Psychiatry · Psychiatry
Personality Disorders
Also known as Personality disorders · Borderline personality disorder · BPD · Antisocial personality disorder · Cluster B
Personality disorders (PD) are enduring, inflexible, and pervasive patterns of inner experience and behaviour that deviate markedly from the expectations of the individual's culture, are stable over time, begin by adolescence or early adulthood, lead to distress or impairment, and are not better explained by another mental disorder, substance use, or a medical condition. DSM-5 groups them into three clusters: Cluster A (odd, eccentric) — paranoid, schizoid, schizotypal; Cluster B (dramatic, emotional, erratic) — antisocial, borderline, histrionic, narcissistic; Cluster C (anxious, fearful) — avoidant, dependent, obsessive-compulsive (OCPD). Borderline personality disorder (BPD) is the most clinically important and most examined: frantic efforts to avoid abandonment, unstable intense relationships, identity disturbance, impulsivity, recurrent self-harm/suicidal behaviour, affective instability, chronic emptiness, inappropriate anger, and transient stress-related paranoia or dissociation. Dialectical behaviour therapy (DBT) is first-line, with mentalization-based therapy (MBT) and schema therapy as alternatives; pharmacotherapy is symptom-targeted only, and benzodiazepines are avoided.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Overview & Definition
Personality is the enduring, characteristic way an individual thinks, feels, behaves, and relates to others — the stable "set point" of a person across time and situations. A personality disorder is diagnosed when this set point becomes inflexible, pervasive, and maladaptive, producing distress or functional impairment and deviating markedly from cultural expectations. The pattern must be stable and long-standing, traceable to adolescence or early adulthood, and not better explained by another mental disorder (Axis I), a substance, or a medical condition.[1]
Although historically dismissed as "treatment-resistant" or "heartsink" patients, modern evidence shows the opposite: BPD is one of the most treatable conditions in psychiatry, with structured psychotherapy producing large effect sizes and high long-term remission rates.[1][5] The clinical skill lies in four moves: (1) recognise the enduring, cross-situational pattern (not an acute episode); (2) distinguish it from Axis I disorders (BPD vs bipolar, ASPD vs substance use, schizotypal vs schizophrenia); (3) set firm, consistent therapeutic boundaries (anticipating splitting rather than personalising it); and (4) initiate structured, evidence-based psychotherapy (DBT, MBT) while using medication only for symptom targets.[2]
The DSM-5 general criteria for any personality disorder
The DSM-5 requires all six of the following to be met before any specific PD is diagnosed:[1]
1. Enduring pattern
- Of inner experience and behaviour that deviates markedly from cultural expectations
- Manifest in ≥2 of: cognition, affectivity, interpersonal functioning, impulse control
2. Pervasive & inflexible
- Stable and long-standing
- Present across a broad range of personal and social situations
3. Distress / impairment
- Clinically significant distress
- Or social, occupational, or other functional impairment
4. Stable & long-standing
- Onset traceable to adolescence or early adulthood
- Not a new or episodic phenomenon
5. Not better explained
- By another mental disorder (Axis I)
- Or by a substance or medical condition
6. Not just developmentally normal
- For children/adolescents, features must persist ≥1 year
- Adult patterns must not be a culturally sanctioned response

Classification
DSM-5 retains a categorical model of ten specific personality disorders organised into three clusters by phenotypic resemblance. This clustering is the exam-centred frame: it predicts comorbidity within a cluster and guides the differential.[2]

Cluster A — "odd, eccentric" (the "Mad" cluster)
Paranoid PD
- Pervasive distrust & suspiciousness
- 4 of 7: suspects exploitation, preoccupied with loyalty doubts, reluctant to confide, reads hidden demeaning meanings, bears grudges, perceives attacks on character, recurrent suspicions regarding fidelity of partner
- Wants relationships but cannot trust
Schizoid PD
- Pervasive detachment from social relationships + restricted emotional expression
- Neither desires nor enjoys close relationships (including family)
- Chooses solitary activities, emotional coldness, indifference to praise/criticism
- Does NOT have psychotic features
Schizotypal PD
- Pervasive social deficits + cognitive/perceptual distortions + eccentric behaviour
- Ideas of reference, magical thinking/odd beliefs, unusual perceptual experiences, odd speech (vague, circumstantial), suspiciousness/paranoid ideation
- Inappropriate/constricted affect, odd behaviour/appearance
- On the schizophrenia spectrum — may benefit from low-dose antipsychotic
- Reality testing intact (distinguishes from schizophrenia)
Cluster B — "dramatic, emotional, erratic" (the "Bad" cluster)
Cluster B is the highest-yield cluster for NEET-PG/INICET: these are the patients who disrupt wards, overdose, get admitted, and dominate the viva.[1]
Antisocial PD (ASPD)
- Pervasive disregard for & violation of the rights of others
- 3 of 7 since age 15: failure to conform to law, deceitfulness, impulsivity/failure to plan ahead, irritability/aggressiveness, reckless disregard for safety, irresponsibility, lack of remorse
- MUST have evidence of conduct disorder before age 15
- Commoner in men; strongly associated with substance use & prison
Borderline PD (BPD)
- Pervasive instability of relationships, self-image, affects, & marked impulsivity
- 5 of 9 criteria
- Highest suicide rate of the PDs
- Responds to DBT/MBT — treatable
- See full criteria box below
Histrionic PD
- Pervasive excessive emotionality & attention-seeking
- 5 of 8: uncomfortable when not the centre of attention, sexually seductive/inappropriate, shallow/shifting emotion, uses appearance to draw attention, impressionistic/vague speech, dramatic/exaggerated, suggestible, considers relationships more intimate than they are
- Commoner in women
Narcissistic PD
- Pervasive grandiosity, need for admiration, & lack of empathy
- 5 of 9: grandiose sense of self-importance, preoccupied with fantasies of success/power/beauty/love, believes special/unique, requires excessive admiration, sense of entitlement, interpersonally exploitative, lacks empathy, envious/believes others envious, arrogant/haughty
- Fragile self-esteem behind the façade — prone to narcissistic injury
- Commoner in men
Cluster C — "anxious, fearful" (the "Sad" cluster)
Avoidant PD
- Pervasive social inhibition, feelings of inadequacy, & hypersensitivity to criticism
- 4 of 7: avoids occupational activities involving interpersonal contact, unwilling to get involved unless certain of being liked, restrained in intimate relationships, preoccupied with criticism/rejection, feels inadequate, views self as inept/unappearing, reluctant to take personal risks
- WANTS relationships but fears rejection (key contrast with schizoid)
Dependent PD
- Pervasive & excessive need to be taken care of → submissive/clinging behaviour & fears of separation
- 5 of 8: difficulty making decisions without reassurance, needs others to assume responsibility, difficulty expressing disagreement, difficulty initiating projects, goes to excessive lengths for nurturance/support, uncomfortable/helpless when alone, urgently seeks new relationship when one ends, preoccupied with fears of being left to care for self
- Commoner in women
Obsessive-Compulsive PD (OCPD)
- Pervasive preoccupation with orderliness, perfectionism, & mental/interpersonal control at the expense of flexibility, openness, & efficiency
- 4 of 8: preoccupied with rules/lists/order to the point of losing the activity's point, perfectionism interfering with task completion, excessively devoted to work to the exclusion of leisure/friendships, overconscientious/inflexible about morality, unable to discard worn-out objects, reluctant to delegate, miserly spending style, rigid & stubborn
- EGO-SYNTONIC (vs OCD ego-dystonic)
- Commoner in men; comorbid with depression, anxiety
Beyond DSM-5 — ICD-11 and the alternative DSM-5 model
The categorical system has well-known problems: high comorbidity, arbitrary thresholds, and "PD-NOS" being the most common diagnosis. Two newer dimensional systems address this, and examiners may probe awareness of the direction of travel.[1]
The DSM-5 Alternative Model for Personality Disorders (AMPD, Section III) uses two pillars: a Level of Personality Functioning scale (0 = little/no impairment to 4 = extreme) measuring self and interpersonal functioning, plus five pathological trait domains (Negative affectivity, Detachment, Antagonism, Disinhibition, Psychoticism). Only six specific PDs are retained in Section III (antisocial, avoidant, borderline, narcissistic, obsessive-compulsive, schizotypal); others are diagnosed as Personality Disorder–Trait Specified (PD-TS).[1]
Epidemiology & Risk Factors
Personality disorders are common in both the general population and clinical settings, yet markedly under-recognised — particularly BPD in men and Cluster C disorders everywhere.[1]
Sex distribution — beware the stereotype
Although the stereotype of BPD is a young woman, community studies show roughly equal prevalence between men and women; men are simply under-diagnosed because they more often present with externalising phenotypes (anger, substance use, violence) that get labelled antisocial or substance use disorder instead. The other recognised sex skew is that ASPD is much commoner in men (male-to-female ratio roughly 3-6:1) and histrionic and dependent PDs are reported more often in women (though referral bias contributes).[2]
Risk factors and aetiology
The strongest and most reproducible aetiological finding in BPD is childhood trauma: roughly 70-80 percent of BPD patients report childhood abuse, neglect, or invalidating caregiving, and the dose-response is consistent — more severe, earlier, and multi-type adversity predicts more severe borderline pathology.[1]
Genetic / temperamental
- BPD heritability ~40-50% (twin studies)
- Inherited temperament: high emotional reactivity, impulsivity, low conscientiousness
- Polygenic — no single 'BPD gene'
- Heritability is expressed through gene-environment interaction
Early environment
- Childhood sexual, physical, emotional abuse
- Neglect, invalidating caregiving (Linehan)
- Parental loss, separation, instability
- Disorganised attachment
Neurobiology
- Amygdala hyperactivity
- Reduced prefrontal/orbitofrontal control
- HPA-axis dysregulation, abnormal DST
- Reduced hippocampal & amygdala volume
- Serotonergic dysregulation (impulsivity/aggression)
Psychological
- Mentalisation failure (inability to read own/others' minds under stress)
- Deficits in emotion regulation
- Schema modes: abandoned child, angry child, punitive parent
Pathophysiology
There is no single "lesion" of a personality disorder. The most coherent account is a trait-based model: inherited or trauma-induced differences in emotion-processing, top-down control, and attachment neurocircuitry produce an enduring phenotype that becomes maladaptive when it collides with adult demands.[1]
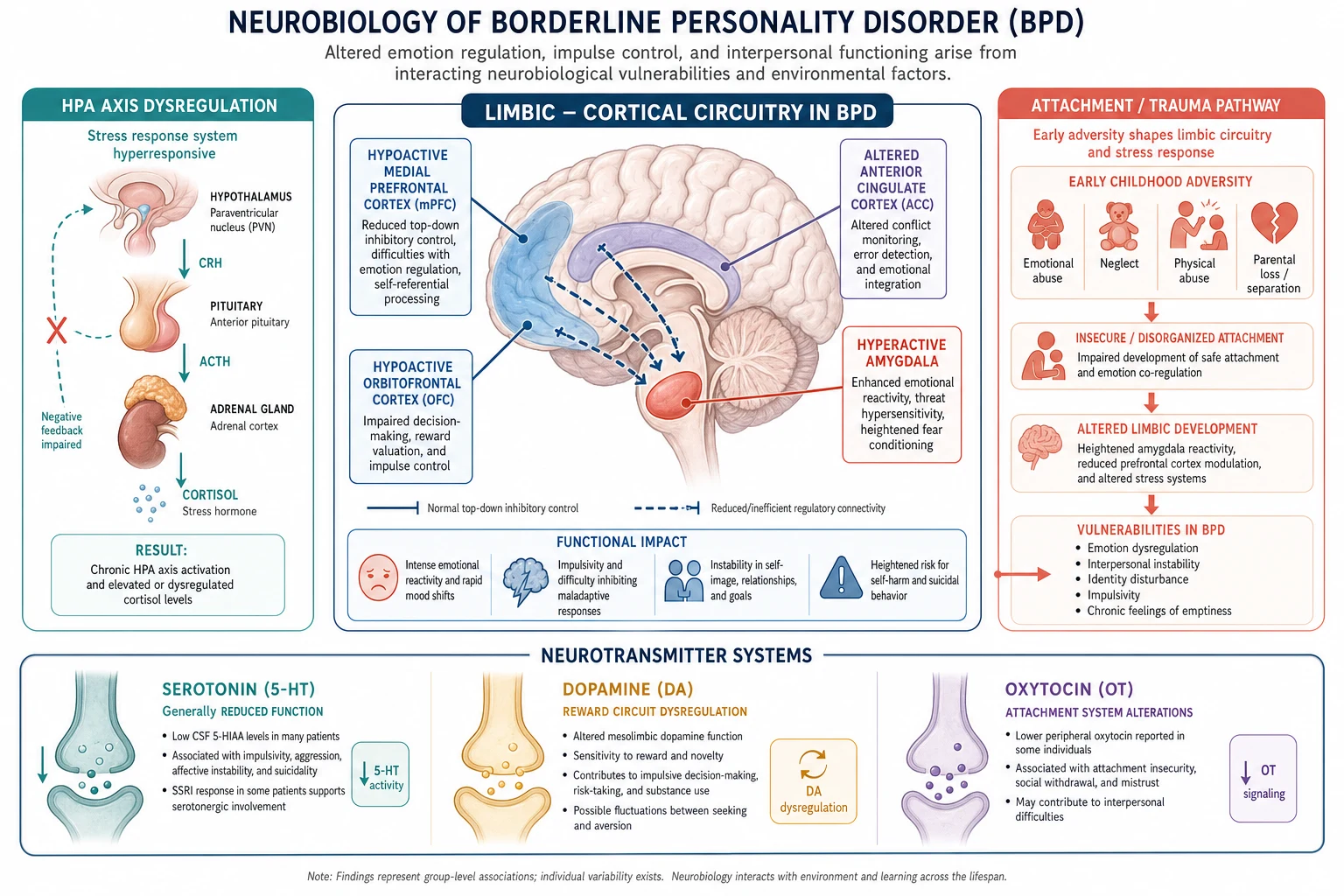
The amygdala-prefrontal imbalance
The single most reproducible finding is hyperactive limbic reactivity with impaired cortical regulation. When shown emotional faces (especially fearful or angry ones), people with BPD show exaggerated amygdala activation; the dorsolateral and ventromedial prefrontal regions that normally dampen this signal fire less. The functional consequence is the clinical picture: intense, rapid, slow-to-resolve emotions paired with poor capacity to inhibit the resulting impulse.[1]
Childhood trauma → sensitised limbic system
Early and repeated adversity appears to kindle the developing limbic system, producing lasting structural change — reductions in hippocampal volume, smaller corpus callosum, and sensitised amygdala reactivity. This explains why BPD and complex PTSD share so many features (affect dysregulation, relationship instability, dissociation) and why the two diagnoses overlap heavily.[1]
Neurotransmitter systems
- Serotonin (5-HT): reduced serotonergic tone in prefrontal cortex correlates with impulsivity, aggression, and suicide — the rationale for SSRIs targeting impulsive-aggressive symptoms even when mood is not depressed.
- Dopamine: dysregulation in reward and stress pathways contributes to anhedonia, emptiness, and stress-induced transient psychosis — the rationale for low-dose antipsychotics for transient psychotic or paranoid symptoms.
- Oxytocin: the attachment neuropeptide; early neglect alters oxytocin signalling, contributing to the intense fear of abandonment and unstable attachments that define BPD.[1]
Mentalisation and the developmental model
From the MBT perspective (Bateman & Fonagy), the core deficit is impaired mentalisation — the capacity to understand behaviour (one's own and others') in terms of underlying mental states (feelings, wishes, intentions).[4] In BPD this capacity, which develops within secure attachment relationships, is fragile and collapses under emotional arousal — the patient then experiences their own and others' feelings as overwhelming and opaque, fuelling impulsivity, splitting, and the chaotic relationships. This model directly justifies a therapy (MBT) that rebuilds mentalisation.
Clinical Presentation
The examiner-friendly way to remember PD presentation is "stable instability": stable in that it is enduring and pervasive, unstable in that moods, relationships, self-image, and behaviour fluctuate dramatically.[1]
Borderline PD — the prototype
A typical BPD presentation in clinical practice: a woman in her twenties (though men present similarly — and are missed) who has, since adolescence, experienced intense, short-lived mood swings triggered by interpersonal events; a string of chaotic, intense relationships that alternate between adoration and contempt; a fragile and shifting sense of self (goals, values, sexual orientation, career plans all feel uncertain); repeated self-harm (cutting, burning, overdoses) typically triggered by abandonment anxiety; chronic feelings of emptiness; intense, inappropriate anger; and transient stress-related paranoia or dissociation that resolves when the stressor passes.[1]
The mood shifts of BPD are reactive and short-lived (minutes to hours, occasionally a day or two), almost always triggered by a perceived interpersonal rejection or abandonment — the single most useful discriminator from bipolar disorder.[2]
Antisocial PD — the forensic presentation
A man (typically) with a childhood conduct disorder history (cruelty to animals/people, fire-setting, truancy, running away, destruction of property, lying, theft, serious rule-breaking before age 15) who, since age 15, shows a pervasive pattern of disregard for others' rights: criminality, deceitfulness, impulsivity, aggression, recklessness, irresponsibility, and an absence of remorse. He presents via the criminal justice system, the emergency department after violence or overdose, or with comorbid substance use. The conduct-disorder-before-15 requirement is non-negotiable — without it the ASPD diagnosis cannot be made (though it may be "antisocial personality traits").[2]
Narcissistic PD — grandiosity and vulnerability
Presents with overt grandiosity, entitlement, and need for admiration, but the clinician's reward is recognising the fragile self-esteem beneath the façade. Narcissistic injury — a perceived slight, criticism, or loss of status — can precipitate rage, severe dysphoria, devaluation of the offending person, or even suicidal crisis. Lack of empathy is the central interpersonal failure; relationships are exploitative and instrumental.[2]
Histrionic PD — the dramatic patient
Presents as dramatic, vivacious, and attention-seeking, with shallow, rapidly shifting emotions, theatrical or exaggerated speech that is long on emotion but short on detail ("impressionistic"), seductive/inappropriate dress or behaviour, and high suggestibility. They are uncomfortable unless the centre of attention.[2]
Cluster A presentations
These patients rarely present to psychiatry for their personality — they tend to present with secondary depression, decompensation under stress, or, for schizotypal, transient psychosis. The clue on interview is the odd, eccentric, or guarded quality: vague or magical ideas (schizotypal), pervasive suspiciousness (paranoid), or emotional coldness and indifference to relationships (schizoid).[2]
Cluster C presentations
Cluster C patients present with anxiety-driven dysfunction: the avoidant patient is socially isolated and impaired by fear of rejection; the dependent patient cannot function autonomously and tolerates abusive relationships to avoid abandonment; the OCPD patient is exhausted, work-obsessed, and in relational conflict over their rigidity, yet sees their behaviour as correct.[2]
Differential Diagnosis
The PD differential is where most marks are won and lost, because examiners deliberately test the mimics. The cardinal principle: diagnose a PD only when the pattern is enduring and not better explained by another disorder.[2]
BPD vs bipolar disorder
- MOOD: BPD shifts are minutes-to-hours, reactive to interpersonal triggers, with rapid return to baseline euthymia; bipolar episodes are days-to-weeks, spontaneous, sustained
- TRIGGER: BPD dysphoria is provoked by perceived abandonment; bipolar is not
- COURSE: BPD traits are chronic since adolescence; bipolar is episodic with normal intervals
- FAMILY HISTORY: bipolar strongly familial; BPD less so
- TREATMENT RESPONSE: bipolar responds to mood stabilisers; BPD to psychotherapy
BPD vs complex PTSD
- Both: trauma history, affect dysregulation, relationship instability, dissociation, self-harm
- cPTSD: PTSD symptoms (re-experiencing, avoidance, hyperarousal) dominate; identity disturbance and fear of abandonment less central
- BPD: fear of abandonment, unstable relationships, impulsivity, identity disturbance are core
- Substantial overlap — many patients meet both; the distinction guides therapy (trauma-focused vs DBT/MBT)
BPD vs histrionic PD
- Both Cluster B, attention-seeking and emotionally dramatic
- Histrionic: shallow affect, no self-harm, no identity disturbance, no abandonment-driven suicidality
- BPD: self-harm, identity disturbance, intense abandonment anxiety, anger
ASPD vs substance use disorder
- Both can produce deceit, irresponsibility, law-breaking
- Establish which came first: ASPD traits present from childhood (conduct disorder) and persist during sobriety; pure SUD behaviours resolve with abstinence
- Often coexist — treat both
Schizotypal PD vs schizophrenia
- Both: odd beliefs, magical thinking, eccentric behaviour, social deficits
- Schizotypal: reality testing INTACT, no frank delusions/hallucinations, chronic trait-level oddity, better functioning
- Schizophrenia: overt psychosis (delusions, hallucinations, thought disorder), deterioration, functional decline
- Schizotypal may decompensate into brief psychosis under stress but recovers
Paranoid PD vs delusional disorder vs schizophrenia (paranoid)
- Paranoid PD: pervasive suspiciousness but NO frank delusions; reality testing preserved; personality-level
- Delusional disorder: fixed, non-bizarre delusions without other schizophrenia features; otherwise normal function
- Schizophrenia paranoid: delusions + hallucinations + thought disorder + functional decline
OCPD vs OCD
- OCPD: ego-SYNTONIC perfectionism, order, control; patient does not see a problem with the traits; treats others as the problem
- OCD: ego-DYSTONIC obsessions & compulsions; patient pleads for relief; insight usually preserved
- OCPD: no true obsessions/compulsions; rigidity is 'just who I am'
- OCD responds to SSRI + CBT/ERP; OCPD to longer-term psychotherapy
Avoidant PD vs schizoid PD
- Both socially isolated
- Avoidant: WANTS relationships but fears rejection; hypersensitive to criticism; lonely
- Schizoid: does NOT desire relationships; indifferent; content in solitude
- Avoidant: anxious, yearning; Schizoid: detached, indifferent
Dependent PD vs BPD
- Both fear separation/abandonment
- Dependent: clingy, submissive, seeks care; lacks BPD's impulsivity, anger, self-harm, identity disturbance
- BPD: reactive, impulsive, chaotic, self-harming; relationships devalued as well as idealised
The "rule out organic" differentials
[2]Clinical & Bedside Assessment
PD diagnosis is clinical, made from a longitudinal history rather than a single interview. The history must establish the four anchoring properties: enduring, pervasive, since early adulthood, causing impairment.[2]
Taking the longitudinal history
- Onset and course — when did the patterns begin? (should trace to adolescence/early adulthood). Have they been stable and persistent, or episodic?
- Pervasiveness — do the behaviours appear across relationships, work, and contexts, or only one (e.g. only with a partner)?
- Relationships — pattern of intensity, instability, idealisation/devaluation, abandonment sensitivity.
- Self-image — sense of identity, goals, values; chronic emptiness.
- Impulsivity and self-harm — overdoses, cutting, reckless behaviours, eating, spending, sex, driving.
- Affect — reactivity, lability, anger, dysphoria, duration of mood shifts.
- Childhood and development — conduct problems before 15 (for ASPD), trauma/abuse/neglect history (for BPD), attachment history.
- Comorbidity — mood, anxiety, substance use, eating, PTSD, ADHD.
- Function — work, relationships, self-care; forensic history.[5]
Mental state examination — what to look for
- Appearance/behaviour: may be appropriate or dramatic/histrionic; self-harm scars (BPD — multiple, old and new, often on forearms/thighs); tattooing/piercing sometimes relevant (not diagnostic).
- Speech: dramatic/impressionistic (histrionic), vague/metaphorical (schizotypal), guarded (paranoid).
- Mood and affect: reactive, labile (BPD); constricted/blunted (schizoid); angry/expansive (ASPD/narcissistic).
- Thought: magical ideas, ideas of reference (schizotypal); suspiciousness (paranoid); grandiosity (narcissistic); chronic emptiness (BPD); transient stress-related paranoia (BPD) — but not fixed delusions.
- Perception: transient dissociation under stress (BPD); no persistent hallucinations (if present, reconsider schizophrenia).
- Insight and judgement: typically partial; traits are often ego-syntonic (especially OCPD, narcissistic, ASPD).[2]
Risk assessment — the non-negotiable step
Every PD assessment must include a structured suicide and self-harm risk assessment. Do not rely on gut feel.[2]
Static risk factors
- Prior suicide attempt (strongest predictor)
- Family history of suicide
- Childhood trauma/abuse
- Male sex (completed suicide)
- Comorbid depression or substance use
- Access to means
Dynamic risk factors
- Current suicidal ideation with plan/intent
- Recent self-harm
- Acute abandonment/loss event
- Hopelessness
- Command hallucinations (if comorbid psychosis)
- Intoxication
Protective factors
- Responsibility to children/family
- Treatment engagement
- Future orientation
- Religious/moral objection to suicide
- Social support
Named tools (used to structure, never to replace, clinical judgement):
- Columbia Suicide Severity Rating Scale (C-SSRS) — the current gold standard; assesses ideation severity, intensity, and behaviour.
- SAD PERSONS — Sex male, Age 45 or over (varies by version), Depression, Previous attempt, Ethanol abuse, Rational thinking loss, Social support lack, Organised plan, No spouse, Sickness. A screening tool only — poor positive predictive value; do not use it to determine admission alone.[2]
Investigations
There is no blood test, scan, or biological marker for any personality disorder. The diagnosis is made clinically from the history and mental state examination against DSM-5 criteria. Investigations serve two purposes: to exclude organic causes and to quantify severity and comorbidity.[2]
Investigations to exclude organic causes
Bloods
- FBC, U&E, LFT, glucose, TFT — exclude metabolic/endocrine mimics
- B12 and folate
- Calcium
- Syphilis and HIV serology
- Lipid/CK if antipsychotic planned
Toxicology
- Urine drug screen — rule out stimulant/cannabis/alcohol as cause or comorbidity
- Blood alcohol level if acute presentation
Neuroimaging
- CT or MRI brain — ONLY if focal neurology, new onset, cognitive impairment, or head injury
- Not routine for PD workup
EEG
- Only if seizure suspected (temporal lobe epilepsy mimic)
- Not routine
Structured diagnostic interviews (specialist setting)
When the diagnosis is uncertain or for research/specialist PD services, structured interviews improve reliability:[4]
- Structured Clinical Interview for DSM-IV/5 Personality Disorders (SCID-II) — clinician-administered, criterion-by-criterion; the reference standard.
- International Personality Disorder Examination (IPDE) — WHO/ICD-aligned, semi-structured, rates each criterion as absent/subthreshold/definite with a 5-year time frame; high reliability.
- These are specialist tools, not used in routine MBBS practice, but examiners may name them.[4]
Severity and screening scales
- Zanarini Rating Scale for Borderline Personality Disorder (ZAN-BPD) — a 9-item clinician-rated scale (one per DSM criterion), each scored 0-4; total 0-36; tracks BPD severity and treatment response. A cut-off of ≥9 supports the diagnosis; changes track response to DBT/MBT.
- McLean Screening Instrument for BPD (MSI-BPD) — a 10-item self-report true/false screen; cut-off ≥7 prompts full assessment. High sensitivity (~80 percent).
- BDI / PHQ-9 — quantify comorbid depression; do not use to diagnose BPD.
- AUDIT / DAST — quantify comorbid substance use.[2]
Why investigations and scales are insufficient
Psychological tests and scales never diagnose a PD in isolation. Diagnosis requires the longitudinal history establishing pervasiveness and stability since early adulthood, integrated with the MSE, informant history where possible, and exclusion of organic causes and Axis I disorders. A high MSI-BPD score in a stressed student without an enduring pattern is not a BPD diagnosis.[2]
Management — Resuscitation
PD itself is rarely an emergency — but its complications (self-harm, overdose, suicidal crisis, behavioural dyscontrol) frequently present acutely. Resuscitative management targets the immediate risk, not the personality.[1]
Acute self-harm or suicide attempt
Admission criteria — when to admit
Admit (briefly, planned) when there is:
- Suicidal intent with plan and access to means, or recent near-lethal attempt.
- Comorbid major mental illness driving risk (depression, psychosis, mania).
- Severe self-harm needing medical/surgical care.
- No safe community alternative or acute psychosocial collapse.[2]
Admission should be brief, structured, and goal-directed (typically days) — prolonged admissions in BPD can reinforce self-harm behaviour, fragment care, and iatrogenically worsen outcome. Modern UK practice (NICE) favours crisis resolution/home treatment teams over admission wherever possible.[2]
Managing splitting during the crisis
Splitting — the patient alternately idealising and devaluing individual staff, sometimes setting them against each other — is most intense during crisis. The antidote is team consistency: a single identified clinician/care coordinator, documented management plans shared across shifts, regular team meetings to agree the plan and boundaries, and a non-reciprocal, calm, boundaried stance. Avoid reacting to flattery or hostility; do not personalise; do not vary the plan in response to escalation.[1]
Management — Definitive & Stepwise
This is the section most directly tested. The non-negotiable principle: structured psychological therapy is first-line for BPD core features; medication is symptom-targeted only; benzodiazepines are avoided.[1]
Psychological therapies — the first-line evidence base
DBT (Dialectical Behaviour Therapy)
- FIRST-LINE, strongest evidence
- Developed by Linehan
- Structure: weekly individual therapy + weekly group skills training + phone coaching + therapist team meeting (1 year minimum, often 12-18 months)
- Four skills modules: MINDFULNESS, DISTRESS TOLERANCE, EMOTION REGULATION, INTERPERSONAL EFFECTIVENESS
- Dialectic: acceptance of the patient as they are + commitment to change
- Linehan 1991 RCT: reduced parasuicide, fewer & shorter admissions, less dropout vs treatment-as-usual
- Indication: chronic self-harm, affect dysregulation, suicidality
MBT (Mentalization-Based Therapy)
- Bateman & Fonagy; equivalent evidence to DBT
- Focus: rebuild capacity to understand own/others' mental states under emotional arousal
- Structure: individual + group, 18 months
- Bateman & Fonagy 2009 RCT: steeper decline in suicide attempts & hospitalisation vs structured clinical management
- Indication: relational chaos, identity disturbance, personality-level dysfunction
Schema Therapy
- Young; integrative (CBT + psychodynamic + experiential)
- Targets early maladaptive schemas and modes (abandoned/abused child, detached protector, punitive parent)
- 20+ sessions; strong emerging evidence
- Indication: deep-rooted entrenched patterns, Cluster C + BPD overlap
TFP (Transference-Focused Psychotherapy)
- Kernberg; psychodynamic, twice-weekly
- Uses the therapeutic relationship to interpret splitting and object-relations dynamics
- Indication: higher-functioning BPD, narcissistic PD
GPM (Good Psychiatric Management)
- Gunderson; less intensive, generalist-friendly
- Case management + supportive therapy + family involvement
- Comparable outcomes to DBT in trials; widely implementable
- Indication: settings without dedicated DBT/MBT programmes
Pharmacotherapy — symptom-targeted, never first-line for core traits
Affective lability, anger, impulsivity
- SSRI: fluoxetine 20-60 mg PO daily, or sertraline 50-200 mg PO daily
- Rationale: serotonergic dysregulation underlies impulsive aggression
- Consider if comorbid depression/anxiety present
- Monitor: activation, suicidality in young people
Affective instability (mood swings)
- Lamotrigine 25-200 mg PO daily (titrate slowly — Stevens-Johnson risk)
- Topiramate 50-200 mg PO daily
- Sodium valproate 500-1500 mg PO daily (AVOID in women of childbearing potential — teratogenic)
- Carbamazepine 400-800 mg PO daily (check interactions, SJS in HLA-B*1502)
- Rationale: mood-stabilisation of rapid affective shifts
Transient psychosis, severe anger, severe impulsivity
- Low-dose second-generation antipsychotic: olanzapine 2.5-10 mg PO daily, aripiprazole 5-15 mg PO daily, risperidone 0.5-2 mg PO daily
- Rationale: dopaminergic dysregulation, impulsivity, stress-induced paranoia
- Time-limited; review regularly; monitor metabolic parameters
- Avoid high-dose or long-term antipsychotic polypharmacy
Comorbid depression
- Treat as a separate Axis I disorder — SSRI first-line
- Augment with psychotherapy
- Caution: BPD patients have higher SSRI-induced activation
AVOID
- BENZODIAZEPINES (disinhibition, paradoxical agitation, dependence, overdose risk in impulsive patients)
- Long-term antipsychotic polypharmacy
- Opioids for emotional distress
Management of other specific PDs
- Antisocial PD: limited evidence for treating core traits. Address comorbid substance use (the most modifiable target), provide cognitive-behavioural programmes addressing criminal thinking, and use contingency management. No drug treats ASPD core features. Traits often attenuate with age ("burnout" by the 40s). Forensic and prison services are central.
- Narcissistic PD: long-term psychodynamic or schema therapy; manage comorbid depression with SSRIs; the alliance is fragile (anticipate devaluation).
- Avoidant PD: CBT targeting social-anxiety schemas; SSRI if comorbid social anxiety disorder (common).
- Dependent PD: CBT focusing on autonomy, decision-making, and assertiveness; address comorbid depression.
- OCPD: longer-term psychotherapy; SSRIs for comorbid depression/anxiety (the OCPD traits themselves are ego-syntonic and rarely the presenting complaint).
- Schizotypal PD: may respond to low-dose antipsychotic (e.g. risperidone) for psychotic-like symptoms; treat comorbid depression.[2]
The stepped pathway
Specific Subtypes & Scenarios
Each PD is examined in its own right. The high-yield detail per subtype:[5]
Paranoid PD
- 4 of 7 criteria
- Pervasive distrust & suspiciousness
- Bears grudges, reluctant to confide, reads hidden meanings
- Differential: delusional disorder (persecutory), paranoid schizophrenia
- Treatment: supportive/CFD therapy; low-dose antipsychotic only if transient psychosis; treat comorbid depression
Schizoid PD
- Does not desire relationships; emotional coldness/detachment
- Indifferent to praise/criticism
- Differential: avoidant (wants relationships), autism, negative-symptom schizophrenia
- Treatment: supportive therapy; address comorbid depression
Schizotypal PD
- On schizophrenia spectrum
- Odd beliefs/magical thinking, ideas of reference, unusual perceptions, odd speech
- Reality testing intact
- Treatment: low-dose antipsychotic for positive-like symptoms; social skills training; treat depression
Antisocial PD
- Conduct disorder before age 15 (mandatory)
- 3 of 7 since age 15
- Comorbid SUD common
- Treatment: CBT, contingency management, treat SUD; no drug for core traits; traits burn out with age
Borderline PD
- 5 of 9 criteria
- Highest suicide rate of the PDs
- DBT/MBT first-line
- Highest remission rate over time (McLean)
Histrionic PD
- 5 of 8 criteria
- Dramatic, attention-seeking, shallow, impressionistic speech, seductive
- Differential: BPD (deeper affect, self-harm), mania (sustained elevation)
- Treatment: psychodynamic therapy; treat comorbid depression
Narcissistic PD
- 5 of 9 criteria
- Grandiosity + need for admiration + lack of empathy (core triad)
- Fragile self-esteem; narcissistic injury → rage/dysphoria
- Treatment: long-term psychodynamic/schema therapy
Avoidant PD
- 4 of 7 criteria
- Wants relationships but fears rejection
- Differential: social anxiety disorder (often comorbid), schizoid
- Treatment: CBT; SSRI for comorbid social anxiety
Dependent PD
- 5 of 8 criteria
- Submissive, clinging, fears separation
- Differential: BPD (impulsivity, anger), agoraphobia
- Treatment: CBT for autonomy/assertiveness; treat comorbid anxiety/depression
OCPD
- 4 of 8 criteria
- EGO-SYNTONIC perfectionism, rigidity, control
- Differential: OCD (ego-dystonic), autistic rigidity
- Treatment: psychotherapy; SSRI for comorbid depression/OCD features
Complications & Pitfalls
Patient-level complications
- Suicide: BPD has the highest suicide rate of the personality disorders — modern cohort estimates are around 5-8 percent (older figures up to 10 percent are now considered too high). Suicide risk peaks in the early years of illness and is elevated by comorbid depression, substance use, and recent loss.[5]
- Repeated self-harm, accidental death, and overdose: chronic impulsivity and self-harm behaviour carry cumulative mortality.
- Comorbidity: depression, anxiety, substance use, eating disorders, PTSD, and ADHD are all common and worsen prognosis if untreated.
- Functional impairment: work instability, recurrent relationship breakdown, social isolation, homelessness.
Iatrogenic complications and pitfalls
Countertransference and clinician burnout
PD work generates strong countertransference — rescue feelings (rescuing the patient), dread, anger, or detachment. Untreated, this drives clinician burnout, inconsistent care, and splitting. Regular supervision, team meetings, and awareness of one's own reactions are protective and improve care.[1]
Prognosis & Disposition
The single most important prognostic fact for an MBBS candidate: BPD is far more treatable than its reputation suggests.[5]
The McLean Study of Adult Development (Zanarini et al.)
The landmark McLean Study prospectively followed 290 BPD inpatients for over 10 years. Key findings:[5]
- Remission was the norm, not the exception: about half had remitted by 2 years; around 88 percent achieved at least a 2-month remission over 10 years; recurrence after sustained remission was uncommon (under 10 percent).
- Symptomatic remission outpaced functional recovery: patients stopped self-harming and mood instability but often remained socially isolated, unemployed, or in dependent living arrangements.
- Predictors of earlier remission: younger age at intake, absence of childhood sexual abuse, higher agreeableness, absence of comorbid substance use.
- Predictors of poorer prognosis: comorbid substance use (the strongest negative predictor), persistent impulsivity, ongoing trauma, untreated comorbid depression.[5]
Disposition
Most PD care is outpatient — a community mental health team plus access to a structured psychotherapy programme (DBT/MBT). Crisis resolution / home treatment teams provide brief escalation in lieu of admission. Admission is reserved for high acute suicide risk, severe self-harm, or comorbid major mental illness, and should be brief and planned.[2]
Special Populations
- Adolescents: DSM-5 permits a PD diagnosis in under-18s if the features have been present for at least one year (with the exception of ASPD, which still requires age 18 plus a conduct-disorder history before 15). Use caution; traits are still developing. Early intervention services and DBT-A (an adolescent-adapted DBT) have emerging evidence for reducing self-harm in adolescents with borderline traits.[1]
- Men: BPD is under-diagnosed in men, who more often present with anger, substance use, and behavioural dyscontrol and get labelled ASPD or SUD. The diagnosis should be actively considered; men with BPD respond equally to DBT/MBT.[2]
- Pregnancy and postpartum: BPD carries increased risk of perinatal depression, relational crisis, and relapse. Risk planning before delivery is essential. Avoid teratogenic mood stabilisers — sodium valproate is contraindicated in women of childbearing potential; lamotrigine needs risk-benefit reassessment and folate; continue psychotherapy. Neonatal teams should be aware of psychotropic exposure.[2]
- Older adults: PD features often attenuate with age; BPD presentation in later life may be quieter. Assess for comorbid cognitive decline, delirium, or physical illness that can mimic or unmask personality change. Adjust medication for reduced clearance and comorbidity.[1]
- Comorbid intellectual disability: avoid diagnostic overshadowing; use informant history and behavioural analysis; rule out physical/communication triggers for behavioural disturbance.[2]
- Forensic and prison populations: ASPD and BPD are highly prevalent. Integrated mental health input within forensic services addresses comorbid SUD, depression, PTSD, and risk; purely punitive models do not change PD.[2]
- Cultural considerations: behaviours that are pathological in one culture may be normative or valued in another (e.g. emotional expressiveness, suspicion in persecuted minorities). Use the DSM-5 Cultural Formulation Interview and obtain cultural consultation; do not over-diagnose PD across cultural lines.[1]
Evidence, Guidelines & Regional Differences
Landmark trials
- Linehan 1991 RCT (Arch Gen Psychiatry) — the first RCT of a psychotherapy for BPD. DBT vs treatment-as-usual in chronically parasuicidal women with BPD showed fewer parasuicidal acts, fewer and shorter admissions, and better therapy retention. Findings on depression/hopelessness did not differ — establishing that DBT's primary benefit is on behavioural dyscontrol, not mood.[3]
- Bateman & Fonagy 2009 RCT (Am J Psychiatry) — outpatient MBT vs Structured Clinical Management (SCM) showed MBT produced a steeper decline in suicide attempts and hospitalisations and greater improvement in depression, anxiety, and social function; benefits sustained at follow-up.[4]
- The McLean Study of Adult Development (Zanarini et al.) — 10-year prospective follow-up of 290 BPD inpatients; established the high remission, slow functional recovery natural history quoted above.[5]
- Cochrane reviews of pharmacotherapy in BPD conclude that no drug treats the core disorder; modest, time-limited symptom-targeted effects only — supporting NICE's caution.[1]
Guidelines and regional deltas
NICE CG78 (UK, 2009, reaffirmed)
- Psychological therapy (DBT or MBT or equivalent) is the primary treatment for BPD
- Do NOT use medication specifically for core BPD or ASPD features
- Use medication briefly for comorbid conditions or severe symptom targets
- Brief, planned admissions; prefer crisis resolution/home treatment teams
- Multidisciplinary, integrated care
DSM-5 (US)
- Categorical 10-PD model (Section II) — primary
- Alternative Model (AMPD, Section III) — dimensional severity + 5 trait domains
- Pharmacotherapy more commonly used in US practice than NICE endorses
ICD-11 (UK/global)
- Abandons most categorical PDs
- Severity rating (mild/moderate/severe/personality difficulty)
- Five trait qualifiers + borderline pattern qualifier
- Encourages dimensional formulation
Indian Psychiatric Society
- Aligns broadly with DSM-5 categorical model
- Emphasises cultural sensitivity in PD diagnosis
- Limited availability of dedicated DBT/MBT programmes — pragmatic use of available structured therapy
Controversies
- The "borderline-bipolar" overlap — BPD and bipolar II share affective instability, impulsivity, and risk behaviours; the tempo/trigger distinction (BPD reactive, minutes-hours; bipolar spontaneous, days-weeks) remains the clinical discriminator. They can coexist.[2]
- The 10 percent BPD suicide figure — modern cohort data suggest the true figure is closer to 5-8 percent; older figures reflected severe inpatient cohorts. The figure should be quoted with this caveat.[5]
- Categorical vs dimensional classification — the field is moving toward dimensional models (AMPD, ICD-11); DSM-5-TR retains the categorical model for clinical use while Section III carries the dimensional alternative.[1]
- Adolescent diagnosis — whether BPD can/should be diagnosed under 18 is contested; current consensus permits it with the 1-year rule, recognising that earlier detection enables earlier effective intervention.[1]
Exam Pearls
CLUSTERS
I DESPAIR
Exam application bank (NEET-PG / INICET)
One-line answer
Personality disorders (PD) are enduring, inflexible, and pervasive patterns of inner experience and behaviour that deviate markedly from the expectations of the individual's culture, are stable over time, begin by adolescence or early adulthood, lead to distress or impairment, and are not better explained by another mental disorder, substance use, or a medical condition. DSM-5 groups them into three clusters: Cluster A (odd, eccentric) — paranoid, schizoid, schizotypal; Cluster B (dramatic, emotional, erratic) — antisocial, borderline, histrionic, narcissistic; Cluster C (anxious, fearful) — avoidant, dependent, obsessive-compulsive (OCPD). Borderline personality disorder (BPD) is the most clinically important and most examined: frantic efforts to avoid abandonment, unstable intense relationships, identity disturbance, impulsivity, recurrent self-harm/suicidal behaviour, affective instab
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard.[1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes.[1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change.[1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each.[2]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory.[1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Personality Disorders.
[1]References
- [1]Leichsenring F, Fonagy P, Heim N, et al. Borderline personality disorder: a comprehensive review of diagnosis and clinical presentation, etiology, treatment, and current controversies. World Psychiatry, 2024.PMID 38214629
- [2]Paris J. Differential Diagnosis of Borderline Personality Disorder. Psychiatric Clinics of North America, 2018.PMID 30447725
- [3]Linehan MM, Armstrong HE, Suarez A, Allmon D, Heard HL. Cognitive-behavioral treatment of chronically parasuicidal borderline patients. Archives of General Psychiatry, 1991.PMID 1845222
- [4]Bateman A, Fonagy P. Randomized controlled trial of outpatient mentalization-based treatment versus structured clinical management for borderline personality disorder. American Journal of Psychiatry, 2009.PMID 19833787
- [5]Zanarini MC, Frankenburg FR, Hennen J, Silk KR. Prediction of the 10-year course of borderline personality disorder. American Journal of Psychiatry, 2006.PMID 16648323