Obstetrics & Gynaecology · Obstetrics & Gynaecology
Postpartum Haemorrhage
Also known as PPH · Obstetric haemorrhage · Primary PPH · Secondary PPH · Major PPH
Postpartum haemorrhage (PPH) = blood loss over 500 mL (vaginal) or over 1000 mL (caesarean) within 24 h (primary); major PPH is over 1000 mL or any loss with shock. Secondary PPH = 24 h to 12 weeks postpartum. 4 Ts: Tone (atony 70%), Trauma (20%), Tissue (9%), Thrombin (1%). Resuscitate and treat the cause in parallel. Uterotonic ladder: oxytocin, ergometrine (avoid hypertension), carboprost (avoid asthma), misoprostol, then tranexamic acid 1 g IV (WOMAN). Mechanical/surgical: Bakri balloon, B-Lynch suture, internal iliac ligation, hysterectomy (last resort).
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags

Overview & Definition
Obstetric haemorrhage remains the single largest direct cause of maternal death worldwide, killing more than 80,000 women every year, the overwhelming majority in low- and middle-income settings where access to skilled birth attendance, blood and surgical theatres is limited.[1] Within this category, postpartum haemorrhage (PPH) — bleeding from the genital tract after delivery — is the dominant event, and it is one of the few emergencies in medicine where a previously well young woman can die within an hour of delivery if the response is slow or disorganised. The physiological reserve of pregnancy (a 40% expansion of blood volume to roughly 5–6 L and a hyperdynamic circulation) means that tachycardia and hypotension are late signs; by the time the blood pressure falls, a woman may already have lost more than a quarter of her circulating volume. The clinical art of PPH is therefore to act on blood loss and signs before the body decompensates, and to run resuscitation and definitive treatment in parallel rather than in sequence.
Primary PPH is excessive bleeding from the genital tract occurring within 24 hours of delivery (the "third" and "fourth" stage of labour). The most widely taught volume thresholds are over 500 mL after vaginal delivery and over 1000 mL after caesarean section. [1] Major (severe) PPH is defined as blood loss over 1000 mL or any blood loss accompanied by signs of haemodynamic instability (tachycardia, hypotension, pallor, altered consciousness), because in practice a woman with significant haemodynamic compromise requires the full PPH response regardless of the millilitres measured. Minor PPH is 500–1000 mL without shock.
WHO definition: the World Health Organization classifies PPH as blood loss of 500 mL or more within 24 h of birth, and severe PPH as loss of 1000 mL or more; visual estimation is used where quantitative measurement is not feasible.[1] RCOG (UK) similarly defines primary PPH as 500 mL (vaginal) or 1000 mL (caesarean) within 24 h, and recommends reclassifying any loss as major (1000–2000 mL) or severe (over 2000 mL) for triggering escalation.[8] ACOG (US) has moved toward a quantitative, cumulative blood-loss approach using calibrated drapes, given the systematic under-estimation of visual loss. Across all three guidelines the action threshold — activate the PPH protocol — is effectively any blood loss that makes the clinician worried, plus the formal 500 mL / 1000 mL cut-offs.
Secondary PPH (also called late or delayed PPH) is abnormal or excessive bleeding occurring from 24 hours up to 12 weeks postpartum. It is far less dramatic than primary PPH but is an important cause of readmission; the typical causes are retained products of conception, puerperal endometritis, and subinvolution of the placental bed, with rare but serious contributors such as uterine arteriovenous malformation or choriocarcinoma.[1]
PPH is further graded by severity to drive the level of response. A useful operational framework taught in obstetric emergency courses (ALARM/ MOET / ALSO) is that blood loss plus physiology, not volume alone, should declare the emergency: a 500 mL loss in a woman who started the pregnancy anaemic with a haemoglobin of 70 g/L is potentially catastrophic, while the same loss in a healthy multipara may be trivial. [8]
PPH — headline numbers
Classification — the 4 Ts
The causes of PPH are organised into the 4 Ts, a mnemonic that doubles as a bedside checklist because the first action after resuscitation is to identify which "T" is bleeding.[1][4]
Tone (70%)
uterine atony
- **Most common cause** — uterus fails to contract
- Spiral arteries stay open → continued bleeding
- Risk: overdistension (twins, macrosomia, polyhydramnios), prolonged labour, multiparity, uterine muscle exhaustion
- Sign: **boggy, soft fundus**
- Management: **uterotonic ladder** (oxytocin → ergometrine → carboprost → misoprostol)
Trauma (20%)
lacerations
- Cervical, vaginal or perineal tears
- Episiotomy site bleeding, uterine rupture, inverted uterus
- Risk: instrumental delivery (forceps/vacuum), prolonged/rapid labour, large baby, episiotomy
- Sign: **firm contracted uterus** but ongoing bleeding
- Management: **inspect, identify, repair** under anaesthesia in theatre
Tissue (9%)
retained products
- Retained placenta or membrane fragments
- Abnormal placentation — placenta accreta/increta/percreta
- Sign: **firm uterus**, placenta incomplete on inspection
- Management: **explore uterus, remove retained tissue** under anaesthesia ± ultrasound
Thrombin (1%)
coagulopathy
- Pre-existing: von Willebrand disease, thrombocytopenia, on anticoagulants
- Acquired: **DIC** (abruption, pre-eclampsia/HELLP, sepsis, retained dead fetus, amniotic fluid embolism)
- Sign: **oozing from puncture sites + IV lines**, persistent bleeding despite firm uterus and no trauma
- Management: **correct the clot** — FFP, cryoprecipitate, platelets per massive transfusion protocol
The percentages are a teaching heuristic rather than a precise audit — cohort studies show atony accounts for 60–80%, trauma 15–25%, tissue 5–10%, and thrombin around 1% (often under-recognised until laboratory clotting returns).[4] More than one T may operate simultaneously: a woman with severe pre-eclampsia who delivers by emergency caesarean can have atony (from a overdistended, magnesium-relaxed uterus), surgical bleeding from the hysterotomy (trauma), and evolving DIC (thrombin) all at once.
Epidemiology & Risk Factors
PPH complicates roughly 5% of all deliveries for the 500 mL threshold, with major PPH (over 1000 mL) in 1–3%, and life-threatening PPH (over 2500 mL or requiring transfusion of 5 or more units) in approximately 0.5%.[1] The incidence has risen over the last two decades in high-income countries, partly attributable to the increase in caesarean delivery rates, older maternal age, multiple pregnancies following assisted reproduction, rising maternal obesity, and greater use of anticoagulants. Despite this rise, case fatality has fallen where systems are strong, reflecting better drills, rapid-response teams and protocolised transfusion.
Risk factors should be identified at booking and again on admission in labour, because 40% of PPH occurs in women with an identifiable antenatal risk factor and a further group are identifiable intrapartum — but a clinically important fraction (around 20%) occur in women with no risk factor at all, which is why every birth attendant must be drilled in the response.[1][4]
Antenatal
identifiable at booking
- **Previous PPH** (most predictive — recurrence risk up to 10–15%)
- Previous retained placenta / manual removal
- Multiparity (grand multipara, para 5 or more)
- Multiple pregnancy, polyhydramnios, macrosomia
- Abnormal placentation (praevia, accreta) — especially with previous caesarean
- Pre-existing coagulopathy, von Willebrand disease, thrombocytopenia, anticoagulants
- Anaemia (low reserve for blood loss)
Intrapartum
identifiable in labour
- **Prolonged labour** (especially prolonged 2nd stage)
- **Prolonged 3rd stage** (over 30 min)
- Operative vaginal delivery (forceps, vacuum)
- Emergency caesarean in labour
- Precipitate labour (tissues torn before they can adapt)
- Chorioamnionitis, prolonged rupture of membranes
- Magnesium sulphate therapy (smooth-muscle relaxation)
- Oxytocin use in labour (receptor down-regulation)
Under-recognised
easily missed
- **Obesity** (BMI over 35) — masks fundal palpation and trauma
- **Maternal age over 35**
- Asian and Black ethnicity (independent risk factor)
- Large baby over 4 kg
- Induction of labour
- General anaesthesia (volatile agents relax the uterus)
India and low-resource settings: PPH is the leading direct cause of maternal mortality, responsible for an estimated 25–30% of maternal deaths in India (and over a quarter across much of sub-Saharan Africa and South Asia).[1] The drivers are structural: widespread maternal anaemia (so a 500 mL loss tips a woman into shock), a high rate of home deliveries without skilled birth attendants, delays in transfer to facilities that can provide blood and surgery, and limited blood-bank access. Misoprostol 600 µg oral/sublingual is WHO-recommended for community-based third-stage prophylaxis where oxytocin and cold chain are unavailable, because it is heat-stable and can be administered by auxiliary midwives.[1] India's national programmes emphasise institutional delivery (Janani Suraksha Yojana), misoprostol for home birth, and referral nets, but the single highest-yield intervention remains universal active management of the third stage with oxytocin.
Pathophysiology
Normal postpartum haemostasis depends on a myometrial mechanism unique to pregnancy. The uterus is supplied by the uterine and ovarian arteries, whose terminal branches — the spiral (coiled) arteries of the endometrium — course through and are surrounded by the interlacing oblique myometrial fibres. When the placenta separates, these spiral arteries are sheared open; the only way they are closed is by myometrial contraction physically compressing them. The classical description, taught for over a century, is that the myometrium acts as "living ligatures" — the muscle fibres are the tourniquet. No clot, however strong, will hold against an open spiral artery if the uterus around it is flaccid. This is why uterine atony is the dominant cause of PPH, and why the entire uterotonic armamentarium is built to make the muscle contract. [4]
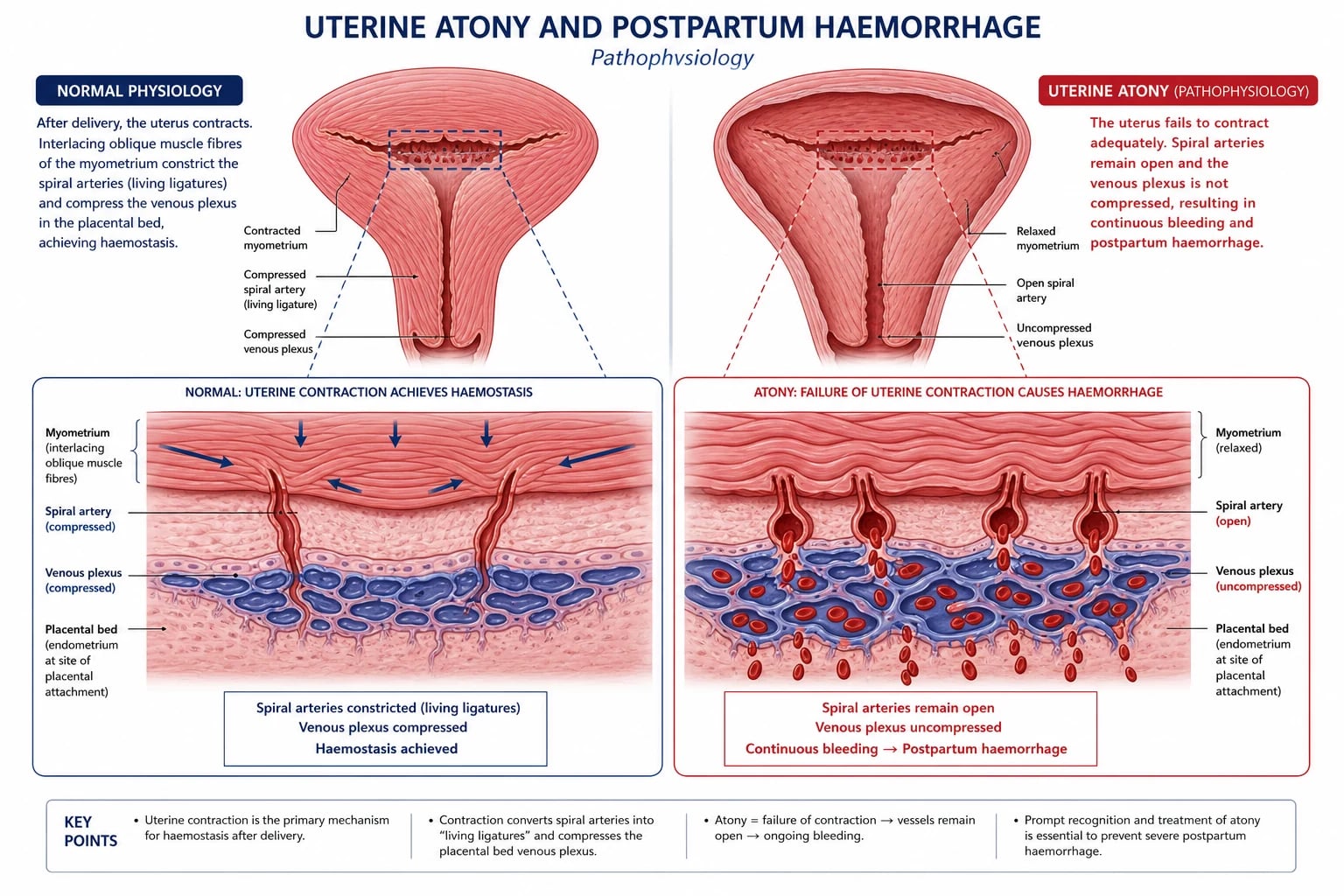
The three pillars of physiological third-stage haemostasis are therefore: (1) a strong myometrial contraction, (2) a competent clotting system, and (3) a complete, empty uterus. Each pillar maps to a "T": failure of contraction is Tone, retained placental tissue that prevents retraction is Tissue, and a failure of clotting is Thrombin. Trauma (the second T) bypasses all three by physically tearing vessels that muscle and clot cannot reach. [4]
Why atony happens. The myometrium becomes exhausted or relaxes when it is overstretched (twins, macrosomia, polyhydramnios), exhausted (prolonged labour, chorioamnionitis), structurally abnormal (fibroids, congenital anomaly), pharmacologically relaxed (magnesium sulphate, volatile anaesthetics, nifedipine, nitroglycerin, prolonged oxytocin with receptor down-regulation) or anatomically unable to contract around a retained placenta. Once the uterus fills with blood it becomes further distended and further atonic — a vicious cycle that the bimanual "rub up the fundus" is designed to break. [4]
Coagulopathy and DIC. Pregnancy is a prothrombotic state (increased fibrinogen to 4–6 g/L, factors VII, VIII, IX, X, XII and von Willebrand factor all rise; protein S falls). The normal pregnant fibrinogen of around 5 g/L is a key defence against bleeding, which is why a fibrinogen below 2 g/L during active PPH is both diagnostic of hypofibrinogenaemia and predictive of progression to severe PPH.[4] DIC in obstetrics is almost always secondary — to placental abruption (releases trophoblastic tissue factor), pre-eclampsia/HELLP, intrauterine fetal death retained for weeks, amniotic fluid embolism, sepsis, or massive haemorrhage itself (consumption + dilution). The laboratory signature is low fibrinogen, prolonged PT/APTT, low platelets, and high D-dimer; clinically it presents as oozing from IV cannula sites, gums and the surgical field.
The fibrinolytic balance and why tranexamic acid works. Clot formation is only half the haemostatic story; the other half is whether the clot is allowed to persist. Plasminogen is converted to plasmin, which digests fibrin (fibrinolysis) and dissolves the clot. In the hyper-fibrinolytic state that accompanies massive obstetric bleeding, clots are lysed almost as fast as they form — particularly in the richly plasminogen-activator-rich placental bed. Tranexamic acid is a lysine analogue that blocks the binding of plasminogen to fibrin, preventing its activation to plasmin and thereby stabilising the clot. This is the mechanistic rationale for the WOMAN trial finding that early TXA reduces death from bleeding.[2] The drug is most effective when the fibrinolytic system is most active — the first hour — which is why timing matters more than dose tuning.
The lethal triad of massive haemorrhage. Sustained blood loss drives three interlocking derangements that each worsen the others: hypothermia (heat lost with shed blood and cold crystalloid), acidosis (poor perfusion → lactate), and coagulopathy (consumption, dilution with crystalloid, and hypothermia-driven platelet and clotting-factor dysfunction). Once the triad is established, clotting fails and bleeding accelerates independent of the original cause — which is why warmed fluids, early blood product replacement in a balanced ratio, and rapid source control are non-negotiable in major PPH.[4]
Shock physiology in PPH. Pregnancy physiology masks early blood loss. Blood volume rises by ~40% by term; cardiac output rises by 30–50%; heart rate is mildly fast at baseline. Class I shock (under 15% loss, up to ~750 mL) is asymptomatic. Class II (15–25%, 750–1500 mL) shows narrowed pulse pressure, mild tachycardia, anxiety — the PPH danger zone. Class III (25–35%, 1500–2000 mL) shows obvious hypotension, tachycardia 110–130, confusion, oliguria. Class IV (over 35%, over 2000 mL) shows lethargy, profound hypotension, cold mottled skin. The trap: the young pregnant myocardium compensates remarkably, so a "normal" blood pressure can hide a 1.5 L loss. Falling blood pressure in PPH is a late, dangerous sign. [4]
Clinical Presentation
PPH is a clinical diagnosis made at the bedside — there is no test that should delay the call for help. The classical presentation is sudden heavy vaginal bleeding after delivery, but three caveats dominate exam stems and real life.[1]
First, visible loss underestimates true loss by 30–50% with visual estimation; blood is soaked into drapes, sheets, the chux pad, and pooling behind the mother. Calibrated drape bags (the E-MOTIVE approach) and weighing swabs correct this.[3] Second, bleeding may be concealed — retained behind a closed cervix or in a distended, atonic uterus, with only a trickle visible externally while litres accumulate internally. Third, shock is out of proportion to visible loss: a 500 mL external loss may accompany a further 1.5 L concealed.
Recognising the depth of shock is what drives the speed and scale of the response. The standard ATLS-style haemorrhagic shock classes translate to a term pregnant woman (blood volume ~5 L) as below — but the cardinal point is that class I and II are the PPH danger zone: a woman who is mildly tachycardic with a narrowed pulse pressure is already in class II and needs the full protocol, not "observation".[1]
Class I
under 15% loss (up to ~750 mL)
- Asymptomatic
- Slight tachycardia (under 100)
- Normal blood pressure and pulse pressure
- **Action:** resuscitate, identify cause, monitor closely
Class II
15-25% loss (~750-1500 mL)
- Tachycardia 100-120
- **Narrowed pulse pressure** (diastolic rises with catecholamines)
- Anxiety, mild pallor, cool peripheries
- **Action:** full PPH protocol — this is the silent danger zone
Class III
25-35% loss (~1500-2000 mL)
- Obvious **hypotension**, tachycardia 110-130
- Confusion, oliguria, marked pallor
- Tachypnoea (air-hunger)
- **Action:** activate massive transfusion, escalate to theatre
Class IV
over 35% loss (over 2000 mL)
- Profound hypotension, tachycardia over 130 or bradycardia (pre-terminal)
- Lethargy, cold mottled skin, anuria
- Imminent cardiac arrest
- **Action:** crash call, perimortem caesarean if arrest, massive transfusion, definitive surgery
Atypical and deceptive presentations examiners test deliberately. The grand multipara with concealed intrauterine bleeding who looks deceptively well. The woman on therapeutic low-molecular-weight heparin who oozes from every puncture site. The caesarean section where bleeding is intra-abdominal (broad ligament haematoma) and the only clue is falling haemoglobin and rising girth. The amniotic fluid embolism presenting as sudden cardiovascular collapse and DIC in the immediate postpartum period. The uterine inversion causing shock disproportionate to bleeding, with a fleshy mass at the cervix/vagina. [4]
Differential Diagnosis
In practice the differential is the 4 Ts, because the bleeding source is almost always within the genital tract. But the discriminators — what distinguishes each T at the bedside — are what the examiner is testing. Three or more should be reproduced with their distinguishing feature.[4]
Uterine atony
Tone
- **Soft, boggy fundus**, easily indented
- Bleeding is dark red, steady, gushing on palpation
- Massaging the fundus firms the uterus and temporarily slows bleeding
- Risk: overdistension, prolonged labour, magnesium
Genital tract trauma
Trauma
- **Firm, well-contracted uterus**
- Bleeding is **bright red**, may be spurting; site identified on speculum exam
- Pain or a vaginal/perineal haematoma; vaginal tear visible
- Risk: instrumental delivery, prolonged 2nd stage, episiotomy
Retained tissue
Tissue
- **Placenta incomplete or undelivered**
- Firm uterus but bleeding continues; lobulated tissue may be felt at the cervix
- Ultrasound shows retained products of conception
- Risk: previous retained placenta, accreta, praevia
Coagulopathy
Thrombin
- **Firm uterus, no trauma, no tissue** but persistent oozing
- Bleeding from IV sites, gums, episiotomy — generalised
- Abnormal clotting studies, low fibrinogen
- Risk: abruption, pre-eclampsia, HELLP, amniotic fluid embolism, sepsis, anticoagulants, vWD
Uterine rupture
surgical emergency
- Sudden cessation of labour pains, fetal distress
- **Loss of fetal station** (head re-ascends); palpable fetal parts abdominally
- Persistent shock with mild or moderate external bleeding (concealed)
- Risk: previous caesarean scar, prolonged labour, oxytocin
Uterine inversion
rare but missed
- **Shock disproportionate** to bleeding
- Fleshy mass at the cervix/vagina; fundus not palpable abdominally
- Severe lower abdominal/lumbar pain, cord may lengthen
- Risk: excessive cord traction on an atonic uterus (mismanaged 3rd stage)
The cannot-miss mimics are amniotic fluid embolism (sudden collapse, hypoxia, DIC — an anaesthetic, not obstetric, bleed in origin) and uterine rupture in the scarred uterus; both need an immediate surgical/anaesthetic response. [4]
Clinical & Bedside Assessment
The first assessment is simultaneous with resuscitation and takes less than two minutes. The team leader performs a focused examination while another team member secures the airway, two large-bore cannulae and oxygen. [8]
The first 2 minutes — simultaneous resuscitation and diagnosis
Massage the fundus (bimanual compression, rub up the fundus) and assess tone — firm or boggy?
Inspect the placenta — complete? Missing cotyledons? Vessels running off the edge (succenturiate lobe)?
Inspect perineum, vagina and cervix under good light for tears; check episiotomy site
Ensure the bladder is empty (catheterise) — a full bladder displaces and atones the uterus
Check clotting — send FBC, clotting, fibrinogen, group & save; crossmatch 4–6 units
Palpate for uterine inversion (fundus absent abdominally) and abdominal rigidity (rupture)
Named signs and manoeuvres. Bimanual uterine compression (the "rub up the fundus"): one hand massages the fundus abdominally through the abdominal wall while the other fist is placed in the anterior fornix (or the whole hand in the vagina) compressing the lower segment against the body of the uterus — both stimulates contraction and directly tamponades the uterine vessels. Hydrostatic balloon tamponade (Bakri) tests the cavity and treats atony. The "4 Ts" rapid screen (fundus, placenta, perineum/cervix, clotting) is the bedside analogue of the diagnostic framework. Visual loss estimation is now supplemented by calibrated drape collection (E-MOTIVE), which detected PPH earlier and reduced severe PPH by 60% in the cluster-randomised trial.[3]
Quantifying loss. The E-MOTIVE trial established that objective blood-loss measurement with a calibrated drape plus a first-response treatment bundle (uterine massage, oxytocin, tranexamic acid, IV fluids, examination) reduces severe PPH from 1.6% to 0.6% — a 60% relative reduction in the primary outcome.[3] This is now WHO-endorsed and is changing practice globally.
Investigations
Do NOT delay treatment for investigations. Treat while drawing blood.[1]
Immediate (bedside)
while resuscitating
- **Group and save** then **crossmatch 4–6 units** (activate massive transfusion protocol)
- **FBC** — haemoglobin and platelets (baseline and trend q15–30 min)
- **Coagulation** — PT/INR, APTT, fibrinogen (target fibrinogen over 2 g/L in active PPH)
- **Kleihauer-Betts** if Rh-negative mother / unsensitised
- ABG/VBG and lactate — assesses shock severity
- U&E, LFT — baseline organ function
Point of care
near-patient
- **ROTEM/TEG** viscoelastic testing where available — guides fibrinogen and platelet/factor replacement in real time
- Haemoglobin point-of-care (HemoCue)
- Bedside glucose (avoid hypoglycaemia in resus)
Imaging
after stabilisation
- **Pelvic ultrasound** — retained products, completion of evacuation, haematoma
- CT pelvis (stable patient) — broad ligament / retroperitoneal haematoma, pseudoaneurysm
- CTA if uterine artery embolisation is planned — localises bleeding vessel
After the event
investigate cause
- Fibrinogen trend, repeat coagulation
- Septic screen if DIC / endometritis
- Debrief and root-cause analysis (each PPH is a critical incident)
The fibrinogen threshold during active PPH is the single most useful laboratory number: a level below 2 g/L predicts progression to severe PPH and is the trigger for cryoprecipitate or fibrinogen concentrate.[4]
Management — Resuscitation
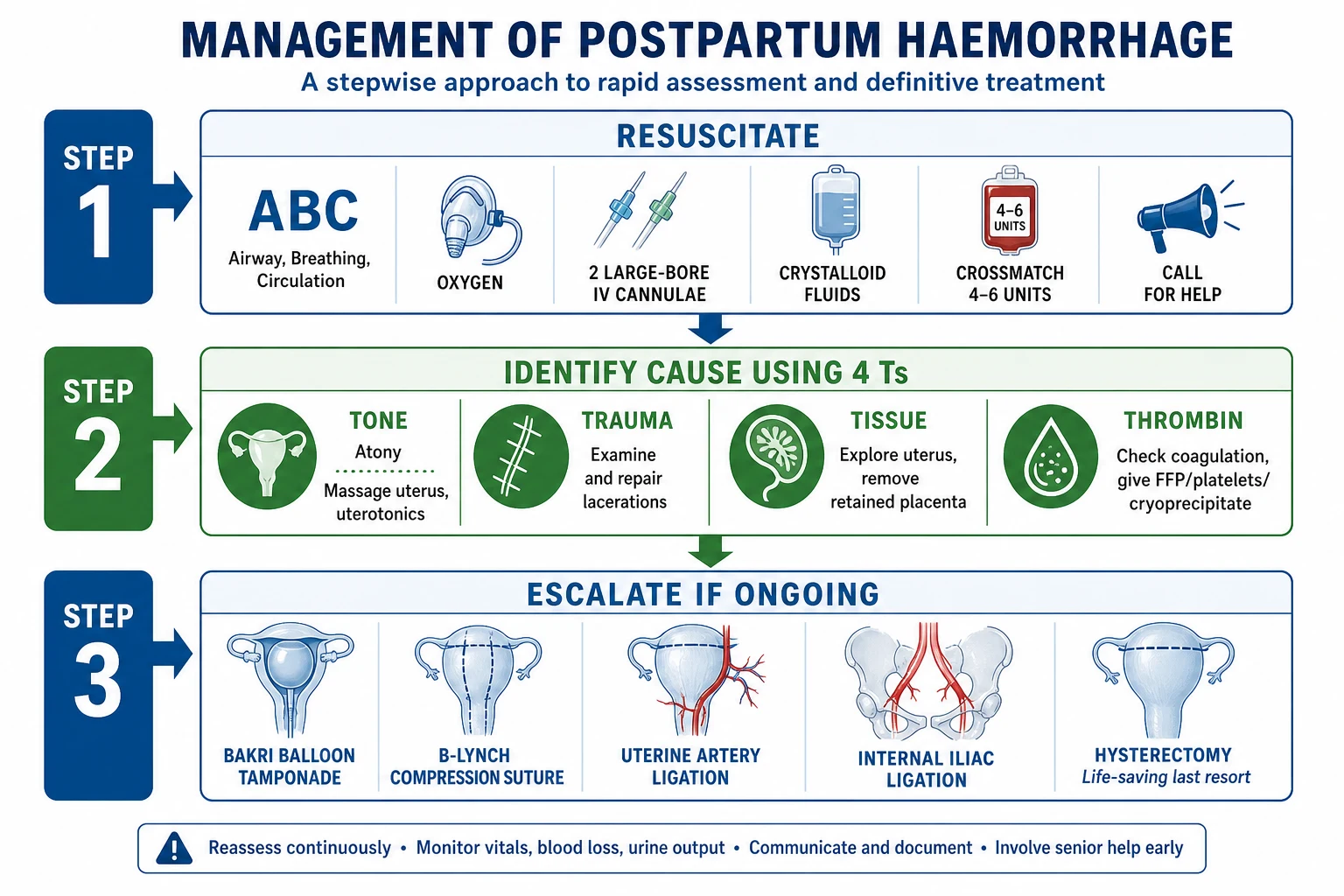
PPH management is a drill, not a thought process. The objective in the first minutes is to buy time — secure the airway, fill the circulation, raise the haematocrit, stop the fibrinolysis — while a second work-stream identifies and treats the cause. These run in parallel, not in series.[1][8]
The PPH resuscitation bundle (run in parallel)
**Call for help** — senior obstetrician, anaesthetist, midwife runner, haematology, theatre. Declare PPH. Assign a team leader and a scribe.
**A — Airway & B — Breathing:** high-flow oxygen 15 L/min via non-rebreather mask; left lateral tilt if antepartum; assess consciousness.
**C — Circulation:** 2 large-bore (14–16 G) IV cannulae; take bloods (FBC, coagulation, fibrinogen, group & save/crossmatch); **crystalloid bolus 1–2 L** warmed Hartmann's or 0.9% saline (20 mL/kg aliquots); insert urinary catheter (output target over 30 mL/h).
**Activate massive transfusion protocol** — target haemoglobin over 70 g/L (over 80 in active bleeding/older); aim for **platelets over 50, fibrinogen over 2 g/L, PT/APTT under 1.5× normal**; transfuse in a balanced ratio (RBC : FFP : platelets approximating 1 : 1 : 1).
**Tranexamic acid 1 g IV over 10 min** within 3 h of onset (WOMAN trial) — give EARLY, do not wait for the cause.<Cite id="2" />
**Warm the patient and the fluids** (forced-air warmer, fluid warmer); hypothermia worsens coagulopathy.
**Identify and treat the cause simultaneously** using the 4 Ts — palpate fundus, inspect placenta, examine perineum/cervix, send clotting.
Tranexamic acid (TXA)
Dose
**1 g IV bolus** within 3 h of PPH onset. Repeat 1 g IV after 30 min if bleeding continues.
Management — Definitive & Stepwise (by the 4 Ts)
Definitive management is cause-specific. The generic rule is to work through the 4 Ts in order, treating whatever you find; most cases declare themselves within the first 5 minutes. [4]
Tone — uterine atony (70%)
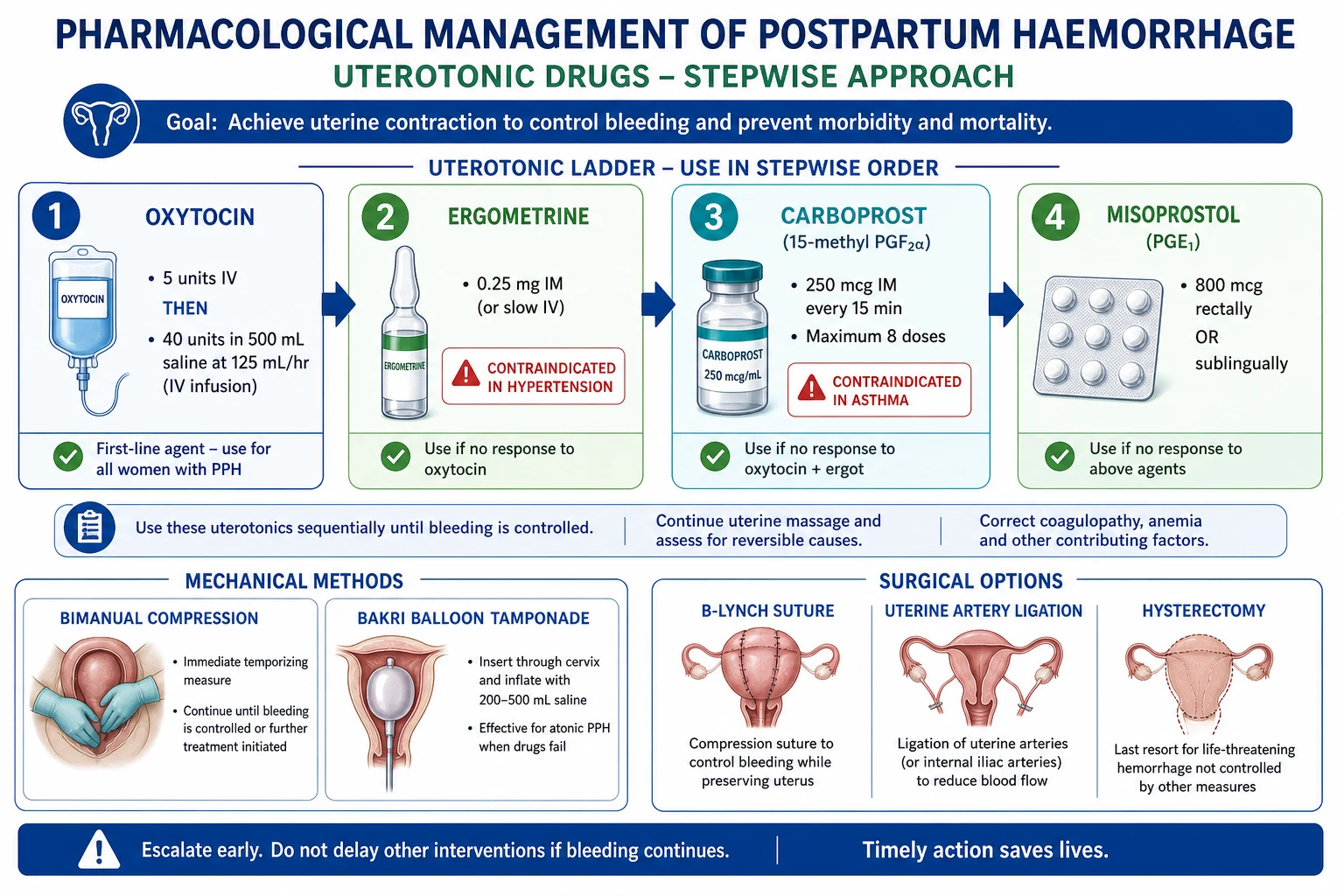
The uterotonic ladder is applied sequentially while continuing resuscitation; each drug has a specific contraindication the examiner will probe.[1][5]
Uterotonic ladder for atonic PPH
**Uterine massage** (bimanual compression, rub up the fundus) — first action, frees the uterus of clots and stimulates contraction.
**Oxytocin** 5 IU slow IV (over 1 min) or 10 IU IM, followed by **infusion 40 IU in 500 mL 0.9% saline at 125 mL/h over 4 h**. (First-line; safe in hypertension and asthma.)
**Ergometrine** 250 µg (0.25 mg) IM or IV (slow). **AVOID in hypertension, pre-eclampsia, eclampsia, cardiac disease** — potent vasoconstrictor that can precipitate hypertensive crisis.
**Carboprost** (15-methyl PGF2α) **250 µg IM every 15 min, maximum 8 doses (2 mg)**. **AVOID in asthma** (bronchoconstrictor — can cause fatal bronchospasm) and contraindicated in active cardiac, pulmonary, renal or hepatic disease.
**Misoprostol** **800 µg rectally or sublingual** (safe in asthma and hypertension; heat-stable; useful in low-resource settings). Repeat once if needed.
**Tranexamic acid 1 g IV** (give EARLY, see above).
If ongoing bleeding → escalate to mechanical and surgical measures (below).
Oxytocin
first-line
- **Dose: 5 IU slow IV over 1 min, or 10 IU IM**; infusion 40 IU in 500 mL saline at 125 mL/h over 4 h
- Acts in 1–3 min (IV)
- **Contraindications: none major** — safe in hypertension, asthma
- Cautions: hypotension if bolused too fast; hyponatraemia if over-infused (antidiuretic effect)
- Side-effects: flushing, nausea, water intoxication with prolonged high-dose
Ergometrine
second-line
- **Dose: 250 µg IM or slow IV**; can repeat at 5 min, max 500 µg (with oxytocin as Syntometrine 500 µg IM)
- Acts in 2–5 min (IM)
- **AVOID: hypertension, pre-eclampsia/eclampsia, cardiac/vascular disease** — powerful vasoconstrictor (sustained uterine + vascular smooth-muscle contraction)
- Side-effects: nausea, vomiting, hypertension, headache, peripheral vasospasm (Raynaud-like)
Carboprost (15-methyl-PGF2α)
third-line
- **Dose: 250 µg deep IM every 15 min, maximum 8 doses (2 mg total)**
- Acts in 5–15 min
- **AVOID: asthma** — bronchoconstrictor, can cause fatal bronchospasm; also avoid in cardiac/pulmonary/renal/hepatic disease
- Side-effects: diarrhoea, vomiting, flushing, fever, bronchospasm, hypertension
Misoprostol (PGE1 analogue)
fourth-line
- **Dose: 800 µg PR or 600 µg SL**; can repeat once after 30 min
- Acts in 10–20 min
- **Safe in asthma and hypertension** — the uterotonic of choice when contraindications limit others
- Heat-stable — key in low-resource and community settings
- Side-effects: shivering (common), pyrexia, diarrhoea
Why oxytocin first? The Cochrane network meta-analyses for both prevention and treatment find oxytocin is the most effective first-line agent with the most favourable safety profile; ergometrine and combination preparations (oxytocin-ergometrine) add efficacy but at the cost of more nausea, vomiting and vasopressor effects.[5][6]
Escalation — mechanical and surgical management of refractory atony
When the uterotonic ladder has been exhausted and the uterus is still atonic, escalation proceeds through a recognised ladder. The objective is to stop the bleeding while preserving the uterus wherever possible — peripartum hysterectomy is a morbidity-dense, fertility-ending last resort. [4]
Mechanical and surgical escalation ladder for refractory atony
**Uterine tamponade — Bakri (hydrostatic) balloon**. Insert into uterine cavity, fill with 250–500 mL warmed saline; provides continuous pressure on the placental bed and the venous plexus. Cheap, fast, uterus-preserving, often definitive. Leave 12–24 h.
**Compression sutures — B-Lynch (brace) suture**. Open laparotomy; place chromic catgut/Vicryl brace sutures that compress the uterus like a corset when tightened. Designed by Christopher B-Lynch (1997). Variants: Cho multiple square, Hayman.
**Uterine artery ligation** (O'Leary). Bilateral ligation of the ascending branch of the uterine artery at the level of the cesarean section incision; reduces pulse pressure to the uterus; uterus usually revascularises from ovarian and vaginal collaterals.
**Internal iliac (hypogastric) artery ligation**. Bilateral; reduces pelvic pulse pressure; requires laparotomy and skilled surgeon; historic mainstay now partly replaced by embolisation.
**Interventional radiology — uterine artery embolisation**. If stable and IR available: gelatin sponge (Gelfoam) particles embolise the uterine arteries; preserves uterus; rebleed possible if vessel recanalises. Not feasible in an unstable patient.
**Peripartum hysterectomy — last resort, life-saving.** Subtotal usually sufficient; proceed if the balloon, sutures and ligation have failed and the woman is exsanguinating. Do NOT delay hysterectomy once the decision is made.
The decision to abandon conservative measures is clinical: a woman in uncontrolled haemorrhage with deranged coagulation who is not responding should move to hysterectomy — the biggest mistake in PPH surgery is delaying the definitive life-saving operation.[4][8]
Trauma (20%)
Traumatic bleeding is surgical. Once the uterus is confirmed firm and the placenta complete, examine the vagina, cervix and perineum under good light, in theatre, with adequate analgesia/anaesthesia. Bleeding points are clipped, ligated and repaired; high vaginal and cervical tears are sutured with absorbable sutures (the upper third of the vagina and cervix may require theatre and an experienced operator). Uterine rupture needs immediate laparotomy and repair (± hysterectomy depending on extent and parity). Uterine inversion must be replaced immediately (Johnson or O'Sullivan manoeuvre — reposition by lifting the uterus through the cervix with the whole hand, often after a uterine relaxant such as terbutaline/nitroglycerin) before giving uterotonics — giving a uterotonic to an inverted uterus traps the inversion. [4]
Tissue (9%)
Examine the placenta meticulously at every delivery: missing cotyledons, torn membranes, and vessels running to the edge (suggesting a succenturiate lobe) all indicate retained tissue. If the placenta is retained beyond 30 minutes, or if retained products are suspected, perform controlled cord traction (with uterotonic); if that fails, manual removal under anaesthesia in theatre with inspection and evacuation of the cavity.[1] In secondary PPH with suspicion of retained products, ultrasound-guided evacuation is the procedure of choice. Abnormal placentation (accreta/increta/percreta) is an increasingly common cause of catastrophic PPH (rising with caesarean rates) and usually needs a planned multidisciplinary approach with conservative surgery, balloon occlusion, or caesarean hysterectomy.
Thrombin (1%)
Coagulopathy is corrected in parallel with the cause and alongside the massive transfusion protocol. Treat the underlying driver (deliver in abruption, manage HELLP, resuscitate sepsis) and replace what is missing:[4]
FFP
factor replacement
- **Dose 10–15 mL/kg** (typically 3–4 units) for PT/APTT over 1.5× normal
- Replaces clotting factors and natural anticoagulants
- Target PT/APTT under 1.5× normal
Cryoprecipitate
fibrinogen
- **Dose 1 pool (5 units, ~10 single-donor units)** when fibrinogen under 2 g/L in active PPH
- Each pool raises fibrinogen by ~1 g/L
- **Target fibrinogen over 2 g/L** (some guidelines over 2.5)
Platelets
platelet count
- **1 adult therapeutic dose** if platelets under 75 × 10⁹/L in active bleeding
- Under 50 × 10⁹/L always transfuse
- Each dose raises count by 20–40 × 10⁹/L
Adjuncts
rescue
- **Vitamin K 10 mg IV** (especially if liver disease / warfarin)
- **Fibrinogen concentrate** (faster, smaller volume than cryo) where available
- **Prothrombin complex concentrate** for warfarin reversal
- **Recombinant factor VIIa** — last-line rescue in refractory PPH, treat the cause first
The widely used massive transfusion protocol delivers blood products in a fixed ratio approximating 1 : 1 : 1 (RBC : FFP : platelets) to avoid the lethal triad of hypothermia, acidosis and dilutional coagulopathy. Viscoelastic testing (ROTEM/TEG) tailors replacement in real time. [4]
Specific Subtypes & Scenarios
Secondary PPH
Bleeding from 24 hours to 12 weeks postpartum. The three classic causes:[1]
Retained products of conception
commonest
- Most frequent cause
- History of incomplete third stage, late bleeding days to weeks postpartum
- Ultrasound shows echogenic material in cavity
- **Management:** ultrasound-guided evacuation, antibiotics, crossmatch
Puerperal endometritis
infection
- Fever, foul lochia, uterine tenderness, raised inflammatory markers
- Risk: prolonged rupture, manual removal, caesarean, retained products
- **Management:** IV broad-spectrum antibiotics (clindamycin + gentamicin ± metronidazole); exclude retained products
Subinvolution of uterus/placental site
delayed contraction
- Failure of the placental site to involute; vessels stay open
- Persistent lochia rubra without infection or retained tissue
- **Management:** course of oral ergometrine or oxytocin ± antibiotics; consider retained products
Rare causes
don't miss
- **Uterine arteriovenous malformation** — pulsatile bleeding, seen on Doppler/CT
- **Choriocarcinoma** — persistent raised β-hCG after delivery; exclude with pregnancy test
- **Retained placental tissue with sepsis** — DIC risk
PPH at caesarean section
Intraoperative blood loss over 1000 mL at caesarean qualifies as PPH. Specific causes include the uterine incision extending into the broad ligament or uterine artery, placenta praevia/accreta (catastrophic bleeding — anticipate and plan), and atony. Have oxytocin running on delivery of the baby, inspect the angles of the hysterotomy, and apply immediate bimanual compression; Balloon tamponade and B-Lynch suture can be placed at the time of laparotomy.[8]
PPH with placenta accreta spectrum
With rising caesarean rates, placenta accreta/increta/percreta is the modern obstetric emergency. Risk: previous caesarean + placenta praevia (risk up to 3% after one, over 60% after four scars). Diagnose antenatally on ultrasound/MRI; plan delivery at 34–36 weeks in a centre of excellence with multidisciplinary input, cell salvage, interventional radiology (prophylactic internal iliac balloon), and consent for caesarean hysterectomy. [4]
Complications & Pitfalls
PPH carries the full morbidity of massive haemorrhage plus several obstetric-specific complications.[1]
- Haemorrhagic shock and death — the endpoint if untreated; maternal death from PPH is a sentinel event. [1]
- Sheehan syndrome — anterior pituitary infarction following profound hypovolaemic shock during PPH (the pituitary is uniquely vulnerable in pregnancy due to a low-flow portal system in an enlarged, vascular gland). Presents as failure to lactate (low prolactin — the earliest sign), then amenorrhoea (low FSH/LH), hypothyroidism (low TSH — fatigue, cold intolerance), and adrenal insufficiency (low ACTH — fatigue, hypotension, hypoglycaemia). Requires lifelong hormone replacement. Now rare in high-resource settings but still seen where PPH is late-resuscitated.
- Acute kidney injury — from prolonged hypotension (acute tubular necrosis); usually reversible but cortical necrosis can occur.
- DIC and coagulopathy — consumption + dilution; worsens the bleeding cycle.
- Transfusion-related harm — TRALI, TACO, transfusion-transmitted infection, alloimmunisation.
- Surgical morbidity — peripartum hysterectomy (infertility), bladder/ureteric injury during ligation/hysterectomy, internal iliac artery ligation rarely causes lower-limb ischaemia.
- Psychological morbidity — PTSD, birth trauma, postnatal depression; ICU admission is itself a risk.
- Recurrence — 10–15% recurrence in next pregnancy; flag for future care.
Prognosis & Disposition
With prompt, protocolised management, the vast majority of women recover fully and leave hospital in 2–4 days. Prognosis is determined by the cause (atony responds to uterotonics; accreta is life-threatening), the time to control (death is a function of uncontrolled haemorrhage time), the reserve of the mother (anaemia, pre-existing disease worsen outcome) and the system (blood and theatre availability). [4]
Disposition: after major PPH, monitor on HDU/ICU for 12–24 h (continued bleeding, coagulopathy, fluid balance, renal function, signs of DIC). Iron replacement (oral or IV ferric carboxymaltose) for postpartum anaemia. Counsel about recurrence and the need for active management of the third stage in future pregnancies, with senior input and crossmatched blood available. Critical-incident review and debrief of every major PPH is mandatory (national maternal death/morbidity surveillance standards). [1]
Special Populations
Jehovah's Witnesses refuse transfusion of major blood components on religious grounds, and the obstetric team must plan for this antenatally, not in a crisis. The acceptable tools are cell salvage (with a continuous circuit, which many Witnesses accept as long as the blood remains in continuity with the body), tranexamic acid, oxytocin, iron and erythropoietin optimisation in the third trimester, and minimising phlebotomy. Document the woman's specific choices in a signed advance directive; arrange multidisciplinary counselling; and accept that mortality from major PPH is markedly higher in this group. Elective caesarean hysterectomy may be discussed in accreta. [8]
Women on anticoagulants (therapeutic LMWH for VTE, warfarin for a mechanical valve, or aspirin/heparin for inherited thrombophilia) bleed from every puncture and suture site. Stop or omit the LMWH, reverse warfarin with vitamin K 10 mg IV plus prothrombin complex concentrate (faster than FFP), give protamine for heparin, and use tranexamic acid aggressively. Plan delivery around anticoagulant timing ("timing of the last dose") and consult haematology early. [4]
Women with inherited bleeding disorders — most commonly von Willebrand disease (the commonest inherited bleeding disorder) and haemophilia carriers — need a coordinated haematology-obstetric plan from booking. Have von Willebrand factor / factor VIII concentrate (or DDAVP where appropriate) available, give third-stage oxytocin mandatorily, and avoid regional anaesthesia only when factor levels are uncorrected. Mild vWD in pregnancy often normalises due to the physiological rise in vWF, but postpartum the levels fall and bleeding may occur days later. [4]
Low-resource and community settings — where theatre, anaesthesia, blood and even electricity are unavailable — demand a pragmatic, evidence-based bundle. The WHO community approach is oxytocin or misoprostol for prophylaxis, uterine massage, tranexamic acid 1 g IV, IV fluids, bimanual compression, and early referral.[1] Misoprostol 600–800 µg oral/sublingual/rectal is the heat-stable uterotonic of choice where oxytocin cold chain cannot be guaranteed, and can be administered by trained community health workers. Early referral before decompensation — and a functioning ambulance/referral chain — is the single biggest determinant of survival.[3]
Previous PPH carries a 10–15% recurrence risk and demands an individualised plan: deliver in a unit with on-site blood and theatre, senior obstetrician present at delivery, active third-stage management with oxytocin, group-and-save on admission (crossmatch if high risk), large-bore IV access, and a low threshold to escalate to uterotonics, balloon and theatre. The single biggest predictor of recurrence is the severity of the index PPH.[1]
Advanced maternal age and grand multiparity (para 5 or more) — the atony risk rises with parity from cumulative myometrial damage and reduced muscle fibre concentration relative to fibrous tissue, and age adds independent vascular and comorbidity risk. These women deserve the same individualised approach as a previous-PPH woman. [4]
Evidence, Guidelines & Regional Differences
Landmark trials and what they changed:
- WOMAN trial (2017, Lancet, 20,060 women): tranexamic acid 1 g IV within 3 h of PPH onset reduced death from bleeding (RR 0.81) with no excess thromboembolism; greatest benefit in the first hour. Now WHO and RCOG first-line.[2]
- E-MOTIVE trial (2023, NEJM): a calibrated-drape early-detection plus first-response treatment bundle (uterine massage, oxytocin, TXA, IV fluids, examination) reduced severe PPH by 60% (4.3% to 1.9% in primary analysis). Reframed PPH as a detectable-and-bundleable emergency.[3]
- Cochrane network meta-analyses: oxytocin is the most effective first-line uterotonic for both prevention and treatment; combination oxytocin-ergometrine is more effective for prevention but with more side-effects.[5][6]
Guideline deltas. WHO (2023): defines PPH as 500 mL, recommends active management of the third stage with oxytocin 10 IU IM, TXA 1 g IV, uterine massage, and misoprostol where oxytocin is unavailable.[1] RCOG Green-top 52 (UK): classifies major (1000–2000 mL) and severe (over 2000 mL) PPH, emphasises major obstetric haemorrhage protocol, balanced transfusion and the uterotonic ladder.[8] ACOG (US): quantitative cumulative blood loss with calibrated receptacles, obstetric haemorrhage bundles (AIM/CMQCC). FIGO (2022): endorses the WHO framework and emphasises fibrinogen over 2 g/L, viscoelastic testing, and a stepwise non-surgical → surgical algorithm.[4] The four guidelines were reviewed side-by-side by Dahlke et al.[7]
WOMAN trial — tranexamic acid in PPH
International, randomised, double-blind, placebo-controlled; 20,060 women in 193 hospitals across 21 countries
Population: Women with clinically diagnosed postpartum haemorrhage after vaginal or caesarean delivery
Key finding
Death from bleeding: 1.5% TXA vs 1.9% placebo (RR 0.81). Hysterectomy and thromboembolism not increased. Greatest survival benefit when given within 1 h (golden hour).
E-MOTIVE — early detection + first-response bundle
International, multicentre, cluster-randomised trial; 78 hospitals across Kenya, Nigeria, South Africa, Tanzania
Population: Around 210,000 vaginal deliveries
Key finding
Severe PPH (primary, over 1000 mL) reduced from 4.3% to 1.9% — a 60% relative reduction. Detection of PPH improved; no serious adverse events attributed to the bundle.
Controversies and uncertainties. Several questions remain live. The optimal timing and dose of tranexamic acid beyond the first 3 h is unclear — late TXA shows no benefit, possibly harm, in subgroup analyses. Whether carbetocin (a long-acting oxytocin analogue) should replace oxytocin for prophylaxis is being settled by the heat-stable carbetocin programme, which addresses cold-chain failure in low-resource settings without yet showing superior efficacy in head-to-head trials. The place of fibrinogen concentrate versus cryoprecipitate is unsettled — concentrate is faster and smaller-volume but expensive. Viscoelastic (ROTEM/TEG)-guided transfusion is gaining ground over fixed-ratio protocols but needs equipment and expertise. The cell-salvage in obstetrics debate (theoretical amniotic fluid embolism risk) is largely resolved in favour of use, with leucocyte depletion filters. Finally, recombinant factor VIIa remains a last-resort, off-label, "before-hysterectomy" rescue with case-series support only.[4]
Prevention — Active Management of the Third Stage
Prevention outperforms treatment. Active management of the third stage of labour (AMTSL) reduces PPH (over 500 mL) by 60% and severe PPH proportionally.[1][6] The three components:
- Prophylactic uterotonic at delivery of the anterior shoulder or within 1 min of birth — oxytocin 10 IU IM is first-line globally (heat-stable carbetocin where oxytocin cold chain is unreliable).[6]
- Controlled cord traction with counter-traction on the suprapubic uterus ( Brandt-Andrews manoeuvre), once the uterus is contracted and placenta separated.
- Uterine massage after placental delivery.
For women at high risk (previous PPH, anaemia, coagulopathy, abnormal placentation, prolonged labour, instrumental delivery): ensure blood crossmatched, two IV cannulae, senior staff present, active third stage, and a low threshold to escalate. [1]
Exam Pearls & High-Yield Minutiae
PPH causes — the 4 Ts
4Ts
uterine atony (70%) — boggy fundus, uterotonic ladder
cervical/vaginal/perineal tears (20%) — examine and repair
retained placenta/products (9%) — explore and remove
coagulopathy (1%) — correct clotting (FFP/cryo/platelets)
Uterotonic ladder contraindications
EC
avoid in HypErtension (vasoconstrictor)
avoid in Asthma (bronchoconstrictor — carboprost = Carbo = Caution Asthma)
Frequently misremembered facts (corrected): [1]
- Ergometrine is the one to avoid in hypertension/pre-eclampsia (NOT carboprost). Carboprost is the one to avoid in asthma.
- Carboprost dose is 250 µg IM q15 min, max 8 doses (2 mg) — examiners ask the maximum.
- Tranexamic acid must be given within 3 h (ideally within 1 h) — late TXA is ineffective.
- Active management reduces PPH by ~60% (not 10, not 90 — a common miscalculation).
- Sheehan syndrome is anterior pituitary necrosis — failure to lactate is the first sign.
- Spiral arteries are the living ligatures compressed by myometrial contraction.
- Fibrinogen target in active PPH is over 2 g/L (not the normal non-pregnant 2).
- B-Lynch suture is a compression (brace) suture, not a ligation.
Complications Recap & When to Escalate
Exam application bank (NEET-PG / INICET)
One-line answer
Postpartum haemorrhage (PPH) = blood loss over 500 mL (vaginal) or over 1000 mL (caesarean) within 24 h (primary); major PPH is over 1000 mL or any loss with shock. Secondary PPH = 24 h to 12 weeks postpartum. 4 Ts: Tone (atony 70%), Trauma (20%), Tissue (9%), Thrombin (1%). Resuscitate and treat the cause in parallel. Uterotonic ladder: oxytocin, ergometrine (avoid hypertension), carboprost (avoid asthma), misoprostol, then tranexamic acid 1 g IV (WOMAN). Mechanical/surgical: Bakri balloon, B-Lynch suture, internal iliac ligation, hysterectomy (last resort).[2]
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard.[5]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes.[5]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change.[1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each.[1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory.[1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Postpartum Haemorrhage.
References
- [1]Vogel JP, Williams M, Gallos I, et al. WHO recommendations on uterotonics for postpartum haemorrhage prevention: what works, and which one? BMJ global health, 2019.PMID 31139461
- [2]WOMAN Trial Collaborators. Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial. Lancet, 2017.PMID 28456509
- [3]Gallos I, Devall A, Martin J, et al.; E-MOTIVE Collaborators. Randomized trial of early detection and treatment of postpartum hemorrhage (E-MOTIVE). N Engl J Med, 2023.PMID 37158447
- [4]Escobar MF, Nassar AH, Theron G, et al. FIGO recommendations on the management of postpartum hemorrhage 2022. Int J Gynaecol Obstet, 2022.PMID 35297039
- [5]Parry Smith WR, Papadopoulou A, Thomas E, et al. Uterotonic agents for first-line treatment of postpartum haemorrhage: a network meta-analysis. Cochrane Database Syst Rev, 2020.PMID 33232518
- [6]Gallos ID, Williams HM, Price MJ, et al. Uterotonic agents for preventing postpartum haemorrhage: a network meta-analysis. Cochrane Database Syst Rev, 2018.PMID 30569545
- [7]Dahlke JD, Mendez-Figueroa H, Maggio L, et al. Prevention and management of postpartum hemorrhage: a comparison of 4 national guidelines. Am J Obstet Gynecol, 2015.PMID 25731692
- [8]Royal College of Obstetricians and Gynaecologists. Prevention and management of postpartum haemorrhage (Green-top Guideline No. 52). BJOG, 2017.PMID 27981719
- [9]Williams EV, Bolaji R, Mortimer A, et al. A cost-effectiveness analysis of early detection and bundled treatment of postpartum hemorrhage alongside the E-MOTIVE trial. Nat Med, 2024.PMID 38844798