Paediatrics · Paediatrics
Pneumonia in Children
Also known as Community-acquired pneumonia in children · Lower respiratory tract infection (LRTI) in children · Acute respiratory infection (ARI) · Childhood pneumonia · Atypical pneumonia in children · Lobar pneumonia · Bronchopneumonia
Pneumonia in children = inflammation of the lung parenchyma, the single leading infectious cause of under-5 mortality globally, responsible for ~700,000 deaths/year (≈14% of all under-5 deaths). The WHO operational definition is cough or difficulty breathing with fast breathing defined by age (over 50/min at 2-12 months, over 40/min at 12 months-5 years, over 20/min at over 5 years). WHO classifies severity into pneumonia (fast breathing only, treat at home with oral amoxicillin), severe pneumonia (lower chest wall indrawing, hospitalise), and very severe pneumonia (danger signs: inability to drink, convulsions, vomiting everything, severe malnutrition, grunting — IV/IM antibiotics urgently). Leading viral cause under 1 year = RSV. Leading bacterial cause = Streptococcus pneumoniae; Hib pneumonia has fallen dramatically with conjugate vaccination. Empirical treatment: oral amoxicillin 80-90 mg/kg/day divided twice daily for 5-7 days for non-severe pneumonia, IV ampicillin + gentamicin (or ceftriaxone) for severe/very severe disease. Complicated empyema requires chest drain ± fibrinolysis with tPA + DNase (MIST2) or VATS. Prevention: PCV13/PCV10, Hib conjugate, measles, influenza annual, exclusive breastfeeding 6 months, hand hygiene, indoor air-pollution reduction, complementary feeding with zinc and vitamin A per WHO.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Overview & Definition
Pneumonia in children is inflammation of the lung parenchyma, typically of infectious origin, producing cough, fever, respiratory distress (tachypnoea, indrawing, grunting, nasal flaring, head nodding), and parenchymal infiltrates on imaging.[24]
It is the leading infectious cause of death in children under 5 worldwide, ahead of acute gastroenteritis, malaria, and measles. The disease burden is concentrated in sub-Saharan Africa and South Asia, where access to vaccines, antibiotics, oxygen, and timely care is constrained.[1][2]
Clinical definition. In hospital and high-resource settings, pneumonia is a clinical-radiographic syndrome: fever, cough, tachypnoea, focal respiratory signs (crepitations, dullness, bronchial breathing, wheeze), and a new parenchymal opacity on chest X-ray. In low-resource and primary-care settings, where chest X-ray is unavailable, the WHO operational definition is used:[5]
"Pneumonia = cough or difficulty breathing plus fast breathing for age."[24]
This single bedside rule has underpinned two decades of reduction in pneumonia mortality at first-level facilities and is the framing every NEET-PG/INICET candidate must know.[24]
Aetiological framing. Pneumonia is caused by a wide range of viruses, bacteria, atypical organisms, and (rarely) parasites. The organism varies sharply by age, and the organism dictates the management (typical bacteria need a beta-lactam; atypical organisms need a macrolide; influenza needs a neuraminidase inhibitor if within 48 h).[5]
The disease is preventable in most cases. Pneumococcal conjugate vaccine (PCV10/PCV13), Hib conjugate vaccine, measles vaccination, annual influenza vaccination, exclusive breastfeeding for 6 months, hand hygiene, smoke-free indoors, and reduction of indoor air pollution are the WHO-anchored prevention pillars.[11][12][13]
Classification
Pneumonia in children is classified along three clinically useful axes: severity (the most important for treatment), pathology (lobar vs bronchopneumonia vs interstitial), and aetiology (typical bacterial, atypical, viral).[13]
By severity — WHO (the operational gold standard)
WHO PNEUMONIA
cough + fast breathing
- **Cough or difficulty breathing**, with **fast breathing** for age
- **2-12 months: over 50/min**
- **12 months-5 years: over 40/min**
- **Over 5 years: over 20/min**
- **No lower chest wall indrawing**, **no danger signs**
- **Home treatment** with oral amoxicillin 5-7 days
WHO SEVERE PNEUMONIA
lower chest wall indrawing
- Cough or difficulty breathing
- **Lower chest wall indrawing** (subcostal/intercostal retractions of the lower chest wall on inspiration)
- **Hospitalise**
- **IV/IM antibiotic**
- **SpO2 <90%** → supplemental oxygen
WHO VERY SEVERE PNEUMONIA
danger signs — emergency
- Any general danger sign:
- **Inability to drink**
- **Convulsions**
- **Vomiting everything**
- **Severe acute malnutrition**
- **Grunting** in young infants (also cyanosis, lethargy, severe dehydration)
- **Emergency**: IV/IM antibiotics, oxygen, supportive care
WHO fast-breathing thresholds and severity cut-offs
By pathology
Lobar pneumonia
confluent consolidation of a lobe
- Most often **Streptococcus pneumoniae**
- Complete alveolar filling with neutrophils, fibrin and red cells
- CXR: lobar opacity, air bronchograms
- Clinical: high fever, rigors, pleuritic pain, lobar signs
Bronchopneumonia
patchy peribronchial consolidation
- Bacteria (pneumococcus, Hib, S aureus), viral-bacterial co-infection
- Patchy consolidation around airways, often multilobar
- CXR: multifocal patchy infiltrates
- Most common pattern in infants and young children
Interstitial (atypical)
diffuse interstitial inflammation
- **Mycoplasma pneumoniae**, Chlamydophila pneumoniae, viruses (RSV, hMPV, influenza, parainfluenza)
- Inflammatory infiltrate in the interstitium without alveolar exudate
- CXR: bilateral diffuse interstitial infiltrates, hyperinflation
- Gradual onset, dry cough, wheeze, often afebrile or low-grade fever
By aetiology — typical, atypical, viral
TYPICAL BACTERIAL
Streptococcus pneumoniae, Hib, S aureus
- **S pneumoniae** — leading bacterial pathogen; lobar, bronchopneumonia
- **Haemophilus influenzae type b** — collapsing lobar pattern in unvaccinated children; now rare where Hib conjugate vaccine is in use
- **Staphylococcus aureus** — post-influenza or in PVL-endemic settings; pneumatocele, empyema, necrotising pneumonia; high mortality
- **Group B Streptococcus, E coli, Listeria monocytogenes** — neonates
- **Klebsiella, Pseudomonas** — hospital-acquired, immunocompromised
ATYPICAL (NON-RESPONSE TO β-LACTAMS)
Mycoplasma, Chlamydophila, Bordetella
- **Mycoplasma pneumoniae** — commonest cause of community-acquired pneumonia in school-age (>5 yr) children; intracellular; needs **macrolide**
- **Chlamydophila pneumoniae** — school-age, often clinically silent
- **Bordetella pertussis** — infants and unvaccinated; paroxysmal cough, lymphocytosis, apnoeas in infants
- **Chlamydia trachomatis** — neonates 4-12 weeks; afebrile, staccato cough, conjunctivitis, eosinophilia
VIRAL
RSV, influenza, hMPV, parainfluenza
- **Respiratory syncytial virus (RSV)** — leading viral cause in children under 5; bronchiolitis and pneumonia in infants
- **Rhinovirus** — most frequent respiratory virus but usually mild URTI; severe disease in infancy
- **Influenza A/B** — seasonal; pneumonia in children or post-influenza staphylococcal superinfection
- **Human metapneumovirus (hMPV)** — RSV-like
- **Parainfluenza 1-3** — croup; type 3 pneumonias in infants
By age — the most useful clinical axis
| Age group | Common pathogens (viral) | Common pathogens (bacterial) | Atypical |
|---|---|---|---|
| Newborn (0-30 days) | RSV, enterovirus | Group B Streptococcus, E coli, Listeria monocytogenes | Chlamydia trachomatis (late-onset) |
| 1-3 months | RSV, rhinovirus | Bordetella pertussis, Streptococcus pneumoniae, Staphylococcus aureus | Chlamydia trachomatis (afebrile, staccato cough, 4-12 wk) |
| 3 months-5 years | RSV, rhinovirus, parainfluenza, influenza, hMPV, bocavirus | Streptococcus pneumoniae, Hib, Mycoplasma pneumoniae (over 3 yr), Staphylococcus aureus (incl. PVL) | Mycobacterium tuberculosis |
| Over 5 years (school age) | Influenza, rhinovirus | Streptococcus pneumoniae, Staphylococcus aureus | Mycoplasma pneumoniae (most common), Chlamydophila pneumoniae |
Epidemiology & Risk Factors
Global burden
Pneumonia has been the leading infectious killer of children under 5 for decades. The GBD 2019 study estimates ~700,000 under-5 deaths annually attributable to lower respiratory infections (LRIs) — about 14% of all under-5 deaths globally — with the bulk falling in sub-Saharan Africa and South Asia.[2][3]
Global pneumonia epidemiology (GBD 2019-2021)
Trend over time
Under-5 pneumonia mortality has fallen substantially over the past three decades — from over 2 million/year in 1990 to ~700,000/year by 2019 — driven by:[24]
- Conjugate vaccines — PCV, Hib — the single largest biomedical lever.[11][12][22]
- Expanded oxygen access — universal pulse oximetry and oxygen concentrators at first-level facilities.[24]
- Standardised case management (WHO IMCI/IMNCI) — amoxicillin for WHO pneumonia.[7][8][24]
- Improved nutrition — exclusive breastfeeding for 6 months, micronutrient supplementation, and reduction of severe acute malnutrition.
- Socioeconomic change — urbanisation, clean-fuel cooking, reduced household crowding.
Even so, the burden plateaued in many countries during the COVID-19 era and health-system disruption; the GBD 2021 update shows a rebound of LRIs to levels comparable to pre-pandemic estimates.[3]
Aetiological epidemiology by age
INFANTS UNDER 1 YEAR
viral dominance, RSV leader
- **RSV** is the leading viral pathogen
- **Streptococcus pneumoniae** is the leading bacterial pathogen (still)
- Rhinovirus, parainfluenza, hMPV, bocavirus, enterovirus all common
- **Bordetella pertussis** in unvaccinated/partially vaccinated infants — apnoeas
- **Chlamydia trachomatis** in 4-12 week olds — afebrile, staccato cough
1-5 YEARS
transitional — pneumococcus + early atypical
- **Streptococcus pneumoniae** still dominates bacterial
- **Staphylococcus aureus** including PVL-positive strains — pneumatocele and necrotising pneumonia
- **Hib** in unvaccinated populations; near-eliminated where conjugate vaccine used
- **Mycoplasma pneumoniae** becomes common from age 3 onward
- Viruses (RSV, influenza, hMPV) still cause up to 60-70% of pneumonia in this age group
OVER 5 YEARS (SCHOOL AGE)
atypical rises, viral still common
- **Mycoplasma pneumoniae** is the leading pathogen overall
- **Chlamydophila pneumoniae** rises in this age band
- **Streptococcus pneumoniae** still important
- Less common: **S aureus**, **S aureus PVL** in post-influenza superinfection
- **Influenza A/B** peaks each winter
Vaccine impact
The conjugate vaccines have transformed childhood pneumonia epidemiology. The Watt 2009 Lancet analysis estimated Hib caused ~8% of pneumonia deaths in children under 5 globally (in the pre-vaccine era); after Hib conjugate introduction, Hib disease in vaccinated populations collapsed.[10][14] PCV10/PCV13 has produced parallel drops in invasive pneumococcal disease and radiologically confirmed pneumonia in vaccinated cohorts.[11][12] The Hanquet 2019 Thorax study confirmed a substantial indirect (herd) effect on older unvaccinated cohorts across Europe.[22]
Risk factors
Child-level risk factors:[2]
- Age: peak incidence 2-12 months; mortality highest in 2-12 month age band.
- Prematurity / low birth weight.
- Non-breastfed, or exclusively breastfed under 6 months.
- Severe acute malnutrition (SAM) — multiplies pneumonia mortality.
- Immunodeficiency — congenital, HIV, chemotherapy, transplantation.
- Chronic lung disease of prematurity (BPD).
- Congenital heart disease, especially cyanotic.
- Sickle-cell disease / functional asplenia — risk of pneumococcal sepsis.
- Recurrent aspiration — neurodisability, GERD, neuromuscular disorders.
- Wheezing — concurrent asthma or viral-triggered wheeze.[3]
Household / environmental risk factors:[2]
- Indoor air pollution — solid-fuel cooking (biomass), second-hand tobacco smoke.
- Household crowding.
- Lack of immunisation.
- Lower socioeconomic status — multiple pathways (poor nutrition, crowding, lower care-seeking).[2]
Care-seeking factors:[2]
- Delayed presentation.
- Inadequate access to oxygen and pulse oximetry.
- Self-medication or inappropriate antibiotics.[2]
Pathophysiology
The two archetypes
The behaviour and treatment of childhood pneumonia are dominated by two anatomical-pathological archetypes — alveolar consolidation (typical bacterial) and small-airway/airway-centred interstitial disease (viral and atypical). They have different microanatomy, different physiology, different imaging, and different first-line antibiotic rationale.[7]
Bacterial alveolar consolidation
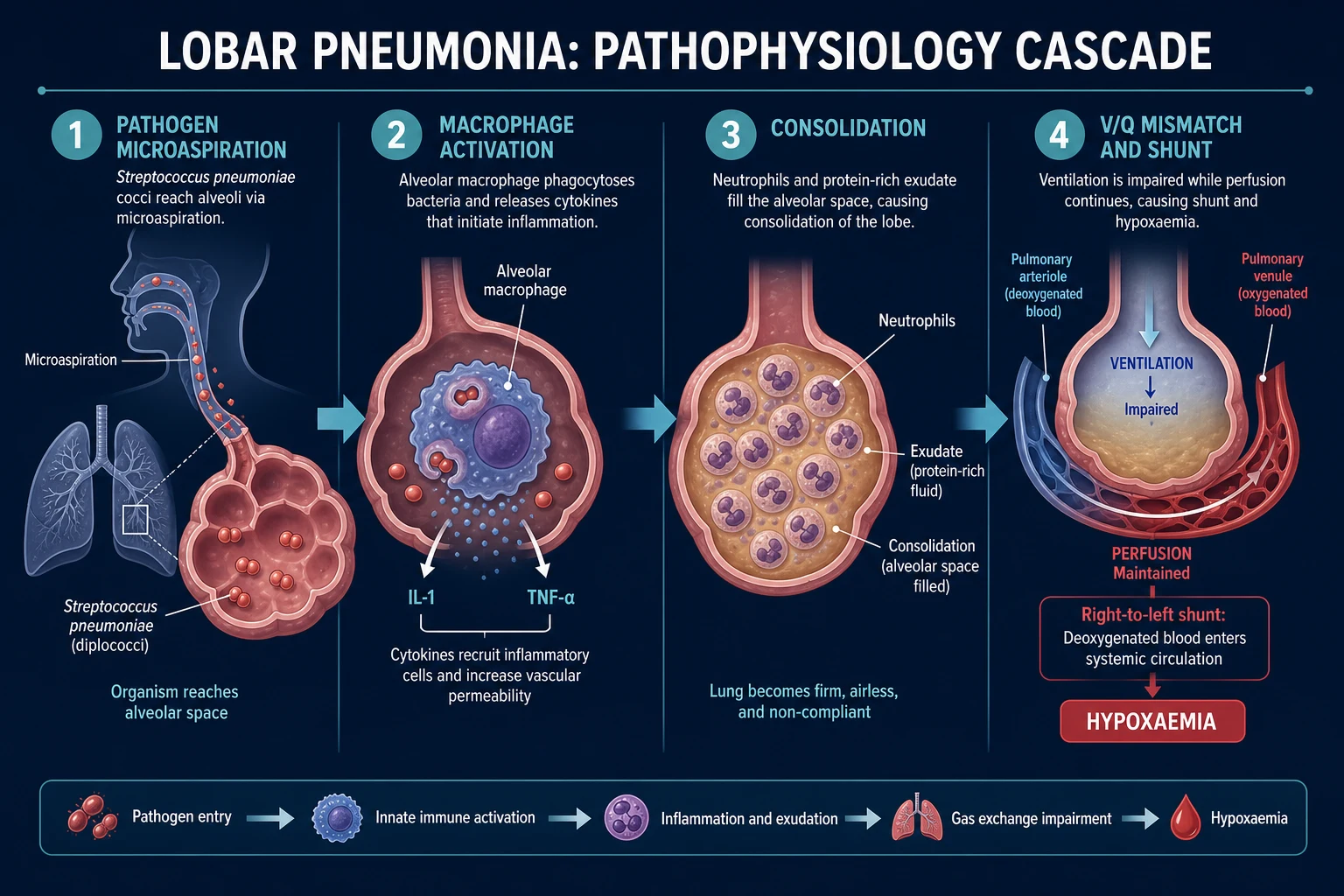
The S pneumoniae model best illustrates the cascade:[11]
- Nasopharyngeal colonisation — pneumococcus colonises the upper airways in roughly 20-40% of healthy children at any time. Colonisation is harmless unless the host's defences fail.
- Micro-aspiration — overflow into the lower respiratory tract occurs physiologically; effective mucociliary clearance and alveolar macrophage function normally contain it.
- Failure of defence — viral upper-respiratory infection (especially influenza), malnutrition, immune suppression, or no prior immunological experience (infants) allow the organism to establish in alveoli.
- Alveolar exudate — exudation of neutrophils, fibrin and red cells into the alveolar air space; this consolidates the alveolus and replaces air with fluid/cells.
- Spread — through the pores of Kohn and canals of Lambert within the lobe (lobar) or via centrilobular airways (bronchopneumonia).
- Impaired gas exchange — perfusion continues but ventilation drops in consolidated regions → shunting → hypoxaemia.
- Systemic signs — pyrogens (IL-1, IL-6, TNF) drive fever, rigors, anorexia, tachycardia.[1]
Viral bronchiolitis and viral pneumonia
The RSV model illustrates viral lower respiratory disease:[1]
- Nasopharyngeal inoculation → viral replication in ciliated epithelial cells.
- Cellular cytotoxicity and immune response — epithelial necrosis, submucosal oedema, lymphocytic infiltrate.
- Mucus hypersecretion and peribronchiolar inflammation — combine with exudate in the small airways.
- Small-airway plugging — produces air trapping and hyperinflation distal to plugs (ball-valve mechanism).
- Interstitial mononuclear infiltrate — interstitial thickening; alveolar air preserved.
- Wheeze and crackles — mixed obstruction and inflammation.
- Hypoxaemia — primarily V/Q mismatch with air-trapping; alveolar collapse in more severe disease.[5]
Viral infection is also the most important risk for secondary bacterial pneumonia: influenza damages airway epithelium and impairs mucociliary clearance, allowing bacterial superinfection (Streptococcus pneumoniae, Staphylococcus aureus) 5-10 days into the illness.[5]
Atypical (interstitial) pneumonia
Mycoplasma pneumoniae binds to sialic acid residues on respiratory epithelium via the P1 adhesin, causes ciliary dysfunction, and produces a subepithelial lymphocytic infiltrate. Bacteria are intracellular and cannot be cultured on routine media, which is why macrolides (which concentrate intracellularly) are required.[16]
The clinical manifestation is subacute: dry cough, low-grade fever, headache, and the x-ray-physical dissociation — interstitial infiltrates on imaging disproportionate to the physical findings.[21]
Necrotising pneumonia — the dangerous complication
Necrotising pneumonia is parenchymal necrosis with multiple thin-walled cavities, pneumatoceles and frequently empyema. It is most commonly caused by:[21]
- Streptococcus pneumoniae serotype 19A (not covered by older PCV7),
- Staphylococcus aureus, particularly Panton-Valentine leukocidin (PVL)-positive strains — epidemic in parts of Europe and elsewhere;[21]
- Less commonly, H. influenzae and Klebsiella.
Complications pathophysiology
| Complication | Pathophysiology |
|---|---|
| Pleural effusion / empyema | Inflammation-driven fluid in pleural space; exudate when pleural fluid protein/LDH ratios meet Light's criteria; pH <7.2, glucose <3.3 mmol/L and LDH over 1000 mark progression to empyema needing drainage[20] |
| Pneumothorax | Rupture of bullae or blebs into pleural space |
| Pneumatocele | Thin-walled air-filled cyst in the lung parenchyma — typically 2-4 weeks after bacterial pneumonia; usually resolves spontaneously[21] |
| Lung abscess | Cavity with pus; aspiration or post-pneumonic; common anaerobes in older children |
| Necrotising pneumonia | Multiple small cavitations; PVL-positive S aureus or serotype 19A pneumococcus[21] |
| Bronchiectasis | Permanent airway dilation following repeated or severe infection |
| Septicaemia / septic shock | Spread of organisms into bloodstream |
| ARDS | Severe parenchymal inflammation → non-cardiogenic pulmonary oedema |
Clinical Presentation
The textbook triad is cough, fever, and tachypnoea — but infants often present atypically, and older children may have subtle features. A complete history must establish:[22]
- Onset and tempo — abrupt = typical bacterial; gradual = atypical/viral.
- Cough character — dry, productive; paroxysms ± whoop; post-tussive vomiting (pertussis).
- Fever — height and pattern; rigours suggest typical bacterial.
- Breathing difficulty — fast breathing, indrawing, grunting, nasal flaring, head nodding, accessory muscle use.
- Feeding / hydration — decreased feeding, vomiting, reduced wet nappies, lethargy.
- Immunisation history — RSV, influenza, PCV, Hib, measles, pertussis, BCG.
- Exposure — household illness, daycare, family TB, fumes/biomass cooking.
- Past medical history — prematurity, BPD, congenital heart disease, recurrent pneumonia (immunodeficiency, malformation, aspiration).
- Drugs / allergies, especially prior antibiotic exposure.
- Skin rash — scarlatiniform (S aureus scarlet fever), maculopapular (measles), vesicular (varicella), urticarial.[21]
Cardinal signs of respiratory distress
Signs of respiratory distress in a child
Typical pattern by aetiology
TYPICAL BACTERIAL (eg pneumococcus)
high fever, lobar signs
- Abrupt onset, high-grade fever, rigors
- Lobar or focal consolidation: dullness, bronchial breathing, crepitations
- Pleuritic chest pain (older children)
- Toxic appearance, poor feeding, dehydration
- Pustular / bulbar conjunctivitis (rare, S pneumoniae)
- CXR: lobar consolidation, air bronchograms
ATYPICAL (Mycoplasma, Chlamydophila)
subacute, dry cough, afebrile
- Gradual onset over days
- Dry, hacking cough; headache, myalgia
- Low-grade or no fever
- Wheezing and crackles out of proportion to systemic signs
- Maculopapular rash, cold agglutinins (~50%)
- CXR: patchy, often bilateral interstitial infiltrates
VIRAL (RSV, influenza)
coryza, wheeze, fine crackles
- Rhinorrhoea, cough, low-grade fever
- Wheezing in infants (especially RSV)
- Tachypnoea, indrawing, poor feeding
- Diffuse fine crackles and wheeze
- CXR: bilateral perihilar interstitial infiltrates and hyperinflation
- Often self-limiting in 5-7 days; antibiotics avoid
Chlamydia trachomatis in young infants (4-12 weeks)
Classic profile: afebrile or low-grade, staccato cough (paroxysmal, single-cycle cough), conjunctivitis, tachypnoea, scattered crepitations, normal or mild interstitial CXR, peripheral eosinophilia. History of maternal STI or untreated maternal conjunctivitis. Treatment: oral erythromycin 50 mg/kg/day in 4 divided doses for 14 days (or azithromycin 10 mg/kg/day for 5 days).[24]
Staph aureus pneumonia (and PVL-positive)
- Post-influenza superinfection (5-10 days into influenza).
- Abrupt onset, high fever, pleuritic pain, rapidly progressive.
- Pneumatoceles, empyema, necrotising pneumonia, pyopneumothorax.
- PVL-positive strains in particular progress rapidly with necrotic lung lesions and are highly lethal if not treated aggressively.[21]
Bordetella pertussis
- Paroxysmal cough ending in inspiratory whoop, post-tussive vomiting, subconjunctival haemorrhage.
- Apnoea as the cardinal feature in infants under 6 months.
- Peripheral blood: marked lymphocytosis (often over 20 ×10⁹/L).
- Confirm with nasopharyngeal swab PCR.
- Treat with azithromycin or erythromycin.[7]
Measles pneumonia
- Coryza, cough, conjunctivitis (the 3 Cs) + Koplik spots → maculopapular rash.
- Pneumonia may be measles-virus pneumonitis or secondary bacterial superinfection (S pneumoniae, S aureus, H influenzae).
- Vitamin A 200,000 IU (over 12 months) or 100,000 IU (under 12 months) × 2 days empirically, then repeat in 4 weeks.[13]
Atypical presentations — the examiner's favourites
INFANT UNDER 3 MONTHS
non-specific presentation
- Poor feeding, lethargy, hypothermia more than fever
- Apnoea (especially pertussis or RSV)
- Subtle grunting instead of cough
- Tachycardia out of proportion to fever — early warning
- Bulging fontanelle if meningismus is missed
SEVERE ACUTE MALNUTRITION
signs blunted, mortality high
- **Hypothermia rather than fever**
- Subtle indrawing — look hard
- Poor or no cough reflex
- Hypoglycaemia is common — check glucose
- Mortality 4-5× higher than well-nourished peers
IMMUNOCOMPROMISED
broad differential
- Fever with hypoxia disproportionate to physical signs
- CXR may be normal early (Pneumocystis)
- Diffuse infiltrates — PJP, CMV, atypical mycobacteria
- Take a thorough exposure, antibiotic, and prophylaxis history
Examining the chest in a child
- Look — tachypnoea, indrawing, nasal flaring, head nodding, asymmetry of chest expansion, scars (chest tubes), central cyanosis, clubbing (chronic pneumonia — consider bronchiectasis, immunodeficiency).
- Feel — tracheal position (push = effusion/mass; pull = collapse), chest expansion (decreased on consolidated side), tactile vocal fremitus (increased over consolidation, decreased over effusion).
- Percuss — dull (consolidation, effusion); hyper-resonant (pneumothorax, large consolidation with air trapping).
- Listen — crackles (crepitations) over consolidation; bronchial breathing with increased vocal resonance = consolidation; absent breath sounds and dullness = effusion; wheeze = bronchospasm (viral, foreign body, asthma).[24]
Differential Diagnosis
The "pneumonia" label is potentially applied to many non-pneumonic conditions. A structured differential is mandatory because missing it changes outcome.[7]
OTHER LOWER-RESPIRATORY PATHOLOGY
airway-centric, not parenchymal
- **Bronchiolitis** — age 1-12 months, URTI prodrome, diffuse wheeze, fine crackles, hyperinflation; RSV PCR positive; no focal signs
- **Asthma** — recurrent episodes, atopic family history, wheeze-dominant, response to bronchodilators; no fever or imaging opacity
- **Croup (parainfluenza laryngotracheobronchitis)** — barking cough, inspiratory stridor
- **Bronchitis** — cough productive of sputum, no focal CXR opacity, no hypoxaemia
- **Pertussis** — paroxysmal cough, whoop, lymphocytosis
PLEURAL & MEDIASTINAL
tracheal deviation, percussion sign
- **Pleural effusion** — primary (TB, malignancy) or parapneumonic; reduced expansion, stony dullness, absent breath sounds, reduced vocal resonance
- **Pneumothorax** — sudden onset pleuritic pain, hyper-resonant, decreased breath sounds, deviated trachea away
- **Mediastinal mass** — tracheal compression, stridor, engorged neck veins
UPPER-RESPIRATORY & ASPIRATION
history keys
- **Foreign-body aspiration** — sudden cough, asymmetric wheeze or hyperexpansion on CXR — left main bronchus (right in infants)
- **Retropharyngeal abscess / croup / epiglottitis** — barking cough, stridor, drooling, neck pain
SYSTEMIC INFECTIONS MIMICKING PNEUMONIA
non-respiratory source
- **Sepsis** — non-localising signs, tachycardia, prolonged CRT, shock
- **Meningitis / encephalitis** — bulging fontanelle, neck stiffness, convulsion, irritability
- **Urinary-tract infection** — infants present with vomiting, fever; always check urinalysis
- **Malaria** — seasonality, hepatosplenomegaly, exchange transfusion criteria
- **Typhoid** — relative bradycardia, rose spots, hepatosplenomegaly
NON-INFECTIOUS MIMICS
history and exam matter
- **Cardiogenic pulmonary oedema** — gallop, hepatomegaly, jugular venous distension (rare in children)
- **Inhaled foreign body** (often missed for weeks)
- **Bronchopulmonary dysplasia / BPD** — chronic oxygen, BPD ex-preterm
- **Cystic-fibrosis exacerbation** — recurrent pneumonia, clubbing, GI symptoms, family history
- **Vasculitis / autoimmune** — Kawasaki shock, SLE pneumonitis
Clinical & Bedside Assessment
The WHO approach is the operational gold standard, and every examiner will expect it reproduced verbatim.[24]
WHO assessment — the key facts
RAPID
Count respiratory rate over 60 s in young infants; >50/min at 2-12 months, >40/min at 1-5 years, >20/min over 5 years = fast breathing
Indrawing (subcostal/intercostal), grunting, nasal flaring, head nodding, cyanosis
SpO2 by pulse oximeter; <90% indicates hypoxaemia needing oxygen
CXR if hospitalised; blood culture if severe; viral PCR; sputum if older child
Inability to drink, convulsions, vomiting everything, severe malnutrition, grunting in a young infant = very severe pneumonia
WHO assessment sequence (use this at first-level facilities and in any exam):[24]
- CHECK FOR DANGER SIGNS — if any, the child has VERY SEVERE pneumonia. Move to emergency care.
- COUNT respirations over a full minute (a young infant's RR is labile; count again if borderline).
- Look for chest indrawing — subcostal/intercostal retractions on inspiration with the chest wall visibly sinking between/below the ribs.
- Listen for grunting — soft, audible expiratory vocalisation in young infants (a sign of impending respiratory failure).
- Stridor, wheeze, or general danger signs (vomiting everything, convulsions, lethargy/unconsciousness).[24]
WHO severity classification — reproduced exactly
| Sign | Pneumonia (home) | Severe pneumonia (hospitalise) | Very severe pneumonia (emergency) |
|---|---|---|---|
| Cough or difficulty breathing | yes | yes | yes |
| Fast breathing | yes | yes or no | yes or no |
| Lower chest wall indrawing | no | yes | yes or no |
| General danger sign | no | no | yes (any) |
| Treatment | Oral amoxicillin home | IV/IM antibiotics, hospital | IV/IM antibiotics, oxygen, emergency |
Additional bedside findings that matter
- Pulse oximetry: target 94-98% in non-cardiac children; <90% triggers oxygen supplementation.
- Capillary refill >2 s — coexisting shock, poor perfusion.
- Hydration — sunken eyes, reduced tears, dry mucosa, decreased urine output, weight change.
- Nutritional status — weight, mid-upper-arm circumference (MUAC, SAM if <11.5 cm in 6-59 months).
- Temp — fever >38.5 °C or hypothermia <36 °C.
- Chest signs — see Examining the chest above.[7]
Investigations
Most childhood pneumonia is a clinical diagnosis. Investigations are risk-stratified.[24]
Imaging
CXR PA + lateral
the cornerstone if available
- Standard if the child is hospitalised or atypical
- Findings: lobar/bronchopneumonic consolidation, interstitial infiltrates, effusion, pneumatocele
- Can confirm empyema (fluid level), pneumothorax (lung-edge, no lung markings beyond), abscess
- WHO guidance: **do not routinely request CXR for WHO pneumonia** (outpatient) — it doesn't change management; reserve for hospitalised or complicated cases
- Lateral is particularly useful for retrocardiac consolidation, effusion, hilar nodes
Chest ultrasound
effusion + pneumothorax
- Excellent for pleural effusion (loculation, depth) — provides safe thoracentesis guidance
- Detects small pneumothoraces and consolidations at the bedside
- Increasingly first-line for parapneumonic effusion assessment
CT chest
complications, mass
- Reserved for complications (necrotising pneumonia), suspected mass, congenital malformation
- Routine CT is excessive in children
Microbiology
Blood culture
yield under 10%
- Standard for hospitalised severe/very severe pneumonia
- Yield typically low (≤10%) in paediatric pneumonia — but positive in young infants more often
- Always take BEFORE antibiotics
- Send culture for: S pneumoniae, S aureus, H influenzae, Enterobacterales
Sputum Gram stain + culture
older children only
- Useful in school-age children who can produce
- Not reliable in infants who swallow secretions
- Less used than in adults
Nasopharyngeal aspirate (NPA) viral PCR
RSV, influenza A/B, hMPV
- Multiplex respiratory PCR: detects RSV, influenza A/B, parainfluenza 1-4, hMPV, rhinovirus, enterovirus, adenovirus
- Influenza PCR drives oseltamivir decision (especially in 48 h window)
- Do NOT replace chest X-ray
Pleural fluid analysis
Light's criteria + pH
- Light's criteria → exudate
- **pH <7.2** OR **glucose <3.3 mmol/L** OR **LDH >1000 IU/L** OR **pus** OR **positive Gram stain/culture** → **complicated parapneumonic effusion / empyema** → chest drain urgently
- Send protein, LDH, glucose, pH, cell count, Gram stain, culture
- Send adenosine deaminase (ADA) if TB suspected
Bloods
- FBC: leucocytosis with left shift suggests bacterial; lymphocytosis suggests pertussis or atypical.
- CRP / procalcitonin (PCT): CRP>100 mg/L, PCT>2 ng/mL — favours bacterial; PCT more specific. Not discriminative in infants or after antibiotic pretreatment.
- U&E / venous blood gas: hyponatraemia (SIADH with pneumonia), raised creatinine (HUS), metabolic acidosis (severe sepsis).
- Glucose: hypoglycaemia in SAM or sepsis.
- Lactate: >2 mmol/L — sepsis, poor perfusion.
- HIV testing: in severe or recurrent pneumonia, in high-prevalence settings, or if WHO guidance supports.
- Tuberculin test (TST or IGRA / QuantiFERON-TB Gold): when TB pneumonia is suspected — persistent symptoms, contact with TB, malnutrition, inconclusive CXR.
- Blood culture × 1 set minimum before antibiotics.
- Arterial blood gas / capillary gas: when the child is severely hypoxaemic, in impending respiratory failure, or for guiding HFNC/CPAP escalation.[5]
Other
- Urine pneumococcal antigen and Legionella urinary antigen — older child, atypical presentation, outbreak setting.
- Serology — cold agglutinins and Mycoplasma IgM (4-fold rise, or single positive IgM with clinical picture).
- Bronchoscopy with bronchoalveolar lavage (BAL): immunocompromised, ventilator-associated, refractory pneumonia.
- ECG and echocardiogram: when myocarditis or pericardial effusion is considered.
- Sputum AFB and GeneXpert MTB/RIF: when TB is suspected.[17]
Management — Resuscitation
The first minutes of very severe pneumonia are about airway, breathing, and circulation — ABCDE — not antibiotics.[5]
Resuscitation sequence for very severe pneumonia
1. Assess and position
2. Oxygen
3. IV/IO access and bloods
4. Empirical IV/IM antibiotics
5. Glucose check
6. Fluids cautiously
7. Continuous monitoring
Oxygen delivery — escalation ladder
Nasal cannula
mild hypoxaemia
- 1-2 L/min in young children
- Well-tolerated, allows feeding
- Humidification recommended in infants
Facemask / simple mask
moderate hypoxaemia
- 5-10 L/min
- FiO2 35-60% depending on flow
- Distress in young children — sedation/calming may be needed
High-Flow Nasal Cannula (HFNC)
escalation beyond standard
- Heated, humidified 1-2 L/kg/min, FiO2 titrated to SpO2
- Reduces work of breathing; well-studied in bronchiolitis
- Increasing evidence for moderate-to-severe pneumonia in children
CPAP
recruitment + support
- Recruits collapsed alveoli, reduces WOB, splints airways
- PEEP 5-10 cm H2O; trial of 30-60 min
- Indicated when standard oxygen fails or persistent SpO2 <90% on SpO2 despite FiO2 >40%
Intubation and mechanical ventilation
last-line respiratory support
- Severe hypoxaemia (PaO2 <60 mmHg on FiO2 >0.6), severe respiratory acidosis (pH <7.2 with rising PaCO2), apnoeas, exhaustion, airway compromise
- Lung-protective ventilation (low tidal volume 5-7 mL/kg); permissive hypercapnia acceptable
Management — Definitive & Stepwise
The pillars are (1) oxygen, (2) appropriate antibiotic, (3) supportive care, (4) fluids + nutrition, (5) monitoring, and (6) prevention of transmission. For complicated disease, (7) procedural management of empyema, (8) necrotising pneumonia care, and (9) follow-up imaging.[13]
Empirical antibiotic selection — by severity
WHO PNEUMONIA (home)
oral amoxicillin
- **Amoxicillin 80-90 mg/kg/day orally in 2-3 divided doses × 5 days** — the WHO-recommended dose is the upper end (80-90 mg/kg/day) to overcome pneumococcal resistance
- Replace with **cefuroxime axetil** if amoxicillin failure or type-1 hypersensitivity (non-anaphylactic)
- Avoid macrolides as first-line in 2-12 months (uncertain age for Mycoplasma)
- Reassess in 48-72 h — if no improvement, escalate
WHO SEVERE PNEUMONIA (hospital, no danger signs)
IV ampicillin + gentamicin OR oral amoxicillin
- **Ampicillin 50 mg/kg IV q6h + Gentamicin 7.5 mg/kg IV/IM q24h**
- Or oral amoxicillin 80-90 mg/kg/day for fully oral pathway if WHO standard
- Change to **Ceftriaxone 50-80 mg/kg/day IV/IM once daily** if poor response at 48 h
- ADD macrolide if atypical suspected (>3 yr, clinical features)
- Add **Vancomycin 15 mg/kg IV q6h** if MRSA suspected (PVL, post-influenza collapse, regional prevalence)
WHO VERY SEVERE PNEUMONIA (emergency)
broad-spectrum IV/IM
- **Ampicillin + Gentamicin** base regimen (above)
- Add **Cefotaxime/Ceftriaxone** if septicaemia, young infant, or poor response
- Add **Macrolide** empirically for atypical coverage
- Add **Vancomycin/Linezolid** for suspected MRSA or PVL-positive S aureus
- Consider **Oseltamivir** for influenza in 48 h window
Paediatric empirical antibiotic doses for pneumonia
Atypical-pathogen consideration
When a school-age child has persistent dry cough, bilateral wheeze or crackles, or inadequate response to a beta-lactam at 48-72 hours, add a macrolide or switch to a macrolide:[16][17][23]
- Azithromycin 10 mg/kg once daily for 3 days — better tolerated than erythromycin.
- Clarithromycin 15 mg/kg/day in 2 divided doses for 7-10 days.
- Erythromycin 50 mg/kg/day in 4 divided doses for 14 days — preferred for pertussis exposure, neonate.[16]
Supportive care — the rest of the bundle
Oxygen and respiratory support
obvious but sometimes forgotten
- SpO2 target 94-98%; <90% triggers oxygen
- Humidified for infants
- Half-hourly position changes; prone in infants
- Encourage age-appropriate activity
Fluids and nutrition
continue feeding, correct dehydration
- Continue breastfeeding and age-appropriate feeding during recovery
- Oral intake preferable; if not tolerating, NG feeds
- IV fluids ONLY for shock, inability to feed, or vomits everything; minimal maintenance; avoid overload (SIADH risk)
- Hypoglycaemia (<3 mmol/L): 2 mL/kg 10% dextrose bolus then maintenance
Antipyretics and comfort
paracetamol or ibuprofen
- **Paracetamol 15 mg/kg PO/PR q4-6h** PRN
- **Ibuprofen 10 mg/kg PO q6-8h** if >6 months
- Avoid aspirin (Reye)
- Avoid regular schedule — only when symptomatic
Bronchodilators and steroids
use selectively
- Bronchodilators (salbutamol) ONLY if clear wheeze/asthma overlap or viral-induced wheeze
- Routine salbutamol in non-wheezy pneumonia: NO
- Corticosteroids: not routine in childhood pneumonia
- Dexamethasone 0.15 mg/kg PO/IV q6h may be considered in severe pneumonia with high inflammatory burden — evidence mixed in children
- Dex. for severe hypoxaemic pneumonia in highly-selected populations — expert-only
Complications — when the bundle isn't enough

Pleural effusion and empyema — the most common pneumonia complication.[20]
- Uncomplicated parapneumonic effusion: 7-10 days of IV antibiotics; serial ultrasound; usually resolves.
- Complicated parapneumonic effusion / empyema: aspiration yields pH <7.2, glucose <3.3 mmol/L, LDH >1000 IU/L, pus, or positive culture/Gram stain. Action: chest drain (small-bore 8-14 Fr preferred) ± intrapleural fibrinolysis.
- Intrapleural fibrinolysis (MIST2 regimen): tPA 10 mg + DNase 5 mg intrapleural twice daily for 3 days — improves drainage success over either agent alone or streptokinase.[19]
- VATS (video-assisted thoracoscopic surgery) — if fibrinolysis fails, or if the child is deteriorating; safe and effective in children.[18]
Pneumothorax — needle aspiration (2nd intercostal space mid-clavicular line or 4th-5th intercostal space anterior axillary line for paediatric small-bore drains), then small-bore chest drain in the triangle of safety.[18]
Pneumatocele — usually conservative; serial CXR; intervention only if large and symptomatic.[18]
Lung abscess — prolonged IV antibiotics (4-6 weeks) targeting anaerobes, S aureus, S pneumoniae; percutaneous drainage if persistent.[11]
Necrotising pneumonia — prolonged IV antibiotics (often 4-6 weeks) covering S aureus (incl. PVL — vancomycin/linezolid if MRSA), pneumococcus, anaerobes; supportive management; surgical lobectomy rarely needed.[5]
When to escalate, when to step down
Reassessment loop
48-72 h after starting antibiotics
If not improving at 48 h
If deteriorating rapidly
Discharge planning
Vaccination and prevention
VACCINES
preventive armour
- **PCV13** (or PCV10) — schedule depends on country; protects against 13/10 pneumococcal serotypes including those most associated with pneumonia
- **Hib conjugate vaccine** — protects against H. influenzae type b
- **Measles vaccination** — prevents measles pneumonia
- **Pertussis vaccination (DTaP/Tdap)** — protects against pertussis pneumonia
- **Influenza vaccination** — annual, especially high-risk groups
- **RSV preventive antibodies (nirsevimab / palivizumab)** — single IM dose in infancy in selected guidelines
NUTRITION
evidence-based
- Exclusive breastfeeding for 6 months
- Complementary feeding from 6 months with adequate protein/energy
- Vitamin A supplementation in deficiency and measles (as per WHO)
- Zinc supplementation in diarrhoea (relates to pneumonia indirectly)
- Prevention and treatment of severe acute malnutrition
ENVIRONMENT
household & community
- Reduction of household air pollution (clean cooking fuels)
- Avoid tobacco smoke exposure (passive smoking)
- Hand hygiene
- Reduction of household crowding
- Prompt care-seeking; community case-management of WHO pneumonia
Specific Subtypes & Scenarios
Neonatal pneumonia
| Organism | Onset | Special features | Treatment |
|---|---|---|---|
| Group B Streptococcus (GBS) | early-onset D1-7 | respiratory distress, sepsis, often from vertical transmission | Ampicillin + aminoglycoside (above) |
| E coli | early/late | sepsis, UTI | Ampicillin + aminoglycoside |
| Listeria monocytogenes | early/late | maternal exposure, meningitis | Ampicillin + aminoglycoside |
| Chlamydia trachomatis | late-onset 2-12 wk | afebrile, staccato cough, conjunctivitis, eosinophilia | Erythromycin / azithromycin |
| RSV / other viruses | any | cough, wheeze, apnoea in preterms | supportive; consider ribavirin in severe immunocompromised |
Staphylococcal pneumonia (PVL-positive and MSSA)
- Often follows influenza, measles, or post-tonsillectomy.
- Pneumatoceles, empyema, pyopneumothorax, necrotising pneumonia.
- Treat: IV anti-staphylococcal beta-lactam (flucloxacillin) ± vancomycin/linezolid if MRSA; chest drain for empyema; prolonged IV course 4-6 weeks.[21]
Mycoplasma pneumoniae — rising
- Commonest pathogen in school-age children with community-acquired pneumonia.[17]
- Can complicate Stevens-Johnson syndrome, cold agglutinin haemolytic anaemia, GBS, polyarthritis.
- Macrolide resistance is rising; consider tetracycline/doxycycline in children >8 years as an alternative.[16][23]
Tuberculous pneumonia
- Subacute presentation (over 2-4 weeks), weight loss, night sweats, persistent CXR opacity with hilar adenopathy.
- Often primary complex: Ghon focus + hilar lymphadenopathy.
- Diagnosis: clinical + CXR + Tuberculin test (or IGRA in older children) + microbiology (gastric aspirate or BAL GeneXpert MTB/RIF).
- Standard 6-month TB regimen (isoniazid + rifampicin × 6 months; pyrazinamide × 2 months; ± ethambutol).[7]
Necrotising pneumonia
- Multiple thin-walled cavitations on CXR, persistent fevers despite appropriate antibiotics.
- Common after pneumococcal serotype 19A or PVL-positive S aureus.[21]
- Management: prolonged IV antibiotics, supportive management, intervention only if severe.
Measles-associated pneumonia
- Direct viral pneumonitis or post-measles bacterial superinfection.
- Treatment: empiric broad-spectrum antibiotics + vitamin A 200,000 IU orally for 2 days; repeat in 4 weeks if SAM or clinical vitamin A deficiency.
- Seek BCG scar; consider TB if symptoms persist.[21]
Recurrent pneumonia
RECURRENT AT SAME SITE
structural anomaly
- **Foreign body**
- **Bronchial stenosis**
- **Congenital lobar emphysema**
- **Bronchogenic cyst**
- **Sequestration**
RECURRENT AT DIFFERENT SITES
host or systemic
- **Immunodeficiency** (humoral, complement, neutrophil)
- **HIV**
- **Cystic fibrosis**
- **Primary ciliary dyskinesia**
- **Asthma** (recurrent wheeze-asthma-misrecognition)
ALLERGIC / ASPIRATION
consider when
- **Gastro-oesophageal reflux with aspiration**
- **Dysphagia, swallow dysfunction**
- **Neurodisability**
Complications & Pitfalls
PLEURAL-PARENCHYMAL
commonest complications
- **Empyema** — pH under 7.2 / glucose under 3.3 mmol/L / pus / positive culture → **chest drain urgently** ± **MIST2 tPA + DNase** or VATS
- **Pneumothorax** — needle then small-bore drain
- **Pneumatocele** — usually conservative
- **Lung abscess** — prolonged antibiotics ± drainage
- **Necrotising pneumonia** — prolonged antibiotics; rarely lobectomy
SYSTEMIC
sepsis, ARDS, HUS
- **Septicaemia and septic shock**
- **ARDS** (Berlin criteria) — non-cardiogenic pulmonary oedema, hypoxaemia, bilateral infiltrates
- **Haemolytic-uraemic syndrome (HUS)** following pneumococcal pneumonia — the *neuraminidase* exposed by the pathogen exposes the T antigen on red cells; IgM binding → haemolysis, schistocytes, thrombocytopenia, AKI. Avoid blood products with plasma if T-antigen status uncertain; use T-activated red-cell washed units
- **Acute kidney injury** from hypovolaemia, sepsis, or HUS
LATE
structural sequelae
- **Bronchiectasis**
- **Failure to thrive** in chronic/recurrent disease
- **Pulmonary function deficit**
- **Post-pneumonic empyema requiring decortication**
PROCEDURAL & SYSTEM
errors to avoid
- **Overprescribing antibiotics for viral URTI**
- **Delaying antibiotics while chasing imaging**
- **Treating pleural effusion empirically with diuretics**
- **Failing to escalate to HFNC/CPAP for persistent hypoxaemia**
- **Failing to recognise empyema**: sending patient home with oral antibiotics, missing chest drain trigger criteria
- **Using under-dose amoxicillin (<80 mg/kg/day)** under-treats modern resistant pneumococci
Prognosis & Disposition
Outcome benchmarks
Disposition decisions:[1]
- WHO pneumonia: home after first dose observed; follow-up at 48-72 h and 7 days.
- Severe pneumonia: hospital admission, ward care; HFNC if needed.
- Very severe pneumonia: high-dependency or PICU; intubation if indicated.
- Empyema: surgical/medical ICU level of care depending on drainage approach.
- Necrotising pneumonia: PICU.[5]
Safety-net advice at discharge:[24]
- Return immediately if breathing worsens, fever recurs, cannot drink, vomits everything, convulsion, or drowsy.
- Complete the full course of oral antibiotic (typically 5 days for WHO pneumonia; longer if severe).
- Avoid tobacco smoke exposure and indoor air pollution.
- Catch-up immunisations (PCV, Hib, measles, pertussis, influenza) on recovery.
- If recurrent pneumonia, follow-up in clinic with CXR and immunological workup.[8]
Special Populations
Severe acute malnutrition (SAM)
Pneumonia is one of the largest contributors to SAM mortality. The WHO IMCI protocol for SAM provides specific guidance:[6]
- Sign blunting: hypothermia rather than fever; subtle indrawing; cough may be quiet.
- Always check glucose (often <3 mmol/L); treat with 2 mL/kg 10% dextrose.
- Empirical antibiotics: include broad Gram-negative cover (e.g. ampicillin + gentamicin).
- Resomal instead of standard ORS for fluid resuscitation in SAM (high potassium, low sodium).
- Careful fluid resuscitation — avoid overload in the malnourished myocardium.[24]
HIV-infected child
The differential widens substantially:[5]
- Pneumocystis jirovecii pneumonia — typically subacute, diffuse bilateral interstitial CXR ("ground glass"), no wheeze, often afebrile, hypoxaemia disproportionate; treat with co-trimoxazole 80/400 mg/kg/day of trimethoprim/sulfamethoxazole in 4 divided doses for 21 days plus corticosteroids if severe.
- Mycobacterium avium complex, CMV, Bartonella, Cryptococcus, TB.
- Repeat PCRs and BAL if necessary.
- Continue co-trimoxazole prophylaxis when stable.[7]
Immunocompromised (transplant, chemotherapy)
- Pre-test for PJP, CMV, RSV, parainfluenza, adenovirus, RSV; broad respiratory viral PCR and BAL routinely.
- Consider empirical co-trimoxazole + broad-spectrum antibacterial + voriconazole/echinocandin if febrile neutropenic.[1]
Sickle-cell disease
- Pneumococcal sepsis is a major risk (functional asplenia); cover with empirical ceftriaxone ± vancomycin.
- Vaccination: PCV, PPSV23, Hib, influenza annually; daily penicillin prophylaxis <5 years.[22]
Cystic fibrosis
- Recurrent pneumonia with Pseudomonas or Staph aureus.
- Chest CT, sweat test.
- Airway clearance and chronic antibiotics as per CF team.[5]
Neurodisability / aspiration
- Consider positioning, thickened feeds, H2-blockers or PPIs for GERD, swallow assessment.
- Recurrent aspiration with right upper-lobe involvement.[1]
Congenital cyanotic heart disease
- Increased pneumonia risk with poor perfusion; the myocardium is at risk.
- Avoid fluid overload.[5]
Evidence, Guidelines & Regional Differences
Landmark evidence
- Hazir Lancet 2008 (SAT trial): demonstrated high-dose oral amoxicillin 80-90 mg/kg/day for 5 days was equivalent to WHO-recommended injectable ampicillin + gentamicin for severe pneumonia in hospitalised children aged 3-59 months — supporting outpatient treatment of severe pneumonia in low-resource settings.[8] This underpins the modern WHO/IMNCI recommendation.
- Hazir ADC 2007: the double-dose amoxicillin RCT showed standard dose 80-90 mg/kg/day was equivalent to 40-45 mg/kg/day — supporting the upper dose as adequate.[7]
- Mulholland Lancet 1997: the Hib PRP-T Gambian trial — 5 cases prevented per 100 vaccinated, demonstrating Hib conjugate efficacy in a high-burden developing setting.[13]
- Watt Lancet 2009 and Wahl Lancet Glob Health 2018: quantified the Hib and pneumococcal pneumonia burden in unvaccinated vs vaccinated settings.[10][11]
- de Benedictis Lancet 2020: a comprehensive review of complicated pneumonia in children.[21]
- PERCH Lancet 2019 (PERCH): defined the aetiology of severe childhood pneumonia in 7 low- and middle-income sites — RSV most prominent, S pneumoniae a major bacterial contributor, similar across African and Asian sites.[5]
- St Peter 2009 (J Pediatr Surg): VATS vs chest tube + fibrinolysis in pediatric empyema — both effective, VATS shorter hospital stay but higher cost.[18]
- Rahman NEJM 2011 (MIST2): tPA + DNase intrapleural superior to either agent alone in adult empyema; widely extrapolated to children and now accepted as standard for complicated paediatric empyema.[19]
- Waites 2004 Clin Microbiol Rev and Kutty 2019 Clin Infect Dis: comprehensive reviews of Mycoplasma pneumoniae in children — clinical, diagnostic, and treatment considerations.[16][17]
- Roberts BTS 2023 Thorax: full BTS pleural disease guideline including parapneumonic effusion/empyema drainage triggers.[20]
- Nair Lancet 2010: quantified RSV's share of global childhood pneumonia.[4]
- Li Lancet 2022 + GBD 2019/2021 Collaborators: the GBD series as the source of contemporary mortality numbers.[1][2][3]
- Italian Intersociety Consensus (Donà Ital J Pediatr 2024): clinical pathways for mild-to-moderate CAP in previously healthy children.[23]
Guidelines
- WHO Pocket Book of Hospital Care for Children, 2nd ed. 2013 — bedside reference for pneumonia management in hospitals.[24]
- WHO IMCI/IMNCI chart booklet — first-level facility framework.
- BTS adult CAP guideline (Lim Thorax 2009) — adult-specific, but cross-cutting principles apply.[9]
- Italian Pediatric Intersociety Consensus (Dona Ital J Pediatr 2024) — example of national paediatric consensus.[23]
Regional deltas
Controversies
- Corticosteroids in childhood pneumonia — meta-analyses in adults show benefit; paediatric evidence is mixed; not routine, considered for severe hypoxaemic pneumonia on a case-by-case basis.
- Vitamin A supplementation — WHO recommends in measles and severe acute malnutrition; routine supplementation in pneumonia without measles/SAM has limited benefit.
- Duration of antibiotic course — 3 days may be non-inferior to 5 days for non-severe pneumonia (green-IMCI Kenya data); 5-7 days remains the mainstream MBBS/NEET-PG approach.
- Criteria for HFNC vs CPAP vs early IMV in severe pneumonia — under active trial.[7]
Exam Pearls
A high-yield summary designed for last-minute revison.[24]
- Pneumonia is the leading infectious cause of under-5 mortality globally: ~700,000 deaths/year, 14% of all under-5 deaths.[1]
- WHO operational definition: cough or difficulty breathing with fast breathing.
- WHO fast-breathing thresholds: 2-12 months >50/min; 1-5 years >40/min; >5 years >20/min.[24]
- Lower chest wall indrawing = severe pneumonia → hospitalise.
- WHO danger signs = very severe pneumonia: inability to drink, convulsions, vomiting everything, severe malnutrition, grunting → emergency care.
- Leading viral cause under 1 year = RSV.[4][15]
- Leading bacterial cause overall = Streptococcus pneumoniae (still, despite PCV).
- Hib pneumonia has fallen dramatically with the introduction of conjugate vaccine.[10][11][13][14]
- Mycoplasma pneumoniae = most common cause of CAP in school-age (>5 yr) children; macrolide is the antibiotic.[16][17]
- PVL-positive Staph aureus in children: pneumatocele, empyema, necrotising pneumonia; cover with vancomycin/linezolid empirically.[21]
- Oral amoxicillin 80-90 mg/kg/day × 5 days for WHO pneumonia (Hazir evidence).[7][8]
- Severe pneumonia: IV ampicillin 50 mg/kg IV q6h + gentamicin 7.5 mg/kg q24h (or ceftriaxone 50-80 mg/kg/day q24h).
- Very severe pneumonia: as above + add macrolide if atypical, ± vancomycin if MRSA, ± oseltamivir if influenza in 48 h.
- SpO2 <90% triggers oxygen; target 94-98% in non-cardiac children (88-92% in BPD).
- Pleural drainage trigger: pH<7.2, glucose <3.3 mmol/L, LDH >1000, pus, positive culture → chest drain + MIST2.[19][20]
- MIST2 intrapleural fibrinolysis: tPA 10 mg + DNase 5 mg twice daily for 3 days.[19]
- VATS (video-assisted thoracoscopic surgery) if fibrinolysis fails.
- PCV13/PCV10 + Hib + measles + annual influenza are the four most important vaccines.
- Chlamydia trachomatis pneumonia in 4-12 weeks: afebrile, staccato cough, conjunctivitis, eosinophilia → erythromycin/azithromycin.
- RSV bronchiolitis ≠ pneumonia, but both can coexist; treatment of bronchiolitis is supportive.
- Bordetella pertussis in infants: paroxysms, whoop, lymphocytosis, apnoeas → macrolide.
- Staphylococcal pneumonia (post-influenza): pneumatoceles, empyema, necrotising pneumonia.
- Severe acute malnutrition pneumonia: blunted signs, hypothermia, hypoglycaemia, broad-cover antibiotics.
- HIV pneumonia differential widens: Pneumocystis, CMV, MAC, TB.
- Antibiotics NOT routine in viral URTI; only indicated in pneumonia meeting WHO severity criteria.
Exam application bank (NEET-PG / INICET)
One-line answer
Pneumonia in children = inflammation of the lung parenchyma, the single leading infectious cause of under-5 mortality globally, responsible for ~700,000 deaths/year (≈14% of all under-5 deaths). The WHO operational definition is cough or difficulty breathing with fast breathing defined by age (over 50/min at 2-12 months, over 40/min at 12 months-5 years, over 20/min at over 5 years). WHO classifies severity into pneumonia (fast breathing only, treat at home with oral amoxicillin), severe pneumonia (lower chest wall indrawing, hospitalise), and very severe pneumonia (danger signs: inability to drink, convulsions, vomiting everything, severe malnutrition, grunting — IV/IM antibiotics urgently). Leading viral cause under 1 year = RSV. Leading bacterial cause = Streptococcus pneumoniae; Hib pneumonia has fallen dramatically with conjugate vaccination. Empirical treatment: oral amoxicillin 80
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard.[7]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes.[21]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change.[12]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each.[24]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory.[24]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Pneumonia in Children.
References
- [1]Li Y, Wang X, Blau DM, et al; GBD 2019 LRI Collaborators. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2019: a systematic analysis. Lancet, 2022.PMID 35598608
- [2]GBD 2019 Lower Respiratory Infections Collaborators. Age-sex differences in the global burden of lower respiratory infections and risk factors, 1990-2019: results from the Global Burden of Disease Study 2019. Lancet Infectious Diseases, 2022.PMID 35964613
- [3]GBD 2021 Lower Respiratory Infections Collaborators. Global, regional, and national incidence and mortality burden of non-COVID-19 lower respiratory infections and aetiologies in 2021, with forecasts to 2050: a systematic analysis from the Global Burden of Disease Study 2021. Lancet Infectious Diseases, 2024.PMID 38636536
- [4]Nair H, Nokes DJ, Gessner BD, et al. Global burden of acute lower respiratory infections due to respiratory syncytial virus in young children: a systematic review and meta-analysis. Lancet, 2010.PMID 20399493
- [5]Pneumonia Etiology Research for Child Health (PERCH) Study Group. Causes of severe pneumonia requiring hospital admission in children without HIV infection from Africa and Asia: the PERCH multi-country case-control study. Lancet, 2019.PMID 31257127
- [6]Deloria Knoll M, Prosperi C, Baggett HC, et al. Introduction to the Site-specific Etiologic Results From the Pneumonia Etiology Research for Child Health (PERCH) Study. Pediatric Infectious Disease Journal, 2021.PMID 34448739
- [7]Hazir T, Fox LM, Nisar YB, et al. Comparison of standard versus double dose of amoxicillin in the treatment of non-severe pneumonia in children aged 2-59 months: a randomised equivalence trial. Archives of Disease in Childhood, 2007.PMID 16547082
- [8]Hazir T, Nisar YB, Nawab S, et al. Ambulatory short-course high-dose oral amoxicillin for treatment of severe pneumonia in children: a randomised equivalency trial. Lancet, 2008.PMID 18177775
- [9]Rothberg MB Community-Acquired Pneumonia. Annals of internal medicine, 2022.PMID 35404672
- [10]Watt JP, Wolfson LJ, O'Brien KL, et al. Burden of disease caused by Haemophilus influenzae type b in children younger than 5 years: global estimates. Lancet, 2009.PMID 19748399
- [11]Wahl B, O'Brien KL, Greenbaum A, et al. Burden of Streptococcus pneumoniae and Haemophilus influenzae type b disease in children in the era of conjugate vaccine: global estimates. Lancet Global Health, 2018.PMID 29903376
- [12]Farrar JL, Burbidge KM, Marciniak M, et al. A systematic review and meta-analysis of the efficacy and effectiveness of pneumococcal vaccines in adults and elderly patients. Pathogens, 2023.PMID 37242402
- [13]Mulholland K, Hilton S, Adegbola R, et al. Randomised trial of Haemophilus influenzae type-b tetanus protein conjugate vaccine for prevention of pneumonia. Lancet, 1997.PMID 9130939
- [14]de Andrade AL, de Andrade JG, Martelli CM, et al. Effectiveness of Haemophilus influenzae b conjugate vaccine on childhood pneumonia: a case-control study in Brazil. International Journal of Epidemiology, 2004.PMID 15075166
- [15]Manzoni P, Figueras-Aloy J, Simões EAF, et al. Defining the Incidence and Associated Morbidity and Mortality of Severe Respiratory Syncytial Virus Infection Among Children with Chronic Diseases. Infectious Diseases and Therapy, 2017.PMID 28653300
- [16]Waites KB, Talkington DF. Mycoplasma pneumoniae and its role as a human pathogen. Clinical Microbiology Reviews, 2004.PMID 15489344
- [17]Kutty PK, Jain S, Taylor TH, et al. Mycoplasma pneumoniae Among Children Hospitalized With Community-acquired Pneumonia. Clinical Infectious Diseases, 2019.PMID 29788037
- [18]St Peter SD, Tsao K, Spilde TL, et al. Thoracoscopic decortication vs tube thoracostomy with fibrinolysis for empyema in children: a prospective, randomized trial. Journal of Pediatric Surgery, 2009.PMID 19159726
- [19]Rahman NM, Maskell NA, West SE, et al. Intrapleural use of tissue plasminogen activator and DNase in pleural infection. New England Journal of Medicine, 2011.PMID 21830966
- [20]Roberts ME, Rahman NM, Maskell NA, et al. British Thoracic Society Guideline for pleural disease. Thorax, 2023.PMID 37433578
- [21]de Benedictis FM, Kerem E, Chang AB, et al. Complicated pneumonia in children. Lancet, 2020.PMID 32919518
- [22]Hanquet G, Krizova P, Valentiner-Branth P, et al. Effect of childhood pneumococcal conjugate vaccination on invasive disease in older adults of 10 European countries: implications for adult vaccination. Thorax, 2019.PMID 30355641
- [23]Donà D, Mazzoni G, Venturelli V, et al. Treatment of mild to moderate community-acquired pneumonia in previously healthy children: an Italian intersociety consensus. Italian Journal of Pediatrics, 2024.PMID 39427174
- [24]Kundu S, Das S, Medhagopal RG An Update on WHO Recommendations on Childhood Pneumonia and Diarrhea (2024). Indian pediatrics, 2025.PMID 40839064