Obstetrics & Gynaecology · Obstetrics & Gynaecology
Cervical Cancer
Also known as Cervical carcinoma · Cancer of cervix · Squamous cell carcinoma of cervix · Cervical intraepithelial neoplasia · HPV-associated cancer
Cervical cancer arises at the cervical transformation zone from persistent infection with high-risk HPV (16/18), whose E6 and E7 oncoproteins disable the p53 and Rb tumour suppressors. Over 10 to 15 years a minority of persistent infections progress through CIN 1 to 3 to invasive carcinoma. Presentation: postcoital or intermenstrual bleeding. Diagnosis: cervical cytology and HPV testing, colposcopy, directed biopsy. FIGO 2018 staging is clinical and radiological. Early disease: radical hysterectomy (Wertheim) or fertility-sparing trachelectomy. Locally advanced: concurrent chemoradiotherapy (cisplatin + EBRT + brachytherapy). Metastatic: cisplatin, paclitaxel, bevacizumab (GOG-240). Largely preventable through HPV vaccination and organised screening.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Overview & Definition
Cervical cancer is a malignant epithelial tumour arising at the transformation zone of the cervix, the metaplastic squamocolumnar junction where the stratified squamous epithelium of the ectocervix meets the columnar epithelium of the endocervical canal. It is the fourth most common cancer in women worldwide, with an estimated 604,000 new cases and 342,000 deaths in 2020, and it remains the leading cause of cancer death in women across much of sub-Saharan Africa, South Asia, and Latin America.[1]
The defining biological fact, and the reason this cancer is unusual among solid tumours, is that it is virtually always caused by a persistent infection with high-risk human papillomavirus (HPV). HPV DNA is detectable in more than 99 percent of cervical carcinomas, and HPV types 16 and 18 alone account for about 70 percent of all cases worldwide.[2] Because the causal agent, the precursor lesion (CIN), and an effective vaccine are all known, cervical cancer is in principle a largely preventable and, if caught early, curable disease. The persistence of high mortality in low-resource settings reflects failures of screening access and treatment, not of biological understanding.
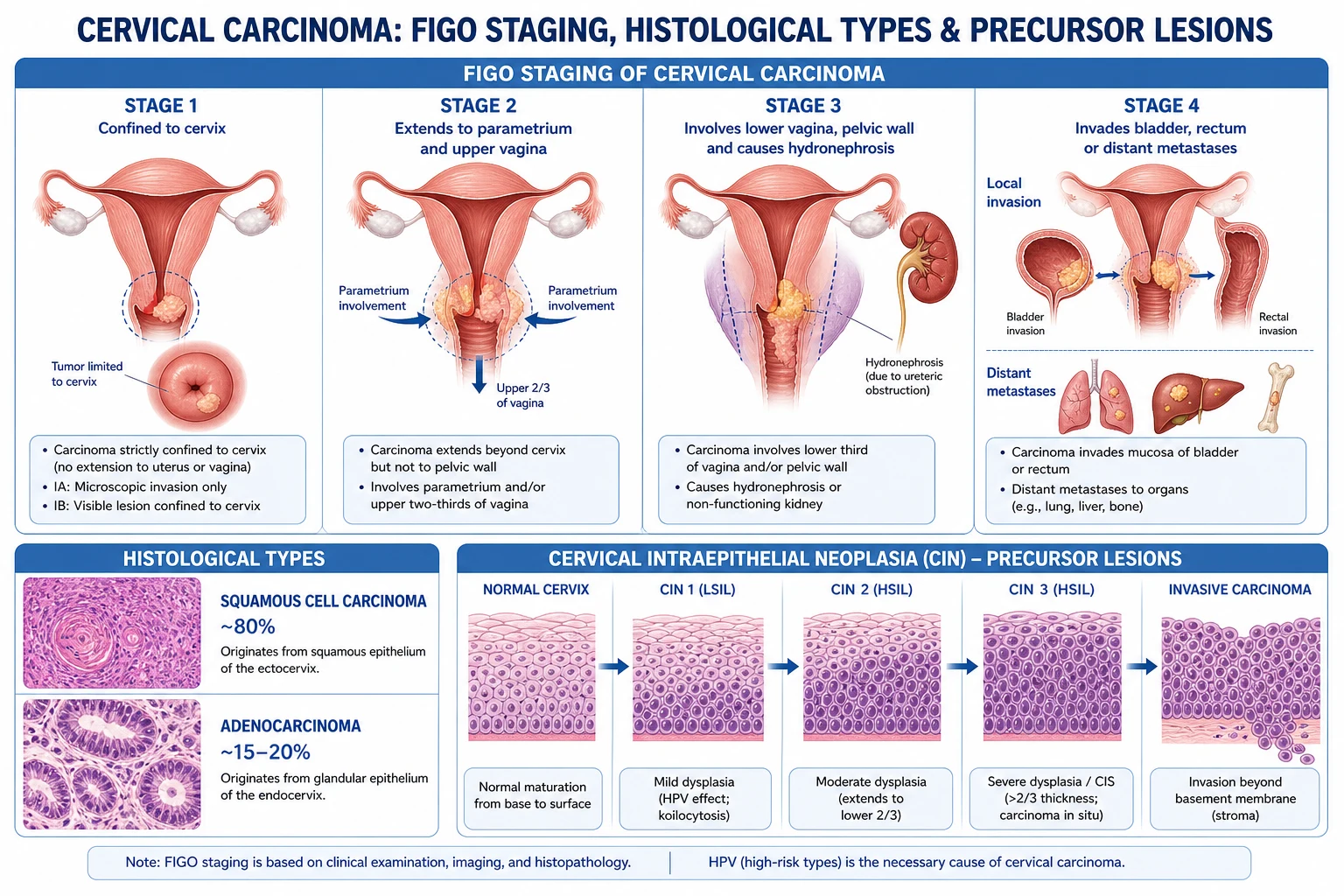
Squamous cell carcinoma accounts for roughly 80 percent of cases and arises from the squamous transformation zone. Adenocarcinoma accounts for 15 to 20 percent, arises from the endocervical glandular epithelium, is harder to detect with conventional cytology, and appears to be increasing in relative frequency in young women. Adenosquamous carcinoma and rare small-cell neuroendocrine carcinoma make up the remainder; the latter is biologically aggressive and managed like other small-cell tumours.[2]
Classification
Cervical neoplasia is classified along three independent axes — histology, the precursor (CIN) spectrum, and the FIGO 2018 stage — because each drives a different clinical decision: histology for prognosis and chemosensitivity, CIN for whether to treat or observe a screen-detected abnormality, and FIGO stage for whether the patient is a surgical or a chemoradiotherapy candidate.
[2]Histological
cell of origin
- **Squamous cell carcinoma** (about 80 percent) — from the transformation zone, keratinising or non-keratinising
- **Adenocarcinoma** (15 to 20 percent) — endocervical glands, often missed on cytology; includes mucinous and villoglandular subtypes
- **Adenosquamous carcinoma** — mixed glandular and squamous, intermediate prognosis
- **Small-cell neuroendocrine carcinoma** — rare, aggressive, HPV 18 linked, treated with etoposide plus cisplatin chemoradiotherapy
Pre-invasive (CIN)
precursor
- **CIN 1 (mild):** dysplasia confined to the lower one third of the epithelium; usual management is observation as most regress
- **CIN 2 (moderate):** lower two thirds; treatment with excision (LLETZ or cone) is usual, especially in women over 25
- **CIN 3 (severe or carcinoma in situ):** full-thickness dysplasia without basement-membrane breach; treatment required
- Reproducible regression of CIN 1 in roughly 60 percent, but untreated CIN 3 progresses to invasion in over 30 percent over 30 years
FIGO 2018
stage
- **Stage I:** confined to the cervix (IA microscopic, IB clinically visible, subdivided by size into IB1, IB2, IB3)
- **Stage II:** beyond the cervix but not to the pelvic wall or lower vagina (IIA upper vagina, IIB parametrium)
- **Stage III:** lower vagina, pelvic wall, hydronephrosis, or pelvic or para-aortic nodes (new IIIC1 or IIIC2)
- **Stage IV:** bladder or rectal mucosa (IVA) or distant metastases (IVB)
Cervical cancer — global burden (GLOBOCAN 2020)
Epidemiology & Risk Factors
Cervical cancer is the fourth most common cancer in women globally and the fourth leading cause of cancer death, after breast, colorectal, and lung cancer. Two-thirds of cases occur in countries classified as low or medium on the Human Development Index, and the burden tracks closely with the failure to deliver organised screening. In sub-Saharan Africa, parts of India, and Melanesia, cervical cancer is the commonest cancer in women; in several of these countries it kills more women than maternal causes.[1]
Peak incidence is in the fifth and sixth decades, but the precursor lesions appear much earlier — median age at CIN 3 detection is around 30 — which is why screening programmes begin in the mid-twenties. Adenocarcinoma disproportionately affects younger women and is the histology most often missed by cytology-based programmes.
[1]Because HPV is the necessary cause, every recognised risk factor works by either increasing exposure to HPV or reducing the probability that an established infection is cleared. The cofactors are best remembered as HPV exposure plus barriers to clearance:[2]
- HPV exposure: early age at first intercourse (under 17, when the transformation zone is most susceptible), multiple sexual partners, a partner with high-risk behaviour, other sexually transmitted infections (chlamydia, herpes simplex type 2) that inflame the cervical epithelium.
- Reduced HPV clearance: cigarette smoking (tobacco carcinogens concentrate in cervical mucus and depress local Langerhans-cell immunity), any cell-mediated immunosuppression (HIV, post-transplant, chronic glucocorticoids), long-term oral contraceptive use, and high parity — each of which roughly doubles the risk of progression per year of persistent infection.
- Access failure: low socioeconomic status, no organised screening, and geographic residence far from colposcopy services are the dominant determinants of who presents with invasive rather than screen-detected disease.
India: Cervical cancer is the second most common cancer in Indian women (after breast cancer) and India accounts for roughly one in four of the world's cervical cancer deaths. The drivers are low screening coverage (under 5 percent of eligible women have ever had a Pap smear), early marriage and sexual debut, high parity, poor genital hygiene, tobacco chewing, and limited HPV vaccine access. In this setting, visual inspection with acetic acid (VIA) followed by same-visit cryotherapy ("screen and treat") is recommended by the WHO as a low-cost, single-visit strategy that does not depend on cytology infrastructure. India's national Cervical Cancer Elimination Plan, aligned with the WHO 90-70-90 targets, is rolling out quadrivalent HPV vaccination for girls aged 9 to 14 alongside HPV-based screening for women aged 30 to 65.
[1]Sub-Saharan Africa: cervical cancer is the commonest cancer and the commonest cause of cancer death in women, amplified by high HIV prevalence. HIV-positive women have a two- to six-fold higher incidence, faster CIN-to-invasion progression, and require intensified screening from sexual debut.
[1]High-income settings (UK, USA, Australia): organised screening plus HPV vaccination have driven incidence down by more than half over 30 years; Australia is on track to be the first country to eliminate cervical cancer (incidence below 4 per 100,000) within the next decade.
Pathophysiology
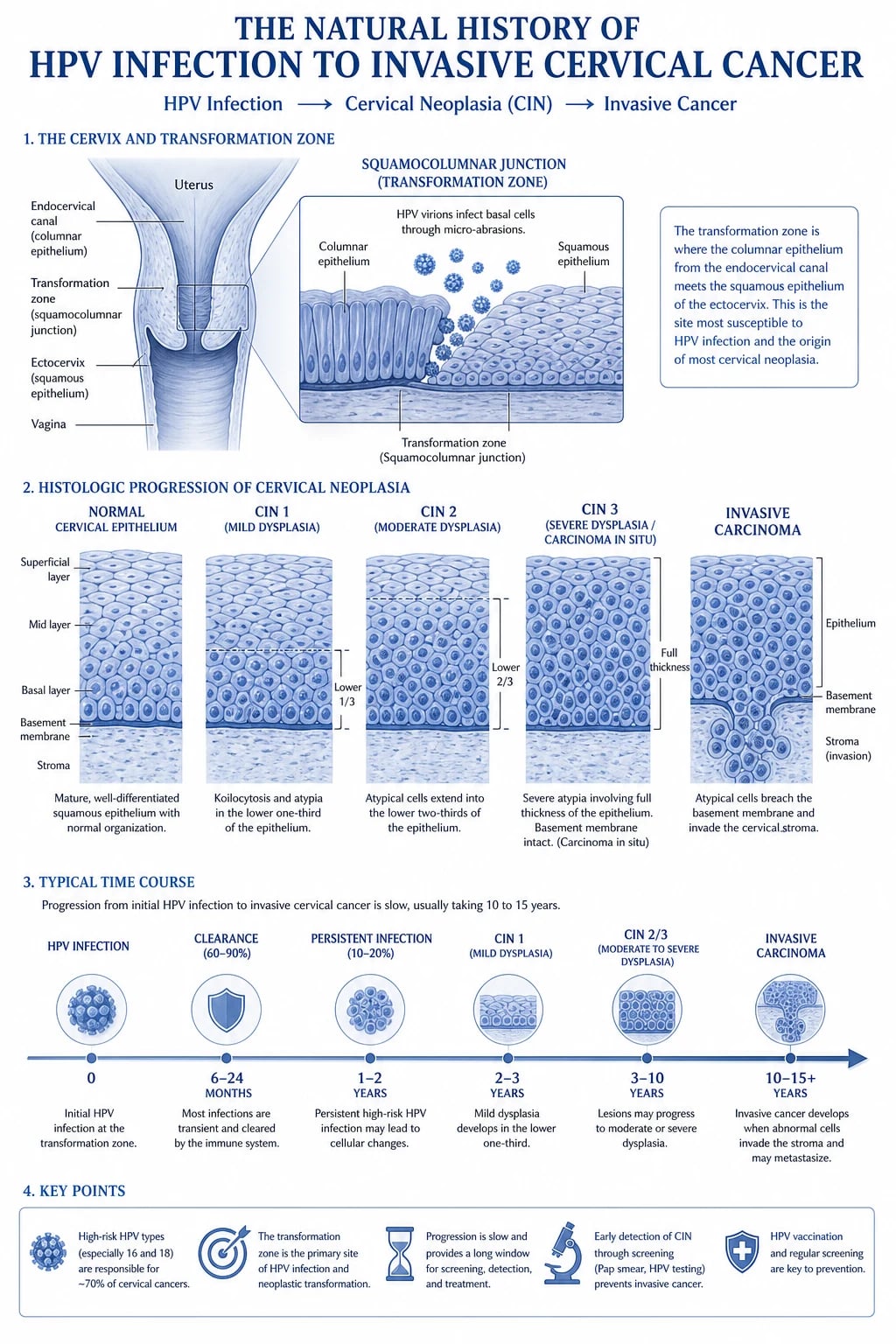
Cervical cancer is the paradigm of a virus-driven malignancy, and the molecular cascade from infection to invasion is one of the most thoroughly mapped in oncology. The chain has five links: entry, integration, oncoprotein hijacking of tumour suppressors, clonal progression through CIN, and stromal invasion.[2]
- Entry. During sexual contact, micro-abrasions expose the basal cells of the squamocolumnar junction to HPV. The virus binds alpha-6 integrin and heparan sulphate proteoglycans and enters the basal keratinocytes. The transformation zone is uniquely vulnerable because active squamous metaplasia provides a population of dividing cells the virus can exploit.
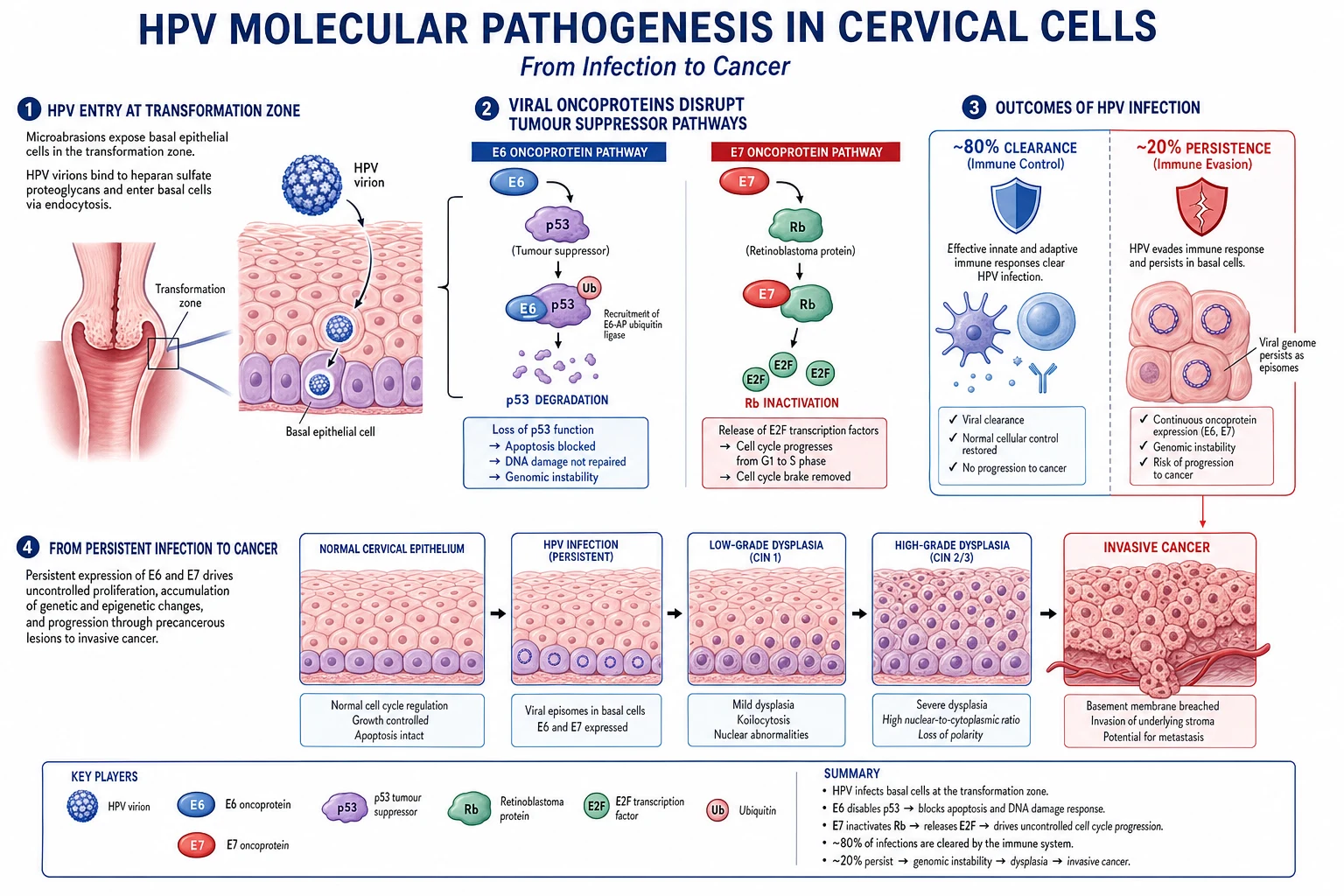
- Episomal persistence versus integration. In a productive infection the viral genome remains episomal (circular, free in the nucleus) and produces infectious virions as the keratinocyte matures. The decisive malignant event is integration of viral DNA into a host chromosome, which disrupts the viral E2 repressor and derepresses E6 and E7 transcription.
- E6 degrades p53. The E6 oncoprotein binds the E6-associated protein (E6-AP) ubiquitin ligase, which then polyubiquitinates p53 for proteasomal degradation. With p53 absent, the cell cannot trigger apoptosis in response to DNA damage; it also reactivates telomerase through hTERT upregulation, conferring replicative immortality.
- E7 inactivates Rb. The E7 oncoprotein binds the retinoblastoma protein (Rb) and the related pocket proteins p107 and p130, freeing E2F transcription factors and pushing the cell through the G1/S checkpoint regardless of DNA damage. The combined loss of p53-mediated apoptosis and Rb-mediated cell-cycle arrest produces uncontrolled proliferation with genomic instability.
HPV oncoproteins and their targets
E67
binds E6-AP and degrades p53 — apoptosis blocked (high-risk HPV only)
the guardian-of-the-genome tumour suppressor normally triggers apoptosis in damaged cells
binds and inactivates Rb — removes the G1/S cell-cycle brake, uncontrolled division
- CIN and progression. The proliferating, genetically unstable clone expands upward through the epithelium as cervical intraepithelial neoplasia: CIN 1 (lower one third), CIN 2 (lower two thirds), and CIN 3 (full thickness, synonymous with carcinoma in situ). The basement membrane is still intact, so there is no invasion.
- Invasion and spread. When the clone breaches the basement membrane it becomes invasive carcinoma, spreading by direct extension (into the parametrium, vagina, bladder, and rectum), lymphatic spread (first to the obturator, internal and external iliac pelvic nodes, then to the common iliac and para-aortic nodes), and, late, haematogenous spread to lung, liver, and bone. Ureteric obstruction producing hydronephrosis and renal failure is a common terminal event.
The clinical importance of this cascade is its tempo: the median time from incident HPV infection to invasive cancer is 10 to 15 years, and most (about 80 percent) HPV infections are cleared by cell-mediated immunity within one to two years. The long, detectable precursor phase is the biological window that makes cytology, HPV testing, and treatment of CIN effective at preventing cancer.
[2]Clinical Presentation
Symptoms track the anatomy of spread. Early invasive disease is often silent and is detected by screening, but as the tumour grows it bleeds on contact, then invades neighbouring structures.
[2] [2]Atypical presentations examiners test deliberately. A young woman on the oral contraceptive pill with intermenstrual bleeding is often dismissed as having a withdrawal bleed or ectropion; a Pap and speculum view are mandatory. An HIV-positive woman may present with rapidly progressive, multifocal disease within a few years of infection. A pregnant woman with postcoital bleeding may be labelled as a cervical ectropion of pregnancy — cervical cancer is the commonest malignancy in pregnancy, and any suspicious lesion is biopsied. An elderly, never-screened woman may present with a foul, blood-stained discharge and hydronephrosis from an advanced endocervical adenocarcinoma that cytology never caught.[2]
Differential Diagnosis
The differential of abnormal cervical bleeding or an abnormal-looking cervix splits into benign cervical lesions, other gynaecological cancers, and infectious causes. The history, speculum appearance, and a directed biopsy separate them.
[2]| Condition | Key distinguishing feature |
|---|---|
| Cervical ectropion (ectopy) | Benign, bright-red, glistening columnar epithelium visible around the os; common in adolescents, pregnancy, and on the combined pill; bleeds on contact but is not friable; cytology normal |
| Cervical polyp | A single, pedunculated, fleshy, freely mobile mass protruding from the os; benign on histology; easily avulsed |
| Cervicitis | Inflamed, oedematous cervix with mucopurulent discharge; positive chlamydia or gonorrhoea PCR; no mass lesion |
| Cervical intraepithelial neoplasia (CIN) | Pre-invasive; no basement-membrane breach; macroscopically normal cervix but acetowhite change on colposcopy; biopsy confirms |
| Endometrial cancer | Postmenopausal or perimenopausal bleeding; uterus may be enlarged; biopsy is from the endometrium (not the cervix); cervix appears normal |
| Metastatic tumour | Rarely a breast, stomach (Krukenberg), or ovarian primary deposits in the cervix; histology and a primary tumour identify it [2] |
Clinical & Bedside Assessment
The bedside assessment serves two purposes: to characterise the lesion (visible mass versus occult disease) and to clinically stage the tumour, because FIGO staging of cervical cancer is fundamentally a clinical-radiological exercise, not a surgical one.[11]
Speculum examination defines the macroscopic growth pattern: an exophytic tumour forms a friable, cauliflower-like mass on the ectocervix (the commonest squamous pattern); an endophytic tumour expands within the endocervical canal, producing a hard, barrel-shaped cervix that may be missed if only the ectocervix is inspected; and an ulcerative tumour destroys the cervical surface. A cervix that bleeds on light touch should be regarded as cancer until biopsy proves otherwise.
[11]Bimanual pelvic examination assesses cervical mobility (a fixed, rigid cervix means parametrial invasion, stage IIB or higher), the size and mobility of the uterus, adnexal masses, and parametrial thickening or nodularity. A formal examination under anaesthesia (EUA) is performed for staging, allowing a relaxed, pain-free assessment of parametrial and vaginal extension.
[11]Cystoscopy and proctoscopy are reserved for suspected advanced disease or symptoms referable to bladder or rectum; biopsy of any abnormal mucosa documents IVA disease. Pelvic node status is assessed radiologically, not by surgical sampling, in the FIGO 2018 system.[11]
Investigations
The investigation strategy has two phases: a screen-and-diagnose phase that finds the lesion and confirms histology, and a stage phase that defines tumour extent. Different tests are right at different points, and examiners expect you to know which.
[11]Screening tests are applied to asymptomatic women on a programme schedule:[7][9]
- Cervical cytology (Pap smear). Cells are scraped from the transformation zone with an Ayre's spatula and endocervical brush, fixed, and reported using the Bethesda system (negative for intraepithelial lesion or malignancy; atypical squamous cells of undetermined significance, ASC-US, or cannot exclude HSIL, ASC-H; low-grade squamous intraepithelial lesion, LSIL; high-grade squamous intraepithelial lesion, HSIL). Liquid-based cytology (LBC, e.g. ThinPrep) has replaced the conventional smear in most programmes — it gives cleaner slides and allows reflex HPV testing from the same vial. Cytology is highly specific (over 95 percent) but only moderately sensitive (50 to 75 percent for high-grade disease in a single round), which is why repeated screening and HPV triage matter.
- HPV DNA testing. Detects high-risk HPV types in cervical cells. It is markedly more sensitive than cytology and, crucially, a negative HPV test confers a much longer (5 to 10 year) low-risk interval. Four large European randomised trials showed that HPV-based screening detects high-grade CIN earlier and reduces invasive cervical cancer incidence compared with cytology.[7]
- HPV mRNA testing (e.g. Aptima) detects E6/E7 mRNA transcripts of high-risk HPV and has comparable sensitivity to DNA testing with slightly higher specificity.[8]
- Visual inspection with acetic acid (VIA). A naked-eye inspection of the cervix after 5 percent acetic acid, with immediate treatment of acetowhite lesions by cryotherapy ("screen and treat"). Recommended by the WHO for low-resource settings without cytology infrastructure.[2]
Diagnostic tests confirm histology once a screen is abnormal or a lesion is visible:[2]
- Colposcopy with directed biopsy is the definitive diagnostic test. A binocular colposcope magnifies the cervix 5- to 40-fold. Five percent acetic acid is applied — dysplastic cells with increased nuclear density turn white (acetowhite), and abnormal vascular patterns (punctuation, mosaic, atypical vessels) are mapped. Schiller's test uses Lugol's iodine: normal glycogenated squamous epithelium stains brown, while dysplastic epithelium (no glycogen) stays pale (iodine-negative). Directed punch biopsies are taken from the most abnormal areas.
- Cervical biopsy (punch) and endocervical curettage sample the ectocervix and endocervical canal respectively; the latter is essential when colposcopy is unsatisfactory or when an endocervical lesion is suspected.
- Cone biopsy (cold-knife cone or large loop excision of the transformation zone, LLETZ) is both diagnostic and therapeutic for CIN, microinvasive disease, or when colposcopy is inadequate — it provides a complete specimen with margins for histological depth-of-invasion measurement.
- Histopathology confirms squamous versus adenocarcinoma, grade, lymphovascular space invasion, and depth of stromal invasion — all of which refine stage and management.
Staging investigations follow FIGO 2018, which is clinical and radiological:[11]
- Pelvic MRI is the best single test for local extent — parametrial invasion, vaginal involvement, tumour volume, and pelvic node status — and is now used to assign the radiological components of stage.
- CT chest, abdomen, and pelvis screens for distant metastases and hydronephrosis.
- 18F-FDG PET-CT is increasingly used for locally advanced disease; it is the most sensitive modality for detecting nodal and distant disease and influences radiotherapy planning.
- Cystoscopy and proctoscopy with biopsy confirm bladder or rectal mucosal involvement (stage IVA).
- Serum — full blood count (anaemia from chronic bleeding), urea and electrolytes and creatinine (renal function, hydronephrosis), and liver function tests.
Management — Resuscitation
Cervical cancer is rarely a time-critical emergency, but two scenarios demand immediate action. The first is life-threatening vaginal haemorrhage from an advanced, necrotic tumour, managed with firm vaginal packing (soaked in tranexamic acid or Monsel's solution), fluid resuscitation and cross-matched blood, urgent gynaecology-oncology referral, and, if uncontrolled, transarterial uterine artery embolisation or emergency palliative radiotherapy, which is highly effective at haemostasis. The second is obstructive uropathy from ureteric compression causing uraemia and hyperkalaemia — a nephrostomy or stent buys time for definitive chemoradiotherapy, which often shrinks the tumour and relieves the obstruction. Uraemic or septic presentation with a fungating pelvic mass is a recognised terminal pathway and warrants palliative-care involvement.[11]
Management — Definitive & Stepwise
The single decision that decides everything else is whether the tumour is early (operable) or locally advanced (chemoradiotherapy). The watershed sits at FIGO IB and depends on tumour size, because radical surgery for tumours over roughly 2 cm carries higher recurrence, and the LACC trial showed minimally-invasive radical hysterectomy is inferior to open.[13]
Early disease — surgery (Stage IA to IB1, and selected IIA1)
Surgical management is stratified by depth of invasion and tumour size.[11][13]
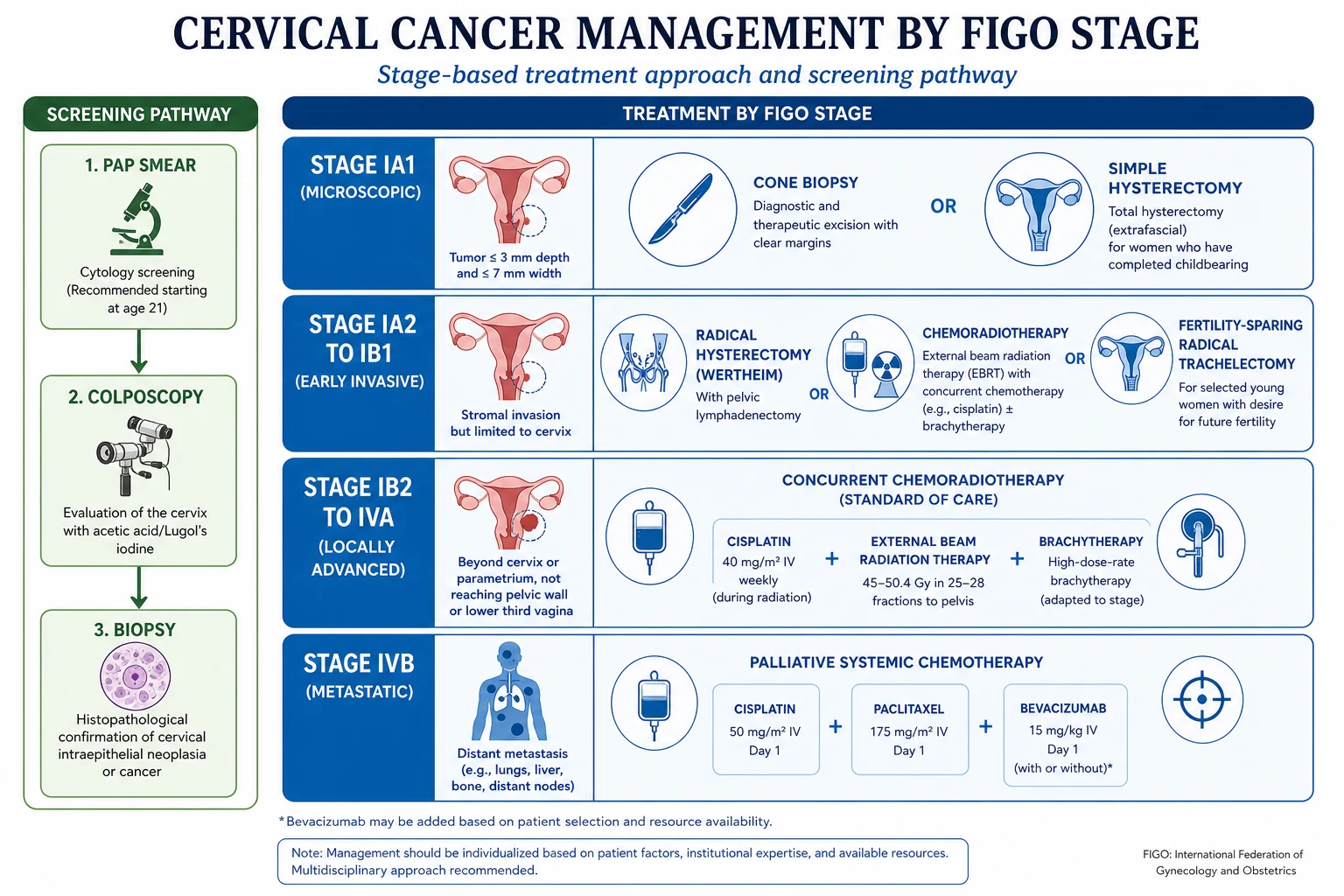
- Stage IA1 without lymphovascular space invasion: cone biopsy (cold-knife cone or LLETZ) with clear margins is curative and preserves fertility. If the family is complete, simple (extrafascial) hysterectomy is definitive.
- Stage IA1 with lymphovascular space invasion, or IA2: modified radical hysterectomy with pelvic lymphadenectomy, or cone biopsy plus pelvic lymphadenectomy for the fertility-sparing candidate.
- Stage IB1 (lesion up to 2 cm) and IIA1: radical hysterectomy (Wertheim's operation) with bilateral pelvic lymphadenectomy. The Wertheim operation removes the uterus, cervix, upper one third of the vagina, parametrium, and uterosacral and cardinal ligaments en bloc, with systematic pelvic node dissection (external, internal iliac, obturator, and common iliac chains). Following the LACC trial, the open abdominal approach is standard; minimally-invasive radical hysterectomy is associated with higher recurrence and lower disease-free survival and is no longer recommended for early-stage disease.[13]
Dose
Fertility-sparing surgery — radical trachelectomy — is offered to young women with stage IA1 with LVSI, IA2, or IB1 (tumour up to 2 cm) who wish to preserve fertility. The cervix, parametrium, and upper vagina are removed with pelvic lymphadenectomy, but the uterine body and ovaries are preserved and a permanent cervical cerclage is placed to support future pregnancies. Systematic review evidence shows oncologic outcomes comparable to radical hysterectomy in well-selected patients, with live-birth rates of 60 to 70 percent thereafter, though second-trimester loss and prematurity are increased.[15]
Locally advanced disease — concurrent chemoradiotherapy (Stage IB2 to IVA)
For tumours larger than 2 cm, those with parametrial invasion, lower-vaginal involvement, nodal disease, or adjacent-organ involvement, concurrent chemoradiotherapy is the standard of care and is superior to radiotherapy alone — an individual-patient-data meta-analysis of 18 randomised trials showed a 6 percent absolute improvement in 5-year survival with the addition of concurrent cisplatin.[12]
The chemoradiotherapy regimen combines external beam radiotherapy, brachytherapy, and concurrent cisplatin:[12][14]
Dose
Metastatic and recurrent disease — systemic therapy (Stage IVB)
For distant metastases or pelvic relapse not amenable to radiotherapy, treatment is palliative systemic chemotherapy. The GOG-240 trial established the triplet of cisplatin, paclitaxel, and bevacizumab (an anti-VEGF monoclonal antibody) as the standard first-line regimen, with a median overall survival of about 17 months versus 13 months for chemotherapy alone. Bevacizumab adds hypertension, thromboembolism, and fistula risk.[14]
Dose
Palliative radiotherapy controls bleeding, pelvic pain, and bone metastases; a pelvic exenteration (anterior, posterior, or total) is occasionally curative for a central pelvic recurrence after chemoradiotherapy in a carefully selected, fit patient.
[11]CIN management (the precursor)
Because most screen-detected disease is CIN, its treatment is examinable. CIN 1 is observed (regression rate about 60 percent) with repeat testing in 12 months, except in older or non-compliant women. CIN 2 and CIN 3 are treated by excision — large loop excision of the transformation zone (LLETZ) in most cases, or cold-knife cone biopsy when the lesion is endocervical, the transformation zone is not fully visible, or microinvasion is suspected. Excision treats the lesion and gives a histological specimen for depth of invasion. Ablative methods (cryotherapy, laser) are acceptable only when colposcopy is satisfactory and invasion has been excluded.[2]
FIGO 2018 Staging — Treatment by Stage
The 2018 FIGO revision (the Bhatla revision) is the staging system in current use. It is clinical and radiological, may use any imaging modality, and subdivided stage IB by tumour size (IB1 up to 2 cm, IB2 over 2 to 4 cm, IB3 over 4 cm) and introduced nodal substages (IIIC1 pelvic nodes, IIIC2 para-aortic nodes), reflecting the prognostic weight of node status made visible by modern imaging.[11]
Stage-specific management
Specific Subtypes & Scenarios
Adenocarcinoma and adenosquamous carcinoma are managed with the same stage-driven algorithm as squamous carcinoma, but they are less chemosensitive and radiation-sensitive and carry a slightly worse stage-for-stage prognosis. They are also the lesions most often missed by cytology, which is why HPV-based primary screening (which detects the causative agent regardless of morphology) has shifted the field.
[2]Small-cell neuroendocrine carcinoma of the cervix is rare, biologically aggressive, and linked to HPV 18. It metastasises early and is managed with etoposide plus cisplatin chemoradiotherapy and more extensive nodal coverage, paralleling small-cell lung cancer.
[2]Cervical cancer in pregnancy is the commonest malignancy diagnosed in pregnancy. The diagnosis is made on Pap and biopsy of any suspicious lesion (a biopsy during pregnancy is safe); a cone biopsy is deferred to the second trimester if essential, to reduce the risk of haemorrhage and pregnancy loss. Management is individualised and multidisciplinary: small early-stage tumours may be monitored until fetal maturity; locally advanced disease may require chemoradiotherapy during pregnancy (chemotherapy is avoided in the first trimester but cisplatin is relatively safe after the first trimester); the route and timing of delivery depend on stage, with caesarean preferred if the tumour is bulky to avoid haemorrhage and obstructed labour.[11]
Cervical cancer in HIV-positive women is an AIDS-defining illness. HPV clearance is impaired, CIN progresses faster, recurrence after treatment is higher, and squamous intraepithelial lesions are more common. Antiretroviral therapy reduces but does not eliminate the risk. HIV-positive women should be screened from sexual debut and more frequently (some guidelines recommend twice-yearly cytology), and any CIN is treated aggressively.[2]
Complications & Pitfalls
Complications fall into disease-related, treatment-related, and psychosocial groups, and examiners test the distinction between them.
[11]Disease complications are the consequences of local invasion and metastasis: ureteric obstruction and renal failure (a leading cause of death), vesicovaginal or rectovaginal fistula from bladder or rectal invasion, lower-limb lymphoedema and deep vein thrombosis from venous and lymphatic compression, severe anaemia from chronic tumour bleeding, and pelvic pain from nerve involvement.
[11]Surgical complications of radical hysterectomy include bladder atony and long-term voiding dysfunction (from autonomic nerve damage — reduced by nerve-sparing techniques), ureteric injury and ureterovaginal fistula, lymphocyst and lymphoedema after pelvic lymphadenopathy dissection, sexual dysfunction, and ovarian failure if oophorectomy is performed. After LACC, the open approach is now standard to avoid the recurrence risk of the minimally-invasive route.[13]
Radiotherapy complications are divided into acute and late. Acute effects include radiation proctitis and cystitis, diarrhoea, skin desquamation, and bone-marrow suppression from pelvic-field irradiation. Late effects include vaginal stenosis and atrophy, radiation enteritis with stricture or fistula, radiation cystitis and haemorrhagic cystitis, ovarian failure (permanent infertility if ovaries are in field, hence ovarian transposition before chemoradiotherapy in young women), and a small second-malignancy risk decades later. Concurrent cisplatin adds nausea, nephrotoxicity, ototoxicity, and myelosuppression.[12]
Bevacizumab-specific complications in metastatic disease include hypertension, proteinuria, arterial thromboembolism, impaired wound healing, and gastrointestinal or genitourinary fistula — the last is a particular concern in irradiated pelvises.[14]
The classic pitfall is dismissing postcoital bleeding as a cervical ectropion or a side-effect of the oral contraceptive pill in a young woman without performing a speculum examination, a Pap, and (if any lesion is visible) a biopsy. A second pitfall is relying on cytology to exclude an endocervical adenocarcinoma, which can be cytology-negative. A third is offering minimally-invasive radical hysterectomy after LACC.
[13]Prognosis & Disposition
Prognosis is driven above all by stage, then by tumour size, nodal status, depth of invasion, lymphovascular space invasion, and histology. The quoted five-year survival figures, by FIGO 2018 stage, are approximately:[11]
Five-year survival by FIGO 2018 stage
Disposal. A woman with early disease treated surgically is followed up with vault cytology and clinical examination at six-monthly to annual intervals for two to five years. A woman treated with chemoradiotherapy is followed clinically and with MRI for response. Suspected recurrence — most often within two years and at the pelvic vault or nodes — is investigated with imaging and biopsy; isolated central pelvic recurrence after chemoradiotherapy may be curable with pelvic exenteration. All patients merit early psychosocial and sexual-health support, and younger women need explicit discussion of fertility and early menopause before treatment.[11][14]
Special Populations
Young women desiring fertility. For stage IA1 with clear margins, cone biopsy preserves fertility. For stage IA2 or IB1 with a tumour up to 2 cm, radical trachelectomy with pelvic lymphadenectomy is the fertility-sparing option of choice, with live-birth rates of 60 to 70 percent thereafter and a permanent cerclage placed at the time of surgery; deliveries are usually by caesarean, and prematurity and second-trimester loss are the principal risks.[15]
HIV-positive women. Cervical cancer is AIDS-defining; screening begins at sexual debut and is more frequent; CIN is treated aggressively because recurrence rates are higher; antiretroviral therapy is essential to restore cell-mediated immunity and HPV clearance.[2]
Pregnant women. Diagnosis is by Pap and biopsy; cone biopsy is second-trimester if essential; management is multidisciplinary and individualised, balancing gestational age, stage, and the mother's wishes (see Subtypes).[11]
Post-transplant and immunosuppressed women are managed like HIV-positive women, with intensified screening from a young age.
[2]Elderly, never-screened women often present with advanced, cytology-negative adenocarcinoma; HPV-based screening and a low threshold for biopsy of any abnormal-looking cervix are essential.
[2]Evidence, Guidelines & Regional Differences
The evidence base for cervical cancer prevention and treatment is unusually mature, built on a small number of landmark trials that reshaped screening, vaccination, and radiotherapy.
[11]Key finding
Key finding
Key finding
Key finding
Key finding
Vaccination evidence. The PATRICIA trial established that the bivalent HPV 16/18 AS04-adjuvanted vaccine (Cervarix) is highly efficacious against HPV 16/18 infection and CIN 2+ caused by those types. The nonavalent vaccine (Gardasil 9) adds coverage of five further high-risk types (31, 33, 45, 52, 58) and prevents around 90 percent of cervical cancers. A Cochrane review confirmed that prophylactic HPV vaccines protect against cervical precancer associated with vaccine types, with no serious safety signal.[3][4][5][6]
Bivalent (Cervarix)
HPV 16, 18
- AS04 adjuvant (MPL)
- Prevents about 70 percent of cervical cancer
- Discontinued in many markets; superseded by Gardasil 9
Quadrivalent (Gardasil)
HPV 6, 11, 16, 18
- Adds low-risk types 6 and 11 (90 percent of genital warts and recurrent respiratory papillomatosis)
- Aluminium adjuvant
- Widely used in national programmes
Nonavalent (Gardasil 9)
HPV 6, 11, 16, 18, 31, 33, 45, 52, 58
- Covers about 90 percent of cervical cancer-causing types plus genital warts
- Current vaccine of choice where available
- Virus-like particle (VLP) subunit vaccine — non-infectious
Vaccination schedule. Given ideally before sexual debut (age 9 to 14) as a two-dose schedule at 0 and 6 to 12 months. A three-dose schedule (0, 2, and 6 months) is given from age 15 to 26, in immunocompromised individuals regardless of age, and to males in gender-neutral programmes. Catch-up vaccination to age 26 is recommended for those not vaccinated earlier; vaccination beyond 26 is individualised.[5][6]
Screening evidence and regional deltas differ between national programmes, and examiners reward knowing the local numbers.
[9] [9]WHO Cervical Cancer Elimination Strategy (2020). The 194 WHO member states adopted the 90-70-90 targets: 90 percent of girls fully vaccinated with HPV vaccine by age 15, 70 percent of women screened with a high-performance test (HPV) by age 35 and again by 45, and 90 percent of women with identified disease treated (90 percent of women with precancer treated, and 90 percent of women with invasive cancer managed). Modelling shows that reaching these targets could reduce cervical cancer mortality by 42 percent by 2045 and put elimination (under 4 cases per 100,000 women) within reach this century.
Controversies. Whether HPV self-sampling at home should become the programme default (it raises uptake), whether to extend screening beyond age 65 in under-screened cohorts, how to manage HPV-positive, cytology-negative women (12-month repeat versus immediate colposcopy versus methylation triage), and whether men should be vaccinated universally versus through herd protection are all live debates. The decline of cytology and rise of HPV testing is the dominant contemporary shift.[8]
Prevention
Because cervical cancer has a single necessary viral cause, a detectable precursor, and an effective vaccine, prevention is the area where medicine has most to offer. Prevention has three pillars: vaccination, screening, and treatment of CIN.
[2]HPV vaccination. The nonavalent Gardasil 9 is the current vaccine of choice, given before sexual debut (age 9 to 14, two doses) with catch-up to 26 (three doses). Real-world programme data show substantial herd protection and an 80 percent-plus reduction in HPV 16/18 infection in vaccinated cohorts.[5][6]
Screening. Organised HPV-based screening (UK, US, Australia, much of Europe) detects CIN before it becomes invasive; VIA-based screen-and-treat is the WHO-endorsed alternative for low-resource settings. The key principle is that screening only works if it is organised, population-based, and accompanied by follow-up and treatment.[7][9]
Treatment of CIN closes the loop — LLETZ or cone biopsy for CIN 2 and 3 prevents progression to cancer, and is the mechanism by which screening saves lives.
[2]Prevention cascade — from vaccine to treated CIN
Two non-negotiable messages. First, vaccinated women still need screening — the vaccine covers about 90 percent of cancer-causing types, not all. Second, smoking cessation reduces the rate of HPV persistence and CIN progression, and is a modifiable risk factor that should be addressed at every visit.
[6]Exam Pearls
- HPV 16 and 18 cause about 70 percent of cervical cancer; the nonavalent vaccine covers about 90 percent by adding types 31, 33, 45, 52, and 58.[2][5]
- E6 degrades p53; E7 inactivates Rb — high-risk HPV only. Remember E6 to 6 letters (p53), E7 to 7 letters (Rb... actually R b is two) — use the Mnemonic instead: E6 hits p53, E7 hits Rb.[2]
- Postcoital bleeding is cervical cancer until proven otherwise — Pap, speculum view, and directed biopsy of any visible lesion.[2]
- Squamous 80 percent, adenocarcinoma 15 to 20 percent — adenocarcinoma is the one missed by cytology.[2]
- Colposcopy with directed biopsy is the definitive diagnostic test; cytology is the screening test.[2]
- CIN 1 mild (lower one third), CIN 2 moderate (lower two thirds), CIN 3 severe or carcinoma in situ (full thickness); CIN 1 observed, CIN 2 and 3 treated with LLETZ or cone.[2]
- FIGO staging is clinical and radiological, not surgical, and uses any imaging; the 2018 revision subdivided IB by size (IB1, IB2, IB3) and added nodal substages IIIC1 (pelvic) and IIIC2 (para-aortic).[11]
- Stage IA1 (under 3 mm invasion): cone biopsy or simple hysterectomy. Stage IA2 to IB1: radical hysterectomy (Wertheim) plus pelvic lymphadenectomy, or trachelectomy for fertility. Stage IB2 to IVA: concurrent chemoradiotherapy. Stage IVB: palliative cisplatin, paclitaxel, bevacizumab (GOG-240).[11][14]
- Concurrent chemoradiotherapy beats radiotherapy alone for locally advanced disease (CCCMAC); open radical hysterectomy beats minimally invasive (LACC).[12][13]
- HPV vaccine given before sexual debut prevents most cancer; vaccinated women still need screening.[5][6]
- HIV-positive women progress faster, present later, and need intensified screening from sexual debut.[2]
- The one-liner: postcoital bleeding plus a friable cervix — biopsy before you theorise.
References
- [1]Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin, 2021.PMID 33538338
- [2]de Sanjose S, Quint WG, Alemany L, et al. Human papillomavirus types in 115,789 HPV-positive women: a meta-analysis from cervical infection to cancer. Int J Cancer, 2012.PMID 22323075
- [3]Arbyn M, Xu L, Simoens C, Martin-Hirsch PPL. Prophylactic vaccination against human papillomaviruses to prevent cervical cancer and its precursors. Cochrane Database Syst Rev, 2018.PMID 29740819
- [4]Paavonen J, Naud P, Salmeron J, et al. (PATRICIA Study Group). Efficacy of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine against cervical infection and precancer caused by oncogenic HPV types (PATRICIA): final analysis of a double-blind, randomised study in young women. Lancet, 2009.PMID 19586656
- [5]Joura EA, Giuliano AR, Iversen OE, et al. A 9-valent HPV vaccine against infection and intraepithelial neoplasia in women. N Engl J Med, 2015.PMID 25693011
- [6]Drolet M, Benard E, Perez N, et al. Population-level impact and herd effects following the introduction of human papillomavirus vaccination programmes: updated systematic review and meta-analysis. Lancet, 2019.PMID 31255301
- [7]Ronco G, Dillner J, Elfstrom KM, et al. Efficacy of HPV-based screening for prevention of invasive cervical cancer: follow-up of four European randomised controlled trials. Lancet, 2014.PMID 24192252
- [8]Arbyn M, Roysters M, Cuschieri K, et al. Accuracy and effectiveness of HPV mRNA testing in cervical cancer screening: a systematic review and meta-analysis. Lancet Oncol, 2022.PMID 35709810
- [9]Curry SJ, Krist AH, Owens DK, et al. (US Preventive Services Task Force). Screening for Cervical Cancer: US Preventive Services Task Force Recommendation Statement. JAMA, 2018.PMID 30140884
- [10]Fontham ETH, Wolf AMD, Church TR, et al. Cervical cancer screening for individuals at average risk: 2020 guideline update from the American Cancer Society. CA Cancer J Clin, 2020.PMID 32729638
- [11]Bhatla N, Berek JS, Cuello Fredes M, et al. Revised FIGO staging for carcinoma of the cervix uteri. Int J Gynaecol Obstet, 2019.PMID 30656645
- [12]Chemoradiotherapy for Cervical Cancer Meta-Analysis Collaboration (CCCMAC). Reducing uncertainties about the effects of chemoradiotherapy for cervical cancer: a systematic review and meta-analysis of individual patient data from 18 randomized trials. J Clin Oncol, 2008.PMID 19001332
- [13]Ramirez PT, Frumovitz M, Pareja R, et al. Minimally Invasive versus Abdominal Radical Hysterectomy for Cervical Cancer. N Engl J Med, 2018.PMID 30380365
- [14]Tewari KS, Sill MW, Long HJ III, et al. Bevacizumab for advanced cervical cancer: final overall survival and adverse event analysis of a randomised, controlled, open-label, phase 3 trial (Gynecologic Oncology Group 240). Lancet, 2017.PMID 28756902
- [15]Sidonie M, et al. Oncologic, pregnancy, and reproductive outcomes of fertility-sparing surgery in early-stage cervical cancer: a systematic review. Surg Oncol, 2026.PMID 42114502