Obstetrics and Gynaecology · Obstetrics and Gynaecology
Endometrial Cancer
Also known as Uterine cancer · Endometrial carcinoma · Endometrioid adenocarcinoma · Uterine serous carcinoma · Cancer of corpus uteri
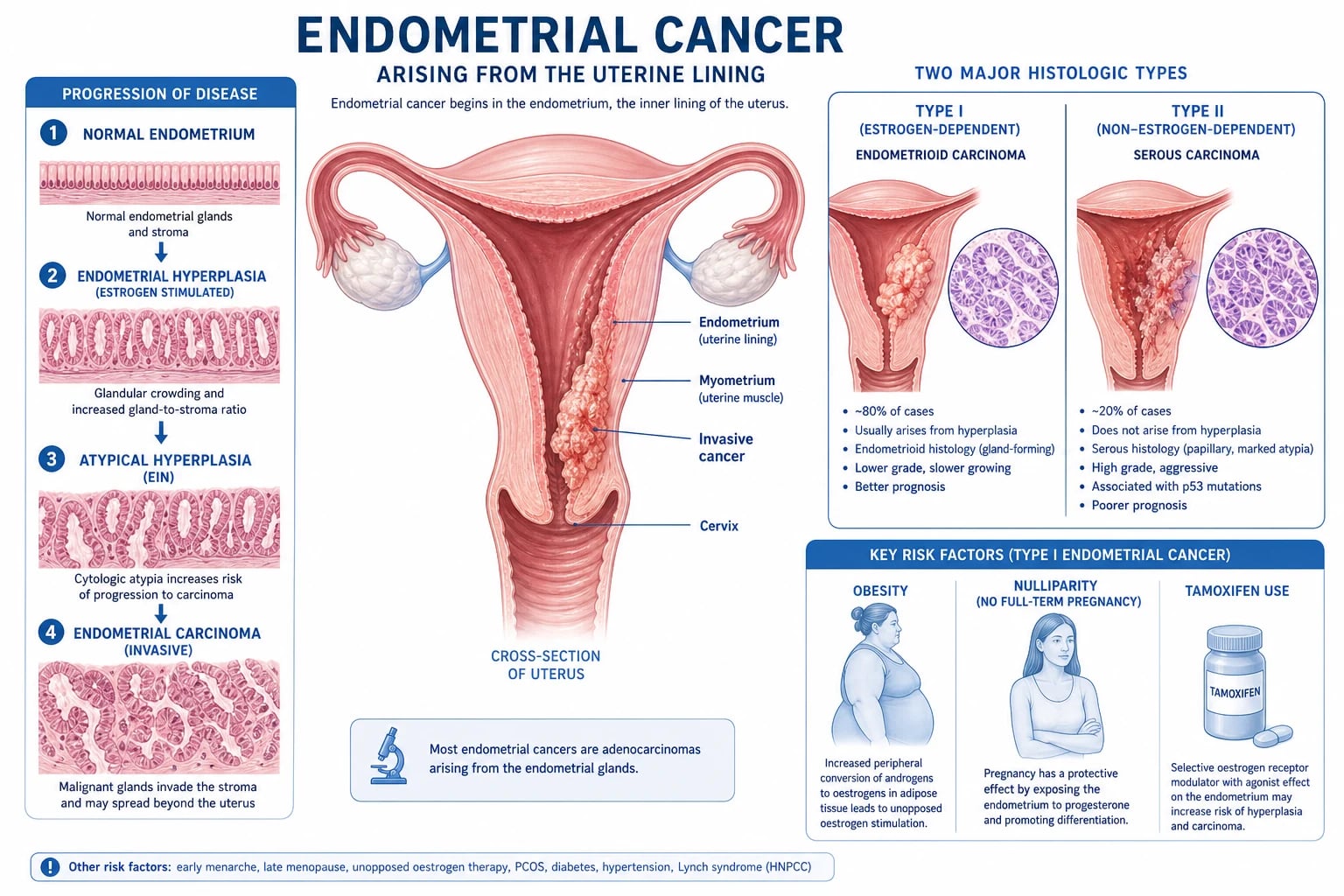
Endometrial cancer is the most common gynaecological malignancy in developed countries and the sixth most common cancer in women. Around 90 per cent present with postmenopausal bleeding, which is cancer until proven otherwise. Two pathogenetic types exist: Type I (endometrioid, 80 per cent) is oestrogen-driven, arising through unopposed oestrogen stimulation, endometrial hyperplasia with atypia and well-differentiated carcinoma, with PTEN, PIK3CA, KRAS and ARID1A mutations and a favourable prognosis; Type II (serous, clear cell, carcinosarcoma, 20 per cent) is not oestrogen-driven, arises in atrophic endometrium, carries TP53 mutations, and is aggressive. Diagnosis is by transvaginal ultrasound (endometrial thickness over 4 to 5 mm in a postmenopausal woman prompts biopsy), pipelle or hysteroscopy and dilation and curettage, and pelvic MRI for myometrial invasion and staging. Treatment is total hysterectomy, bilateral salpingo-oophorectomy, plus sentinel or full lymph node assessment, with adjuvant vault brachytherapy for intermediate risk (PORTEC), external beam radiotherapy and chemotherapy (carboplatin and paclitaxel) for high-risk and advanced disease, and high-dose progestin for fertility-sparing management of grade 1 disease.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Exam tags
Red flags
Overview & Definition
Endometrial cancer is a malignant epithelial tumour arising from the glandular epithelium that lines the uterine cavity. It is the most common gynaecological malignancy in developed countries and the sixth most common cancer in women worldwide, with an estimated 417,000 new cases and 97,000 deaths in 2020.[1] Unlike cervical cancer (which is dominated by low-resource settings), endometrial cancer is a disease of affluence, ageing, and obesity: the highest incidence is seen in North America and Europe, and the global rise is driven by the obesity epidemic, increasing life expectancy, and the fall in cervical cancer mortality from screening. Lifetime risk in a developed country is approximately 3 per cent, meaning roughly one woman in 30 will develop it.[1][2]
The clinical importance of endometrial cancer lies in its early presentation. Because the endometrium lines a cavity that communicates with the vagina, even a small superficial tumour bleeds — and bleeding is reported. Around 90 per cent of women present with postmenopausal bleeding, and most of these have early-stage, surgically curable disease. The challenge for the clinician is not treating advanced cancer, but the systematic, evidence-based triage of every woman who bleeds after the menopause so that the 5 to 10 per cent with cancer are identified without over-investigating the 90 per cent with benign causes.[2]
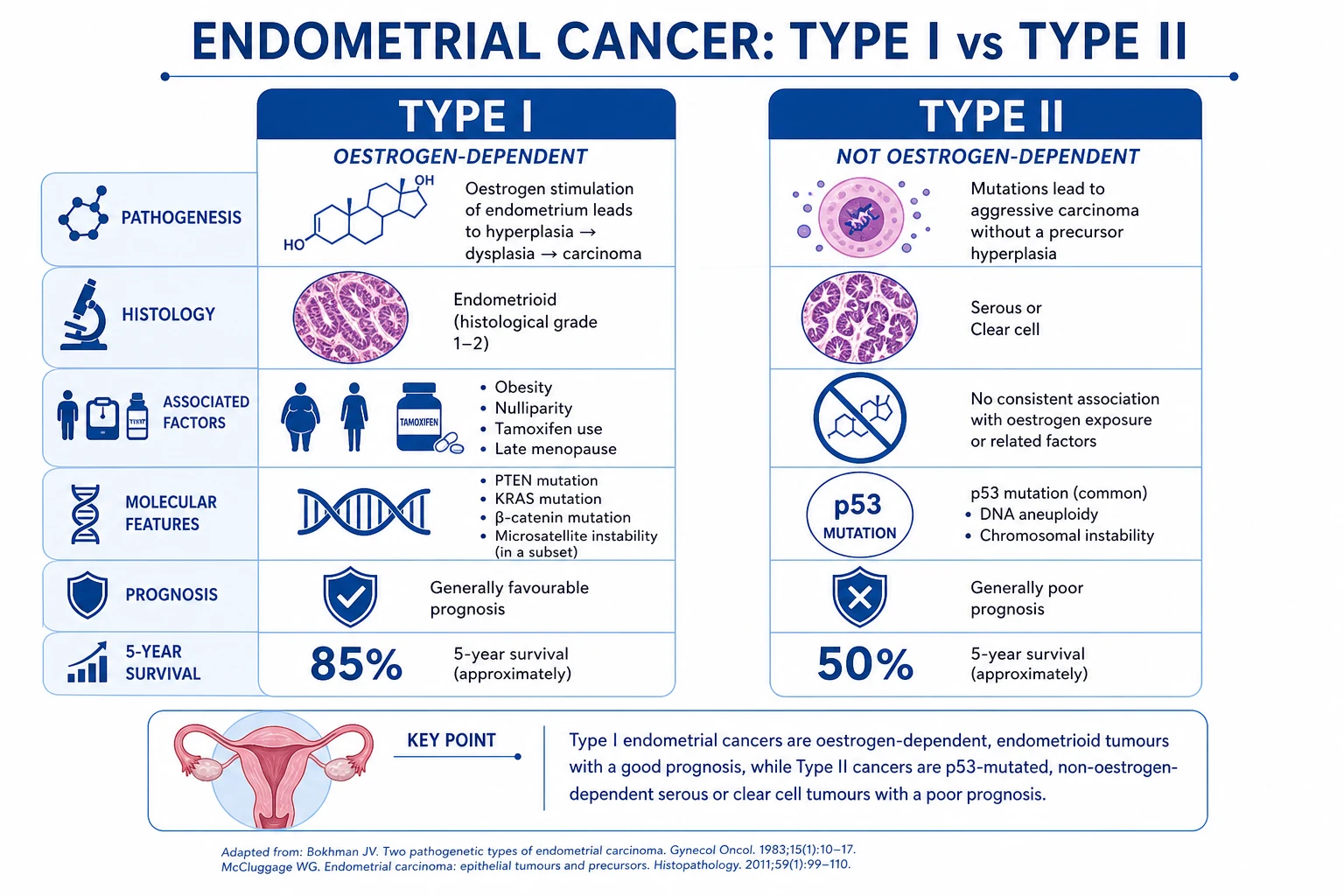
The disease is best understood through the Bokhman dualistic model, proposed in 1983 and refined by modern genomics. Type I tumours (about 80 per cent) are oestrogen-driven, low-grade endometrioid adenocarcinomas that develop in perimenopausal or postmenopausal women with a background of unopposed oestrogen stimulation (obesity, nulliparity, late menopause, polycystic ovary syndrome, oestrogen-only hormone replacement therapy, tamoxifen). They are preceded by endometrial hyperplasia with atypia, carry a characteristic mutational profile (PTEN loss, PIK3CA, KRAS, ARID1A, microsatellite instability), and have an excellent prognosis with five-year survival over 85 per cent. Type II tumours (about 20 per cent) are high-grade serous, clear cell, or carcinosarcomas that arise in atrophic endometrium of older, thinner women, are not oestrogen-driven, carry TP53 mutations, present at a more advanced stage, and carry a poor prognosis even when apparently early.[5][16]
The 2023 FIGO revision (the Berek revision) incorporated molecular classification into staging for the first time, formally recognising four molecular subgroups defined by The Cancer Genome Atlas — POLE-ultramutated, mismatch repair deficient (MMRd), p53-abnormal (copy-number high), and p53-wildtype (no specific molecular profile, NSMP) — and assigning them stage modifiers. The FIGO 2009 system remains the staging framework most undergraduate and postgraduate exams test, but every candidate must know that 2023 molecular classification now refines prognosis and treatment.[4][6]
Classification
Endometrial cancer is classified along three independent axes: histology (which sets prognosis and chemosensitivity), the Bokhman pathogenetic type (which sets biology and risk profile), and the molecular subtype (the modern TCGA classifier that increasingly drives adjuvant therapy). Each axis answers a different examiner question.[2][12]
Type I — endometrioid (80 per cent)
oestrogen-driven
- Endometrioid adenocarcinoma, FIGO grades 1 to 3; grade 1 well-differentiated, grade 3 poorly differentiated
- Driven by unopposed oestrogen; preceded by atypical endometrial hyperplasia (complex hyperplasia with atypia)
- Mutational profile: PTEN loss (40 to 80 per cent), PIK3CA (over 50 per cent), KRAS (15 to 30 per cent), ARID1A (over 30 per cent), CTNNB1 (beta-catenin), microsatellite instability (20 to 30 per cent)
- Affected women are typically obese, perimenopausal or postmenopausal, nulliparous, diabetic, with PCOS, on oestrogen-only HRT or tamoxifen
- Favourable prognosis: five-year survival 85 to 95 per cent in stage I
Type II — non-endometrioid (20 per cent)
TP53-driven, aggressive
- Uterine serous carcinoma (most common Type II), clear cell, carcinosarcoma (malignant mixed Mullerian tumour), undifferentiated and dedifferentiated carcinoma
- Not oestrogen-driven; arises in atrophic endometrium of older, thinner women
- Mutational profile: TP53 mutation (over 90 per cent of serous), HER2 amplification (30 per cent of serous), FBXW7, PPP2R1A, PIK3CA
- Often presents at advanced stage with deep myometrial invasion, lymphovascular space invasion, and extrauterine spread; serous may have intraperitoneal and omental disease resembling ovarian cancer
- Poor prognosis: five-year survival 40 to 60 per cent stage-for-stage
Endometrioid
the common histology
- Glands with variable atypia; graded 1 (well differentiated, under 5 per cent solid), 2 (moderately differentiated, 5 to 50 per cent solid), 3 (poorly differentiated, over 50 per cent solid)
- May show squamous differentiation (morules), mucinous change, or ciliated cells — does not change grade or prognosis
- Most are Type I and oestrogen-driven
Serous
aggressive papillary
- Papillary architecture with marked nuclear atypia and psammoma bodies; behaves like ovarian high-grade serous carcinoma
- Frequent TP53 mutation and HER2 amplification; high risk of nodal and intraperitoneal spread even with minimal myometrial invasion
- Requires carboplatin and paclitaxel chemotherapy, with trastuzumab if HER2-positive
Clear cell
rare and aggressive
- Hobnail and clear cells containing glycogen; ARID1A mutations common
- Poor prognosis even in stage I; treated like serous with adjuvant chemotherapy
Carcinosarcoma
mixed malignant Mullerian tumour
- Biphasic tumour: malignant epithelial (carcinomatous) plus malignant stromal (sarcomatous) components
- Now classified as a metaplastic carcinoma of epithelial origin; behaves aggressively
- Treated with staging surgery plus carboplatin and paclitaxel; ifosfamide-based regimens used historically
Mucinous and others
rare
- Mucinous: at least 50 per cent of cells contain intracytoplasmic mucin; usually low-grade endometrioid variant with excellent prognosis
- Squamous, transitional (Walthard), undifferentiated, and dedifferentiated (undifferentiated component alongside a low-grade endometrioid component) are very rare
Endometrial cancer — global burden and key numbers
Epidemiology & Risk Factors
Endometrial cancer is the commonest gynaecological cancer in developed countries and the second commonest globally (after cervical cancer, which dominates low-resource settings). Incidence rises steeply after the menopause, with peak age 60 to 70 years, and the median age at diagnosis is around 63. Around 4 per cent of cases occur before age 45, where the question of fertility-sparing management becomes central.[1][2]
The single unifying principle behind nearly every risk factor is unopposed oestrogen exposure of the endometrium. Oestrogen drives glandular proliferation; progesterone (produced by the corpus luteum after ovulation, or supplied exogenously) counterbalances this proliferation into a secretory pattern. Any state in which oestrogen is high and progesterone is relatively or absolutely low — obesity, nulliparity, anovulation, oestrogen-only HRT, an oestrogen-secreting tumour — leaves the endometrium under sustained mitogenic pressure, driving it through hyperplasia and atypia into carcinoma. The Type II tumours (serous, clear cell) are the exception: they are not oestrogen-driven, and they share only age as a risk factor.[2][5]
Risk factors and their approximate relative risks
The full risk factor list, grouped by mechanism, is:[2][14]
- States of unopposed oestrogen. Obesity (the dominant driver in developed countries, where adipose tissue aromatises androstenedione to oestrone), nulliparity and infertility (no protective progestational cycles), early menarche and late menopause (more lifetime oestrogen years), chronic anovulation and polycystic ovary syndrome (no corpus luteum, no progesterone), oestrogen-only hormone replacement therapy (oestrogen given without an opposing progestogen), oestrogen-secreting ovarian tumours (granulosa cell tumour, thecoma), and cirrhosis (impaired hepatic metabolism of oestrogens).
- Tamoxifen. Used as adjuvant therapy for oestrogen-receptor-positive breast cancer, tamoxifen is an antagonist at the breast but a partial agonist at the endometrium, roughly doubling the risk of endometrial cancer with five years of use; the tumours are predominantly low-grade endometrioid but may be high-grade. The benefit of tamoxifen in preventing breast cancer recurrence far outweighs the endometrial risk, but any vaginal bleeding on tamoxifen must be investigated.
- Genetic predisposition. Lynch syndrome (hereditary nonpolyposis colorectal cancer, HNPCC), caused by germline mutations in the MLH1, MSH2, MSH6, PMS2, or EPCAM mismatch repair genes, carries a 40 to 60 per cent lifetime risk of endometrial cancer (often higher than the colorectal cancer risk in women), typically diagnosed around age 50. Endometrial cancer is frequently the first (sentinel) cancer in women with Lynch syndrome. Cowden syndrome (PTEN mutation) carries a 20 to 30 per cent lifetime risk. BRCA1 mutations may modestly increase risk.
- Metabolic and lifestyle factors. Diabetes mellitus (insulin is a mitogen for the endometrium; risk roughly doubled), hypertension (often coexists with obesity and diabetes — the "corpus cancer syndrome" triad of obesity, diabetes, and hypertension described by Elwood), and physical inactivity (independent of obesity). [2]
United Kingdom and United States. Endometrial cancer is the commonest gynaecological malignancy and the fourth commonest cancer in women overall, with age-standardised incidence of 20 to 30 per 100,000 and rising at 1 to 2 per cent per year, driven by the obesity epidemic. The lifetime risk is approximately 3 per cent (1 in 30). Around 75 per cent of cases are diagnosed at stage I. Mortality is comparatively low because of early presentation.
[1]India and South Asia. The reported incidence is lower than in the West (age-standardised 5 to 10 per 100,000), partly because of lower obesity prevalence, higher parity, and shorter life expectancy in some regions, but the incidence is rising rapidly with urbanisation, increasing obesity, falling parity, and longer lifespan. Most Indian centres report stage I disease in 60 to 70 per cent at diagnosis. The Indian population also has a substantial burden of Lynch syndrome and a high prevalence of diabetes, both of which amplify risk. [1]
Sub-Saharan Africa and other low-resource settings. Endometrial cancer is far less common than cervical cancer in these regions, but under-diagnosis is likely; presentations are often late because healthcare access is limited and the symptom of postmenopausal bleeding is not widely recognised as a danger sign. [1]
Global trend. The worldwide burden is projected to rise by 50 to 100 per cent over the next two decades as obesity rises and populations age — the only major cancer whose incidence is increasing substantially in high-income countries.
Protective factors are the mirror image of the risk factors, all sharing the property of either lowering lifetime oestrogen exposure or supplying an opposing progestogen: combined oral contraceptive pill use (reduces risk by 30 to 50 per cent with five years of use, with protection lasting 30 years), multiparity and breastfeeding (progesterone-rich states), cigarette smoking (anti-oestrogenic, though the cardiovascular and oncological harms far outweigh this benefit), progestin-containing HRT or the levonorgestrel intrauterine system (opposes oestrogen), and physical activity and weight loss.[15]
Risk factors for Type I endometrial cancer
OBESE-PCOS
the dominant risk factor in developed countries — peripheral aromatisation of androgens to oestrone
the cardinal symptom; any postmenopausal bleeding demands investigation
the unifying mechanism — oestrogen-only HRT, anovulation, granulosa cell tumour
Lynch syndrome (40 to 60 per cent lifetime risk), Cowden (PTEN)
more cumulative lifetime oestrogen years
no protective progestational cycles
partial oestrogen agonist on endometrium, roughly doubles risk
polycystic ovary syndrome — chronic anovulation
the corpus cancer syndrome triad of obesity, diabetes, hypertension
Pathophysiology
The molecular pathology of endometrial cancer is one of the best characterised among solid tumours, thanks to the 2013 TCGA integrated genomic analysis by Kandoth and colleagues, which defined four molecular subgroups that now underpin the FIGO 2023 staging and the choice of adjuvant therapy.[12]
Type I — the oestrogen-driven, hyperplasia-to-carcinoma sequence
Type I tumours follow a recognisable, stepwise progression from normal endometrium through hyperplasia to carcinoma, mirroring the adenoma-carcinoma sequence of the colon. The driver is sustained oestrogen stimulation of the endometrium without the cyclic opposing effect of progesterone. The classical sequence is:[2][5]
- Normal cycling endometrium — oestrogen drives proliferation in the follicular phase, progesterone converts it to secretion in the luteal phase, and menstruation sheds the layer.
- Simple endometrial hyperplasia without atypia — glands increase in number and show cystic dilatation; risk of progression to cancer under 3 per cent. Managed with progestin or observation; reversible.
- Complex hyperplasia without atypia — glands crowd together with irregular outlines but no cytological atypia; progression risk 3 to 8 per cent.
- Atypical endometrial hyperplasia (complex hyperplasia with atypia, or endometrial intraepithelial neoplasia, EIN) — crowded glands with cytological atypia; 25 to 40 per cent have a coexistent endometrial carcinoma at hysterectomy, and progression risk if untreated is 25 to 50 per cent. This is the immediate cancer precursor and demands treatment — usually hysterectomy, or progestin for the fertility-sparing candidate.
- Well-differentiated endometrioid adenocarcinoma (FIGO grade 1) — glands with stromal invasion. [2]
The molecular events of this sequence were mapped by TCGA. The earliest and most common is loss of PTEN (the phosphatase that antagonises PI3K signalling, lost in 40 to 80 per cent of endometrioid cancers), followed by PIK3CA mutation (over 50 per cent, activating the same pathway), KRAS mutation (15 to 30 per cent, activating MAPK signalling), ARID1A mutation or loss (over 30 per cent, a chromatin-remodelling gene), CTNNB1 (beta-catenin) mutation (15 to 30 per cent), and microsatellite instability (20 to 30 per cent, from mismatch repair deficiency — sporadic MLH1 promoter methylation or germline Lynch syndrome). The PI3K-AKT-mTOR pathway is the dominant oncogenic driver and the target of modern drug development.[12]
Type II — TP53-driven, de novo aggressive carcinomas
Type II tumours do not follow the hyperplasia sequence. They arise de novo in atrophic endometrium, often from a precursor called endometrial glandular dysplasia or, for serous tumours, from endometrial intraepithelial carcinoma — a non-invasive lesion that already carries the full TP53 mutation and can spread transcoelomically like ovarian high-grade serous carcinoma. The defining molecular event is TP53 mutation, present in over 90 per cent of serous carcinomas, which produces aberrant p53 protein that accumulates in the nucleus (diffuse strong immunohistochemical staining) or, less commonly, is completely absent (null pattern) — both patterns indicate loss of the DNA-damage checkpoint.[2][16]
HER2 (ERBB2) amplification occurs in about 30 per cent of uterine serous carcinomas and is the target of trastuzumab added to carboplatin-paclitaxel chemotherapy. PIK3CA mutations also occur in Type II tumours. Carcinosarcomas carry mutations in both epithelial and stromal components, with TP53 and PIK3CA predominating; they are now understood to be metaplastic carcinomas rather than true mixed tumours.[2]
The four TCGA molecular subgroups and ProMisE classification
The 2013 TCGA analysis divided endometrial carcinoma into four molecular subgroups, and the ProMisE (Proactive Molecular Risk Classifier for Endometrial Cancer) algorithm operationalised this into a clinically usable classifier using immunohistochemistry for mismatch repair proteins and p53, plus POLE sequencing. These four subgroups now appear as stage modifiers in the FIGO 2023 staging system.[4][12][13]
POLE-ultramutated
excellent prognosis
- Catalytic (exonuclease) domain mutation of POLE (the leading-strand DNA polymerase), causing an ultramutated phenotype (over 100 mutations per megabase)
- About 7 per cent of all endometrioid cancers, mostly grade 3, in younger women
- Excellent prognosis even in high-grade or advanced-stage disease; adjuvant therapy may be de-escalated
- Stage IA-IB POLE-mutant tumours are down-staged in FIGO 2023
Mismatch repair deficient (MMRd)
intermediate, often Lynch
- Loss of MLH1, MSH2, MSH6, or PMS2 by immunohistochemistry; high microsatellite instability and high mutational burden
- About 25 to 30 per cent; sporadic (MLH1 promoter methylation) in most, germline Lynch syndrome in 10 to 20 per cent
- Intermediate prognosis; enriched for lymphovascular invasion and nodal disease
- Candidates for immune checkpoint inhibitor therapy (pembrolizumab, dostarlimab) — MSI-H tumours respond well
p53-abnormal (copy-number high)
poor prognosis, mostly Type II
- Abnormal p53 immunohistochemistry (diffuse strong or completely null) or TP53 mutation; high copy-number alterations, low mutation burden
- About 25 per cent; enriched for serous, clear cell, and high-grade endometrioid histologies; most Type II tumours
- Highest recurrence and mortality; benefits most from adjuvant chemotherapy (PORTEC-3)
- Stage I p53-abnormal tumours with myometrial invasion are up-staged in FIGO 2023
p53-wildtype / NSMP
intermediate, often Type I
- No specific molecular profile: intact mismatch repair, normal p53, no POLE mutation — a diagnosis of exclusion
- About 40 per cent; mostly low-grade endometrioid in obese women
- Intermediate prognosis; risk driven by traditional factors (grade, depth of invasion, age)
- Standard risk-stratified adjuvant therapy
The clinical relevance of molecular classification is now substantial: POLE-mutant tumours may avoid adjuvant therapy even when high-grade; p53-abnormal tumours benefit from chemotherapy (PORTEC-3 showed chemoradiotherapy improved survival in this subgroup); and MMRd tumours are candidates for immunotherapy and trigger universal Lynch syndrome screening.[13]
Pattern of spread
Endometrial cancer spreads by direct extension (into the myometrium, then the cervix, then beyond the uterus into parametrium, bladder, and rectum), lymphatic spread (to pelvic nodes — obturator, internal and external iliac — then para-aortic nodes, with risk proportional to depth of myometrial invasion and grade), transcoelomic (intraperitoneal spread, particularly characteristic of serous carcinoma, producing omental disease and ascites resembling ovarian cancer), and, late, haematogenous to lung, liver, and bone. Lymphovascular space invasion is an independent prognostic factor for nodal and distant recurrence.[2]
Clinical Presentation
Endometrial cancer is the paradigm of a cancer whose biology saves lives by announcing itself early. Because the tumour lines the uterine cavity, even a small lesion bleeds, and bleeding prompts the patient to seek care.[2]
[2] [3]The symptoms and signs by stage are:[2]
- Early disease (stage I) — the common presentation. Postmenopausal bleeding (90 per cent), typically a single episode of bright or dark red spotting or heavier bleeding, often painless. Perimenopausal or reproductive-age women present with heavy, prolonged, irregular, or intermenstrual bleeding rather than clear-cut postmenopausal bleeding. Postcoital bleeding and a watery, serous, or blood-stained vaginal discharge may precede frank bleeding.
- Locally advanced disease (stage II to III). Invasion of the cervix produces a bloody or purulent discharge and dyspareunia; parametrial extension produces pelvic pressure or pain; a large uterus may cause urinary frequency or a palpable abdominal mass.
- Advanced disease (stage IV). Weight loss, anorexia, fatigue, anaemia of chronic disease; bowel or bladder symptoms from invasion (haematuria, pneumaturia, rectal bleeding, fistula); lower limb lymphoedema from lymphatic or venous obstruction; ascites and pleural effusion in serous carcinoma with transcoelomic spread. [2]
Atypical presentations examiners test deliberately.[2]
- The young obese woman with polycystic ovary syndrome presenting with chronic anovulatory bleeding may be labelled as having dysfunctional bleeding and managed with the oral contraceptive pill without biopsy — a missed endometrial cancer. Any woman under 45 with persistent abnormal bleeding plus risk factors (obesity, PCOS, nulliparity) should have endometrial sampling.
- The woman on tamoxifen who develops any vaginal bleeding must be investigated — tamoxifen doubles the endometrial cancer risk and the bleeding is not "expected".
- The thin elderly woman with uterine serous carcinoma may present with a small primary tumour but extensive intraperitoneal disease, ascites, and omental involvement, mimicking ovarian cancer.
- The asymptomatic woman in whom a thickened endometrium is found incidentally on ultrasound performed for another reason (ovarian cyst, fibroids) — the thickness threshold for investigation still applies.
- The woman with Lynch syndrome should be under surveillance and may be diagnosed with endometrial cancer as her first (sentinel) malignancy, often before age 50. [2]
Differential Diagnosis
The differential of postmenopausal bleeding splits into benign endometrial and cervical-vaginal causes, other gynaecological cancers, and systemic causes. The history, speculum and bimanual examination, transvaginal ultrasound, and endometrial biopsy separate them.[2]
| Condition | Distinguishing features |
|---|---|
| Atrophic vaginitis and endometrial atrophy | The commonest benign cause (60 to 80 per cent of PMB). Thin, pale, dry vagina on speculum; atrophic, fragile epithelium bleeds on contact. Endometrium thin (under 4 mm) on TVUS; biopsy if not on HRT shows atrophic glands without atypia. Treated with topical oestrogen. |
| Endometrial hyperplasia with or without atypia | Heavy or irregular bleeding; thickened endometrium on TVUS; biopsy confirms hyperplasia. Atypical hyperplasia is the immediate precursor and is treated as for cancer. |
| Endometrial polyp | A focal echogenic mass within the cavity on TVUS, best seen on saline infusion sonohysterography; hysteroscopic polypectomy is diagnostic and therapeutic. Most are benign but a small proportion harbour carcinoma. |
| Cervical cancer | Postcoital, intermenstrual, or postmenopausal bleeding; visible lesion on speculum; abnormal cervical screening test; biopsy of the cervix (not the endometrium) confirms. |
| Submucosal fibroid | Heavy menstrual or intermenstrual bleeding; visible as a hypoechoic submucosal mass on TVUS; hysteroscopic myomectomy is diagnostic and therapeutic. |
| Hormone replacement therapy-related bleeding | Unscheduled bleeding in a woman on sequential or continuous combined HRT; investigation is still required to exclude cancer. |
| Oestrogen-secreting ovarian tumour | Granulosa cell tumour or thecoma in a postmenopausal woman produces oestrogen that stimulates the endometrium; presents with PMB and an adnexal mass. |
| Vaginal cancer | Rare; postmenopausal or postcoital bleeding; visible lesion in the vagina; biopsy confirms. |
| Coagulopathy or anticoagulant therapy | Rare cause of PMB; systemic bleeding history; abnormal coagulation studies. |
In the reproductive-age woman the differential of heavy or irregular bleeding includes anovulatory cycles (especially PCOS), pregnancy-related bleeding (miscarriage, ectopic, retained products), adenomyosis, fibroids, pelvic inflammatory disease, and thyroid dysfunction — but endometrial cancer must be considered and biopsied in any woman over 45 with abnormal bleeding, or younger with risk factors.[2]
Clinical & Bedside Assessment
The focused assessment of a woman with postmenopausal bleeding has two purposes: to characterise the bleeding and exclude local causes, and to identify risk factors and comorbidities that shape both investigation and treatment.[3]
History. Establish that the bleeding is genuinely postmenopausal — the date of the last menstrual period, any HRT (type, regimen, adherence), and the pattern of bleeding (number of episodes, amount, colour, relation to intercourse, associated discharge or pain). Take a full gynaecological and obstetric history (parity, infertility, previous cervical screening, previous hyperplasia or polyps, age at menarche and menopause). Screen systematically for risk factors: obesity (BMI), diabetes, hypertension, tamoxifen (and the breast cancer it was given for), oestrogen-only HRT, polycystic ovary syndrome, nulliparity, and a family history of Lynch-associated cancers (colorectal, endometrial, ovarian, gastric, urothelial) at a young age. Ask about systemic symptoms suggesting advanced disease — weight loss, fatigue, bowel or bladder symptoms, bone pain. Always ask about current medications (especially anticoagulants, which can cause bleeding).[3]
Examination. BMI (obesity is the dominant risk factor and shapes the surgical approach), blood pressure (hypertension), and general inspection for signs of anaemia or cachexia. Abdominal examination for masses, hepatomegaly, or ascites (advanced serous carcinoma). Speculum examination to inspect the cervix and vagina — exclude cervical cancer, polyps, vaginitis, or vaginal atrophy as the source of bleeding, and take a cervical screening test if due. Bimanual pelvic examination to assess uterine size, mobility, and tenderness, adnexal masses, and parametrial thickening or nodularity (advanced disease). Examine for metastatic disease if locally advanced — supraclavicular lymphadenopathy, pleural effusion, lower limb lymphoedema.[3]
Investigations
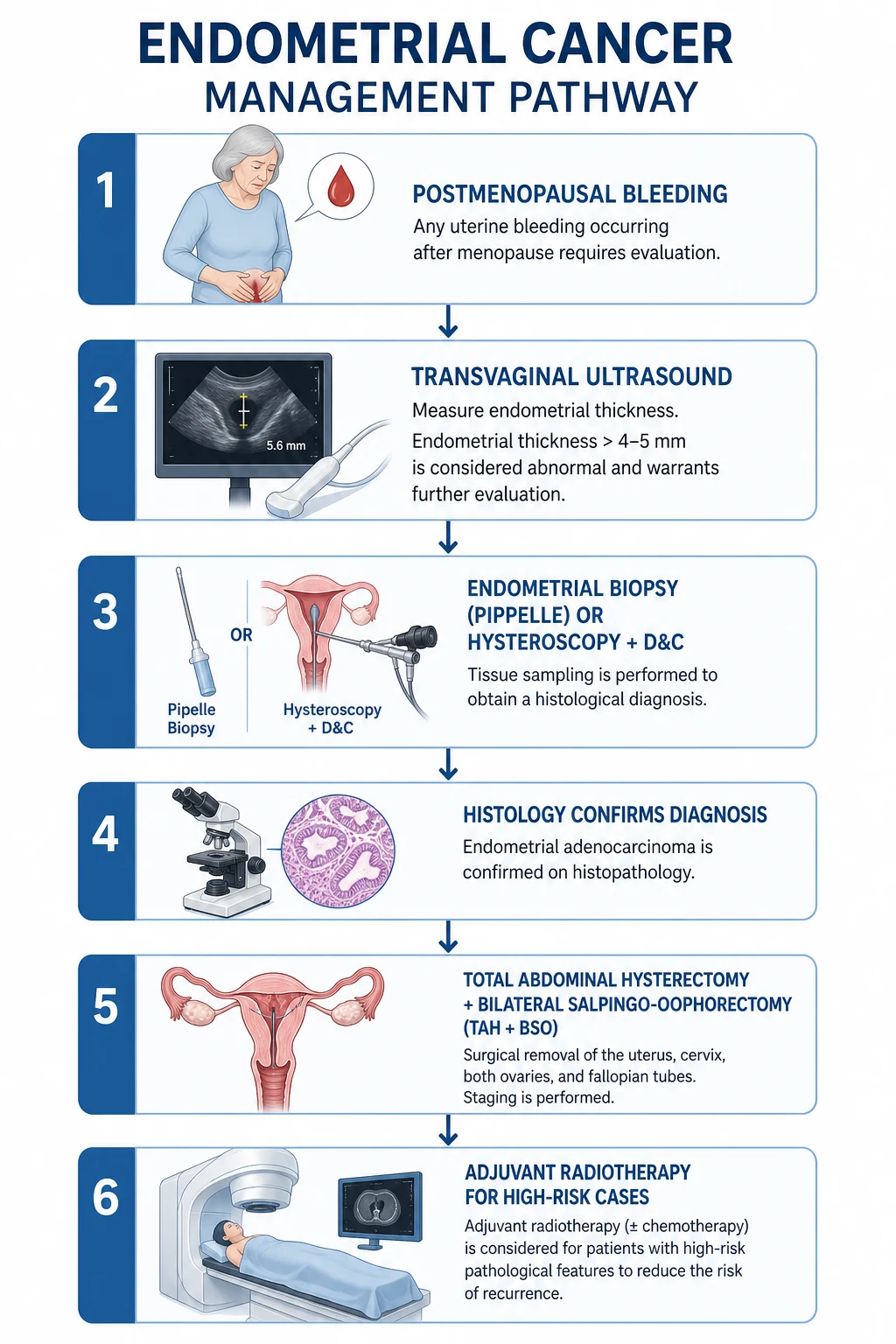
The investigation pathway is a two-step diagnostic cascade: a first-line triage of all women with postmenopausal bleeding (transvaginal ultrasound plus endometrial sampling), followed by staging of confirmed cancers (pelvic MRI, with chest-abdomen-pelvis CT or PET-CT for high-risk histology).[3]
Step 1 — Confirm the diagnosis
Transvaginal ultrasound (TVUS) is the first-line investigation in any woman with postmenopausal bleeding.[3]
- The single most important measurement is endometrial thickness (double-layer). In a postmenopausal woman not on HRT, an endometrial thickness of 4 mm or more has a sensitivity of over 95 per cent and a negative predictive value of over 95 per cent for endometrial cancer — the threshold below which cancer is sufficiently unlikely that biopsy may be omitted in a woman without other risk factors.
- Most units use a 4 to 5 mm threshold: at 5 mm, the risk of cancer in a woman with PMB is about 7 per cent; below 4 mm it is under 1 per cent. Women on continuous combined HRT use the same 4 to 5 mm threshold; women on sequential (cyclic) HRT are scanned at the end of the progestin phase, when the endometrium should be thinnest.
- Tamoxifen thickens the endometrium by subendometrial cystic atrophy, reducing the specificity of TVUS — biopsy is recommended for any bleeding in a tamoxifen user regardless of thickness.
- In a perimenopausal or reproductive-age woman, the threshold approach does not apply (the endometrium cycles normally); persistent abnormal bleeding plus risk factors mandates biopsy. [3]
Endometrial biopsy (pipelle) is performed in the outpatient clinic and is the standard method of obtaining histology.[3]
- The pipelle device is a thin plastic suction cannula that samples 10 to 25 per cent of the endometrial surface. Sensitivity for endometrial cancer is 90 per cent or more for global disease but only 60 to 80 per cent for focal lesions (polyps, focal carcinoma), where it may miss the lesion.
- It is well tolerated, requires no anaesthesia, and can be performed at the same visit as TVUS. The histology confirms hyperplasia versus carcinoma, distinguishes endometrioid from serous or clear cell, and assigns grade. [3]
Hysteroscopy with directed biopsy and dilation and curettage (D and C) is the gold standard for diagnosis.[3]
- Hysteroscopy allows direct visualisation of the uterine cavity, identification of focal lesions (polyps, submucosal fibroids, focal carcinoma) that pipelle may miss, and targeted biopsy or polypectomy.
- Performed under local anaesthesia in the outpatient setting or under general anaesthesia. Indications: a non-diagnostic or inadequate pipelle, persistent bleeding with negative pipelle, a focal lesion on imaging, or a high clinical suspicion despite negative biopsy.
- The combination of hysteroscopy plus dilation and curettage is the most sensitive technique for endometrial cancer (over 95 per cent) but is more invasive and expensive than pipelle; it is reserved for cases where pipelle is inconclusive. [3]
Saline infusion sonohysterography is a useful adjunct when TVUS shows a thickened endometrium and the question is whether the abnormality is diffuse (hyperplasia) or focal (polyp).[3]
Histopathology of the biopsy confirms the diagnosis and provides the key information that drives staging and treatment: histotype (endometrioid versus serous, clear cell, carcinosarcoma), grade (FIGO 1 to 3), oestrogen and progesterone receptor status, and (on the hysterectomy specimen) depth of myometrial invasion, cervical stromal involvement, lymphovascular space invasion, and nodal status.[2]
Step 2 — Stage the disease
Pelvic MRI is the imaging test of choice for local staging.[3]
- The key questions MRI answers are depth of myometrial invasion (under 50 per cent — inner half — versus 50 per cent or more — outer half), cervical stromal involvement, extrauterine extension (parametrium, bladder, rectum), and pelvic and para-aortic nodal enlargement.
- Depth of invasion is the principal determinant of nodal metastasis risk (under 5 per cent for grade 1 inner-half invasion, rising to over 40 per cent for grade 3 outer-half invasion) and of the decision to perform lymph node dissection.
- MRI is most useful for high-grade histologies (serous, clear cell, grade 3 endometrioid), suspected deep invasion, or when fertility-sparing management is being considered. [3]
CT chest, abdomen, and pelvis screens for distant metastases and is indicated for high-risk histologies (serous, clear cell, carcinosarcoma), suspected advanced disease, or where MRI suggests nodal or extrauterine spread.[3]
18F-FDG PET-CT is increasingly used for high-grade or advanced disease and for detection of nodal and distant disease that influences management; it is the most sensitive modality for nodal metastases.[3]
Serum CA-125 is elevated in advanced disease, particularly serous carcinoma with intraperitoneal spread; it is useful as a baseline and for monitoring response in advanced disease, but it is not a screening test.[2]
Other bloods. Full blood count (anaemia from chronic bleeding), urea and electrolytes and creatinine, liver function tests, and coagulation screen if anticoagulated. A glucose and HbA1c in obese or diabetic women, given the metabolic syndrome association.[3]
Step 3 — Universal Lynch syndrome screening
All women diagnosed with endometrial cancer should undergo universal screening for Lynch syndrome by immunohistochemistry for the four mismatch repair proteins (MLH1, MSH2, MSH6, PMS2) on the tumour specimen.[3][13]
- Loss of one or more MMR proteins triggers reflex testing: if MLH1 is lost, MLH1 promoter methylation testing distinguishes sporadic (methylation-positive, the commonest) from germline Lynch (methylation-negative). If MLH1 is intact but another protein is lost (or any loss without MLH1 methylation), proceed to germline genetic testing.
- Universal screening identifies the 3 to 5 per cent of endometrial cancers that are Lynch-associated, enables cascade testing of relatives, and identifies women at high risk of subsequent colorectal, ovarian, and other Lynch cancers for surveillance.
- MMR-deficient tumours are also candidates for immunotherapy (pembrolizumab, dostarlimab) in advanced disease, and the MMRd status refines the molecular classification used in FIGO 2023 staging.[13]
Management — Resuscitation
Endometrial cancer rarely presents as a true emergency, because the dominant symptom — postmenopausal bleeding — is typically light and intermittent. Two scenarios, however, demand immediate action.[3]
Severe or torrential vaginal bleeding from an advanced, necrotic tumour is uncommon but can cause haemodynamic compromise. Management follows the standard trauma resuscitation principles: secure two large-bore intravenous cannulae, send blood for full blood count, group and cross-match, and coagulation; resuscitate with intravenous crystalloid and transfuse packed red cells for haemodynamic instability or symptomatic anaemia. Tranexamic acid 1 g intravenously every 8 hours reduces fibrinolysis (use cautiously — it is pro-thrombotic in a cancer patient). High-dose progestin (medroxyprogesterone acetate 200 to 400 mg orally daily, or megestrol acetate 160 to 320 mg orally daily) can slow bleeding over 1 to 2 weeks by suppressing the oestrogen-driven tumour. Vaginal packing with a tranexamic-acid- or Monsel's-solution-soaked pack tamponades bleeding. Definitive haemostasis in advanced, unresectable disease is achieved with palliative radiotherapy (highly effective) or uterine artery embolisation.[3]
Symptomatic anaemia from chronic blood loss is the commonest preoperative issue — transfuse to a haemoglobin over 80 g/L (or over 100 g/L in symptomatic cardiovascular disease) before surgery, and correct iron deficiency with intravenous iron where appropriate.[3]
Obstructive uropathy or bowel obstruction from advanced disease is managed with nephrostomy or ureteric stent (relieving uraemia and hyperkalaemia) and conservative or surgical management of obstruction, respectively, before definitive oncological treatment. [3]
Management — Definitive & Stepwise
Surgery — the cornerstone
Total hysterectomy with bilateral salpingo-oophorectomy is the cornerstone of treatment for endometrial cancer, providing cure for most stage I disease and defining stage for all.[3]
- Surgical approach. The laparoscopic or robotic approach is preferred over open laparotomy for apparent stage I disease — it gives shorter hospital stay, less blood loss, fewer wound complications, and equivalent oncological outcomes. Vaginal hysterectomy is an option in selected women (prolapse, significant obesity, comorbidities). Laparotomy is reserved for large uteri, advanced disease, or when minimally invasive access is not feasible.
- Bilateral salpingo-oophorectomy is performed because the ovaries are a site of metastasis (5 to 10 per cent) and synchronous ovarian cancer (2 to 5 per cent), and because oestrogen produced by the ovaries could drive any residual disease. In a premenopausal woman with a clearly low-grade, early-stage tumour, ovarian conservation may be discussed to avoid surgically induced menopause, but the standard is bilateral removal.
- Peritoneal washings are taken on opening the abdomen for cytology (positive washings up-stage the disease in some systems). [3]
Lymph node assessment is the most debated component of staging surgery.[3][11]
- Systematic pelvic and para-aortic lymphadenectomy removes the obturator, external iliac, internal iliac, and common iliac (and para-aortic) nodal chains. Two large randomised trials (the Mayo-led systematic lymphadenectomy trials) showed that routine complete lymphadenectomy does not improve survival in women with low-risk disease and adds morbidity (lymphoedema, lymphocyst, nerve injury, longer operating time). It is therefore reserved for women at intermediate or high risk of nodal metastasis — typically those with grade 3 endometrioid, deep (50 per cent or more) myometrial invasion, serous or clear cell histology, or suspected nodes on imaging.
- Sentinel lymph node biopsy has emerged as the standard alternative to full lymphadenectomy for apparent early-stage disease. The FIRES trial (Rossi and colleagues) showed that sentinel node biopsy with fluorescent indocyanine green and cervical injection detected nodal metastases with high sensitivity and negative predictive value, with far less morbidity than full dissection. It is now the recommended approach for surgical staging of intermediate-risk disease at most centres.[11]
Dose
Risk stratification and adjuvant therapy
After surgery, women are stratified into risk groups that determine the need for adjuvant radiotherapy, chemotherapy, or both. The widely used ESGO/ESTRO/ESP and the PORTEC trial framework define these groups.[3][7][8][9][10]
Low risk
stage IA grade 1 to 2
- Stage IA, endometrioid grade 1 to 2, under 50 per cent myometrial invasion, no lymphovascular space invasion
- Five-year recurrence risk under 5 per cent
- **No adjuvant therapy** — surgery alone is curative; observation
Intermediate risk
PORTEC criteria
- Stage IA grade 3, or stage IB grade 1 to 2 (over 50 per cent invasion)
- PORTEC-1 high-intermediate risk: age over 60 plus two of grade 3, outer-half invasion, or lymphovascular space invasion
- **Vaginal vault brachytherapy** is the adjuvant therapy of choice (PORTEC-2 showed it is non-inferior to external beam radiotherapy for vaginal recurrence, with far fewer gastrointestinal and toxicity side-effects)
- External beam pelvic radiotherapy if additional risk factors
High-intermediate risk
GOG 99 / PORTEC HIR
- Combination of older age, grade 2 to 3, outer-half myometrial invasion, lymphovascular space invasion
- **Vaginal brachytherapy plus or minus pelvic external beam radiotherapy**
- PORTEC-2 established brachytherapy alone as sufficient for most
High risk
stage II, III, or aggressive histology
- Stage II (cervical stromal involvement), stage III (serosa, adnexa, vagina, nodes), serous or clear cell histology, carcinosarcoma, or grade 3 with deep invasion
- **Pelvic external beam radiotherapy plus chemotherapy with carboplatin and paclitaxel** (PORTEC-3 showed chemoradiotherapy improved failure-free and overall survival compared with radiotherapy alone in high-risk disease)
- Vaginal brachytherapy boost as indicated
Advanced and metastatic
stage IVB
- Distant metastases or unresectable disease
- **Systemic chemotherapy** (carboplatin and paclitaxel) plus or minus **hormonal therapy** (progestin, aromatase inhibitor) for low-grade oestrogen-receptor-positive disease
- Immunotherapy for MMRd tumours (pembrolizumab, dostarlimab); trastuzumab for HER2-positive serous carcinoma
Adjuvant radiotherapy
Vaginal vault brachytherapy delivers a high radiation dose to the vaginal vault (the commonest site of recurrence) with rapid fall-off, sparing the bladder and rectum. It is the adjuvant therapy of choice for intermediate-risk disease following the PORTEC-2 trial, which showed equivalent vaginal recurrence control to external beam radiotherapy with significantly fewer gastrointestinal and quality-of-life side-effects. The standard regimen delivers 21 Gy in 3 fractions (high-dose-rate) or 30 Gy in 5 fractions to the vaginal surface.[9]
External beam pelvic radiotherapy delivers 45 to 50 Gy in 25 to 28 fractions to the pelvis, treating the vaginal vault, parametrium, and pelvic nodes. It is used for high-intermediate and high-risk disease, often combined with vaginal brachytherapy boost. Acute side-effects include diarrhoea, cystitis, fatigue, and skin reaction; late effects include vaginal stenosis, radiation enteritis, cystitis, lymphoedema, and a small second-malignancy risk.[3]
Adjuvant and palliative chemotherapy
Carboplatin and paclitaxel is the standard chemotherapy regimen for high-risk, advanced, and recurrent endometrial cancer.[3][10]
Dose
The PORTEC-3 trial established that adjuvant chemoradiotherapy (two cycles of cisplatin concurrent with radiotherapy, then four cycles of carboplatin and paclitaxel) improved failure-free and overall survival compared with radiotherapy alone in high-risk endometrial cancer, particularly in stage III and serous histology. This is now the standard for high-risk disease.[10]
HER2-targeted therapy. For HER2-positive uterine serous carcinoma, the Fader 2018 randomised phase II trial showed that adding trastuzumab to carboplatin and paclitaxel improved progression-free survival.[18]
Hormonal therapy
High-dose progestin is the treatment of choice for fertility-sparing management of selected young women with grade 1, stage IA endometrioid endometrial cancer confined to the endometrium, who wish to preserve fertility.[3][19]
Dose
Hormonal therapy for advanced or recurrent disease. For low-grade, oestrogen-receptor-positive tumours, progestins (medroxyprogesterone, megestrol), aromatase inhibitors (letrozole, anastrozole), and tamoxifen have response rates of 15 to 30 per cent with low toxicity, and are particularly useful in slow-growing recurrent endometrioid cancer.[3]
Immunotherapy
For mismatch repair deficient or microsatellite instability-high (MSI-H) tumours, immune checkpoint inhibitors (pembrolizumab, dostarlimab) produce durable responses. Pembrolizumab plus lenvatinib (a multitargeted tyrosine kinase inhibitor) is approved for advanced or recurrent endometrial cancer that is not MSI-H, based on the KEYNOTE-775 trial. These agents have transformed the management of advanced disease.[13]
FIGO Staging — 2009 and 2023
The FIGO 2009 staging system (the Creasman revision) is the framework most undergraduate exams test, but the FIGO 2023 revision (the Berek revision) layered molecular classification on top. Every candidate must know both.[6][4]
[6]Key features of FIGO 2009. Stage I is confined to the uterus, divided by depth of myometrial invasion (IA under half, IB half or more). Stage II is cervical stromal involvement without extrauterine spread. Stage III is local or regional spread (serosa or adnexa — IIIA; vagina or parametrium — IIIB; pelvic nodes — IIIC1; para-aortic nodes — IIIC2). Stage IV is bladder or bowel mucosa (IVA) or distant metastases (IVB). Stage I is surgical-pathological; stages II to IV combine surgical, pathological, and radiological findings.[6]
FIGO 2023 revision. The Berek revision layered the four TCGA molecular subgroups onto the anatomic stage. POLE-mutant stage IA to IB tumours are down-staged (because of excellent prognosis). p53-abnormal stage IA tumours with any myometrial invasion are up-staged. MMRd and aggressive histologies carry their own modifiers. The anatomic framework remains the 2009 structure, but molecular classification now refines both prognosis and adjuvant therapy decisions.[4][13]
Stage-specific management — endometrial cancer
Specific Subtypes & Scenarios
Uterine serous carcinoma
Uterine serous carcinoma accounts for 5 to 10 per cent of endometrial cancers but a disproportionate share of deaths. It is the prototypical Type II tumour — TP53 mutation, HER2 amplification in 30 per cent, aggressive behaviour with intraperitoneal spread resembling ovarian high-grade serous carcinoma. Even small, apparently early-stage tumours carry a high risk of nodal and intraperitoneal disease, so surgical staging includes omentectomy and peritoneal biopsies in addition to standard surgery. Adjuvant carboplatin and paclitaxel is given for all stages, with trastuzumab added for HER2-positive disease (the Fader 2018 randomised phase II trial showed improved progression-free survival).[18]
Clear cell carcinoma
Clear cell carcinoma of the endometrium is rare (under 5 per cent), histologically similar to its ovarian counterpart, and carries a poor prognosis even in stage I. ARID1A mutations are common. Management parallels serous carcinoma — full surgical staging with omentectomy, and adjuvant carboplatin and paclitaxel for high-risk disease.[2]
Carcinosarcoma (malignant mixed Mullerian tumour)
Carcinosarcoma is a biphasic tumour with malignant epithelial and stromal components, now understood to be a metaplastic carcinoma of epithelial origin. It behaves aggressively, metastasises early, and is treated with staging surgery plus carboplatin and paclitaxel (or historical ifosfamide-based regimens).[2]
Atypical endometrial hyperplasia
Atypical endometrial hyperplasia (complex hyperplasia with atypia, or endometrial intraepithelial neoplasia) is the immediate precursor of Type I endometrial cancer. The critical fact for the exam is that 25 to 40 per cent of women with atypical hyperplasia on biopsy have a coexistent endometrial carcinoma at hysterectomy — therefore a diagnosis of atypical hyperplasia warrants definitive management. Hysterectomy is the standard treatment in women who have completed childbearing. High-dose progestin (oral medroxyprogesterone, megestrol, or the levonorgestrel intrauterine system) is used for the fertility-sparing candidate, with close endometrial surveillance sampling every 3 months — response rates are 60 to 75 per cent but recurrence is common.[17][19]
Fertility-sparing management of grade 1 endometrial cancer
Selected young women with grade 1 endometrioid endometrial cancer confined to the endometrium (stage IA, no myometrial invasion on MRI), with no lymphovascular space invasion, who strongly wish to preserve fertility, may be managed with high-dose oral progestin (medroxyprogesterone 400 to 600 mg daily, or megestrol 160 to 320 mg daily) or the levonorgestrel intrauterine system, with endometrial sampling every 3 months to assess response. Definitive hysterectomy is recommended once childbearing is complete because the recurrence rate after regression is 25 to 40 per cent. This must be a multidisciplinary team decision with careful counselling.[19]
Endometrial cancer and tamoxifen
Women on tamoxifen for oestrogen-receptor-positive breast cancer have approximately a 2 to 3 times increased risk of endometrial cancer, predominantly low-grade endometrioid but occasionally high-grade. The benefit of tamoxifen in preventing breast cancer recurrence outweighs this risk, and routine screening (ultrasound or biopsy) of asymptomatic women on tamoxifen is not recommended — but any vaginal bleeding on tamoxifen must be investigated with TVUS and endometrial biopsy.[2]
Lynch syndrome and endometrial cancer
Endometrial cancer is frequently the sentinel (first diagnosed) cancer in women with Lynch syndrome, often presenting in the perimenopausal years. Management of the cancer itself is standard, but the diagnosis of Lynch syndrome triggers cascade genetic testing of relatives and a structured surveillance programme: annual or biennial colonoscopy (for colorectal cancer, the dominant Lynch risk), and consideration of risk-reducing total hysterectomy and bilateral salpingo-oophorectomy once childbearing is complete (typically around age 40 to 45, individualised).[3][13]
Endometrial cancer in pregnancy
Endometrial cancer in pregnancy is extremely rare, because the high progesterone state of pregnancy is protective against oestrogen-driven tumours. When it does occur, management is multidisciplinary and individualised; small, low-grade tumours may be managed conservatively until delivery, with definitive surgery postpartum.[2]
Complications & Pitfalls
Complications fall into disease-related, treatment-related, and psychosocial groups.[3]
Disease complications are the consequences of local invasion and metastasis: vaginal vault recurrence (the commonest site, prevented by brachytherapy), pelvic sidewall and nodal recurrence, distant metastases to lung, liver, and bone, bowel or bladder invasion producing fistula or obstruction, lower limb lymphoedema from lymphatic or venous compression, and severe anaemia from chronic tumour bleeding. [3]
Surgical complications of hysterectomy and lymphadenectomy include bleeding, infection, visceral injury (bladder, ureter, bowel), vault dehiscence, deep vein thrombosis and pulmonary embolism (cancer is prothrombotic; prophylaxis with low molecular weight heparin and sequential compression devices is mandatory), and lymphoedema after full lymphadenectomy (the principal morbidity, in 5 to 25 per cent — much reduced with sentinel node biopsy).[11]
Radiotherapy complications are divided into acute and late. Acute effects include diarrhoea, radiation cystitis, skin desquamation, and bone marrow suppression. Late effects include vaginal stenosis and atrophy (the principal late effect, mitigated by vaginal dilator use), radiation enteritis with stricture, fistula or chronic diarrhoea, radiation cystitis with haematuria, lymphoedema, ovarian failure if ovaries are in field (avoided by bilateral oophorectomy at surgery anyway), and a small second malignancy risk decades later.[3]
Chemotherapy complications of carboplatin and paclitaxel include myelosuppression (thrombocytopenia, neutropenia), peripheral neuropathy (paclitaxel — often persistent), hypersensitivity reactions, alopecia, fatigue, nausea, and nephrotoxicity.[10]
Psychosocial complications include the impact of surgically induced menopause (hot flushes, bone loss, sexual dysfunction), body image disturbance, anxiety about recurrence, and the burden of surveillance. [3]
Classic pitfalls. Dismissing perimenopausal bleeding as dysfunctional or attributing it to the oral contraceptive pill without biopsy; relying on a single pipelle for a focal lesion (a polyp harbouring cancer may be missed); failing to investigate any bleeding on tamoxifen; under-treating uterine serous carcinoma as if it were a low-grade endometrioid tumour (serous requires chemotherapy even in stage I); and forgetting to screen for Lynch syndrome in every newly diagnosed case.[2][3]
Prognosis & Disposition
Prognosis is driven above all by stage, then by histology and grade, depth of myometrial invasion, lymphovascular space invasion, nodal status, age, and molecular subgroup. The overall five-year survival for all stages combined is approximately 80 per cent, reflecting the predominance of early-stage Type I disease. Endometrial cancer has the most favourable survival of all gynaecological malignancies, largely because of its early presentation with bleeding.[2][3]
Five-year survival by FIGO stage
Molecular subgroup prognosis. POLE-mutant tumours have the best prognosis (five-year disease-specific survival over 95 per cent even in high-grade disease); p53-abnormal tumours have the worst (recurrence rate 30 to 50 per cent); MMRd and NSMP are intermediate. These prognoses now drive adjuvant therapy de-escalation (POLE) and escalation (p53-abnormal) decisions.[13]
Disposition. A woman with early-stage disease treated surgically is followed up with clinical examination and (for high-risk disease) vault cytology or imaging at 3 to 6 monthly intervals for two to five years, then annually — though evidence for intensive surveillance is limited, and most recurrences are detected by symptoms rather than routine testing. Recurrence is treated with surgery (if isolated and resectable), radiotherapy (if not previously irradiated), hormonal therapy (for low-grade ER-positive recurrence), or chemotherapy — and immunotherapy for MMRd tumours. All patients merit early psychosocial and sexual-health support, and younger women need explicit discussion of fertility and early menopause before treatment.[3]
Special Populations
Young women (under 45) wishing to preserve fertility. For grade 1 endometrioid cancer confined to the endometrium on MRI, with no lymphovascular space invasion and MMR-proficient status, high-dose oral progestin or the levonorgestrel intrauterine system with strict 3-monthly sampling is the fertility-sparing option. Response rates are 60 to 75 per cent; recurrence is 25 to 40 per cent after regression. Definitive hysterectomy is recommended once childbearing is complete.[19]
Women with Lynch syndrome. Endometrial cancer is frequently the sentinel cancer; management of the cancer itself is standard, but the diagnosis triggers cascade testing of relatives, intensive colonoscopic surveillance, and consideration of risk-reducing total hysterectomy and bilateral salpingo-oophorectomy once childbearing is complete (around age 40 to 45).[3]
Obese women. Obesity makes surgery technically more challenging (higher conversion rate from laparoscopic to open, longer operating time, higher wound complication rate) and amplifies anaesthetic risk (sleep apnoea, difficult airway, venous thromboembolism). Laparoscopic and robotic approaches are particularly valuable in obese women. Bariatric surgery before or after cancer treatment may be considered to reduce the risk of recurrence and of other obesity-related cancers.[2]
Elderly and comorbid women. Endometrial cancer is common in women over 75, many of whom have significant comorbidity. Laparoscopic or vaginal surgery (with lower morbidity than open) is preferred where possible; frailty assessment informs the decision to operate or to use primary radiotherapy in unfit women who cannot tolerate surgery.[3]
Pregnant women. Endometrial cancer in pregnancy is exceptionally rare because pregnancy is a high-progesterone protective state. Management is multidisciplinary, balancing gestational age, stage, and the mother's wishes; small low-grade tumours may be managed conservatively until delivery.[2]
Women on tamoxifen. Any vaginal bleeding on tamoxifen demands TVUS and biopsy. Routine screening of asymptomatic women on tamoxifen is not recommended (low yield, high false-positive rate from tamoxifen-induced subendometrial cystic change).[2]
Evidence, Guidelines & Regional Differences
The modern evidence base for endometrial cancer adjuvant therapy rests on a small number of landmark randomised trials that defined risk-group management.[3]
Key finding
Key finding
Key finding
Key finding
Key finding
Key finding
Key finding
Guidelines and regional deltas.[3]
Europe (ESGO/ESTRO/ESP). The 2021 ESGO/ESTRO/ESP guidelines (Concin and colleagues) provide the most detailed risk-stratified framework, integrating molecular classification and defining the indications for surgery, radiotherapy, chemotherapy, and targeted therapy. Endorsed across most European national societies. [3]
Controversies. Whether molecular classification should drive adjuvant therapy de-escalation for POLE-mutant tumours even in advanced disease; the role of immunotherapy in the adjuvant setting for MMRd tumours; the optimal lymph node strategy (sentinel node versus full dissection versus none) in low-risk disease; and the role of ovarian conservation in premenopausal women with low-grade early-stage disease. The shift to molecular classification is the dominant contemporary change.[4][13]
Prevention
Endometrial cancer is unusual among cancers in having identifiable, modifiable risk factors and a recognised precursor lesion, making prevention a real possibility.[2][15]
Prevention cascade for endometrial cancer
Combined oral contraceptive pill. The Collaborative Group on Epidemiological Studies meta-analysis of 36 studies showed that each five years of oral contraceptive use reduces endometrial cancer risk by about 25 per cent, with protection persisting for 30 years after stopping. This is the most powerful single protective factor.[15]
Progestin in hormone replacement therapy. The Million Women Study confirmed that oestrogen-only HRT increases endometrial cancer risk in women with a uterus, while combined (opposed) HRT does not — and combined HRT is the standard for any woman with a uterus requiring HRT. The levonorgestrel intrauterine system (Mirena) provides effective endometrial protection during oestrogen replacement and may have a role in treating atypical hyperplasia.[14][17]
Lynch syndrome surveillance. Women with confirmed Lynch syndrome undergo intensive colorectal surveillance (colonoscopy every 1 to 2 years from age 25 to 35) and are counselled about the option of risk-reducing total hysterectomy and bilateral salpingo-oophorectomy once childbearing is complete.[3]
Exam Pearls
- Endometrial cancer is the most common gynaecological malignancy in developed countries and the sixth most common cancer in women worldwide.[1]
- Any postmenopausal bleeding is endometrial cancer until proven otherwise — transvaginal ultrasound (endometrial thickness over 4 to 5 mm) plus endometrial biopsy is the diagnostic pathway.[2]
- Type I (endometrioid, 80 per cent) is oestrogen-driven through hyperplasia with atypia; Type II (serous, clear cell, 20 per cent) is TP53-driven and aggressive.[5][16]
- Risk factors cluster around unopposed oestrogen: obesity (dominant), nulliparity, early menarche, late menopause, PCOS, oestrogen-only HRT, tamoxifen, diabetes; protective: combined OCP, multiparity, progestin.[2][15]
- Lynch syndrome carries a 40 to 60 per cent lifetime endometrial cancer risk; endometrial cancer is often the sentinel cancer; universal MMR immunohistochemistry is recommended on all endometrial cancers.[3]
- Pipelle biopsy is the standard outpatient test; hysteroscopy with D and C is the gold standard.[3]
- Surgery is the cornerstone: total hysterectomy and bilateral salpingo-oophorectomy, plus sentinel node biopsy (FIRES trial) or full lymphadenectomy for intermediate or high risk.[3][11]
- Adjuvant therapy is risk-stratified: low risk — observation; intermediate — vaginal vault brachytherapy (PORTEC-2); high risk — chemoradiotherapy (PORTEC-3).[9][10]
- Carboplatin AUC 5 to 6 plus paclitaxel 175 mg per m² every 3 weeks for 6 cycles is the standard chemotherapy for high-risk and advanced disease.[3][10]
- Fertility-sparing high-dose progestin (medroxyprogesterone 400 to 600 mg daily, or megestrol 160 to 320 mg daily) for grade 1, stage IA disease in selected young women.[19]
- Atypical hyperplasia on biopsy carries a 25 to 40 per cent risk of coexistent carcinoma — definitive treatment (hysterectomy) or progestin with close follow-up.[17]
- The four TCGA molecular subgroups (POLE-ultramutated, MMRd, p53-abnormal, NSMP) are incorporated into FIGO 2023 staging and drive adjuvant therapy.[4][12]
- Trastuzumab added to carboplatin-paclitaxel for HER2-positive uterine serous carcinoma (Fader 2018).[18]
- Tamoxifen doubles endometrial cancer risk — any bleeding on tamoxifen must be investigated.[2]
- The one-liner: postmenopausal bleeding in an obese woman — transvaginal ultrasound and biopsy before you theorise.
References
- [1]Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin, 2021.PMID 33538338
- [2]Lu KH, Broaddus RR. Endometrial Cancer. N Engl J Med, 2020.PMID 33207095
- [3]Concin N, Matias-Guiu X, Vergote I, et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int J Gynecol Cancer, 2021.PMID 33397713
- [4]Berek JS, Matias-Guiu X, Creutzberg C, et al. FIGO staging of endometrial cancer: 2023. Int J Gynaecol Obstet, 2023.PMID 37337978
- [5]Bokhman JV. Two pathogenetic types of endometrial carcinoma. Gynecol Oncol, 1983.PMID 6822361
- [6]Creasman W. Revised FIGO staging for carcinoma of the endometrium. Int J Gynaecol Obstet, 2009.PMID 19345353
- [7]Keys HM, Roberts JA, Brunetto VL, et al. A phase III trial of surgery with or without adjunctive external pelvic radiation therapy in intermediate risk endometrial adenocarcinoma: a Gynecologic Oncology Group study. Gynecol Oncol, 2004.PMID 14984936
- [8]Creutzberg CL, van Putten WL, Koper PC, et al. Surgery and postoperative radiotherapy versus surgery alone for patients with stage-1 endometrial carcinoma: multicentre randomised trial. PORTEC Study Group. Post Operative Radiation Therapy in Endometrial Carcinoma. Lancet, 2000.PMID 10791524
- [9]Nout RA, Smit VT, Putter H, et al. Vaginal brachytherapy versus pelvic external beam radiotherapy for patients with endometrial cancer of high-intermediate risk (PORTEC-2): an open-label, non-inferiority, randomised trial. Lancet, 2010.PMID 20206777
- [10]de Boer SM, Powell ME, Mileshkin L, et al. Adjuvant chemoradiotherapy versus radiotherapy alone for women with high-risk endometrial cancer (PORTEC-3): final results of an international, multicentre, open-label, randomised, phase 3 trial. Lancet Oncol, 2018.PMID 29449189
- [11]Rossi EC, Kowalski LD, Scalici J, et al. A comparison of sentinel lymph node biopsy to lymphadenectomy for endometrial cancer staging (FIRES trial): a multicentre, prospective, cohort study. Lancet Oncol, 2017.PMID 28159465
- [12]Kandoth C, Schultz N, Cherniack AD, et al. Integrated genomic characterization of endometrial carcinoma. Nature, 2013.PMID 23636398
- [13]Leon-Castillo A, de Boer SM, Powell ME, et al. Molecular Classification of the PORTEC-3 Trial for High-Risk Endometrial Cancer: Impact on Prognosis and Benefit From Adjuvant Therapy. J Clin Oncol, 2020.PMID 32749941
- [14]Beral V, Bull D, Reeves G, et al. (Million Women Study Collaborators). Endometrial cancer and hormone-replacement therapy in the Million Women Study. Lancet, 2005.PMID 15866308
- [15]Collaborative Group on Epidemiological Studies on Endometrial Cancer. Endometrial cancer and oral contraceptives: an individual participant meta-analysis of 27 276 women with endometrial cancer from 36 epidemiological studies. Lancet Oncol, 2015.PMID 26254030
- [16]Suarez AA, Felix AS, Cohn DE. Bokhman Redux: Endometrial cancer "types" in the 21st century. Gynecol Oncol, 2017.PMID 27993480
- [17]Gallos ID, Shehmar M, Thangaratinam S, et al. Oral progestogens vs levonorgestrel-releasing intrauterine system for endometrial hyperplasia: a systematic review and metaanalysis. Am J Obstet Gynecol, 2010.PMID 20934679
- [18]Fader AN, Roque DM, Siegel E, et al. Randomized Phase II Trial of Carboplatin-Paclitaxel Versus Carboplatin-Paclitaxel-Trastuzumab in Uterine Serous Carcinomas That Overexpress Human Epidermal Growth Factor Receptor 2/neu. J Clin Oncol, 2018.PMID 29584549
- [19]Ramirez PT, Frumovitz M, Bodurka DC, et al. Hormonal therapy for the management of grade 1 endometrial adenocarcinoma: a literature review. Gynecol Oncol, 2004.PMID 15385122