Psychiatry · Psychiatry
Somatic Symptom Disorder & Related Disorders
Also known as Somatic symptom disorder (SSD) · Illness anxiety disorder · Hypochondriasis · Conversion disorder · Functional neurological symptom disorder (FND) · Psychological factors affecting medical condition · Factitious disorder · Health anxiety · Medically unexplained symptoms
The somatic symptom and related disorders (SSRD) are a DSM-5-TR cluster defined by EXCESSIVE thoughts, feelings, and behaviours related to somatic symptoms or health concerns, NOT by absence of disease. Somatic Symptom Disorder (SSD): one or more distressing somatic symptoms plus disproportionate concern, persistent health anxiety, or excessive time/energy devoted to symptoms for at least 6 months. Illness Anxiety Disorder (IAD, hypochondriasis): preoccupation with having or acquiring a serious illness with minimal/no somatic symptoms. Conversion/FND: motor or sensory symptoms incompatible with recognised neurological disease, NOT consciously produced. Factitious = falsification/induction for the sick role; malingering = feigning for external gain. Pathophysiology: catastrophic misinterpretation of bodily sensation in a hyperactivated interoceptive network (anterior insula + ACC), reinforced by checking/reassurance/avoidance. Diagnosis is clinical (use PHQ-15 and Whiteley-7), with targeted (not shotgun) investigations. Management: CBT first-line, antidepressants (SSRIs even without depression), regular scheduled GP visits, single medical home, AVOID repeated unnecessary tests and opioids. ALWAYS reassess an acute change in a known SSD patient for genuine new disease.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Exam tags
Red flags
Overview & Definition
The somatic symptom and related disorders (SSRD) sit at the fault line between medicine and psychiatry, and they are among the most common, most costly, and most poorly understood presentations in clinical practice. Up to 20–50% of primary-care consultations involve medically unexplained somatic symptoms, and these patients are among the highest utilisers of healthcare resources, with repeated investigations, multiple specialist referrals, and frequent emergency-department attendances.[3][6]
The conceptual revolution in DSM-5 (2013, refined in DSM-5-TR 2022) was to abandon the requirement that symptoms be "medically unexplained." The disorders are now defined by the maladaptive cognitive, affective, and behavioural responses to bodily symptoms or health concerns — not by the absence of a medical disease. A patient with genuine ischaemic heart disease can still be diagnosed with SSD if their concern, anxiety, and time/energy devoted to cardiac symptoms are disproportionate and persistent. This single shift reframes the disorder from a wastebasket of exclusion ("we can't explain it, so it must be psychiatric") to a positive diagnosis of a treatable neuropsychiatric syndrome.[5][1]
The clinical skill in this cluster is to (1) recognise the positive diagnostic pattern, (2) validate the patient's distress ("these symptoms are real"), (3) avoid repeated unnecessary investigations (each normal result provides only transient reassurance and reinforces the illness behaviour cycle), (4) establish a single medical home with regular scheduled appointments regardless of symptoms, (5) deliver evidence-based treatment (CBT, antidepressants, and — for FND — specialist physiotherapy), and (6) keep a genuine medical eye on the patient so a new organic illness is never missed under the label 'functional'.[2][1]
Classification
The DSM-5-TR cluster of Somatic Symptom and Related Disorders contains six distinct entities, distinguished along four axes: (a) the presence and prominence of somatic symptoms, (b) the cognitive/affective/behavioural profile, (c) whether symptoms are consciously produced, and (d) whether there is external incentive.[5]
Somatic Symptom Disorder (SSD)
- Criterion A: ≥1 distressing somatic symptoms
- Criterion B: excessive thoughts/feelings/behaviours (disproportionate concern, persistent high health anxiety, or excessive time/energy)
- Criterion C: persistent ≥6 months
- Symptoms NEED NOT be medically unexplained — SSD can co-exist with genuine medical disease
- Commonest of the cluster (~5–7% lifetime prevalence)
Illness Anxiety Disorder (IAD)
- Preoccupation with HAVING or ACQUIRING a serious illness
- Somatic symptoms ABSENT or MILD
- High health anxiety; excessive health-related behaviours (checking, doctor-shopping, internet) OR maladaptive avoidance
- Persistent ≥6 months; not better explained by another disorder
- Two subtypes: care-seeking vs care-avoidant
Conversion / Functional Neurological Symptom Disorder (FND)
- ≥1 altered voluntary motor or sensory symptom
- Clinical findings show incompatibility with recognised neurological/medical disease (positive signs, e.g. Hoover)
- Symptom NOT consciously produced (key distinction from factitious/malingering)
- Causes distress/impairment
- Subtypes: weakness/paralysis, abnormal movement, swallowing/speech, attacks/seizures, sensory loss, mixed, dissociative
Psychological Factors Affecting Medical Condition (PFAMC)
- A diagnosed general medical condition is adversely affected by psychological/behavioural factors
- Examples: stress-exacerbated asthma, non-adherence worsening diabetes, anxiety amplifying IBD
- The medical condition is REAL; the psych factors worsen it
- Distinct from SSD (which is a primary psychiatric diagnosis)
Factitious Disorder
- Falsification or induction of physical/psychological signs/symptoms
- Intent to deceive; inducing factors evident
- Motive is INTERNAL — assumption of the sick role (no external reward)
- Subtypes: imposed on self (Munchausen), imposed on another (Munchausen by proxy / Fabricated or Induced Illness)
- Consciously produced — distinguishes from conversion
Malingering (NOT a mental disorder)
- Intentional production of false or grossly exaggerated symptoms
- Motivation is EXTERNAL incentive (money, opioid drugs, paid leave, avoiding prosecution, shelter)
- Not a DSM/ICD mental disorder — it is a behaviour
- Suspect when there is clear external incentive + inconsistency on examination
The terminology is itself examinable. The ICD-11 (effective 2022) uses the umbrella term Bodily Distress Disorder (BDD) for the equivalent construct, and the Lancet 2024 review by Löwe and colleagues advocates the broader term persistent physical symptoms to capture the dimensional, transdiagnostic nature of these presentations.[1]
The numbers examiners reward
Epidemiology & Risk Factors
Somatic symptom and related disorders are common across all cultures and all healthcare settings, but their shape is shaped by both biology and the cultural interpretation of distress.[1][6]
Lifetime prevalence is approximately 5–7% for SSD in the general population and 1.3–10% for IAD depending on setting (higher in medical specialty clinics, cardiology, neurology). Conversion disorder / FND has an incidence of roughly 4–12 per 100,000 per year in population studies, rising to 5–10% of neurology outpatient populations. The female-to-male ratio is approximately 2:1 for SSD and conversion; IAD is roughly equal between sexes.[7]
Onset is typically in adolescence to early adulthood; conversion peaks in late adolescence/young adulthood. New-onset conversion after age 50 is uncommon and warrants especially careful exclusion of organic disease (stroke, MS, motor neuron disease, paraneoplastic syndromes).[7]
Risk factors cluster into the classic 3-P framework (Predisposing, Precipitating, Perpetuating) that is itself examinable: [1]
Predisposing (diathesis)
- Childhood adversity — abuse, neglect, parental illness or somatisation (somatic learning model)
- Alexithymia — difficulty identifying and describing emotions
- Female sex
- Lower educational / socioeconomic status
- Health-anxious personality trait
- Genetic loading — heritability of somatisation ~20 to 30 percent
- Family modelling of illness behaviour
Precipitating (trigger)
- Recent physical illness or injury (even minor)
- Major life stressor — bereavement, divorce, job loss
- Frightening health-related event (relative's sudden cardiac death)
- False-positive screening test, a 'health scare'
- Surgical procedure / anaesthetic
- Recent infection (e.g. post-COVID syndrome)
Perpetuating (maintenance)
- Iatrogenic reinforcement — each unnecessary test/reassurance 'rewards' illness behaviour with transient relief that fades
- Avoidance — prevents disconfirmation of catastrophic belief
- Secondary gain — tangible benefits of the sick role
- Comorbid depression and anxiety (lower pain threshold, more somatic focus)
- Substance use (opioids, benzodiazepines)
- Stigma and clinician frustration — cycle of disengagement
Cultural epidemiology and culture-bound syndromes are high-yield and examinable. The cluster has distinctive cultural expressions that are not simply SSD but overlap with it: [1]
- Dhat syndrome (India and South Asia) — excessive concern about semen loss in urine, with weakness, fatigue, sexual dysfunction; listed in ICD-10 (F48.0) and recognised in DSM-5-TR's cultural concepts of distress. Treated with sex education, CBT, and SSRI where depression comorbid.
- Kufungisisa ("thinking too much") — Zimbabwean cultural expression of distress overlapping with anxiety-depression and somatic symptoms; listed in DSM-5-TR.
- Taijin kyofusho (Japan) — fear of giving offence through one's appearance or body odour (a culture-relative variant of social/body-dysmorphic anxiety).
- Brain fag (West African students) — somatic symptoms of cognitive exhaustion (headache, neck pain, blurred vision) under study pressure.
- Ataque de nervios (Latin America) — episodes of shouting, trembling, dissociation, often after family stressor; overlaps with conversion/dissociation.
- Kayak angst (Inuit) — dissociative panic during hunting. [1]
Comorbidity is the rule rather than the exception: 50–80% of SSD patients have a comorbid depressive or anxiety disorder, personality disorders (cluster B borderline, histrionic; cluster C) are common, and substance use disorders (alcohol, analgesics) frequently complicate chronic presentations. The bidirectional relationship between mood and somatic symptoms is itself part of the pathophysiology — treating one often improves the other.[1]
Pathophysiology
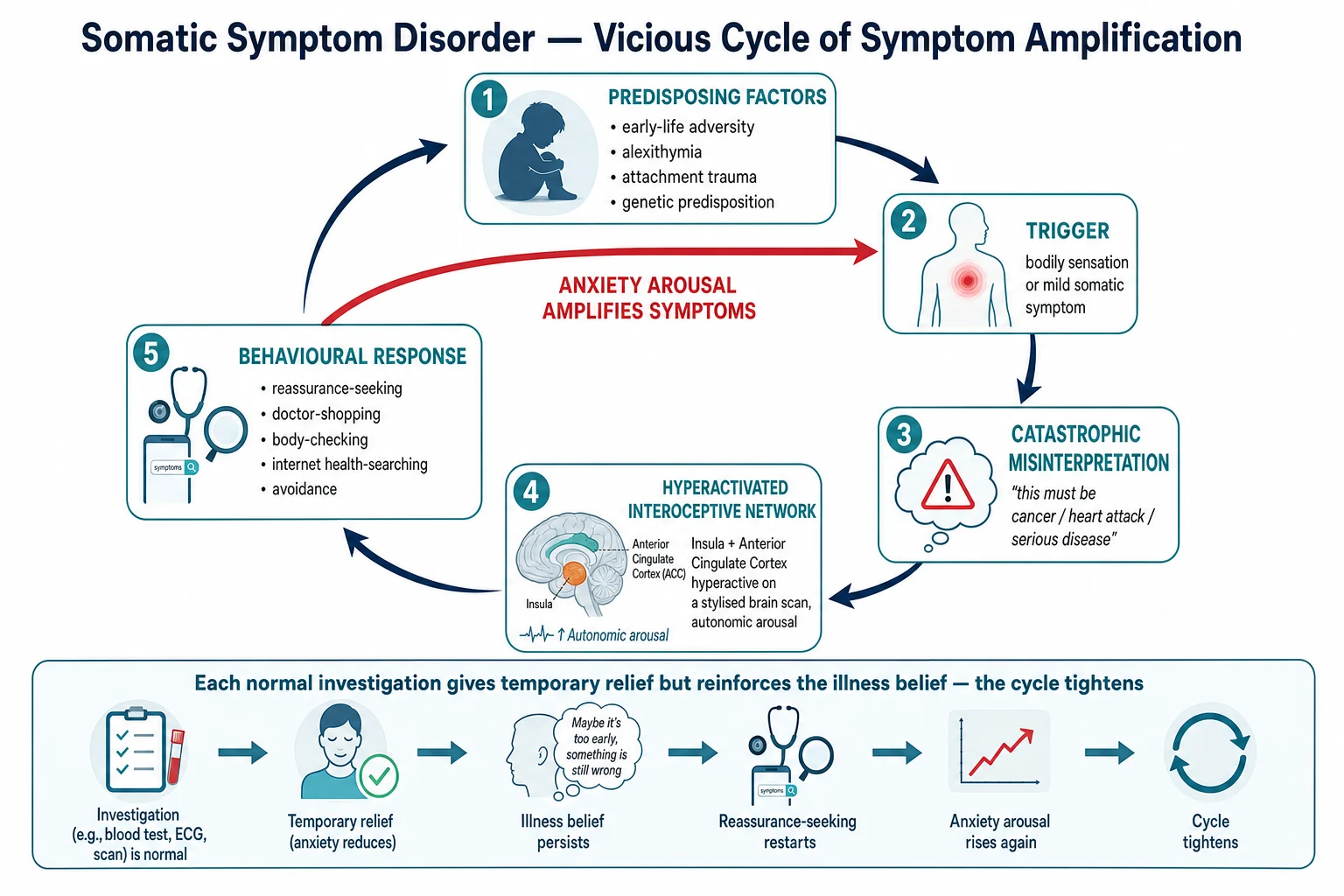
The SSRD are best understood through an integrated cognitive-behavioural + neurobiological model. There is no single lesion; the disorder arises from a maladaptive interaction between predisposing vulnerability, triggering events, amplifying cognitive appraisal, hyperactive brain networks, and reinforcing behaviours.[1][2]
The cognitive-behavioural model (Salkovskis & Warwick)
The dominant theoretical model, and the one CBT targets, is the cognitive-behavioural cycle: [1]
- A bodily sensation arises (often a normal physiological event — bowel peristalsis, a premature atrial beat, muscle tension).
- The patient catastrophically misinterprets the sensation ("the chest twinge is a heart attack," "the stomach rumble is cancer," "the headache is a brain tumour").
- Anxiety is generated.
- Anxiety drives autonomic arousal (palpitations, sweating, muscle tension, hyperventilation), which generates more physical sensations — the body feeds the cycle physiologically.
- The patient engages in safety behaviours — checking the body, seeking reassurance, doctor-shopping, internet searching, avoiding activity — each of which reduces anxiety only transiently and reinforces the illness belief.
- The cycle tightens with each revolution; symptoms intensify and generalise.[2]
The interoceptive network: the neurobiology of amplification
Functional MRI studies show consistent hyperactivity of the anterior insula and anterior cingulate cortex — the brain's interoceptive (body-state mapping) and salience networks. The anterior insula constructs a moment-to-day map of internal body state; when it is hyperactive, normal sensations are detected and amplified — the somatic spotlight phenomenon. Directing attention to a body part lowers the threshold for symptom perception (try attending to your breathing now).[1]
Somatosensory amplification is the perceptual correlate: the patient experiences normal or mild sensations as intense, distressing, and threatening. This is not conscious exaggeration — the brain genuinely registers the signal as louder. [1]
Predisposing, precipitating, and perpetuating — the 3 Ps
Predisposing → Precipitating → Perpetuating (the formulation framework)
THE 3 Ps
Childhood adversity, alexithymia, attachment trauma, family illness modelling, genetic loading (diathesis that lowers threshold)
Trigger: bodily sensation, physical illness/injury, life stressor, bereavement, health scare, surgery
Maintenance: iatrogenic reinforcement (unnecessary tests), avoidance, secondary gain, comorbid mood/anxiety, opioid/benzo use
The psychodynamic perspective and conversion
For conversion disorder / FND, the psychodynamic tradition (Freud, Janet) framed symptoms as the somatosensory expression of unresolved psychic conflict — the painful affect is "converted" into a physical symptom. Primary gain = intrapsychic relief (the conflict is banished from consciousness); secondary gain = tangible external advantages of the sick role (avoiding work, family attention). Modern neuropsychiatric models retain the formulation but emphasise functional disconnection between motor-programming and conscious-awareness circuits, rather than repression.[7]
Why conversion symptoms are real
This is exam-critical: conversion symptoms are NOT feigned. The patient genuinely experiences the weakness, the blindness, the seizure. Motor programmes and conscious awareness are dissociated. La Belle Indifférence — the apparent lack of distress about a severe deficit, classically described by Charcot — is present in only ~30% of cases and is neither universal nor diagnostic.[7]
Clinical Presentation
There is no single presentation; the cluster presents across the entire symptom spectrum. What unites the presentations is the pattern: a distressing symptom, persistent health anxiety or illness behaviour, functional impairment, and a trajectory of repeated normal investigations and multiple specialist contacts.[2]
Somatic Symptom Disorder (SSD)
Patients present with one or more recurrent somatic symptoms — typically pain (chest, back, abdominal, pelvic, headache), gastrointestinal (bloating, nausea, IBS-like symptoms, abdominal pain), cardiovascular (palpitations, chest tightness), or neurological (headache, dizziness, fatigue) — that are distressing and persistent for at least 6 months, accompanied by excessive thoughts, feelings, or behaviours (the B-criterion): [1]
- Disproportionate thoughts about the seriousness of the symptoms ("this stomach pain must be pancreatic cancer").
- Persistent high level of anxiety about health or symptoms (constant vigilance, frequent checks).
- Excessive time and energy devoted to the symptoms or health concerns (multiple doctor visits, hours daily on health websites, repeated testing). [1]
The patient typically has a thick medical record of multiple normal investigations, multiple specialist referrals, and frequent healthcare contacts. They may be on multiple medications including analgesics, PPIs, and anxiolytics. They often describe being dismissed or disbelieved by previous clinicians, and the therapeutic relationship may already be strained.[1]
Illness Anxiety Disorder (IAD, hypochondriasis)
Patients are preoccupied with the idea of having or acquiring a serious illness — most commonly cancer, heart disease, HIV, ALS, or dementia. Somatic symptoms are absent or mild. Two behavioural subtypes: [1]
- Care-seeking type — frequent doctor visits, demands for tests and scans, repeated internet searching, body-checking (lumps, rashes, temperature, blood pressure); reassurance produces only transient relief.
- Care-avoidant type — avoids doctors, hospitals, health information, and even thinking about illness; fears that any contact will confirm the dreaded diagnosis.[4]
Conversion / Functional Neurological Symptom Disorder (FND)
A positive diagnosis is made on incompatible clinical findings, not on exclusion. Presentations include:[7]
- Motor — limb weakness or paralysis; tremor; dystonia; myoclonus; gait abnormality (knee-buckling, dragging); functional (spasmodic) dysphonia; aphonia; stuttering.
- Sensory — patches of anaesthesia (often midline-splitting, not respecting dermatomes); blindness; deafness; tunnel vision (tubular, constricted concentrically, which is physiologically impossible in organic disease).
- Episodic — dissociative (non-epileptic) seizures (PNES) — see below.
- Mixed — combinations of the above. [1]
Dissociative (non-epileptic) seizures — distinguishing features
Dissociative (non-epileptic) seizure
- Eyes CLOSED (resists passive opening)
- Asynchronous, out-of-phase thrashing; pelvic thrusting
- Side-to-side head movement; large-amplitude movements
- Crying, weeping, vocalisation during event
- Recall of event; may resist tongue depressor
- No postictal confusion; rapid recovery
- No tongue biting, urinary incontinence, or injury typical of epilepsy
- Occurs in wakefulness; stop with distraction/no-stimulation
- Video-EEG: NO epileptiform activity during event
Epileptic (generalised tonic-clonic) seizure
- Eyes OPEN
- In-phase, rhythmic tonic then clonic activity
- Stereotyped; cyanosis common
- Amnesia for event; cannot recall
- Postictal confusion, drowsiness;Todd's paresis
- Tongue biting (lateral edge), urinary incontinence, fall injury common
- EEG during event shows epileptiform activity
- Stereotyped, brief (under 2 minutes)
Psychological Factors Affecting Other Medical Condition (PFAMC)
A patient with a diagnosed medical condition — diabetes, asthma, IHD, COPD, IBD — whose illness course is adversely affected by psychological or behavioural factors. The three commonest patterns: non-adherence (insulin omission, missed inhalers), stress-exacerbation (anxiety driving asthma attacks or IBD flares), and health-anxiety amplification (cardiac phobia after an MI). [1]
Factitious disorder and malingering — the deception axis
- Factitious disorder — the patient falsifies or induces symptoms (e.g. contaminating urine samples, injecting insulin to cause hypoglycaemia, heating thermometers, inducing wounds). The motive is internal — assumption of the sick role. Munchausen syndrome = chronic, severe, with peregrination (wandering between hospitals). Munchausen by proxy (now "Factitious Disorder Imposed on Another" / Fabricated or Induced Illness, FII) — a caregiver induces illness in a dependent (usually a child); this is child abuse and must be reported.
- Malingering — intentional production of false or exaggerated symptoms for external incentive (financial compensation, opioid drugs, paid leave, avoiding military service or prosecution). Not a mental disorder; suspected when there is clear external incentive + inconsistency on examination. [1]
Atypical presentations
- Elderly — health anxiety often intensifies with normal ageing and bereavement; new-onset somatisation is uncommon and warrants careful exclusion of depression, dementia, delirium, polypharmacy side effects, and vitamin deficiencies (B12, D). Avoid over-investigation; SSRIs at half starting dose.
- Pregnancy/postpartum — foetal-focused illness anxiety (worry about congenital anomaly), hyperemesis as a somatic focus, postnatal depression with somatic features; sertraline preferred SSRI in pregnancy (lowest fetal risk); avoid benzodiazepines and paroxetine in first trimester.
- Children/adolescents — common presentations are recurrent abdominal pain, headache, fatigue, school avoidance, and pseudoseizures; strong association with family illness modelling and school stressor; family-based CBT; prognosis often better than adults.
- Cultural syndromes — Dhat, Kufungisisa, Brain fag, Ataque de nervios, Taijin kyofusho — see Epidemiology; a culturally-informed formulation is essential.
- Post-COVID syndrome — persistent fatigue, breathlessness, "brain fog" following COVID-19; overlaps with SSD; requires validation, paced rehabilitation, screening for depression/anxiety, and explicit avoidance of dismissing as "all in the head."
- Intellectual disability / autism — SSD-like presentations common; adapt assessment (visual aids, concrete language); exclude comorbid physical disease; involve carers. [1]
Differential Diagnosis
The differential has two layers: (1) distinguish the SSRD cluster from organic disease (always rule out first), and (2) distinguish within the psychiatric and behavioural differential.[2][6]
Layer 1: organic disease (always exclude first)
| Presenting symptom | Organic differential to actively exclude |
|---|---|
| Chest pain | Ischaemic heart disease, PE, aortic dissection, pericarditis, oesophageal spasm |
| Neurological deficit | Stroke, TIA, MS, motor neuron disease, myasthenia, Guillain-Barré, spinal cord compression |
| Seizure | Epilepsy, syncope, hypoglycaemia, cardiac arrhythmia |
| Weakness | Myasthenia, MND, polymyositis, electrolyte disturbance |
| Abdominal pain | IBD, peptic ulcer, biliary disease, malignancy, mesenteric ischaemia |
| Fatigue | Hypothyroidism, anaemia, malignancy, chronic infection, autoimmune disease |
| Headache | Migraine, space-occupying lesion, temporal arteritis, idiopathic intracranial hypertension |
The rule of thumb: an acute change, a new objective sign, weight loss, fever, night sweats, neurological dysfunction, or a symptom inconsistent with the established pattern warrants genuine reassessment.[1]
Layer 2: psychiatric and behavioural differential
Major depressive disorder with somatic symptoms
- Depressed mood and anhedonia are PRIMARY
- Sleep, appetite, libido, energy disturbance
- Somatic symptoms are part of melancholic syndrome
- Treat mood first — somatic symptoms often improve
- Bidirectional: 50 to 80 percent of SSD patients have comorbid depression
Generalised anxiety disorder (GAD)
- Worry is BROAD (work, family, finances, future) — not health-specific
- IAD worry is health-specific
- Both may coexist; treat the GAD too
- Sleep disturbance, muscle tension, fatigue, irritability
Panic disorder
- DISCRETE acute attacks (10 minutes) with autonomic features
- Anticipatory anxiety between attacks
- IAD = chronic low-grade health worry without discrete attacks
- May overlap: panic attacks drive illness anxiety in some patients
Hypochondriacal delusion (psychosis/depression)
- FIXED false belief of disease, often bizarre ('my organs are rotting', 'I am dead - Cotard')
- Unshakeable despite all evidence
- Not amenable to CBT; treat underlying psychosis/depression with antipsychotic/antidepressant
- IAD = overvalued idea, not delusional
OCD with illness obsessions
- Recognised as ego-DYSTONIC, resisted
- Compulsive rituals (counting, checking)
- Insight relatively preserved
- IAD health behaviours are ego-SYNTONIC ('I really am at risk')
Body dysmorphic disorder
- Preoccupation with perceived DEFECT in APPEARANCE (nose, skin, hair)
- Not internal disease or function
- Repetitive mirror-checking, grooming, comparison
- SSRI first-line; CBT with exposure and response prevention
The high-yield distinction: SSD/conversion vs factitious vs malingering
| Feature | SSD / Conversion / FND | Factitious | Malingering |
|---|---|---|---|
| Consciously produced? | No | Yes | Yes |
| Motive | None (distress is real) | Internal — sick role | External — money, drugs, leave, avoiding prosecution |
| External incentive | Absent | Absent | Present |
| Classification | Mental disorder (DSM/ICD) | Mental disorder (DSM/ICD) | NOT a mental disorder |
| Disclosure under anaesthesia | Symptoms persist | Symptoms resolve | Symptoms may resolve |
| Typical pattern | Doctor-shopping, thick chart, repeated normal tests | Wandering (peregrination), atypical presentation, induced findings | Coincides with external incentive (litigation, claim, court date) |
Clinical & Bedside Assessment
The diagnosis is clinical. There is no blood test or scan for SSD. The skill is in listening for the pattern, eliciting illness behaviour, performing a focused (not shotgun) examination, and applying named clinical signs for suspected FND.[2]
The history
- Symptom onset and evolution — context, timing, course, precipitants.
- Illness behaviour — number of doctor visits in past year, internet health-searching hours, body-checking, reassurance-seeking pattern.
- Healthcare utilisation — number of investigations, hospital admissions, specialist referrals, current medications.
- Psychosocial stressor — recent life event, bereavement, relationship breakdown, financial stress, work problems.
- Childhood adversity — abuse, neglect, parental illness, family somatisation modelling.
- Family history — of anxiety, depression, somatisation.
- Comorbid mood/anxiety — screen for depression (PHQ-9), anxiety (GAD-7).
- Cultural background — culturally-shaped expressions of distress (Dhat, Kufungisisa, etc.).
- Insight and engagement — willingness to consider psychological contribution. [1]
Functional analysis of the symptom (A-B-C)
- A (Antecedent) — what was happening just before? (stressor, sensation, situation).
- B (Behaviour) — what does the patient do in response? (checking, avoiding, calling doctor).
- C (Consequence) — what happens? (attention, time off work, relief that fades, anxiety that rises). [1]
Mental State Examination
- Appearance/behaviour — often anxious, vigilant, may bring large folders of test results, may appear tense or preoccupied.
- Speech — typically normal; may be slow or circumstantial around symptom detail.
- Mood — anxious, low, or incongruously blunted (La Belle Indifférence in FND).
- Thought — preoccupation with illness; catastrophic cognitions ("this must be cancer"); overvalued ideas (not delusional) in IAD.
- Perception — usually normal; dissociation may occur in conversion.
- Insight — often partial; may resist psychological framing.
- Judgement — variable. [1]
Functional neurological examination signs (positive diagnostic signs for FND)
These are positive signs of incompatibility, not negative signs of exclusion. Their presence supports an FND diagnosis when combined with the clinical pattern. [1]
Positive signs of functional neurological disorder
FND SIGNS
Hip extension weakness in paralysed limb REAPPEARS when testing the contralateral hip flexion (complementary limb movement)
'Collapse' weakness on initial testing that becomes strong with sustained effort — different from organic true weakness
Functional tremor ENTRAINS to the rhythm of contralateral repetitive tapping; organic tremor does not
Sensory loss splits at the MIDLINE (does not respect dermatomes) — sensory loss 'on the half of the body'
Vertigo with no nystagmus, or nystagmus that does not fatigue or reverse on caloric testing
Knee-buckling on stance without falls (paradoxical: very unstable gait but no injury)
Tubular/tunnel vision that does not expand with distance — physiologically impossible in organic disease
Functional aphonia with preserved cough and normal vocal cord movement on indirect laryngoscopy
The Hoover sign is the single highest-yield clinical sign in conversion/FND: with the patient supine, place your hand under the heel of the "weak" leg and ask them to lift the good leg against resistance. In organic weakness, the paralysed leg pushes down into your hand (complementary extensor response). In functional weakness, the heel does NOT push down — the complementary limb movement is absent, but reappears when you test extension of the affected limb directly. [1]
Validated screening scales — reproduced
PHQ-15 (Patient Health Questionnaire-15) — 15 somatic symptom items, each scored 0 (not bothered at all), 1 (bothered a little), 2 (bothered a lot). Cut-points: 5–9 mild, 10–14 moderate, 15–30 severe somatic symptom severity.[6]
Items cover the commonest somatic presentations: stomach pain, back pain, pain in arms/legs/joints, menstrual cramps/pain (women), headaches, chest pain, dizziness, fainting spells, heart pounding/racing, shortness of breath, constipation/loose stools/diarrhoea, nausea/gas/indigestion, feeling tired/low energy, trouble sleeping, low interest in sex. (Menstrual item omitted in men, scored as 0; total adjusted to 30.) [1]
Whiteley-7 scale (illness worry) — 7 items from the Whiteley Index, scored on a 5-point Likert; a cut-off of ≥3 positive items screens for illness anxiety disorder.[4]
SSD-12 (Somatic Symptom Disorder–B Criteria Scale) — 12 items measuring the B-criterion (excessive thoughts, feelings, and behaviours); useful for documenting SSD severity and tracking response. [1]
Bedside assessment of risk
- Suicide risk — comorbid depression raises suicide risk; chronic pain and opioid access raise overdose risk. Assess formally (see suicide-risk-assessment topic).
- Risk of iatrogenic harm — number of investigations, polypharmacy, opioid/benzodiazepine use.
- Functional impairment — work, relationships, mobility, self-care.
- Risk of disengagement — past pattern of dropping out of care; stigma. [1]
Investigations
The principle of investigation in SSRD is targeted, time-limited, and clinically indicated — not "shotgun workup." Each test should answer a specific clinical question. Routine reassurance-driven repeat testing is harmful: each normal result provides only transient relief that fades, and reinforces the patient's belief that the next test might find something, locking the vicious cycle tighter.[2][1]
Baseline screen (one-time, comprehensive)
To exclude occult disease and comorbidity, and to provide a baseline that supports a positive (not exclusionary) diagnosis: [1]
- Full blood count, ESR/CRP — anaemia, inflammation, infection.
- Urea & electrolytes, liver function tests — renal/hepatic disease.
- Thyroid function (TSH) — exclude hyperthyroidism (anxiety, palpitations) or hypothyroidism (fatigue, depression).
- Fasting glucose, HbA1c — diabetes.
- Vitamin B12, folate, vitamin D — deficiency mimics fatigue and somatic complaints, especially in elderly.
- Urinalysis — infection, diabetes, renal disease.
- ECG if any cardiac symptoms (palpitations, chest pain). [1]
Targeted investigations by presentation
| Presentation | Targeted investigation |
|---|---|
| Chest pain | ECG, troponin (if appropriate), consider CT coronary / angiography; rule out ischaemic heart disease |
| Seizure | Video-EEG monitoring; MRI brain; prolactin (rises after generalised tonic-clonic seizure, not PNES) |
| Focal neurological deficit | MRI brain and spine; rule out stroke, MS, MND |
| GI symptoms | Faecal calprotectin; coeliac serology; targeted endoscopy if red flags |
| Fatigue | TFT, FBC, ferritin, B12, HIV, viral hepatitis; sleep study if OSA suspected |
| Headache | Neuroimaging if red-flag features (new, focal, progressive, worst-ever, systemic) |
Investigations to AVOID or limit
- Repeated "defensive" investigations to reassure — explicitly harmful.
- Whole-body scans without clinical indication — high rate of incidental findings that fuel further spirals.
- Repeated troponin/ECG in a patient with established non-cardiac chest pain.
- Repeated EEGs without new clinical features.
- Invasive procedures (angiography, endoscopy) without clear clinical indication. [1]
Document explicitly: "Tests are not being repeated because they are clinically unnecessary and would reinforce the illness cycle; a clear plan is in place if symptoms change." [1]
Functional neurological disorder workup
- A single neurology assessment by a clinician trained in FND (positive signs, not just exclusion).
- Video-EEG monitoring for suspected dissociative seizures — capturing an event with no epileptiform activity is diagnostic.
- MRI brain where focal signs raise concern for stroke/MS.
- Rule in by positive clinical signs (Hoover, entrainment, midline sensory split) rather than by extensive imaging. [1]
Management — Resuscitation

SSD is rarely an acute emergency, but several acute scenarios require urgent, structured care:[2]
- Acute severe conversion (e.g. dissociative seizure, functional coma): ABCDE assessment first. For dissociative seizures, ensure airway safety, place in recovery position, do NOT routinely give IV benzodiazepines (risk of respiratory depression, reinforces illness behaviour, masks the diagnosis). Most episodes self-terminate within minutes. Reassure calmly, reduce stimulation (bystanders, lights, noise).
- Suicide risk or overdose in a patient with comorbid depression: formal suicide risk assessment; treat the overdose medically; urgent psychiatric review; do not discharge without psych review.
- Acute medical emergency mislabelled 'functional': a patient with known SSD who develops genuine chest pain, focal deficit, or seizure-like activity MUST be assessed for new organic disease (vital signs, focused examination, clinically-indicated tests) before any assumption of functional cause.
- Severe agitation/distress: de-escalation, calm environment, address any precipitating stressor; short-acting benzodiazepine only if severe and short-term, with explicit care given dependence and withdrawal risk. [1]
Management — Definitive & Stepwise
Treatment is multimodal, stepped, and long-term. The evidence base supports CBT first-line, antidepressants (especially SSRIs), specialist physiotherapy for FND, and structured primary-care follow-up.[1][2]
Universal principles (apply to ALL SSRD patients)
The eight universal principles of SSD management
VALIDATE
Symptoms are REAL; do not dismiss. ('I believe your symptoms; they are distressing.')
Build a therapeutic alliance; consistent clinician; trust over time
Avoid REPEATED unnecessary investigations — each reinforces illness behaviour
Single medical home / consistent clinician coordinates care, reduces fragmentation
Regular SCHEDULED appointments every 2 to 4 weeks REGARDLESS of symptoms — containment, reduces ER
Shift focus from disease-finding to symptom management and functional improvement
Treat depression and anxiety aggressively — often improves somatic symptoms
Shared understanding of the disorder (the 'faulty alarm' explanation); collaborative goals
The consultation script (when no disease is found)
When the workup is negative, the consultation matters more than any test. A four-step script works well: [1]
- Acknowledge and validate — "Your symptoms are real and distressing."
- Give a positive diagnostic label — "This is functional neurological disorder / somatic symptom disorder / recurrent bodily distress. It's a recognised condition with a name and a treatment."
- Explain with a shared model — "Think of your nervous system like a faulty alarm — it's sounding even though there's no fire. The signal is real, but the wiring needs retraining."
- Set collaborative functional goals — "Together we'll work on improving your function, sleep, mood, and activity — not chasing another test." [1]
First-line psychological treatment: CBT
Cognitive Behavioural Therapy is the most evidence-based intervention for SSD, IAD, and FND. 8–16 sessions with a trained therapist. Components:[8]
- Psychoeducation — the vicious-cycle model.
- Cognitive restructuring — challenging catastrophic illness beliefs ("the headache means brain tumour").
- Behavioural experiments — reducing safety behaviours (checking, body-scanning, internet).
- Graded return to activity — re-introducing avoided activities.
- Attention retraining — shifting the somatic spotlight.
- Sleep, relaxation, and stress management. [1]
Cochrane reviews and multiple meta-analyses confirm CBT reduces symptom severity, healthcare utilisation, and functional impairment in SSD, with effect sizes that exceed antidepressant monotherapy.[8][1]
Specialist psychological therapies
- Psychodynamic interpersonal therapy (PIT) — for complex somatic presentations where early relationship patterns underpin distress.
- Acceptance and commitment therapy (ACT) — for chronic pain/SSD overlap.
- Mindfulness-based cognitive therapy (MBCT) — for anxiety/depression comorbidity and chronic symptoms. [1]
Pharmacological treatment
SSRIs (first-line antidepressant)
- Sertraline 25 to 50 mg starting, titrate to 100 to 200 mg
- Citalopram 10 to 20 mg starting, titrate to 40 mg (20 mg if elderly/QT-prolonged)
- Escitalopram 5 to 10 mg starting, titrate to 20 mg
- Paroxetine 10 to 20 mg (avoid in pregnancy)
- Effective EVEN WITHOUT comorbid depression (independent analgesic/interoceptive effect)
- Start LOW, titrate SLOWLY, expect 6 to 8 weeks for effect
- Pre-warn about side effects to prevent misinterpretation as new disease
SNRIs (pain-predominant)
- Duloxetine 30 to 60 mg daily — strong evidence for chronic musculoskeletal pain, fibromyalgia, neuropathic pain
- Venlafaxine 37.5 to 75 mg starting, titrate to 150 to 225 mg
- Useful where pain is the dominant somatic symptom
- Monitor blood pressure (noradrenergic effect)
TCAs (chronic pain overlap)
- Amitriptyline 10 to 25 mg nocte (low dose)
- Effective for chronic pain, fibromyalgia, migraine prophylaxis, IBS
- Anticholinergic side effects limit use in elderly
- Useful for sleep disturbance + pain
Drugs to AVOID
- OPIOIDS for chronic non-cancer pain — dependence, hyperalgesia, overdose death
- Long-term BENZODIAZEPINES — dependence, withdrawal, cognitive impairment
- Repeated courses of ANTIBIOTICS for unexplained symptoms
- ANTIPSYCHOTICS unless comorbid psychosis
- Polypharmacy in elderly — Beers criteria
Antidepressant prescribing principles in SSD: SSRIs have evidence in somatoform disorders even in the absence of comorbid depression — the effect is partly independent of antidepressant action (analgesic and interoceptive effects). Start at half the usual dose, titrate slowly, set explicit expectations of 6–8 weeks for effect, and pre-warn about side effects so they are not misinterpreted as new disease. Treating comorbid depression/anxiety often improves somatic symptoms.[2]
Functional neurological disorder pathway
A specific, evidence-based pathway has emerged for FND:[7]
- Positive diagnosis by neurology — using the clinical signs (Hoover, entrainment), not just exclusion.
- Psychoeducation using a shared explanatory model — "your nervous system software has a glitch, the hardware is fine."
- Specialist FND physiotherapy — motor retraining (the Nielsen/Jordbru evidence base); specifically-designed programmes that re-train movement.
- CBT — reframe catastrophic beliefs, address comorbidity.
- Treat comorbid anxiety and depression — common and treatable.
- Graded return to function — occupational therapy input, vocational rehab. [1]
Stepped care
- Step 1 (primary care, all patients) — psychoeducation, guided self-help, exercise, sleep hygiene, depression/anxiety screening, regular scheduled reviews.
- Step 2 (mild to moderate) — group or individual CBT in primary care; consider SSRI.
- Step 3 (moderate to severe) — specialist CBT + SSRI/SNRI; coordinated MDT.
- Step 4 (severe / refractory) — combined MDT, pain programme, functional restoration programme, inpatient for severe functional decline. [1]
Escalation triggers
- Significant functional decline (loss of work, mobility, independence).
- Suicide risk or overdose.
- Opioid dependence developing.
- Repeated high-cost admissions.
- Diagnostic uncertainty with possible organic disease.
- Severe self-neglect. [1]
Specific Subtypes & Scenarios
Somatic Symptom Disorder (SSD) — subtype profiles
- Pain-predominant SSD — chronic non-cancer pain; SSRI/SNRI/TCA, CBT for pain, ACT, multidisciplinary pain programme; avoid opioids.
- GI-predominant SSD (IBS-like) — gut-directed CBT, low-FODMAP diet where indicated, low-dose TCA (amitriptyline 10–25 mg nocte), SSRI.
- Cardiac-preoccupation SSD (non-cardiac chest pain, cardiac neurosis) — exercise testing and CT coronary to document absence of disease; CBT for cardiac anxiety; SSRI; cardiac rehabilitation.
- Multisystem SSD — coordinated single-clinician care, integrated care plan. [1]
Illness Anxiety Disorder (IAD)
- Care-seeking subtype — CBT focused on reducing reassurance-seeking and body-checking; SSRI; scheduled reviews with strict no-extra-tests contract.
- Care-avoidant subtype — outreach, anxiety-focused CBT, graded exposure to health information; SSRI; avoid forcing clinic attendance. [1]
Conversion / FND
- Functional weakness/paralysis — specialist FND physiotherapy + CBT; treat comorbidity; positive shared explanation.
- Functional movement disorder (tremor, dystonia) — specialist movement-disorder physiotherapy, CBT.
- Dissociative seizures (PNES) — diagnosis by video-EEG; psychoeducation; CBT-informed therapy; SSRI for comorbid depression; AEDs are NOT effective (no epilepsy to treat).
- Functional sensory symptoms — reassurance, CBT, treat comorbidity.
- Functional speech symptoms (aphonia, dysphonia) — speech and language therapy, laryngeal examination to exclude organic cause. [1]
Factitious disorder
- Confrontation — gentle, non-punitive, with psychiatric support; some patients acknowledge and accept help.
- Psychotherapy — CBT or psychodynamic.
- Harm reduction — minimise iatrogenic harm from unnecessary procedures; coordinated single-clinician care; early identification across hospitals.
- Munchausen by proxy / FII — child protection referral mandatory; multi-agency safeguarding. [1]
PFAMC
- Treat the underlying medical condition optimally.
- Address the psychological factor: non-adherence (motivational interviewing, simplification), stress (CBT, relaxation), anxiety amplification (SSRI, CBT).
- Integrated medical + psychiatric care. [1]
Cultural syndromes
- Dhat syndrome — combined sex education, reassurance about normal physiology, SSRI where depression comorbid, CBT, family counselling; recognise cultural context.
- Kufungisisa — culturally-adapted CBT, problem-solving therapy, treat comorbid depression.
- Brain fag — stress management, study skills, relaxation, treat comorbid anxiety. [1]
Complications & Pitfalls
Iatrogenic harm (the commonest complication)
- Repeated unnecessary investigations — radiation exposure, complications of invasive procedures (angiography, endoscopy), harmful incidental findings driving further spirals.
- Polypharmacy — multiple analgesics, PPIs, anxiolytics; opioid dependence; benzodiazepine dependence.
- Iatrogenic anxiety — "your scan showed a small spot, we need to follow it up." [1]
Functional decline
Loss of employment, education, relationships, mobility, independence; chronic disability; significant caregiver burden. [1]
Comorbidity and suicide risk
Depression (50–80% comorbidity), anxiety, substance use (alcohol, analgesics), personality disorders. Suicide risk is elevated in comorbid depression and chronic pain — assess formally. [1]
The costliest pitfall: missing organic disease
Assuming a symptom is 'functional' and missing genuine new pathology. Any acute change in a known SSD patient warrants genuine medical reassessment — vital signs, focused examination, clinically-indicated tests. The diagnostic label of SSD never exempts a patient from being treated as a patient.[2]
Loss of trust / stigma
The 'heartsink patient' label damages care. Patients feel dismissed, clinicians feel frustrated, the cycle of disengagement and re-presentation accelerates. The therapeutic alliance IS the treatment. [1]
Factitious complications
Self-induced injury, infection, organ damage (insulin, contamination, injected substances); iatrogenic harm from unnecessary procedures; reported mortality in severe Munchausen. [1]
Treatment-related
SSRI side effects (nausea, headache, sexual dysfunction, initial anxiety) misinterpreted as new disease; benzodiazepine dependence if used long-term; opioid-induced hyperalgesia. [1]
Prognosis & Disposition
SSD / IAD prognosis
Typically chronic, fluctuating course over years. Approximately 30–50% of patients achieve significant improvement with CBT; relapse is common with new stressors. Longer duration of untreated illness and stronger illness behaviour predict poorer outcome. Treatment of comorbid depression/anxiety improves prognosis. Quality of life often remains impaired even when symptom counts fall.[1][4]
Conversion / FND prognosis
Approximately 50% of patients achieve substantial improvement with specialist MDT care. Positive prognostic markers: acute onset, clear precipitant, short duration, good premorbid function, absence of comorbid personality disorder, engagement with treatment, a clear shared explanatory model. Poor prognostic markers: chronicity, compensation/legal involvement, severe personality disorder, recurrent admissions, severe comorbid depression. [1]
Dissociative seizures (PNES) prognosis
Variable. Approximately one-third achieve seizure freedom with appropriate treatment; up to half continue to have seizures long-term. Quality of life often remains impaired. Misdiagnosis as epilepsy delays correct treatment by an average of 7–10 years, during which patients receive harmful, ineffective antiepileptic drugs. [1]
Factitious disorder prognosis
Notoriously difficult; few patients engage in sustained treatment; recurrence common; mortality reported in severe cases. [1]
Healthcare utilisation
Structured SSD care (single clinician, scheduled visits, no repeated investigations) reduces ED visits, admissions, and costs substantially — even when symptoms themselves persist. This is one of the highest-yield interventions in the field. [1]
Disposition
Most SSD, IAD, and FND patients are managed as outpatients in primary care with specialist input. Inpatient care is rarely needed: severe functional decline, suicide risk, complex MDT assessment, severe self-neglect, or diagnostic uncertainty requiring observation. ED management: brief assessment, exclude acute organic cause, return to GP/specialist pathway; avoid admission for reassurance. [1]
Special Populations
Children and adolescents
Common somatisation presentations: recurrent abdominal pain, headache, fatigue, school avoidance, pseudoseizures. Strong association with family illness modelling, school stressor, and parental anxiety. Management is family-based CBT, engagement of school, and avoidance of medicalisation. Prognosis often better than in adults. [1]
Pregnancy and postpartum
- Pregnancy-related illness anxiety — foetal-anomaly worry, hyperemesis as somatic focus.
- Postnatal depression with somatic features.
- SSRIs in pregnancy: sertraline preferred (lowest fetal risk); avoid paroxetine in first trimester (cardiac), avoid benzodiazepines (neonatal withdrawal, floppy baby).
- FND may emerge or relapse postpartum; reassure and treat. [1]
Elderly
- New-onset somatisation is uncommon — rule out dementia, depression, delirium, polypharmacy side effects, and vitamin deficiencies (B12, D).
- Health anxiety increases with normal ageing and bereavement.
- Address polypharmacy; review the Beers criteria; avoid over-investigation.
- SSRIs at half starting dose; monitor hyponatraemia, falls, and QTc. [1]
Cultural context
- Recognise culture-bound syndromes (Dhat in India, Kufungisisa in Zimbabwe, Brain fag, Ataque de nervios, Taijin kyofusho).
- Use a cultural formulation interview; involve cultural brokers/interpreters.
- Avoid pathologising normal cultural expressions of distress. [1]
Learning disability / autism
- SSD-like presentations common; difficulty articulating distress verbally.
- Adapt assessment (visual aids, concrete language); exclude comorbid physical disease; involve carers; sensory sensitivities may amplify symptoms. [1]
Comorbid chronic disease
Patients with diabetes, IHD, COPD, IBD frequently have PFAMC (psychological factors worsening their medical condition). Integrated medical + psychiatric care improves outcomes and reduces complications. [1]
Post-COVID syndrome
Persistent physical symptoms (fatigue, breathlessness, brain fog) following COVID-19 overlap with SSD. Requires validation, paced rehabilitation, screening for depression/anxiety, and explicit avoidance of dismissing as 'all in the head'. The biopsychosocial model is essential — the symptoms are real, the framing matters. [1]
Evidence, Guidelines & Regional Differences
DSM-5 (2013) and DSM-5-TR (2022) — the conceptual revolution
DSM-5 replaced the DSM-IV Somatoform Disorders cluster (somatisation disorder, hypochondriasis, pain disorder, undifferentiated somatoform disorder, conversion) with the Somatic Symptom and Related Disorders cluster. Key changes: [1]
- Dropped the requirement that symptoms be 'medically unexplained' — the disorder is now defined by the positive B-criterion (excessive thoughts, feelings, behaviours).
- Hypochondriasis was split: ~75% of patients reclassified as SSD; ~25% reclassified as IAD.
- Pain disorder was folded into SSD with pain as the predominant symptom.
- DSM-5-TR (2022) added clarifying text and emphasised that SSD can be diagnosed in a patient WITH active medical disease.[5]
ICD-11 (effective 2022)
Introduced Bodily Distress Disorder (BDD) — a similar construct to SSD. Recognises the dimensional nature and de-emphasises the explained/unexplained dichotomy. The ICD-11 also retains separate codes for Dissociative neurological symptom disorder (the equivalent of conversion/FND).[1]
CBT evidence
Cochrane reviews and multiple RCTs confirm CBT reduces symptom severity, healthcare utilisation, and functional impairment in SSD, IAD, and FND. Allen et al (2006) randomised controlled trial of CBT for somatisation in Archives of Internal Medicine showed significant improvement versus usual care.[8] Meta-analyses by Kleinstäuber, van Dessel, and Ozel confirm effect sizes that exceed antidepressant monotherapy.
Antidepressant evidence
Kroenke's foundational review on somatoform symptom management established the role of antidepressants even in the absence of comorbid depression.[6] Meta-analyses show modest benefit of SSRIs in somatoform disorders, with effect sizes smaller than CBT.
Functional neurological disorder
The 2025 systematic review and meta-analysis by Finkelstein et al (JNNP) pooled incidence and prevalence data for FND.[7] Randomised trials of specialist physiotherapy (Nielsen, Jordbru, and others), and CBT trials for PNES (LaFrance, Goldstein) support the modern MDT pathway.
Controversies
- B-criterion subjectivity: critics argue the B-criterion has modest inter-rater reliability.
- Over-medicalisation: some argue the SSD construct over-diagnoses normal health anxiety.
- Neurology vs psychiatry of FND: now reframed as a genuine neuropsychiatric disorder with positive signs — not a diagnosis of exclusion. The neurology and psychiatry communities now collaborate.
- Stigma of 'heartsink patient': the anti-stigma movement has shifted the field from 'all in your head' to a genuinely biopsychosocial model where interoceptive network dysfunction is real and measurable. [1]
Regional deltas
Exam Pearls
High-yield for NEET-PG/INICET
- DSM-5-TR SSD: ≥1 somatic symptom + excessive thoughts/feelings/behaviours (disproportionate concern, persistent high health anxiety, OR excessive time/energy) + persistent ≥6 months. Symptoms NEED NOT be medically unexplained.
- Illness Anxiety Disorder: preoccupation with HAVING/ACQUIRING serious illness; somatic symptoms ABSENT or MILD; ≥6 months; care-seeking vs care-avoidant subtypes.
- Conversion disorder: motor/sensory symptom INCOMPATIBLE with recognised disease; NOT consciously produced; psychological factors associated.
- Factitious disorder: falsification/induction WITH intent to deceive; motive = sick role (internal). Malingering: feigning for EXTERNAL gain (money, drugs, leave, avoiding prosecution).
- PFAMC: psychological/behavioural factors worsen a diagnosed general medical condition.
- DSM-5 dropped 'medically unexplained symptoms' — SSD can co-exist with genuine medical disease.
- Hoover sign — hip extension weakness that returns when testing contralateral hip flexion — the classic conversion/FND motor sign.
- Dissociative seizures (PNES): eyes CLOSED, asynchronous thrashing, pelvic thrusting, side-to-side head, recall, no postictal confusion — distinguish from epileptic seizures.
- La Belle Indifférence — apparent lack of distress about a severe deficit — classic but present in only ~30% and NOT diagnostic.
- First-line treatment: CBT. Antidepressants (SSRIs) — even without depression. AVOID opioids, long-term benzodiazepines, repeated unnecessary investigations.
- Regular scheduled GP appointments (every 2 to 4 weeks) reduce ER visits and investigation demand — the containment principle.
- PHQ-15 ≥10 = moderate-to-severe somatic symptom burden; Whiteley-7 ≥3 screens positive for illness anxiety.
- Acute change in a known SSD patient — ALWAYS reassess for genuine new medical disease. Never assume functional.
- 3 Ps formulation: Predisposing (childhood adversity, alexithymia, family modelling) → Precipitating (life stressor, health scare) → Perpetuating (reassurance-seeking, avoidance, iatrogenic reinforcement).
- Cultural syndromes: Dhat (India), Kufungisisa (Zimbabwe), Brain fag, Ataque de nervios, Taijin kyofusho, Kayak angst.
- Antidepressant dosing in SSD: start LOW, titrate SLOWLY, expect 6–8 weeks for effect — patients are somatically hypersensitive to side effects.
- Commonest single comorbidity is depressive or anxiety disorder (50–80%) — treating it often improves the somatic symptoms.
- ICD-11 term: Bodily Distress Disorder. DSM-5-TR term: Somatic Symptom Disorder. The shift is from 'unexplained' to 'maladaptive response'.
- Interoceptive network (anterior insula + anterior cingulate cortex) is hyperactive on fMRI — this is the measurable neurobiology of amplification.
- Munchausen by proxy = Fabricated or Induced Illness (FII) = child abuse — mandatory child-protection referral. [1]
Exam application bank (NEET-PG / INICET)
One-line answer
The somatic symptom and related disorders (SSRD) are a DSM-5-TR cluster defined by EXCESSIVE thoughts, feelings, and behaviours related to somatic symptoms or health concerns, NOT by absence of disease. Somatic Symptom Disorder (SSD): one or more distressing somatic symptoms plus disproportionate concern, persistent health anxiety, or excessive time/energy devoted to symptoms for at least 6 months. Illness Anxiety Disorder (IAD, hypochondriasis): preoccupation with having or acquiring a serious illness with minimal/no somatic symptoms. Conversion/FND: motor or sensory symptoms incompatible with recognised neurological disease, NOT consciously produced. Factitious = falsification/induction for the sick role; malingering = feigning for external gain. Pathophysiology: catastrophic misinterpretation of bodily sensation in a hyperactivated interoceptive network (anterior insula + ACC), reinfo
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Somatic Symptom Disorder & Related Disorders.
References
- [1]Löwe B, Conrad R, Bär KJ, et al. Persistent physical symptoms: definition, genesis, and management Lancet, 2024.PMID 38879263
- [2]Sauer KS, Witthöft M, Rief W. Somatic Symptom Disorder and Health Anxiety: Assessment and Management Neurol Clin, 2023.PMID 37775202
- [3]Henningsen P, Zipfel S, Herzog W. Management of functional somatic syndromes Lancet, 2007.PMID 17368156
- [4]Kikas K, Werner-Seidler A, Upton E. Illness Anxiety Disorder: A Review of the Current Research and Future Directions Curr Psychiatry Rep, 2024.PMID 38748190
- [5]Dimsdale JE, Creed F, Escobar J, et al. Somatic symptom disorder: an important change in DSM J Psychosom Res, 2013.PMID 23972410
- [6]Kroenke K. Symptoms, syndromes, and the value of psychiatric diagnostics in patients who have functional somatic disorders Med Clin North Am, 2006.PMID 16843765
- [7]Finkelstein SA, Liu M, Rosenblum JD, et al. Incidence and prevalence of functional neurological disorder: a systematic review J Neurol Neurosurg Psychiatry, 2025.PMID 39663114
- [8]Allen LA, Woolfolk RL, Escobar JI, Gara MA, Hamer RM. Cognitive-behavioral therapy for somatization disorder: a randomized controlled trial Arch Intern Med, 2006.PMID 16864762