myoclonic jerks from cerebral hypoperfusion
- Always check an ECG for long-QT / Brugada / arrhythmia masquerading as seizure
- Anoxic myoclonus after a cardiac arrest is NOT convulsive SE and is treated differently
Postictal / toxic-metabolic encephalopathy
- The comatose post-convulsion patient — distinguish from NCSE only with EEG
- Metabolic encephalopathy: correctable cause (Na, glucose, Ca, ammonia), EEG shows slowing not evolving seizure
- Sepsis/delirium and stroke can both mimic NCSE — EEG resolves the question
Drug-induced movement / rigidity
- Serotonin syndrome (clonus, hyperreflexia, autonomic signs, serotonergic drug)
- Neuroleptic malignant syndrome (lead-pipe rigidity, fever, antipsychotic)
- Tramadol / antidepressant / isoniazid myoclonus — toxidrome history; EEG not epileptic
Decerebrate / decorticate posturing
- A brainstem or cerebral hemisphere sign, NOT epileptic
- Stereotyped, stimulus-triggered, sustained posturing; EEG shows no seizure
- Indicates severe structural brain injury — image urgently
The single most useful bedside discriminators between true GCSE and PNES are EEG (gold standard), the lactate (markedly elevated in true convulsive SE, normal in PNES), eye closure (PNES patients force their eyes shut and resist opening), and the tempo and variability of the movements (PNES is waxing, waning and out-of-phase; GCSE is stereotyped and synchronous).[5]
Common precipitants of status epilepticus — A V I D M E N
AVIDMEN
the single commonest cause in known epilepsy
stroke — ischaemic or haemorrhagic
meningitis, encephalitis, neurocysticercosis (India)
alcohol withdrawal, drug toxicity (TCAs, INH)
hyponatraemia, hypoglycaemia, hypocalcaemia, hepatic/renal failure
hypoxic-ischaemic, autoimmune/paraneoplastic (anti-NMDAR)
primary or metastatic brain tumour
Clinical & Bedside Assessment
Immediate bedside assessment is ABCDE plus timing. Secure the airway with an adjunct or recovery position, give high-flow oxygen, obtain IV access, time the seizure precisely from onset, and check capillary glucose at once — hypoglycaemia is rapidly reversible and is the classic mimic and precipitant that must never be missed. Draw bloods for glucose, U&E, LFT, calcium, magnesium, FBC, CRP, blood gas and lactate, AED levels, toxicology (including alcohol), and beta-hCG in every woman of childbearing age (an eclamptic seizure changes the entire first-line drug).[2][4]
Examine for the precipitant while resuscitating: fever and meningism point to CNS infection; a focal neurological deficit to stroke, tumour or abscess; signs of chronic liver or renal disease to a metabolic cause; needle marks, alcohol on the breath or withdrawal tremor to substance-related causes; and neurocutaneous stigmata (cafe-au-lait, ash-leaf spots) to an underlying neurocutaneous syndrome. Grade consciousness with the Glasgow Coma Scale (eye 1–4, verbal 1–5, motor 1–6; range 3–15) and set the threshold for intubation at GCS under 8, loss of airway reflexes, or the need for anaesthesia in refractory SE.[4]
Two bedside rules decide the answer to many exam questions. First, give IV thiamine (high-dose, e.g. 250 to 500 mg) before any glucose in the alcohol-misusing or malnourished patient — glucose alone can precipitate Wernicke encephalopathy. Second, a patient who has stopped overtly convulsing but remains comatose after GCSE is in non-convulsive SE until proven otherwise — request an urgent EEG rather than assuming the seizure has ended.[5]
Investigations
The immediate bedside test is capillary glucose; the emergency blood panel is venous glucose, U&E, LFT, calcium, magnesium, FBC, CRP, blood gas and lactate, toxicology, AED levels and beta-hCG. An ECG is done in every patient — both to exclude a long-QT arrhythmia or cardiac syncope masquerading as seizures, and to monitor the cardiac effects of fosphenytoin or phenytoin (PR prolongation, QRS widening, hypotension).[4]
Neuroimaging — once the patient is stabilised and the seizure controlled — begins with CT brain acutely to exclude haemorrhage, mass effect, large stroke or abscess. MRI brain is obtained later for aetiology (hippocampal signal change in mesial temporal sclerosis or acute neuronal injury, cortical swelling, tumour, cortical vein thrombosis). Imaging is deferred until the airway and seizure are controlled; never delay treatment for a scan, and never send an unstable or actively convulsing patient to the scanner.[4]
Lumbar puncture is indicated when CNS infection is suspected (fever, meningism, immunocompromised, unclear cause in a young child) and is deferred until raised ICP or a mass lesion is excluded by CT and the patient is stable, with coagulation checked. Send CSF for cells, protein, glucose (with a paired plasma glucose), Gram stain, culture, viral PCR (especially HSV) and, where the clinical picture fits, autoimmune or paraneoplastic antibodies (anti-NMDA-receptor, LGI1, GAD). Start empiric antimicrobial therapy (ceftriaxone plus acyclovir, plus vancomycin if listeria is possible) before imaging if the suspicion of meningitis or encephalitis is high.[4]
EEG is mandatory in four situations: whenever NCSE is suspected (the comatose or confused post-convulsion patient), in all refractory and super-refractory SE, to titrate the anaesthetic infusion to burst-suppression, and in any patient who fails to recover consciousness after a convulsion. The electrographic signature of SE is rhythmic spikes or spike-wave discharges that evolve in frequency, morphology and field; PLEDs or lateralised periodic discharges (LPDs) may represent SE in the right clinical context. Continuous EEG (cEEG) is the monitoring standard for any comatose patient after GCSE, because NCSE is otherwise undetectable.[4][5]
Management — Resuscitation
The first five minutes are time-critical stabilisation. The guiding principle is that treatment is time-critical: give the benzodiazepine at 5 minutes — every minute of delay reduces the response rate and increases mortality.[2]
The first 5 minutes — ABCDE plus glucose and the clock
Airway / Breathing
Airway adjunct or recovery position, suction secretions, high-flow oxygen via mask (target SpO2 94–98%); prepare to bag-valve-mask ventilate if apnoeic
Circulation / IV access
Large-bore IV access x2; send bloods (glucose, U&E, LFT, Ca/Mg, FBC, CRP, gas, lactate, AED levels, tox, beta-hCG); ECG monitor and blood pressure
Glucose
Check capillary glucose immediately; if low (under 3 mmol/L) give 50 mL of 50% dextrose IV (children 2 mL/kg of 25%); give IV thiamine 250–500 mg BEFORE glucose in alcohol misuse
Time the seizure
Establish exact onset from witnesses; if 5 min or more of continuous seizure, OR two seizures without recovery, treat as SE — give the benzodiazepine NOW
Treat the precipitant
Empiric antibiotics/antivirals if infection suspected, correct electrolytes, Naloxone if opioid suspected, pyridoxine (vitamin B6) if INH overdose suspected
Intubate and ventilate when GCS is under 8, airway reflexes are lost, respiratory failure develops from aspiration, or refractory SE mandates anaesthesia. Treat the precipitant concurrently — empiric ceftriaxone plus acyclovir if infection is suspected, glucose for hypoglycaemia, electrolyte correction, and pyridoxine for isoniazid-induced SE (a classic exam stem in India).[4]
Management — Definitive & Stepwise
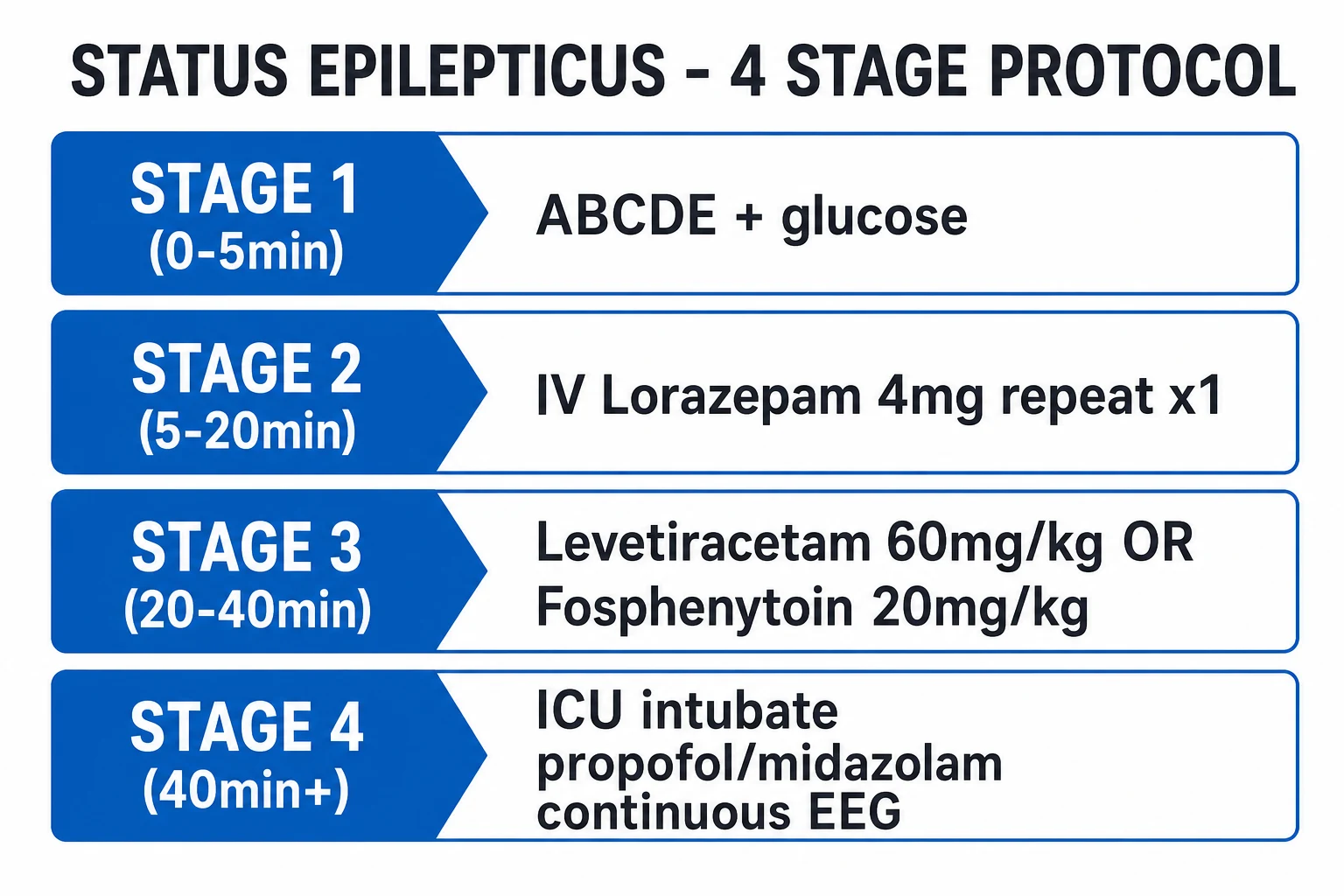
The four-stage protocol is the single highest-yield piece of reproducing knowledge in this topic. Reproducing the drug, dose, route and timing verbatim is what the examiner is testing. The times below are the AES 2016 guideline framework; many UK and Indian protocols compress stages 1–2 and use a 0–5, 5–10, 10–30, over-30 sequence — both are acceptable if the doses are correct.[2][4]
The four-stage status epilepticus protocol
Stage 1 (0–5 min) — stabilisation. ABCDE, oxygen, IV access, bedside glucose, bloods (including AED levels), ECG, and a full set of vital signs. Set up the protocol and call for senior and ICU help early.[2]
Stage 2 (5–20 min) — emergent IV benzodiazepine. Give IV lorazepam 4 mg (0.1 mg/kg in adults and children) as a slow push over up to 2 minutes; repeat once after 10 minutes if still seizing. Alternatives: IV diazepam 10 mg (shorter acting, higher recurrence risk — repeat at 5 to 10 min; risk of accumulation with repeated doses), or — if no IV access — IM midazolam 10 mg (0.2 mg/kg; the RAMPART trial showed IM midazolam at least as effective and safe as IV lorazepam in the pre-hospital setting, and it is the drug of choice when an IV cannot be quickly secured).[2][3]
Stage 3 (20–40 min) — urgent control with a second-line antiseizure drug. If still seizing after an adequate benzodiazepine (= established SE), give one of: IV levetiracetam 60 mg/kg (max 4.5 g) over 10 to 15 minutes; OR IV fosphenytoin 20 mg PE/kg (max 150 mg PE/min, with continuous cardiac monitoring — risk of hypotension and arrhythmia); OR IV sodium valproate 40 mg/kg (max 3 g, max 10 mg/kg/min; avoid in pregnancy and active liver disease). The ESETT trial (2019) established that these three agents are equally effective and safe at aborting established convulsive SE, stopping the seizure in roughly half of patients within 20 minutes of infusion — levetiracetam is often preferred in practice for ease of administration, with no cardiac monitoring required and no major drug interactions. Where fosphenytoin is unavailable (common in India), IV phenytoin 20 mg/kg at a maximum of 50 mg/min (slower in the elderly) with cardiac monitoring is an acceptable alternative.[2][6]
Stage 4 (over 40 min / refractory) — ICU and anaesthesia. Intubate (using a rapid-sequence induction with care to avoid a long-acting paralytic that obscures the neurological exam) and transfer to ICU. Start an anaesthetic infusion titrated with continuous EEG to burst-suppression or complete seizure abolition for 24 to 48 hours before a slow wean. Define refractory SE (ongoing despite benzodiazepine plus one adequate second-line agent) and super-refractory SE (ongoing or recurring over 24 hours after onset of anaesthetic infusion).[4]
Stage 2 — emergent benzodiazepine
- IV lorazepam 4 mg (0.1 mg/kg), repeat once at 10 min — preferred (longer CNS dwell time)
- IV diazepam 10 mg (0.15–0.2 mg/kg) — shorter acting, higher recurrence, accumulation risk
- IM midazolam 10 mg (0.2 mg/kg) if no IV (RAMPART); buccal/intranasal midazolam in community
Stage 3 — second-line AED
- IV levetiracetam 60 mg/kg (max 4.5 g) — no cardiac monitoring, no interactions, ESETT-preferred for ease
- IV fosphenytoin 20 mg PE/kg (max 150 mg PE/min, cardiac monitor) — or phenytoin 20 mg/kg max 50 mg/min
- IV valproate 40 mg/kg (max 3 g) — avoid in pregnancy and liver disease; (lacosamide, phenobarbital as alternatives)
Stage 4 — refractory anaesthesia
- Propofol: 1–2 mg/kg bolus then 2–10 mg/kg/h (watch propofol infusion syndrome over 48 h)
- Midazolam: 0.2 mg/kg bolus then 0.05–2 mg/kg/h (tachyphylaxis; rapid onset, short half-life)
- Thiopentone/pentobarbital: 5 mg/kg bolus then 1–5 mg/kg/h (deep burst-suppression, ileus, immunosuppression)
Paediatric weight-based doses: lorazepam 0.1 mg/kg IV, midazolam 0.5 mg/kg IM (or 0.2 mg/kg IV/buccal/intranasal), levetiracetam 60 mg/kg, fosphenytoin 20 mg PE/kg, valproate 40 mg/kg. In the community or pre-hospital setting, rectal diazepam (0.5 mg/kg) or buccal/intranasal midazolam (0.5 mg/kg) is used by caregivers and ambulance crews. Drugs with no current role in standard SE management include intramuscular phenytoin (harmful — erratic, painful absorption) and paraldehyde (obsolete, destroys plastic tubing).[2][4]
Adverse effects to monitor at every stage: benzodiazepines — respiratory depression, hypotension, sedation; phenytoin and fosphenytoin — hypotension, arrhythmia (PR and QRS widening), infusion-site reactions and purple-glove syndrome (phenytoin extravasation); valproate — thrombocytopenia, hyperammonaemia, hepatotoxicity, pancreatitis; propofol — propofol infusion syndrome (metabolic acidosis, rhabdomyolysis, cardiac failure) with prolonged high-dose use beyond 48 hours; midazolam — tachyphylaxis with prolonged infusion; thiopentone — hypotension, paralytic ileus, immunosuppression and prolonged ICU stay.[4]
Specific Subtypes & Scenarios
Non-convulsive SE (NCSE). Suspect it in any comatose or confused patient after a seizure, and confirm with EEG. Treat with an IV benzodiazepine trial or a non-sedating antiseizure drug (levetiracetam, lacosamide) rather than immediate anaesthesia — the goal is to abort the seizure without obscuring the neurological examination. Over-sedation is a real trap: it converts an assessable patient into a ventilated one and hides the very findings needed to guide management.[5]
Refractory and super-refractory SE. Once SE persists into stage 4, intubate, use an anaesthetic infusion (propofol, midazolam or thiopentone/pentobarbital) with continuous EEG, and titrate to burst-suppression or seizure abolition for 24 to 48 hours before a slow wean. If the cause is autoimmune (anti-NMDA-receptor encephalitis, anti-LGI1, anti-GAD), add immunotherapy early — IV methylprednisolone, IV immunoglobulin and plasma exchange — because untreated autoimmune SE is among the most refractory forms and responds to immunosuppression, not to escalating anaesthesia alone. The ketogenic diet is a recognised rescue therapy for super-refractory cases, and ketamine (an NMDA antagonist) infusion is increasingly used as a third- or fourth-line agent.[4]
Eclamptic SE. The drug of choice is IV magnesium sulphate (4 g loading over 5 to 10 minutes, then 1 to 2 g/h maintenance infusion, with monitoring of reflexes, respiratory rate and urine output), alongside obstetric planning for delivery — the definitive treatment of eclampsia is delivery of the fetus. Magnesium — not a benzodiazepine-first approach — is first-line for eclamptic seizures because it both controls the seizure and prevents recurrence; benzodiazepines (lorazepam) are added only if magnesium fails to terminate the convulsion. Avoid sodium valproate as a second-line agent in pregnancy.[4]
Alcohol-withdrawal SE. Give a benzodiazepine (IV lorazepam or diazepam) to terminate the seizure and IV thiamine (250 to 500 mg) before any glucose to prevent Wernicke encephalopathy, then continue a benzodiazepine loading regimen (e.g. symptom-triggered lorazepam or diazepam using CIWA-Ar) to prevent further withdrawal seizures and delirium tremens. [1]
Febrile SE in children. Abort with a benzodiazepine, treat the fever, and investigate for CNS infection (especially bacterial meningitis) with a low threshold for LP. A single febrile SE does not itself mandate long-term AED prophylaxis, but recurrent or atypical febrile SE, or a prolonged first episode, warrants neurology follow-up.[2]
Post-anoxic SE after cardiac arrest. Managed within targeted temperature management (32 to 36 degrees Celsius for 24 hours); carries a guarded prognosis, and continuous EEG is essential to detect myoclonic or non-convulsive SE, which may be the only sign of ongoing injury. Myoclonic SE post-arrest (Lance-Adams in survivors) is a distinct entity with its own prognosis.[4]
Complications & Pitfalls
Prolonged convulsive SE causes systemic complications that are themselves life-threatening: hypoxia and aspiration pneumonitis, lactic acidosis, hyperpyrexia (which worsens neuronal injury), rhabdomyolysis with acute kidney injury (and compartment syndrome), hyperkalaemia, disseminated intravascular coagulation, neurogenic pulmonary oedema, and fractures (shoulder dislocation, vertebral compression). Neurological complications include hippocampal injury and mesial temporal sclerosis, cognitive impairment, permanent focal neurological deficit, and a markedly increased risk of future epilepsy. Treatment-related complications include benzodiazepine-induced respiratory depression (necessitating intubation), phenytoin or fosphenytoin hypotension and arrhythmia, propofol infusion syndrome, prolonged ICU stay with nosocomial infection and venous thromboembolism, and the morbidity of prolonged anaesthesia.[4]
The key diagnostic pitfalls are four. First, missing NCSE in a comatose patient because no EEG was requested. Second, misdiagnosing PNES as refractory SE and escalating a non-epileptic patient to anaesthesia — the EEG would have been flat. Third, not treating a reversible precipitant (hypoglycaemia, hyponatraemia, infection) while escalating the pharmacological ladder. And fourth — the commonest and most harmful error — under-dosing the first benzodiazepine, which produces apparent "refractoriness" purely from an inadequate dose and drives premature escalation to anaesthesia. The corrective is simple: give the full first dose of lorazepam (4 mg in an adult), not a timid 1 or 2 mg.[5]
[1]Prognosis & Disposition
Mortality is over 20 percent overall, rising to 30 to 40 percent in refractory SE and higher still in the elderly and in anoxic aetiology. It is worst with an anoxic cause (post-cardiac-arrest myoclonic SE, where mortality can exceed 70 percent) and best with alcohol-withdrawal or AED non-adherence (often under 5 percent when the cause is reversed). Aetiology is the single most important determinant of outcome, ahead of duration and age — a fact examiners repeatedly test.[4]
The Status Epilepticus Severity Score (STESS) stratifies outcome at the bedside from four variables, each scored: [1]
STESS component
- Level of consciousness (worst): 0 = awake/reactive, 1 = confused/somnolent, 2 = stupor/coma, 3 = coma
- Worst seizure type: 0 = simple partial / absence, 1 = complex partial, 2 = generalised convulsive, 3 = non-convulsive / subtle under anaesthesia
- Age: 0 = under 65, 1 = 65 or over
- Prior seizures / known epilepsy: 0 = yes (a protective factor), 1 = no
Interpretation
- Range 0 to 6 (higher = worse)
- STESS 0 to 3 → good outcome likely (survival, return to baseline) — favour full treatment
- STESS 4 to 6 → poor outcome likely (death, severe disability) — but never used to withhold treatment in real time
- Validated across adult SE; less reliable in anoxic aetiology and in the elderly
Disposition. Refractory SE, intubated patients, those with GCS under 8, and the haemodynamically unstable need ICU. A patient whose SE is controlled early with a clearly reversible precipitant (e.g. a missed phenytoin dose) may be managed on a monitored ward after a period of observation. Long term, optimise chronic AED therapy and adherence before discharge, because the risk of recurrent SE and of new-onset epilepsy is elevated for months to years after an episode — brief counselling on adherence, seizure first-aid, and driving restrictions is part of safe discharge.[4]
Special Populations
Children use weight-based dosing (lorazepam 0.1 mg/kg IV; midazolam 0.5 mg/kg IM, or 0.2 mg/kg IV/buccal/intranasal; levetiracetam 60 mg/kg; fosphenytoin 20 mg PE/kg). In febrile SE always look for meningitis with a low threshold for LP, and consider pyridoxine (vitamin B6) deficiency in infants under 18 months with refractory SE. Rectal diazepam or buccal/intranasal midazolam is used by caregivers in the community.[2]
The elderly have higher mortality, commoner metabolic and vascular causes (stroke, haemorrhage, metabolic derangement in the context of polypharmacy and renal impairment), lower drug doses (reduced clearance and increased sensitivity), more comorbidity, and frequently present with NCSE as fluctuating confusion — easily mistaken for delirium and missed without a low EEG threshold.[4]
Pregnancy and eclampsia. Magnesium sulphate is first-line for eclamptic seizures; coordinate early with obstetrics, plan delivery, and avoid valproate as a second-line agent in pregnancy. Eclampsia can occur up to several weeks postpartum — a seizure in late pregnancy or the puerperium is eclampsia until excluded.[4]
Immunocompromised patients (HIV, transplant, chemotherapy) carry a high suspicion for CNS infection (toxoplasmosis, lymphoma, CMV, cryptococcal meningitis, progressive multifocal leukoencephalopathy) and for autoimmune or paraneoplastic encephalitis (anti-NMDA-receptor) as a cause of refractory SE. Image early, LP once safe, and send autoimmune panels.[4]
Hepatic or renal impairment requires dose adjustment: caution with valproate in liver disease (hepatotoxicity, hyperammonaemia); levetiracetam is renally cleared (reduce dose in CKD); phenytoin is highly protein-bound (request free phenytoin levels in uraemia, as total levels are misleading).[4]
Evidence, Guidelines & Regional Differences
RAMPART (2012) — IM vs IV for prehospital SE
N Engl J Med 2012;366:591-600
Multicentre randomised non-inferiority trial (Silbergleit et al.)
Key finding
In prehospital convulsive SE, IM midazolam (10 mg adults) terminated seizures more often and with no more adverse events than IV lorazepam. Take-home: when IV access is unavailable, IM midazolam is not a compromise — it is the drug of choice.
Practice change
IM midazolam is the drug of choice when IV access is unavailable.
ESETT (2019) — three second-line agents for established SE
N Engl J Med 2019;381:2103-2113
Randomised comparative trial (Kapur et al.)
Key finding
In benzodiazepine-refractory convulsive SE, levetiracetam 60 mg/kg, fosphenytoin 20 mg PE/kg and valproate 40 mg/kg were equally effective and safe — each stopped the seizure within 20 min in roughly half of patients. Levetiracetam is preferred for ease (no cardiac monitoring, no interactions).
Practice change
Levetiracetam, fosphenytoin and valproate are interchangeable second-line agents; levetiracetam preferred for ease.
The landmark evidence and guideline base is as follows:[1][2][4]
- ILAE 2015 operational definition (Trinka) introduced the t1/t2 time points — the basis for treating GCSE at 5 minutes and recognising injury risk at 30.
- AES 2016 evidence-based guideline (Glauser) formalised the staged protocol: IV lorazepam first-line, IM midazolam if no IV, levetiracetam/fosphenytoin/valproate as second-line.
- RAMPART (2012) established IM midazolam as the pre-hospital drug when IV access is unavailable.[3]
- ESETT (2019) established the equivalence of the three second-line agents.[6]
- UK — NICE NG217 (2022) and the older CG159 / NICE guideline on epilepsies: the staged protocol mirrors the AES guideline, with IV lorazepam 4 mg first-line, repeated once after 10 min, IM/buccal/intranasal midazolam if no IV, then levetiracetam, fosphenytoin (or phenytoin) or valproate as second-line, then anaesthesia for refractory SE. NICE emphasises treating the precipitant and considering NCSE in any patient who does not recover consciousness.
- US — AES 2016 guideline as above; the Neurocritical Care Society guideline (2012) adds detail on continuous EEG and ICU management of refractory SE.
- India — NFSEN (National Facility Support for Epilepsy) and the Indian Epilepsy Society broadly mirror international guidance; phenytoin is more available and affordable than fosphenytoin (so phenytoin 20 mg/kg at max 50 mg/min is widely used as second-line), and midazolam by infusion is commonly used for refractory SE. Neurocysticercosis and CNS tuberculosis must be considered as precipitants.
- Europe — ESETT-aligned practice, with growing use of levetiracetam as the preferred second-line agent and standardised ICU pathways for refractory and super-refractory SE.
The role of continuous EEG as the monitoring standard — in all refractory SE, all super-refractory SE, and in any comatose patient after GCSE to exclude NCSE — is now a near-universal guideline recommendation across regions.[4]
Exam Pearls
- SE = continuous seizure over 5 min OR two seizures without recovery — treat at 5 min, not 30.[1]
- Lorazepam 4 mg IV first (or IM midazolam 10 mg if no IV); repeat lorazepam once at 10 min. Give the full first dose — under-dosing is the commonest error.[2]
- Second-line (post-ESETT): levetiracetam 60 mg/kg OR fosphenytoin 20 mg PE/kg OR valproate 40 mg/kg — all equivalent; levetiracetam easiest.[6]
- Refractory = intubate, anaesthetic infusion (propofol / midazolam / thiopentone), continuous EEG to burst-suppression for 24–48 h before weaning.[4]
- Always check glucose, give thiamine in alcohol misuse, treat the precipitant, send cultures and AED levels.[4]
- Time-dependent pharmacoresistance: GABA-A receptors internalise, NMDA/AMPA upregulate — hence benzodiazepines lose effect the longer you wait.[4]
- Hippocampus (CA1/CA3) is the most vulnerable region; mesial temporal sclerosis is the long-term consequence.[5]
- NCSE in a comatose patient after GCSE = urgent EEG — do not assume the seizure is over just because motor activity stopped.[5]
- Eclamptic seizure = IV magnesium sulphate 4 g then 1–2 g/h, not benzodiazepine-first.[4]
- STESS 0–3 = good outcome; 4–6 = poor — but never used to withhold treatment in real time.[4]
- Aetiology is the strongest determinant of outcome (anoxic worst; non-adherence or alcohol-withdrawal best).[4]
- Give IV thiamine before glucose in the alcohol-misusing patient to prevent Wernicke encephalopathy.[4]
- Pyridoxine (vitamin B6) for isoniazid-induced SE; naloxone if opioid overdose suspected.[4]
Exam application bank (NEET-PG / INICET)
One-line answer
Status epilepticus (SE) is a continuous seizure lasting over 5 minutes, or recurrent seizures without recovery between them — a neurological emergency with mortality over 20 percent. The protocol is staged and time-critical: (1) IV lorazepam 4 mg (repeat once at 10 min); (2) IV levetiracetam 60 mg/kg or fosphenytoin 20 mg PE/kg or valproate 40 mg/kg; (3) refractory — ICU, intubation, anaesthetic infusion (propofol or midazolam) with continuous EEG. Always secure the airway, give oxygen, check and treat glucose and electrolytes, and find and treat the precipitant (AED non-adherence, infection, alcohol withdrawal, metabolic disturbance, stroke, tumour). [1]
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Status Epilepticus.
References
- [1]Trinka E, Cock H, Hesdorffer D, et al. A definition and classification of status epilepticus--Report of the ILAE Task Force on Classification of Status Epilepticus Epilepsia, 2015.PMID 26336950
- [2]Glauser T, Shinnar S, Gloss D, et al. Evidence-Based Guideline: Treatment of Convulsive Status Epilepticus in Children and Adults: Report of the Guideline Committee of the American Epilepsy Society Epilepsy Curr, 2016.PMID 26900382
- [3]Silbergleit R, Durkalski V, Lowenstein D, et al. Intramuscular versus intravenous therapy for prehospital status epilepticus N Engl J Med, 2012.PMID 22335736
- [4]Trinka E, Leitinger M. Management of Status Epilepticus, Refractory Status Epilepticus, and Super-refractory Status Epilepticus Continuum (Minneap Minn), 2022.PMID 35393970
- [5]Hirsch LJ, Gaspard N. Status epilepticus Continuum (Minneap Minn), 2013.PMID 23739110
- [6]Kapur J, Elm J, Chamberlain JM, et al. Randomized Trial of Three Anticonvulsant Medications for Status Epilepticus N Engl J Med, 2019.PMID 31774955