Obstetrics & Gynaecology · Obstetrics & Gynaecology
Miscarriage & Recurrent Pregnancy Loss
Also known as Miscarriage · Spontaneous abortion · Recurrent pregnancy loss · RPL · Threatened miscarriage · Missed miscarriage · Blighted ovum
Miscarriage (spontaneous abortion) is the loss of a pregnancy before 24 weeks of gestation (the threshold of viability). It is the commonest complication of pregnancy, affecting about 1 in 5 clinically recognised pregnancies (and far more when biochemical losses are counted). The clinical types are distinguished by the cervical os and ultrasound viability: threatened (bleeding, closed os, viable fetus), inevitable (bleeding, open os), incomplete (partial passage, open os, ongoing bleeding), complete (all passed, closed os), missed (fetal demise, retained), and septic (infection — an emergency). Recurrent pregnancy loss (RPL) is 3 or more consecutive first-trimester losses. The commonest cause overall is chromosomal abnormality of the embryo (over 50 percent); the most important treatable cause of RPL is antiphospholipid syndrome. Diagnosis rests on transvaginal ultrasound (TVS) using the NICE non-viability criteria plus serial beta-hCG; management offers expectant, medical (mifepristone plus misoprostol) or surgical (suction evacuation) options, with anti-D for all Rh-negative women.<Cite id="1" /<Cite id="2" /
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Exam tags
Red flags

Overview & Definition
Miscarriage, or spontaneous abortion, is the loss of a pregnancy before 24 weeks of gestation — the threshold of fetal viability in the UK. United States practice often uses 20 weeks of gestation or a fetal weight under 500 g. It is the commonest complication of pregnancy: about 1 in 5 (15 to 20 percent) of clinically recognised pregnancies end in miscarriage, and the true figure is far higher when biochemical and unrecognised conceptions are included, since over half of all fertilised ova fail to establish a continuing pregnancy. Losses are conventionally divided into early (before 12 weeks) — the large majority — and late (second-trimester, 12 to 24 weeks), which have a different cause profile and carry greater maternal risk.[1]
The topic is high-yield because of four examinable pillars. First, the classification (threatened, inevitable, incomplete, complete, missed, septic) is decided by the cervical os and by ultrasound viability — a classic viva and MCQ discriminator. Second, the transvaginal ultrasound criteria for non-viability are explicit and must never be misapplied, because a false-positive diagnosis of loss can lead to the destruction of a wanted, viable pregnancy. Third, the three management options (expectant, medical, surgical) are genuinely equivalent in outcome, so patient choice drives selection. Fourth, recurrent pregnancy loss has a structured workup whose centrepiece — antiphospholipid syndrome — is the one cause with a proven, treatable answer. Running through all of it is the clinical skill of compassionate communication: most women blame themselves, and the reassurance that the commonest cause is a random, non-recurrent chromosomal error is itself therapeutic.[1][2]
A clinically useful distinction is the PUL — pregnancy of unknown location. When a woman bleeds in early pregnancy and the initial TVS shows neither an intrauterine nor an ectopic pregnancy, the pregnancy is of unknown location until serial hCG and repeat imaging resolve it. This framing protects against two errors: declaring a loss prematurely, and missing an ectopic.
[1]Miscarriage — the headline numbers
Classification
The clinical types of miscarriage are distinguished by two findings at speculum examination — the cervical os (open or closed) — combined with what has been passed and the ultrasound appearance. Getting this classification right determines management, and it is the single most frequently tested fact in the topic.
[1]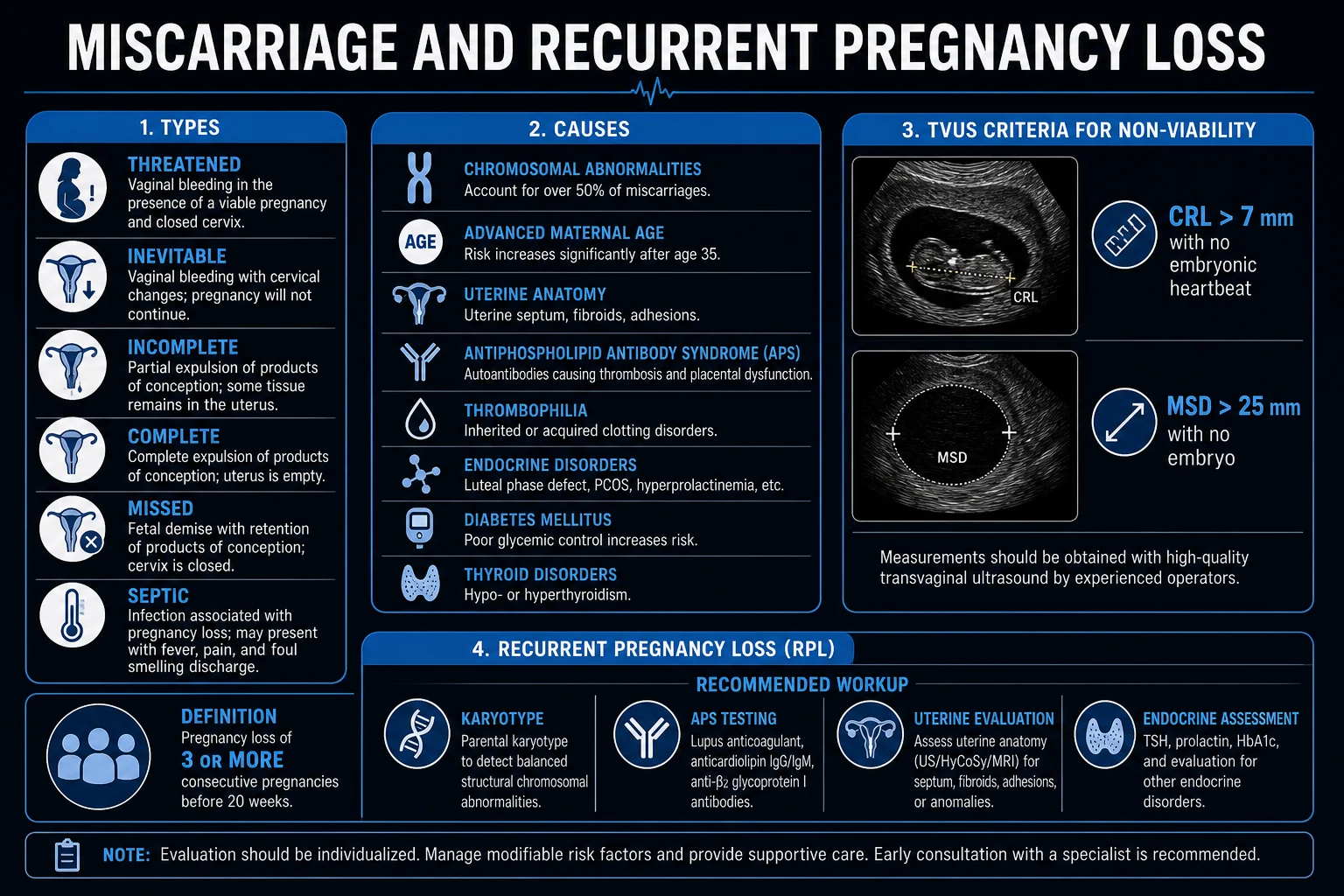
Threatened
closed os, viable
- Vaginal bleeding, **closed internal cervical os**
- **Viable intrauterine fetus** on TVS (positive heartbeat)
- About 1 in 4 women bleed in early pregnancy; most continue
- Management: reassurance, rescan if bleeding persists, anti-D if Rh-negative
Inevitable
open os, not passed
- Bleeding plus cramping, **internal os OPEN**
- Products of conception **not yet passed**
- Process is underway and cannot be reversed
- Manage as a pregnancy in the process of loss
Incomplete
partial passage plus bleeding
- **Partial passage** of products, os remains open
- **Ongoing, often heavy, bleeding** — commonest acute presentation
- Risk of haemorrhage and infection
- Often needs medical or surgical evacuation
Complete
passed, closed os
- All products of conception passed
- **Cervical os closed**, bleeding and pain settling
- Confirm on scan or history; usually no further treatment needed
- Anti-D if Rh-negative; contraception and follow-up advice
Missed
demise, retained
- **Fetal demise with retained products**, os closed
- Minimal or no bleeding; loss of pregnancy symptoms
- Includes anembryonic (blighted ovum) and embryo with no heartbeat
- Offer expectant, medical or surgical management
Septic
infection — emergency
- **Fever, uterine tenderness, foul discharge**, tachycardia
- Retained infected products; history of unsafe procedure
- Life-threatening — can progress to septic shock and ARDS
- **IV antibiotics plus urgent evacuation**
A threatened miscarriage carries a good prognosis: once a fetal heartbeat is documented at 6 to 8 weeks, the risk of subsequent loss falls to under 5 percent in women without bleeding and to around 10 to 15 percent with bleeding. An inevitable or incomplete miscarriage is the typical acute presentation needing assessment for blood loss and a decision on evacuation. A missed miscarriage is often an ultrasound surprise at a routine scan, which makes the repeat-scan rule (below) so important. Septic miscarriage is now rare where safe services exist but remains an obstetric emergency where unsafe procedures are performed.
[1]Recurrent pregnancy loss (RPL)
[1] [1]RPL affects about 1 to 2 percent of couples trying to conceive. Crucially, even unexplained RPL has a reassuring outlook: supportive care alone yields a live birth in roughly 55 to 75 percent of subsequent pregnancies.
[1]Epidemiology & Risk Factors
The single strongest determinant of miscarriage risk is maternal age, driven by the rising rate of oocyte aneuploidy. Risk is about 10 percent at age 25, 20 percent at 35, 50 percent at 40, and over 90 percent at 45. The biological basis is that female oocytes arrest in prophase of meiosis I before birth and resume division decades later; the longer the oocyte is held in arrest, the more the meiotic spindle and cohesion complex degrade, so that nondisjunction — and therefore aneuploidy — becomes steadily more likely. Paternal age over 40 contributes a smaller additional risk through rising sperm aneuploidy and DNA fragmentation.
[1]Risk factors group logically into maternal, anatomic, endocrine, thrombophilic, infectious, lifestyle and iatrogenic categories:
[1]- Maternal age — the dominant factor (see above); also a predictor of recurrence.
- Previous miscarriage — risk rises with each successive loss; after one loss about 20 percent, after two about 28 percent, after three about 43 percent.
- Anatomic — congenital uterine anomalies (septum is the one most strongly linked to loss), diethylstilboestrol exposure in utero, cervical insufficiency, submucosal fibroids, intrauterine adhesions (Asherman).
- Endocrine — uncontrolled type 1 or type 2 diabetes (HbA1c elevated pre-conception), thyroid disease, polycystic ovary syndrome, poorly controlled hyperprolactinaemia.
- Thrombophilic — antiphospholipid syndrome (acquired), and inherited thrombophilias (factor V Leiden, prothrombin gene mutation, protein C/S and antithrombin deficiency), particularly linked to late loss.
- Infectious — listeria, toxoplasma, syphilis, malaria, brucella; often modifiable.
- Lifestyle and environment — smoking (roughly doubles risk), alcohol (no safe dose in pregnancy), obesity, very high caffeine intake, recreational drugs.
- Iatrogenic — teratogenic drugs (warfarin, retinoids, methotrexate, some anticonvulsants), invasive prenatal procedures.
Importantly, a single first-trimester loss is usually a sporadic chromosomal event — recurrence risk is low, and most women go on to a successful next pregnancy. This single fact is the cornerstone of post-miscarriage counselling.
[1]Aetiology
Miscarriage is usually the result of interplay between embryo, endometrium, placental perfusion, and maternal health. The relative importance of each cause shifts with gestational age, maternal age, and whether the loss is sporadic or recurrent. A systematic aetiological framework is essential for counselling and for directing investigation in recurrent loss.
[1]Chromosomal abnormalities
Chromosomal abnormalities of the embryo are the single largest cause of first-trimester miscarriage, identified in 50 to 70 percent of losses. The spectrum is dominated by autosomal trisomies, monosomy X, triploidy, and structural rearrangements inherited from a balanced translocation carrier. Most numerical errors arise from meiotic nondisjunction in the maternal oocyte, reflecting the biology of an oocyte arrested in prophase I for years. The error is usually non-recurrent, which is why a single chromosomal loss carries a good prognosis.[1]
Uterine and cervical factors
Congenital uterine anomalies are found in up to 20 percent of women with recurrent miscarriage, and the septate uterus is the anomaly most strongly linked to first-trimester loss. Other anatomic causes include submucosal fibroids, intrauterine adhesions (Asherman syndrome), and cervical insufficiency — the latter presenting with painless second-trimester dilation. Acquired uterine cavity disease from previous surgery, infection, or over-vigorous curettage can also compromise implantation and placental bed development.[2]
Endocrine and metabolic disease
Uncontrolled diabetes, thyroid disease (hypothyroidism and hyperthyroidism), hyperprolactinaemia, and polycystic ovary syndrome can all increase miscarriage risk. The mechanism is often a combination of poor pre-implantation endometrial quality, luteal-phase progesterone deficiency, and altered early vascular adaptation. Optimising metabolic control before conception is one of the most effective interventions; an HbA1c in the target range before pregnancy reduces both aneuploidy-independent and pregnancy complication risk.[2]
Immunological and thrombophilic causes
Antiphospholipid syndrome (APS) is the most important treatable acquired cause of recurrent miscarriage. It is diagnosed by persistent lupus anticoagulant, anticardiolipin, or anti-beta-2-glycoprotein-I antibodies, and acts by causing placental microvascular thrombosis and infarction. Inherited thrombophilias (factor V Leiden, prothrombin gene mutation, protein C, protein S, and antithrombin deficiency) are more strongly associated with late first-trimester and second-trimester losses, but routine screening is not recommended in uncomplicated recurrent loss because trial evidence has not shown benefit from heparin in unselected cases.[1]
Infection and environmental exposures
Systemic infections such as listeria, toxoplasmosis, syphilis, malaria, brucella, and parvovirus B19 can precipitate miscarriage, particularly in endemic areas or immunocompromised hosts. Local genital-tract infection and chronic endometritis are active areas of research in recurrent loss. Lifestyle factors independently raise risk: smoking approximately doubles the risk, and heavy alcohol use, obesity, high caffeine intake, and recreational drugs also contribute. Ionising radiation, certain solvents, and teratogenic drugs (warfarin, retinoids, methotrexate, some anticonvulsants) can cause loss.[2]
A note on causation
After one or even two losses, it is often impossible to assign a specific cause. In recurrent loss, the diagnostic yield of the standard workup is only about 50 to 60 percent; the remainder is classified as unexplained. Even in unexplained recurrent loss, the prognosis remains good with supportive care, so counselling should be balanced and hopeful.[1]
Pathophysiology
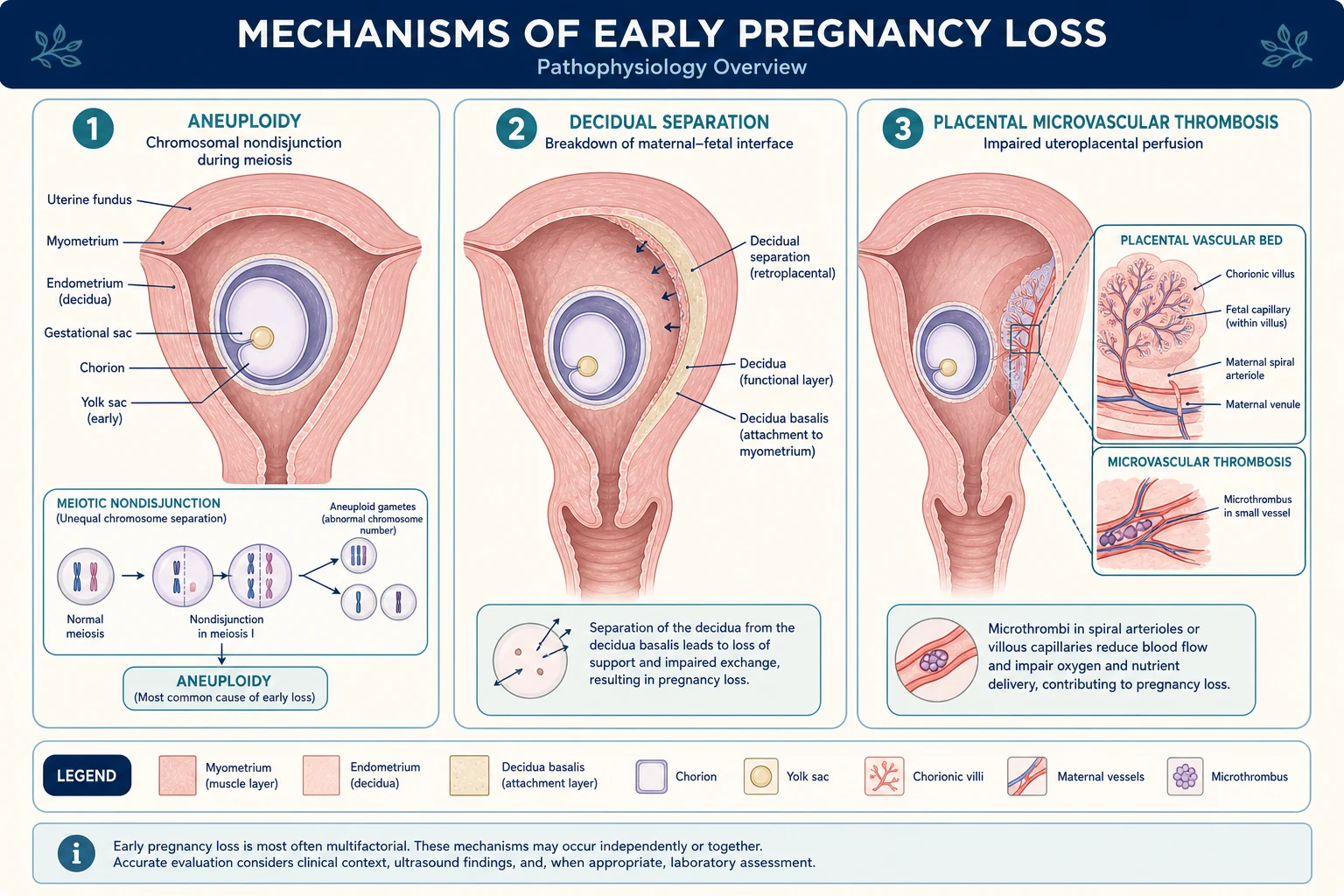
Successful early pregnancy depends on three integrated processes — a euploid embryo, an adequately remodelling decidua and spiral artery bed, and a functioning placental endocrine unit (hCG and progesterone) — held in immunological tolerance by the maternal-fetal interface. Miscarriage results when any of these fails.
[1]Chromosomal abnormalities — the dominant mechanism
Chromosomal abnormalities of the embryo are the commonest cause, found in over 50 percent and up to 70 percent of first-trimester losses. They fall into several recognisable patterns:
[1]- Autosomal trisomies are the largest group. Trisomy 16 is the single most frequent and is virtually always lethal; trisomies of 21, 18, 13, 22 and 15 are also common. Most arise from meiotic nondisjunction — failure of homologous chromosomes (meiosis I) or sister chromatids (meiosis II) to separate, producing a gamete with an extra chromosome. The error is usually maternal, in the oocyte.
- Monosomy X (45,X, Turner syndrome) is the commonest single chromosomal abnormality in early loss. It typically arises from loss of the paternal sex chromosome; it is the only viable human monosomy, but the great majority of 45,X conceptions are lost in the first trimester.
- Triploidy (69,XXX/XXY/XYY) — three full sets of chromosomes, often from diandry (dispermy — two sperm fertilising one oocyte) or digyny (a diploid oocyte). Diandric triploidy gives a partial mole appearance with an enlarged placenta; digynic triploidy gives a small placenta and growth-restricted fetus.
- Tetraploidy (92,XXXX) — usually lethal and a post-zygotic error.
- Structural rearrangements — a small but important minority (3 to 5 percent of couples with RPL) carry a balanced parental translocation (reciprocal or Robertsonian). The parent is phenotypically normal, but gametes receive an unbalanced complement, producing recurrent losses or live-born children with congenital abnormalities (for example, Down syndrome from a Robertsonian translocation).
The consequence of a lethal chromosomal error is embryonic developmental arrest. The embryo may never form (an anembryonic gestation or blighted ovum — a gestational sac with a yolk sac but no embryo), or it may form and then stop growing and lose its heartbeat (an embryonic or fetal missed loss). On ultrasound the gestational sac becomes irregular or empty, its margins become distorted, and the pregnancy resolves as the trophoblast fails.
[1]Decidual separation and bleeding
Once the trophoblast and decidua begin to separate from the uterine wall, the maternal decidual sinusoids are opened, producing the vaginal bleeding that brings the woman to care. Uterine contractions — felt as cramping — accompany the expulsion of products. In an incomplete loss, retained tissue keeps the cervix open and the bleeding ongoing; in a complete loss, the uterus contracts down, the os closes, and bleeding settles. The amount of blood lost can be substantial, and the haemodynamic picture (tachycardia, hypotension) rather than the reported volume should guide resuscitation.
[1]Placental endocrine failure — hCG and progesterone
A viable early pregnancy is sustained by human chorionic gonadotrophin (hCG), produced by the syncytiotrophoblast, which rescues the corpus luteum and maintains progesterone secretion until the luteoplacental shift at around 7 to 10 weeks. Progesterone is the hormone of pregnancy maintenance — it stabilises the decidual endometrium, suppresses uterine contractility, and modulates the maternal immune response. When an embryo is non-viable, hCG production falls, progesterone support is withdrawn, and the decidua breaks down. This endocrine logic underpins two clinical tools: the serial hCG trend (a failing pregnancy shows a sub-63-percent rise in 48 hours) and the progesterone level (under 25 nmol/L suggests a non-viable pregnancy). It also explains the rationale for mifepristone in medical management — by blocking progesterone receptors it actively destabilises the pregnancy.
[1]Spiral artery remodelling and placental thrombosis
For a pregnancy to progress beyond the first trimester, the extravillous trophoblast must invade and remodel the maternal spiral arteries, converting them from narrow, high-resistance vessels into dilated, low-resistance channels that deliver the increasing blood flow the fetus demands. When this remodelling fails — as in antiphospholipid syndrome, inherited thrombophilias, or severe hypertensive disease — the placental bed suffers microvascular thrombosis and infarction, placental perfusion falls, and the pregnancy fails, often in the late first or second trimester. This is the placental mechanism that links thrombophilia to recurrent and late loss, and it is why anticoagulation can improve outcome in APS-related RPL.
[1]Immunological tolerance
Pregnancy is a natural allograft — the fetus carries paternal antigens yet is not rejected. Tolerance depends on HLA-G expression by the trophoblast (which protects it from maternal cytotoxic T cells), on a balanced population of uterine natural killer cells, and on regulatory T-cell activity. Disturbances in these mechanisms are an active area of research in unexplained RPL, though no single immunological test yet has a proven treatment attached to it.
[1]Late-loss mechanisms
Late (second-trimester) losses have a distinct mechanism profile: cervical insufficiency (painless dilation with bulging membranes, from a congenital, traumatic — cone biopsy/LEEP — or iatrogenic cause), major uterine anomalies (septum), severe maternal infection (e.g. chorioamnionitis), placental abruption, and antiphospholipid syndrome with placental thrombosis. These mechanisms are why the RPL workup emphasises uterine anatomy and the thrombophilias.[1]
Clinical Presentation
The classic presentation is vaginal bleeding with lower abdominal cramping in a woman who knows or suspects she is pregnant. The amount of bleeding ranges from light spotting to heavy loss with clots and tissue. Pain is usually central and cramping in character, which helps distinguish miscarriage from the lateral, often shoulder-tip, pain of a ruptured ectopic. Specific features define each type:
[1]- Threatened — lighter bleeding, closed os, viable fetus on scan; pregnancy symptoms (nausea, breast tenderness, urinary frequency) preserved. About 1 in 4 women bleed at some point in early pregnancy and most continue.
- Inevitable — moderate to heavy bleeding with cramping; os open; products not yet passed. The woman often describes the bleeding as heavier than a period.
- Incomplete — partial passage of tissue (she may describe "something coming away"), open os, ongoing or heavy bleeding; the commonest presentation needing acute care.
- Complete — all products passed; bleeding and pain settling; os closed. The woman often reports that the pain resolved once tissue passed.
- Missed — often a routine-scan finding; the woman reports loss of pregnancy symptoms (nausea gone, breasts no longer tender) but may have minimal or no bleeding.
- Septic — fever, pelvic/abdominal pain, foul-smelling vaginal discharge, uterine tenderness, tachycardia; a history of an unsafe procedure is the key clue.
Atypical presentations examiners test deliberately:
[1]- Unrecognised or unplanned pregnancy — a woman may attribute early heavy bleeding to a late, heavy period (a biochemical or "chemical" pregnancy loss, detectable only on a pregnancy test around the time of the expected period).
- Older women — higher baseline miscarriage risk, more comorbidity, and often a long path to conception with IVF; the psychological stakes are high.
- IVF pregnancies — higher early-loss rate and greater emotional investment; an early scan is routine.
- Women on anticoagulation or with a bleeding diathesis — bleeding may be heavier and management must coordinate the haematological and obstetric issues.
- A woman who presents in shock — assume a ruptured ectopic or sepsis until proven otherwise; resuscitate first, investigate second.
Interpreting pain, bleeding and haemodynamics
The character of pain and the volume of bleeding are useful, but they are not definitive. A woman with a threatened miscarriage can pass surprisingly large clots, while a missed miscarriage can be entirely silent. What matters is the clinical trajectory.
[1]- Threatened miscarriage is usually described as light spotting, often brownish, with mild cramping. About one in four women has some first-trimester bleeding; once a live embryo with a heartbeat is seen on scan, the majority continue to term. Still, the woman must be safety-netted: a threatened miscarriage can evolve into an inevitable or incomplete loss, and Rh-negative women need anti-D.
- Inevitable and incomplete miscarriage are the classic acute presentations. Bleeding is usually heavier than a period, bright red, and accompanied by clots and tissue. Pain is central, cramping, and may come in waves as the uterus contracts. The open cervical os tells you that the process is active and cannot be stopped. Haemodynamic instability — tachycardia, postural drop, or hypotension — means the bleeding is significant and surgical evacuation is needed.
- Missed miscarriage is often discovered when symptoms of pregnancy regress. A woman may say her nausea has gone, her breasts are no longer tender, or she has lost the metallic taste in her mouth. Because there is no active bleeding, the diagnosis rests on ultrasound, and the repeat-scan rule is essential to avoid a false-positive diagnosis of loss.
- Septic miscarriage should be suspected when there is fever, tachycardia, uterine tenderness, and foul discharge, especially after an unsafe termination or instrumentation. The woman may have been unwell for days before seeking care. This is an emergency: sepsis can progress rapidly to septic shock, acute respiratory distress syndrome, and disseminated intravascular coagulation.
Two practical rules always apply: assess the haemodynamic status before taking a long history, and never assume a closed os means the bleeding is not serious. A closed os with a viable fetus is reassuring, but a closed os with retained infected products can still cause sepsis, and a closed os in an ectopic pregnancy is the most dangerous situation of all. The cervical os is the single most reliable clinical sign; do not be misled by the amount of blood alone, and always confirm the diagnosis with transvaginal ultrasound when bleeding occurs in early pregnancy.
[1]Differential Diagnosis
Every woman with bleeding in early pregnancy must be assumed to have a pregnancy of unknown location until a viable intrauterine pregnancy is confirmed — because the differential contains a life-threatening mimic (ectopic) and several look-alikes.
[1]Ectopic pregnancy
must exclude
- Amenorrhoea plus (usually lateral) pain plus dark scanty bleeding
- **Empty uterus** on TVS plus adnexal mass or free fluid
- Closed OR open os; cervical motion tenderness on bimanual
- Can rupture to haemorrhagic shock — always exclude first; discriminatory hCG zone applies
Implantation bleed
benign
- Light spotting around the time of the expected period
- Viable intrauterine pregnancy on scan
- Self-limiting; no intervention needed; reassurance
Cervical cause
local lesion
- Cervical polyp, ectropion, or (rarely) cervical cancer
- Bleeding often on contact or after intercourse
- Viable intrauterine pregnancy — visualise the cervix on speculum
Molar pregnancy
vesicular
- Heavy bleeding plus passage of **vesicles** (grape-like)
- Uterus **large for dates**, very high hCG, theca-lutein cysts, hyperemesis
- Snowstorm ultrasound; risk of persistent trophoblastic disease
Non-pregnancy causes
exclude pregnancy first
- Corpus luteum cyst rupture or haemorrhage (acute pain, no amenorrhoea)
- Urinary tract infection, gastroenteritis, appendicitis
- ALWAYS do a pregnancy test first — a positive test changes everything
The pivotal reflex is: bleeding in early pregnancy equals TVS to locate the pregnancy and exclude ectopic, supported by a serial quantitative beta-hCG. The distinguishing features are the character of the pain (central/cramping in miscarriage vs lateral/constant or shoulder-tip in ectopic), the volume of bleeding (heavy with products in miscarriage vs dark and scanty in ectopic), and the ultrasound (intrauterine vs empty uterus with an adnexal mass).
[1]Clinical & Bedside Assessment
Begin with ABCs and haemodynamic status — tachycardia, hypotension and pallor signal significant bleeding or sepsis and demand resuscitation rather than a prolonged history. Tachycardia and postural drop are early signs; hypotension is late. Focused assessment then covers:
[1]- History — last menstrual period and gestation; the amount of bleeding (pads per hour, presence of clots, tissue passed); pain (site, character, severity); obstetric history including previous losses and their gestation; Rh status; medical conditions (diabetes, thyroid, APS, thrombophilia); medications (especially anticoagulants and teratogens); and any history of an unsafe procedure.
- Speculum examination — assess the cervical os (open or closed: the classification hinge); the source and volume of bleeding; whether products of conception are visible at the os (and remove them gently, as this alone may reduce bleeding); and exclude local cervical causes (polyp, ectropion, trauma).
- Bimanual examination — uterine size and tenderness, adnexal masses or tenderness, and cervical excitation (pain on moving the cervix, which raises the suspicion of ectopic or PID).
Findings are then interpreted together with a transvaginal ultrasound. A tender, boggy uterus with an open os and heavy bleeding points to incomplete miscarriage; a closed os with a viable fetus points to threatened loss; a tender uterus with fever and discharge is septic until proven otherwise. In a shocked patient, resuscitate first and image in parallel or after — never delay life-saving surgery (for a suspected ruptured ectopic) for a scan.
[1]Investigations
Transvaginal ultrasound (TVS) — the diagnostic cornerstone
TVS determines whether a pregnancy is intrauterine, whether it is viable, and what has been passed or retained. To avoid the catastrophic error of declaring a viable pregnancy non-viable, NICE NG126 sets conservative, never-isolated thresholds that must be confirmed on a repeat scan at least 7 days apart when there is any doubt:
[1] [1]The discriminatory zone is the related concept that helps interpret an early scan: at a serum beta-hCG of around 1500 to 2000 IU/L, a healthy intrauterine pregnancy should be visible on TVS. An hCG above this level with an empty uterus raises the suspicion of ectopic; an hCG below it with an empty uterus is a pregnancy of unknown location that needs serial hCG and repeat scanning.[1]
Serial beta-hCG
A quantitative serum beta-hCG is interpreted dynamically. In a normally developing early intrauterine pregnancy, beta-hCG approximately doubles every 48 hours (a rise of at least 53 percent by older criteria, now usually quoted as at least 63 percent); a rise of less than 63 percent in 48 hours is suspicious for a non-viable or ectopic pregnancy, and a falling beta-hCG confirms a failing pregnancy but does not locate it — ectopic must still be excluded by scan. A useful bedside calculation is the hCG ratio (the 48-hour value divided by the baseline): a ratio of under 1.66 suggests an abnormal pregnancy. Progesterone is sometimes used as an adjunct (a level under 25 nmol/L suggests a non-viable pregnancy; over 60 nmol/L is reassuring), but TVS and serial hCG are the primary tools.
[1]Scan-hCG concordance and the pregnancy of unknown location
When the ultrasound is inconclusive, the relationship between the scan and the quantitative hCG becomes the decision map. A normal intrauterine pregnancy should show:
[1]- A gestational sac by 5 weeks (beta-hCG roughly 1,000 to 2,000 IU/L).
- A yolk sac by 5.5 weeks.
- A fetal pole with heartbeat by 6 to 6.5 weeks.[1]
If the scan is empty but the hCG is below the discriminatory zone, classify the pregnancy as a pregnancy of unknown location (PUL) and repeat hCG in 48 hours. If the hCG rises normally and reaches the discriminatory zone, rescan; if the uterus is still empty, strongly suspect ectopic. If the hCG falls, the pregnancy is failing regardless of location; falling hCG with an empty uterus can still represent a resolving ectopic or an intrauterine miscarriage that has already passed.
[1]Pitfalls to avoid:
[1]- Do not diagnose miscarriage from a single hCG value.
- Do not diagnose miscarriage from a single borderline scan — always repeat in at least 7 days.
- Do not discharge a woman with a PUL without a clear plan for serial hCG and repeat imaging.
- Remember that multiple pregnancy can produce higher hCG for gestational age and may show more than one gestational sac.
Bloods and microbiology
- Full blood count — to assess anaemia, the platelet count, and (in sepsis) the white-cell count.
- Group and save / crossmatch — if bleeding is heavy or the woman is Rh-negative (to plan anti-D and, if needed, transfusion).
- Blood cultures, CRP, high vaginal swab — if septic miscarriage is suspected.
- Coagulation screen — in heavy bleeding or suspected sepsis, to detect incipient DIC.
Histopathology
Any tissue passed or evacuated should be sent for histology to confirm products of conception and to exclude molar pregnancy (which changes follow-up dramatically). In RPL, karyotyping of the products (by array comparative genomic hybridisation or QF-PCR) can reveal whether a loss was due to aneuploidy — useful prognostically and for counselling.
[1]Recurrent pregnancy loss workup
After 2 to 3 consecutive losses the structured workup is:
[1]- Parental peripheral blood karyotype — to detect a balanced reciprocal or Robertsonian translocation (3 to 5 percent of couples with RPL).
- Antiphospholipid antibodies — lupus anticoagulant, anticardiolipin (IgG/IgM), and anti-beta-2-glycoprotein-I, repeated at 12 weeks to confirm persistence (the APS laboratory criteria).
- Uterine assessment — 3D pelvic ultrasound, saline infusion sonohysterography, or hysteroscopy to detect a septum or other anomaly; hysterosalpingography if tubal assessment is also needed.
- Endocrine — TSH and HbA1c; consider prolactin and a PCOS screen.
- Inherited thrombophilia screen — factor V Leiden, prothrombin gene mutation, protein C, protein S, antithrombin (especially after a late loss).
- Karyotype of products, where available, from any future loss.
Management — Resuscitation
The immediate, time-critical bundles address the two emergencies — haemorrhage and sepsis:
[1]Management — Definitive & Stepwise
Threatened miscarriage
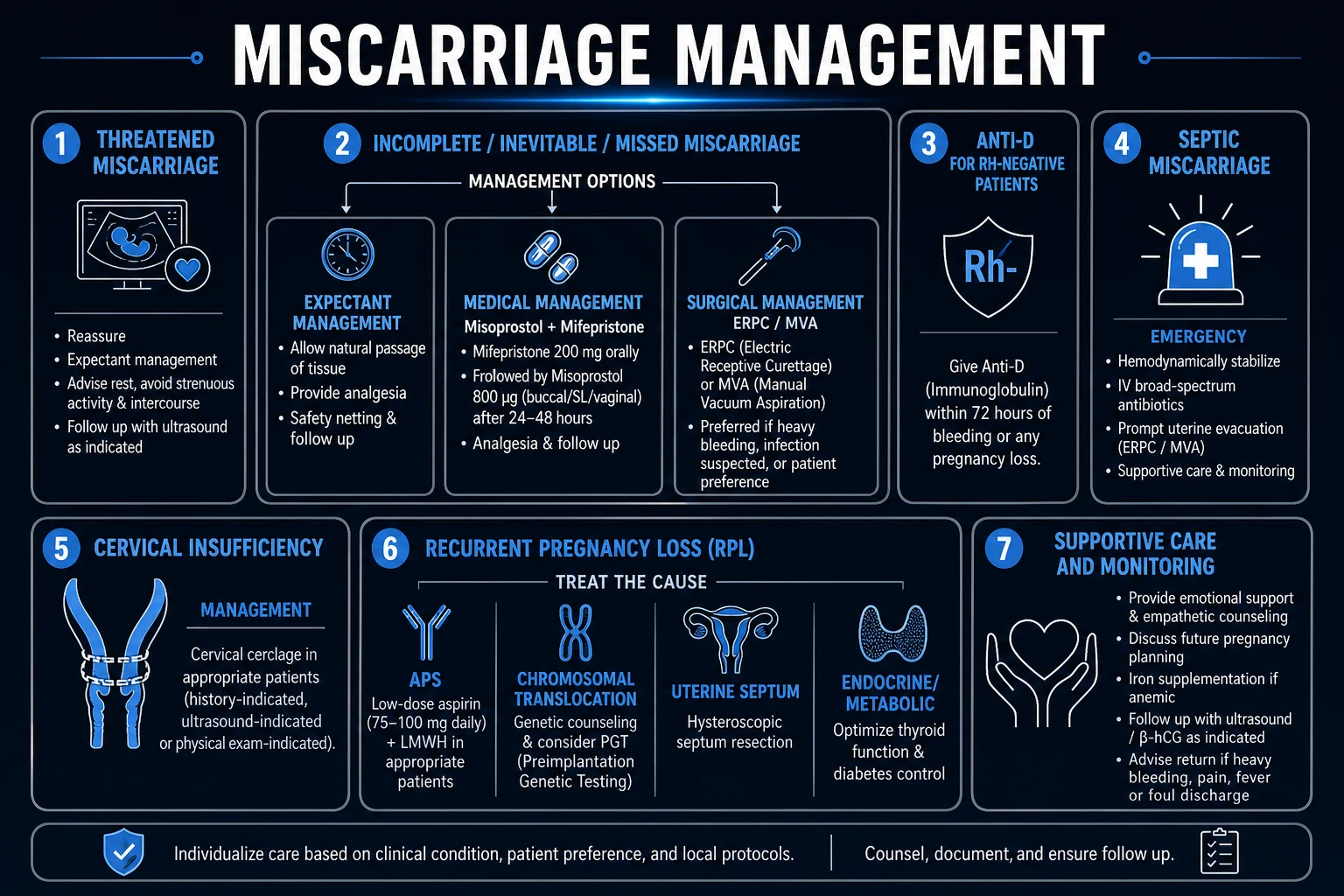
Reassure, manage expectantly, and rescan only if bleeding persists or worsens. The traditional restrictions on intercourse, travel, and bed rest are not evidence-based and should not be advised — they impose guilt without benefit. Give anti-D to Rh-negative women. Document a clear safety-net (return immediately if bleeding becomes heavy, with clots, or if fever or severe pain develops).
[1]Missed, inevitable or incomplete miscarriage (stable)
Three options, with patient choice driving selection — the MIST and related trials show broadly equivalent outcomes across expectant, medical and surgical approaches. Counsel each woman on the success rates, the expected experience (pain, bleeding, time), the need for follow-up, and the surgical risks, then let her choose:
[1]- Expectant — allow natural passage over 7 to 14 days; success is over 50 percent and up to 80 percent for early losses. Suitable for stable women with a small amount of retained tissue who prefer to avoid intervention. Review if bleeding becomes heavy or the process is incomplete on follow-up scan at 7 to 14 days.
- Medical — mifepristone 200 mg orally followed 1 to 2 hours later by misoprostol 800 microgram vaginal (or 600 microgram sublingual), with a repeat misoprostol dose after 24 hours if needed. Mifepristone pretreatment (a progesterone-receptor antagonist that primes the cervix and sensitises the uterus to prostaglandin) significantly improves complete-evacuation rates versus misoprostol alone (MifeMiso trial, Lancet 2020). Provide adequate analgesia (e.g. NSAIDs plus paracetamol; opiates for severe pain) and antiemetics. Suitable for women who prefer an active process but wish to avoid surgery.[3]
- Surgical — suction evacuation / ERPC (electric vacuum or manual vacuum aspiration). Preferred when there is heavy bleeding, sepsis, persistent bleeding after expectant or medical management, or where the woman chooses it. Cervical priming with misoprostol reduces cervical trauma. Manual vacuum aspiration (MVA) under local anaesthesia is an effective, low-cost outpatient option for early loss, with a lower complication rate than sharp curettage and no need for general anaesthesia.
Surgical techniques and safety
[1]Surgical management is the default when bleeding is heavy, infection is present, or expectant/medical management has failed. It is also the right choice when a woman wants a rapid, controlled resolution. The standard operation is uterine evacuation by suction rather than sharp curettage, because suction is quicker, safer, and less likely to cause Asherman syndrome.
[1]- Electric vacuum aspiration (EVA) uses a powered suction pump and is usually performed under general or regional anaesthesia in an operating theatre. It is appropriate for any first-trimester loss, including those with heavier bleeding or more substantial tissue.
- Manual vacuum aspiration (MVA) uses a handheld syringe to generate suction. It can be performed in the outpatient or clinic setting under local anaesthetic with oral analgesia. MVA is effective for pregnancies up to around 12 weeks, has low complication rates, and avoids the risks of general anaesthesia. It is the preferred surgical option in many low-resource settings.
- Dilatation and curettage (D&C) with a sharp curette is now discouraged for first-trimester evacuation because it carries a higher risk of uterine perforation, infection, and intrauterine adhesions. Suction is preferred for routine management.
Cervical priming with misoprostol 400 to 800 microgram vaginally or sublingually 1 to 3 hours before surgery softens the cervix and reduces cervical trauma, especially in nulliparous women. It is particularly helpful when the pregnancy is over 10 weeks or when the cervix is unfavourable.
[1]After evacuation, all tissue should be sent for histology. A follow-up visit or scan is arranged to confirm that the uterus is empty; if products remain, repeat evacuation or medical treatment may be needed.
[1]Whichever path is chosen: anti-D 250 IU IM within 72 hours for every Rh-negative woman, adequate analgesia, and a follow-up review (clinical or ultrasound) to confirm complete evacuation.[1]
Complete miscarriage
Confirm on history and scan; no further treatment is required. Provide anti-D if Rh-negative, contraception and pre-conception advice (folic acid, optimise chronic disease), and offer a follow-up for support.
[1]Surgical complications — know them
- Uterine perforation — occurs in roughly 1 to 4 per 1000 evacuations; suspect if there is unexpected pain, bleeding, or visceral injury; manage expectantly if small and stable, laparoscopically or laparotomically if bleeding or organ damage.
- Cervical trauma — reduced by cervical priming (misoprostol) and careful dilatation.
- Haemorrhage — from retained tissue or atony; managed by completing evacuation and uterotonics.
- Infection — post-evacuation endometritis; reduced by aseptic technique; treat with antibiotics.
- Asherman syndrome — intrauterine adhesions from over-vigorous curettage; prevented by using suction rather than sharp curettage and gentle technique.
- Anaesthetic complications — relevant to the woman's fitness for general anaesthesia; an argument for MVA under local anaesthesia in suitable cases.
Recurrent pregnancy loss — treat the cause
- Antiphospholipid syndrome: low-dose aspirin 75 mg once daily plus prophylactic low-molecular-weight heparin (e.g. enoxaparin 40 mg subcutaneous once daily) from confirmation of a viable pregnancy through to 6 weeks postpartum. This combination substantially improves live-birth rate. Warfarin is teratogenic and contraindicated in pregnancy.
- Parental translocation: genetic counselling and consideration of preimplantation genetic testing (PGT); outcomes are reasonable even without PGT, so couples should be counselled on both options.
- Uterine septum: hysteroscopic resection (metroplasty) before the next pregnancy in selected cases.
- Endocrine disease: optimise thyroid and glycaemic control pre-conception (HbA1c in the target range before conception in diabetes).
- Inherited thrombophilia: the ALIFE2 trial showed that LMWH did not improve live-birth rates in women with recurrent miscarriage and inherited thrombophilia compared with standard care; routine heparin is therefore not recommended for this indication, though aspirin plus LMWH remains appropriate in confirmed APS.[5]
- Unexplained RPL: supportive care, early scanning and reassurance in the next pregnancy; progesterone may help women with a history of loss and first-trimester bleeding (PRISM trial). Prognosis remains good (over 55 to 75 percent live birth).[4]
Anti-D Immunoglobulin
Every Rh-negative woman who has a miscarriage, threatened miscarriage, or any uterine bleeding in pregnancy should be offered anti-D immunoglobulin to prevent Rh sensitisation. Sensitisation can cause haemolytic disease of the fetus and newborn in subsequent pregnancies, and once it has occurred it cannot be reversed.[1]
Rationale and timing
In Rh-negative women, a small feto-maternal haemorrhage of Rh-positive fetal cells can occur during any uterine bleeding, trauma, or invasive procedure. The maternal immune system then produces anti-D antibodies that can attack fetal red cells in a future pregnancy. Anti-D immunoglobulin binds fetal Rh-positive red cells in the maternal circulation before they can trigger primary sensitisation. The standard dose is 250 IU intramuscularly within 72 hours of the sensitising event; give it as soon as possible after the diagnosis of miscarriage or after bleeding, but it is still worthwhile up to 72 hours later (and may still offer some benefit up to 10 days, though 72 hours remains the recommended window).[2]
When to give anti-D
Offer anti-D to every Rh-negative woman with:
[1]- Threatened miscarriage with bleeding at any gestation under 12 weeks (current UK guidance offers it even for first-trimester bleeding).
- Inevitable, incomplete, complete, or missed miscarriage — whether managed expectantly, medically, or surgically.
- Surgical evacuation — especially suction curettage or manual vacuum aspiration.
- Septic miscarriage — give as soon as the woman is stable enough; do not delay antibiotics for anti-D.
- Ectopic pregnancy — any surgical management or significant bleeding; use local guidance for medically managed ectopic pregnancy.
Additional testing
If the bleeding is heavy, particularly after trauma or after a potentially sensitising event at or after 20 weeks, a Kleihauer-Betke test (or flow-cytometric equivalent) can be used to estimate the volume of feto-maternal haemorrhage and guide the need for additional anti-D. This is not usually required in first-trimester miscarriage.
[1]Documentation and follow-up
Record the Rh status, the dose, the site of injection, and the batch number in the notes. Advise the woman to seek the same for any future bleeding in pregnancy. Anti-D is one of the most effective preventive interventions in obstetrics, but it is easily forgotten in the distress of a miscarriage.
[1]Ectopic Pregnancy — the Must-Exclude Differential
A woman with bleeding in early pregnancy is assumed to have a pregnancy of unknown location until a viable intrauterine pregnancy is demonstrated. The most important reason for this rule is to avoid missing an ectopic pregnancy, which is the leading cause of first-trimester maternal death and can present with almost identical symptoms to miscarriage.[1]
Clinical clues that point to ectopic
- Pain is lateral, constant, or radiating to the shoulder tip (from diaphragmatic irritation by intraperitoneal blood), whereas miscarriage pain is usually central and cramping.
- Bleeding is typically dark and scanty, often described as prune-juice spotting.
- Cervical excitation on bimanual examination is a warning sign.
- Syncope, shoulder-tip pain, or haemodynamic collapse suggest rupture and intraperitoneal bleeding.
Ultrasound and hCG interpretation
On transvaginal ultrasound, an ectopic pregnancy classically shows an empty uterus with an adnexal mass or free fluid in the pouch of Douglas. The discriminatory zone is the serum beta-hCG level above which a normal intrauterine pregnancy should be visible on TVS; this is usually quoted as 1,500 to 2,000 IU/L for TVS. If the hCG is above the discriminatory zone and the uterus is empty, suspect ectopic or non-viable pregnancy. If below it, the pregnancy is too early to locate — repeat hCG in 48 hours and rescan.[2]
Serial hCG in suspected ectopic
A healthy intrauterine pregnancy should show a beta-hCG rise of at least 63 percent over 48 hours. An ectopic pregnancy usually rises more slowly or may plateau, while a failing intrauterine pregnancy often falls. A single hCG value is never diagnostic — the trend and the scan together determine management.
[1]Practical rule
Never discharge a woman with bleeding in early pregnancy without either confirming a viable intrauterine pregnancy on scan or arranging a clear follow-up plan with serial hCG and repeat imaging.
[1]Specific Subtypes & Scenarios
Cervical insufficiency
A distinct and surgically remediable cause of late, painless second-trimester loss. The cervix dilates painlessly with bulging or prolapsing membranes in an otherwise well woman, without the contractions of labour. Risk factors are congenital (collagen disorders such as Ehlers-Danlos), traumatic (cone biopsy, LEEP, previous dilatation, obstetric tears), iatrogenic (repeated evacuations), and DES exposure in utero. Diagnosis is clinical (a history of painless mid-trimester loss) and increasingly ultrasound-based (a cervical length under 25 mm). Management is cerclage — a suture placed around the cervix to keep it closed. Three flavours:
[1]- History-indicated cerclage at 12 to 14 weeks for women with 3 or more previous second-trimester losses or preterm births.
- Ultrasound-indicated cerclage (rescue) when serial scans show a short cervix under 25 mm before 24 weeks.
- Transabdominal cerclage for women in whom a vaginal suture has failed or is not anatomically possible, placed before conception or in early pregnancy.
Cerclage is contraindicated in active infection, active labour, ruptured membranes, or heavy bleeding. The Cervical Insufficiency topic covers this in depth.
[1]Molar pregnancy (gestational trophoblastic disease)
A must-not-miss mimic and a true neoplastic process. Molar pregnancy is a form of gestational trophoblastic disease caused by abnormal fertilisation. It can mimic miscarriage because it presents with bleeding and is diagnosed on ultrasound in early pregnancy.[2]
Genetics and classification
- Complete mole: Usually 46,XX or 46,XY with all paternal chromosomes (diandric diploidy). There is no fetal tissue, and the risk of persistent trophoblastic disease is around 15 to 20 percent in Western series and higher in some Asian populations.
- Partial mole: Usually triploid (69 chromosomes) with two paternal and one maternal set. A fetus or fetal parts may be present, often with growth restriction and congenital anomalies. The risk of persistent trophoblastic disease is lower, about 1 to 5 percent.
Presentation and diagnosis
The classic presentation is heavy first-trimester bleeding with passage of vesicles (grape-like tissue), a uterus large for dates, and very high hCG. Women may have severe hyperemesis, early pre-eclampsia, or biochemical thyrotoxicosis because hCG has weak thyroid-stimulating activity. On ultrasound, a complete mole shows a heterogeneous intrauterine mass with multiple small cystic spaces classically described as a "snowstorm" or "bunch of grapes". A partial mole may show focal cystic spaces in an enlarged placenta alongside a malformed fetus.[1]
Management
- Suction evacuation is the treatment of choice. Give syntocinon/oxytocin during or after the procedure to reduce bleeding and uterine atony.
- Because the uterus is large and soft and trophoblast is vascular, there is a higher risk of perforation and heavy bleeding; evacuation should be performed by an experienced operator and cross-matched blood should be available.
- Send all tissue for histology; the diagnosis of molar pregnancy changes follow-up completely.
Follow-up
After evacuation, serial serum hCG is mandatory:
[1]- Weekly until hCG is negative on three consecutive occasions.
- Then monthly for six months for a complete mole (and often for a partial mole according to local protocol).
- Reliable contraception is essential during follow-up so that a new pregnancy does not confound hCG interpretation.
A rise or plateau in hCG indicates persistent trophoblastic disease and requires referral to a trophoblastic disease centre for staging and treatment, usually with single-agent methotrexate. Choriocarcinoma is rare but curable when treated early.
[1]Anembryonic gestation (blighted ovum)
A gestational sac with a yolk sac but no embryo — the commonest form of missed miscarriage. It usually reflects an early lethal chromosomal error. Managed as a missed miscarriage with the three options above.
[1]Recurrent pregnancy loss
See the dedicated workup and treatment sections above. The take-home message for exams: APS is the commonest treatable cause and warrants aspirin plus LMWH; everything else is supportive or cause-specific.
[1]Complications & Pitfalls
Miscarriage is usually uncomplicated, but several serious outcomes must be anticipated and prevented.
[1]Haemorrhage and anaemia
Heavy bleeding is most common in incomplete miscarriage when retained tissue prevents the uterus from contracting and the cervix from closing. The key clinical error is to rely on the reported number of pads rather than on haemodynamic signs. Tachycardia and postural dizziness are early warnings; hypotension is late. Resuscitation with crystalloid, cross-matched blood, and urgent evacuation is required for uncontrolled bleeding. After a significant bleed, check the full blood count and start oral iron if the woman is anaemic.
[1]Infection and sepsis
Retained products of conception are a nidus for infection, particularly after unsafe termination or incomplete evacuation. Organisms are usually mixed aerobic and anaerobic, including Escherichia coli, Streptococcus, Staphylococcus, and gram-negative bacilli. Sepsis can progress rapidly from pyrexia and tachycardia to shock, ARDS, and DIC. The principle is antibiotics plus source control: give broad-spectrum IV antibiotics promptly and evacuate the uterus. Delaying evacuation to obtain imaging is unsafe once the diagnosis is clear.
[1]Retained products of conception
On follow-up, a thickened or heterogeneous endometrium with ongoing bleeding suggests retained products. The options are expectant, medical misoprostol, or repeat suction evacuation. The choice depends on symptoms, size of retained tissue, and the woman's preference. Persistent retained products can cause chronic bleeding, anaemia, or infection.
[1]Asherman syndrome
Over-vigorous or repeated curettage can damage the basalis layer of the endometrium, leading to intrauterine adhesions and Asherman syndrome. The woman presents with secondary amenorrhoea, reduced menstrual flow, infertility, or recurrent miscarriage. The risk is reduced by using suction rather than sharp curettage, gentle technique, and cervical priming. Established adhesions are treated by hysteroscopic adhesiolysis, sometimes followed by an intrauterine device or balloon to prevent re-adhesion and oestrogen to promote endometrial regrowth.
[1]Cervical trauma and uterine perforation
Uterine perforation occurs in roughly 1 to 4 per 1,000 surgical evacuations. Risk factors include an inexperienced operator, an unfavourable or undilated cervix, and retroverted uterus. Perforation may be suspected when the instrument passes beyond the expected uterine cavity, or when there is unexpected pain, bleeding, or injury to adjacent bowel or bladder. Small perforations in stable patients can be managed expectantly with antibiotics and observation; larger perforations, bleeding, or organ injury need laparoscopic or laparotomic repair. Cervical priming reduces cervical tearing.
[1]Rh sensitisation
Omitting anti-D immunoglobulin in an Rh-negative woman is a preventable error with lifelong consequences. Sensitisation can cause haemolytic disease of the fetus and newborn in future pregnancies, ranging from mild jaundice to hydrops fetalis and stillbirth. Give 250 IU intramuscularly within 72 hours for any bleeding or miscarriage, and document the administration.[1]
Psychological morbidity
Grief, guilt, anxiety, depression, and post-traumatic stress are common after miscarriage. Many women blame themselves for stress, exercise, diet, or an accidental fall, despite evidence that most losses are chromosomal and non-recurrent. Every miscarriage encounter should include empathic communication, clear explanation, and follow-up counselling. Signposting to peer-support organisations and offering early review in the next pregnancy are valuable parts of care.
[1]The common diagnostic trap
The classic error — and a frequent exam trap — is declaring a pregnancy non-viable on a single borderline scan. The NICE criteria exist precisely to prevent this; when in doubt, repeat the scan at least 7 days later.[2]
Prognosis & Disposition
After a single miscarriage the chance of a successful next pregnancy is over 85 percent, and even after three consecutive losses roughly 55 to 75 percent of women have a live birth with supportive care alone. Prognosis worsens with advancing maternal age, an increasing number of prior losses, and the presence of a chromosomal translocation or untreated APS. Treated APS (aspirin plus LMWH) roughly doubles the live-birth rate compared with untreated disease. Most women are managed as outpatients; admission is reserved for heavy bleeding, sepsis, significant anaemia, or social or psychological need. A safety-net of easy re-presentation and a follow-up review closes the episode, and pre-conception advice (folic acid 400 microgram daily, optimisation of chronic disease, smoking cessation) sets up the next pregnancy optimally.
[1]Follow-up, pre-conception counselling and the next pregnancy
The care of a woman after miscarriage does not end once the bleeding stops. Structured follow-up improves psychological recovery, ensures complete evacuation, and prepares the woman for the safest possible next pregnancy.
[1]Immediate follow-up
All women should have access to advice or a follow-up appointment within 2 to 3 weeks, or sooner if bleeding is heavy, pain is severe, or fever develops. For women managed expectantly or medically, a follow-up transvaginal ultrasound or serum beta-hCG confirms complete evacuation. A persistent thickened endometrium with ongoing bleeding suggests retained products and may need repeat medical or surgical management. Any tissue passed or evacuated should be sent for histology, and in recurrent loss or suspected molar pregnancy the products should be considered for karyotyping by array comparative genomic hybridisation or QF-PCR.[2]
Pre-conception advice
Before the next pregnancy, review modifiable risks and chronic disease:
[1]- Start folic acid 400 microgram daily (5 mg daily in women with diabetes, obesity, or anticonvulsant use) and continue until at least 12 weeks of gestation.
- Optimise glycaemic control, thyroid function, and blood pressure.
- Stop smoking and reduce alcohol; limit caffeine to under 200 mg/day (roughly two cups of coffee).
- Aim for a healthy BMI, because obesity is associated with both miscarriage and later pregnancy complications.
- Review medications — stop warfarin, retinoids, and other teratogens; switch to safer alternatives before conception.[1]
Supportive care in the next pregnancy
For women with recurrent or unexplained loss, the next pregnancy is often an anxious time. Early viability scanning at 6 to 7 weeks provides reassurance and allows prompt intervention if APS is diagnosed. For women with APS, start aspirin at conception and add LMWH once a viable intrauterine pregnancy is confirmed. For women with a history of loss and first-trimester bleeding, vaginal progesterone 400 mg twice daily may be offered until 16 weeks, based on the PRISM trial subgroup findings.[4]
Psychological support
Many women need more than a clinical review. Grief, anxiety, and guilt are common, and a significant minority develop depression or post-traumatic stress. Offer empathic listening, clear explanations of why the loss occurred, and information about support organisations. A follow-up appointment specifically to discuss grief and future fertility is often appreciated. Partners also grieve and should be included when appropriate.
[1]When to refer
Referral to a dedicated early pregnancy assessment unit or recurrent miscarriage clinic is appropriate for women with heavy or unusual bleeding, suspected ectopic or molar pregnancy, recurrent loss, or significant psychological distress. In RPL clinics, a multidisciplinary team of obstetricians, haematologists, endocrinologists, and counsellors can deliver coordinated care. Women with two consecutive second-trimester losses, or a second-trimester loss with a suspicious history of cervical insufficiency, should also be referred for consideration of cervical cerclage. Early referral and a planned pregnancy package improve outcomes and reduce anxiety.
[1]Special Populations
- Recurrent pregnancy loss — full structured workup after 2 to 3 losses; APS is the most important treatable cause; even unexplained RPL has a good prognosis.
- Advanced maternal age — counsel on age-related aneuploidy risk; offer non-invasive prenatal testing or PGT-A within IVF where appropriate; set realistic expectations.
- After IVF — higher early-loss rate and greater emotional investment; offer an early scan, psychological support, and PGT for translocation carriers.
- Rh-negative women — anti-D within 72 hours for every sensitising event (bleeding or miscarriage), including first-trimester bleeding under current guidance.
- Women on anticoagulation — coordinate with haematology; switch warfarin to LMWH pre-conception or at a positive test (warfarin is teratogenic).
- Women with diabetes — optimise glycaemic control pre-conception (HbA1c in target) to reduce aneuploidy-independent loss; folic acid 5 mg daily.[1]
Evidence, Guidelines & Regional Differences
[1]WHO identifies unsafe abortion-related septic miscarriage as a leading, preventable cause of maternal mortality in settings where safe termination services are restricted. Access to safe medical and surgical management, anti-D, and post-miscarriage contraception is a global reproductive-health priority.
Landmark trials
- MifeMiso trial (Chu et al., Lancet 2020, PMID 32853559): a randomised, double-blind, placebo-controlled trial of 711 women with missed miscarriage in the UK. Mifepristone 200 mg orally followed by misoprostol completed miscarriage within seven days in approximately 83 percent of women versus 76 percent with misoprostol alone, and reduced the need for surgical intervention. This changed UK and many international guidelines.[3]
- PRISM trial (Coomarasamy et al., N Engl J Med 2019, PMID 31067371): 4,153 women with early pregnancy bleeding were randomised to vaginal progesterone 400 mg twice daily or placebo until 16 weeks. Overall, progesterone did not significantly increase live birth, but a pre-specified subgroup analysis showed a substantial benefit in women with a history of three or more previous miscarriages and first-trimester bleeding. Progesterone is therefore offered in selected cases.[4]
- ALIFE2 trial (Quenby et al., Lancet 2023, PMID 37271152): randomised women with recurrent miscarriage and confirmed inherited thrombophilia to LMWH or standard care. The trial showed no improvement in live-birth rate with LMWH, leading to a recommendation against routine heparin for inherited thrombophilia in recurrent loss. This does not apply to antiphospholipid syndrome, where aspirin plus LMWH remains the standard of care.[5]
- APS laboratory criteria: persistent lupus anticoagulant, moderate-to-high-titre anticardiolipin IgG/IgM, or anti-beta-2-glycoprotein-I on two occasions at least 12 weeks apart, as defined by the Sydney classification criteria. This is the basis for the diagnosis and treatment of APS-related recurrent miscarriage.[1]
Exam Pearls
The classification hinge — read the cervical os
CLOSE
Threatened miscarriage — reassure
Missed miscarriage
Inevitable or incomplete — products passing, manage actively
Infection — IV antibiotics plus urgent evacuation
Complete miscarriage
RPL workup — the causes to test for
CRAMP
Parental karyotype for balanced translocation
APS — lupus anticoagulant, anticardiolipin, anti-beta-2-GP-I (the key treatable cause)
Uterine septum on 3D ultrasound or hysteroscopy
TSH, HbA1c — thyroid disease and diabetes
Inherited thrombophilia screen
The one-liners examiners reward:
[1]- "Miscarriage equals loss before 24 weeks; about 1 in 5; chromosomal abnormality is the single commonest cause (over 50 percent)."
- "The cervical os decides the type: closed and viable equals threatened; open equals inevitable or incomplete; closed and retained equals missed; infection equals septic."
- "CRL at least 7 mm with no heartbeat; MSD at least 25 mm with no embryo — and repeat the scan to avoid a false positive."
- "Beta-hCG rising less than 63 percent in 48 hours equals non-viable or ectopic."
- "RPL equals 3 or more consecutive losses; the commonest treatable cause is antiphospholipid syndrome — aspirin 75 mg plus LMWH."
- "Anti-D 250 IU IM within 72 hours to every Rh-negative woman with bleeding or miscarriage."
- "After one miscarriage, the chance of success next time is over 85 percent — reassure."
- "Anembryonic sac with no embryo equals blighted ovum."
- "Septic miscarriage: IV antibiotics plus urgent evacuation — never forget retained products and an unsafe-procedure history."
- "Cervical insufficiency: painless second-trimester dilation with bulging membranes — consider cerclage if viable."
- "Complete mole has no fetus and is androgenetic; partial mole is triploid with a fetus."
- "Molar pregnancy follow-up is serial hCG to detect persistent trophoblastic disease."[1]
References
- [1]Deng T, Liao X, Zhu S. Recent Advances in Treatment of Recurrent Spontaneous Abortion. Obstetrical and Gynecological Survey, 2022.PMID 35672876
- [2]Jeve YB, Davies W. Evidence-based management of recurrent miscarriages. Journal of Human Reproductive Sciences, 2014.PMID 25395740
- [3]Chu JJ, Devall AJ, Beeson LE, et al. Mifepristone and misoprostol versus misoprostol alone for the management of missed miscarriage (MifeMiso): a randomised, double-blind, placebo-controlled trial. The Lancet, 2020.PMID 32853559
- [4]Coomarasamy A, Devall AJ, Cheed V, et al. A Randomized Trial of Progesterone in Women with Bleeding in Early Pregnancy. New England Journal of Medicine, 2019.PMID 31067371
- [5]Quenby S, Booth K, Hiller L, et al. Heparin for women with recurrent miscarriage and inherited thrombophilia (ALIFE2): an international open-label, randomised controlled trial. The Lancet, 2023.PMID 37271152