Obstetrics & Gynaecology · Obstetrics & Gynaecology
Ectopic Pregnancy
Also known as Tubal pregnancy · Extrauterine pregnancy · Ruptured ectopic · Heterotopic pregnancy · Cornual pregnancy · Caesarean scar pregnancy
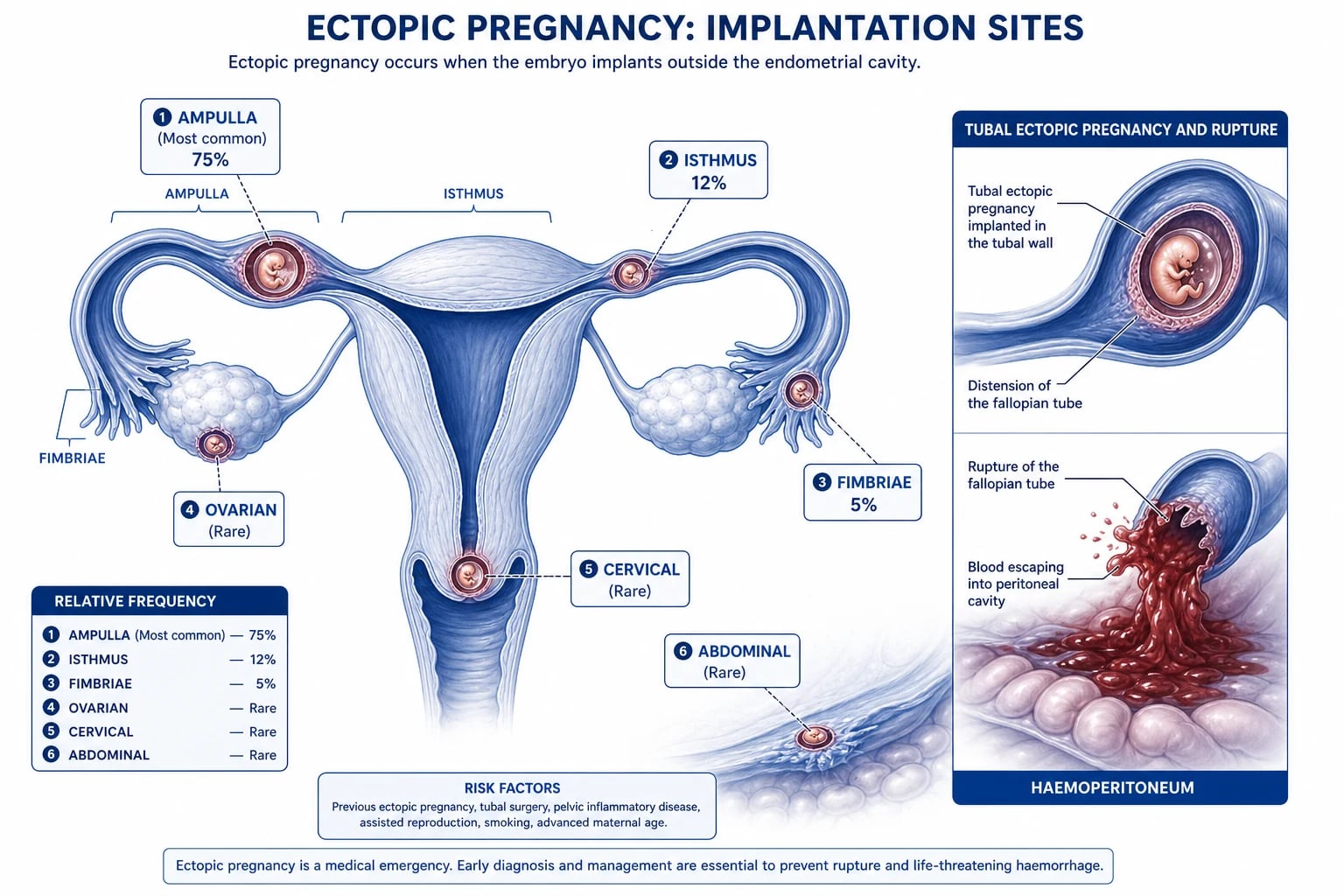
Ectopic pregnancy = implantation of a fertilized ovum outside the uterine cavity. About 95% are tubal (ampulla 75%, isthmus 12%, fimbria 5%, interstitial 2%). Incidence 1 to 2% of pregnancies and 2 to 3% with IVF. Classic triad: missed period + unilateral abdominal pain + dark vaginal bleeding. Diagnosis: quantitative serum beta-hCG + transvaginal ultrasound. Discriminatory zone: at beta-hCG over 1500 to 2000 IU/L an intrauterine gestational sac should be visible on TVS. Shoulder tip pain + collapse = ruptured ectopic (haemoperitoneum). Stable unruptured: methotrexate 50mg per metre squared IM (under 3.5cm, beta-hCG under 5000, no cardiac activity) or laparoscopic salpingostomy or salpingectomy. Ruptured: emergency laparoscopy or laparotomy + salpingectomy. Always give Anti-D to Rh-negative women.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Overview & Definition
Ectopic pregnancy is the implantation of a fertilised ovum outside the normal endometrial lining of the uterine cavity. The conceptus may lodge anywhere along its journey from ovulation to the endometrium — most often inside the fallopian tube, but also in the ovary, cervix, caesarean scar, abdominal cavity, or rarely within a previous hysterotomy scar. The tube, unlike the uterus, lacks a thick muscular wall and a specialised decidua capable of supporting deep placentation; as the gestational sac enlarges, the tube stretches, thins, erodes into tubal vessels, and eventually ruptures, producing catastrophic intraperitoneal haemorrhage that may exceed two litres in minutes.[1][2]
Ectopic pregnancy is the leading cause of maternal death in the first trimester in the developed world and accounts for 3 to 4% of all pregnancy-related deaths in the United States despite representing only 1 to 2% of pregnancies.[4] The dramatic fall in case-fatality over the last forty years (from 35 deaths per 10,000 ectopics in 1970 to roughly 3 to 4 per 10,000 today) is the direct result of sensitive beta-hCG assays, high-resolution transvaginal ultrasound (TVS), and methotrexate therapy — allowing most ectopics to be diagnosed and treated before they rupture.[1][2]
The clinical challenge is therefore no longer the resuscitation of a haemorrhaging woman (although that still happens, particularly in resource-limited or late-presenting settings) but the disciplined investigation of every woman of reproductive age who presents with abdominal pain, vaginal bleeding, syncope, or gastrointestinal symptoms. The single most important reflexive test in emergency gynaecology is the urine or serum pregnancy test.[2]
Classification
Ectopic pregnancies are classified anatomically by implantation site and clinically by haemodynamic stability and rupture status. Both axes drive management.[1]
Tubal (about 95%)
fallopian tube
- **Ampulla (about 75%)** — most common; thin wall but capacious lumen; typically ruptures at 6 to 8 weeks
- **Isthmus (about 12%)** — narrowest segment, thick muscular wall, ruptures EARLIER (4 to 6 weeks) due to poor distensibility
- **Fimbriae (about 5%)** — pregnancy can be expelled into the peritoneum (tubal abortion) or re-implant on the ovary
- **Interstitial / cornual (about 2%)** — within the uterine muscular wall; ruptures LATER (10 to 14 weeks) but with MASSIVE bleeding from the uterine and ovarian artery anastomosis
Non-tubal (about 5%)
rare sites
- **Ovarian** — extremely rare; mimics a corpus luteum or ovarian tumour; treated by wedge resection or oophorectomy
- **Cervical** — implants in cervical stroma; presents with profuse PAINLESS vaginal bleeding; surgery causes catastrophic haemorrhage, so methotrexate preferred
- **Caesarean scar** — rising with rising caesarean rates; risk of placenta accreta spectrum and uterine rupture
- **Abdominal** — rarest; can grow to viability but carries very high maternal mortality; broad ligament, omentum, bowel
Clinical / management-based
haemodynamic status
- **Stable, unruptured** — methotrexate or laparoscopic salpingostomy or salpingectomy
- **Ruptured with shock** — emergency laparoscopy or laparotomy with salpingectomy; resuscitate concurrently
- **Chronic / leaking** — slow intermittent tubal leak forming a pelvic haematocele; subacute anaemic presentation
- **Heterotopic** — simultaneous intrauterine and ectopic pregnancy; rare spontaneously (about 1 in 30,000), common with IVF (up to 1 in 100)
Epidemiology & Risk Factors
The incidence of ectopic pregnancy is 1 to 2% of all recognised pregnancies in the United Kingdom and United States, with a case-fatality of about 0.2 per 1000 ectopic pregnancies in the developed world.[1][4] After one ectopic pregnancy the recurrence risk is 10 to 15%; after two it is over 30%. With IVF and other assisted reproductive techniques, the rate rises to 2 to 5% because embryos can migrate out of the uterine cavity or because underlying tubal disease prompted IVF in the first place.[2]
Epidemiology at a glance
Risk factors — anything that damages the tube or delays ovum transit[1][2]
The risk factor hierarchy below is a high-yield memorisation block. Anything that scars, narrows, or impairs ciliary function in the tube predisposes to ectopic implantation. The risk attributable to each factor is approximate and multiplicative when factors co-exist.[1][2]
- Pelvic inflammatory disease (PID) — the single most important risk factor. Past chlamydial or gonococcal infection causes salpingitis, ciliary loss, and tubal adhesions; previous chlamydia confers an odds ratio of about 3 to 4. Sub-clinical ('silent') chlamydia is a particularly under-recognised contributor.[1][2]
- Previous ectopic pregnancy — recurrence risk 10 to 15% after one, 25 to 30% after two; the damaged contralateral tube is the substrate.
- Previous tubal surgery — including tubal ligation (failed sterilisation presents as ectopic in 30 to 50% of cases), tubal re-anastomosis, fimbrioplasty, and surgery for hydrosalpinx.
- IVF and assisted reproduction — 2 to 5% ectopic rate due to embryo migration, high tubal fluid volume, and underlying tubal disease. Also the principal setting for heterotopic pregnancy.
- Intrauterine contraceptive device (IUCD) at conception — the IUCD prevents intrauterine pregnancy very effectively but offers less protection against ectopic; therefore if a pregnancy does occur with an IUCD in situ, the proportion of ectopics is higher (around 15 to 50%). The copper IUCD also slightly increases absolute ectopic risk versus no method because it does not fully suppress ovulation.
- Smoking — dose-dependent impairment of tubal ciliary motility and gamete transport; current smokers have an OR of about 1.6 to 3, and risk falls after cessation.
- Increasing maternal age — risk rises sharply after 35; women 40 and over have two to three times the risk of women under 25, partly from cumulative tubal exposure and cumulus oophorus ageing.
- Endometriosis and pelvic adhesions from any cause (appendicitis, endometrioma surgery, pelvic surgery).
- Diethylstilboestrol (DES) exposure in utero — historically important; causes congenital tubal anomalies. Mostly of historical interest now.
- Congenital tubal anomalies, including septate or hypoplastic tubes — rare.
- Progesterone-only contraception failure — slight increase in ectopic proportion when pregnancy occurs, though absolute ectopic risk is lower than no method.
India and South Asia: genital tuberculosis (Mycobacterium tuberculosis causing endometrial and tubal involvement) is a major and often under-recognised cause of ectopic pregnancy in endemic areas, producing characteristic 'beaded' tubes on hysterosalpingography. Untreated chlamydia and gonorrhoea from limited STI screening remain the largest absolute contributor. Late presentation of ruptured ectopic in haemorrhagic shock is common in rural settings because of transport delays, limited access to ultrasound, and out-of-hospital deliveries; case-fatality in this setting can exceed 1 to 2%. Anti-D availability must be ensured in district hospitals. In sub-Saharan Africa the picture is similar, with the additional burden of post-infective tubal damage from unsafe abortion.[4]
Pathophysiology
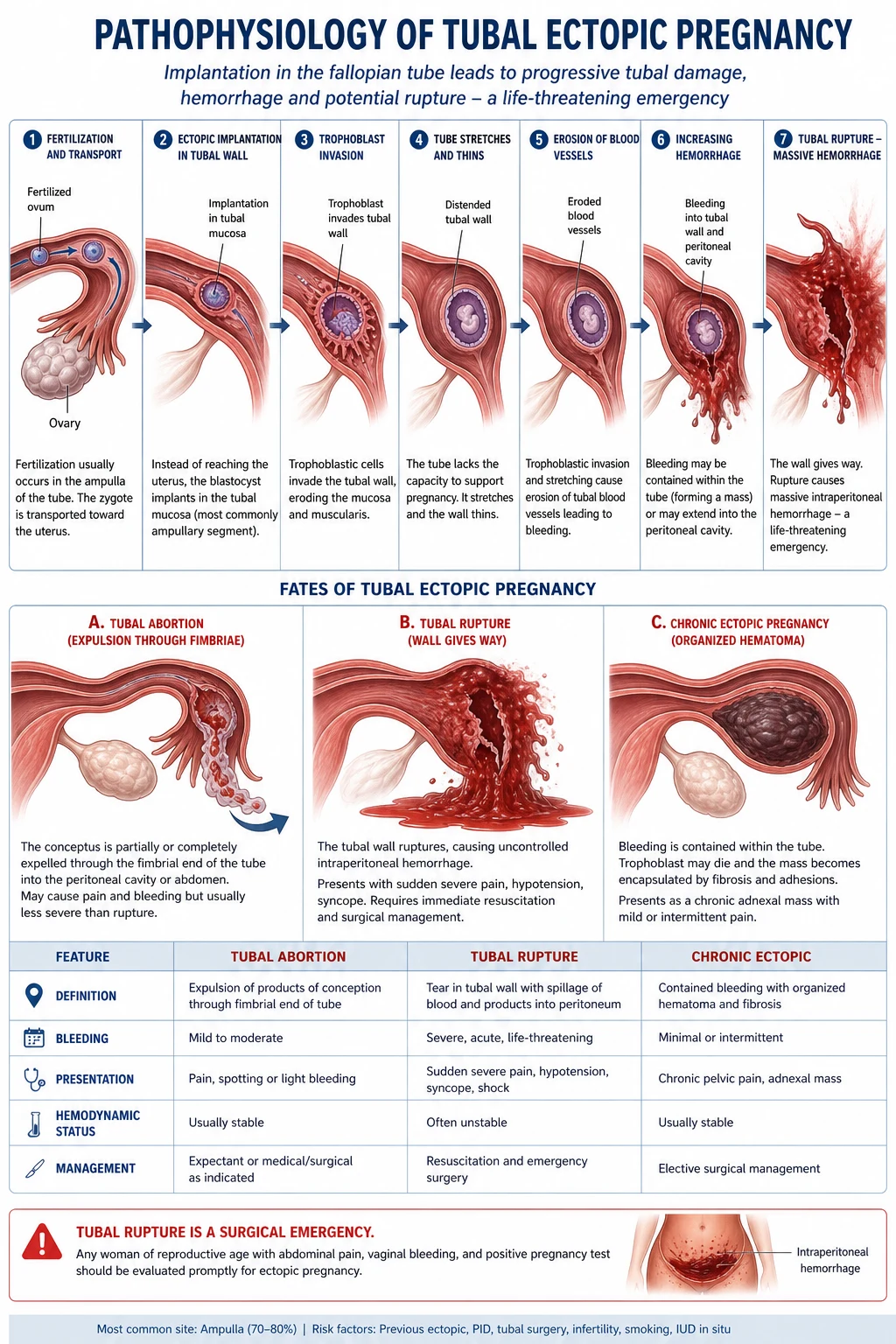
The normal journey of a fertilised ovum from the ampulla to the endometrium takes about three days, propelled by tubal cilia and smooth-muscle contraction. Ectopic implantation arises when that journey is interrupted or delayed so that the embryo implants before reaching the endometrium. The mechanism is therefore one of embryo retention, not embryo abnormality.[1]
The sequence is as follows.[1][2]
- Delayed ovum transit — tubal ciliary dysfunction or scarring (from PID, endometriosis, smoking, prior surgery, or DES exposure) prevents the embryo from reaching the endometrium within the implantation window.[1][2]
- Tubal implantation — the blastocyst implants on the tubal mucosa. The trophoblast then invades the tubal muscularis because the tube lacks a stratum spongiosum of decidua to limit invasion.
- Vascular erosion and tubal distension — the trophoblast erodes into the submucosal plexus and the arcuate vessels of the mesosalpinx, producing intraluminal and intramural bleeding. The tube distends; the muscularis thins. The pregnancy itself is poorly supported because tubal stroma cannot decidualise normally.
- Outcome depends on site and vascularity:
- Tubal abortion — most common in fimbrial and ampullary ectopics; the pregnancy separates from the tubal wall and is expelled into the peritoneal cavity, producing limited self-limiting bleeding.
- Tubal rupture — most common in isthmic ectopics (narrow lumen, poor distensibility) and in interstitial ectopics (massive vascular supply from uterine and ovarian artery anastomosis). Rupture produces sudden, torrential intraperitoneal haemorrhage — 2 to 3 litres can accumulate within minutes.
- Tubal mole — embryo dies but is retained; trophoblast persists and continues to produce beta-hCG, producing chronic symptoms.
- Clinical consequences of rupture — sudden severe lower-abdominal pain, diaphragmatic irritation from haemoperitoneum producing referred shoulder-tip pain via the phrenic nerve (C3, C4, C5 shares roots with the diaphragm), syncope and hypovolaemic shock (pallor, tachycardia, hypotension, cold clammy skin, confusion).
The decidual cast — a shed endometrial lining shaped like the uterine cavity — is sometimes passed vaginally and is a clue that a pregnancy has occurred but is failing or extrauterine; it should not be confused with products of conception.[2]
Clinical Presentation
The triad is classic but incomplete in many patients. Some present with only one element (e.g., isolated shoulder-tip pain or syncope), and the unwary examiner may attribute early gastrointestinal symptoms (nausea, diarrhoea, dizziness on standing) to gastroenteritis. The single most important reflexive test is the pregnancy test.[2]
Symptoms by clinical scenario[1]
- Unruptured ectopic (the common modern presentation): mild, intermittent unilateral pelvic pain, scanty dark vaginal bleeding, missed period, breast tenderness or other early-pregnancy symptoms; vital signs normal.[1]
- Leaking or chronic ectopic: recurrent brief episodes of pain over days to weeks as small amounts of blood leak from the fimbrial end and form a pelvic haematocele; anaemic, low-grade fever, dyspareunia, and a tender adnexal mass on examination.
- Ruptured ectopic (emergency): sudden tearing lower-abdominal pain, shoulder-tip pain (especially on lying flat), syncope or presyncope, nausea and vomiting, signs of class III or IV haemorrhagic shock (HR over 120, BP under 90 systolic, cold clammy peripheries, reduced urine output, altered mental state).
- Cervical ectopic: profuse, painless bright-red vaginal bleeding; the cervix is enlarged, barrel-shaped, and bluish; bimanual examination may provoke catastrophic bleeding.
- Interstitial (cornual) ectopic: non-specific amenorrhoea with vague unilateral pain until 10 to 14 weeks, then sudden collapse from massive bleeding.
- Caesarean scar ectopic: painless early bleeding in a woman with a previous caesarean; uterine rupture risk is high if the pregnancy continues.
- Heterotopic pregnancy: the intrauterine pregnancy dominates the ultrasound; the ectopic is missed because the clinician stops looking. Always scan both adnexae in IVF pregnancies, especially with persistent pain or falling haematocrit despite a viable IUP.
- Abdominal pregnancy: persistent abdominal pain, persistent nausea, fetal parts felt easily just under the abdominal wall, abnormal lie; can rarely progress to late second or third trimester.
- General: pallor, tachycardia, hypotension (in rupture); low-grade fever from peritoneal blood irritation is common and not a reliable sign of infection.[1]
- Abdomen: lower abdominal tenderness, often with guarding and rebound if ruptured; a palpable adnexal mass (haematocele or enlarged tube) in about 20%; shoulder-tip pain reproduced on lying flat if haemoperitoneum.
- Speculum: closed cervical os with dark scanty bleeding (unlike the open os and heavier bleeding of an inevitable miscarriage); rarely, products of conception are seen at the os (then think miscarriage or tubal abortion with passage).
- Bimanual examination: cervical motion tenderness ('chandelier sign'), adnexal tenderness, adnexal fullness or mass; an enlarged, soft uterus (the uterine decidua has developed in response to the ectopic's beta-hCG). Bimanual examination should be deferred if the patient is unstable or until the ectopic has been localised.
Differential Diagnosis
The differential of acute pelvic pain with vaginal bleeding in early pregnancy is broad. The classical triad of ectopic overlaps with miscarriage, and the acute rupture overlaps with any cause of acute abdominal pain in a young woman. A pregnancy test must be done first because it dictates the rest of the differential.[1]
| Condition | Key distinguishing feature |[1] |---|---| | Spontaneous miscarriage | Central, cramping suprapubic pain; heavier bright-red bleeding with clots and products of conception; open cervical os; uterus appropriately sized; TVS shows intrauterine pregnancy (failing or failed) | | Threatened miscarriage | Mild cramping, light bleeding, closed cervical os; viable intrauterine pregnancy on TVS | | PID / acute salpingitis | Bilateral lower abdominal pain, fever, vaginal discharge; usually no amenorrhoea; cervical motion tenderness and adnexal tenderness bilaterally; raised inflammatory markers | | Ovarian cyst rupture | Sudden pain at ovulation (mid-cycle) or with trauma; no amenorrhoea; TVS shows cyst with collapsed walls and free fluid; beta-hCG negative | | Ovarian torsion | Sudden severe pain with nausea and vomiting; tender adnexal mass; absent Doppler flow on TVS; pregnancy test usually negative | | Acute appendicitis | Migratory pain to right iliac fossa, anorexia, low-grade fever; no amenorrhoea; pregnancy test may be incidental positive | | Corpus luteum rupture | Mid-cycle sudden pain; small amount of free fluid; usually self-limiting; pregnancy test negative (unless a co-existing pregnancy) | | Urinary tract infection or ureteric colic | Dysuria, frequency, haematuria; loin-to-groin colic for stones; urinalysis positive; pregnancy test negative | | Gastroenteritis | Cramping central pain, vomiting, diarrhoea; frequently misdiagnoses ruptured ectopic — pregnancy test will distinguish | | Degenerating fibroid | Sharp localised pain, low-grade fever; uterine enlargement on examination; TVS shows fibroid with cystic change | | Round ligament pain (in an existing IUP) | Bilateral or unilateral groin pain in a known intrauterine pregnancy; benign, self-limiting |
Clinical & Bedside Assessment
ABCDE approach — especially if ruptured or unstable[1]
- A / B: high-flow oxygen by mask (15 L per minute via non-rebreather); secure airway if collapsed.[1]
- C: two large-bore 14 to 16 G intravenous cannulae, bloods (group and save, crossmatch 4 to 6 units, FBC, U&E, LFT, coagulation, beta-hCG), start warmed Hartmann's or 0.9% sodium chloride bolus (1 to 2 L) per major haemorrhage protocol. Activate the massive transfusion protocol if class III shock.
- D: assess level of consciousness — confusion and drowsiness are late signs of hypovolaemia.
- E: expose for full examination, keep warm (avoid hypothermia-induced coagulopathy).
Focused abdominal and pelvic examination[2]
- Abdomen: inspect for distension; palpate for tenderness, guarding, rebound (peritonism from blood), masses. Measure fundal height if uterus is palpable.[2]
- Speculum (gentle): inspect cervix and vagina; note bleeding, products of conception, or a closed os; take endocervical and high-vaginal swabs if infection suspected.
- Bimanual examination (gentle): cervical motion tenderness, adnexal tenderness, mass, fullness in the pouch of Douglas. Defer if unstable — vagal stimulation on a hypovolaemic patient can precipitate cardiac arrest.
- Vaginal examination in suspected cervical or caesarean scar ectopic must be extremely gentle — catastrophic bleeding can be provoked.
Always perform a urine or serum pregnancy test in any woman of reproductive age (consider up to age 50 to 55) presenting with abdominal pain, vaginal bleeding, syncope, gastrointestinal symptoms, or shock. This single reflex saves lives.[2]
Investigations
The diagnostic engine of modern ectopic management is the serial quantitative serum beta-hCG combined with TVS. The two tests are interpreted together, never in isolation.[1][2]
Key diagnostic thresholds to memorise
The investigations, in order[1]
- Urine pregnancy test (beta-hCG): qualitative, sensitive to about 25 IU/L; the first investigation in any woman of reproductive age with abdominal pain or bleeding. A negative urine test in a symptomatic patient can be confirmed with a more sensitive serum beta-hCG.[1]
- Quantitative serum beta-hCG: the cornerstone. Single values are interpreted against the discriminatory zone — the beta-hCG level above which a normal intrauterine pregnancy should be visible on TVS. The widely quoted zone is 1500 to 2000 IU/L for TVS and 3500 to 6500 IU/L for transabdominal ultrasound. A beta-hCG above the discriminatory zone with an empty uterus on TVS = ectopic until proven otherwise. Below the zone, serial beta-hCG at 48 hours distinguishes a viable IUP (rise 63 to 100% in 48 hours in 85% of viable pregnancies, with the slowest 15% rising at least 35%) from a failing pregnancy of unknown location (PUL).
- Transvaginal ultrasound (TVS): the principal diagnostic imaging modality, performed in every stable patient with a positive pregnancy test and pain or bleeding. Findings in ectopic pregnancy:
- Empty uterus with endometrial thickening and a 'pseudosac' (a small collection of fluid in the uterine cavity surrounded by a single layer of decidua — distinguish from a true gestational sac which has a 'double decidual sign' and a yolk sac).
- Adnexal mass: a complex adnexal mass, a gestational sac containing a yolk sac or embryo (definitive), or a hyperechoic 'ring of fire' around an ectopic on colour Doppler (sensitive but not specific — a corpus luteum can look identical).
- Embryonic cardiac activity in the adnexa is pathognomonic.
- Free fluid in the pouch of Douglas (an organised, echogenic collection suggests haemoperitoneum from rupture or tubal abortion). Echogenic free fluid greater than one-third of the way up the uterus anteriorly, or fluid in the hepatorenal (Morison's) pouch, indicates significant haemoperitoneum.
- Full blood count: anaemia from chronic leak or acute bleed; leukocytosis is common and unreliable for infection; baseline haemoglobin before surgery or methotrexate.
- Blood group and antibody screen, crossmatch 4 to 6 units if ruptured or pre-operative.
- Serum progesterone: a level under 20 to 25 nmol/L (under 6 to 8 ng/mL) suggests a non-viable pregnancy (ectopic or failing IUP) and can speed triage; a level over 60 nmol/L favours a viable IUP. Not used alone to locate the pregnancy.
- Urea, electrolytes, liver function tests, coagulation screen — baseline before methotrexate or surgery.
- Diagnostic laparoscopy — the historic gold standard, now reserved for: (a) haemodynamic instability precluding ultrasound; (b) inconclusive TVS and rising beta-hCG; (c) suspected heterotopic pregnancy with persisting pain. Allows simultaneous diagnosis and treatment.
A 27-year-old has beta-hCG 1800 IU/L and an empty uterus on TVS — what now?
This is a pregnancy of unknown location (PUL) above the discriminatory zone. The next step is repeat TVS by an experienced sonographer within 48 hours and serial beta-hCG at 48 hours. If beta-hCG is rising subnormally or TVS confirms an adnexal mass, manage as ectopic. If the patient becomes unstable at any point, proceed to diagnostic laparoscopy.[1]
Management — Resuscitation
Ruptured ectopic with shock is a surgical emergency. Resuscitation proceeds concurrently with preparation for theatre and continues into the operating room. The two cardinal errors are (1) delaying surgery for confirmatory imaging in an unstable patient, and (2) forgetting Anti-D in a Rh-negative woman.[1][2]
Resuscitation pathway for the unstable ectopic
Recognise
Call for help
ABC
Bloods
Consent and theatre
Anti-D
Management — Definitive
Definitive management of a confirmed ectopic pregnancy is stratified by haemodynamic stability, size and beta-hCG, presence of cardiac activity, the patient's wish to preserve fertility, and her reliability to attend follow-up. Three pathways exist: expectant, medical, and surgical.[1]
Expectant management
Selected patients with very low and falling beta-hCG may resolve spontaneously because the tubal pregnancy undergoes a tubal abortion or mole. Strict criteria:[1]
- beta-hCG under 1500 IU/L and falling on serial measurement (the lower the level, the higher the success).[1]
- Asymptomatic or only mild pain; no evidence of rupture.
- Ectopic mass under 3 cm and no cardiac activity.
- Reliable for follow-up: weekly serum beta-hCG until negative (typically two to three weeks, sometimes longer).
Follow-up is mandatory because a small proportion rupture even with falling titres. About 70 to 90% of selected patients resolve; treatment is needed if beta-hCG rises, symptoms worsen, or there is new free fluid.[1][5]
Medical management — methotrexate
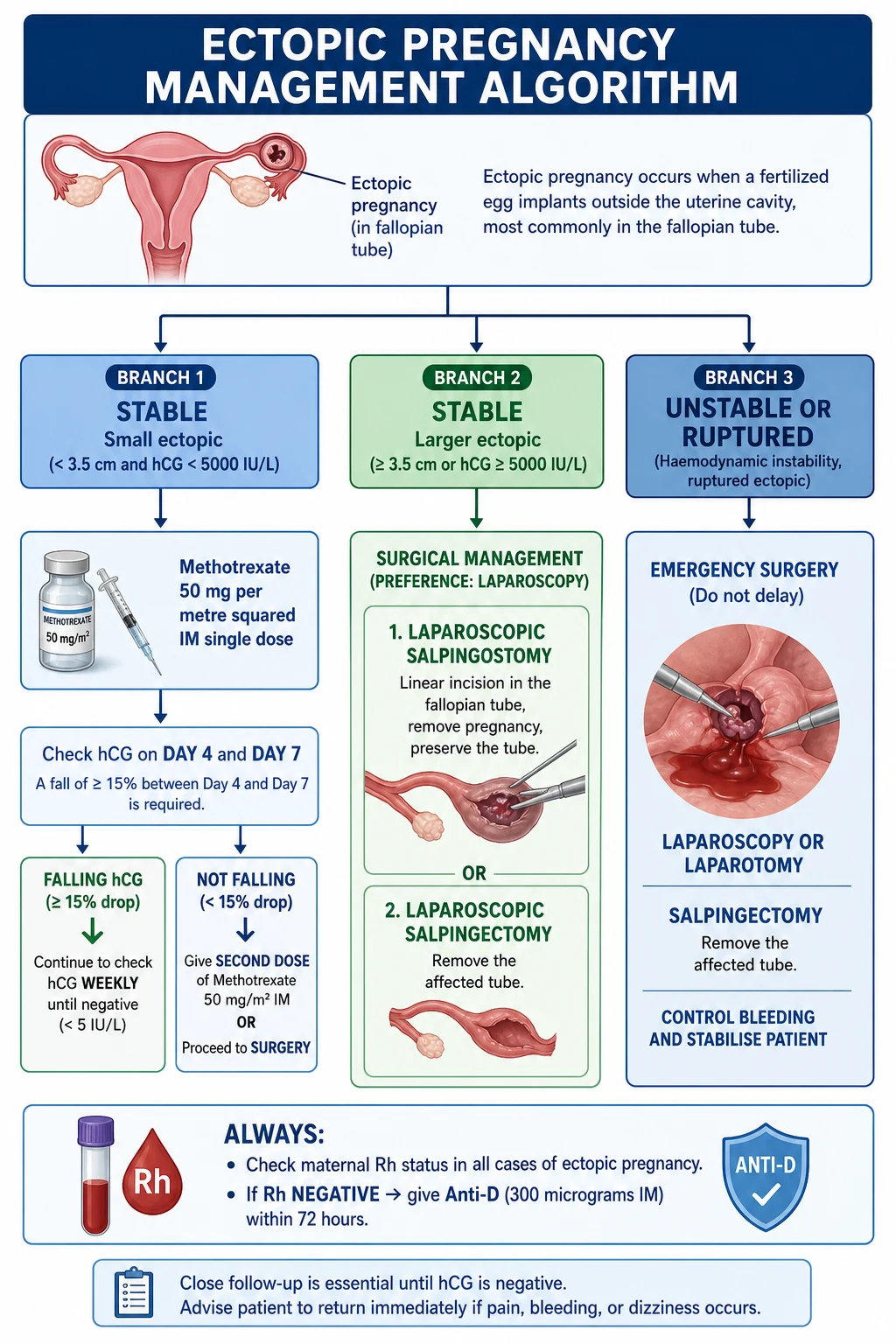
Methotrexate is a folate antagonist that inhibits dihydrofolate reductase, blocking DNA synthesis in rapidly dividing trophoblast. Single-dose intramuscular methotrexate is first-line medical therapy for stable unruptured ectopic pregnancy meeting strict criteria.[1][2]
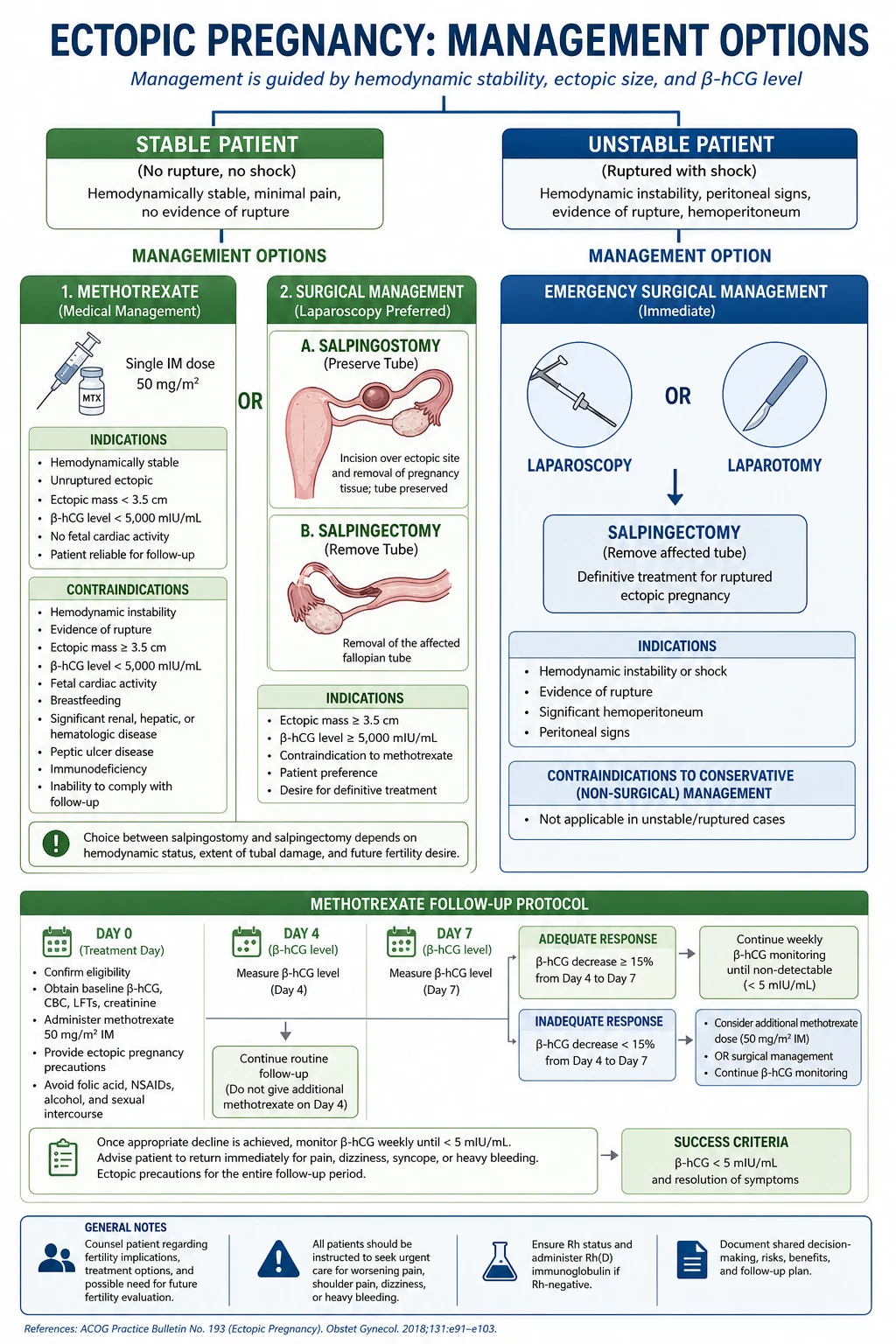
Criteria for single-dose methotrexate (50 mg per metre squared IM):[1]
- Haemodynamically stable, no signs of rupture, mild or no pain.[1]
- Unruptured tubal ectopic confirmed on TVS.
- Ectopic mass under 3.5 cm in maximum diameter.
- Serum beta-hCG under 5000 IU/L (success falls as the titre rises — roughly 90% under 5000, 80% under 10,000, and 60 to 70% over 10,000).
- No fetal cardiac activity on TVS (relative contraindication; some protocols allow higher doses).
- Patient able and willing to comply with follow-up (mandatory day 4, day 7, then weekly beta-hCG).
- No contraindications: normal full blood count (neutrophils over 1.5, platelets over 100), normal liver function (transaminases under twice the upper limit of normal), normal renal function. No active pulmonary disease (rare methotrexate pneumonitis), no peptic ulcer disease, no breastfeeding, no immunocompromise. Reliable contraception for the treatment cycle and for three months afterwards (because methotrexate is teratogenic).
Protocol and follow-up[1]
- Day 1: measure baseline FBC, U&E, LFT, beta-hCG; administer methotrexate 50 mg per metre squared intramuscularly (single dose). Calculate body surface area and round to the nearest milligram.[1][5]
- Day 4: repeat serum beta-hCG (often rises transiently as trophoblast breaks down).
- Day 7: repeat serum beta-hCG and FBC, U&E, LFT.
- If beta-hCG has fallen by at least 15% between day 4 and day 7: continue weekly serum beta-hCG until it is undetectable (typically three to seven weeks).
- If the fall is less than 15%: give a second dose of methotrexate (about 15 to 20% of patients) or proceed to surgery.
- If rising: high risk of rupture — proceed to surgery.
- Patient advice during treatment: avoid alcohol, folic acid and folate-containing multivitamins (antagonise methotrexate), NSAIDs (compete for renal tubular secretion), excessive sun exposure (photosensitivity), and vigorous activity or sexual intercourse (risk of rupture). Use reliable contraception and avoid pregnancy for three months after the dose.
- Warning signs to return immediately: severe abdominal pain, shoulder-tip pain, syncope, heavy vaginal bleeding, fever, severe mouth ulcers, or shortness of breath.
Methotrexate side effects: stomatitis, gastritis, transient transaminitis, bone marrow suppression (rare with single dose), pleuritis or pneumonitis (rare but serious — stop and investigate if respiratory symptoms).[1]
Success rate: approximately 85 to 95% when criteria are met; tubal patency after methotrexate is similar to after surgery, with subsequent intrauterine pregnancy rates of about 60 to 70% and recurrent ectopic rates of about 10 to 15%.[2][3]
Surgical management
Laparoscopy is the default surgical approach for the stable or even the haemodynamically compromised (with appropriate anaesthetic and surgical expertise) patient, with shorter recovery, less blood loss, fewer adhesions, and better cosmesis than laparotomy. Laparotomy is reserved for the haemodynamically unstable patient when laparoscopic expertise is unavailable, or for the rupture of an interstitial or cornual ectopic where control of the uterine and ovarian artery supply is required.[1][3]
The 2014 ESEP randomised trial (Mol et al, Lancet) compared salpingotomy with salpingectomy in 446 women with a tubal pregnancy and a healthy contralateral tube and found no difference in the cumulative ongoing pregnancy rate by natural conception at three years (about 60% in each arm) — but salpingotomy was associated with a higher rate of persistent trophoblast (7 versus 0.4%) and required more additional treatment. Salpingotomy was also not cost-effective. The take-home message: salpingectomy is at least as good as salpingotomy when the contralateral tube is healthy, and avoids persistent trophoblast.[3]
1. Linear salpingostomy (salpingotomy)[1]
- A longitudinal linear incision on the anti-mesenteric border of the tube over the ectopic, with gentle evacuation of the pregnancy products. The tube is left to heal by secondary intention; the incision is usually not sutured.[1]
- Indication: stable patient who wishes to preserve the tube, especially when the contralateral tube is damaged or absent and future fertility is desired; unruptured ampullary ectopic.
- Risk: persistent trophoblast in 5 to 10% — mandatory weekly serum beta-hCG until negative. Rising titres after salpingostomy are treated with methotrexate.
2. Salpingectomy[1]
- Total or partial removal of the fallopian tube with the ectopic, secured at the cornu and the mesosalpinx with diathermy, clips, or loops.[1]
- Indication: ruptured ectopic, large ectopic (over 3.5 cm), recurrent ectopic in the same tube, uncontrolled bleeding, severe tubal damage, heterotopic pregnancy where the IUP is to be preserved, or patient choice.
- No risk of persistent trophoblast.
3. Partial salpingectomy (segmental resection) — for isthmic ectopics where the diseased segment is removed and the tube may be re-anastomosed later.[1]
4. Emergency laparotomy (if unstable or laparoscopy not available): rapid lower-midline or Pfannenstiel incision, rapid control of bleeding by clamping the infundibulopelvic ligament, salpingectomy, evacuate haemoperitoneum, autotransfusion (cell salvage) where available.[1]
Special surgical scenarios
- Cornual or interstitial ectopic: laparoscopic cornual resection with suture closure, or in unstable rupture a classical laparotomy with wedge resection; methotrexate (local or systemic) may be used for early stable cases. Risk of massive bleeding from the uterine and ovarian artery supply.[2]
- Cervical ectopic: methotrexate preferred (systemic or direct intra-sac injection); surgical evacuation risks catastrophic bleeding. If surgery is unavoidable: uterine artery embolisation, Foley catheter balloon tamponade, cervical cerclage stitch, or balloon tamponade, with hysterectomy as last resort.
- Caesarean scar ectopic: systemic methotrexate plus or minus local potassium chloride injection into the sac, with or without dilation and curettage under transabdominal ultrasound guidance; uterine artery embolisation may be combined. Hysterectomy reserved for uncontrolled bleeding.
- Ovarian ectopic: wedge resection or partial oophorectomy; oophorectomy if bleeding uncontrolled.
- Heterotopic pregnancy (IVF): salpingectomy for the ectopic (avoids methotrexate, which would terminate the desired intrauterine pregnancy), with careful preservation of the IUP.
Anti-D and post-treatment care
Always check maternal Rh status in any woman with ectopic pregnancy, miscarriage, antepartum haemorrhage, or sensitising event. Give anti-D immunoglobulin 250 IU IM to all Rh-negative women within 72 hours (use 500 IU if gestation over 20 weeks or large bleed). Anti-D prevents isoimmunisation that could cause haemolytic disease of the fetus and newborn (HDFN) in a future pregnancy.[1]
Post-treatment: routine 6-week follow-up to confirm beta-hCG is negative (especially after methotrexate or salpingostomy), offer psychological support and contraception, discuss the early pregnancy unit (EPU) referral for the next pregnancy (early TVS at 6 to 7 weeks to confirm intrauterine location), and screen for and treat any underlying STI.[1]
Methotrexate follow-up — the FALL protocol
FALL
serum beta-hCG on day 4 and day 7 after the dose
compare day 4 and day 7 beta-hCG to measure response
give a second dose of methotrexate or proceed to surgery
if beta-hCG falls by at least 15%, continue weekly until undetectable
Risk factors for ectopic — TUBAL PAIN
TUBAL PAIN
previous tubal ligation, re-anastomosis, or fimbrioplasty
assisted reproduction (2 to 5% ectopic rate)
PID — chlamydia, gonorrhoea — most common risk factor
rising maternal age
pregnancy with an IUCD in situ is more likely to be ectopic
10 to 15% recurrence after one, 25 to 30% after two
congenital or DES-induced tubal anomalies
endometriosis, appendicitis, adhesions
dose-dependent ciliary impairment
Specific Subtypes & Scenarios
Each non-ampullary ectopic has its own diagnostic trap and management plan and is favourite SAQ or viva territory.[1]
Interstitial (cornual) pregnancy implants in the interstitial portion of the tube — the 1 to 2 cm of tube that traverses the uterine wall. Because the surrounding myometrium is thick and vascular, the pregnancy grows painless for longer (10 to 14 weeks) before the wall thins and ruptures catastrophically into the broad ligament or peritoneum, with massive bleeding from the anastomosis of the uterine and ovarian arteries. Diagnosis is difficult: the sac looks intrauterine on TVS, but the myometrial mantle is thin (under 5 mm) on all sides ('interstitial line sign'). Risk factors include IVF, previous cornual surgery, and previous salpingectomy. Management is systemic or local methotrexate for early stable cases; laparoscopic cornual resection for stable cases; emergency laparotomy with wedge resection or hysterectomy for rupture. Maternal mortality is the highest of all ectopics at 2 to 2.5%.[2]
Cervical pregnancy implants in the cervical stroma below the level of the internal os. It presents with painless, profuse, bright-red vaginal bleeding because the cervix is rich in vessels but lacks contractile myometrium to retract and stop bleeding. On TVS the gestational sac is within the cervical canal, the internal os is closed, and the uterine body is empty ('hourglass' uterus). Dilation and curettage is contraindicated as first-line because it provokes catastrophic bleeding. Systemic or local methotrexate is first-line; adjuncts for uncontrolled bleeding include Foley balloon tamponade (24 to 48 hours), cervical cerclage stitch, bilateral uterine artery embolisation, and as a last resort hysterectomy.[1]
Caesarean scar pregnancy implants in the fibrous scar of a previous caesarean section. Its incidence is rising in step with the global caesarean rate (now roughly 1 in 2000 to 1 in 2000 pregnancies in some series). On TVS the gestational sac is implanted in the anterior lower uterine segment at the scar, with thin or absent myometrium between the sac and the bladder. Risks of progression include uterine rupture and placenta accreta spectrum. Management combines systemic methotrexate, local potassium chloride or methotrexate injection into the sac, dilation and curettage under transabdominal ultrasound guidance, and bilateral uterine artery embolisation; hysterectomy for haemorrhage.[1]
Ovarian pregnancy is the most common non-tubal ectopic after cervical and caesarean scar. Diagnostic criteria (Spielberg) require that the tube and fimbriae are intact, the gestational sac occupies the ovary, the sac is connected to the uterus by the ovarian ligament, and ovarian tissue is confirmed histologically in the sac wall. Management is ovarian wedge resection or oophorectomy.[1]
Abdominal pregnancy is rare (1 in 10,000 pregnancies) but can be life-threatening. Primary abdominal pregnancy implants directly in the peritoneal cavity; secondary follows tubal rupture with re-implantation on bowel, omentum, broad ligament, or liver. Diagnosis is often missed. Suspicious features include persistent abdominal pain, easily palpable fetal parts, abnormal lie, and an empty uterus on TVS with a separate adnexal mass. Management is laparotomy with removal of the fetus and placenta (the placenta is left in situ if it cannot be safely removed because its vascular supply cannot be controlled). Maternal mortality is up to 20%, and perinatal mortality is very high.[2]
Heterotopic pregnancy — simultaneous intrauterine and ectopic pregnancy — is rare in spontaneous conceptions (about 1 in 30,000) but occurs in 1 in 100 IVF pregnancies (and up to 1 in 30 in some high-order multiple transfer protocols). The diagnosis is frequently missed because the intrauterine pregnancy is identified on ultrasound and the clinician stops looking. Always scan both adnexae in any IVF pregnancy with pain, falling haematocrit, or persistent symptoms despite a viable IUP. Management is salpingectomy (not methotrexate, which would terminate the IUP); the IUP usually continues normally.[1]
Persistent trophoblast is a complication (rather than a subtype) of salpingostomy and methotrexate: residual trophoblastic tissue continues to produce beta-hCG and can rupture weeks later. Mandatory weekly serum beta-hCG until negative after either treatment; rising titres are treated with methotrexate (or repeat surgery if rupture occurs).[3]
Complications & Pitfalls
Disease-related complications[1]
- Tubal rupture with massive intraperitoneal haemorrhage — the leading cause of death; can be 2 to 3 litres within minutes.[1]
- Chronic anaemia and pelvic haematocele from intermittent tubal leak.
- Infection of retained haemoperitoneum or pelvic haematocele (rare).
- Recurrence — 10 to 15% after one ectopic, 25 to 30% after two.
- Subfertility — tubal damage reduces future intrauterine pregnancy rates.
- Psychological impact — grief, anxiety about future pregnancies.
Treatment-related complications[1]
- Persistent trophoblast — 5 to 10% after salpingostomy, 4 to 15% after methotrexate; detected by serial beta-hCG; risks late rupture.[1][3]
- Methotrexate side effects — stomatitis, gastritis, transient transaminitis, photosensitivity, bone marrow suppression (rare), pneumonitis (rare but serious). Teratogenic — must avoid pregnancy for three months.
- Surgical complications — bleeding, infection, visceral injury (especially to bowel during laparoscopy), anaesthetic risks.
- Rh sensitisation if Anti-D omitted in a Rh-negative woman.
- Missing the diagnosis in a 'stable' woman who then ruptures — the leading cause of preventable death. The lesson: pregnancy test in any woman of reproductive age with abdominal pain or bleeding.[1]
- Misdiagnosing an interstitial ectopic as an intrauterine pregnancy because the sac appears within the uterus. Look at the myometrial mantle on all sides of the sac.
- Misinterpreting the 'pseudosac' as a true gestational sac — a true sac has a yolk sac and a 'double decidual sign'; a pseudosac is central, irregular, and lacks the double decidual sign.
- Stopping ultrasound when an IUP is found — missing a heterotopic pregnancy in an IVF patient. Always image both adnexae.
- Forgetting to give Anti-D to a Rh-negative woman within 72 hours.
- Forgetting post-methotrexate or post-salpingostomy follow-up — persistent trophoblast can rupture weeks later.
- Treating a pregnancy of unknown location with methotrexate before serial beta-hCG confirms the diagnosis — methotrexate will terminate a viable IUP.
- Delaying surgery for imaging in an unstable patient — go to theatre.
- Performing dilation and curettage on a cervical ectopic — catastrophic bleeding.
- Underestimating the volume of blood lost — a young woman may maintain her blood pressure until 30% of her volume is gone, then collapse.
Prognosis & Disposition
Future fertility and recurrence after ectopic
The prognosis for future fertility depends on the management used, the state of the contralateral tube, and the underlying tubal pathology. The ESEP trial (Mol et al, 2014) showed that in women with a healthy contralateral tube, salpingostomy and salpingectomy produced equivalent cumulative ongoing pregnancy rates by natural conception (about 60% at three years) — so salpingectomy is preferred because it avoids persistent trophoblast.[3] With a damaged contralateral tube, salpingostomy (tube preservation) may be the better choice; subsequent conception may require IVF.
After any ectopic pregnancy, advise the patient to:[1]
- Attend the early pregnancy unit (EPU) in the next pregnancy for TVS at 6 to 7 weeks to confirm intrauterine location.
- Use reliable contraception for three months after methotrexate (teratogenic).
- Be screened for and treated for chlamydia and other STIs; consider hysterosalpingography or laparoscopy and dye if subfertility persists.
Disposition[1]
- Stable, methotrexate-treated: discharged with safety-net advice and weekly beta-hCG follow-up until undetectable. Return immediately for severe pain, shoulder-tip pain, syncope, or fever.[1]
- Stable, surgically treated: discharge within 24 to 48 hours of laparoscopic salpingectomy; routine 6-week follow-up.
- Unstable / ruptured: high-dependency or intensive care postoperatively; transfuse as needed; consider cell salvage where available.
- All patients: Rh status check and Anti-D if negative; chlamydia screening; psychological support; contraception counselling; EPU referral card for next pregnancy.
Special Populations
- IVF and assisted reproduction patients: ectopic risk 2 to 5%; heterotopic pregnancy risk up to 1 in 100. Every IVF pregnancy should have early TVS at 6 to 7 weeks confirming intrauterine location with both adnexae assessed. Persistent pain or falling haematocrit despite a viable IUP should prompt a search for a heterotopic ectopic.[1]
- Previous ectopic pregnancy: 10 to 15% recurrence. Early TVS in the next pregnancy is mandatory.
- IUCD in situ at conception: if a pregnancy occurs with an IUCD, 15 to 50% are ectopic. Remove the IUCD if visible strings are accessible and arrange urgent TVS and beta-hCG.[1]
- Genital tuberculosis (endemic areas — India, South Asia, sub-Saharan Africa): causes tubal destruction with characteristic 'beaded' or 'lead-pipe' tubes; high ectopic rate even after successful anti-tubercular therapy. High index of suspicion in any patient with a past history of infertility and chronic pelvic pain from endemic regions.[4]
- Adolescents (under 18): late presentation is common because of denial of pregnancy and fear of disclosure; maintain a low threshold for pregnancy testing.
- Perimenopausal women (over 45): pregnancy is rare but ectopics still occur; the diagnosis is often missed because pregnancy is not considered.
- Patients on anticoagulation, with coagulopathy, or refusing blood products: coordinate with haematology; cell salvage and tranexamic acid may be needed; manage in a centre with bloodless medicine expertise.
Evidence, Guidelines & Regional Differences
- Sensitive beta-hCG assays and high-resolution TVS (1980s onward) transformed ectopic pregnancy from a disease diagnosed at rupture to one diagnosed and treated before rupture. Case-fatality fell from about 35 deaths per 10,000 ectopics in 1970 to 3 to 4 per 10,000 today.[4][1]
- Methotrexate for ectopic pregnancy (Stovall, 1991; Lipscomb, 1999) established single-dose IM methotrexate as effective first-line medical therapy for selected patients, with success rates of 85 to 95%.[1]
- The ESEP trial (2014) settled the salpingostomy versus salpingectomy debate in women with a healthy contralateral tube — they are equivalent for future fertility, and salpingectomy is preferred because it avoids persistent trophoblast.[3]
- CDC surveillance (MMWR, 2012) identified illicit drug use and delayed presentation as key drivers of ectopic-related death in a Florida cluster, with maternal mortality ratios rising to 2.5 per 100,000 live births in 2009 to 2010.[4]
Guideline differences by region[1][2]
India and low-resource settings: genital tuberculosis is a major additional cause of ectopic pregnancy; late presentation of ruptured ectopic is common in rural areas due to limited ultrasound and transport delays; access to emergency laparoscopy is limited, so open surgery is often the only option. Anti-D availability must be ensured. PID from untreated STIs (chlamydia, gonorrhoea) is the commonest underlying cause; screen and treat for STIs to prevent recurrence. In sub-Saharan Africa and South Asia, ectopic-related maternal mortality remains 10- to 20-fold higher than in high-income settings. The WHO and FIGO prioritise early pregnancy unit development, access to TVS, and methotrexate for stable cases.[4]
Where the evidence is weak or controversial[1][5]
- The discriminatory zone is statistical, not absolute; modern multi-specialty units may use 2000 or 3500 IU/L as a more conservative threshold because some normal IUPs are not visible on TVS at 1500 IU/L, particularly with less experienced sonographers. Treating a PUL with methotrexate before a viable IUP is excluded risks terminating a wanted pregnancy.[1][5]
- The best management of a caesarean scar ectopic is not settled; current options (systemic methotrexate, local injection, hysteroscopic resection, uterine artery embolisation, laparoscopic resection) have not been compared in randomised trials.
- Whether repeat-dose methotrexate is preferable to surgery for the 15 to 20% who fail first-dose methotrexate is being studied.
Prevention
Ectopic pregnancy cannot always be prevented, but risk can be reduced by tackling the upstream causes.[1]
- STI screening and treatment — screen sexually active women under 25 for chlamydia annually; treat chlamydia and gonorrhoea promptly and trace contacts. Each prevented episode of salpingitis prevents future ectopics.[1]
- Smoking cessation — reduces dose-dependent tubal ciliary impairment.
- Safe sexual health and contraception — reduces unplanned pregnancy and STI transmission.
- Single-embryo transfer in IVF — reduces heterotopic pregnancy risk versus double-embryo transfer.
- Early pregnancy surveillance in women with previous ectopic, tubal surgery, or known tubal disease — early TVS at 6 to 7 weeks.
- Prompt diagnosis of any pregnancy of unknown location by serial beta-hCG and TVS prevents rupture.
Exam Pearls
- Triad: amenorrhoea + abdominal pain + vaginal bleeding = ectopic until proven otherwise.[1]
- Most common site: ampulla (about 75%).[1]
- Most common risk factor: PID (chlamydia).[1]
- Discriminatory zone: beta-hCG 1500 to 2000 IU/L should show an intrauterine sac on TVS.[1][2]
- Subnormal beta-hCG rise in 48 hours (under 63%) suggests non-viable or ectopic pregnancy.
- Shoulder tip pain + collapse = ruptured ectopic (haemoperitoneum, diaphragmatic irritation via the phrenic nerve C3 to C5).[2]
- Methotrexate criteria: unruptured, under 3.5 cm, beta-hCG under 5000 IU/L, no cardiac activity, stable, compliant, no contraindications.[1]
- Methotrexate follow-up: day 4 and day 7 beta-hCG, need at least 15% fall between them; otherwise second dose or surgery.[1]
- Single dose methotrexate: 50 mg per metre squared IM.[1]
- ALWAYS check Rh status, give Anti-D 250 IU IM within 72 hours to Rh-negative women.[1]
- Pregnancy test first in any woman of reproductive age with abdominal pain.[2]
- Salpingostomy preserves the tube but risks persistent trophoblast (5 to 10%); salpingectomy removes the tube and is preferred when the contralateral tube is healthy (ESEP trial, 2014).[3]
- Interstitial (cornual): ruptures LATER (10 to 14 weeks) with MASSIVE bleeding (uterine artery). Myometrial mantle under 5 mm on all sides = interstitial line sign.
- Cervical ectopic: profuse PAINLESS bleeding; methotrexate, NOT dilation and curettage.[1]
- Heterotopic: IUP AND ectopic simultaneously; IVF risk 1 in 100. Always scan both adnexae.[1]
- Recurrence 10 to 15% after one ectopic, 25 to 30% after two; early TVS in next pregnancy.[1]
- Pseudosac in uterus = decidual reaction to ectopic beta-hCG; distinguish from true gestational sac (look for yolk sac and double decidual sign).
- Three classic trap answers: 'pregnancy test positive + empty uterus + adnexal mass' = ectopic; 'shoulder tip pain in a young woman' = ruptured ectopic; 'profuse painless bleeding in early pregnancy' = cervical ectopic.
References
- [1]American College of Obstetricians and Gynecologists' Committee on Practice Bulletins—Gynecology; Barnhart KT, Franasiak JM. ACOG Practice Bulletin No. 193: Tubal Ectopic Pregnancy. Obstetrics & Gynecology, 2018.PMID 29470343
- [2]Barnhart KT. Clinical practice. Ectopic pregnancy. New England Journal of Medicine, 2009.PMID 19625718
- [3]Mol F, van Mello NM, Strandell A, Strandell K, Jurkovic D, Ross J, Barnhart KT, Yalcinkaya TM, Verhoeve HR, Graziosi GCM, Koks CAM, Klinte I, Hogström L, Janssen ICAH, Kragt H, Hoek A, Trimbos-Kemper TCM, Broekmans FJM, Willemsen WNP, Ankum WM, Mol BW, van Wely M, van der Veen F, Hajenius PJ; European Surgery in Ectopic Pregnancy (ESEP) study group. Salpingotomy versus salpingectomy in women with tubal pregnancy (ESEP study): an open-label, multicentre, randomised controlled trial. Lancet, 2014.PMID 24499812
- [4]Centers for Disease Control and Prevention (CDC). Ectopic pregnancy mortality — Florida, 2009-2010. MMWR Morbidity and Mortality Weekly Report, 2012.PMID 22337175
- [5]Hajenius PJ, Mol F, Mol BW, Bossuyt PM, Ankum WM, van der Veen F. Interventions for tubal ectopic pregnancy. Cochrane Database of Systematic Reviews, 2007.PMID 17253448