Obstetrics and Gynaecology · Obstetrics and Gynaecology
Contraception
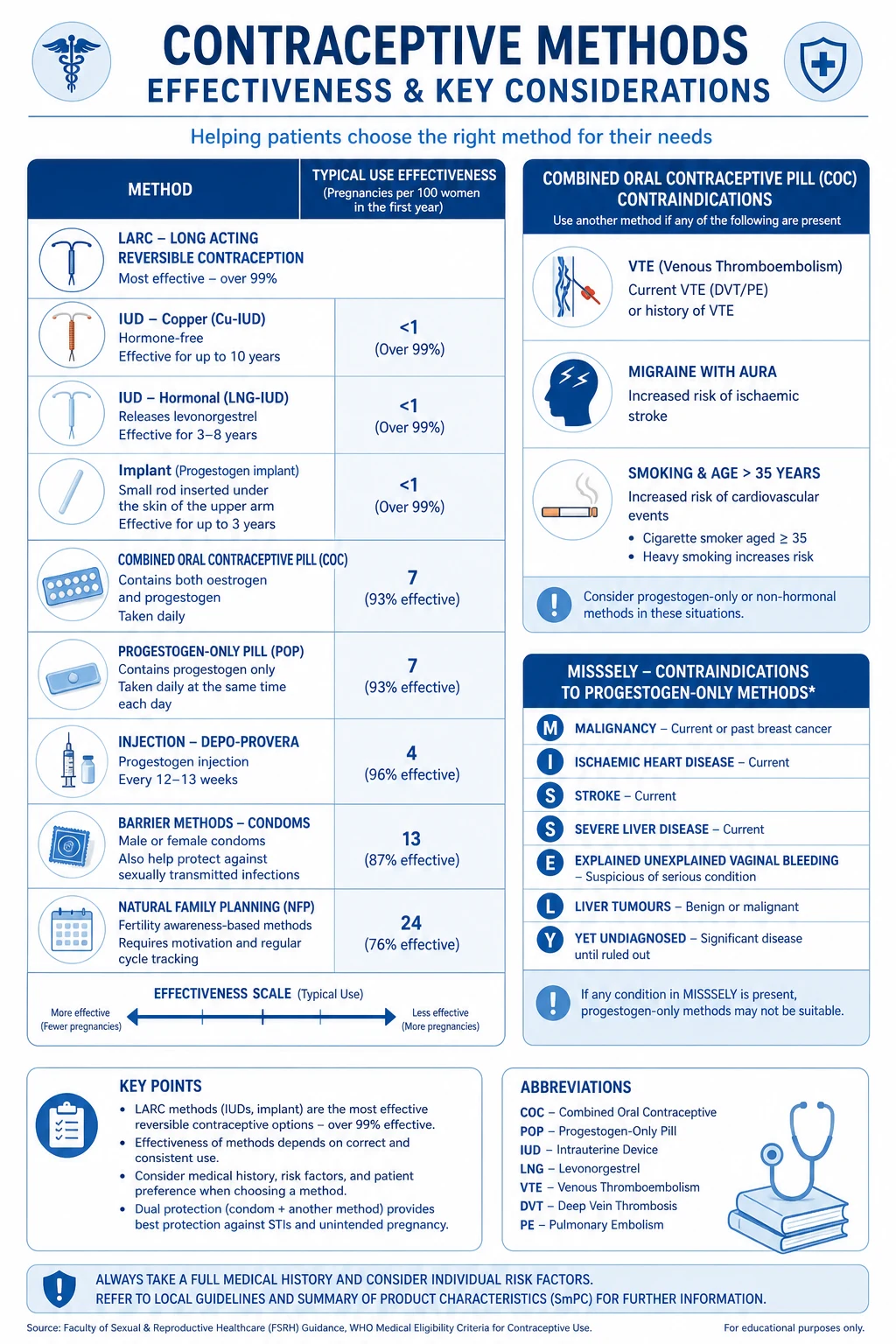
Contraception methods span hormonal (combined oral contraceptive pill, progestogen-only pill, implant, injectable, hormonal intrauterine system), intrauterine (copper IUD), barrier (condom, diaphragm), natural (fertility awareness, lactational amenorrhoea), emergency contraception, and permanent sterilisation. Choice depends on efficacy, safety, side effects, reversibility, coital independence, age, comorbidities, and patient preference. Long-acting reversible contraception (LARC) — copper IUD, LNG-IUS, implant — is most effective and offered first-line. UK Medical Eligibility Criteria (UKMEC) categorise every method from 1 (no restriction) to 4 (unacceptable risk) across medical conditions.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags

Overview & Definition
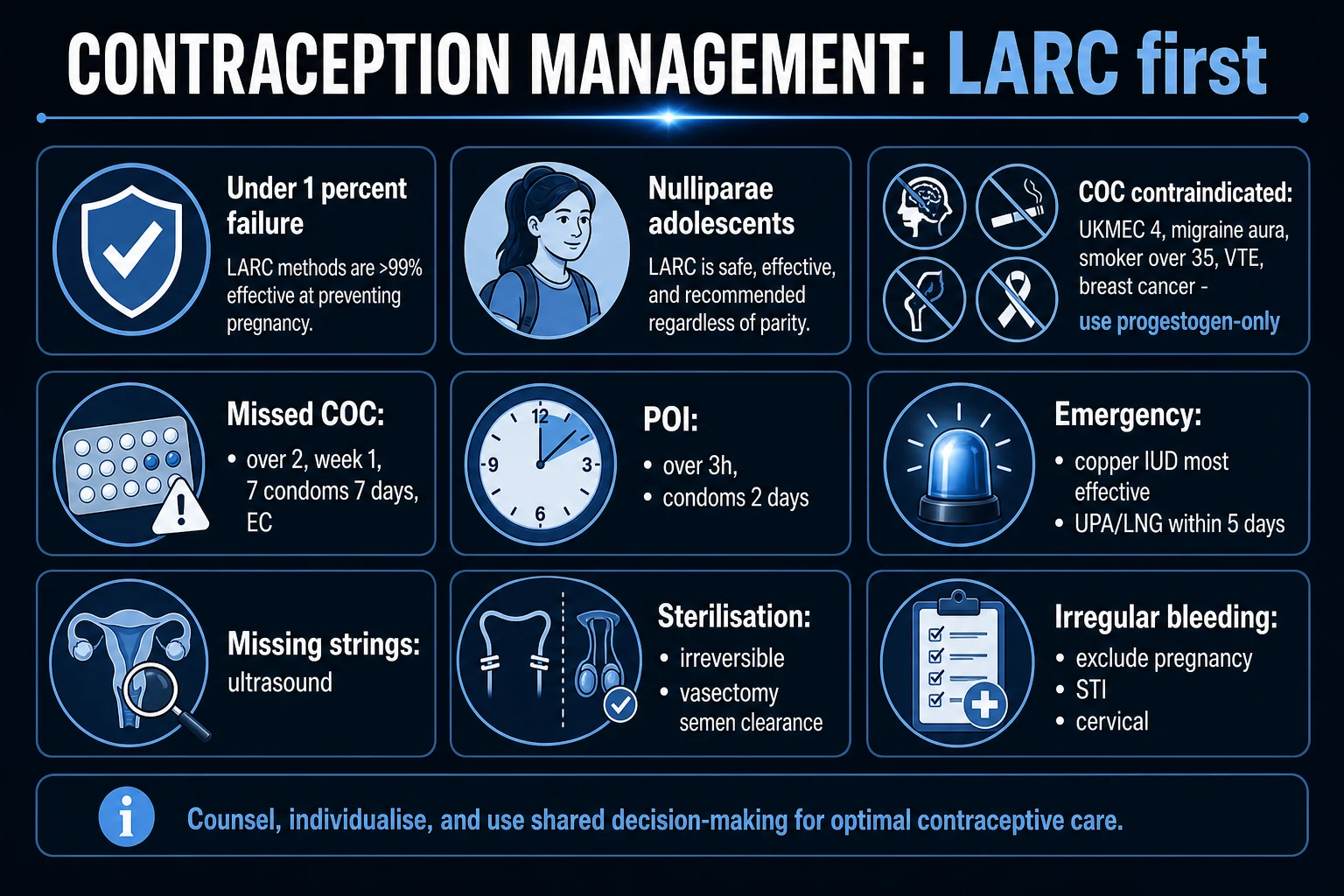
Contraception is the intentional prevention of pregnancy following unprotected sexual intercourse (UPSI). Method choice balances efficacy, safety, side-effect profile, reversibility, coital independence, acceptability, cost and the woman's medical, obstetric and sexual history. The guiding clinical principle in UK and international guidance is to offer long-acting reversible contraception (LARC) first — copper-bearing intrauterine device (Cu-IUD), levonorgestrel-releasing intrauterine system (LNG-IUS), the subdermal etonogestrel implant, and depot medroxyprogesterone acetate — because these methods are user-independent and have the lowest typical-use failure rates.[1][2]
Efficacy is expressed as the perfect-use failure rate (correct and consistent use) and the typical-use failure rate (allowing for missed pills, late re-attendance, displacement and human error). For LARC the two figures are nearly identical; for user-dependent methods such as the combined pill, patch, ring, condom and fertility awareness, the typical-use failure rate is many times higher than the perfect-use rate, which is why unintended pregnancy concentrates among pill and condom users. Trussell's analysis of US data placed typical first-year failure of the pill at about 9 percent and the condom at 18 percent, against under 1 percent for LARC.[4]
The UK Medical Eligibility Criteria (UKMEC) are applied at every consultation. UKMEC is a four-category scale that grades the safety of each method in the presence of a given medical condition, allowing clinicians to choose safely without withholding effective contraception unnecessarily.[1]
[1]Classification
Contraceptive methods are most usefully grouped by efficacy tier and duration of action. LARC methods deliver contraception for months to years without user action and share typical-use failure under 1 percent. Short-acting hormonal methods (combined pill, patch, ring, progestogen-only pill) require daily, weekly or monthly adherence. Barrier methods are coitally dependent and also protect against sexually transmitted infection (STI). Natural methods rely on avoiding or timing intercourse. Sterilisation is permanent. Emergency contraception is a back-up after method failure or UPSI.
[1]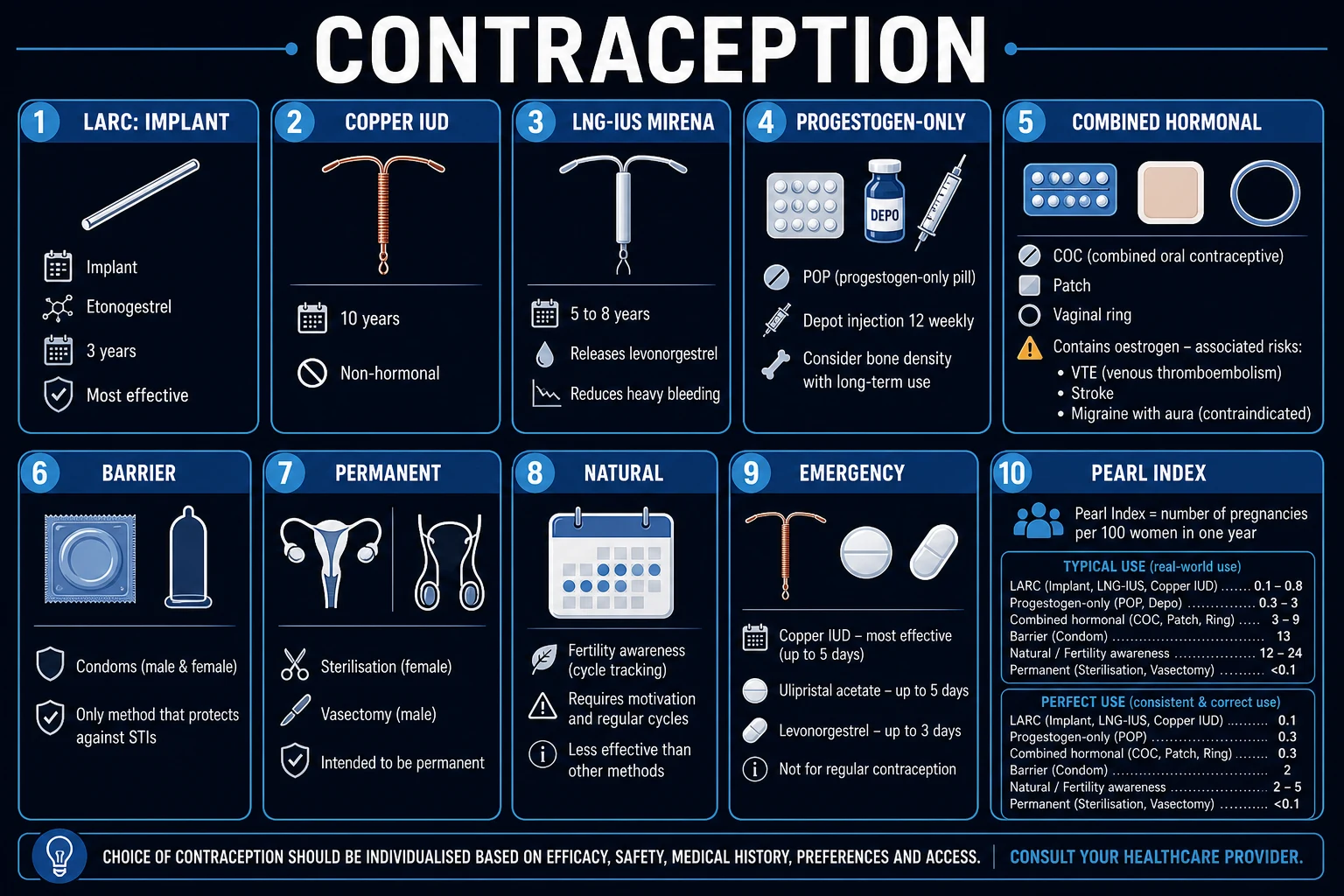
LARC — typical-use failure under 1 percent
- Subdermal etonogestrel implant (Nexplanon) — 68 mg, 3 years, failure 0.05 percent
- Copper IUD (Cu-IUD) — 5 to 10 years, non-hormonal, failure 0.8 percent
- Levonorgestrel IUS 52 mg (Mirena) — 8 years contraception (5 years HRT/endometrial protection); Jaydess 13.5 mg 3 years
- DMPA injection 150 mg IM q12wk — typical-use failure 4 percent (adherence-dependent dosing) but perfect-use 0.2 percent
Short-acting hormonal
- Combined oral contraceptive (COC) — ethinylestradiol 20 to 35 mcg plus progestogen; typical-use 9 percent, perfect-use 0.3 percent
- Combined transdermal patch (Evra) — weekly; 91 percent effective typical use
- Combined vaginal ring (NuvaRing) — monthly; 91 percent effective typical use
- Progestogen-only pill (POP) — desogestrel 75 mcg or norethisterone 350 mcg or levonorgestrel 30 mcg daily; 91 percent typical use
Barrier — STI protection
- Male latex/polyurethane condom — 82 percent typical use; only method protecting against HIV and STI
- Female condom (FC2) — 79 percent typical use
- Diaphragm with spermicide — 88 percent typical use
- Cervical cap — 71 to 86 percent, parity dependent
Natural and permanent
- Fertility awareness (symptothermal) — 76 to 88 percent typical use
- Lactational amenorrhoea (LAM) — 98 percent if all three criteria met
- Withdrawal — 78 percent typical use
- Female sterilisation (tubal occlusion) — over 99.5 percent, failure 1 in 200
- Vasectomy — over 99.8 percent; lowest failure of any method
Epidemiology & Risk Factors
In the UK the combined oral contraceptive pill and the male condom remain the most commonly used reversible methods, each chosen by about a quarter of contraceptive users, while LARC uptake has risen steadily with the publication of effectiveness data and NICE guidance to about 12 to 15 percent of women of reproductive age. Sterilisation accounts for around 7 percent. Uptake patterns mirror availability, clinician confidence, and reimbursement; countries with state-funded LARC programmes show the steepest fall in unintended teenage pregnancy.[1][2]
Unintended pregnancy affects 30 to 50 percent of all pregnancies globally. The risk is concentrated in women under 25, those on lower incomes, late presenters for postnatal contraception, and — most importantly — users of user-dependent methods who experience method failure or discontinuation. The Contraceptive CHOICE project in the United States demonstrated that when counselling removes cost and access barriers and offers LARC first, three-quarters of women choose a LARC method and unintended pregnancy and abortion rates fall dramatically.[2]
Risk factors for contraceptive failure include inconsistent or incorrect use, enzyme-inducing drug co-prescription, late restart after the pill-free interval, vomiting or severe diarrhoea within 3 hours of pill-taking, BMI over 35 for some oral emergency methods, and device expulsion or perforation. Risk factors for serious contraceptive harm — chiefly arterial or venous thrombosis on combined hormonal contraception — are summarised by the UKMEC framework and include age, smoking, hypertension, migraine with aura, prior VTE, thrombophilia, obesity, and immobility.[1][5]
Pathophysiology
Contraception interrupts the reproductive cascade at one or more of four points: ovulation, gamete transport, fertilisation, or implantation. Understanding the mechanism explains each method's efficacy, side-effect profile, and eligibility.
[1]Combined hormonal contraception (CHC) — the combined oral contraceptive pill, the transdermal patch, and the vaginal ring — contains a synthetic oestrogen (ethinylestradiol 20 to 35 mcg, or mestranol; estradiol valerate in newer pills) plus a progestogen. The oestrogen component suppresses follicle-stimulating hormone (FSH), preventing a dominant follicle from developing, while the progestogen suppresses the luteinising hormone (LH) surge that triggers ovulation. The progestogen also thickens cervical mucus (impairing sperm penetration), thins the endometrium (reducing receptivity to implantation), and reduces tubal motility. The oestrogen component additionally stabilises the endometrium (improving cycle control and reducing breakthrough bleeding) and potentiates the progestogenic suppression of ovulation. The thrombotic, vascular, and hepatic risks of CHC are attributable to the oestrogen component; the progestogenic effects drive most cycle, mucus, and endometrial actions.[1][5]
Progestogen-only methods — the progestogen-only pill, the etonogestrel implant, depot medroxyprogesterone acetate, and the LNG-IUS — share the same core actions: thickening of cervical mucus and thinning of the endometrium, with variable suppression of ovulation. The traditional POP (levonorgestrel, norethisterone) suppresses ovulation in only about half of cycles and relies mainly on mucus and endometrial effects; desogestrel 75 mcg suppresses ovulation in around 97 percent of cycles, which is why its missed-pill window is more forgiving. The etonogestrel implant suppresses ovulation almost completely; DMPA suppresses ovulation and ovarian oestradiol production profoundly (often producing hypo-oestrogenaemia); the LNG-IUS acts locally on the endometrium and cervix and only partially suppresses ovulation, so most women continue to ovulate.[1]
The copper-bearing IUD is the only long-acting, non-hormonal, locally acting method. Copper ions release into the uterine and tubal fluid, creating a sterile inflammatory reaction in the endometrium that is toxic to ova and sperm and prevents fertilisation; copper also inhibits sperm motility and capacitation. When inserted after ovulation the device prevents implantation. This is why the Cu-IUD is the most effective emergency contraception and why it tends to increase menstrual blood loss and dysmenorrhoea. The LNG-IUS instead produces a thin, inactive endometrium and viscous cervical mucus, which is why it dramatically reduces menstrual loss and is licensed for heavy menstrual bleeding.[1]
Sterilisation interrupts anatomical gamete transport — occluding or dividing the fallopian tubes in women and the vas deferens in men — and is intended to be permanent. Natural methods identify or avoid the fertile window. Lactational amenorrhoea relies on the hyperprolactinaemia of exclusive breastfeeding suppressing gonadotropin-releasing hormone pulsatility, which prevents ovulation for up to 6 months postpartum.
[1]Clinical Presentation
The "presentation" in contraception is rarely a symptom; it is a request — for contraception, for emergency contraception, for a method change, or for a complication review. A purposeful consultation captures the relevant history and applies UKMEC.
[1]At initiation the focused history covers menstrual pattern and cycle, obstetric history (parity, mode of delivery, complications), lactation, sexual history (frequency, partner(s), STI risk, prior UPSI in the current cycle), medical history (venous or arterial thromboembolism, thrombophilia, cardiovascular disease, migraine — distinguishing with and without aura — hypertension, diabetes with vascular disease, liver disease, breast cancer, SLE, post-transplant status), medications (especially enzyme inducers: rifampicin, rifabutin, antiepileptics — carbamazepine, phenytoin, phenobarbital, primidone, oxcarbazepine, topiramate — St John's wort, certain antiretrovirals), smoking, alcohol, weight/BMI, and plans for future fertility. A focused examination measures blood pressure, BMI, and (where indicated) breast and pelvic examination. A cervical screening test is performed only if due.[1]
At follow-up or unscheduled review the key symptoms and their causes are:
[1]- Unscheduled or irregular bleeding on POP, implant, DMPA, or LNG-IUS — common in the first 3 to 6 months; investigate if heavy, persistent, or new after a stable interval, by excluding infection (chlamydia, gonorrhoea), pregnancy, gynaecological pathology (cervical, endometrial), and device issues (expulsion, perforation).
- Amenorrhoea — pregnancy first; then expected on DMPA (over 50 percent by 12 months) and LNG-IUS (20 to 80 percent depending on device and year).
- Chest pain, dyspnoea, calf pain or swelling, sudden severe headache, visual disturbance, focal neurology, or jaundice on CHC — treat as VTE, PE, ischaemic stroke, or hepatic complication until proven otherwise.
- Severe lower abdominal pain in an IUD/IUS user — perforation, pelvic infection, pregnancy (intrauterine or ectopic), or expulsion.
- Missing threads on IUD/IUS review — expulsion, perforation, or simply retracted; locate by ultrasound.
- Acne, weight change, mood change, breast tenderness, headache — common androgenic or hormonal side effects; usually settle within 3 months but drive discontinuation if persistent.
Differential Diagnosis
The most frequent diagnostic problem is unscheduled bleeding or amenorrhoea in a contraceptive user. The differential is approached systematically; the contraceptive method is a diagnosis of exclusion, made only after the dangerous and treatable causes are excluded.
[1]Pregnancy-related
- Intrauterine pregnancy — positive urinary hCG, missed withdrawal bleed, breast tenderness, nausea
- Ectopic pregnancy — especially relevant in IUD users; unilateral pain, vaginal bleeding, shoulder tip pain, collapse; urgent β-hCG and ultrasound
- Implantation or decidual bleed — light, brief; exclude pregnancy
Infection
- Chlamydia trachomatis — often silent; postcoital or intermenstrual bleeding
- Neisseria gonorrhoeae — purulent discharge, pelvic pain
- Pelvic inflammatory disease — bilateral adnexal tenderness, cervical motion tenderness, fever; risk highest in first 3 weeks after IUD insertion
Gynaecological pathology
- Cervical — ectropion, polyp, dysplasia or cancer; speculum examination and up-to-date cervical screening
- Endometrial — polyp, hyperplasia, carcinoma; especially in women over 40 with persistent unscheduled bleeding
- Structural — fibroids (submucosal bleeding), adenomyosis
Endocrine / physiological
- Perimenopause — irregular cycles, vasomotor symptoms, FSH over 25 IU/L on two samples
- Polycystic ovary syndrome — oligomenorrhoea, hyperandrogenism
- Thyroid dysfunction — check TSH; prolactinoma — galactorrhoea, headache
A 28-year-old on the implant reports 3 weeks of unscheduled bleeding and left-sided pelvic pain. What is the first investigation?
Exclude pregnancy and ectopic with a urinary or serum β-hCG — do not attribute bleeding to the implant until pregnancy is excluded. Then screen for chlamydia and gonorrhoea and arrange a pelvic ultrasound to confirm implant position and adnexal anatomy.
Clinical & Bedside Assessment
The bedside assessment in contraception is brief and protocol-driven. The aim is to identify UKMEC 3 and 4 conditions and to recognise complications.
[1]History — as detailed above. Quantify smoking in cigarettes per day (the 35-year and 15-cigarette thresholds matter for UKMEC). Establish migraine phenotype by asking specifically about aura — focal neurological symptoms (visual, sensory, motor, speech) developing over 5 minutes and lasting under 60 minutes before headache; aura makes CHC UKMEC 4. Document any personal or strong family history (first-degree relative under 45) of VTE. Establish the postpartum day and breastfeeding status. List all medications including over-the-counter St John's wort.[1][8]
Examination — blood pressure, weight, height and BMI. Breast examination in women with breast symptoms or over 35 with family history. Speculum and bimanual pelvic examination if STI screen, cervical screening, or device check is needed. Auscultation of the heart and lungs if cardiovascular symptoms. Examine the calves for swelling and tenderness if VTE is suspected. For the implant, palpate the insertion site and document the position.
[1]Named signs relevant to complications:
- Homans' sign (calf pain on dorsiflexion) — historical and unreliable for DVT; diagnosis is by D-dimer and Doppler ultrasound.
- Lost threads at IUD/IUS review — locate device by ultrasound; consider perforation or expulsion.
- Visible thread length change — possible device displacement.
Investigations
Routine investigations before starting contraception are minimal. The principle is targeted testing driven by history and UKMEC.
[1]Before CHC
- Blood pressure and BMI at baseline
- Cervical screening if due
- STI screen if risk identified
- Pregnancy test if UPSI since last menstrual period
Before LARC
- STI screen if risk identified, ideally before IUD/IUS insertion
- Pregnancy test if UPSI in the cycle and quick-start considered
- No routine bloods; no routine pelvic exam required for COC
- Hb if heavy menstrual bleeding before copper IUD
Selected indications
- Thrombophilia screen only if personal or strong family history of VTE — never 'routine'
- Lipid and glucose screen if multiple cardiovascular risk factors
- TSH if menstrual irregularity or symptoms
- FSH if perimenopausal (over 40) to interpret bleeding
For complications
- D-dimer, Doppler ultrasound or CTPA for suspected VTE
- β-hCG and transvaginal ultrasound for suspected ectopic
- Pelvic ultrasound to locate a lost IUD/IUS; plain abdominal X-ray or CT if ultrasound cannot find it (perforation)
- Endometrial biopsy if persistent unscheduled bleeding over age 40 or high risk
Management — Resuscitation
Contraceptive emergencies are rare but time-critical. The key syndromes are combined-hormonal-contraception-related thromboembolism or stroke, uterine perforation or pelvic infection with an IUD/IUS, and septic miscarriage with an IUD in situ.
[1]Management — Definitive & Stepwise
The definitive management is method selection guided by efficacy, UKMEC, and patient preference, with LARC offered first. NICE Clinical Guideline 30 (long-acting reversible contraception) directs clinicians to actively offer LARC to reduce unintended pregnancy, and the FSRH provides detailed eligibility and initiation guidance that the UKMEC paper summarises.[1][2]
Combined oral contraceptive (COC) pill
The COC combines ethinylestradiol 20 to 35 mcg (low-dose is preferred — 20 to 30 mcg; 35 mcg in some formulations) with a progestogen (levonorgestrel, norethisterone, ethynodiol, norgestimate; or third- and fourth-generation desogestrel, gestodene, drospirenone, dienogest; estradiol valerate and nomegestrol acetate in newer pills). The standard regimen is 21 active tablets followed by a 7-day pill-free interval (or 7 inert tablets), during which a withdrawal bleed occurs; an extended regimen (84 active days plus 7 placebo, or continuous use) suppresses menstruation. Start on day 1 to 5 of the cycle for immediate contraceptive cover, or quick-start any day after excluding pregnancy with 7 days of additional precautions. Benefits: predictable cycle control, lighter and less painful periods, improvement of acne and hirsutism, reduction in functional ovarian cysts, and a significant reduction in ovarian, endometrial, and colorectal cancer risk that persists for decades after stopping. Risks: VTE (around 2- to 4-fold higher than non-users, with third- and fourth-generation progestogens and higher oestrogen doses carrying higher risk), ischaemic stroke and myocardial infarction (rare, mainly in smokers and hypertensives), a small increase in breast and cervical cancer, hypertension, and hepatic adenoma. The oestrogen-related VTE risk is dose-dependent and formulation-dependent.[1][5]
Progestogen-only pill (POP)
Two clinical types. The traditional POP (levonorgestrel 30 mcg, norethisterone 350 mcg) thickens cervical mucus and thins the endometrium and suppresses ovulation in only about half of cycles; it must be taken within the same 3-hour window each day (the "3-hour rule"). Desogestrel 75 mcg (Cerelle, Cerazette, Aizea, others) suppresses ovulation in around 97 percent of cycles and has a 12-hour missed-pill window. Take one tablet daily without a break, starting on day 1 to 5 of the cycle for immediate cover or quick-start with 7 days of precautions. Advantages: no oestrogen-related VTE risk, suitable when CHC is contraindicated, safe in breastfeeding from the immediate postpartum period, UKMEC 2 even in current VTE on anticoagulation. Disadvantages: irregular bleeding or amenorrhoea, small risk of functional ovarian cysts, strict timing (especially for traditional POP), and no cycle control.[1]
Injectable: depot medroxyprogesterone acetate (DMPA)
DMPA 150 mg intramuscularly every 12 weeks (or 104 mg subcutaneously every 13 weeks). Start within day 1 to 5 of cycle for immediate cover; quick-start with 7 days precautions. After childbirth, give from day 21 if not breastfeeding or from 6 weeks if breastfeeding. Advantages: high perfect-use efficacy, independent of daily adherence, amenorrhoea in over half by 12 months, reduces sickle-cell crisis and seizure threshold, suitable for CHC-contraindicated women. Disadvantages: delayed return of fertility of up to 1 year after the last dose, weight gain (around 2 to 3 kg in the first year, sometimes more), unscheduled bleeding in the first months, loss of bone mineral density that may not fully reverse, and a small UK signal of increased fracture risk with long-term use. The FSRH recommends reviewing continued use at 2 years in women with other osteoporosis risk factors and considering alternatives, weighing benefits against bone risk.[1][7]
Subdermal implant (Nexplanon)
A single 68 mg etonogestrel rod inserted subdermally in the inner upper arm under local anaesthetic; provides contraception for 3 years, with effectiveness maintained in heavier women. Insert within day 1 to 5 of the cycle for immediate cover or quick-start with 7 days precautions; effective within 24 hours if started correctly. Most effective reversible method available (typical-use failure around 0.05 percent). Disadvantages: unscheduled bleeding is the commonest reason for discontinuation (around 1 in 5 women in the first year), headaches, acne, breast tenderness, mood change. Removal requires a trained clinician. Enzyme inducers reduce efficacy — use alternative contraception and avoid the implant if long-term enzyme inducer use is anticipated.[1]
Intrauterine contraception
Copper-bearing IUD (Cu-IUD) — a T-shaped plastic frame wound with copper wire; licensed for 5 or 10 years depending on device (380 mm² surface area devices last 10 years). Non-hormonal; immediate return to fertility on removal; the most effective emergency contraception. Side effects: heavier, longer, more painful periods (most pronounced in the first 3 to 6 months), small risk of perforation (about 1 in 1000 insertions), expulsion (3 to 5 percent, highest in first 3 months and within 3 months of delivery), and pelvic infection (highest in first 3 weeks after insertion).[1][2]
Levonorgestrel-releasing intrauterine system (LNG-IUS) — Mirena 52 mg (8 years for contraception, 5 years for endometrial protection on HRT and heavy menstrual bleeding), Levosert/Benilexa 52 mg (5 to 6 years), Kyleena 19.5 mg (5 years), Jaydess 13.5 mg (3 years). Releases levonorgestrel locally, producing a thin, inactive endometrium and viscous cervical mucus with only partial systemic absorption. Reduces menstrual blood loss by 70 to 95 percent and is licensed for heavy menstrual bleeding and endometrial protection during HRT; many women become amenorrhoeic. Fewer hormonal side effects than systemic progestogens because of low serum levels. Same insertion risks as the Cu-IUD.[1]
Barrier methods
The male latex condom is the only method (with the female condom) that protects against STI including HIV, and dual protection (condom plus hormonal or intrauterine method) is advised for all women at STI risk. Use a new condom for each act, withdraw while still erect, and avoid oil-based lubricants with latex (degradation). The female condom (FC2) is polyurethane or nitrile and can be inserted before intercourse. The diaphragm (with spermicide, ideally a cervical cap) must be fitted and left in place for at least 6 hours after intercourse. Spermicides (nonoxynol-9) used alone have high failure and may increase HIV transmission with frequent use.[1]
Natural methods
Fertility awareness-based methods identify the fertile window (around ovulation, with sperm survival up to 5 days and ovum survival 12 to 24 hours) using calendar, basal body temperature, cervical mucus, or combined (symptothermal) indicators; typical-use failure 12 to 24 percent and demands motivation and training. Lactational amenorrhoea method (LAM) is 98 percent effective when all three criteria are met: exclusive breastfeeding on demand day and night, the baby is under 6 months old, and the woman remains amenorrhoeic. Withdrawal has a typical-use failure around 22 percent. These methods protect against STI not at all.[1]
Sterilisation
Female sterilisation — laparoscopic tubal occlusion with clips, rings, or diaphragms, or salpingectomy (which also reduces ovarian cancer risk); hysteroscopic tubal cannulation/implants (Essure) have been withdrawn from the market in many countries. Failure rate about 1 in 200; regret is commoner in women under 30 and around the time of a pregnancy. If sterilisation fails the pregnancy is more likely to be ectopic. Vasectomy — day-case local anaesthetic procedure to divide or occlude the vas deferens; the most effective method of contraception but not immediately effective. Two consecutive semen analyses must show azoospermia (or rare non-motile sperm under 100 000 per mL), typically after 20 ejaculations and 12 weeks, before the man can rely on the procedure; alternative contraception is essential in the interim.[1]
Emergency contraception
Emergency contraception is offered after UPSI, method failure, or sexual assault. A copper IUD inserted within 5 days of the first unprotected intercourse in the cycle, or within 5 days of the earliest expected ovulation, is the most effective emergency contraception (over 99 percent), and it provides ongoing contraception. Ulipristal acetate 30 mg as a single oral dose within 120 hours of UPSI is a progesterone receptor modulator that delays ovulation; it is more effective than levonorgestrel and retains efficacy in higher BMI, though evidence is limited above BMI 35. Levonorgestrel 1.5 mg as a single oral dose within 72 hours (efficacy falls sharply after 72 hours) works mainly by suppressing or delaying the LH surge; for women over 70 kg or with BMI over 26, a double dose (3 mg) is recommended. Enzyme-inducing drugs reduce the efficacy of levonorgestrel — a double dose (3 mg) is advised; an IUD is preferable. Ulipristal can be reduced by progestogen-containing contraception — wait 5 days after ulipristal before starting or restarting hormonal contraception, and use condoms meanwhile. The Cochrane review confirms that ulipristal is superior to levonorgestrel, and the IUD is superior to both.[3][6]
Stepwise Management
Consultation
Focused history and brief examination; identify UKMEC 3 or 4 conditions; assess STI risk; establish preferences, future fertility plans, and acceptability.
LARC first
Offer the implant, Cu-IUD, or LNG-IUS first, and DMPA if appropriate; explain that LARC is most effective and reversible.
Apply UKMEC
For every condition and medication, assign the UKMEC category; document the discussion, especially for category 3.
Initiation
Start within day 1 to 5 of cycle for immediate cover, or quick-start with 7 days of additional precautions after excluding pregnancy.
Counselling
Cover benefits, common side effects (especially unscheduled bleeding), the missed-pill rules, STI protection, red-flag symptoms, and follow-up.
Follow-up
Review IUD/IUS at 3 to 6 weeks (strings, expulsion, infection, pregnancy); review pill, patch, ring, implant or DMPA at 3 months then annually or as needed.
Switching
Overlap appropriately (e.g. continue previous method for 7 days when switching CHC to POP); never leave a gap.
Stopping
Document the reason; advise that fertility returns immediately for most methods (delayed up to 1 year for DMPA); offer pre-conception folic acid.
Missed-pill rules
The Faculty of Sexual and Reproductive Healthcare simplified the missed-pill rules. For a combined pill: a pill taken more than 24 hours late counts as missed. One missed pill — take it as soon as remembered, continue the pack, no additional precautions. Two or more missed pills (over 48 hours late) — take the most recent missed pill, continue the pack daily, use condoms or abstain for 7 days, and use emergency contraception if unprotected sex occurred in the pill-free interval or the first 7 days of the current pack, or if more than seven pills were missed. For the progestogen-only pill: a traditional POP taken more than 3 hours late (over 12 hours late for desogestrel) is missed — take it as soon as remembered, continue daily, and use additional precautions for 2 days (48 hours).[1]
Specific Subtypes & Scenarios
Migraine with aura
- CHC is UKMEC 4 — unacceptable stroke risk; aura and oestrogen dose independently raise risk
- POP, implant, LNG-IUS, and Cu-IUD are UKMEC 1 or 2 — safe alternatives
- Migraine without aura under 35 with no other risk: CHC UKMEC 2; over 35 or worsening: UKMEC 3
Smoking
- Under 35: CHC UKMEC 1 to 2
- Over 35, fewer than 15 cigarettes a day: CHC UKMEC 3
- Over 35, 15 or more cigarettes a day: CHC UKMEC 4
Venous thromboembolism
- History of VTE: CHC UKMEC 4
- POP, implant, LNG-IUS UKMEC 2; Cu-IUD UKMEC 1
- Known thrombophilia: CHC UKMEC 4; POP/implant/LNG-IUS UKMEC 2 to 4 depending on type
Hypertension
- Controlled under 140/90: CHC UKMEC 3
- Sustained over 160/100: CHC UKMEC 4
- Vascular disease: CHC UKMEC 4; progestogen-only methods acceptable
Diabetes
- Uncomplicated: CHC UKMEC 2
- Nephropathy, retinopathy, neuropathy, or over 20 years duration: CHC UKMEC 3 to 4
- Progestogen-only and intrauterine methods UKMEC 1 to 2
Breast cancer
- Current or recent: all hormonal methods UKMEC 4
- Cu-IUD UKMEC 1; LNG-IUS UKMEC 4 in current disease
- Past (over 5 years disease-free): POP UKMEC 3
Breastfeeding and postpartum
- POP, implant, Cu-IUD, LNG-IUS from immediately postpartum (implant and IUD usually from 4 weeks)
- CHC from 6 weeks postpartum if not breastfeeding and no VTE risk factors; withhold until day 21 minimum
- Avoid CHC before 6 weeks postpartum if breastfeeding
Enzyme-inducing drugs
- Rifampicin, rifabutin, antiepileptics (carbamazepine, phenytoin, phenobarbital, primidone), St John's wort, some antiretrovirals
- Reduce COC, POP, patch, ring, implant efficacy — use Cu-IUD or DMPA, or condoms and additional precautions throughout and for 28 days after stopping
- LNG emergency contraception dose doubled (3 mg); ulipristal not recommended; Cu-IUD preferred
Perimenopause and menopause — contraception is needed until the woman is over 50 and has had 12 months of amenorrhoea (or over 50 with FSH over 25 IU/L on two occasions). The LNG-IUS provides contraception plus endometrial protection for HRT. Adolescents — LARC is first-line; Fraser competence governs prescribing under 16 in the UK. Women with BMI over 35 — CHC is acceptable (UKMEC 2) but oral emergency contraception is less effective; a Cu-IUD for emergency contraception is preferred. Women with cardiac disease — UKMEC assessment; the Cu-IUD is often safest. Learning or physical disability — consent and capacity assessment (Mental Capacity Act); LARC may need general anaesthesia for insertion.[1]
Complications & Pitfalls
Combined hormonal
- VTE 2 to 4 times non-user risk; third/fourth-generation progestogens and higher oestrogen doses higher risk
- Ischaemic stroke and MI — rare, concentrated in smokers, hypertensives, migraine with aura
- Hypertension, cholestasis, hepatic adenoma, gallstones
- Small increase in breast and cervical cancer; reduced ovarian, endometrial, colorectal cancer
- Mood change, breakthrough bleeding, breast tenderness, nausea
Progestogen-only
- Unscheduled bleeding — commonest reason for discontinuation, especially implant and POP
- Acne, mood change, weight gain (most marked on DMPA)
- Functional ovarian cysts (usually asymptomatic)
- Bone mineral density loss on DMPA — may not fully reverse; small UK fracture signal
Intrauterine
- Perforation about 1 in 1000 at insertion (risk highest in lactation)
- Expulsion 3 to 5 percent, highest within 3 months
- Pelvic infection highest in first 3 weeks — screen for STI before insertion if at risk
- Pregnancy with IUD in situ — higher relative risk of ectopic; remove if possible
- Lost threads — locate by ultrasound; rule out perforation or expulsion
Sterilisation
- Failure — 1 in 200 (female) and under 1 in 2000 (vasectomy after clearance)
- Regret — up to 15 percent in women under 30 at sterilisation
- Ectopic pregnancy if tubal occlusion fails
- Surgical risks of laparoscopy — bleeding, infection, visceral injury, anaesthesia
- Vasectomy is not immediately effective — confirm azoospermia on two samples before relying on it
Classic pitfalls — prescribing CHC to a woman with migraine with aura (UKMEC 4); relying on the COC pill-free interval when enzyme-inducing drugs are co-prescribed; missing the diagnosis of ectopic pregnancy in an IUD user with abdominal pain; failing to confirm azoospermia before clearing a vasectomy patient; under-dosing levonorgestrel emergency contraception in women over 70 kg or on enzyme inducers; and forgetting that the LNG-IUS for HRT endometrial protection expires at 5 years even though it lasts 8 years for contraception.[1]
Prognosis & Disposition
Contraception is highly effective when used correctly and consistently; the population burden of unintended pregnancy falls with LARC access. LARC methods achieve typical-use failure under 1 percent, while user-dependent methods (pill, condom, fertility awareness) carry typical-use failure of 9 to 24 percent. Fertility returns immediately after stopping the pill, patch, ring, POP, implant, Cu-IUD, or LNG-IUS, and after vasectomy once azoospermia is confirmed; DMPA delays return of fertility by a median of 9 to 10 months from the last injection.[1][2]
Disposition: initiation and most follow-up are outpatient; IUD/IUS insertion is a day-case clinic procedure. Same-day emergency contraception is offered in primary care, sexual health clinics, and pharmacies. The emergency department is reserved for complications — suspected VTE/PE, stroke, perforation, ectopic, or sepsis. The safety-net is explicit counselling of red-flag symptoms (chest pain, dyspnoea, calf pain, severe headache, visual change, severe abdominal pain) and a 24-hour contact for unscheduled bleeding, lost threads, or pregnancy concerns.
[1]Special Populations
Adolescents
- LARC first-line — implant, IUS, Cu-IUD
- Fraser competence governs under-16 prescribing in UK; confidentiality assured
- Emergency contraception available over the counter and free in sexual health services
- STI protection with condoms alongside LARC ('dual protection')
Postpartum and breastfeeding
- POP, implant, LNG-IUS, Cu-IUD acceptable immediately (IUD/IUS usually from 4 weeks)
- CHC deferred to at least 6 weeks postpartum if breastfeeding, day 21 if not, and longer if VTE risk
- LAM effective if exclusive breastfeeding, under 6 months, amenorrhoeic
Perimenopause (over 40)
- Continue contraception to age 55 or 12 months amenorrhoea if over 50
- LNG-IUS doubles as contraception and HRT endometrial protection
- Be alert to gynaecological pathology in new unscheduled bleeding
BMI over 35
- CHC acceptable (UKMEC 2) but VTE risk higher
- VTE risk further raised by immobility — CHC UKMEC 3 to 4
- Oral emergency contraception less effective — Cu-IUD preferred for emergency
- DMPA associated with weight gain
Disability and capacity
- Mental Capacity Act assessment; best-interest decision-making if lacking capacity
- LARC often preferred but insertion may need sedation or general anaesthesia
- Safeguarding and consent paramount
Medical comorbidity
- Apply UKMEC to every condition — CHC contraindicated in VTE, migraine with aura, smoking over 35, uncontrolled hypertension, active breast cancer, decompensated liver disease
- Progestogen-only and intrauterine methods safe in most CHC-contraindicated women
- Cu-IUD is hormone-free and safe in nearly all conditions
Evidence, Guidelines & Regional Differences
The UK Medical Eligibility Criteria (UKMEC), adapted from the WHO Medical Eligibility Criteria, is the UK standard and is summarised in the FSRH guidance; the 2016 update refined categories for breastfeeding, diabetes, and HIV, among others.[1] NICE Clinical Guideline 30 (Long-acting reversible contraception) directs clinicians to increase LARC uptake to reduce unintended pregnancy. The WHO Medical Eligibility Criteria (5th edition, 2015) is the international standard with broadly congruent categories.
[1] [1]The WHO MEC (5th edition) and its wheel app are the global reference. Many low- and middle-income settings prioritise DMPA (self-administrable), implants, and Cu-IUD through community-based distribution. Hormonal emergency contraception is on the WHO Essential Medicines List.
Landmark evidence — Winner and colleagues (NEJM 2012, the Contraceptive CHOICE project) showed that LARC methods had failure rates 10 to 20 times lower than the pill, patch, or ring, with continuation highest for the IUD and implant.[2] Lidegaard and colleagues (BMJ 2011) quantified the VTE risk of combined pills, showing that third- and fourth-generation progestogens and higher oestrogen doses carry the highest risk, informing the preferential prescribing of levonorgestrel- or norethisterone-containing pills.[5] Glasier and colleagues (Lancet 2010) demonstrated that ulipristal is non-inferior and overall superior to levonorgestrel for emergency contraception, and the Cochrane review (Shen 2019) confirmed this hierarchy with the Cu-IUD most effective of all.[3][6] Kyvernitakis and colleagues (Osteoporosis International 2017) reported a UK signal of increased fracture risk with DMPA, informing counselling on long-term use.[7]
Controversies — the absolute VTE risk on CHC remains low (around 9 to 10 per 10 000 woman-years, against 2 to 3 per 10 000 in non-users), and the contraceptive benefit usually outweighs it; the choice of progestogen is a risk modifier. The bone-density effect of DMPA is largely reversible and must be balanced against the substantial contraceptive and non-contraceptive benefits. The role of LNG-IUS for HRT endometrial protection beyond 5 years is an area of active review.
[5]Exam Pearls
- Migraine with aura = absolute contraindication to CHC (UKMEC 4) — the single most tested UKMEC fact. Stroke risk is amplified by oestrogen dose.[8]
- Smoking plus age over 35 plus CHC — UKMEC 4 if 15 or more cigarettes per day; UKMEC 3 if fewer.
- DMPA delays fertility by up to 1 year and reduces bone density — unique among reversible methods.[7]
- Copper IUD is the most effective emergency contraception (over 99 percent, within 5 days) and the only non-hormonal LARC.[6]
- Desogestrel POP suppresses ovulation in about 97 percent of cycles — hence the 12-hour window versus the 3-hour window for traditional POPs.
- Lactational amenorrhoea — 98 percent effective only if all three criteria (exclusive breastfeeding, baby under 6 months, amenorrhoea) are met.
- Vasectomy is not immediately effective — two azoospermic samples (typically at 12 and 16 weeks) before relying on it.
- Implant is the most effective reversible method (typical-use failure about 0.05 percent) but unscheduled bleeding drives discontinuation.[2]
- CHC VTE risk is formulation-dependent — levonorgestrel and norethisterone lowest; desogestrel, gestodene, drospirenone, and cyproterone higher.[5]
Exam application bank (NEET-PG / INICET)
One-line answer
Contraception methods span hormonal (combined oral contraceptive pill, progestogen-only pill, implant, injectable, hormonal intrauterine system), intrauterine (copper IUD), barrier (condom, diaphragm), natural (fertility awareness, lactational amenorrhoea), emergency contraception, and permanent sterilisation. Choice depends on efficacy, safety, side effects, reversibility, coital independence, age, comorbidities, and patient preference. Long-acting reversible contraception (LARC) — copper IUD, LNG-IUS, implant — is most effective and offered first-line. UK Medical Eligibility Criteria (UKMEC) categorise every method from 1 (no restriction) to 4 (unacceptable risk) across medical conditions.
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Contraception.
References
- [1]Percy L The new UK Medical Eligibility Criteria (UKMEC): what has changed? J Fam Plann Reprod Health Care, 2016.PMID 27069041
- [2]Winner B, Peipert JF, Zhao Q, et al. Effectiveness of long-acting reversible contraception N Engl J Med, 2012.PMID 22621627
- [3]Glasier AF, Cameron ST, Fine PM, et al. Ulipristal acetate versus levonorgestrel for emergency contraception: a randomised non-inferiority trial and meta-analysis Lancet, 2010.PMID 20116841
- [4]Trussell J Contraceptive failure in the United States Contraception, 2011.PMID 21477680
- [5]Lidegaard O, Nielsen LH, Skovlund CW, et al. Risk of venous thromboembolism from use of oral contraceptives containing different progestogens and oestrogen doses: Danish cohort study, 2001-9 BMJ, 2011.PMID 22027398
- [6]Shen J, Che Y, Showell E, et al. Interventions for emergency contraception Cochrane Database Syst Rev, 2019.PMID 30661244
- [7]Kyvernitakis I, Kostev K, Nassour T, et al. The impact of depot medroxyprogesterone acetate on fracture risk: a case-control study from the UK Osteoporos Int, 2017.PMID 27461017
- [8]Batur P, Yao M, Bucklan J, et al. Use of combined hormonal contraception and stroke: A case-control study of the impact of migraine type and estrogen dose on ischemic stroke risk Headache, 2023.PMID 36752588