Psychiatry · Psychiatry
Child & Adolescent Psychiatry
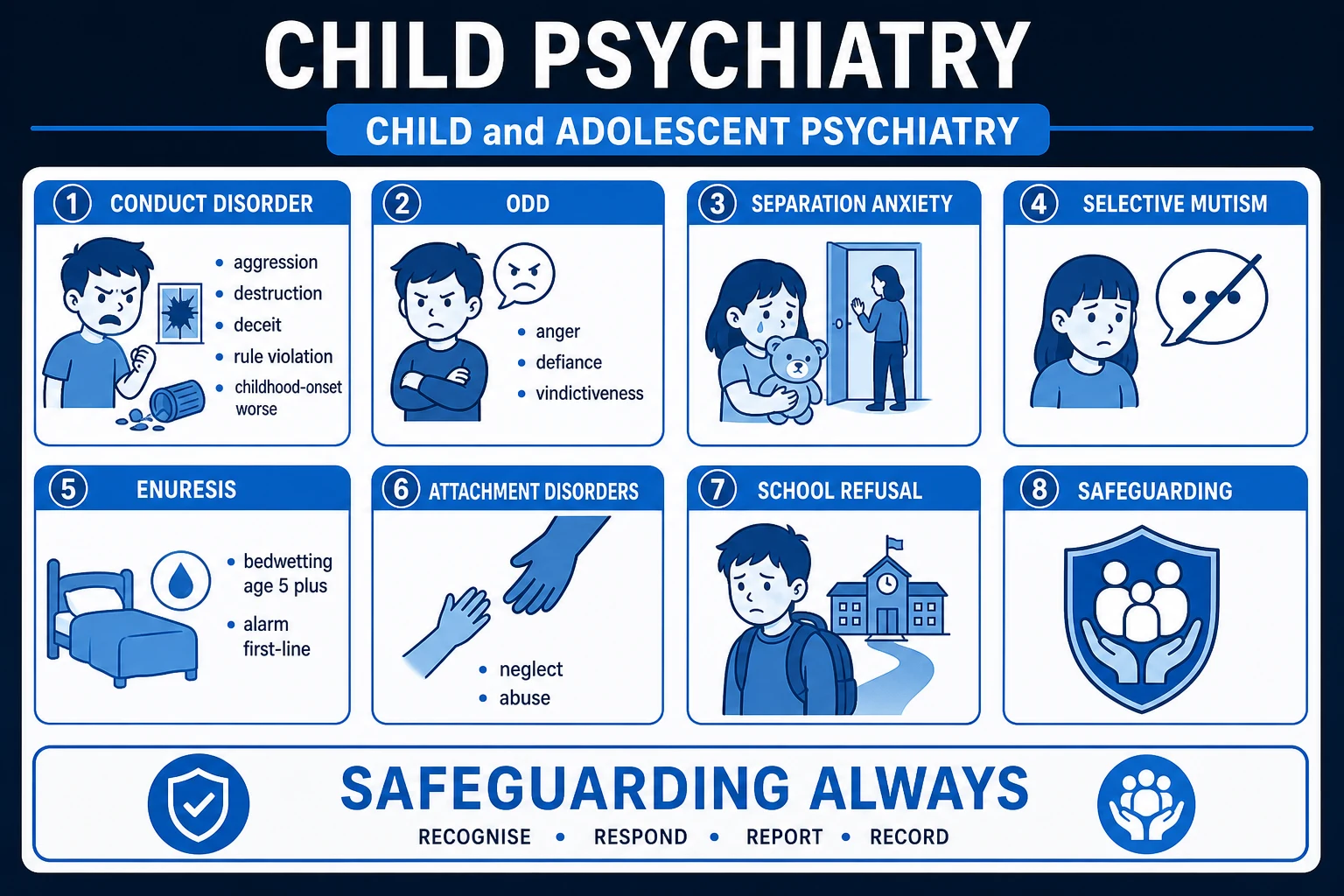
Also known as Child psychiatry · Paediatric mental health · Conduct disorder · Oppositional defiant disorder · Separation anxiety disorder · Selective mutism · Enuresis · Encopresis · Reactive attachment disorder · School refusal
Child and adolescent psychiatry covers mental disorders from birth to age 18, with every symptom assessed in developmental context against age-appropriate norms. The high-yield disorders are: Conduct disorder (CD) — a repetitive, persistent pattern of behaviour that violates the rights of others or age-appropriate norms (aggression to people/animals, destruction of property, deceit/theft, serious rule violation; at least 3 of 15 criteria in 12 months); Oppositional defiant disorder (ODD) — angry/irritable mood, argumentative/defiant behaviour, vindictiveness without aggression or rights violation; Separation anxiety disorder — excessive, developmentally inappropriate fear of separation lasting at least 4 weeks; Selective mutism — consistent failure to speak in social situations despite speaking elsewhere; Enuresis — repeated involuntary urination, age at least 5; Encopresis — repeated faecal soiling, age at least 4; and the attachment disorders (reactive attachment disorder, disinhibited social engagement disorder) that follow grossly pathogenic care. Management is built on one principle: behavioural and psychological interventions are first-line — parent training programmes (Triple P, Incredible Years, PCIT) for ODD/CD, CBT for anxiety/depression, the enuresis alarm (not drugs) for bedwetting, treating constipation first for encopresis, and safeguarding every child. Medication is a last resort in children.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags

Overview & Definition
Child and adolescent psychiatry is the branch of psychiatry concerned with the assessment, diagnosis and treatment of mental disorders in children and young people from birth to 18 years. It differs from adult psychiatry in five ways that decide almost every exam answer:[1]
- Developmental context is everything. A symptom is abnormal only if it is inappropriate for the child's age and developmental stage. A two-year-old's tantrum is normal; the same behaviour in an eight-year-old, persisting across settings and impairing function, is not. Always ask: "Is this behaviour expected at this age, in this setting, at this frequency and severity?"
- The family is central to both cause and treatment. Most childhood disorders are maintained or ameliorated by the family environment, and parent training is often more effective than treating the child directly.
- School is the child's main social environment. School liaison, educational accommodation, anti-bullying work and gradual reintegration are core therapeutic tools — particularly for school refusal, selective mutism and anxiety.
- Most conditions improve with early intervention, and untreated childhood disorders seed adult psychopathology (CD is the developmental precursor of antisocial personality disorder; separation anxiety of adult panic/agoraphobia).
- Safeguarding is every doctor's responsibility. Abuse, neglect and exploitation must be actively considered and acted on in every child seen — the safety of the child is paramount.[4]
The clinical skill in child psychiatry is therefore not making a single diagnosis (the categories are well defined) but integrating information from multiple informants (child, parents, school), placing the behaviour in its developmental and family context, recognising comorbidity (which is the rule, not the exception), and constructing a multimodal, multi-agency treatment plan — while keeping the child safe.[2]
Classification
Child psychiatric disorders are grouped in the DSM-5 and ICD-11 into broad clusters. This topic covers the high-yield categories most often examined:[1][3]
- Disruptive, impulse-control and conduct disorders — Oppositional defiant disorder (ODD) and Conduct disorder (CD); intermittent explosive disorder; pyromania; kleptomania.
- Anxiety disorders of childhood — Separation anxiety disorder; selective mutism; social anxiety; generalised anxiety; specific phobia.
- Trauma- and stressor-related disorders — Reactive attachment disorder (RAD); disinhibited social engagement disorder (DSED); post-traumatic stress disorder; adjustment disorders.
- Elimination disorders — Enuresis; encopresis.
- Neurodevelopmental disorders (covered in dedicated topics) — ADHD, autism spectrum disorder, intellectual disability, specific learning disorders, tic disorders/Tourette syndrome.[1]
ODD
- Angry/irritable mood, argumentative/defiant behaviour, vindictiveness
- at least 4 symptoms for 6 months, causing distress/impairment
- Does NOT violate the rights of others
- Often precedes CD; treat with parent training
- Irritable subtype predicts later depression/anxiety
CD
- Aggression to people/animals, destruction of property, deceit/theft, serious rule violation
- at least 3 of 15 criteria in past 12 months, at least 1 in past 6 months
- DOES violate the rights of others / age-appropriate norms
- Childhood-onset (before 10) worse prognosis, callous-unemotional traits
- Parent training + Multisystemic Therapy for severe cases
Separation anxiety
- Excessive, developmentally inappropriate fear about separation
- Lasts at least 4 weeks (children)
- Distress when separated, worry about harm to attachment figures, school refusal
- CBT with exposure first-line
- May precede adult panic/agoraphobia
The CD severity specifiers (DSM-5) are themselves examined: mild = few conduct problems causing minor harm; moderate = number and effect between mild and severe; severe = many problems causing considerable harm. The callous-unemotional (CU) traits specifier is added when the child shows lack of guilt or empathy, shallow affect, and unconcern about performance — this marks a more severe, treatment-resistant form with strong genetic loading.[1]

Epidemiology & Risk Factors
Worldwide, 10 to 20 percent of children and adolescents have a diagnosable mental disorder, and half of all lifetime mental illness begins by age 14 — yet most go unrecognised and untreated. Recognition and early intervention are therefore among the most consequential things a doctor can do.[2]
Child & adolescent psychiatry — key numbers
Risk factors for the disruptive behaviour disorders (CD/ODD) cluster at multiple levels and are favourite examiner territory:[1][3]
- Child level — male sex (for CD), difficult temperament, callous-unemotional traits, low heart rate and low cortisol (low autonomic arousal = sensation-seeking), low IQ, ADHD, learning disability.
- Family level — harsh, inconsistent or abusive parenting; parental mental illness, substance misuse or criminality; parental conflict and domestic violence; large sibship; low socio-economic status.
- School/peer level — school failure, bullying (victim or perpetrator), peer delinquency, school exclusion.
- Community level — neighbourhood deprivation, exposure to violence, lack of safe recreational space.[3]
Special populations with markedly elevated rates of all child psychiatric disorders: looked-after and foster children, refugees and asylum-seekers, children exposed to war or disaster, and children of parents with severe mental illness or substance dependence.[6]
Pathophysiology
Child psychiatric disorders arise from the interaction of genetic vulnerability with early environmental experience acting on a developing brain. The central, examinable principle is that the brain is highly plastic in childhood — the same plasticity that makes the child vulnerable to adversity (neglect, trauma, harsh parenting) also makes early intervention effective.[1][6]
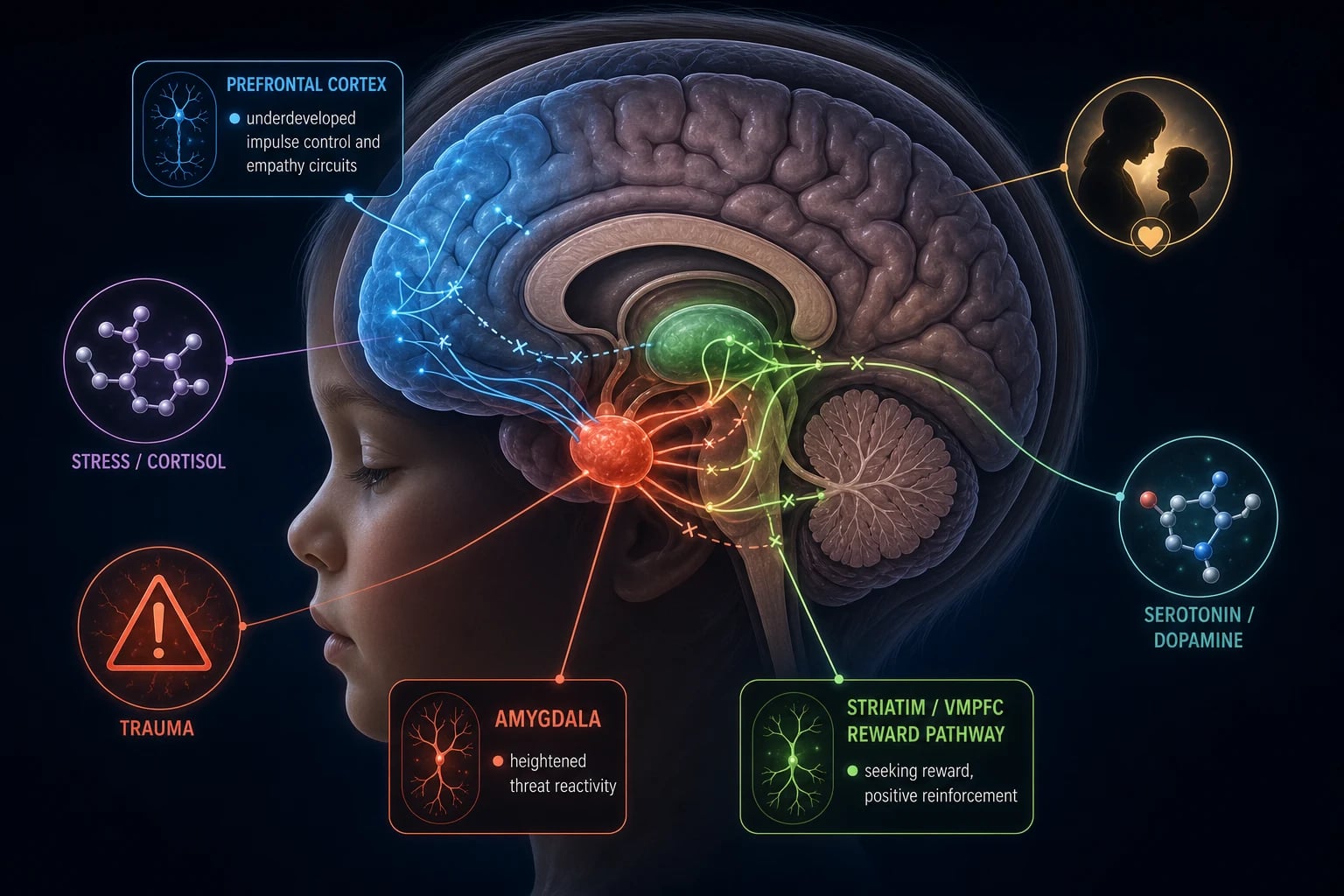
Conduct disorder exemplifies the gene-environment model. Heritability is about 50 percent, but genes act by modulating how the child responds to — and selects — environments. The core neural finding is disruption in the amygdala-prefrontal circuit that subserves empathy, threat processing and impulse control:[1]
- Reduced amygdala reactivity to others' distress cues (fearful/sad faces) → the child does not learn the aversive emotional value of harming others → callous-unemotional traits (lack of empathy and guilt).
- Impaired prefrontal top-down control (ventromedial and dorsolateral prefrontal cortex) → poor inhibition, impulsivity, inability to weigh long-term consequences.
- Low autonomic arousal (low resting heart rate, low cortisol) → under-aroused children seek sensation through risky, aggressive behaviour to raise arousal to a comfortable level.
- Striatal reward-processing differences → heightened sensitivity to immediate reward relative to punishment, biasing toward rule-breaking.[6]
The environmental layer amplifies this: harsh and inconsistent parenting, parental modelling of aggression, exposure to violence, and association with delinquent peers all reinforce antisocial learning. Adverse childhood experiences (ACEs) — abuse, neglect, household dysfunction — produce lasting changes in the hypothalamic-pituitary-adrenal (HPA) axis (dysregulated cortisol), in amygdala volume and reactivity, and in prefrontal-limbic connectivity, which underpin the attachment disorders, PTSD and much of the emotional dysregulation seen clinically.[2][6]
Separation anxiety arises from a combination of insecure attachment, parental overprotection or anxiety (modelled), and temperamental behavioural inhibition, with dysregulation of threat circuits and the HPA axis producing an exaggerated, persistent fear response to separation cues.[2]
Enuresis is best understood as a maturational disorder with three interacting mechanisms:[5]
- Failure of arousal from sleep — the child does not wake to the sensation of a full bladder (the most important factor; the problem happens during sleep).
- Reduced nocturnal surge of arginine-vasopressin (AVP) — at night a normal child secretes extra AVP to concentrate urine and reduce volume; enuretic children have an inadequate AVP surge, producing nocturnal polyuria that exceeds bladder capacity. (This is the rationale for desmopressin, a synthetic AVP analogue.)
- Reduced functional bladder capacity / detrusor overactivity in some children.[5]
Enuresis is strongly genetic: an autosomal dominant trait with about 44 percent of children affected if one parent was enuretic and 77 percent if both parents were — a favourite MCQ fact.[5]
Clinical Presentation
Conduct disorder
A repetitive and persistent pattern of behaviour in which the rights of others or major age-appropriate societal norms are violated, with at least 3 of the following 15 criteria present in the past 12 months, with at least 1 in the past 6 months, grouped into four categories:[1][3]
Aggression to people and animals (1) often bullies, threatens or intimidates others; (2) often initiates physical fights; (3) has used a weapon that can cause serious harm; (4) has been physically cruel to people; (5) has been physically cruel to animals; (6) has stolen while confronting a victim; (7) has forced someone into sexual activity.[4]
Destruction of property (8) has deliberately engaged in fire-setting with the intention of causing serious damage; (9) has deliberately destroyed others' property (other than by fire-setting).[1]
Deceitfulness or theft (10) has broken into someone else's house, building or car; (11) often lies to obtain goods or favours or to avoid obligations (i.e. "cons" others); (12) has stolen items of non-trivial value without confronting a victim (shoplifting, forgery).[1]
Serious violation of rules (13) often stays out at night despite parental prohibitions, beginning before age 13; (14) has run away from home overnight at least twice (or once for a prolonged period); (15) is often truant from school, beginning before age 13.[3]
Specify onset type: childhood-onset (at least one symptom before age 10) — more often male, physically aggressive, with callous-unemotional traits and poor long-term prognosis; adolescent-onset — less aggression, better prognosis, less likely to progress to adult antisocial personality disorder.[3]
Oppositional defiant disorder
A pattern of angry/irritable mood, argumentative/defiant behaviour, or vindictiveness lasting at least 6 months, with at least 4 symptoms present during that interaction with at least one individual who is not a sibling, causing distress or impairment. Crucially, ODD does not involve aggression toward people or animals, destruction of property, theft or deceit, or serious rule violation — those move the diagnosis to CD.[3]
- Angry/irritable mood: often loses temper; is often touchy or easily annoyed; is often angry and resentful.
- Argumentative/defiant behaviour: often argues with authority figures or adults; often actively defies or refuses to comply with requests or rules; often deliberately annoys others; often blames others for mistakes or misbehaviour.
- Vindictiveness: has been spiteful or vindictive at least twice within the past 6 months.[4]
Separation anxiety disorder
Developmentally inappropriate and excessive fear or anxiety concerning separation from those to whom the individual is attached, lasting at least 4 weeks in children (6 months in adults), causing significant distress or impairment:[2]
- Recurrent excessive distress when separation from home or major attachment figures occurs or is anticipated.
- Persistent and excessive worry about losing major attachment figures, or about possible harm to them (illness, injury, disaster, death).
- Persistent reluctance or refusal to go out, away from home, to school or elsewhere, for fear of separation.
- Persistent and excessive fear or reluctance about being alone or without major attachment figures at home or in other settings.
- Persistent reluctance or refusal to sleep away from home or to go to sleep without being near a major attachment figure.
- Repeated nightmares involving the theme of separation.
- Repeated complaints of physical symptoms (headache, abdominal pain, nausea, vomiting) when separation occurs or is anticipated.[2]
Selective mutism
Consistent failure to speak in specific social situations in which there is an expectation for speaking (e.g. at school, with peers) despite speaking in other situations (e.g. at home with family), lasting at least 1 month (not limited to the first month of school, which is normal shyness), causing distress or impairment. The child may communicate by gesture, nodding or whispering, or may be entirely mute in the feared setting. Social anxiety disorder is the commonest comorbidity; the child is not autistic and has normal language in safe settings.[2]
Enuresis
Repeated voiding of urine into bed or clothes, whether involuntary or intentional, with: chronological age at least 5 years (or equivalent developmental level); behaviour occurring at least twice a week for 3 consecutive months, or causing significant distress/impairment; and not attributable to a substance or medical condition. Specify:[5]
- Primary (never been consistently dry for 6 months) versus secondary (was dry, then relapsed — often after a psychological stressor or medical event).
- Monosymptomatic (night-time only, no day-time symptoms) versus non-monosymptomatic (day-time symptoms too — overactive bladder, urgency, voiding dysfunction).
- Nocturnal only versus diurnal (day-time) only versus both.[5]
Encopresis
Repeated passage of faeces into inappropriate places (clothing, floor), whether involuntary or intentional, with: chronological age at least 4 years (or developmental equivalent); at least once a month for 3 months; not attributable to a substance or medical condition other than constipation. The vast majority of cases are constipation with overflow — the rectum is loaded with hard stool and liquid stool leaks around it. Specify with constipation and overflow incontinence (commonest, treat constipation) versus without constipation and overflow incontinence (rarer, more behavioural).[5]
Attachment disorders (after grossly pathogenic care)
Both require a history of extreme insufficient care (social neglect, deprivation, repeated changes of primary caregiver, rearing in unusual settings that severely limit opportunity to form selective attachments) that is judged responsible for the pattern.[2]
- Reactive attachment disorder (RAD): a pattern of emotionally withdrawn/inhibited behaviour toward adult caregivers — the child minimally seeks or responds to comfort when distressed; persistent social and emotional disturbance (minimal social/emotional responsiveness, limited positive affect, unexplained irritability/sadness/fearfulness even in non-threatening interactions); onset before age 5; developmental age at least 9 months.
- Disinhibited social engagement disorder (DSED): a pattern of behaviour involving reduced or absent reticence in approaching unfamiliar adults — the child approaches, talks to or goes off with unfamiliar adults with no checking back; overly familiar verbal or physical behaviour; diminished or absent checking back with the adult caregiver after venturing away; willingness to go off with an unfamiliar adult with minimal or no hesitation.[2]
Atypical presentation in adolescents
The adolescent brain is in a period of heightened reward-seeking and ongoing prefrontal maturation, so disorders often present through risk behaviour rather than reported symptoms: school refusal and declining attendance; emergent self-harm and suicidality (suicide is among the leading causes of adolescent death); substance use; eating disorders; emerging borderline/emotionally unstable personality features; first-episode psychosis or mania; and delinquency and gang involvement. Always assess risk to self and others and safeguarding in any adolescent presentation.[2]
Differential Diagnosis
Behavioural disturbance in a child is rarely diagnostic on its own. The differentials that decide marks:[1][2]
- CD versus ODD — the pivot is whether the behaviour violates the rights of others. ODD is defiant, hostile and vindictive but involves no aggression, no destruction of property, no theft or deceit, and no serious rule violation. The moment a child bullies with confrontation, sets fires, steals or is truant before age 13, the diagnosis is CD, not ODD.
- CD versus ADHD — children with ADHD are impulsive and may lash out, but the aggression is reactive, short-lived and not goal-directed, lacks sustained antisocial intent, and sits alongside inattention and hyperactivity. The two are highly comorbid (about 40 percent of ADHD), but the diagnoses are distinct and both should be made when criteria are met.
- CD versus antisocial personality disorder (ASPD) — ASPD cannot be diagnosed before age 18 and requires evidence of CD before age 15. CD is the developmental precursor; not every child with CD develops ASPD, but a diagnosis of ASPD in adulthood is invalid without a history of CD in childhood.
- School refusal — a presenting complaint, not a diagnosis. Distinguish the cause: separation anxiety (child wants to stay home with attachment figure, distressed, with parental awareness); bullying or school-based trauma (child fears school specifically); depression (anergia, anhedonia, low mood); specific or social phobia; and truancy (the CD child skips school without anxiety and without parental knowledge).
- Selective mutism versus autism spectrum disorder — the autistic child has a pervasive social-communication deficit and restricted/repetitive behaviours across all settings; the selectively mute child speaks normally in safe settings (e.g. at home) and has no restricted/repetitive behaviours.
- Enuresis — always exclude organic causes first: urinary tract infection (dipstick and culture), diabetes mellitus (polyuria, polydipsia, weight loss), diabetes insipidus (failure of AVP — central or nephrogenic), chronic constipation (loaded rectum irritates the bladder), obstructive sleep apnoea, spinal cord lesion (neurological signs on examination, especially diurnal symptoms), and child sexual abuse (secondary enuresis, especially with other behavioural or somatic signs).
- Behavioural disturbance from a physical cause — unrecognised hearing or visual impairment, thyroid dysfunction, sleep disorder, medication side-effect (e.g. stimulants, steroids), constipation (causing pain and irritability), dental pain, and abuse can all masquerade as a psychiatric presentation in a child who cannot articulate the problem. A hearing and vision check and a focused physical examination are part of every child psychiatric assessment.
- Attachment disorder versus autism/ADHD — RAD and DSED arise specifically after grossly pathogenic care and centre on the child's social engagement with caregivers; autism is present from early development regardless of care quality, and ADHD centres on inattention/hyperactivity/impulsivity rather than attachment behaviour.[4]
Clinical & Bedside Assessment
Assessment is multi-informant and multi-setting — a behaviour reported only at school, or only at home, tells a different story from one that is pervasive. Interview the child alone (age-appropriate), the parents/carers alone, and obtain a school report (teacher SDQ or structured report).[2]
History components:[2]
- Presenting complaint in the child's and parents' own words; onset, course, severity, settings, triggers, consequences.
- Developmental history — pregnancy, birth, perinatal complications; developmental milestones (motor, language, social); temperament; attachment history.
- Family history — parental mental illness, substance misuse, criminality, domestic violence, family functioning, family psychiatric history.
- Adverse childhood experiences (ACEs) — abuse (physical, sexual, emotional), neglect (physical, emotional), household dysfunction (parental separation, household mental illness, incarceration, substance use, domestic violence). Use trauma-informed questioning.
- Social and educational history — friendships, bullying (victim or perpetrator), school attendance and attainment, peer group, screen time, online safety, exploitation risk.[6]
Standardised screening tools:[2]
- Strengths and Difficulties Questionnaire (SDQ) — a brief, well-validated 25-item screening questionnaire for 4 to 17 year-olds, completed by parents, teachers and (for 11 to 17 year-olds) the young person themselves. Yields a total difficulties score and five subscales (conduct, emotional, hyperactivity/inattention, peer relationships, prosocial behaviour). The SDQ is the single most useful triage tool in child mental health and is examinable.[2]
- Vanderbilt ADHD Diagnostic Rating Scale — when ADHD comorbidity is suspected.
Mental state examination adapted for the child: observe play and drawing (projective material), the interaction with the parent (attachment quality, parental responsiveness, coercive cycles), speech and language (for developmental level), mood and affect, thought form and content, perceptual abnormalities, insight and engagement. In younger children, much of the MSE is gathered through observation and play rather than direct questioning.[2]
Safeguarding assessment in every case: ask about and actively look for abuse, neglect, domestic violence and exploitation; examine for unexplained or patterned injuries; be alert to fabricated or induced illness and to child sexual exploitation in adolescents. Know your local child-protection referral pathway — the duty is to refer and protect, not to single-handedly confirm.[6]
Risk assessment: assess self-harm and suicide (especially in adolescents — ask directly, do not believe the myth that asking increases risk), risk to others (aggression, sexual behaviour), risk of exploitation, risk of neglect, and risk of school exclusion and offending. Document the risk assessment and plan.[2]
Investigations
There are no biological tests for the child psychiatric disorders — diagnosis is clinical, against DSM-5 or ICD-11 criteria, using the multi-informant assessment described above. Investigations are used to exclude organic causes of specific presentations and to characterise comorbidity.[1][5]
CD/ODD: clinical diagnosis. Use the SDQ for triage and to track response; structured diagnostic interview (e.g. K-SADS) in specialist settings. Always screen for comorbid ADHD (Vanderbilt), autism, depression, anxiety, learning disability and substance misuse.[1]
Enuresis — the workup is focused and proportionate:[5]
- Urinalysis (dipstick) and culture — to exclude UTI and diabetes mellitus (glycosuria). This is mandatory in every child with new or worsening enuresis.
- Blood glucose if glycosuria or polyuria/polydipsia.
- Voiding/fluid diary — to document nocturnal volume, daytime frequency and fluid intake, and to guide treatment (and demonstrate nocturnal polyuria).
- Renal and bladder ultrasound — only if there is a history of recurrent UTI, abnormal stream, day-time symptoms suggesting bladder dysfunction, or a family history of renal disease. Routine ultrasound is not required in straightforward monosymptomatic nocturnal enuresis.
- Spinal imaging (lumbar spine X-ray or MRI) — only if there are neurological signs on examination or day-time symptoms suggesting a spinal cord lesion (e.g. tethered cord).[5]
Selective mutism: hearing assessment (audiometry), speech and language evaluation, and observation of the child across settings (home, school, clinic) to confirm the discrepancy. Rule out a communication disorder (stuttering, articulation disorder, language disorder) before attributing muteness to an anxiety mechanism.[1]
Separation anxiety: clinical diagnosis; screen for comorbid depression, bullying, abuse and specific phobia. Physical examination to reassure that the somatic complaints (abdominal pain, headache) are not organic.[1]
Attachment disorders: corroborate the history of pathogenic care (social care records, foster-care history); assess for comorbid developmental trauma, fetal alcohol spectrum disorder (FASD), neglect-related growth failure and developmental delay; examine for the stigmata of abuse and neglect.[1]
Management — Resuscitation
Acute child psychiatric emergencies demand safety first and a calm, de-escalating environment.[2]
Acute behavioural disturbance: ensure the safety of the child, family and staff; reduce stimuli (quiet room, trusted adult); use verbal de-escalation (acknowledge feelings, offer choices, avoid confrontation); involve parents early; physical intervention and medication are last-resort measures to prevent serious harm, used only by trained staff with appropriate monitoring and authorisation.[4]
Self-harm or suicidal adolescent: treat as an emergency. Take all talk of self-harm seriously; do not leave the young person alone; remove means (medications, sharp objects, ligature points); conduct a structured risk assessment (intent, plan, access to means, protective factors, previous attempts); arrange urgent CAMHS assessment; consider admission to a place of safety if risk is high; make a safeguarding referral.[3]
Disclosed or suspected abuse or neglect: the immediate priority is the safety of the child. Do not attempt to investigate single-handedly — preserve any forensic evidence, do not interrogate the child, document the disclosure verbatim in the child's words, and refer immediately to the safeguarding lead and children's social care. Where there is a risk of immediate serious harm, the child may need to be removed to a place of safety. The doctor's duty is to refer and protect, not to confirm the diagnosis.[2]
Severe malnutrition or medical instability from an eating disorder: paediatric admission for refeeding (see the eating-disorders topic) — refeeding syndrome is a medical emergency.[2]
Acute psychosis or mania in an adolescent: urgent CAMHS assessment; rule out an organic cause (drug intoxication or withdrawal — especially cannabis and stimulants — encephalitis, head injury); assess risk; consider an antipsychotic under specialist supervision; admit if risk is high.[2]
Management — Definitive & Stepwise
The overarching principle, repeated because it is the single most testable point in child psychiatry: psychological and behavioural interventions are first-line; medication is reserved for when these are insufficient or for specific indications.[1][4]
Disruptive behaviour disorders (ODD / CD) — the parent is the treatment vehicle
First-line for ODD and mild-to-moderate CD — parent training programmes (NICE CG158 first recommendation). These are group-based programmes for lower-severity cases and individual programmes for more complex families. They teach consistent, calm, contingent discipline; positive reinforcement of prosocial behaviour; emotional coaching; and problem-solving, and reduce conduct problems by 20 to 40 percent.[4]
- Incredible Years — for children aged 2 to 12; group-based; builds positive parent-child interaction and reduces coercive cycles.
- Triple P (Positive Parenting Program) — flexible (universal to targeted); teaches positive parenting and behaviour management.
- Parent-Child Interaction Therapy (PCIT) — live-coached, dyadic, for ages 2 to 7; two phases (child-directed interaction building the relationship, parent-directed interaction teaching discipline).[4]
Severe CD — Multisystemic Therapy (MST): an intensive, home- and community-based intervention that addresses the family, peer, school and neighbourhood systems simultaneously, delivered by a small caseload therapist over 3 to 5 months. Functional Family Therapy (FFT) and multidimensional treatment foster care are evidence-based alternatives for adolescents with serious antisocial behaviour.[4]
Child-focused adjuncts: problem-solving skills training and CBT-based anger management for the child have modest efficacy alone but are best combined with parent work. School-based programmes (classroom management, social-skills groups) reinforce gains.[4]
Medication — last resort, specialist-only: no drug treats the core disorder of ODD or CD. Risperidone (an atypical antipsychotic), at low dose (e.g. 0.5 to 1 mg daily, titrated slowly), reduces aggression in severe CD that has not responded to psychosocial intervention — but with significant cost: weight gain, hyperprolactinaemia, sedation, metabolic effects (dyslipidaemia, hyperglycaemia) and extrapyramidal symptoms, all of which demand baseline and ongoing monitoring. Methylphenidate or other stimulants are used only when comorbid ADHD is present (treating the ADHD often improves conduct symptoms). The evidence for antipsychotic use in foster-care and looked-after children has been criticised as disproportionate and must be scrutinised.[3]
Separation anxiety disorder
- First-line: CBT with exposure — age-appropriate cognitive behavioural therapy with graded exposure to separation, combined with parent work to reduce accommodation (the parental behaviours that inadvertently maintain the anxiety, such as always being available, allowing co-sleeping, excusing school absence).
- Family involvement is essential; address parental anxiety and overprotection.
- SSRIs (e.g. sertraline or fluoxetine) are added when CBT is insufficient and symptoms are severe — fluoxetine is the SSRI with the most evidence and is the one licensed for use in children in many jurisdictions. Monitor for emergent suicidality in the first weeks (the FDA black-box warning applies to all antidepressants in those under 25).[4]
Selective mutism
- First-line: behavioural intervention — stimulus fading (gradually introducing new people into a setting where the child speaks), shaping (rewarding successive approximations to speech), positive reinforcement for speech, and removal of pressure to speak. Cognitive behavioural therapy adapted for the child's age. Family and school involvement is critical — the school must be part of the exposure plan and must not allow the child's mutism to be inadvertently reinforced (e.g. by accepting only gestures).
- Speech and language therapy to address any comorbid communication difficulty.
- SSRI (e.g. fluoxetine) in severe, treatment-resistant cases under specialist supervision.
- Early treatment is key — outcome is better the sooner intervention begins; untreated selective mutism frequently evolves into social anxiety disorder.[4]
Enuresis — the alarm is first-line, not the drug
- General measures first: reassurance (the condition is common and improves spontaneously — about 15 percent resolve per year without treatment); avoid blame and punishment (these worsen the problem); regular daytime fluid intake, limit evening fluids; toileting before bed; reward systems (e.g. star charts for dry nights — reinforce the behaviour of getting up to void, not just dryness).
- First-line specific treatment: the enuresis alarm (body-worn or bed-mat alarm that wakes the child at the first drop of urine, conditioning arousal to bladder fullness). It has a 60 to 70 percent success rate with motivated families and a lower relapse rate than desmopressin, but requires a committed family and a minimum 6 to 8 week trial. It is the treatment of choice for monosymptomatic nocturnal enuresis in a motivated child over age 7.[5]
- Pharmacological — desmopressin: a synthetic arginine-vasopressin analogue (e.g. 200 to 400 micrograms orally, or sublingual/orodispersible preparation, at bedtime) that reduces nocturnal urine volume. It works rapidly (useful for sleepovers, school trips, short-term symptom control) but has a high relapse rate on stopping and so is generally second-line to the alarm, or used where the alarm is unsuitable or has failed. Restrict evening fluids when giving desmopressin to avoid hyponatraemia.
- Imipramine (a tricyclic antidepressant) was historically used but is now rarely favoured because of cardiotoxicity in overdose and the availability of safer alternatives.
- Oxybutynin (an anticholinergic) is added when there are day-time symptoms suggesting detrusor overactivity or in non-monosymptomatic enuresis.
- Treatment of constipation (if present) often resolves enuresis — a loaded rectum mechanically irritates the bladder.
Encopresis — treat the constipation first
- The majority of encopresis is constipation with overflow: the rectum is loaded with hard stool and liquid stool leaks around it. Disimpaction first (polyethylene glycol/PEG, e.g. macrogol, in escalating doses; or lactulose), then maintenance stool softener and a behavioural toileting programme (regular scheduled toilet sits after meals, foot support, positive reinforcement for toileting and for clean pants).
- Address the dietary contributors (fibre, fluid).
- Once constipation is treated, the overflow soiling resolves.
- For the rarer encopresis without constipation, the problem is more behavioural — address the underlying behavioural/psychological factors and use behavioural toileting.[2]
Attachment disorders — repair the environment
- Stable, nurturing placement is the foundation — a consistent, emotionally available caregiver. Without removing the pathogenic care, no therapy works.
- Trauma-informed therapeutic caregiving and attachment-focused therapy (e.g. dyadic developmental psychotherapy principles), delivered by specialists.
- Address the environment (safeguarding, social care, support for the carer).
- No medication treats reactive attachment disorder or disinhibited social engagement disorder; treat comorbidities (ADHD, PTSD) on their own merits.[3]
School refusal — a multimodal plan
- Identify and address the cause (separation anxiety, bullying, depression, specific phobia, learning difficulty).
- CBT for the underlying anxiety/mood disorder.
- Gradual, planned reintegration with the school — negotiated reduced timetable, a named safe adult/quiet space, anti-bullying work.
- Family involvement to support attendance and reduce accommodation.
- Persistent refusal with severe impact warrants specialist CAMHS involvement.[3]
Specific Subtypes & Scenarios
Childhood-onset CD (before age 10)
- More often male, physically aggressive
- Higher rates of callous-unemotional traits
- Poor prognosis — about 50 percent progress to antisocial personality disorder
- Stronger genetic/neurobiological loading
- Needs intensive, early, multimodal intervention
Adolescent-onset CD
- Onset after age 10
- Less physical aggression, more rule violation and delinquency
- Better prognosis — less likely to persist into adulthood
- More influenced by peer delinquency and situational factors
- Responds well to MST and family therapy
CD with callous-unemotional traits
- DSM-5 specifier: lack of guilt/empathy, shallow affect, unconcern about performance
- Reduced amygdala reactivity to distress cues
- More severe, more treatment-resistant
- Higher genetic loading
- Treat with intensive parent training + MST; medication more often needed for aggression
ODD subtypes (DSM-5): the angry/irritable mood presentation predicts later depression and anxiety; the defiant/vindictive presentation more often progresses to CD. Recognising the irritable ODD child flags a higher mood-disorder risk and prompts closer monitoring.[3]
Enuresis subtypes drive treatment: primary enuresis (never dry) suggests a maturational cause and responds well to the alarm; secondary enuresis (relapse after being dry) prompts a search for a precipitant (stressor, UTI, abuse, diabetes). Non-monosymptomatic enuresis (day-time symptoms) requires urological assessment and often an anticholinergic alongside the alarm; monosymptomatic nocturnal enuresis is the classic indication for the alarm.[5]
Adolescent-specific scenarios: emergent borderline/emotionally unstable personality features (self-harm, instability of mood and relationships, fear of abandonment) are addressed with dialectical behaviour therapy (DBT-A) and specialist CAMHS; first-episode psychosis needs early intervention in psychosis (EIP) services; substance use disorder needs adolescent-specific addiction services; eating disorders need specialist eating-disorder CAMHS. Transition planning to adult services should begin from around age 14, with a structured handover.[2]
Complications & Pitfalls
Untreated CD: progression to antisocial personality disorder in adulthood (especially childhood-onset CD with CU traits — about 50 percent); criminality and imprisonment; substance misuse; school dropout and unemployment; relationship breakdown; intimate partner violence; and earlier mortality (accident, suicide, violence).[1]
ODD: many children remit, but about 30 percent progress to CD; the irritable subtype carries a heightened risk of later depression and anxiety.[1]
Enuresis: the main complication is low self-esteem, bullying and parental punishment — punishment is harmful, worsens the problem and must be actively discouraged. Untreated enuresis can produce secondary behavioural and emotional problems; it is highly treatable and treatment is rewarding.[2]
Untreated attachment disorder: lifelong relationship difficulties, personality disorder, substance misuse, and vulnerability to further abuse and exploitation.[1]
Adolescent self-harm: repetition is common, and completed suicide is among the leading causes of adolescent death — every episode of adolescent self-harm warrants a serious risk assessment and follow-up.[3]
Classic pitfalls:[1]
- Missing abuse or neglect — the cardinal sin. Always consider safeguarding; a behavioural presentation may be the only sign of maltreatment.
- Treating CD with medication alone — antipsychotics do not treat the core disorder; without parent training and environmental change, gains are absent or unsustainable.
- Punishing enuresis — the child is not wetting deliberately; punishment worsens shame and the problem.
- Failing to address school factors in school refusal and selective mutism — the school is half the treatment.
- Diagnosing autism in a selectively mute child — check whether the child speaks normally in safe settings.
- Not screening for and treating comorbidity — CD with untreated ADHD, or enuresis with untreated constipation, will not resolve.
- Not transitioning adolescents to adult services — losing a vulnerable young person at the CAMHS-adult boundary is a well-known failure with serious consequences.
- Over-prescribing antipsychotics, especially to looked-after children — scrutinise every prescription against the indication and the monitoring.[6]
Prognosis & Disposition
Conduct disorder: childhood-onset CD has the poorest prognosis — about half of these children develop antisocial personality disorder. Adolescent-onset CD has a substantially better prognosis and often remits in adulthood. Callous-unemotional traits worsen prognosis across both types. Good prognostic factors: higher IQ, prosocial skills, a supportive and consistent family, school engagement, two biological parents in a low-conflict home, absence of CU traits, and early, multimodal intervention.[1][3]
ODD: many children remit; about 30 percent progress to CD; the irritable subtype is at elevated risk of mood and anxiety disorders.[1]
Separation anxiety: usually resolves with treatment; untreated, it can persist into adulthood as panic disorder and agoraphobia (a recognised developmental sequence).[1]
Selective mutism: better outcome with early treatment; if untreated it can persist and evolve into social anxiety disorder.[1]
Enuresis: the spontaneous resolution rate is about 15 percent per year; the alarm produces a 60 to 70 percent cure rate. Most children become dry by adolescence regardless, but treatment spares years of distress and low self-esteem.[5]
Disposition: most children are managed in primary care with parent advice, the SDQ, and signposting; moderate cases in community CAMHS (tier 2/3); severe, complex or risky presentations in specialist multi-disciplinary CAMHS (tier 3/4) or, rarely, inpatient adolescent units. Always agree a safety plan and follow-up at every contact.[3]
Special Populations
- Looked-after and foster children: very high rates of attachment disorders, PTSD, CD, depression and substance misuse. Need specialist CAMHS, placement stability, therapeutic foster care and trauma-informed care. Antipsychotic prescribing is disproportionately high and must be scrutinised.[6]
- Adolescents and the law: Gillick competence — a child under 16 in the UK can consent to treatment if they demonstrate sufficient understanding and intelligence (the Fraser guidelines apply specifically to contraception). Confidentiality is important to the therapeutic relationship but has limits — safeguarding overrides confidentiality when a child is at risk. Plan transition to adult services from around age 14, with a structured, named-handover process.
- Neurodevelopmental comorbidity (autism, ADHD, intellectual disability): extremely common. Adapt the assessment (visual supports, sensory considerations, shorter sessions, information from school); adapt behavioural interventions (more concrete, more visual, more repetition); use medication cautiously and monitor closely; rule out a physical cause of behaviour change (pain, infection, constipation, dental problems, medication side-effect) in a child who cannot articulate distress.[2]
- Child abuse and neglect: safeguarding is paramount. Use multi-agency working (social care, education, health, police where indicated). Mandatory reporting provisions vary by jurisdiction — know your local duty. Provide trauma-informed care that prioritises safety, trust, choice, collaboration and empowerment.[6]
- Learning disability: high rates of behavioural problems, often reflecting unmet physical or communicative need. Adapt communication; always exclude a physical cause of new behaviour; behavioural approaches are first-line.
- Refugee and asylum-seeking children: high rates of trauma, PTSD, depression and anxiety; consider language and cultural factors in assessment (use trained interpreters, not family members); be alert to trafficking and exploitation; address the social determinants (housing, legal status, separation from family).[6]
Evidence, Guidelines & Regional Differences
NICE Clinical Guideline 158 (2013, updated): Antisocial behaviour and conduct disorders in children and young people — the cornerstone UK guidance. Recommends group parent training programmes first-line for ODD and CD of moderate or lesser severity (Incredible Years, Triple P, Strengthening Families), individual programmes (PCIT) for more complex cases, and Multisystemic Therapy / Functional Family Therapy for adolescents aged 11 to 17 with severe CD. Child-focused programmes (CBT, problem-solving) are adjuncts. Medication is not routinely recommended; risperidone may be considered short-term for severe aggression that has not responded to psychosocial intervention, under specialist supervision.[4]
AACAP (American Academy of Child and Adolescent Psychiatry) practice parameters guide assessment and treatment of ODD/CD and broadly concur with NICE on parent training first-line and medication last-resort.[2]
Cochrane systematic reviews confirm that parent training programmes are effective for CD/ODD, and that Multisystemic Therapy reduces adolescent antisocial behaviour and out-of-home placement. CBT is effective for childhood anxiety disorders; for moderate-to-severe cases, the combination of CBT plus an SSRI (fluoxetine) outperforms either alone, with monitoring for emergent suicidality.[2]
[4] [3] [3]Controversies:[2]
- Risperidone and other antipsychotics in CD — the balance between modest efficacy for aggression and substantial metabolic, prolactin and sedative side effects in a developing child, and the disproportionate prescribing to looked-after children.
- The antidepressant-suicidality debate — the FDA black-box warning on SSRIs in under-25s reduced prescribing but may have increased adolescent suicide through untreated depression; the consensus is that SSRIs (especially fluoxetine) are effective for moderate-to-severe adolescent depression and anxiety with monitoring, and that the risk of untreated illness exceeds the drug risk.
- The boundary between normal adolescent risk-taking and pathology — over-medicalising normative development versus missing treatable disorder.
- The transition cliff between CAMHS and adult services, at which many vulnerable young people are lost to follow-up.[2]
Exam Pearls
Conduct disorder categories — ADDS
ADDS
to people/animals — bullying, fighting, weapons, cruelty, forced sex
of property — fire-setting, vandalism
breaking in, conning, shoplifting, forgery
staying out before 13, running away, truancy before 13
ODD versus CD — the pivot
RIGHTS
CD violates the RIGHTS of others; ODD does not
CD aggression is goal-directed; ODD defiance is reactive
CD is more severe than ODD; CD may progress to ASPD
ODD often precedes CD — the developmental ladder
Both: PARENT TRAINING first-line, medication last resort
Callous-unemotional traits = CD specifier, worst prognosis
- CD is AGGRESSIVE; ODD is DEFIANT. The presence of aggression, property destruction, theft/deceit or serious rule violation makes it CD, not ODD. Childhood-onset CD (before age 10) = worse prognosis.
- Callous-unemotional traits are the DSM-5 specifier for CD (lack of empathy/guilt, shallow affect); they mark the most severe, treatment-resistant form.
- Parent training programmes (Triple P, Incredible Years, PCIT) are first-line for ODD/CD. MST for severe CD. Medication is NOT first-line.
- Antisocial personality disorder requires age at least 18 AND evidence of CD before age 15.
- Selective mutism: speaks at home, mute at school. CBT + school involvement. Not autism.
- Enuresis: age at least 5. Rule out UTI, diabetes, constipation. The ALARM is first-line (60 to 70 percent success, low relapse), not desmopressin. Desmopressin (a synthetic AVP analogue) is for short-term use; it has a high relapse on stopping. Restrict evening fluids to avoid hyponatraemia.
- Enuresis is genetic — autosomal dominant trait; 44 percent if one parent, 77 percent if both.
- Encopresis: treat CONSTIPATION first — PEG/lactulose disimpaction + maintenance + behavioural toileting; overflow soiling resolves once the rectum is empty.
- Separation anxiety: at least 4 weeks in children. CBT with exposure first-line; SSRI if severe (monitor for suicidality).
- RAD: emotionally withdrawn, does not seek comfort. DSED: overly familiar with strangers. Both follow grossly pathogenic care (neglect, institutionalisation).
- Safeguarding ALWAYS assessed. Mandatory referral if abuse suspected. The child's safety is paramount — refer and protect, do not single-handedly confirm.
- Medication is a LAST RESORT in children. Risperidone (short-term, specialist) for severe CD aggression; SSRIs (fluoxetine) for severe anxiety/depression; stimulants only if comorbid ADHD.
- SDQ (Strengths and Difficulties Questionnaire) = the brief 25-item screening tool for 4 to 17 year-olds.
- Gillick competence: an under-16 can consent to treatment if they fully understand. Safeguarding overrides confidentiality.
- Suicide is a leading cause of adolescent death — always assess risk in adolescents; take all self-harm seriously.
- Untreated separation anxiety can become adult panic/agoraphobia; untreated CD can become ASPD; untreated selective mutism can become social anxiety. Early intervention matters.
- CYP-IAPT (UK) and the four-tier CAMHS structure (tier 1 primary care to tier 4 specialist inpatient) organise UK child mental health services.[4]
Exam application bank (NEET-PG / INICET)
One-line answer
Child and adolescent psychiatry covers mental disorders from birth to age 18, with every symptom assessed in developmental context against age-appropriate norms. The high-yield disorders are: Conduct disorder (CD) — a repetitive, persistent pattern of behaviour that violates the rights of others or age-appropriate norms (aggression to people/animals, destruction of property, deceit/theft, serious rule violation; at least 3 of 15 criteria in 12 months); Oppositional defiant disorder (ODD) — angry/irritable mood, argumentative/defiant behaviour, vindictiveness without aggression or rights violation; Separation anxiety disorder — excessive, developmentally inappropriate fear of separation lasting at least 4 weeks; Selective mutism — consistent failure to speak in social situations despite speaking elsewhere; Enuresis — repeated involuntary urination, age at least 5; Encopresis — repeated fa
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard.[6]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes.[4]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change.[1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each.[1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory.[1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Child & Adolescent Psychiatry.
References
- [1]Fairchild G, Hawes DJ, Frick PJ, et al. Conduct disorder. Nature Reviews Disease Primers, 2019.PMID 31249310
- [2]Paulus FW, Bachmann CJ, Gortz-Dorten A, et al. Emotional Dysregulation in Children and Adolescents With Psychiatric Disorders. Frontiers in Psychiatry, 2021.PMID 34759846
- [3]Bachmann CJ, Lempp T, Gortz-Dorten A, et al. Recognition and management of children and adolescents with conduct disorder. Child and Adolescent Psychiatry and Mental Health, 2024.PMID 38281951
- [4]Pilling S, Turner K, Rendell A, et al. Recognition, intervention, and management of antisocial behaviour and conduct disorders in children and young people: summary of NICE guidance. BMJ, 2013.PMID 23535256
- [5]Kamperis K, Mahler B, Rittig S, et al. Nocturnal enuresis in children: The role of arginine-vasopressin. Handbook of Clinical Neurology, 2021.PMID 34238464
- [6]Samson JA, Bernier A, McMahon RJ, et al. Practitioner Review: Neurobiological consequences of childhood maltreatment - clinical and therapeutic implications. Journal of Child Psychology and Psychiatry, 2024.PMID 37609790