Psychiatry · Psychiatry
Obsessive-Compulsive Disorder (OCD)
Also known as Obsessive-compulsive disorder · OCD · Obsessions and compulsions · Compulsive disorder
Obsessive-compulsive disorder (OCD) is a chronic, disabling mental disorder characterised by obsessions (intrusive, unwanted, recurrent thoughts, images or urges that cause marked anxiety or distress) and/or compulsions (repetitive behaviours or mental acts the person feels driven to perform to neutralise the obsession or prevent a dreaded outcome), that are time-consuming (over 1 hour per day) or cause clinically significant distress and impairment. Patients have insight (recognise the obsessions as irrational) but cannot resist them — this distinguishes OCD from psychosis (no insight), delusional disorder and OCPD (ego-syntonic). Common themes: contamination/washing, doubt/checking, symmetry/ordering/counting, forbidden/taboo thoughts (sexual, religious, aggressive, somatic), hoarding. Lifetime prevalence about 2 to 3 percent; onset typically adolescence to early adulthood; average 11 to 17 years delay to diagnosis because patients hide symptoms. DSM-5-TR moved OCD out of the Anxiety Disorders into its own 'Obsessive-Compulsive and Related Disorders' category (siblings: body dysmorphic disorder, hoarding disorder, trichotillomania, excoriation disorder). Treatment: ERP (exposure and response prevention) is the gold-standard psychological therapy; SSRIs at HIGH doses (higher than depression — fluoxetine up to 60 mg, sertraline 200 mg, paroxetine 60 mg, fluvoxamine 300 mg); clomipramine when SSRI fails; antipsychotic augmentation (risperidone, aripiprazole) for refractory. Sudden-onset OCD in a child: consider PANDAS (post-strep autoimmune); check ASO titre.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Exam tags
Red flags

Overview & Definition
Obsessive-compulsive disorder (OCD) is a chronic, often disabling psychiatric disorder in which the patient experiences obsessions (intrusive, unwanted, recurrent thoughts, images, or urges that cause marked anxiety or distress) and/or compulsions (repetitive behaviours or mental acts the person feels driven to perform according to rigid rules, in response to an obsession, aimed at preventing or reducing anxiety or a dreaded event, and not connected in a realistic way to what they are designed to neutralise or prevent).[1] The World Health Organization ranked OCD among the top 10 most disabling medical conditions worldwide by years lost to disability.[10]
The clinical skill in OCD is not missing it. Patients hide their symptoms for an average of 11 to 17 years before correct diagnosis because of shame, magical thinking, and fear of being judged "mad". GPs miss it in around half of cases — the patient presents instead with depression, anxiety, alcohol misuse, or a physical complaint driven by the compulsions (e.g., dermatitis from washing).[1] The cardinal skill is to ask directly: "Do you get unpleasant thoughts that keep coming back even though you try to push them away? Do you feel you have to do things over and over — wash, check, count, repeat — even though you know it doesn't make sense?"[5]
The hallmark that defines true OCD — and that examiners repeatedly test — is that the patient recognises the obsessions as irrational but cannot resist them. This insight distinguishes OCD from delusional disorder and from obsessive-compulsive personality disorder (OCPD), in which the traits are ego-syntonic and not resisted.[1]
Classification
OCD is classified by diagnostic system (DSM-5-TR vs ICD-11) and by symptom dimension.[1][6]
DSM-5-TR change — the high-yield examinable fact: OCD has been moved out of the Anxiety Disorders (where it sat from DSM-III to DSM-IV-TR) into its own category, the "Obsessive-Compulsive and Related Disorders".[1] The rationale: OCD has a distinct neurobiology (cortico-striato-thalamo-cortical circuit dysfunction), distinct family aggregation, distinct treatment response (high-dose SSRI, ERP, antipsychotic augmentation, clomipramine), and a distinct symptom structure (obsessions and compulsions, not the diffuse worry of GAD).[5]
The Obsessive-Compulsive and Related Disorders (DSM-5-TR): [1]
- Obsessive-compulsive disorder (the prototype).
- Body dysmorphic disorder — preoccupation with a perceived flaw in appearance.
- Hoarding disorder — persistent difficulty discarding possessions regardless of value, leading to clutter and impairment. (Previously a subtype of OCD in DSM-IV; now its own disorder — patients are distressed by discarding, not by intrusive thoughts.)
- Trichotillomania (hair-pulling disorder) — recurrent pulling out of one's hair.
- Excoriation (skin-picking) disorder — recurrent skin-picking.
- Substance/medication-induced OCRD and OCRD due to another medical condition.[1]
DSM-5-TR specifiers (examiner favourite):[1]
- Insight specifier: good or fair insight (recognises OCD beliefs are definitely/probably not true); poor insight (thinks they are probably true); absent insight/delusional beliefs (completely convinced they are true). OCD with absent insight is still OCD — not a psychotic disorder — and is treated with SSRI + antipsychotic.
- Tic-related specifier (DSM-5-TR): a current or past history of a tic disorder. Tic-related OCD has more symmetry, ordering, counting, somatic and forbidden thoughts, an earlier male onset, and a better response to antipsychotic augmentation.[1]
Symptom-dimension classification (reproducible — Mataix-Cols multidimensional model):[12] Most patients have several dimensions. The five major reproducible factors:
- Contamination / washing — the commonest; obsessions about germs/dirt/illness, compulsive hand-washing, cleaning, avoiding public places, doorknobs, toilets.
- Doubt / checking — pathological doubt that something bad has been (or will be) done; checking locks, switches, stoves, that no one was harmed.
- Symmetry / ordering / counting / repeating — need for exactness, "just right" feeling, counting, repeating actions a set number of times.
- Forbidden / taboo thoughts (aggressive, sexual, religious, somatic) — intrusive harm/sexual/blasphemous thoughts; mental rituals (praying, counting, mental review). "Pure-O" presentation.
- Hoarding — difficulty discarding (now separate DSM-5 disorder when primary).[12]
OCD
- Ego-DYSTONIC — patient resists, distressed
- Episodic symptoms with compulsions
- Insight usually present (good/fair)
- Anxiety-driven rituals
- Treat: ERP + high-dose SSRI
OCPD (personality)
- Ego-SYNTONIC — patient embraces perfectionism
- Lifelong pervasive TRAITS, not episodes
- No insight sought — 'this is how I am'
- Preoccupation with order/control/rules
- Treat: psychotherapy; medication generally ineffective
GAD (generalised anxiety)
- Worries about REAL-LIFE concerns (money, family, health)
- Not intrusive/absurd — worries are realistic
- No compulsions
- Episodic worry, no rituals
- Treat: SSRI + CBT for worry
Illness anxiety (hypochondriasis)
- Preoccupation with HAVING a serious illness
- Misattribution of bodily symptoms
- Reassurance-seeking/health-checking
- Treat: CBT for health anxiety + SSRI
Phobia
- Fear of a SPECIFIC external object/situation
- Avoidance, not rituals
- Circumscribed trigger
- No ego-dystonic intrusive thoughts
- Treat: graded exposure CBT
Psychosis / delusional disorder
- No insight; bizarre or systematised delusions
- No compulsions; thought disorder
- Reality-testing lost
- Treat: antipsychotic first-line
Epidemiology & Risk Factors
OCD is common, chronic, and disabling — and substantially under-recognised.[1][10]
Prevalence (Ruscio 2010, NCS-R):[10]
- Lifetime prevalence: ~2 to 3 percent of the general population (about 1 in 40 adults).
- 12-month prevalence: ~1.2 percent.
- Subclinical obsessions/compulsions: present in ~25 to 30 percent of people — far more common than full OCD (the dimensional view of OC symptoms). [1]
OCD — the numbers examiners want
- Bimodal peaks: a childhood peak (around age 10 to 12) and an early-adult peak (late teens to early 20s). About 25 percent of cases begin before age 10, and 80 percent before age 18.
- Sex ratio overall 1:1, but males have earlier onset (often prepubertal) and more sexual, religious and symmetry themes; females have slightly later onset (often peripartum spikes) and more contamination, washing and cleaning themes. [1]
- Genetic / family: first-degree relatives of an OCD proband have a 3 to 12-fold increased risk; heritability is estimated at 40 to 50 percent in adult-onset and 45 to 65 percent in paediatric-onset (the paediatric form is the more genetic subtype).[7]
- Perinatal complications — prematurity, low birth weight, maternal smoking.
- Infection — Group A beta-haemolytic streptococcal (GAS) infection triggering PANDAS/PANS in genetically susceptible children.[13]
- Childhood trauma / adversity — emotional, sexual or physical abuse is over-represented in adult OCD.
- Other neuroinflammatory / autoimmune disorders (e.g., post-encephalitic, basal ganglia disease).
- Peripartum period — pregnancy and postpartum are established triggers for new-onset or worsening OCD (often intrusive infant-harm thoughts).[5]
Comorbidity burden — almost universal in OCD (about 90 percent lifetime):[1][10]
- Major depression in 50 to 67 percent (often secondary to OCD chronicity).
- Other anxiety disorders in up to 75 percent (social anxiety disorder, panic disorder, GAD).
- Tic disorders / Tourette syndrome in up to 30 percent of paediatric OCD (and 20 to 30 percent of adult OCD).
- Body dysmorphic disorder, eating disorders, alcohol/substance use (often self-medication).
- OCPD in 25 to 30 percent (overlap; the personality disorder coexists with OCD).
- Bipolar disorder — increased rate; this matters because antidepressant monotherapy can switch mood.
- Schizophrenia-spectrum — about 12 to 30 percent of patients with schizophrenia have prominent OC symptoms (and OCD is over-represented in schizophrenia relatives). [1]
Pathophysiology
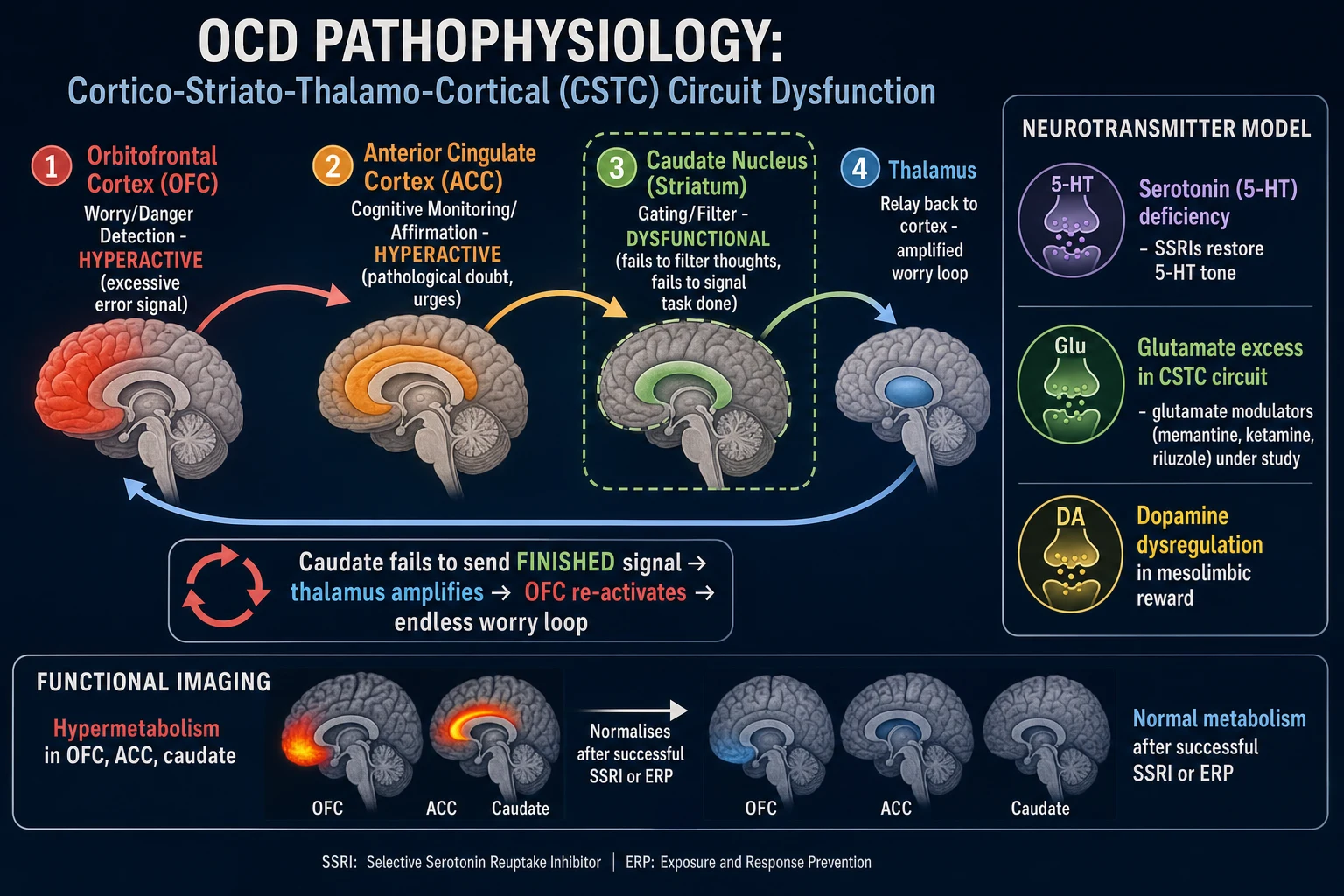
OCD is a disorder of the cortico-striato-thalamo-cortical (CSTC) circuit — the brain's error-detection, gating and habit-learning loop. The dominant model for 30 years, it integrates neuroimaging, neuropsychology, genetics, and treatment response.[1][4]
The CSTC loop — how it normally works, and how it breaks in OCD:[4]
The CSTC loop runs orbitofrontal cortex (OFC) → anterior cingulate cortex (ACC) → caudate nucleus (striatum) → globus pallidus/substantia nigra → thalamus → back to OFC. In health, the loop detects when an action or thought needs attention, signals when it is "done" or "no longer relevant", and gates (filters out) irrelevant signals. The striatum (caudate) is the gating/filtering station.[4]
In OCD the loop gets stuck: [1]
- The orbitofrontal cortex (OFC) — the brain's "worry / error signal" detector — fires excessively (hypermetabolic on PET/fMRI), generating a persistent "something is wrong / there is danger" signal that the patient experiences as an obsession.[1]
- The anterior cingulate cortex (ACC) — which monitors for cognitive conflict and "errors" — also fires excessively, generating the pathological doubt ("did I lock the door? did I harm someone?") and the affective urgency that drives the compulsion.
- The caudate nucleus fails to gate/filter the worry signal — it does not signal "task done" or "this is irrelevant" — so the worry does not extinguish.[4]
- The thalamus relays the unfiltered worry signal back to the OFC, re-activating the obsession in an endless loop.[1]
The compulsion (washing, checking, mental prayer) is a behavioural attempt to neutralise the obsession — and it provides temporary relief by activating the dopaminergic reward pathway. But the relief is short-lived and reinforces the loop (negative reinforcement), driving the next compulsion.[1]
Functional neuroimaging — the convergent biomarker:[1][4]
PET and fMRI consistently show hypermetabolism / hyperperfusion of the OFC, ACC and head of the caudate nucleus in symptomatic OCD patients. Crucially, successful treatment — whether by SSRI, clomipramine, ERP or neurosurgery — produces a measurable normalisation of OFC/caudate activity. This is the strongest neurobiological evidence for the CSTC model and is examiner-rewarded.[4]
Neurotransmitter model (high-yield — explains the drug ladder):[1][4]
- Serotonin (5-HT) dysregulation — the basis of SSRI efficacy. Why OCD requires higher SSRI doses and longer trials (8 to 12 weeks vs 4 to 6 weeks for depression): high-dose SSRI downregulates postsynaptic 5-HT receptors and remodels CSTC activity over weeks — a delayed structural/functional effect, not an acute serotonin boost.[1]
- Glutamate excess in the CSTC circuit — the basis of the glutamate-modulating investigational agents (memantine, riluzole, ketamine, N-acetylcysteine) used off-label or in research for refractory OCD.[4]
- Dopamine dysregulation in the mesolimbic reward pathway (which drives the "reward" of the compulsion) and in the basal ganglia (especially in tic-related OCD) — the basis for antipsychotic (D2 antagonist) augmentation of SSRIs.[3]
Neuropsychological deficits (examiner favourite — what the patient cannot do):[1]
- Cognitive inflexibility / set-shifting deficit — difficulty switching strategy when rules change (Wisconsin Card Sort Test, trail-making).
- Impaired response inhibition — difficulty suppressing a pre-potent response (Stroop, Go/No-Go).
- Abnormal error processing — over-signalling of "error" (the OFC/ACC over-fire at perceived errors); patients are hypersensitive to feeling "not quite right".
- Doubt intolerance / inflated responsibility — the patient feels responsible for catastrophic outcomes they did not cause. [1]
Genetics — high heritability, polygenic:[7][8]
- Twin studies: heritability 40 to 50 percent in adult OCD, 45 to 65 percent in paediatric-onset OCD.[7]
- Candidate gene studies long focused on SLC1A1 (EAAC1) — a glutamate transporter expressed in the CSTC circuit.[4]
- IOCDF-GC and OCGAS meta-analysis (2018, Mol Psychiatry) revealed the polygenic architecture of OCD.[7]
- Strom et al. (2025, Nature Genetics) genome-wide meta-analysis identified 30 genome-wide significant loci associated with OCD — the largest genetic study to date, implicating glutamatergic and serotonergic pathways and early neurodevelopment.[8]
PANDAS pathophysiology (high-yield paediatric scenario):[13]
Paediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infections (PANDAS) is an autoimmune hypothesis: Group A beta-haemolytic streptococcal (GAS) pharyngitis triggers the production of anti-streptococcal antibodies (ASO, anti-DNase B) that cross-react with basal ganglia (caudate) antigens, producing abrupt-onset OCD, tics, choreiform movements, emotional lability, separation anxiety, and urinary symptoms — within weeks of a GAS infection. The mechanism is analogous to Sydenham chorea in rheumatic fever. ASO and anti-DNase B titres are elevated; MRI may show caudate enlargement. Treatment involves antibiotic eradication of strep (penicillin V, azithromycin), SSRI for OCD, ERP, and (controversial) IVIG or plasmapheresis for severe cases. The concept remains debated; many clinicians prefer the broader PANS (Paediatric Acute-onset Neuropsychiatric Syndrome) label that does not require strep.[13]
OCD pathophysiology — the CSTC loop
LOOP
Cortico-Striato-Thalamo-Cortical (CSTC) circuit stuck in a repetitive cycle
Orbitofrontal cortex (worry/error) + Anterior cingulate (doubt) both over-fire
Striatum cannot signal 'task done' — worry not extinguished
ERP breaks the loop by preventing the compulsion; SSRI raises 5-HT tone; functional imaging normalises
Clinical Presentation
The clinical picture of OCD is obsessions and compulsions that consume time, cause distress, and impair function — but the content varies enormously across the five symptom dimensions, and patients often hide their symptoms for years.[1][5]
Reproduce DSM-5-TR criteria verbatim (examiner favourite):[1]
Criterion A — presence of obsessions, compulsions, or both: [1]
- Obsessions are defined by (1) recurrent and persistent thoughts, urges, or images that are experienced, at some time during the disturbance, as intrusive and unwanted, and that in most individuals cause marked anxiety or distress; and (2) the individual attempts to ignore or suppress such thoughts, urges, or images, or to neutralise them with some other thought or action (i.e., by performing a compulsion).
- Compulsions are defined by (1) repetitive behaviours (e.g., hand-washing, ordering, checking) or mental acts (e.g., praying, counting, repeating words silently) that the individual feels driven to perform in response to an obsession or according to rules that must be applied rigidly; and (2) the behaviours or mental acts are aimed at preventing or reducing anxiety or distress, or preventing some dreaded event or situation; however, these behaviours or mental acts are not connected in a realistic way with what they are designed to neutralise or prevent, or are clearly excessive. [1]
Criterion B — the obsessions or compulsions are time-consuming (e.g., take more than 1 hour per day) or cause clinically significant distress or impairment in social, occupational, or other important areas. [1]
Criterion C — not attributable to the physiological effects of a substance or another medical condition. [1]
Criterion D — not better explained by another mental disorder. [1]
The five symptom dimensions (reproduce with examples):[12]
| Dimension | Typical obsession | Typical compulsion |
|---|---|---|
| Contamination / washing | "The doorknob is covered in germs; I will get AIDS / cancer / food poisoning" | Repeated hand-washing (often with bleach), showering for hours, avoiding public toilets, household cleaning rituals |
| Doubt / checking | "Did I lock the door? Did I run someone over? Did I leave the stove on? Did I harm a child?" | Returning to check locks, switches, the road, the stove; door-to-door asking if anyone was hurt; reviewing CCTV |
| Symmetry / ordering / counting / repeating | "It doesn't feel right"; need for exactness; counting to a 'safe' number | Arranging objects symmetrically; repeating actions a fixed number of times; counting steps, breaths, words |
| Forbidden / taboo thoughts (aggressive, sexual, religious, somatic) | "I might stab my baby"; "I am a paedophile"; "I had a blasphemous thought, God will punish me"; "I have cancer" | Mental rituals — counter-thoughts, silent prayer, mental review of the day, mental checking of arousal; reassurance-seeking |
| Hoarding (now DSM-5 separate when primary) | "I might need this one day; throwing it away feels wrong" | Difficulty discarding; accumulating; clutter |
Hallmarks that examiners reward:[1][5]
- Insight is present — the patient recognises the obsessions as irrational but cannot resist. This is the cardinal feature that distinguishes OCD from psychosis.
- Magical thinking — the patient believes that thinking the thought can make the event happen ("If I think about my mother dying, it will happen, unless I count to seven").
- Avoidance — patients avoid triggers (public toilets, knives, religious images, news of disasters, the baby's bath).
- Reassurance-seeking — repeatedly asking family "Is everything OK? Did I harm anyone?".
- Family accommodation — family members become drawn into the rituals (washing for the patient, providing reassurance, following rules); this reinforces OCD and is a target of family-based ERP.[5]
- Hidden symptoms — patients hide their rituals for years due to shame; the average delay to diagnosis is 11 to 17 years.[1]
Atypical / masked presentations (examiner favourite):[1][2]
- "Pure-O" OCD — primarily obsessions and mental compulsions (counting, praying, mental review, mental checking). No visible behaviour. Patients are often missed because there is "nothing to see". Common themes: aggressive, sexual, religious. Mental rituals are still compulsions and must be targeted in ERP.
- Paediatric OCD — children may not articulate insight; rituals may be framed as "rules"; family involvement is essential; check for PANDAS/PANS in sudden-onset cases.[2][13]
- Peripartum OCD — onset in pregnancy or postpartum. Classic content: intrusive infant-harm thoughts ("I might drown the baby in the bath"); mother may avoid the infant, change nappies with gloves, refuse to bathe the baby. This is not postpartum psychosis (no delusions, hallucinations or thought disorder) and is not child abuse — but safeguarding assessment is essential.[5]
- Tourette-related / tic-related OCD — earlier male onset; more somatic, symmetry, counting, "just right" themes; compulsions may blend with tics; better response to antipsychotic augmentation.[1]
- Late-onset elderly OCD — rule out organic cause (basal ganglia stroke, post-encephalitic, CO poisoning, basal ganglia tumour, normal pressure hydrocephalus) with MRI; pharmacotherapy as usual but at lower doses.
- OCD with absent insight (DSM-5 specifier) — the patient is delusionally convinced of the obsession (e.g., "I know my hands are contaminated with HIV"). This is still OCD — not psychosis — and responds to SSRI + antipsychotic.[1]
Differential Diagnosis
A patient with intrusive thoughts or repetitive behaviour is not necessarily OCD. The differential is broad and examiners test it specifically.[1][5]
The single most-tested differential: OCPD vs OCD:[1]
| Feature | OCD (ego-dystonic) | OCPD (ego-syntonic) |
|---|---|---|
| Insight | Recognises thoughts/behaviour as irrational, wants to stop | Believes the traits are correct ("this is how I am") |
| Symptoms | Episodes of obsessions and compulsions | Lifelong pervasive traits (perfectionism, control, order) |
| Distress | Distressed by the symptoms | Distressed only when routines are disrupted |
| Anxiety | Anxiety-driven rituals | Not anxiety-driven |
| Treatment | ERP + SSRI effective | Psychotherapy; medication generally ineffective |
Psychiatric differentials:[1][5]
- Generalised anxiety disorder (GAD) — worries are about real-life concerns (money, family, health), not intrusive/absurd; no compulsions; worries are not resisted.
- Major depression with ruminations — ruminations are mood-congruent (pessimistic thoughts about worthlessness, death), not resisted; no compulsions; episodic course.
- Illness anxiety disorder (formerly hypochondriasis) — preoccupation with having a serious disease; reassurance-seeking/health-checking; specific content.
- Specific phobia / social anxiety — fear of a specific external trigger; avoidance, not rituals; circumscribed trigger.
- Body dysmorphic disorder — preoccupation with a perceived flaw in appearance (DSM-5 OCRD sibling).
- Hoarding disorder — difficulty discarding, distress at discarding; clutter (DSM-5 OCRD sibling).
- Trichotillomania / excoriation disorder — body-focused repetitive behaviours; not preceded by intrusive thoughts.
- Tic disorders / Tourette syndrome — tics are involuntary, sudden, stereotyped; compulsions are anxiety-driven, can be delayed, often have a "just right" feeling; differentiate because tics respond to dopamine antagonists.
- Autism spectrum disorder — restricted/repetitive interests are ego-syntonic and pleasurable, not anxiety-driven; social-communication deficits.
- Anorexia nervosa — obsessions about weight/shape; ego-syntonic; specific content.
- Psychotic disorders / delusional disorder — delusions are bizarre or systematised, no insight, thought disorder; reality-testing lost; OCD with absent insight is non-bizarre, themed, anxiety-driven.
- OCD due to another medical condition — basal ganglia stroke, post-encephalitic (e.g., herpes encephalitis), CO poisoning, traumatic brain injury, basal ganglia tumour, Sydenham chorea, Huntington disease. [1]
Substance-induced / medical differentials:[1]
- Stimulant intoxication (cocaine, amphetamines, caffeine) — stereotypy and compulsive behaviour; resolves with abstinence.
- Carbon monoxide poisoning — basal ganglia injury → OCD-like symptoms.
- Post-streptococcal — Sydenham chorea, PANDAS.[13]
Clinical & Bedside Assessment
OCD is diagnosed clinically by careful history and mental state examination, supported by severity rating scales. There is no blood test or scan.[1][5]
History — ask directly and non-judgementally (patients hide symptoms): [1]
- Screening questions: "Do you have unpleasant thoughts or images that keep coming back even though you try to push them away? Do you have to do things over and over — wash, check, count, repeat — even though you know it doesn't make sense? Do these things take more than an hour of your day, or get in the way of your life?"[1]
- Detail each symptom dimension — content of obsessions (contamination, harm, sexual, religious, symmetry, somatic), content of compulsions (washing, checking, ordering, counting, mental acts), time spent per day, distress, avoidance.
- Insight — does the patient recognise the thoughts as irrational? (drives the DSM-5 specifier and treatment plan).
- Functional impairment — work, school, relationships, self-care; inability to leave the house; family accommodation.
- Comorbidity screen — depression (PHQ-9), anxiety (GAD-7), bipolar (MDQ — important before SSRI), tics/Tourette, autism, alcohol/substance (AUDIT-C), eating disorder, body dysmorphic, suicide risk.
- Risk — suicidal ideation (lifetime up to 36 percent; assess with specific questions), self-harm from compulsions (dermatitis, excoriation, scalding), neglect, impact on children/dependents.[5]
- Family history — OCD, tics/Tourette, anxiety disorders (3 to 12-fold increased risk).
- Onset and course — age of onset, precipitants (pregnancy, infection, trauma), waxing-waning pattern.
- Paediatric history — sudden onset with tics/choreiform movements/urinary symptoms → ask about recent sore throat, fever → screen for PANDAS (ASO titre, anti-DNase B, throat swab).[2][13]
Standardised severity scales (reproduce the names examiners want):[5][9]
| Scale | Items | Range | Use |
|---|---|---|---|
| Y-BOCS (Yale-Brown Obsessive-Compulsive Scale) | 10 items (5 obsessions, 5 compulsions), each 0-4 | 0-40 | Gold-standard severity scale; the scale examiners reward |
| Y-BOCS Symptom Checklist | Categorical checklist of obsessions and compulsions | — | Identify content domains |
| DY-BOCS (Dimensional Y-BOCS) | Symptom dimensions + severity | — | Dimensional assessment |
| OCI-R (Obsessive-Compulsive Inventory-Revised) | 18 items | 0-72 | Self-report; brief |
| OCI-CV | Children's version | — | Paediatric self-report |
| CY-BOCS | Children's Y-BOCS | 0-40 | Paediatric clinician-administered |
Reproduce Y-BOCS severity bands verbatim (examiner favourite):[9]
- 0 to 7 — subclinical / no OCD symptoms
- 8 to 15 — mild OCD
- 16 to 23 — moderate OCD
- 24 to 31 — severe OCD
- 32 to 40 — extreme OCD [1]
Reproduce Y-BOCS treatment response definitions (Mataix-Cols 2022, examiner favourite):[9]
- Treatment response — 30 to 35 percent reduction in total Y-BOCS score.
- Remission — total Y-BOCS 12 or less (full remission); total Y-BOCS 8 or less (excellent remission).
- Treatment resistance — failure of two or more adequate SSRI trials (12 weeks each at maximum tolerated dose) plus an adequate trial of ERP (at least 13 hours). [1]
Mental state examination — what to look for: [1]
- Appearance and behaviour — visible compulsions (hand-washing, checking, arranging), excoriation, dermatitis, exhaustion.
- Speech — usually normal; slowed by mental rituals.
- Mood and affect — anxious, distressed, depressed.
- Thought — obsessions revealed (with permission and trust); magical thinking; exclude thought disorder, delusions, hallucinations.
- Insight — usually good/fair; assess specifier.
- Risk — suicidal ideation, intent, plan. [1]
Investigations
OCD is a clinical diagnosis — there is no blood test, genetic test, or brain scan required to diagnose it.[1][5]
Baseline investigations BEFORE starting an SSRI:[5]
- Weight (baseline for monitoring; SSRIs can cause weight change).
- Blood pressure, heart rate.
- ECG if cardiac history, family history of sudden death under 40, or before citalopram/escitalopram in those with QTc risk factors (these SSRIs dose-dependently prolong QTc; citalopram max 20 mg in over 65s).
- LFTs, U&E — baseline; SSRIs can cause SIADH (especially in elderly); LFTs before clomipramine.
- Pregnancy test in women of childbearing potential — paroxetine and clomipramine are best avoided in pregnancy (paroxetine: cardiac defects; clomipramine: neonatal withdrawal).
- Screening for comorbidities — PHQ-9 (depression), GAD-7 (anxiety), AUDIT-C (alcohol), MDQ (bipolar screen — important to exclude before SSRI to avoid mood switch). [1]
In paediatric sudden-onset OCD — screen for PANDAS/PANS:[2][13]
- ASO titre and anti-DNase B (anti-streptococcal antibodies).
- Throat swab for GAS.
- Consider Cunningham panel (anti-neuronal antibodies; commercially available but controversial).
- MRI brain (rule out basal ganglia lesion) if focal neurology or cognitive decline. [1]
Neuroimaging — MRI brain — only when indicated, not routine:[1]
- Late-onset OCD (over 35 years new-onset).
- Focal neurological signs or cognitive decline.
- Post-encephalitic picture, CO poisoning, head trauma.
- Suspicion of basal ganglia lesion. [1]
Reproduce DSM-5-TR criteria verbatim — the diagnostic gold standard:[1]
See the Clinical Presentation section above for the full Criteria A-D. [1]
What MUST be excluded before diagnosing OCD?[1][5]
- Active substance use disorder (especially stimulants).
- Untreated bipolar disorder — antidepressant monotherapy can precipitate mania (always screen with MDQ; stabilise mood first).
- Psychotic disorder — thought disorder, bizarre delusions, hallucinations (the OCD-with-absent-insight specifier is non-bizarre and themed; if bizarre/systematised, treat as psychosis).
- OCPD — ego-syntonic traits, no distress, lifelong.
- Another medical condition producing OCD-like symptoms (basal ganglia disease, post-encephalitic, CO poisoning). [1]
Management — Resuscitation / Immediate Concerns
OCD has no acute-resuscitation phase in the sense of a cardiac or septic emergency, but safety-critical scenarios require immediate action.[5]
Immediate safety-critical scenarios:[5]
- Suicidal ideation or attempt — lifetime suicidal ideation in OCD is up to 36 percent, with completed suicide risk about double the general population. Risk is highest with comorbid major depression, impulsivity, or substance use. Assess risk directly: ideation, intent, plan, access to means, protective factors. Crisis team involvement; admission if high risk.
- Severe self-injury from compulsions — dermatological damage from over-washing (irritant/chemical dermatitis, skin breakdown, scalds, ocular damage from blepharitis); medical/surgical assessment; infection control; modify compulsion (e.g., substitute wet wipes for bleach) as part of ERP.
- Neglect of children or dependent adults — a parent so absorbed in rituals that children are neglected, or who involves children in rituals. Safeguarding referral mandatory; ERP must include family accommodation work.
- Acute deterioration / rapid-onset in a child — rule out PANDAS/PANS (ASO titre, throat swab); paediatric urgent referral; antibiotic treatment of strep.[13]
- Serotonin syndrome — if combined serotonergic agents (SSRI + clomipramine + tramadol + MAOI, etc.): clonus, hyperreflexia, autonomic instability, hyperthermia. Stop serotonergics; supportive care; cyproheptadine, benzodiazepines; cooling.
- Catatonia (rare, in severe OCD) — lorazepam challenge; ECT if refractory.
Management — Definitive & Stepwise
Treatment is severity-stratified, multimodal, and long-term. The framework below follows NICE CG31 (UK) and international consensus (Fineberg 2020 ICNP position statement).[1][5]
The two pillars of OCD treatment:[1][5]
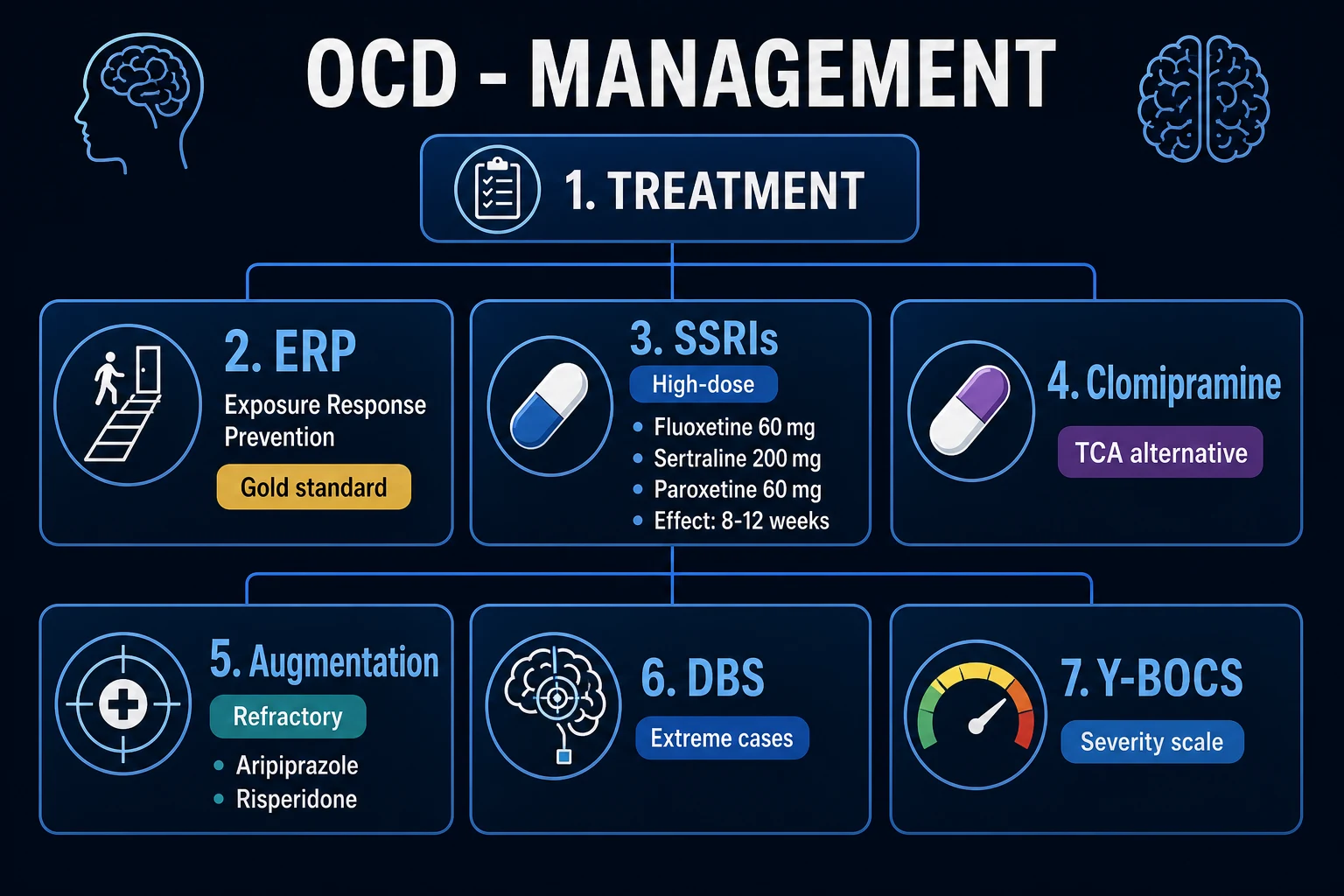
- Exposure and Response Prevention (ERP) — the gold-standard psychological therapy.
- Pharmacotherapy — SSRIs at HIGH doses (higher than depression); clomipramine as an effective alternative. [1]
Step 1 — Mild OCD: ERP (or low-intensity guided self-help based on ERP).[5]
ERP is first-line for mild OCD and as the core component for moderate-severe. Technique: the patient is systematically exposed to the obsession-trigger (e.g., touching a doorknob for contamination OCD; watching a horror scene for harm-avoidance OCD) while the therapist prevents the compulsion (no handwashing; no mental counter-thought). Anxiety initially rises, then habitualises (extinction learning). Repeated exposures across 13 to 20 sessions reduce the obsession's power. Effect size is large (around 1.5); 60 to 80 percent of patients improve. ERP is at least as effective as medication, and the Foa 2005 RCT showed ERP alone was more effective than clomipramine alone, with combination not superior to ERP alone.[11]
Cognitive therapy is added for taboo/harm/sexual/religious obsessions where there is no clear behavioural compulsion to prevent — it targets inflated responsibility, magical thinking, thought-action fusion (the belief that thinking the thought makes the event happen) and intolerance of uncertainty.[1]
Step 2 — Moderate to severe OCD: ERP + an SSRI at HIGH dose (combined).[5]
SSRIs are first-line pharmacotherapy. Crucially, OCD requires higher SSRI doses than depression, and the onset of effect is slower (8 to 12 weeks vs 4 to 6 weeks for depression) — because high-dose SSRI produces a delayed 5-HT receptor downregulation and CSTC circuit remodelling, not an acute serotonin boost.[1][5]
SSRI dose ladder (reproduce — doses are HIGHER than for depression):[1][5]
| Drug | Starting dose | Titration | Typical effective | Max |
|---|---|---|---|---|
| Fluoxetine | 20 mg OD | increase by 20 mg every 2-4 weeks | 40-60 mg OD | 80 mg OD |
| Sertraline | 50 mg OD | increase by 50 mg every 1-2 weeks | 150-200 mg OD | 200 mg OD |
| Paroxetine | 20 mg OD | increase by 10-20 mg every 2-4 weeks | 40-60 mg OD | 60 mg OD |
| Fluvoxamine | 50-100 mg OD | increase by 50 mg every 4-7 days | 200-300 mg OD | 300 mg OD |
| Citalopram | 20 mg OD | titrate over weeks | 20-40 mg OD | 40 mg OD (20 mg in over 65s) — QTc |
| Escitalopram | 10 mg OD | titrate over weeks | 10-20 mg OD | 20 mg OD — QTc |
Step 3 — Failed first SSRI (inadequate response after 12 weeks at max tolerated dose): switch SSRI or use clomipramine.[5]
- A second SSRI trial (different agent) succeeds in some patients.
- Clomipramine (a TCA, mostly serotonergic) is an effective alternative when an SSRI fails. Dose: start 25 mg OD, titrate to 100-250 mg OD (max 250 mg). It requires ECG (QTc) and LFT monitoring; anticholinergic, antihistaminergic and alpha-blocking side effects are common (dry mouth, constipation, sedation, orthostatic hypotension, urinary retention); overdose is lethal (QTc, sodium-channel blockade, seizures). Clomipramine is particularly useful when comorbid depression is present.[1]
Step 4 — Treatment-refractory OCD (failed ≥2 SSRI trials + ERP + clomipramine): antipsychotic augmentation.[3][5]
Antipsychotics are used as AUGMENTATION to an ongoing SSRI/clomipramine — NOT as monotherapy. The Bloch 2006 systematic review (Mol Psychiatry) showed that haloperidol and risperidone have the best evidence; aripiprazole is also widely used. The effect is small but real, especially in tic-related OCD.[3]
| Augmenting agent | Starting dose | Effective dose | Notes |
|---|---|---|---|
| Risperidone | 0.5 mg OD | 0.5-3 mg/day | Most evidence; useful in tic-related OCD |
| Haloperidol | 0.5-1 mg OD | 1-5 mg/day | Best evidence (Bloch 2006) |
| Aripiprazole | 2.5-5 mg OD | 5-15 mg/day | Widely used; partial D2 agonist |
| Quetiapine, olanzapine | 25-50 mg, 2.5-5 mg | titrate | Less evidence; metabolic monitoring |
Step 5 — Highly refractory OCD: investigational / neurostimulation.[4][5]
- Glutamate modulators (off-label/investigational): memantine (NMDA antagonist), riluzole (glutamate modulator), ketamine (NMDA antagonist, single-dose studies), N-acetylcysteine (glutamate/cysteine modulator).[4]
- Intravenous clomipramine — bypasses first-pass metabolism; specialist use.
- Intensive ERP programme — residential/day programme (e.g., 5-day intensive ERP).
- Deep Brain Stimulation (DBS) — bilateral stimulation of the nucleus accumbens / ventral capsule / subthalamic nucleus / anterior limb of internal capsule for extreme treatment-refractory OCD; requires specialist multidisciplinary assessment and ethical/regulatory approval.[5]
- Neurosurgery — anterior capsulotomy or anterior cingulotomy — last-resort ablative procedures for the most severe refractory cases; rarely performed.[5]
Phases of treatment:[5]
- Acute phase — 12 weeks to establish response (ERP + SSRI titrated to max tolerated).
- Continuation phase — 6 to 12 months at effective dose (relapse prevention).
- Maintenance phase — 1 to 2 years minimum; many patients require lifelong treatment. Relapse is common on discontinuation — particularly in the first 6 months off SSRI. [1]
Psychoeducation and family involvement:[5]
- Educate patient and family about the CSTC model — OCD is a neurobiological disorder, not a weakness or character flaw.
- Address family accommodation — family must be coached to stop providing reassurance and stop participating in rituals (this is the most powerful reinforcer of OCD).
- Support groups: OCD Action (UK), International OCD Foundation (IOCDF), OCD-UK, Indian OCD forums. [1]
OCD themes — the five dimensions
SCUFF
Need for exactness; counting; repeating; 'just right' feeling
Germ obsessions; hand-washing; cleaning; avoiding toilets/doorknobs
Aggressive, sexual, religious, somatic obsessions; mental rituals
Religious blasphemy, paedophile fears, harm thoughts toward loved ones
Family accommodation — drawn into rituals — must be coached to stop (ERP family component)
Specific Subtypes & Scenarios
Symptom dimension subtypes (each handled distinctly):[12]
- Contamination/washing — classic ERP (touch trigger, prevent washing); SSRI for severity; address avoidance.
- Doubt/checking — ERP (check once, leave); cognitive therapy for pathological doubt.
- Symmetry/ordering/counting/repeating — ERP (do task once, leave 'asymmetric'); harder to treat; often tic-related.
- Forbidden/taboo thoughts (Pure-O) — cognitive therapy first-line (there is no behavioural compulsion to prevent — the compulsions are mental); ERP targets the mental rituals (e.g., prevent the silent prayer after the intrusive thought). High shame; reassure the patient that intrusive harm/sexual thoughts do not indicate desire and are common in the general population.
- Hoarding (now DSM-5 separate when primary) — hoarding-specific CBT (motivational interviewing, categorisation training, discarding practice); SSRIs less effective than in OCD; harm reduction approach to clutter. [1]
Tic-related OCD (DSM-5-TR specifier):[1]
- Earlier male onset; more somatic, symmetry, "just right", counting themes.
- Better response to antipsychotic (D2 antagonist) augmentation — risperidone, aripiprazole.
- Differentiate tics (involuntary, sudden, stereotyped, no preceding anxiety) from compulsions (anxiety-driven, can be delayed, "just right" feeling). [1]
- PANDAS criteria (reproduce): (1) presence of OCD and/or tic disorder; (2) prepubertal onset; (3) episodic course characterised by abrupt onset and dramatic symptom exacerbations; (4) temporal relationship to GAS infection; (5) neurologic abnormalities (choreiform movements, hyperactivity).[13]
- PANS (Paediatric Acute-onset Neuropsychiatric Syndrome) — broader; abrupt onset OCD/eating disorder + neuropsychiatric symptoms; does not require strep.
- Workup: ASO titre, anti-DNase B, throat swab; consider Cunningham panel.
- Treatment: antibiotic eradication of strep (penicillin V, azithromycin if penicillin-allergic); SSRI (lower starting dose, slow titration); ERP; tonsillectomy if recurrent; IVIG or plasmapheresis for severe cases (controversial evidence).[13]
Peripartum OCD:[5]
- Onset in pregnancy or postpartum; classic content: intrusive infant-harm thoughts.
- Mother may avoid the infant, change nappies with gloves, refuse to bathe the baby.
- Distinguish from postpartum psychosis (no delusions, hallucinations or thought disorder in OCD; mother has insight and is distressed by the thoughts).
- ERP first-line; sertraline preferred SSRI (lowest breast-milk transfer); avoid paroxetine (cardiac defects) and clomipramine.
- Safeguarding assessment — but intrusive harm thoughts are common, ego-dystonic, and rarely acted upon; involve perinatal mental health team. [1]
Treatment-resistant OCD (failed ≥2 SSRI + ERP + clomipramine):[5]
- Augmentation with antipsychotic (risperidone, aripiprazole, haloperidol).[3]
- Glutamate modulators (memantine, ketamine, riluzole, NAC).[4]
- Intensive ERP (residential/day programme).
- DBS (nucleus accumbens / ventral capsule / STN) for the most refractory.
- Anterior capsulotomy (rarely performed ablative surgery).
OCD with comorbidities (each handled distinctly):[1]
- OCD + depression — treat both; SSRI effective for both; ERP can be harder when severe depression impairs engagement.
- OCD + bipolar disorder — avoid antidepressant monotherapy (precipitates mania); stabilise mood with mood stabiliser/atypical antipsychotic first, add SSRI cautiously.
- OCD + schizophrenia — antipsychotic + SSRI; some antipsychotics (clozapine) can worsen OC symptoms.
- OCD + tic/Tourette — add antipsychotic (risperidone, aripiprazole) earlier.
- OCD + autism spectrum — adapt ERP; lower doses; behavioural emphasis. [1]
Complications & Pitfalls
- Functional impairment — occupational (unemployment, sick leave), academic (school drop-out), marital (divorce rates elevated), social isolation. Severe contamination OCD can leave patients housebound.
- Suicide — lifetime suicidal ideation 25 to 36 percent; completed suicide risk about double the general population; risk highest with comorbid depression, impulsivity, and substance use.
- Medical complications of compulsions — irritant/chemical dermatitis, skin breakdown, scalds from hot water, ocular damage from blepharitis, repetitive strain injury, infections from over-washing.
- Family/carer burden — family accommodation consumes hours; children of affected parents are at risk of neglect.
- Comorbidity burden — depression (50-67 percent), other anxiety disorders (up to 75 percent), tics, alcohol/substance use (self-medication), bipolar switching on SSRI. [1]
Treatment complications:[1][5]
- SSRI adverse effects — GI upset (nausea, diarrhoea), sexual dysfunction (anorgasmia, decreased libido — common and under-reported), headache, insomnia or sedation, sweating, hyponatraemia (SIADH — especially in elderly), QTc prolongation (citalopram, escitalopram — dose-dependent), serotonin syndrome (with combined serotonergic agents — clonus, hyperreflexia, autonomic instability, hyperthermia).
- Clomipramine — anticholinergic (dry mouth, constipation, urinary retention, blurred vision), sedation, orthostatic hypotension, weight gain, QTc prolongation, lethal in overdose (sodium-channel blockade → arrhythmia, seizures).
- Antipsychotic augmentation — metabolic syndrome (weight gain, dyslipidaemia, hyperglycaemia), hyperprolactinaemia, extrapyramidal symptoms, sedation.
- ERP dropout — 25 to 30 percent; ERP is emotionally demanding. [1]
Classic diagnostic and treatment pitfalls (the high-yield errors examiners test):[1][5]
- Not asking directly about obsessions/compulsions — patients hide symptoms; the average delay to diagnosis is 11 to 17 years. Always screen for OCD in any patient presenting with depression, anxiety, alcohol misuse, or unexplained dermatitis.
- Using depression-dose SSRIs for OCD — the commonest treatment error. OCD requires higher doses (fluoxetine 60 mg, sertraline 200 mg, paroxetine 60 mg, fluvoxamine 300 mg).[1]
- Stopping the SSRI too early — effect takes 8 to 12 weeks in OCD; many patients are labelled "treatment-resistant" after only 4 to 6 weeks.
- Inadequate ERP — under-dosed (a few sessions rather than the recommended 13 to 20 hours); not preventing the compulsion; not addressing mental rituals.
- Missing comorbid bipolar disorder — SSRI monotherapy precipitates mania. Always screen with MDQ before SSRI.
- Missing comorbid depression — untreated depression impairs engagement with ERP.
- Not addressing family accommodation — the family continues to provide reassurance and participate in rituals, reinforcing OCD.
- Confusing OCD with OCPD — OCPD is ego-syntonic, lifelong, trait-level; medication generally ineffective; psychotherapy is the treatment.
- Confusing OCD with psychosis — OCD with absent insight is still OCD; treat with SSRI + antipsychotic, not antipsychotic alone.
- Missing PANDAS in a child — abrupt-onset OCD + tics + urinary symptoms post-strep; check ASO titre.[13]
- Using antipsychotic monotherapy for OCD — antipsychotics are augmentation, not monotherapy (unless comorbid psychosis/tics).
Prognosis & Disposition
OCD is chronic and waxing-waning in most patients, but treatment substantially improves function.[1][10]
Course and outcomes:[1]
- Complete remission: ~20 percent.
- Partial remission: ~28 percent.
- Persistent symptoms despite treatment: ~50 percent.
- Most patients improve substantially with treatment; few are entirely symptom-free. [1]
Predictors of good prognosis:[1][2]
- Younger onset (paediatric OCD often improves substantially).
- Good insight.
- Shorter duration of untreated illness.
- Contamination/washing subtype (responds well to ERP).
- Mood reactivity, absence of comorbid tics or personality disorder.
- Good treatment adherence; completed ERP.
- No family accommodation. [1]
Predictors of poor prognosis:[1]
- Male sex, earlier onset with tics (tic-related OCD).
- Comorbid OCPD, hoarding subtype (the hardest to treat).
- Comorbid major depression, bipolar disorder, schizophrenia.
- Absent insight.
- Long delay to treatment.
- Family accommodation continues.
- Treatment resistance. [1]
- ERP produces 60 to 80 percent improvement.
- SSRI produces 40 to 60 percent response.
- Combined ERP + SSRI is best for moderate-severe.
- Antipsychotic augmentation adds a smaller but real benefit in refractory cases.[3]
Disposition:[5]
- Outpatient management for most patients — primary care for stable maintenance; specialist (psychiatrist + CBT therapist) for active treatment.
- Intensive day programme / residential for severe or refractory.
- Inpatient for suicide risk, severe self-neglect, catatonia, or for initiation of clomipramine with cardiac monitoring.
- Urgent specialist referral if over 1 hour/day of compulsions, significant impairment, treatment-resistant, or paediatric with PANDAS features. [1]
Long-term follow-up:[5]
- Mild OCD on ERP — review at end of ERP, then as needed.
- On SSRI — review at 2, 4, 8, 12 weeks (titration); then 6-monthly when stable.
- Treatment-resistant — specialist review, regular Y-BOCS monitoring, MDT.
- Relapse prevention plan — early warning signs, ERP booster sessions, never stop SSRI abruptly (taper over 4 to 8 weeks to avoid discontinuation syndrome). [1]
Special Populations
Children and adolescents:[2]
- Onset common; family involvement is essential.
- CBT/ERP first-line, adapted for age (the therapist uses cartoon materials, parental coaching, exposure tasks framed as 'detective work'). Family-based ERP is the gold standard for paediatric OCD.
- SSRI added if moderate-severe — fluoxetine first-line in children over 8 (FDA-approved); sertraline over 6; lower starting doses; watch for activation, behavioural disinhibition and suicidal ideation (FDA black-box warning on antidepressants in under-25s).
- PANDAS/PANS in sudden-onset cases — ASO titre, antibiotic eradication of strep.[13]
- Children may not articulate insight — do not withhold the diagnosis.
PANDAS / PANS:[13]
- Penicillin V (or azithromycin) for strep eradication.
- SSRI (lower dose, slow titration).
- ERP.
- IVIG or plasmapheresis for severe cases (controversial).
- Prophylactic antibiotics to prevent recurrence in some centres. [1]
Pregnancy and breastfeeding:[5]
- ERP first-line — no teratogenic risk.
- Sertraline preferred SSRI if medication needed — lowest breast-milk transfer; widely considered safest in lactation.
- Avoid paroxetine in first trimester (cardiac defects) and clomipramine (neonatal withdrawal).
- Fluoxetine — relatively safe but higher breast-milk transfer than sertraline.
- Untreated maternal OCD is associated with poorer obstetric and child outcomes — weigh risks; involve perinatal psychiatry MDT. [1]
Peripartum onset (intrusive infant-harm thoughts):[5]
- ERP first-line; sertraline preferred.
- Reassure mother: intrusive harm thoughts are common in the postpartum and rarely acted upon; the distress they cause is itself a marker of maternal protective intent.
- Distinguish from postpartum psychosis — no delusions, hallucinations or thought disorder in OCD.
- Safeguarding assessment if mother is avoiding infant; involve perinatal mental health team. [1]
Elderly:[1]
- Lower SSRI doses; watch SIADH (especially in frail elderly with comorbidity).
- Citalopram max 20 mg in over 65s (QTc).
- Rule out organic OCD — basal ganglia stroke, post-encephalitic, CO poisoning, normal pressure hydrocephalus; MRI brain if late-onset or focal neurology. [1]
Comorbid bipolar disorder:[1]
- Avoid antidepressant monotherapy — precipitates mania.
- Stabilise mood first (mood stabiliser or atypical antipsychotic), then add SSRI cautiously with close monitoring. [1]
Comorbid schizophrenia:[1]
- Antipsychotic + SSRI.
- Some antipsychotics (especially clozapine) can worsen OC symptoms. [1]
Intellectual disability and autism:[1]
- Lower SSRI doses; adapt ERP (behavioural emphasis, simpler exposure tasks); expect more side effects; involve carers. [1]
Tic-related OCD:[1]
- Add antipsychotic (risperidone, aripiprazole) earlier; SSRIs less effective alone. [1]
Evidence, Guidelines & Regional Differences
DSM-5-TR (2022) — the diagnostic classification change:[1]
- OCD was moved out of the Anxiety Disorders (DSM-III to DSM-IV-TR) into its own "Obsessive-Compulsive and Related Disorders" category — driven by distinct neurobiology (CSTC circuit), family aggregation, treatment response, and symptom structure.[1]
- Insight specifier (good/fair, poor, absent/delusional) — OCD with absent insight is still OCD.
- Tic-related specifier — current or past tic disorder; predicts better response to antipsychotic augmentation.
- Hoarding disorder separated from OCD into its own diagnosis.
ICD-11 (2022, 6B20):[6]
- WHO largely harmonised ICD-11 with DSM-5 — OCD is now under "Obsessive-Compulsive or Related Disorders", with subtypes for obsessions, compulsions, and mixed. The previous ICD-10 F42 was retained in legacy but is now superseded.[6]
NICE CG31 (UK, 2005, updated) — stepped care:[5]
- Step 1: identify, assess, psychoeducation.
- Step 2 (mild): low-intensity ERP-based guided self-help, brief CBT.
- Steps 3-4 (moderate-severe): CBT including ERP (13-20 hours per patient) OR an SSRI; combined if monotherapy insufficient.
- Step 5 (refractory): specialist multidisciplinary team; combined intensive ERP + SSRI; consider clomipramine, antipsychotic augmentation, intensive day programme. [1]
Landmark trials:[11]
- Foa 2005 (Am J Psychiatry) — randomised, placebo-controlled trial of ERP, clomipramine, combined, and placebo in OCD. ERP was more effective than clomipramine; combined was not superior to ERP alone. Key message: ERP is the most powerful single treatment; combined ERP + SSRI is best for severe OCD.[11]
- Bloch 2006 systematic review (Mol Psychiatry) — antipsychotic augmentation (especially haloperidol and risperidone) is effective in treatment-refractory OCD; effect is small but real, particularly in tic-related OCD.[3]
- Ruscio 2010 (Mol Psychiatry, NCS-R) — definitive epidemiology: lifetime prevalence 2 to 3 percent; substantial comorbidity and impairment; strong treatment gap.[10]
- IOCDF-GC/OCGAS 2018 (Mol Psychiatry) — meta-analysis revealed the polygenic architecture of OCD.[7]
- Strom 2025 (Nature Genetics) — genome-wide meta-analysis identifying 30 genome-wide significant loci; the largest genetic study to date.[8]
- Fineberg 2020 ICNP position statement — international consensus on stepped pharmacological and psychological care.[5]
- Mataix-Cols 2022 — operational definitions of treatment response and remission (Y-BOCS 30-35 percent reduction; remission ≤12).[9]
Regional guideline differences:[1][5]
- US (APA / FDA-approved for OCD) — fluoxetine, fluvoxamine, sertraline, paroxetine, clomipramine are FDA-approved for OCD. Citalopram/escitalopram are used off-label.
- UK (NICE CG31) — sertraline, fluoxetine, fluvoxamine, paroxetine, citalopram, escitalopram, and clomipramine are all licensed; sertraline and clomipramine are preferred choices in NICE implementation.
- India — fluoxetine, sertraline, fluvoxamine, paroxetine, and clomipramine are widely available and used; ERP availability is more limited; behavioural therapy is often delivered by clinical psychologists in tertiary centres. [1]
- PANDAS existence and treatment — the diagnostic category is debated; many clinicians prefer the broader PANS label; IVIG and plasmapheresis evidence is mixed.
- Deep brain stimulation target selection (nucleus accumbens vs ventral capsule vs STN vs anterior limb of internal capsule) is still being refined.
- Capsulotomy vs DBS — DBS is reversible and adjustable; capsulotomy is ablative and irreversible; both reserved for the most refractory cases.
- Long-term SSRI safety — sexual dysfunction, weight change, QTc, hyponatraemia; many patients require lifelong treatment.
- Over-prescription in mild OCD where ERP alone is sufficient. [1]
Exam Pearls
- OCD = obsessions (intrusive, recurrent, unwanted thoughts/images) + compulsions (repetitive acts/mental acts to reduce anxiety); over 1 hour per day; significant distress; insight present.[1]
- DSM-5-TR moved OCD OUT of Anxiety Disorders into its own Obsessive-Compulsive and Related Disorders category (siblings: body dysmorphic, hoarding, trichotillomania, excoriation).[1]
- Insight specifier: good/fair, poor, absent (delusional) — still OCD, not psychosis.[1]
- Distinguish OCD (ego-dystonic, resisted, anxiety-driven) from OCPD (ego-syntonic perfectionism, traits, lifelong, no distress).[1]
- Five symptom dimensions: contamination/washing, doubt/checking, symmetry/ordering/counting, forbidden/taboo thoughts (sexual/aggressive/religious), hoarding.[12]
- SSRIs at HIGH doses (fluoxetine 60 mg, sertraline 200 mg, paroxetine 60 mg, fluvoxamine 300 mg) — much higher than depression doses; effect at 8 to 12 weeks.[1][5]
- Clomipramine (TCA) is an effective alternative when SSRI fails; mechanism via serotonergic reuptake inhibition; ECG/LFT monitoring; lethal in overdose.
- Antipsychotic AUGMENTATION (risperidone, haloperidol, aripiprazole) — not monotherapy — for refractory OCD; Bloch 2006 meta-analysis.[3]
- ERP (exposure and response prevention) is the gold-standard psychological therapy; expose to trigger, prevent compulsion, anxiety habitualises; Foa 2005 showed ERP more effective than clomipramine.[11]
- Y-BOCS: 10 items, 0-4 each, total 0-40; response 30 to 35 percent reduction; remission total ≤12 (or ≤8 excellent).[9]
- PANDAS: sudden-onset paediatric OCD + tics + choreiform movements + urinary symptoms after GAS strep; check ASO titre and anti-DNase B; treat strep with penicillin V.[13]
- CSTC circuit: orbitofrontal cortex + ACC hyperactive; caudate fails to filter; thalamus relays worry back to cortex in an endless loop.[4]
- Functional imaging (PET/fMRI) normalises after successful SSRI or ERP — a treatment biomarker.[4]
- Lifetime prevalence 2 to 3 percent; onset adolescence/early adulthood; 11 to 17 years delay to diagnosis; chronic waxing-waning course.[10]
- Suicide risk is elevated (lifetime ideation up to 36 percent) — assess, especially with comorbid depression.[1]
- Hoarding is now its own DSM-5 disorder — difficulty discarding, distress at discarding, clutter; not at intrusive thoughts.[1]
- Peripartum OCD: intrusive infant-harm thoughts are common, ego-dystonic, rarely acted upon — distinguish from postpartum psychosis.[5]
- OCD + bipolar: NEVER antidepressant monotherapy — stabilise mood first.[1]
- Heritability 40 to 50 percent (adult), 45 to 65 percent (paediatric); first-degree relatives 3 to 12-fold risk.[7]
- Glutamate hypothesis: memantine, ketamine, riluzole, NAC under study for refractory OCD.[4]
Exam application bank (NEET-PG / INICET)
One-line answer
Obsessive-compulsive disorder (OCD) is a chronic, disabling mental disorder characterised by obsessions (intrusive, unwanted, recurrent thoughts, images or urges that cause marked anxiety or distress) and/or compulsions (repetitive behaviours or mental acts the person feels driven to perform to neutralise the obsession or prevent a dreaded outcome), that are time-consuming (over 1 hour per day) or cause clinically significant distress and impairment. Patients have insight (recognise the obsessions as irrational) but cannot resist them — this distinguishes OCD from psychosis (no insight), delusional disorder and OCPD (ego-syntonic). Common themes: contamination/washing, doubt/checking, symmetry/ordering/counting, forbidden/taboo thoughts (sexual, religious, aggressive, somatic), hoarding. Lifetime prevalence about 2 to 3 percent; onset typically adolescence to early adulthood; average 11
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Obsessive-Compulsive Disorder (OCD).
References
- [1]Hirschtritt ME, Bloch MH, Mathews CA. Obsessive-Compulsive Disorder: Advances in Diagnosis and Treatment JAMA, 2017.PMID 28384832
- [2]Krebs G, Heyman I. Obsessive-compulsive disorder in children and adolescents Arch Dis Child, 2015.PMID 25398447
- [3]Bloch MH, Landis-Weaver C, Kelmendi B, Coric V, Panza KE, Leckman JF. A systematic review: antipsychotic augmentation with treatment refractory obsessive-compulsive disorder Mol Psychiatry, 2006.PMID 16585942
- [4]Pittenger C, Bloch MH, Williams K. Glutamate abnormalities in obsessive compulsive disorder: neurobiology, pathophysiology, and treatment Pharmacol Ther, 2011.PMID 21963369
- [5]Fineberg NA, Brown A, Reghunandanan S, Pampaloni I. Clinical advances in obsessive-compulsive disorder: a position statement by the International College of Obsessive-Compulsive Spectrum Disorders Int Clin Psychopharmacol, 2020.PMID 32433254
- [6]Stein DJ, Kogan CS, Atmaca M, et al. Mental, behavioral and neurodevelopmental disorders in the ICD-11: an international perspective on key changes and controversies BMC Med, 2020.PMID 31983345
- [7]International Obsessive Compulsive Disorder Foundation Genetics Collaborative (IOCDF-GC) and OCD Collaborative Genetics Association Studies (OCGAS). Revealing the complex genetic architecture of obsessive-compulsive disorder using meta-analysis Mol Psychiatry, 2018.PMID 28761083
- [8]Strom NI, Gerring R, Bhatt JM, et al. Genome-wide analyses identify 30 loci associated with obsessive-compulsive disorder Nat Genet, 2025.PMID 40360802
- [9]Mataix-Cols D, Alonso P, Heras JV, et al. Operational Definitions of Treatment Response and Remission in Obsessive-Compulsive Disorder Capture Meaningful Improvements in Everyday Life Psychother Psychosom, 2022.PMID 36382651
- [10]Ruscio AM, Stein DJ, Chiu WT, Kessler RC. The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication Mol Psychiatry, 2010.PMID 18725912
- [11]Foa EB, Liebowitz MR, Kozak MJ, et al. Randomized, placebo-controlled trial of exposure and ritual prevention, clomipramine, and their combination in the treatment of obsessive-compulsive disorder Am J Psychiatry, 2005.PMID 15625214
- [12]Mataix-Cols D, do Rosario-Campos MC, Leckman JF. A multidimensional model of obsessive-compulsive disorder Am J Psychiatry, 2005.PMID 15677583
- [13]Garvey MA, Swedo SE. PANDAS: the search for environmental triggers of pediatric neuropsychiatric disorders. Lessons from rheumatic fever J Child Neurol, 1998.PMID 9733286