Obstetrics & Gynaecology · Obstetrics & Gynaecology
Pre-eclampsia & Eclampsia
Also known as Pre-eclampsia · Eclampsia · HELLP syndrome · Toxaemia of pregnancy · Hypertensive disorder of pregnancy · Pregnancy-induced hypertension
Pre-eclampsia is a multi-system disorder of pregnancy defined by new-onset hypertension (two readings at or above 140/90 mmHg, 4 hours apart) after 20 weeks' gestation accompanied by proteinuria (over 300 mg per 24 hours, protein-creatinine ratio over 30 mg/mmol, or dipstick 2+) OR maternal end-organ dysfunction (renal, hepatic, neurological, haematological) OR uteroplacental dysfunction (fetal growth restriction). Eclampsia is the occurrence of tonic-clonic seizures in a woman with pre-eclampsia, not attributable to another cause. HELLP syndrome (Haemolysis, Elevated Liver enzymes, Low Platelets) is a severe variant. The pathogenesis is a two-stage process: defective trophoblast invasion of the spiral arteries causing placental ischaemia, which then releases anti-angiogenic factors (sFlt-1, soluble endoglin) that drive generalised maternal endothelial dysfunction — explaining the hypertension, proteinuria, and multi-organ injury. Delivery is the only definitive cure, but timing balances maternal safety against fetal maturity. Magnesium sulphate is first-line for seizure prophylaxis and treatment, halving the risk of eclampsia (MAGPIE trial). Aspirin 75 to 150 mg daily from 12 weeks prevents preterm pre-eclampsia in high-risk women.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Overview & Definition
Pre-eclampsia is a multi-system disorder unique to human pregnancy and one of the leading causes of maternal and perinatal mortality worldwide[1]. It is the most important medical condition a candidate must master in obstetrics — it is examined at every level from final-professional MBBS through NEET-PG and INICET, and it kills women quickly if missed. The central principle to hold in mind is this: delivery is the only definitive cure, because the disease originates in the placenta and resolves when the placenta is removed. The clinical art lies in deciding when to deliver — a decision that balances maternal safety against fetal maturity — and in recognising the warning signs of imminent eclampsia so that magnesium sulphate can be given before a seizure occurs[2].
The disorder sits within a family of hypertensive disorders of pregnancy, which together account for an estimated 14 per cent of global maternal deaths and are the leading single cause of maternal mortality in low- and middle-income countries[13][14]. Worldwide, pre-eclampsia complicates roughly 3 to 8 per cent of pregnancies, with eclampsia occurring in about 0.3 per cent in high-income settings and up to 1 per cent in resource-limited settings[14]. In India, pre-eclampsia and eclampsia together contribute an estimated 10 to 15 per cent of all maternal deaths, driven by late antenatal booking, anaemia, and limited access to facility delivery[13].
The modern definition has moved beyond the old "hypertension plus proteinuria plus oedema" triad. Oedema is now considered non-diagnostic because it is near-universal in normal pregnancy, and proteinuria is no longer mandatory if end-organ damage is present. This shift matters because it captures women with severe disease — including HELLP — who may have minimal or even absent proteinuria and would have been missed under the old definition[1].
Pre-eclampsia is therefore defined as new-onset hypertension (systolic at or above 140 mmHg or diastolic at or above 90 mmHg, on two occasions at least 4 hours apart after rest, in a previously normotensive woman) developing after 20 weeks of gestation, accompanied by one or more of[1]:
- Proteinuria — over 300 mg per 24 hours, OR a protein-to-creatinine ratio of at least 30 mg per mmol (or at least 0.3 mg per mg), OR a urine dipstick of 2+ or more when quantitative testing is unavailable.
- Maternal end-organ dysfunction — renal (serum creatinine at or above 1.1 mg per dL or a doubling of baseline), hepatic (transaminases at least twice the upper limit of normal or severe right-upper-quadrant or epigastric pain unresponsive to analgesia), neurological (new-onset headache unresponsive to analgesia, visual disturbance, or altered sensorium), or haematological (platelets under 100 times 10 to the 9 per litre, or disseminated intravascular coagulation).
- Uteroplacental dysfunction — fetal growth restriction, abnormal umbilical artery Doppler, or intrauterine fetal demise. [1]
Eclampsia is the occurrence of generalised tonic-clonic seizures in a woman with pre-eclampsia, not attributable to another cause. It may occur antepartum (around half of cases), intrapartum (about 20 per cent), or postpartum (about 30 per cent), most often within the first 48 hours after delivery but occasionally up to 6 weeks postpartum[2]. Crucially, around one in five women who present with eclampsia have no prior diagnosis of pre-eclampsia, which is why any seizure after 20 weeks must be managed as eclampsia until proven otherwise[2].
Classification
The hypertensive disorders of pregnancy are classified into four overlapping categories. Distinguishing them at the bedside determines surveillance intensity and the threshold to investigate and deliver. [1]
Gestational hypertension
new HTN, no proteinuria
- BP at or above 140/90 after 20 weeks, in previously normotensive woman
- **No proteinuria and no end-organ damage**
- Resolves by 12 weeks postpartum; if it persists, reclassify as chronic HTN
- Up to **25 per cent progress to pre-eclampsia** — close surveillance essential
Pre-eclampsia
HTN plus proteinuria or organ dysfunction
- BP at or above 140/90 after 20 weeks
- **Plus** proteinuria over 300 mg per 24h OR end-organ/uteroplacental dysfunction
- With severe features: BP at or above 160/110, platelets under 100, transaminases over 2x, creatinine at or above 1.1, pulmonary oedema, headache or visual disturbance
- **Delivery at 37 weeks** (non-severe) or **34 weeks** (severe)
Chronic hypertension
before 20 weeks
- HTN predating pregnancy, or diagnosed before 20 weeks
- Persists beyond 12 weeks postpartum
- **Superimposed pre-eclampsia** if sudden worsening BP, new proteinuria, or end-organ damage develop
- Higher baseline risk of fetal growth restriction and abruption
Eclampsia
pre-eclampsia plus seizures
- **Tonic-clonic seizures** in pre-eclampsia, not attributable to another cause
- Antepartum, intrapartum, or postpartum (usually within 48h)
- Medical emergency — magnesium, BP control, deliver
- Recurrent seizure risk until placenta removed

Within pre-eclampsia, two operational sub-classifications are examinable. Pre-eclampsia with severe features (ACOG/NICE terminology) is diagnosed when any one severe criterion is present and mandates magnesium for seizure prophylaxis and an accelerated delivery timeline. Pre-eclampsia is also divided by gestational age into early-onset (under 34 weeks, typically a placental phenotype with fetal growth restriction and more severe course) and late-onset (at or after 34 weeks, often de novo near term, a maternal phenotype with less growth restriction)[1]. HELLP syndrome carries its own sub-classification: the Mississippi system grades severity by platelet nadir (Class 1 platelets under 50, Class 2 platelets 50 to 100, Class 3 platelets 100 to 150 times 10 to the 9 per litre) and the Tennessee system distinguishes partial from complete HELLP. Lower platelet counts correlate with worse maternal outcome[12].
Epidemiology & Risk Factors
Pre-eclampsia affects roughly 3 to 8 per cent of pregnancies globally; eclampsia complicates about 1 to 2 per cent of pre-eclamptic women in settings without prophylactic magnesium[13][14]. The burden is profoundly unequal — case fatality from eclampsia reaches 14 per cent in resource-limited settings versus under 2 per cent in high-income countries[13].
The risk factors cluster into three groups, and they should be actively sought at the booking visit so that aspirin prophylaxis can be offered to high-risk women[1]:
Pre-eclampsia — risk stratification at booking
The full list, worth memorising for viva, is: nulliparity; age over 35 or under 18; previous pre-eclampsia or family history (mother or sister); pre-existing hypertension, renal disease, diabetes, or antiphospholipid syndrome; autoimmune disease (SLE); obesity; multiple pregnancy; interpregnancy interval over 10 years; in-vitro fertilisation (especially donor egg); new partner; African ancestry; low dietary calcium; high inter-pregnancy weight gain[1].
There is one paradoxical protective factor that examiners like to test: maternal smoking, which roughly halves the risk of pre-eclampsia (relative risk around 0.6). The mechanism is thought to involve carbon-monoxide-mediated inhibition of anti-angiogenic sFlt-1 release. This is not a clinical recommendation — smoking causes far greater harm — but it is a recognised biological association and a favourite MCQ stem. Other protective factors include prolonged prior sperm exposure with the same partner, and adequate dietary calcium in deficient populations. [1]
[1]Pathophysiology
Pre-eclampsia is a two-stage disease, and the candidate who can articulate both stages fluently will answer any pathophysiology question at any level[3][4].
Stage one — the placental stage (asymptomatic, first and second trimester). In a healthy pregnancy, extravillous trophoblasts invade the maternal decidual and myometrial segments of the spiral arteries during the second wave of invasion (around 14 to 16 weeks), converting them from narrow, high-resistance, muscular vessels into wide, low-resistance, flaccid conduits capable of delivering the large blood volume the placenta demands. In pre-eclampsia this remodelling is incomplete or absent: the spiral arteries retain their muscular wall and vasoreactivity, the placenta is underperfused, and a state of placental oxidative stress and ischaemia develops. This is why the disease requires a placenta — it occurs in molar pregnancies, rarely in abdominal pregnancies, and resolves when the placenta is delivered. The molecular abnormality is partly immunological: inadequate maternal tolerance of paternal antigens explains the excess risk in nulliparity, new partners, and donor-egg pregnancies. [1]
Stage two — the maternal stage (clinical, after 20 weeks). The ischaemic placenta releases a cascade of anti-angiogenic factors into the maternal circulation. The two best characterised are soluble fms-like tyrosine kinase-1 (sFlt-1) — a splice variant of the VEGF receptor-1 that acts as a circulating decoy, binding and neutralising vascular endothelial growth factor (VEGF) and placental growth factor (PIGF) — and soluble endoglin, which inhibits transforming growth factor-beta signalling and impairs nitric oxide–mediated vasodilation. Levine and colleagues showed in landmark NEJM papers that sFlt-1 levels rise and PIGF levels fall weeks before the onset of clinical disease, and that the sFlt-1 to PIGF ratio is now a validated diagnostic and predictive biomarker[4][5].
The depletion of free VEGF and PIGF produces generalised maternal endothelial dysfunction. The damaged endothelium has three downstream consequences that explain every clinical feature of the disease[3]:
- Vasospasm — loss of nitric-oxide-mediated relaxation raises systemic vascular resistance, producing the hypertension.
- Increased vascular permeability — the leaky endothelium allows protein and fluid to escape into the interstitium, producing proteinuria, oedema, haemoconcentration, and (in the lungs) pulmonary oedema.
- Platelet activation and microthrombus formation — the injured endothelium exposes tissue factor and consumes platelets, producing thrombocytopenia and, in severe disease, disseminated intravascular coagulation. [1]
The end-organ damage follows directly from these mechanisms: in the kidney, glomerular endotheliosis (swelling of the glomerular endothelial cells with loss of fenestrae) produces proteinuria and a falling creatinine clearance; in the liver, periportal necrosis and intra-parenchymal haemorrhage stretch the capsule and cause the classic right-upper-quadrant pain and transaminitis; in the brain, failed cerebral autoregulation at high pressures plus endothelial dysfunction produces vasogenic and cytotoxic oedema — the posterior reversible encephalopathy syndrome (PRES) pattern — which underlies the headache, visual disturbance, and seizures; and at the placenta, ongoing ischaemia and infarction drive fetal growth restriction and, in extreme cases, abruption. [1]
Why magnesium sulphate works. Magnesium acts centrally, not peripherally. It is a competitive antagonist of the NMDA receptor, it stabilises neuronal membranes, it inhibits acetylcholine release at the neuromuscular junction (hence the loss of reflexes as a toxicity sign), and it causes modest cerebral vasodilation. It does not meaningfully lower systemic blood pressure. The MAGPIE trial established that prophylactic magnesium halves the risk of eclampsia in women with pre-eclampsia (relative risk 0.42) and reduces maternal mortality[6], and the Cochrane review confirmed it is superior to diazepam and phenytoin for both prophylaxis and treatment of eclampsia[7][8].
Two-stage pathophysiology — P-E-A-C-E
PEACE
stage one: defective spiral artery remodelling by trophoblasts
stage two: generalised maternal endothelial injury is the final common pathway
sFlt-1 (traps VEGF/PIGF) and soluble endoglin released by the ischaemic placenta
vasospasm, proteinuria, oedema, platelet consumption
glomerular endotheliosis, hepatic necrosis, cerebral oedema (PRES), pulmonary oedema
Clinical Presentation
The classical triad of hypertension, proteinuria, and oedema is now historical — oedema is non-diagnostic, and proteinuria is optional if end-organ damage is present. The modern presentation is therefore dominated by the severity symptoms, which are the harbingers of imminent eclampsia and which every candidate must be able to recite fluently[1][2].
The symptoms of severe disease and imminent eclampsia are: [1]
- Severe, persistent headache — frontal or occipital, not relieved by paracetamol or rest.
- Visual disturbance — scotomata (blind spots), photopsia (flashes), blurred vision, diplopia, or in extreme cases cortical blindness (occipital PRES).
- Epigastric or right-upper-quadrant pain — liver capsule stretch from periportal necrosis or subcapsular haematoma; often mistaken for gastritis or cholecystitis.
- Nausea and vomiting — particularly prominent in HELLP.
- Sudden onset of marked facial or hand oedema, or rapid weight gain (over 1 kg per week) from capillary leak.
- Dyspnoea — from pulmonary oedema.
- Oliguria — under 25 mL per hour, from renal involvement.
- Altered sensorium, confusion, or hyperreflexia with clonus. [1]
The signs of imminent eclampsia at the bedside are the pivotal examination findings — recognising them in time to give magnesium is a pass-or-fail clinical skill[2]:
- Hyperreflexia — brisk deep tendon reflexes.
- Ankle clonus — sustained, especially when sustained (more than 2 to 3 beats) and asymmetric.
- Papilloedema on fundoscopy, with retinal arteriolar spasm, haemorrhages, or exudates.
- A rapidly rising or uncontrolled blood pressure.
- Tachypnoea and basal crackles indicating pulmonary oedema. [1]
Atypical presentations are a deliberate trap in examinations because the textbook picture is absent. Three scenarios deserve particular emphasis: [1]
- HELLP syndrome with minimal or no hypertension. A woman may present with malaise, nausea, and right-upper-quadrant pain and a blood pressure only marginally raised, yet have catastrophic thrombocytopenia and transaminitis. Missing this by attributing the pain to gastritis is a classic and fatal error[12].
- De novo postpartum pre-eclampsia and eclampsia. A woman with a previously normal pregnancy can present with hypertension, headache, or even a first seizure up to 6 weeks postpartum (most often within the first 48 hours). Postpartum eclampsia accounts for a disproportionate share of maternal deaths because the diagnosis is not anticipated[2].
- Early-onset severe disease with fetal growth restriction as the dominant feature. The fetus may have been small for weeks before the mother becomes symptomatic, reflecting long-standing placental insufficiency.
The tempo of presentation is often insidious: a woman may have felt well until a few hours before presenting with a severe headache, and eclampsia can be the first manifestation in around a fifth of cases — which is why any seizure after 20 weeks is eclampsia until proven otherwise[2].
Differential Diagnosis
The differential diagnosis of pre-eclampsia divides into two practical questions at the bedside: "Is this hypertension pre-eclampsia or something else?" and, when a seizure or epigastric pain dominates, "What else could this be?" [1]
Hypertension after 20 weeks — distinguishing the four hypertensive disorders is covered in the Classification section. The bedside discriminator is the presence of proteinuria or end-organ damage: gestational hypertension has none; chronic hypertension predates pregnancy or precedes 20 weeks; pre-eclampsia requires one of the additional criteria. Superimposed pre-eclampsia is diagnosed when a woman with known chronic hypertension develops new or worsening proteinuria, sudden worsening hypertension, or new end-organ damage[1].
Pre-existing renal disease enters the differential when proteinuria is found at booking or before 20 weeks — these women have a baseline elevated creatinine and proteinuria and a high background risk of superimposed pre-eclampsia; the diagnosis is superimposed if there is a sudden worsening or new haematuria/hypertension. [1]
The eclampsia differential — causes of seizure after 20 weeks. Eclampsia is by far the most common cause of a new seizure in the second half of pregnancy, but the alternatives must be actively excluded because their treatment differs completely[2]:
| Mimic | Distinguishing feature |
|---|---|
| Epilepsy | Known history of epilepsy; pre-existing EEG abnormality; typically normal blood pressure and no proteinuria |
| Cerebral vein thrombosis | Often postpartum; focal deficit, headache, seizures; CT or MR venography shows the clot |
| Stroke (ischaemic or haemorrhagic) | Focal neurological deficit; imaging confirms; may complicate severe pre-eclampsia itself |
| Hypertensive encephalopathy | Extreme BP without proteinuria; PRES pattern on MRI |
| Amniotic fluid embolism | Sudden collapse, hypoxia, DIC around delivery; not primarily a seizure |
| Sepsis / cerebral malaria | Fever, peripheral smear positive (malaria); sepsis screen positive |
| Hyponatraemia or hypoglycaemia | Electrolytes and glucose deranged; corrects with treatment |
| Substance withdrawal | History; autonomic signs |
The HELLP and epigastric-pain differential. HELLP is misdiagnosed in up to half of cases because it masquerades as other conditions. The critical mimics are[12]:
- Acute fatty liver of pregnancy (AFLP) — the most dangerous confusion. AFLP presents with malaise, vomiting, hypoglycaemia, coagulopathy, encephalopathy, and a high ammonia, typically in the third trimester. The Swansea criteria support the diagnosis. Unlike HELLP, AFLP is dominated by liver failure rather than haemolysis and thrombocytopenia, and the hypoglycaemia and encephalopathy are earlier and deeper. Both demand urgent delivery.
- Viral hepatitis — positive viral serology (hepatitis A, B, E); no haemolysis or thrombocytopenia; bilirubin proportionally higher than transaminases.
- Cholecystitis — right-upper-quadrant pain with a positive Murphy sign, fever, gallstones on ultrasound; normal platelets and LFTs (unless biliary obstruction).
- Thrombotic thrombocytopenic purpura (TTP) and haemolytic uraemic syndrome (HUS) — predominantly haematological, with profound thrombocytopenia and ADAMTS13 deficiency (TTP) or renal failure (HUS); pregnancy can trigger both.
- Disseminated intravascular coagulation — a complication rather than a mimic, but seen in abruption, sepsis, and amniotic fluid embolism.
- Peptic ulcer disease, pancreatitis, and hepatic rupture — present with abdominal pain; amylase or lipase raised in pancreatitis; hepatic rupture produces shock and a falling haematocrit. [1]
The unifying principle: a woman in the second half of pregnancy with epigastric or right-upper-quadrant pain, malaise, or new hypertension should always have a full blood count, liver function tests, and a blood film — looking for the HELLP pattern — before the symptoms are dismissed as gastritis[12].
Clinical & Bedside Assessment
The focused assessment of a woman with suspected or confirmed pre-eclampsia aims to answer three questions in sequence: how severe is the disease, is eclampsia imminent, and how is the fetus?[1]
Blood pressure measurement must be technically correct, because the diagnosis turns on it. Seat the woman at 45 degrees after 5 minutes of rest, use the correct cuff size (the bladder should encircle at least 80 per cent of the arm), place the cuff at the level of the heart, and record the fifth Korotkoff sound (disappearance) as the diastolic pressure. Use the same arm each time. Confirm with a second reading at least 4 hours apart, unless the pressure is severe (at or above 160/110), in which case confirm within minutes and begin treatment. [1]
The bedside examination proceeds systematically: [1]
- Cardiovascular and fluid status: heart rate, blood pressure, JVP, basal lung auscultation for crackles (pulmonary oedema), oxygen saturation, peripheral oedema (sacral as well as pedal).
- Abdomen: right-upper-quadrant tenderness (liver capsule), epigastric tenderness, fundal height and abdominal palpation for fetal lie and size (growth restriction), uterine tenderness or tone (abruption), and fetal movements.
- Neurological: conscious level, visual acuity and fields, fundoscopy for papilloedema and retinal arteriolar spasm, and — the pivotal bedside signs — deep tendon reflexes and ankle clonus. Brisk reflexes with sustained clonus are the warning that magnesium is needed now.
- Urine: bedside dipstick; 2+ or more warrants quantitative confirmation. [1]
If a seizure occurs (suspected eclampsia): place the woman in the left lateral position (relieves aortocaval compression and protects the airway from aspiration), do not restrain her or put anything in her mouth, maintain the airway with a jaw thrust, give high-flow oxygen, call for senior obstetric and anaesthetic help, establish intravenous access, and prepare to give magnesium sulphate[2]. Continuous CTG monitoring is started and the fetus is assessed. The seizure is usually self-limiting (1 to 2 minutes); prolonged or recurrent seizures require additional magnesium and may need intubation.
During magnesium therapy, the bedside monitoring is non-negotiable and is the single most examinable safety point: patellar reflexes every 30 minutes (loss is the first sign of toxicity), respiratory rate (under 12 per minute is danger), oxygen saturation, and hourly urine output (must be over 25 mL per hour, because magnesium is renally excreted and accumulates in oliguria)[7].
Investigations
The investigation strategy serves three purposes: to confirm the diagnosis and grade severity, to establish a baseline for trending, and to assess fetal wellbeing[1].
Maternal blood tests
- Full blood count — platelets under 100 times 10 to the 9 per litre is a severe feature and a HELLP criterion; haemoglobin may fall from haemolysis; haematocrit rises from haemoconcentration in capillary leak.
- Blood film — schistocytes (fragmented red cells) confirm microangiopathic haemolysis in HELLP.
- Lactate dehydrogenase (LDH) — over 600 IU/L supports haemolysis and is a marker of severity.
- Bilirubin — raised (over 1.2 mg per dL), mostly indirect, from haemolysis.
- Liver function tests — AST and ALT at least twice the upper limit of normal (over 70 IU/L is the HELLP Tennessee criterion) indicate hepatic involvement.
- Serum creatinine — at or above 1.1 mg per dL (97 micromol per L) or a doubling of baseline is a severe feature; a rising trend is more ominous than any single value.
- Uric acid — often raised and supportive but not diagnostic; reflects reduced renal clearance.
- Coagulation screen — PT, APTT, fibrinogen, and D-dimer to detect DIC, which complicates about 10 per cent of severe pre-eclampsia and most HELLP.
- Group and screen — in anticipation of delivery or possible haemorrhage. [1]
Urine
- 24-hour protein collection — over 300 mg is the historical gold standard but is slow.
- Protein-to-creatinine ratio (PCR) — at least 30 mg per mmol (or 0.3 mg per mg) on a random sample is the modern preferred test; it correlates well with the 24-hour result and is available within the hour.
- Dipstick — 2+ or more is the trigger for quantitative confirmation when PCR is unavailable (dipstick is poorly reproducible). [1]
Angiogenic biomarkers
- Placental growth factor (PIGF) — a low PIGF (under 100 pg per mL) or an sFlt-1 to PIGF ratio of 38 or more strongly rules in pre-eclampsia; a ratio under 38 has a very high negative predictive value for ruling out pre-eclampsia presenting within the next 1 to 2 weeks. These tests are NICE-approved as rule-out tests in suspected pre-eclampsia and shorten the diagnostic pathway[1].
Fetal assessment
- Cardiotocography (CTG) — continuous fetal heart rate monitoring, particularly in severe disease or during magnesium therapy.
- Ultrasound — fetal growth, estimated fetal weight, and amniotic fluid volume (oligohydramnios suggests placental insufficiency).
- Umbilical artery Doppler — raised resistance, or absent or reversed end-diastolic flow, confirms placental insufficiency and influences delivery timing.
- Biophysical profile — composite of CTG, fetal tone, movement, breathing, and amniotic fluid volume. [1]
Severity assessment tools
The fullPIERS model (published 2021) is a validated, Multicentre-derived tool that estimates the probability of a maternal near-miss or death within 48 hours, from a small set of variables (gestational age, chest pain or dyspnoea, oxygen saturation, platelet count, creatinine, and aspartate aminotransferase). The NICE and ACOG severe-feature criteria are the bedside tool used to decide who needs magnesium and accelerated delivery[1].
Monitoring frequency in established disease
In severe pre-eclampsia, repeat blood pressure every 15 minutes, platelets and LFTs every 6 to 12 hours, and urine output hourly. In non-severe disease, blood pressure and symptoms can be checked 2 to 3 times per week as an outpatient, with bloods weekly. [1]
Management — Resuscitation
The resuscitation phase applies when a woman presents with eclampsia, severe features, or unstable disease. The goals are, in order: stop the seizure, control the blood pressure, protect the airway and oxygenation, and then plan delivery — never deliver an unstable patient[2][6].
Eclamptic seizure — the emergency sequence: [1]
- Left lateral position and airway protection (jaw thrust); high-flow oxygen at 15 L per minute by non-rebreather mask.
- Call for help — senior obstetrician, anaesthetist, midwife, neonatal team.
- IV magnesium sulphate — loading dose 4 g given over 5 to 10 minutes, followed by a maintenance infusion of 1 g per hour (Zuspan regimen). Continue for 24 hours after delivery or 24 hours after the last seizure, whichever is later[6][15].
- Control the blood pressure — IV labetalol or hydralazine to bring the pressure under 160/110 (see below).
- Fluid restrict — crystalloid at 80 mL per hour or 1 mL per kg per hour to avoid pulmonary oedema.
- Continuous CTG, indwelling catheter for hourly urine output, reflexes and respiratory rate every 30 minutes.
- Plan delivery once the mother is stabilised (typically after the loading dose and BP control); vaginal delivery is acceptable if feasible and not contraindicated.
Severe hypertension control. A blood pressure at or above 160/110 is a medical emergency because the risk of maternal intracerebral haemorrhage rises steeply. The aim is to bring the pressure safely under 160/110 over 1 to 2 hours, then to a maintenance target of 140 to 150 over 90 to 100 mmHg. Over-rapid reduction causes placental hypoperfusion and fetal distress. The IV agents of choice are: [1]
- IV labetalol — 20 mg over 2 minutes, repeated every 10 minutes escalating to 40 then 80 mg (maximum 300 mg total), followed by an infusion of 20 to 160 mg per hour.
- IV hydralazine — 5 mg over 4 to 5 minutes, repeated every 20 minutes to a maximum of 20 mg, then infusion of 5 to 10 mg per hour. A fluid bolus of 250 mL crystalloid before hydralazine can blunt reflex tachycardia.
- Oral nifedipine 10 mg (modified release preferred) when IV access is unavailable; onset within 30 minutes. [1]
Fluid balance deserves a warning of its own. Pulmonary oedema from iatrogenic fluid overload is a leading cause of preventable maternal death in pre-eclampsia, because the leaky endothelium cannot tolerate excess fluid and hypoalbuminaemia lowers oncotic pressure. Restrict maintenance fluid to 80 mL per hour or 1 mL per kg per hour, use crystalloid only, and avoid boluses unless the woman is hypovolaemic or oliguric with raised lactate. A central line may be needed in pulmonary oedema or renal failure[1].
Oxytocin is the uterotonic of choice at delivery; ergometrine and the ergot derivatives are contraindicated because they precipitate severe hypertension. [1]
[1]Management — Definitive & Stepwise
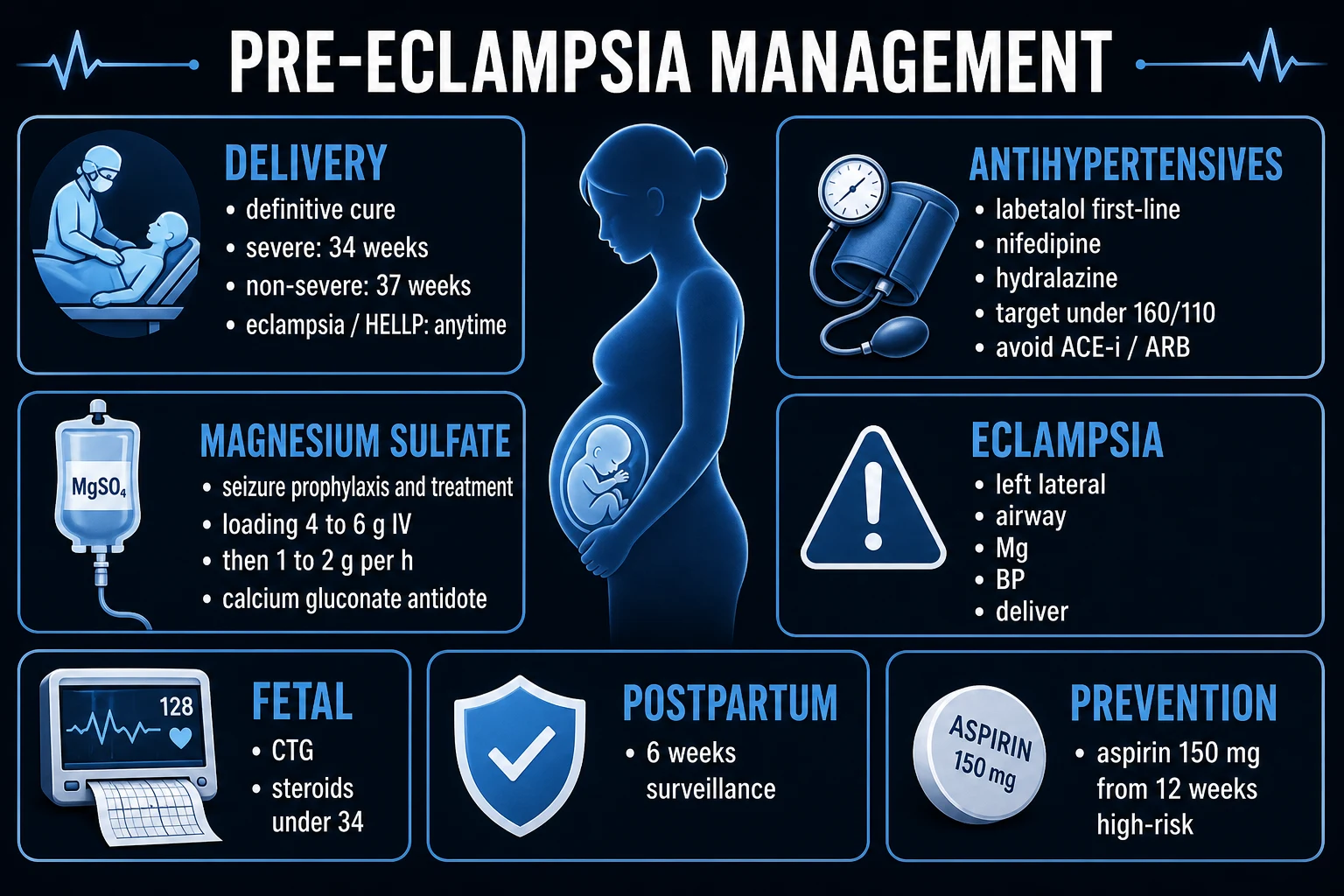
Definitive management has four pillars delivered in sequence: antihypertensive control of mild-to-moderate hypertension, magnesium for seizure prophylaxis in severe disease, delivery at the appropriate gestation, and postpartum care and counselling[1].
Pillar one — antihypertensive therapy
Antihypertensives are given to all women with pre-eclampsia to reduce the risk of maternal stroke; the threshold and route depend on severity. [1]
- Oral agents for BP at or above 140/90 (and under 160/110):
- Labetalol 200 mg orally twice daily, titrated to a maximum of 800 mg per day — first-line; combined alpha- and beta-blocker; avoid in asthma, heart block, and severe bradycardia.
- Nifedipine modified-release 10 to 20 mg orally twice daily — a calcium-channel blocker; safe and effective.
- Methyldopa 250 mg orally three times daily, maximum 1 g per day — centrally acting; avoid postpartum because it causes depression; safe in breastfeeding.
- IV agents for severe hypertension (at or above 160/110): labetalol or hydralazine as detailed in resuscitation, or oral nifedipine if IV is unavailable.
- Drugs that are contraindicated in pregnancy: ACE inhibitors and angiotensin receptor blockers (fetal renal agenesis, oligohydramnios, neonatal renal failure and skull hypoplasia), atenolol (fetal growth restriction), diuretics (reduce placental perfusion; only for pulmonary oedema), nitroprusside (cyanide toxicity). [1]
Pillar two — magnesium sulphate for seizure prophylaxis and treatment
Magnesium sulphate is given to every woman with severe features of pre-eclampsia (prophylaxis) and to every woman with eclampsia (treatment), and is continued for 24 hours postpartum or 24 hours after the last seizure[6][7][15].
Two regimens are examinable; both achieve equivalent therapeutic levels of 4 to 7 mEq per litre (4.8 to 8.4 mg per dL): [1]
- Zuspan (intravenous) regimen — preferred where IV access is established. Loading: 4 to 6 g of 20 per cent magnesium sulphate intravenously over 5 to 10 minutes. Maintenance: 1 to 2 g per hour by infusion pump. Continue 24 hours after delivery or last seizure.
- Pritchard (intramuscular) regimen — preferred in resource-limited settings without infusion pumps or reliable IV access. Loading: 4 g of 20 per cent solution IV over 5 minutes plus 10 g of 50 per cent solution deep intramuscularly (5 g into each buttock). Maintenance: 5 g of 50 per cent solution deep intramuscularly into alternate buttocks every 4 hours. [1]
Monitoring during magnesium therapy must be done continuously and documented: (1) patellar reflexes present every 30 minutes — loss is the first sign of toxicity; (2) respiratory rate at or above 12 per minute; (3) urine output at least 25 mL per hour (at least 100 mL over 4 hours) — magnesium is renally excreted and accumulates in oliguria or renal failure; (4) oxygen saturation. Draw a serum magnesium level if oliguria, renal impairment, or signs of toxicity develop. [1]
Recurrent seizure despite the loading dose is treated with a further 2 g IV bolus over 5 minutes (or 2 to 4 g). If seizures continue despite adequate magnesium, IV diazepam (5 to 10 mg) or phenytoin is second-line, but only after magnesium — magnesium is superior to both[7].
Magnesium toxicity — recognition and treatment. Toxicity is directly proportional to serum level and is the key viva topic. The clinical sequence is: [1]
| Serum magnesium (mg per dL) | Clinical effect |
|---|---|
| 4 to 7 | Therapeutic range |
| 8 to 10 | Loss of deep tendon reflexes (first warning) |
| 13 to 15 | Respiratory depression, respiratory arrest |
| Over 25 | Cardiac arrest |
Treatment of toxicity: stop the infusion immediately, give oxygen, ventilate if respiratory depression, and administer the antidote calcium gluconate 10 per cent, 10 mL (1 g) intravenously slowly over 10 minutes — calcium directly antagonises magnesium at the neuromuscular junction and myocardium. Re-check serum magnesium and renal function. [1]
Magnesium toxicity — progressive signs
WARN
loss of patellar reflex is the FIRST sign — check every 30 minutes
respiratory rate under 12, then respiratory depression and arrest
antidote: calcium gluconate 10% 10 mL (1 g) IV slowly
8-10 mg/dL reflexes lost; 13-15 respiratory arrest; over 25 cardiac arrest
Pillar three — delivery (the definitive cure)
Delivery is the only definitive treatment for pre-eclampsia, because removing the placenta removes the source of the anti-angiogenic factors and sFlt-1 levels fall over the following 48 hours. The decision is one of timing and route[1].
- Pre-eclampsia without severe features: plan delivery at 37 weeks of gestation, by induction of labour or caesarean section as obstetrically indicated. Expectant management up to 37 weeks with twice-weekly maternal and fetal surveillance is safe.
- Pre-eclampsia with severe features: deliver at 34 weeks of gestation, OR earlier if there is any maternal or fetal deterioration. The indications for immediate delivery regardless of gestation are: eclampsia, HELLP syndrome, pulmonary oedema, disseminated intravascular coagulation, placental abruption, abnormal fetal monitoring (CTG), or intrauterine fetal demise, and uncontrolled severe hypertension despite maximum therapy.
- Expectant management under 34 weeks with severe features is an option only in a stable woman in a tertiary centre, with the goal of gaining fetal maturity with corticosteroids. It requires intensive monitoring (blood pressure, platelets, LFTs, CTG) and a low threshold to abandon and deliver.
- Route of delivery: vaginal delivery is preferred if feasible and not contraindicated, because caesarean section in severe pre-eclampsia carries additional anaesthetic and surgical risk. Caesarean is reserved for the usual obstetric indications or an unfavourable cervix at very preterm gestations. Control blood pressure throughout labour and continue magnesium. [1]
Corticosteroids for fetal lung maturation are given if delivery is anticipated before 34 weeks (some guidelines extend to under 35 weeks and 6 days): betamethasone 12 mg intramuscularly every 24 hours for two doses, or dexamethasone 6 mg intramuscularly every 12 hours for four doses. Antenatal corticosteroids are the single most effective intervention to reduce neonatal respiratory distress syndrome, intraventricular haemorrhage, and necrotising enterocolitis in the preterm neonate. [1]
Pillar four — postpartum care
- Continue magnesium sulphate for 24 hours after delivery (or 24 hours after the last seizure in eclampsia), because the risk of postpartum eclampsia is highest in this window and early discontinuation increases that risk[15].
- Continue antihypertensives; blood pressure often peaks on day 3 to 6 postpartum and then declines. Adjust doses as the pressure falls. Methyldopa should be stopped postpartum.
- Monitor for fluid balance — oliguria is common immediately postpartum from the magnesium and the autonomic shifts; watch for pulmonary oedema.
- Review at 2 weeks and 6 weeks; blood pressure usually normalises by 6 to 12 weeks. Persistent hypertension at 12 weeks mandates reclassification as chronic hypertension and long-term management.
- Counsel on recurrence and cardiovascular risk: pre-eclampsia recurs in 15 to 20 per cent of subsequent pregnancies (25 to 65 per cent if early-onset severe), and confers a 2- to 4-fold lifelong increase in cardiovascular disease (hypertension, ischaemic heart disease, stroke, cardiovascular death) — pre-eclampsia is now regarded as a cardiovascular risk equivalent[1].
Prevention
Prevention targets the placental stage of the disease and is the most rewarding intervention in obstetrics[9][11].
- Aspirin 75 to 150 mg daily from 12 weeks is recommended for high-risk women (one high-risk or two moderate-risk factors per NICE/ISSHP). It works by inhibiting thromboxane relative to prostacyclin, improving placental vasculature. The ASPRE trial (Rolnik, 2017) showed that aspirin 150 mg daily from 11 to 14 until 36 weeks reduced preterm pre-eclampsia by 62 per cent in women screened as high-risk by first-trimester combined testing[11]. Roberge's meta-analyses confirmed that doses over 100 mg and initiation before 16 weeks are more effective than 75 mg started later[9][10]. Regional dosing varies: ACOG recommends 81 mg, NICE and ISSHP recommend 75 to 150 mg, India typically uses 75 mg.
- Calcium supplementation 1 to 1.5 g per day reduces pre-eclampsia in women with low dietary calcium intake (common in resource-limited settings).
- Close antenatal surveillance of blood pressure and urine, and identification of high-risk women at booking.
- Avoid smoking cessation as a prevention strategy — despite the paradoxical association, smoking causes far greater harm. Weight management before pregnancy is the only modifiable lifestyle intervention with consistent evidence.
HELLP Syndrome
HELLP syndrome — Haemolysis, Elevated Liver enzymes, Low Platelets — is a severe variant of pre-eclampsia that may present with minimal or absent hypertension or proteinuria and is therefore frequently misdiagnosed as gastritis, hepatitis, or cholecystitis[12].
Diagnostic criteria (Tennessee): haemolysis (abnormal peripheral smear, LDH over 600, or bilirubin over 1.2 mg per dL), AST at least 70 IU/L, and platelets under 100 times 10 to the 9 per litre. The Mississippi classification grades severity by platelet nadir: Class 1 under 50, Class 2 at 50 to 100, Class 3 at 100 to 150 times 10 to the 9 per litre — lower counts predict worse outcome. [1]
Clinical features: malaise (around 90 per cent), nausea and vomiting, right-upper-quadrant or epigastric pain (liver capsule stretch), oedema, and hypertension that may be mild. Proteinuria may be minimal. Up to 15 per cent have no hypertension[12].
Complications are disproportionately severe: disseminated intravascular coagulation, placental abruption, acute kidney injury, hepatic rupture or subcapsular haematoma, pulmonary oedema, retinal detachment, and eclampsia. Maternal mortality is around 1 per cent and perinatal mortality 7 to 20 per cent, mostly from prematurity and abruption. [1]
Management: urgent delivery is the definitive treatment (the disease deteriorates rapidly), with magnesium sulphate for seizure prophylaxis, antihypertensives for BP control, and supportive care — correction of coagulopathy with platelets and fresh-frozen plasma, transfusion for anaemia, and vigilant monitoring for hepatic rupture. Corticosteroids (high-dose dexamethasone) have been used to hasten platelet recovery, but the evidence is inconsistent and they are not routinely recommended for fetal indication. The role of corticosteroids specifically to improve maternal outcome remains debated[12].
Hepatic rupture — a catastrophic complication — presents with sudden severe right-upper-quadrant or shoulder-tip pain, shock, and a falling haematocrit. Management is resuscitation, urgent imaging (CT or ultrasound), and emergency surgery (haemostatic packing, embolisation, or liver transplant in extreme cases). [1]
Specific Subtypes & Scenarios
Early-onset pre-eclampsia (under 34 weeks) has a predominantly placental phenotype: severe, often with fetal growth restriction and abnormal Doppler, longer latency needed, and the highest recurrence in future pregnancies. Management is expectant in a tertiary centre with corticosteroids and close monitoring, unless deterioration mandates delivery[1].
Late-onset pre-eclampsia (34 weeks or more) has a more maternal phenotype: less growth restriction, often de novo near term, more commonly associated with maternal obesity and advanced age. Delivery is usually indicated at diagnosis or shortly thereafter if severe. [1]
Superimposed pre-eclampsia — on a background of chronic hypertension — is suspected when there is sudden worsening hypertension, new proteinuria, or new end-organ damage. These women have a higher baseline risk and a lower threshold to deliver; aspirin prophylaxis is indicated from 12 weeks. [1]
Postpartum pre-eclampsia and eclampsia present within 6 weeks of delivery (most often within 48 hours) and may have no antenatal diagnosis. New-onset hypertension with headache or visual symptoms, or a new seizure, requires magnesium and antihypertensives exactly as antepartum, plus exclusion of retained placenta, sepsis, and other causes. Oestrogen-containing contraception is relatively contraindicated until blood pressure has normalised[2].
Eclampsia itself, as a scenario, requires the full resuscitation sequence described above. Around half of eclamptic seizures are antepartum, about a fifth intrapartum, and around 30 per cent postpartum. The risk of recurrence within the same pregnancy is significant, which is why magnesium is continued for 24 hours[2].
Multiple pregnancy carries a higher risk of pre-eclampsia (around 3-fold), earlier onset, and a lower threshold to investigate; aspirin is indicated. Women with renal disease, autoimmune disease (SLE, APS), or diabetes are at high risk and warrant aspirin from 12 weeks plus intensified surveillance. [1]
Complications & Pitfalls
Maternal complications: eclampsia, HELLP syndrome, disseminated intravascular coagulation (around 10 per cent of severe cases), pulmonary oedema (often iatrogenic from fluid overload — a leading preventable cause of death), acute kidney injury (acute tubular necrosis, rarely cortical necrosis), stroke (intracerebral or subarachnoid haemorrhage — the leading cause of maternal death in pre-eclampsia), hepatic rupture or subcapsular haematoma, retinal detachment and cortical blindness, placental abruption, acute respiratory distress syndrome, and magnesium toxicity[1][13].
Fetal complications: fetal growth restriction (in up to 25 per cent of early-onset disease), prematurity (iatrogenic and spontaneous), placental abruption, intrauterine fetal demise, and neonatal complications of prematurity (respiratory distress syndrome, intraventricular haemorrhage, necrotising enterocolitis, hypoglycaemia, and long-term cardiovascular and neurodevelopmental risk). [1]
The classic pitfalls — every one an examinably avoidable error: [1]
- Relying on oedema or weight gain as diagnostic — oedema is non-diagnostic; proteinuria or end-organ damage is required.
- Missing HELLP with a normal blood pressure — always check platelets and LFTs in any woman with epigastric or right-upper-quadrain pain, malaise, or nausea in the third trimester[12].
- Not checking reflexes during magnesium therapy — the loss of reflexes is the first sign of toxicity and precedes respiratory depression.
- Giving sublingual nifedipine — precipitous hypotension and fetal distress; use modified-release oral.
- Giving ergometrine for postpartum haemorrhage — it causes dangerous hypertension; use oxytocin with or without misoprostol or carboprost (note carboprost is also relatively contraindicated in asthma).
- Aggressive fluid loading — pulmonary oedema is a leading iatrogenic cause of death.
- Delayed delivery in eclampsia or HELLP — the disease only resolves once the placenta is removed.
- Forgetting postpartum surveillance — magnesium for 24 hours postpartum; blood pressure peaks at day 3 to 6.
- Mismanaging magnesium in renal failure or oliguria — reduce or omit the maintenance dose and check levels.
- Stopping magnesium too early postpartum — increases the risk of postpartum eclampsia[15].
Prognosis & Disposition
Pre-eclampsia resolves within 6 weeks postpartum, with blood pressure normalising by 12 weeks. Blood pressure that remains elevated at 12 weeks is reclassified as chronic hypertension and managed long-term[1].
Maternal mortality in severe disease is 1 to 2 per cent in high-income settings; eclampsia case fatality is under 2 per cent with magnesium but reaches 14 per cent in resource-limited settings[13]. The leading causes of maternal death are cerebral haemorrhage, pulmonary oedema, hepatic rupture, and DIC.
Perinatal outcomes depend on gestation at delivery and the degree of placental insufficiency: fetal growth restriction complicates up to a quarter of early-onset disease, prematurity is common, and perinatal mortality is 1 to 2 per cent in high-income settings and up to 25 per cent in low-resource settings[13].
Recurrence in the next pregnancy is 15 to 20 per cent overall, rising to 25 to 65 per cent after early-onset severe disease or HELLP[1]. Subsequent pregnancies should be managed with aspirin prophylaxis, early booking, and intensified surveillance.
Long-term maternal risk is now a major focus: pre-eclampsia is a cardiovascular risk equivalent, conferring a 2- to 4-fold increase in future hypertension, ischaemic heart disease, stroke, and cardiovascular death, and an increased risk of chronic kidney disease and cognitive decline. Women should be counselled at the postnatal visit, encouraged to maintain a healthy weight and blood pressure, and followed up in primary care for cardiovascular risk factor modification[1].
Disposition: severe pre-eclampsia and eclampsia require admission to a high-dependency or delivery suite with continuous monitoring; HELLP and eclampsia warrant critical care involvement. Women with non-severe pre-eclampsia can be managed on the antenatal ward or as outpatients with twice-weekly review. After delivery, the postnatal review at 2 and 6 weeks addresses blood pressure, recurrence counselling, contraception, and cardiovascular risk. [1]
Special Populations
Remote from term (under 34 weeks, stable): expectant management in a tertiary centre is appropriate to gain fetal maturity — give corticosteroids, continue close maternal and fetal monitoring (daily blood pressure, platelets and LFTs every 6 to 12 hours, continuous CTG), use a 48-hour window of magnesium during stabilisation if severe, and deliver promptly at the first sign of maternal or fetal deterioration[1].
Postpartum (up to 6 weeks): new-onset hypertension or seizure postpartum is managed with magnesium and antihypertensives exactly as antepartum; assess for retained placenta, review medications, and counsel on contraception (oestrogen-containing combined oral contraception is relatively contraindicated until blood pressure is normal; progestogen-only methods are safe)[2].
Chronic hypertension and superimposed pre-eclampsia: labetalol, nifedipine, and methyldopa are safe in pregnancy; target a blood pressure under 140/90 (around 135/85); offer aspirin 75 to 150 mg from 12 weeks; monitor for superimposed disease with a low threshold to investigate[1].
Renal disease or transplant: high baseline risk; aspirin prophylaxis, collaborative nephrology care, low threshold to investigate, and individualised delivery timing. [1]
Multiple pregnancy: higher risk, earlier onset; aspirin from 12 weeks and intensified surveillance. [1]
Anaemia (common in India): worsens outcome and increases the risk of stroke and heart failure; correct with iron, folate, and transfusion as indicated[13].
Previous early-onset severe pre-eclampsia: aspirin 75 to 150 mg from 12 weeks, calcium 1 to 1.5 g per day if low intake, early booking, and close surveillance throughout. [1]
Evidence, Guidelines & Regional Differences
Landmark trials and what they changed: [1]
- MAGPIE trial (Altman, Lancet 2002) — randomised over 10,000 women with pre-eclampsia to magnesium sulphate versus placebo; magnesium halved the risk of eclampsia (relative risk 0.42) and reduced maternal mortality; established magnesium as the global standard[6].
- Cochrane reviews (Duley 2010) — magnesium is superior to diazepam (RR 0.44 for recurrence) and phenytoin (RR 0.21) for treating eclampsia, and reduces the risk of eclampsia when given prophylactically[7][8].
- ASPRE trial (Rolnik, NEJM 2017) — first-trimester combined screening plus aspirin 150 mg daily from 11 to 14 until 36 weeks reduced preterm pre-eclampsia by 62 per cent in high-risk women[11].
- Roberge meta-analyses (AJOG 2018) — aspirin at doses over 100 mg started before 16 weeks is more effective than 75 mg started later; aspirin also reduces fetal growth restriction, preterm birth, and perinatal mortality[9][10].
- Abalos WHO multicountry survey (BJOG 2014) — quantified the global burden of maternal and perinatal adverse outcomes from pre-eclampsia and eclampsia, highlighting the disproportionate burden in low-resource settings[13].
Guidelines — major regional documents: [1]
- ACOG Practice Bulletin 222 (2020) — United States; aspirin 81 mg from 12 weeks; magnesium for severe features; delivery at 37 (non-severe) and 34 (severe) weeks.
- NICE NG133 (2019) — United Kingdom; aspirin 75 to 150 mg from 12 weeks; prefers quantitative PCR over 30 mg per mmol; magnesium and delivery thresholds aligned with ACOG.
- ISSHP 2018 — International Society; harmonises definitions and accepts the role of angiogenic biomarkers.
- GOI / FOGSI / RCOG-aligned India guidelines — aspirin 75 mg from 12 weeks; the Pritchard intramuscular magnesium regimen is preferred in rural and IV-access-poor settings; community health workers (ASHAs) play a crucial role in blood pressure monitoring and referral[13].
India: Pre-eclampsia and eclampsia are a leading cause of maternal mortality (10 to 15 per cent of maternal deaths). Late antenatal booking, anaemia, and limited access to facility delivery increase eclampsia risk. The Pritchard intramuscular magnesium regimen is widely used in resource-limited settings where infusion pumps and reliable IV access are unavailable. Community health workers (ASHAs) are central to blood pressure screening and referral. Aspirin 75 mg from 12 weeks is the standard prophylactic dose. UK (NICE NG133): aspirin 75 to 150 mg, prefers quantitative PCR over 30 mg per mmol, accepts angiogenic biomarkers as rule-out tests. US (ACOG 222): aspirin 81 mg, accepts dipstick 2+ when quantitative testing unavailable. Global: magnesium sulphate is the universally accepted anticonvulsant of choice (WHO Essential Medicines List).
Where the evidence is weak or debated: the routine use of corticosteroids specifically to improve maternal outcome in HELLP (rather than fetal lung maturation); the optimal duration of magnesium postpartum; whether angiogenic biomarkers should be universal; and the role of treating mild chronic hypertension in pregnancy (the CHAP trial showed benefit but the threshold for treatment of mild gestational hypertension remains debated). The optimal aspirin dose (81 mg versus 150 mg) and whether all women or only screened high-risk women should receive aspirin are also areas of ongoing refinement. [1]
Exam Pearls
These are the one-liners, frequently-misremembered facts, and high-yield minutiae that examiners reward[1][6][12]:
- Oedema is NOT diagnostic — removed from the modern definition; proteinuria or end-organ damage is required.
- The first sign of magnesium toxicity is loss of deep tendon reflexes; the antidote is calcium gluconate 10% 10 mL (1 g) IV.
- Sublingual nifedipine is contraindicated — it causes precipitous hypotension and fetal distress; use modified-release oral.
- Delivery is the only cure — 37 weeks non-severe, 34 weeks severe, immediately for eclampsia, HELLP, or deterioration.
- Antihypertensive target: under 160/110 urgently, then 140 to 150 over 90 to 100. ACE inhibitors, ARBs, atenolol, diuretics, and nitroprusside are contraindicated.
- Magnesium regimens: Zuspan (IV, 4 to 6 g load then 1 to 2 g per hour) for modern practice; Pritchard (IM, 4 g IV plus 10 g IM load then 5 g IM every 4 hours) for resource-limited settings.
- HELLP mnemonic: Haemolysis (LDH over 600, schistocytes, bilirubin over 1.2), Elevated Liver enzymes (AST or ALT over 70), Low Platelets (under 100 times 10 to the 9 per L). AFLP is the key mimic (hypoglycaemia, coagulopathy, encephalopathy).
- Prevention: aspirin over 100 mg (150 mg UK/India, 81 mg ACOG) from 12 weeks in high-risk women; calcium 1 to 1.5 g per day if low intake.
- Postpartum pre-eclampsia or eclampsia can occur up to 6 weeks; continue magnesium for 24 hours post-delivery.
- Two-stage pathophysiology: abnormal placentation then anti-angiogenic factors (sFlt-1 high, PIGF low) then generalised endothelial dysfunction.
- Gestational hypertension progresses to pre-eclampsia in 15 to 25 per cent — surveillance is essential.
- Pre-eclampsia is a cardiovascular risk equivalent — 2- to 4-fold lifelong increase in cardiovascular disease; counsel and follow up.
- fullPIERS predicts maternal near-miss; NICE/ACOG severe features drive the decision to give magnesium and deliver.
- Labetalol is first-line (combined alpha- and beta-blocker); avoid in asthma and heart block; methyldopa is avoided postpartum because it causes depression.
- The seizure in eclampsia is a tonic-clonic seizure — left lateral position, airway, magnesium loading, control BP, then deliver.
- Smoking paradoxically halves the risk of pre-eclampsia (a biological association, not a recommendation). [1]
Exam application bank (NEET-PG / INICET)
One-line answer
Pre-eclampsia is a multi-system disorder of pregnancy defined by new-onset hypertension (two readings at or above 140/90 mmHg, 4 hours apart) after 20 weeks' gestation accompanied by proteinuria (over 300 mg per 24 hours, protein-creatinine ratio over 30 mg/mmol, or dipstick 2+) OR maternal end-organ dysfunction (renal, hepatic, neurological, haematological) OR uteroplacental dysfunction (fetal growth restriction). Eclampsia is the occurrence of tonic-clonic seizures in a woman with pre-eclampsia, not attributable to another cause. HELLP syndrome (Haemolysis, Elevated Liver enzymes, Low Platelets) is a severe variant. The pathogenesis is a two-stage process: defective trophoblast invasion of the spiral arteries causing placental ischaemia, which then releases anti-angiogenic factors (sFlt-1, soluble endoglin) that drive generalised maternal endothelial dysfunction — explaining the hypert [1]
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Pre-eclampsia & Eclampsia.
[1] [1]References
- [1]Wu P, Green M, Myers JE. Hypertensive disorders of pregnancy BMJ, 2023.PMID 37391211
- [2]Fishel Bartal M, Sibai BM. Eclampsia in the 21st century Am J Obstet Gynecol, 2022.PMID 32980358
- [3]von Dadelszen P, Magee LA. Pre-eclampsia: an update Curr Hypertens Rep, 2014.PMID 24915961
- [4]Levine RJ, Maynard SE, Qian C, et al. Circulating angiogenic factors and the risk of preeclampsia N Engl J Med, 2004.PMID 14764923
- [5]Levine RJ, Lam C, Qian C, et al. Soluble endoglin and other circulating antiangiogenic factors in preeclampsia N Engl J Med, 2006.PMID 16957146
- [6]Altman D, Carroli G, Duley L, et al. (MAGPIE Trial Collaborative Group). Do women with pre-eclampsia, and their babies, benefit from magnesium sulphate? The Magpie Trial: a randomised placebo-controlled trial Lancet, 2002.PMID 12057549
- [7]Duley L, Gulmezoglu AM, Henderson-Smart DJ, Chou D. Magnesium sulphate and other anticonvulsants for women with pre-eclampsia Cochrane Database Syst Rev, 2010.PMID 21069663
- [8]Duley L, Matar HE, Almerie MQ, Hall DR. Alternative magnesium sulphate regimens for women with pre-eclampsia and eclampsia Cochrane Database Syst Rev, 2010.PMID 20687086
- [9]Roberge S, Nicolaides K, Demers S, Hyett J, Chaillet N, Bujold E. Aspirin for the prevention of preterm and term preeclampsia: systematic review and metaanalysis Am J Obstet Gynecol, 2018.PMID 29138036
- [10]Roberge S, Bujold E, Nicolaides KH. Meta-analysis on the effect of aspirin use for prevention of preeclampsia on placental abruption and antepartum hemorrhage Am J Obstet Gynecol, 2018.PMID 29305829
- [11]Rolnik DL, Wright D, Poon LC, et al. Aspirin versus Placebo in Pregnancies at High Risk for Preterm Preeclampsia N Engl J Med, 2017.PMID 28657417
- [12]Jayawardena L, Hsieh S, Liang C, Zhao Y, Bain J, Bhide A. Diagnosis and management of pregnancies complicated by haemolysis, elevated liver enzymes and low platelets syndrome in the tertiary setting Intern Med J, 2020.PMID 31062430
- [13]Abalos E, Cuesta C, Carroli G, et al. Pre-eclampsia, eclampsia and adverse maternal and perinatal outcomes: a secondary analysis of the World Health Organization Multicountry Survey on Maternal and Newborn Health BJOG, 2014.PMID 24641531
- [14]Abalos E, Cuesta C, Grosso AL, Chou D, Say L. Global and regional estimates of preeclampsia and eclampsia: a systematic review Eur J Obstet Gynecol Reprod Biol, 2013.PMID 23746796
- [15]Quist-Nelson J, Parker P, Ali A, Berghella V, Saccone G. Early magnesium discontinuation postpartum and eclampsia risk: A systematic review and meta-analysis Pregnancy Hypertens, 2024.PMID 39018830