Psychiatry · Psychiatry
Attention Deficit Hyperactivity Disorder (ADHD)
Also known as ADHD · Attention deficit hyperactivity disorder · Attention deficit disorder · ADD · Hyperkinetic disorder
ADHD is a neurodevelopmental disorder characterised by persistent, pervasive, impairing inattention, hyperactivity, and impulsivity with onset before age 12 and symptoms present in two or more settings (home, school, work). Prevalence about 5 percent of children, 2.5 percent of adults; clinic male-to-female ratio 3:1 (community 2:1); heritability 74 to 88 percent — among the highest in psychiatry. DSM-5-TR: 6+ inattention and/or 6+ hyperactivity-impulsivity symptoms in children (5+ in adults 17+), for at least 6 months, several before age 12, in 2+ settings, causing impairment, not better explained. Three presentations: predominantly inattentive, predominantly hyperactive-impulsive, combined. Treat: behavioural parent-training first for children under 6; stimulants first-line for 6+ (methylphenidate blocks dopamine/noradrenaline transporters; lisdexamfetamine promotes release — 70 to 80 percent response); atomoxetine (non-stimulant SNRI, for substance use, tics, anxiety); alpha-2 agonists (guanfacine, clonidine — hyperactivity, tics, sleep). Combined stimulant + behavioural therapy best for moderate-severe. Adult ADHD: lisdexamfetamine first-line (NICE). Monitor on stimulants: growth (height/weight 6-monthly), BP/HR, appetite, sleep, mood, tics. ADHD persists into adulthood in ~60 percent.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Overview & Definition
Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder characterised by a persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development. It is the commonest neurodevelopmental disorder of childhood and one of the most treatable conditions in psychiatry — stimulants produce a response rate of 70 to 80 percent, among the highest in medicine.[1]
The clinical skill in ADHD is not the diagnosis itself (that is clinical, made by DSM-5-TR criteria) but five interlocking competencies:[5]
- Diagnose correctly — symptoms must be pervasive (across 2+ settings, e.g. home AND school) and persistent (since before age 12), not just situational fidgeting or post-pubertal distractibility.
- Distinguish from mimics — normal age-appropriate activity, anxiety, depression, sleep deprivation, hyperthyroidism, hearing/visual impairment, autism, trauma, substance intoxication.
- Initiate evidence-based treatment in the right order — behavioural parent-training first under age 6; stimulants first-line 6 and over; combined stimulant + behavioural therapy for moderate-severe.
- Select the agent for the patient — atomoxetine or alpha-2 agonist when there is comorbid substance use, tics/Tourette, anxiety, or adult preference for a non-stimulant.
- Monitor for stimulant adverse effects — growth (height/weight centiles), appetite, sleep, mood, BP/HR, tics, diversion — and recognise that ADHD persists into adulthood in ~60 percent.[1][7]
Classification
ADHD is classified by diagnostic system (DSM-5-TR vs ICD-11 vs legacy DSM-IV/ICD-10) and by symptomatic presentation.[9][10]
DSM-5-TR presentations (the system used in NEET-PG / USMLE / NICE):[9]
- Combined presentation — meets criteria for both inattention AND hyperactivity-impulsivity for the past 6 months. (The commonest presentation in clinic-referred children.)
- Predominantly inattentive presentation — meets inattention criteria but not (or fewer than) hyperactivity-impulsivity criteria. Common in girls and adults; under-diagnosed because the child is quiet and day-dreaming rather than disruptive. (This is what was called "ADD" in the legacy DSM-IV.)
- Predominantly hyperactive-impulsive presentation — meets hyperactivity-impulsivity criteria but not inattention. More common in younger children.[3]
Severity specifiers (DSM-5-TR):[9]
- Mild — few, if any, symptoms in excess of those required for diagnosis, with no more than minor functional impairment.
- Moderate — symptoms or functional impairment between mild and severe.
- Severe — many symptoms in excess of those required, or symptoms cause marked functional impairment.
- In partial remission — full criteria were previously met, but fewer than the required symptoms have been present for the past 6 months, with continued clinically significant impairment.[3]
Cross-diagnostic-system distinctions (a common exam trap):[9][10]
DSM-5-TR (US, India, much of world)
- Neurodevelopmental disorder under 'Neurodevelopmental Disorders'
- Onset of several symptoms before age 12 (changed from DSM-IV's before 7)
- Children: 6+ of 9 inattention and/or 6+ of 9 hyperactivity-impulsivity
- Adults/adolescents 17+: 5+ in either domain
- Symptoms in 2+ settings, impairing, not better explained
- Three presentations: inattentive, hyperactive-impulsive, combined
ICD-11 (WHO)
- Renamed 'Attention deficit hyperactivity disorder' (replaces 'Hyperkinetic disorder' of ICD-10)
- Now classified under Neurodevelopmental disorders (6A05)
- Onset in early childhood; pervasively impaired across settings
- Largely harmonised with DSM-5 — much narrower gap than DSM-IV vs ICD-10
- Specifiers for inattention-only and combined presentations
ICD-10 'Hyperkinetic disorder'
- Legacy term, stricter than DSM-IV
- Required onset before age 7, pervasive across settings, and all three of inattention, overactivity AND impulsivity
- Used in older European/UK research — lower prevalence than DSM ADHD
- Now superseded by ICD-11 ADHD

Epidemiology & Risk Factors
- Children and adolescents: ~5 percent worldwide (Polanczyk's systematic review and meta-regression: pooled prevalence ~5.3 percent; prevalence is remarkably stable across geographic regions when uniform methodology is applied — dispelling the myth of a "US-only" diagnosis).
- Adults: ~2.5 percent (full-criteria ADHD). The 60-percent persistence rule applies: of every 10 children with ADHD, about 6 still meet criteria or have subthreshold impairing symptoms as adults.
- Sex ratio: clinic-referred children show M:F ≈ 3:1 to 4:1; community samples show ~2:1. The discrepancy arises because girls more often have the inattentive presentation, are less disruptive, and present with internalising comorbidity — leading to systematic under-diagnosis and under-treatment.[6]
Heritability — among the highest in psychiatry:[1][5]
- Twin studies place heritability at 74 to 88 percent — comparable to schizophrenia and bipolar disorder, and higher than major depression or anxiety.
- Adoption and sibling studies converge: biological relatives of probands have a 2- to 8-fold higher rate of ADHD than adoptive relatives.
- Susceptibility genes (each small effect): DAT1/SLC6A3 (dopamine transporter — the target of methylphenidate), DRD4 (especially the 7-repeat allele of the D4 receptor), DRD5, SNAP25, BDNF, CNVs at 16p13.11, 22q11.2 (overlap with autism and schizophrenia).
- First-degree relatives of a child with ADHD have ~an 8-fold risk of ADHD compared with the general population.[3]
ADHD — the numbers examiners want
Environmental risk factors (small individual effect, multifactorial with the genetic load):[1]
- Prenatal: maternal smoking, alcohol and illicit drug use during pregnancy.
- Perinatal: prematurity and low birth weight (one of the most consistent associations).
- Toxins: lead exposure, polychlorinated biphenyls (PCBs), organophosphate pesticides.
- Early deprivation: severe institutional care (Romanian adoptee studies).
- Traumatic brain injury in childhood.
- Psychosocial adversity: family conflict, low socio-economic status, inconsistent parenting — these worsen outcome but do not cause ADHD.
- Iron deficiency and sleep disruption can worsen symptoms or mimic ADHD.[5]
Myths to refute (frequently examined):[1][5]
- ADHD is not caused by refined sugar, food additives, the Feingold diet target salicylates, excessive television/screen time, or poor parenting. These may aggravate behaviour in any child but robust meta-analytic evidence does not support a causal role.
- ADHD is not simply a "modern" or "Western" diagnosis — equivalent syndromes are described across cultures and centuries.[5]
Pathophysiology
ADHD is a disorder of catecholamine signalling in the prefrontal cortex and connected circuits. The prefrontal cortex (PFC) — particularly the dorsolateral PFC (working memory, organisation, planning) and anterior cingulate (attention allocation, error detection) — governs executive function and top-down inhibition.[1][5]
The catecholamine / inverted-U hypothesis (the mechanism examiners reward):[1]
The PFC depends on optimal — not maximal — dopamine and noradrenaline signalling to gate the right signal and suppress noise. This relationship follows an inverted-U dose-response curve:[1]
- Too little catecholamine (the ADHD state) → weak signal-to-noise → distractibility, poor sustained attention, weak inhibitory control.
- Optimal catecholamine (post-stimulant, or post-exercise, or intrinsically in non-ADHD brains) → strong signal-to-noise → focused attention, goal-directed behaviour, impulse control.
- Too much catecholamine (stress, very high stimulant dose) → noise amplification → overfocus, anxiety, stereotypy.[2]
This explains the "paradox" that a stimulant calms hyperactivity — it is not paradoxical; it restores PFC catecholamine tone to the apex of the inverted-U.[1]
Brain regions implicated (functional and structural neuroimaging converge):[1][5]
- Dorsolateral prefrontal cortex — working memory, planning, organisation.
- Anterior cingulate cortex — attention allocation, conflict/error monitoring.
- Striatum (caudate and putamen) — response inhibition, motor control, reward; volumes are reduced and asymmetry reversed in ADHD.
- Cerebellum — smaller vermis, especially posterior-inferior; motor timing and attention.
- Corpus callosum — reduced size of splenium and rostral body.
- Overall: cortical maturation lag of roughly 2 to 3 years in children with ADHD, most marked in the PFC (Shaw et al. neurodevelopmental trajectory studies).[8]
The four dopamine pathways — know which one does what (high-yield):[2]
| Pathway | Origin → target | Function | Effect of dysregulation in ADHD |
|---|---|---|---|
| Mesocortical | VTA → prefrontal cortex | Cognition, motivation, executive function | Inattention, executive dysfunction (the core ADHD deficit) |
| Mesolimbic | VTA → nucleus accumbens | Reward, motivation, reinforcement | Delay aversion, reward deficiency, impulsivity |
| Nigrostriatal | Substantia nigra → striatum | Motor control | Hyperactivity, motor tics |
| Tuberoinfundibular | Hypothalamus → pituitary | Prolactin inhibition | Spared in ADHD (relevant for antipsychotic, not stimulant, adverse effects) |
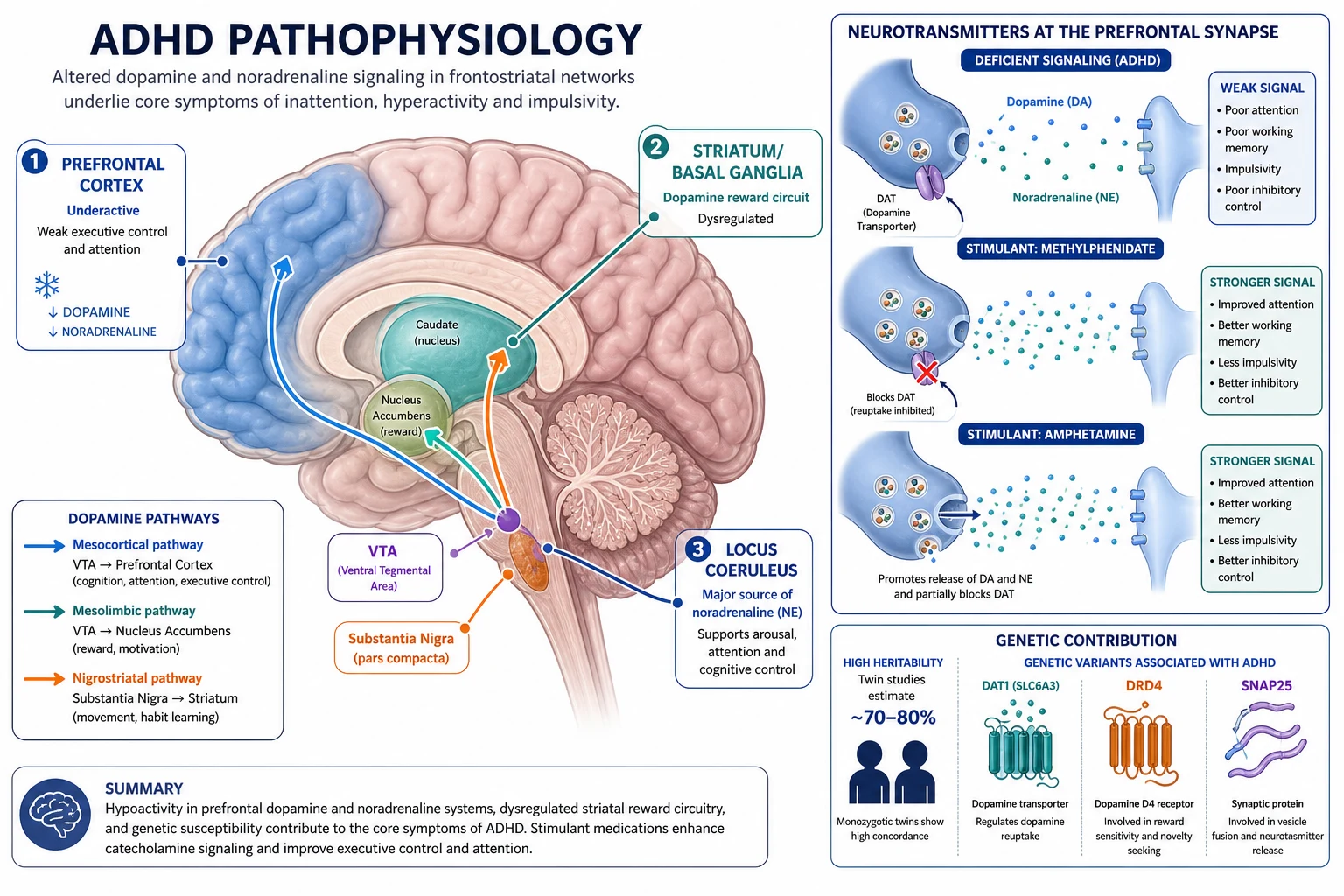
How the stimulants work (mechanism — core examinable detail):[4][5]
- Methylphenidate — blocks the dopamine transporter (DAT) and noradrenaline transporter (NET) at the pre-synaptic membrane → increases synaptic DA and NA in the PFC and striatum → restores the inverted-U apex.
- Amphetamines (dexamfetamine, mixed amphetamine salts, lisdexamfetamine) — block DAT/NET AND promote release of cytosolic catecholamines by reversing transporter direction AND inhibit monoamine oxidase → larger synaptic DA/NA rise. Lisdexamfetamine is a prodrug (L-lysine coupled to dexamfetamine; cleaved by red-blood-cell esterase to active dexamfetamine) → slow onset, low peak, less abuse/diversion potential — first-line in adults.
- Atomoxetine — selective noradrenaline reuptake inhibitor (blocks NET); modest DA effect in PFC (where DA is cleared by NET, not DAT). Non-addictive, slower onset (4-6 weeks).
- Alpha-2 agonists (guanfacine, clonidine) — stimulate post-synaptic alpha-2A receptors in the PFC, strengthening PFC network connectivity and reducing locomotor hyperactivity; useful for tics, oppositionality and sleep.[2]
Two neuropsychological models (high-yield for vivas):[1]
- Barkley's executive-function / inhibition model — primary deficit is behavioural inhibition (inhibit, stop, delay); secondary deficits cascade into working memory, self-regulation of affect, internalisation of speech, reconstitution.
- Sonuga-Barke's dual-pathway model — (1) executive dysfunction (PFC/striatal) AND (2) delay aversion (limbic/reward) — a child who finds waiting for reward so aversive that they choose smaller immediate reward; explains why ADHD is not purely cognitive.[8]
Clinical Presentation
ADHD presents differently across the lifespan and across presentations.[1][9]
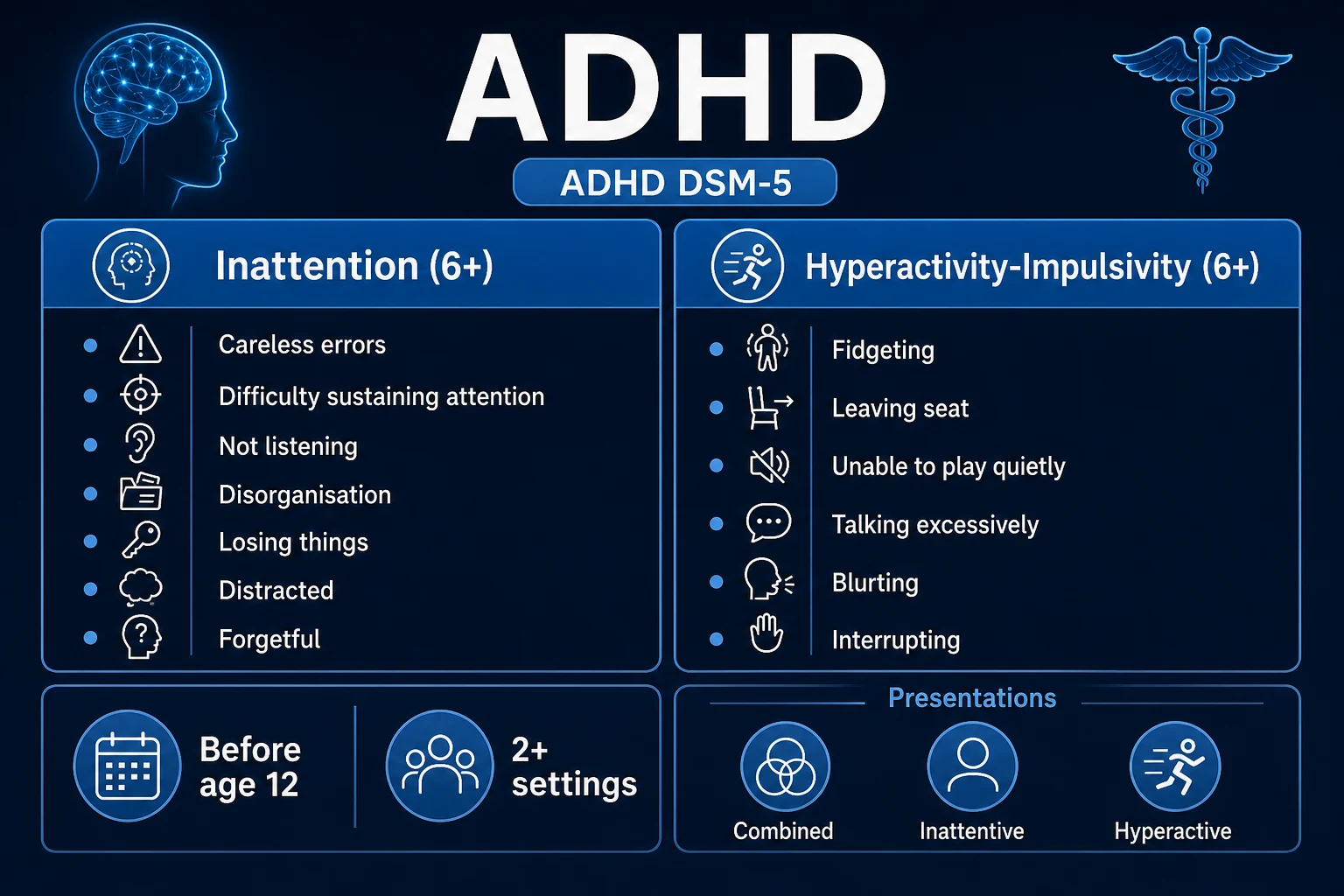
The 18 DSM-5-TR symptoms — reproduce verbatim (examiner favourite):[9]
Inattention (9 symptoms; 6+ needed in children, 5+ in adults):[1]
- Often fails to give close attention to details or makes careless mistakes in schoolwork, work or other activities.
- Often has difficulty sustaining attention in tasks or play activities.
- Often does not seem to listen when spoken to directly.
- Often does not follow through on instructions and fails to finish schoolwork, chores or workplace duties (not due to oppositional behaviour or failure to understand).
- Often has difficulty organising tasks and activities.
- Often avoids, dislikes or is reluctant to engage in tasks that require sustained mental effort.
- Often loses things necessary for tasks or activities.
- Often is easily distracted by extraneous stimuli.
- Often is forgetful in daily activities.[1]
Hyperactivity-impulsivity (9 symptoms; 6+ children, 5+ adults):[1]
- Often fidgets with or taps hands or feet, or squirms in seat.
- Often leaves seat in situations when remaining seated is expected.
- Often runs about or climbs in situations where it is inappropriate (in adults, may be subjective restlessness).
- Often unable to play or engage in leisure activities quietly.
- Often 'on the go', acting as if 'driven by a motor'.
- Often talks excessively.
- Often blurts out an answer before a question has been completed.
- Often has difficulty waiting their turn.
- Often interrupts or intrudes on others.[5]
Preschool (under 6) — excessive, pervasive motor activity; dangerous behaviour (running off, climbing); difficulty settling in group childcare; very short attention span; high intensity; impulsivity. Must be distinguished from age-appropriate activity by pervasiveness and impairment.[8]
School-age (6-12) — underachievement relative to ability; homework battles; distractibility; losing books/equipment; disruptive classroom behaviour; fidgeting; calling out; accidents and injuries (broken bones, head injury, accidental poisoning); strained peer relationships (impulsivity → conflicts).[1]
Adolescence (13-18) — declining academic performance as executive-function load increases; risky behaviour (alcohol, drugs, early sexual activity, dangerous driving); conflict with authority; driving risk (the single biggest excess mortality in adolescent ADHD is motor-vehicle crashes); mood swings; comorbid SUD emergence.[1]
Adulthood — the hyperactivity of childhood becomes an internal restlessness ("I can't relax, my brain won't switch off"). Salient features: lifelong inattention and disorganisation; time blindness (chronic lateness, missed deadlines); restlessness (mental, not motor); emotional dysregulation (low frustration tolerance, quick temper); task-completion failure; traffic accidents; job instability; relationship strain; higher rates of divorce, bankruptcy, incarceration. Many present only when a child is diagnosed and the parent recognises themselves.[1][7]
Atypical / masked presentations (examiner favourite):[1]
- Girls with the inattentive presentation — quiet, day-dreaming, anxious, "not working to potential"; referred late or never; more internalising comorbidity (anxiety, depression, self-harm).
- High-IQ children — compensate until academic/work load exceeds their coping strategies; present with burnout, anxiety, "I always knew I was different".
- Adults presenting with depression or anxiety — secondary to lifelong untreated ADHD; always screen with ASRS in any adult with chronic disorganisation, time blindness and emotional dysregulation.[3]
Differential Diagnosis
A child or adult with inattention/hyperactivity is not necessarily ADHD. The differential is broad and must be actively excluded.[1][5]
Medical / organic differentials:[1]
| Differential | Distinguishing features |
|---|---|
| Hyperthyroidism | Tachycardia, weight loss, heat intolerance, goitre, tremor, anxiety; check TSH/T4 |
| Hearing or vision impairment | Functional inattention; audiogram / vision screen; child is inattentive only in noisy/visually-demanding contexts |
| Sleep disorders (OSA, insufficient sleep) | Snoring, witnessed apnoea, daytime somnolence, obesity; sleep history / polysomnography; symptoms resolve with sleep restoration |
| Iron-deficiency anaemia | Fatigue, pallor, pica; FBC + ferritin; restless legs overlap |
| Lead poisoning | Pica, pica exposure (old paint), microcytic anaemia, basophilic stippling; blood lead level |
| Absence seizures | Brief (10-sec) staring spells, abrupt onset/offset, no response to touch, multiple per day; EEG with 3-Hz spike-and-wave |
| Fetal alcohol spectrum disorder | Prenatal alcohol exposure, characteristic facial features, growth restriction, neurocognitive deficits |
| Fragile X syndrome | Long face, large ears, post-pubertal macro-orchidism, intellectual disability, family history; genetic testing |
| Traumatic brain injury / post-concussion | Clear temporal relationship; cognitive symptoms post-injury |
| William / 22q11.2 deletion syndromes | Dysmorphism, cardiac anomalies, developmental delay |
Psychiatric differentials (each distinguished by pattern and course):[1]
ADHD
- Trait-level, chronic since early childhood
- Pervasive across settings
- No mood elevation, no trauma trigger required
- Improves (not worsens) with stimulant
- Inverted-U catecholamine response
Anxiety disorder (incl. GAD)
- Worry and fear are prominent, often situational
- Autonomic hyperarousal, muscle tension, sleep difficulty
- Onset often later than age 12
- Attention fails in feared/anxious contexts; cognitive bias to threat
- Worsens with stimulant; treat with SSRI/CBT
Major depression
- Episodic low mood, anhedonia, low energy
- Concentration impaired but context is depressed mood
- Psychomotor retardation (NOT hyperactivity)
- Sleep and appetite disturbance
- Treat with SSRI/therapy; stimulant may worsen agitation
Bipolar disorder (mania/hypomania)
- Episodic, distinct mood elevation or irritability
- Decreased need for sleep (NOT insomnia)
- Grandiosity, pressured speech, flight of ideas
- Goal-directed risk-taking, hypersexuality
- Stabilise mood FIRST; stimulants can precipitate mania
Autism spectrum disorder (ASD)
- Social-communication deficits
- Restricted, repetitive interests and routines
- Sensory hyper/hypo-reactivity
- Insistence on sameness (NOT impulsivity)
- Treatment is behavioural; stimulant more side-effect prone
Oppositional defiant disorder (ODD)
- Hostility and defiance toward authority figures
- Temper outbursts, argumentativeness, vindictiveness
- Not characterised by inattention
- Often COMORBID with ADHD (40-60%)
- Treat ADHD first; PMT; risperidone only if severe aggression
Substance intoxication/withdrawal
- Stimulants (cocaine, methamphetamine), caffeine
- Temporal relationship to substance
- Resolves with abstinence
- Urine drug screen
- Treat SUD before diagnosing ADHD
Clinical rule (examiner favourite): the presence of a comorbidity does not exclude ADHD — ADHD is highly comorbid. About 60 to 70 percent of children with ADHD have at least one comorbidity (ODD ~40 percent, anxiety ~30 percent, depression ~15-30 percent, tics/Tourette ~20 percent, SUD in adolescence/adulthood ~30-50 percent, learning disability ~30-45 percent). Diagnose both, treat both.[1][5]
Clinical & Bedside Assessment
ADHD is diagnosed clinically by careful history, observation, and standardised rating scales across settings. There is no blood test or scan.[1][7]
History — take it across two or more settings:[7]
- Developmental history — pregnancy/birth (prematurity, low birth weight, maternal smoking/alcohol), milestones, early temperament ("always on the go"), speech and language, motor coordination.
- Symptom history — onset (before age 12 for DSM-5-TR), domains affected, situational variability, pervasiveness (home, school, with relatives, in clubs/sport, at work), impairment (academic, social, family, self-esteem, safety).
- Family history — ADHD, autism, tics/Tourette, mood/anxiety disorders, SUD, learning disability, sudden cardiac death in young relatives (relevant to stimulant safety).
- School / occupational history — teacher reports, school reports, exam results, work appraisals, disciplinary records, driving record.
- Comorbidity screen — ODD, conduct disorder, anxiety, depression, tics/Tourette, autism, SUD, learning disability, sleep disorder.
- Psychosocial — family functioning, parenting style, adverse childhood experiences (trauma, abuse, neglect, deprivation), peer relationships, bullying.[5]
Standardised rating scales (reproduce the names examiners want):[1][7]
| Scale | Age | Rater | Use |
|---|---|---|---|
| SNAP-IV | Children | Parent + teacher | The Swanson, Nolan and Pelham — 18- or 90-item; maps directly onto DSM-5 symptoms |
| Conners-3 | Children/adolescents | Parent, teacher, self | Comprehensive; DSM-5-aligned; long and short forms |
| Vanderbilt | Children 6-12 | Parent + teacher | NICE/AACAP-recommended; screens for comorbid ODD/conduct/anxiety/depression |
| Strengths and Difficulties Questionnaire (SDQ) | 4-17 | Parent, teacher, self | Brief universal screener (free) |
| Brown ADD Scales | Children/adults | Self/parent | Executive-function-focused |
| Adult ADHD Self-Report Scale (ASRS-v1.1) | Adults | Self | 6-item Part A screener; 4 of 6 in shaded boxes = positive screen; the WHO/ASRS — first adult ADHD screener |
Why BOTH parent/carer AND teacher reports are mandatory for a child: ADHD must be pervasive across two or more settings to meet DSM-5-TR criterion C. A child who is inattentive at home but settles well at school, or vice versa, does not have ADHD — that pattern points to a contextual trigger (family conflict, learning difficulty, bullying, sleep restriction).[1][7]
Physical examination (every patient, before stimulants):[7]
- Growth: height, weight, plotted on centile chart (baseline for stimulant monitoring).
- Cardiovascular: heart rate, blood pressure, auscultation for murmurs; ask specifically about syncope, chest pain, palpitations on exertion, family history of sudden cardiac death under 40, and known structural heart disease — these are the triggers for an ECG and cardiology referral before starting a stimulant.[7]
- Neurologic screen — abnormal movements, tics (eye-blinking, facial grimacing, throat-clearing, shoulder shrugging), dysmorphism (fragile X), focal deficit.
- Sensory — hearing (audiogram if any concern), vision (Snellen).
- Skin — café-au-lait patches (NF1), ash-leaf macules (tuberous sclerosis).
Assess for comorbidity at every visit — ODD, conduct disorder, anxiety, depression, tics, autism, SUD, learning disability. Comorbidity changes the treatment plan.[7]
Investigations
ADHD is a clinical diagnosis — there is no blood test, no genetic test, no brain scan required to diagnose it.[1][7]
Baseline investigations BEFORE starting a stimulant:[7]
- Height and weight on centile chart (baseline for growth monitoring).
- Blood pressure and heart rate (baseline for cardiovascular monitoring).
- ECG — only if cardiac history, symptoms (syncope, chest pain, palpitations on exertion), family history of sudden cardiac death under 40, or known structural heart disease. Routine ECG in asymptomatic children without cardiac history is not required by NICE NG87.[7]
- Consider (only if clinically indicated): TFTs (TSH, free T4) if hyperthyroid features; FBC and ferritin if pallor/pica; lead level if pica/old paint exposure; sleep study if snoring/witnessed apnoea; EEG if staring spells/absences suspected; formal psychoeducational assessment if learning difficulty suspected.
Reproduce DSM-5-TR criteria verbatim (examiner favourite):[9]
Criterion A — a persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development, as characterised by (1) and/or (2):
- Inattention: six (or more) of the following symptoms have persisted for at least 6 months to a degree inconsistent with developmental level and negatively impacting social/academic activities (5+ for age 17 and older): the nine symptoms listed above.
- Hyperactivity and impulsivity: six (or more) of the following symptoms for at least 6 months (5+ for 17 and older): the nine symptoms listed above.[3]
Criterion B — several inattentive or hyperactive-impulsive symptoms present prior to age 12 years. (DSM-IV required onset before age 7; DSM-5-TR relaxed this to before age 12.)[7]
Criterion C — several inattentive or hyperactive-impulsive symptoms are present in two or more settings (e.g. at home, school, or work; with friends or relatives; in other activities).[7]
Criterion D — there is clear evidence that the symptoms interfere with or reduce the quality of social, academic, or occupational functioning.[7]
Criterion E — the symptoms do not occur exclusively during the course of schizophrenia or another psychotic disorder and are not better explained by another mental disorder (e.g. mood disorder, anxiety disorder, dissociative disorder, personality disorder, substance intoxication/withdrawal).[9]
ASRS-v1.1 adult screener (reproduce):[1] Six-item Part A questions ask how often in the past 6 months the patient has: (1) failed to give close attention to detail/made careless mistakes; (2) difficulty sustaining attention; (3) difficulty organising; (4) avoided work requiring sustained mental effort; (5) fidgeting; (6) acted 'driven by a motor'. Each scored Never/Rarely/Sometimes/Often/Very Often. Four or more of the six responses in the shaded boxes (Sometimes/Often/Very Often for items 1-3, Often/Very Often for items 4-6) = positive screen — refer for full diagnostic assessment.
When are further investigations indicated?[7]
- Sleep study (polysomnography) — snoring, witnessed apnoea, daytime somnolence, obesity → screen for obstructive sleep apnoea.
- EEG — brief staring spells unresponsive to touch, multiple per day → screen for absence seizures.
- Formal psychoeducational assessment (WISC/WAIS + WRAT/WIAT) — significant discrepancy between ability and achievement → screen for learning disability (specific learning disorder).
- Genetic testing — dysmorphism, intellectual disability, family history → fragile X (FMR1), 22q11.2 deletion, karyotype.[7]
What MUST be excluded before diagnosing adult ADHD?[7] Active untreated substance use disorder, current mania/hypomania or psychosis, or symptoms that occur only in the context of these — ADHD cannot be confidently diagnosed during acute SUD, mania, or psychosis; reassess once stabilised.
Management — Resuscitation / Immediate Concerns
ADHD has no acute-resuscitation phase in the sense of a septic or cardiac emergency, but safety-critical situations demand immediate action.[1][7]
Immediate safety-critical scenarios:[7]
- Suicidal ideation on atomoxetine (FDA black-box warning) — stop atomoxetine; safety assessment; treat suicidality; consider switch to stimulant.
- Severe aggression / self-harm / comorbid crisis — crisis intervention, hospitalisation if needed, treat comorbid mood/psychosis; do NOT initiate ADHD medication during acute psychiatric crisis.
- Cardiovascular symptoms on stimulant — sudden chest pain, syncope, palpitations on exertion, severe hypertension, tachyarrhythmia → STOP the stimulant immediately, take an ECG, take a focused cardiac history (family history of sudden cardiac death under 40, known structural heart disease, long-QT syndrome), examine, and refer to cardiology.[7]
- New psychosis on stimulant (rare, usually high-dose or predisposed) — stop stimulant; assess and treat psychosis; resume ADHD treatment only with specialist input once psychosis resolved.
- Severe, persistent tics or Tourette exacerbation on stimulant — reduce dose or switch to atomoxetine or alpha-2 agonist.
- Acute stimulant overdose (accidental or intentional; diversion-related) — syndrome of sympathomimetic excess: agitation, hypertension, tachycardia, hyperthermia, mydriasis, seizures, rhabdomyolysis. Manage with benzodiazepines (lorazepam 2-4 mg IV, titrate), alpha-blockers (phentolamine) for hypertension, cooling, IV fluids, supportive care; avoid beta-blockers alone (unopposed alpha stimulation).[1]
Driving safety — newly diagnosed adults on stimulants should be counselled that ADHD confers a significantly higher risk of motor-vehicle crashes (2-4-fold), and effective treatment reduces this risk. The General Medical Council (UK) and equivalent bodies require patients to be advised; in India, no formal DVLA-equivalent notification is required for stable ADHD on treatment.[7]
Management — Definitive & Stepwise
Treatment is age-stratified, severity-stratified, and multimodal. The framework below follows NICE NG87 (UK) and AACAP 2019 (US) with India/regional notes.[1][7][8]
Step 1 — Recognise, assess, and offer general advice. Psychoeducation (child, parents, school); address sleep, diet, exercise; consider environmental modifications at school (seating near teacher, chunking tasks, movement breaks).[7]
Step 2 — Pre-school children (under 6): behavioural therapy FIRST, no medication.[8]
- Group parent-training programme (the gold-standard first-line for under-6) — Incredible Years, Triple P (Positive Parenting Program), Triple-step Parent-Child Interaction Therapy (PCIT). These teach consistent limit-setting, positive reinforcement, ignoring low-level undesirable behaviour, and structured routine.
- Behavioural classroom interventions — token economy, daily report card.
- Medication is NOT first-line under 6. Use only if severe impairment unresponsive to a course of behavioural intervention; if used, start at low dose (e.g. methylphenidate 1.25-2.5 mg/day) under specialist supervision.[4]
Step 3 — School-age (6-17) and adults: stimulants first-line, behavioural as adjunct.[7][8]
Stimulants (first-line for 6+ and adults — see drug table):[2][4]
| Drug | Class / mechanism | Formulation | Starting dose | Titration | Typical effective dose | Max |
|---|---|---|---|---|---|---|
| Methylphenidate (Ritalin, Concerta, Equasym, Medikinet) | Blocks DAT/NET | IR (Ritalin), MR/ODT, OROS (Concerta) | 5 mg IR bd (child); 18 mg OD Concerta | Weekly increases | ~1 mg/kg/day IR; Concerta 36-54 mg OD | IR 60 mg/day (some 1 mg/kg); Concerta 54-108 mg/day |
| Lisdexamfetamine (Vyvanse, Elvanse) | Prodrug → dexamfetamine; promotes DA/NA release + reverses transporter | Capsule (chewable/ dispersion) | 30 mg OD (adult/child 6+) | Weekly by 20 mg | 50-70 mg OD | 70 mg OD |
| Dexamfetamine (Dexedrine) | Promotes release + reverses transporter | IR, MR | 5 mg od-bd | Weekly | 20-40 mg/day | 60 mg/day |
| Mixed amphetamine salts (Adderall) | Combination | IR, XR | 5 mg od | Weekly | 20-40 mg/day | 40 mg/day (US) |
Non-stimulant drugs (when stimulants fail/are contraindicated, or comorbidity dictates):[2][4][7]
| Drug | Class / mechanism | Starting dose | Effective dose | Onset | Indication |
|---|---|---|---|---|---|
| Atomoxetine (Strattera) | Selective NA reuptake inhibitor | 0.5 mg/kg/day for 7 days | 1.2-1.4 mg/kg/day | 4-6 weeks | Substance use comorbidity; tics/Tourette; anxiety; adult preference |
| Guanfacine MR (Intuniv) | Alpha-2A agonist | 1 mg OD | 4-7 mg/day (weight-banded) | Days-weeks | Hyperactivity, oppositionality, tics, sleep |
| Clonidine MR (Kapvay) | Alpha-2 (non-selective) agonist | 0.1 mg OD | 0.1-0.4 mg/day | Days-weeks | Hyperactivity, tics, sleep, oppositionality |
Adult ADHD — NICE NG87 stepped approach:[7]
- Drug treatment is first-line for adults with moderate/severe ADHD (different from children — behavioural therapy alone is rarely sufficient in adults).
- Lisdexamfetamine first-line; switch to methylphenidate if lisdexamfetamine is poorly tolerated or ineffective.
- Atomoxetine if substance use comorbidity, intolerance to stimulants, or patient preference for non-stimulant.
- CBT for executive function as adjunct; workplace and educational accommodations; driving advice.[2]
Monitoring on stimulants (mandatory):[7]
- Height and weight at baseline, then 6-monthly, plotted on centile chart. If growth velocity slows by more than expected (around 1 cm/year height deficit in early treatment), consider drug holidays, dose reduction, or switch to atomoxetine.
- Blood pressure and heart rate at baseline, after each dose change, and at 3-6-monthly review.
- ECG if any cardiac symptoms or family history of sudden cardiac death.
- Appetite, sleep, mood, tics at every visit — taken from parent AND child/adult.
- Diversion/misuse — lisdexamfetamine preferred; no early refills; controlled-drug prescribing rules.
- Drug holidays — optional weekend/school-holiday breaks to mitigate growth/appetite effects; balance against rebound and functional impairment.[7]
Contraindications to stimulants:[7]
- Symptomatic cardiovascular disease, structural heart defects, cardiomyopathy, arrhythmia, known long-QT.
- Severe anxiety, agitation, or psychosis (stimulants can worsen).
- Hyperthyroidism (uncontrolled).
- Glaucoma (narrow-angle).
- Current MAOI use (hypertensive crisis).
- History of substance use disorder — relative contraindication; prefer lisdexamfetamine (prodrug) or atomoxetine.
- Severe tic disorder / Tourette — not absolute; many tolerate stimulants; consider atomoxetine or alpha-2 agonist first.[7]
Combined / multimodal therapy for moderate-severe: the MTA Cooperative Group 14-month randomised trial (1999) showed combined medication management + behavioural therapy was superior to community care and to behavioural therapy alone for core ADHD symptoms; long-term follow-up showed the medication advantage attenuates but combined remained best for some outcomes.[3] Network meta-analyses (Cortese 2018; Catalá-López 2017) confirm stimulants and atomoxetine effective; behavioural alone less so for core symptoms.[2][4]
Specific Subtypes & Scenarios
ADHD with comorbid tics or Tourette syndrome — prefer alpha-2 agonists (guanfacine, clonidine) or atomoxetine; stimulants are NOT absolutely contraindicated and many children tolerate them well; the older view that stimulants precipitate tics has been revised.[5]
ADHD with comorbid anxiety or depression — stimulants may improve mood by reducing functional impairment; SSRIs are safe to combine with stimulants; atomoxetine is useful when anxiety is prominent (also has anti-anxiety effect). Treat both.[2]
ADHD with comorbid bipolar disorder — stabilise the mood FIRST (mood stabiliser/atypical antipsychotic); add stimulant only once euthymic, with close monitoring — stimulants can precipitate mania in the untreated bipolar patient.[1]
ADHD with comorbid autism spectrum disorder — lower stimulant doses; expect more adverse effects (irritability, tics); behavioural intervention is a bigger component; atomoxetine and alpha-2 agonists often better tolerated.[1]
ADHD with comorbid substance use disorder — prefer atomoxetine or lisdexamfetamine (prodrug, less abuse/diversion); avoid short-acting stimulants; treat the SUD concurrently; do NOT withhold ADHD treatment — treating ADHD reduces SUD relapse risk.[5]
ADHD with comorbid oppositional defiant disorder (ODD) or conduct disorder (CD) — combined stimulant + behavioural parent management training is first-line; risperidone (low dose, 0.5-1 mg/day) only if severe aggression is refractory and after careful risk-benefit discussion (weight gain, metabolic, prolactin).[1]
Pre-school ADHD (under 6) — behavioural parent-training first; medication only if severe impairment unresponsive to behavioural course; if used, low-dose methylphenidate under specialist supervision.[8]
Adult ADHD — lisdexamfetamine first-line (NICE); methylphenidate alternative; atomoxetine if substance use; ASRS screener for diagnosis; CBT for executive function (planning, prioritising, time management); workplace and educational accommodations (extra time in exams, structured environment); driving advice.[7]
ADHD in girls and women — inattentive presentation more common; under-diagnosed; more internalising comorbidity; hormonal effects — premenstrual worsening, pregnancy/postpartum vulnerability; consider premenstrual pattern when planning drug timing.[1]
ADHD in intellectual disability — lower doses; more behavioural input; expect more adverse effects; use established rating scales modified for developmental level.[1]
Complications & Pitfalls
Stimulant adverse effects (and management):[1][7]
- Appetite suppression and weight loss — common; give stimulant with/after breakfast, high-calorie evening meal, drug holidays.
- Growth delay — ~1 cm/year height velocity reduction in early treatment, often normalises by adulthood; monitor centile chart; drug holidays if marked.
- Insomnia / sleep disturbance — avoid late afternoon IR; switch to MR; address sleep hygiene; melatonin if needed.
- Headache, abdominal pain — common, usually mild; reduce dose.
- Irritability and rebound — particularly as the dose wears off (afternoon for IR); switch to MR or add a small IR top-up dose; some children have a 'zombie' effect at too-high dose — reduce.
- Tachycardia, hypertension — monitor; reduce dose if persistent; check for hyperthyroidism.
- Jitteriness, anxiety — reduce dose; consider atomoxetine.
- Bruxism, skin-picking — dose-related; reduce.
- Psychosis (rare, high-dose, predisposed) — stop stimulant; assess; refer.
- Tics — not necessarily caused by stimulants; many tolerate; reduce dose or switch.
- Priapism (rare with methylphenidate) — medical emergency.[7]
Atomoxetine adverse effects (and management):[1][7]
- Abdominal pain, decreased appetite, nausea — common; take with food.
- Somnolence or fatigue — give in evening; reduce dose.
- Mood swings, irritability — reduce or switch.
- Hepatotoxicity (rare but FDA black-box) — stop if jaundice, RUQ pain, raised LFTs; check LFTs.
- Suicidal ideation (FDA black-box in children/adolescents) — monitor mood; stop if emerges.
- Cardiovascular — small rise in BP/HR; monitor.[2]
Alpha-2 agonist adverse effects:[7]
- Sedation, dry mouth, constipation — common; give at bedtime.
- Hypotension, bradycardia — monitor; caution in those with conduction defects.
- Rebound hypertension on abrupt withdrawal — taper slowly.[7]
Diversion and misuse — stimulants are Schedule II (US) / Class B (UK) controlled drugs; prescribed under controlled-drug regulations; lisdexamfetamine prodrug preferred; no early refills; monitor用量.[7]
Cardiovascular concern — small but measurable rise in BP/HR; concern about sudden death in those with structural heart disease — screen by history, examination, ECG if indicated; avoid in symptomatic cardiac disease.[7]
Classic diagnostic and treatment pitfalls:[1][5]
- Diagnosing from one setting only (teacher reports hyperactive but parents say fine) — fails pervasiveness criterion.
- Missing comorbid anxiety, depression, ODD, ASD, SUD — undertreating.
- Mislabelling autism or fragile X as ADHD — different treatment.
- Ignoring sleep deprivation / OSA / insufficient sleep — mimics and worsens ADHD.
- Failing to screen adults — adult ADHD is highly treatable and under-recognised; screen with ASRS in any adult with lifelong inattention, disorganisation, time blindness and emotional dysregulation.
- Withholding medication in adolescents with SUD history — treating ADHD reduces SUD relapse.
- Initiating stimulant during acute mania/psychosis/SUD intoxication — wait until stabilised.[4]
Prognosis & Disposition
Persistence: ADHD persists into adulthood in ~60 percent — about 15 percent meet full criteria and ~45 percent are in partial remission (subthreshold but impairing). Hyperactivity symptoms decline most with age; inattention and executive dysfunction persist.[1][5]
Predictors of good outcome: early diagnosis, treatment adherence, absence of comorbid conduct disorder and SUD, intact and supportive family, average or higher IQ, access to educational accommodations, good response to medication.[1]
Predictors of poor outcome: untreated ADHD; comorbid conduct disorder (the single biggest adverse prognostic factor); family history of antisocial behaviour or SUD; low socio-economic status; academic failure; early substance use; driving offences; family conflict.[1]
Long-term risks of untreated ADHD: school drop-out, unemployment and job instability, motor-vehicle crashes (the leading cause of excess mortality in adolescent ADHD), substance use disorders, incarceration (over-represented in prison populations), relationship breakdown, divorce, bankruptcy, suicide. Effective treatment substantially reduces these risks.[5]
Follow-up cadence:[7]
- Titration phase — weekly review until effective dose found.
- Stable phase — 3-6-monthly specialist review (growth, BP/HR, symptoms, comorbidity, side effects, functioning, school/work).
- Shared care — GP continues prescribing under shared-care protocol once stable; specialist reviews annually.[5]
When can medication be reviewed or withdrawn?[7] When the patient has been symptom-free and functionally recovered for at least 1 year, consider a carefully supervised trial off medication (typically in late adolescence or adulthood) — reinitiate if symptoms recur. Always stop stimulants gradually (taper to avoid rebound, especially with alpha-2 agonists to avoid rebound hypertension).
Special Populations
Pre-school children (under 6) — behavioural parent-training first; medication only if severe impairment unresponsive to behavioural course; lower stimulant doses; methylphenidate is only licensed from age 6 in the UK (NICE NG87).[7][8]
Girls and women — inattentive presentation; under-diagnosed; more internalising comorbidity; premenstrual symptom worsening; careful screening; consider hormonal effects.[1]
Pregnancy and breastfeeding — weigh risk-benefit in perinatal psychiatry MDT; stimulants cross the placenta and are excreted in breast milk; data are limited; methylphenidate is sometimes continued if benefits outweigh (small increased risk of cardiac defects reported); lisdexamfetamine generally avoided in pregnancy; atomoxetine has limited data; involve perinatal psychiatry for individualised decision.[7]
Adults — lifelong traits, executive-function deficits, driving risk, employment, relationships, comorbidities; lisdexamfetamine first-line (NICE); ASRS screener; CBT for executive function; workplace accommodations.[7]
Substance use comorbidity — prefer atomoxetine or lisdexamfetamine (prodrug); avoid short-acting stimulants; treat SUD concurrently.[5]
Intellectual disability / autism — lower stimulant doses; more behavioural input; expect more adverse effects; atomoxetine and alpha-2 agonists often better tolerated.[1]
Elderly — limited evidence; cardiovascular and polypharmacy comorbidity raise risk; start low and go slow; atomoxetine often preferred.[1]
Evidence, Guidelines & Regional Differences
Landmark trials:[3]
- MTA Cooperative Group 14-month randomised trial (1999, Arch Gen Psychiatry) — 579 children randomised to medication management (methylphenidate titrated), behavioural therapy, combined, or community care. Combined was superior to community care and to behavioural alone for core ADHD symptoms at 14 months. Long-term follow-up (2009) showed the medication advantage attenuated over time; combined remained best for some outcomes. Key message: multimodal, individualised treatment is best.[3]
- Cortese 2018 (Lancet Psychiatry) — network meta-analysis of medications in children, adolescents and adults; methylphenidate in children/adolescents and amphetamines in adults were the most efficacious in the short term; tolerability favoured methylphenidate in children/adolescents.[4]
- Catalá-López 2017 (PLoS One) — network meta-analysis confirming stimulants and atomoxetine effective in children/adolescents; behavioural therapy alone less effective for core symptoms.[2]
International consensus:[5]
- Faraone et al. World Federation of ADHD International Consensus Statement (2021, Neurosci Biobehav Rev) — 208 evidence-based conclusions; ADHD is a valid, heritable, neurobiological disorder; effective treatment exists; untreated ADHD carries substantial lifelong risk.[5]
Guidelines and regional differences:[7][8][9][10]
- NICE NG87 (UK, 2018, updated 2024)[7] — group parent-training first under 6; methylphenidate first-line for 6-17 after specialist diagnosis; lisdexamfetamine first-line for adults; atomoxetine/guanfacine alternatives; ECG only if cardiac history; shared care with GP.
- AACAP 2019 (US, Pediatrics)[8] — behavioural therapy first for pre-school (4-5 years); stimulant medication (preferably with behavioural) for 6-11; stimulant +/- behavioural for 12-18; emphasises parent training and school supports.
- DSM-5-TR (2022, US)[9] — onset before 12 (was 7 in DSM-IV); adults 17+ need 5+ symptoms (was 6); three presentations.
- ICD-11 (2022, WHO)[10] — renamed 'ADHD' (replaces 'Hyperkinetic disorder' of ICD-10); now under Neurodevelopmental Disorders (6A05); harmonised with DSM-5.
Indian context (IAP / Indian Psychiatric Society): methylphenidate first-line for 6 and over (strictly controlled — Schedule X in India, restricted to specialists); atomoxetine available; behavioural parent-training and school programme; specialist (paediatrician or psychiatrist) initiation. Lisdexamfetamine availability varies; atomoxetine widely used.[9]
- Overdiagnosis / medicalisation — broadened DSM-5 criteria and reduced age-of-onset threshold raised concern; prevalence rise partly reflects better recognition, not just overdiagnosis.
- Long-term stimulant effects — growth (~1 cm/year early, often normalises), cardiovascular (small BP/HR rise; sudden death only in structural heart disease), diversion.
- Neuroethics of cognitive enhancement — stimulant use by those without ADHD to enhance performance; medical and ethical concerns.[6]
ADHD — MTA / mnemonic for the management order
MOTIV8
First-line stimulant for children 6+ — blocks DAT/NET
DSM-5-TR criterion B — was 7 in DSM-IV
Criterion C — pervasiveness; parent AND teacher reports
6+ of 9 in each domain (children); 5+ (adults)
SNAP-IV, Conners-3, Vanderbilt (children); ASRS (adults)
First-degree relatives have ~8-fold increased risk; heritability 74-88%
Exam Pearls
- ADHD = inattention + hyperactivity + impulsivity since before age 12, in 2+ settings, impairing, not better explained.[9]
- Prevalence ~5 percent children, ~2.5 percent adults; M:F 3:1 clinic, 2:1 community; heritability 74 to 88 percent (twin studies).[6]
- DSM-5-TR thresholds: 6+ of 9 inattention and/or 6+ of 9 hyperactivity-impulsivity in children; 5+ in adults 17+; symptoms at least 6 months; several before age 12 (was before 7 in DSM-IV).[9]
- Three presentations: predominantly inattentive (the old "ADD"), predominantly hyperactive-impulsive, combined.[9]
- Mechanism: underactive prefrontal cortex; deficient dopamine/noradrenaline at PFC synapse; inverted-U dose-response — stimulants restore the apex, hence a stimulant can calm hyperactivity.[5]
- Methylphenidate = blocks DAT/NET; amphetamines (lisdexamfetamine) = promotes release + reverses transporter; atomoxetine = selective NA reuptake inhibitor (slower, non-addictive; black-box hepatotoxicity and suicidal ideation); guanfacine/clonidine = alpha-2 agonists (hyperactivity, tics, sleep, oppositionality).[4]
- Lisdexamfetamine is a prodrug (cleaved by RBC esterase to dexamfetamine) — slow onset, less abuse/diversion, first-line in adults (NICE).[7]
- Behavioural therapy first under 6; stimulants first-line 6+; combined stimulant + behavioural best for moderate-severe (MTA trial).[3][8]
- Stimulant monitoring: height/weight 6-monthly (centile chart), BP/HR, appetite, sleep, mood, tics; ECG only if cardiac history.[7]
- Comorbidity dictating first-line: tics/Tourette/SUD/anxiety → atomoxetine or alpha-2 agonist; bipolar → stabilise mood FIRST.[1]
- ASRS-v1.1: 6-item adult screener, 4 of 6 in shaded boxes = positive.[1]
- MTA trial (1999): landmark; combined medication + behavioural best short-term.[3]
- ADHD persists in ~60 percent of adults (full ~15 percent, partial ~45 percent).[1]
- Classic differentials: hyperthyroidism, sleep apnoea, hearing/visual impairment, absence seizures, fragile X, fetal alcohol spectrum disorder, lead poisoning, autism, anxiety, bipolar (stabilise mood first).[1]
- Cardiovascular: avoid stimulants in symptomatic cardiac disease, structural heart defects, long-QT, severe hypertension, uncontrolled hyperthyroidism.[7]
- Atomoxetine black-boxes: hepatotoxicity AND suicidal ideation.[1]
- Driving risk: 2-4-fold increased motor-vehicle crashes in untreated ADHD; treatment reduces risk.[1]
Exam application bank (NEET-PG / INICET)
One-line answer
ADHD is a neurodevelopmental disorder characterised by persistent, pervasive, impairing inattention, hyperactivity, and impulsivity with onset before age 12 and symptoms present in two or more settings (home, school, work). Prevalence about 5 percent of children, 2.5 percent of adults; clinic male-to-female ratio 3:1 (community 2:1); heritability 74 to 88 percent — among the highest in psychiatry. DSM-5-TR: 6+ inattention and/or 6+ hyperactivity-impulsivity symptoms in children (5+ in adults 17+), for at least 6 months, several before age 12, in 2+ settings, causing impairment, not better explained. Three presentations: predominantly inattentive, predominantly hyperactive-impulsive, combined. Treat: behavioural parent-training first for children under 6; stimulants first-line for 6+ (methylphenidate blocks dopamine/noradrenaline transporters; lisdexamfetamine promotes release — 70 to 80
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard.[1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes.[1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change.[1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each.[2]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory.[1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Attention Deficit Hyperactivity Disorder (ADHD).
References
- [1]Thapar A, Cooper M, Jefferies R, Stergiakouli E. Attention deficit hyperactivity disorder. Lancet, 2016.PMID 26386541
- [2]Catalá-López F, Hutton B, Núñez-Beltrán A, et al. The pharmacological and non-pharmacological treatment of attention deficit hyperactivity disorder in children and adolescents: A systematic review with network meta-analyses of randomised trials. PLoS One, 2017.PMID 28700715
- [3]MTA Cooperative Group. A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder. Archives of General Psychiatry, 1999.PMID 10591283
- [4]Cortese S, Adamo N, Del Giovane C, et al. Comparative efficacy and tolerability of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: a systematic review and network meta-analysis. Lancet Psychiatry, 2018.PMID 30097390
- [5]Faraone SV, Banaschewski T, Coghill D, et al. The World Federation of ADHD International Consensus Statement: 208 Evidence-based conclusions about the disorder. Neuroscience & Biobehavioral Reviews, 2021.PMID 33549739
- [6]Polanczyk G, de Lima MS, Horta BL, Biederman J, Rohde LA. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. American Journal of Psychiatry, 2007.PMID 17541055
- [7]Posner J, Polanczyk GV, Sonuga-Barke E Attention-deficit hyperactivity disorder. Lancet (London, England), 2020.PMID 31982036
- [8]Subcommittee on Attention-Deficit/Hyperactivity Disorder, Steering Committee on Quality Improvement and Management, Wolraich M, et al. ADHD: clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics, 2011.PMID 22003063
- [9]First MB Diagnostic and statistical manual of mental disorders, 5th edition, and clinical utility. The Journal of nervous and mental disease, 2013.PMID 23995026
- [10]Döpfner M, Banaschewski T [Classification of Attention Deficit-/Hyperactivity Disorder in ICD-11]. Zeitschrift fur Kinder- und Jugendpsychiatrie und Psychotherapie, 2021.PMID 34974734