Psychiatry · Psychiatry
Suicide Risk Assessment & Prevention
Also known as Suicide risk assessment · Suicidal ideation · Self-harm · Suicide prevention · Deliberate self-harm
Suicide is a leading cause of death worldwide. Risk assessment is a core clinical skill: ask directly about ideation, plan, intent, means, and preparatory acts. Risk factors (male sex, older/young adult age, psychiatric disorder — depression in 60 percent, previous attempt = strongest predictor, hopelessness, substance use, access to lethal means) are weighed against protective factors (social support, reasons for living). Risk stratification drives disposition: high risk = urgent admission; moderate = crisis team, remove means, safety plan; low = outpatient plus safety plan. ALWAYS document.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Exam tags
Red flags
Overview & Definition
Suicide is among the most consequential clinical events a doctor will ever encounter, and suicide risk assessment is the most high-stakes clinical skill in medicine — a missed assessment can cost a life, while an uncalibrated one can strip a person of their liberty. The World Health Organization estimates that well over 700,000 people die by suicide each year, making it a leading cause of death worldwide and the second or third leading cause of death in adolescents and young adults. For every death there are many more attempts, and the lifetime prevalence of suicidal thoughts in the general population is substantial.[1]
The single most important principle of assessment is to ask directly about suicide. A pervasive and dangerous myth is that asking about suicide "plants the idea" and increases risk — the evidence is the opposite. Direct, non-judgemental questioning provides relief, signals that the clinician is willing to hear the worst, and opens a conversation that the person may have been waiting years to have.[1][2]
A precise vocabulary matters because each term carries different management and prognostic implications. The terms below are not interchangeable: [1]
Suicidal ideation
- Thoughts of ending one's own life
- Ranges from passive ('I wish I wouldn't wake up') to active ('I want to kill myself')
- Frequency, intensity, duration and controllability are quantified
Suicidal intent
- Subjective conviction that one intends to act on the thoughts
- Higher intent correlates with more lethal methods and lower likelihood of rescue
- Assessed from the patient and from the circumstances of any attempt
Suicide plan
- Specificity of method, time, place, and preparation
- A detailed, lethal, rehearsed plan = high risk
- Includes preparatory acts (giving away possessions, writing a note, obtaining means)
Suicide attempt
- A self-directed, potentially injurious behaviour with some intent to die
- Outcome may be fatal or non-fatal
- Distinguished from NSSI by the presence of any intent to die
Deliberate self-harm (DSH)
- Intentional self-injury regardless of motivation
- May be suicidal or non-suicidal
- Term preferred in UK/Indian usage; encompasses the spectrum
NSSI
- Non-suicidal self-injury: deliberate tissue damage without intent to die
- Function is affect regulation, self-punishment, or communication
- DSM-5-TR recognises it as a distinct condition for further study; ICD-6 draft status evolving

The diagnostic frameworks have shifted suicidality from a symptom to a target in its own right. DSM-5-TR includes Suicidal Behavior Disorder (requiring, within the prior 24 months, a suicide attempt, plus a criterion of intent excluding NSSI and accidental/psychotic-command acts) and Non-Suicidal Self-Injury as conditions for further study. ICD-11 introduces the standalone category Suicide attempt and separates it from Non-suicidal self-injury, giving clinicians discrete codes that recognise intent as a clinical variable rather than a mere feature of another disorder. Understanding this nomenclature lets you communicate risk precisely — saying "the patient has active ideation, a specific plan, but no intent and no preparatory acts" tells a colleague far more than "the patient is suicidal."[1]
Classification
Suicide risk is best classified along two axes that are clinically useful rather than theoretically pure: (1) the temporal/nosological category of the suicidal phenomenon, and (2) the stratified level of risk that drives disposition. Classification along the first axis is shown above (ideation, plan, intent, attempt). The second — risk stratification — is the output of assessment and the input to management. [1]
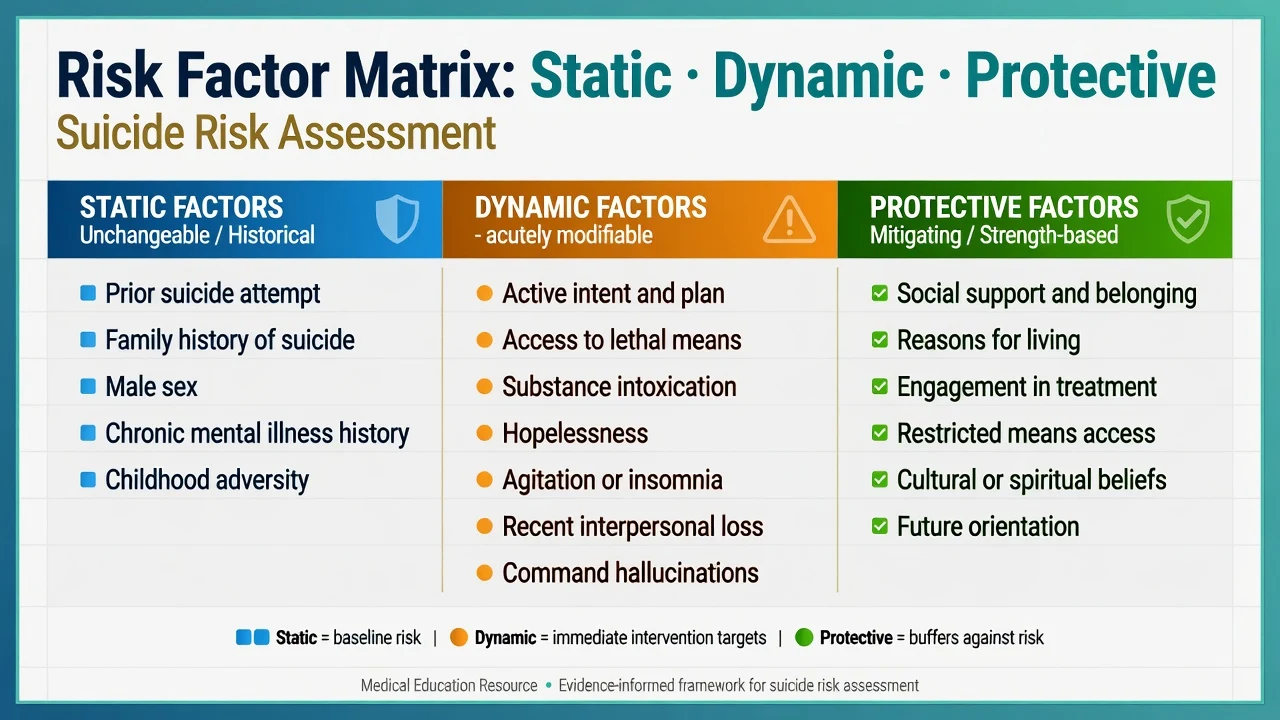
Risk factors cluster into recognisable groups. The figure below and the mnemonic that follows organise the static and dynamic factors an examiner expects you to enumerate, weighed against protective factors that pull in the opposite direction. [1]
The numbers examiners reward
Suicide warning signs (mnemonic — warning signs, not predictors)
IS PATH WARM
Threatening, talking, or writing about suicide
Increased or excessive use
No reason to live
Agitation, insomnia, panic
Feeling there is no way out
Nothing to live for; better predictor than mood severity
From friends, family, society
Rage, seeking revenge
Risky acts without thinking
Dramatic shift, often the deceptive 'calm' before an attempt
The distinction between risk factors (longer-term, population-level associations that raise baseline vulnerability) and warning signs (acute, proximal indicators that risk is rising now) is conceptually important and examinable. A risk factor such as a family history cannot be modified today; a warning sign such as recent gun purchase can be acted on within the hour. [1]
Epidemiology & Risk Factors
Suicide is a global phenomenon but its shape is regional. The WHO estimates over 700,000 deaths annually — roughly one every 40 seconds — and suicide ranks among the top causes of death in people aged 15 to 29 worldwide. India carries a disproportionate burden: National Crime Records Bureau data report tens of thousands of suicides annually, and the Mental Healthcare Act 2017 decriminalised attempted suicide (repealing the practical effect of Section 309 IPC), presuming anyone who attempts suicide to be "under severe stress" and entitled to rehabilitation rather than prosecution.[1]
The epidemiological patterns every candidate must know are the following: [1]
- The gender paradox. Women make more suicide attempts; men die by suicide more often — the male-to-female completion ratio is roughly 3 to 4:1 in most countries. The gap reflects men's greater use of highly lethal methods (firearms, hanging) and lower help-seeking. This is one of the highest-yield facts in psychiatry.
- Age. Two peaks: adolescents and young adults (15 to 24) and older adults (over 65, with the highest completion rate in those over 75, especially men living alone after bereavement).
- Psychiatric disorder is the largest single risk domain. Roughly 90 percent of people who die by suicide have a diagnosable psychiatric disorder at post-mortem psychological autopsy. Depression is implicated in about 60 percent of suicides; the lifetime suicide rate in major depression is approximately 6 percent. Bipolar disorder carries a similar lifetime rate. Schizophrenia has a lifetime suicide rate of about 5 to 10 percent, typically early in the illness in a young, single male during a post-psychotic depressive phase. Borderline personality disorder has a suicide completion rate near 10 percent. Anorexia nervosa and alcohol/substance use disorders carry markedly elevated rates.
- Previous attempt = single strongest individual predictor. A prior attempt multiplies risk roughly 5 to 10-fold and remains predictive lifelong.[2]
- Hopelessness (the conviction that suffering will not improve) predicts suicide more strongly than the severity of depressive symptoms — a finding from Beck's work that examiners reward.
- Access to lethal means. Firearms in the home (a gun in the home doubles-to-quadruples suicide risk); large medication hoards; pesticides and organophosphates in rural Asia (the leading means of suicide death worldwide by absolute numbers).
- Recent loss or psychosocial crisis — bereavement, relationship breakdown, job loss, financial ruin, public humiliation, or a recent medical diagnosis.
- Family history of suicide (independent of diagnosed illness), reflecting shared genetic loading and modelling.
- Chronic pain, chronic illness, and disabling neurological disease (multiple sclerosis, traumatic brain injury, epilepsy, Huntington disease, HIV).
Static risk factors (cannot change today)
- Previous attempt
- Family history of suicide
- Male sex, older/young-adult age
- Chronic mental illness
- History of childhood abuse / adversity
Dynamic risk factors (modifiable now)
- Active psychiatric symptoms (depression, psychosis)
- Substance intoxication
- Hopelessness and insomnia
- Access to lethal means
- Social isolation / acute crisis
Protective factors (pull the other way)
- Responsibility to children / family
- Social support and integration
- Religious / cultural prohibition
- Engagement with services
- Problem-solving and coping capacity
- Fear of death / reasons for living
Protective factors are not the opposite of risk factors — they are independent variables that lower the probability of acting on suicidal thoughts and must be documented with the same care. Pregnancy and responsibility for young children are powerful protectors; genuine social integration; religious faith that proscribes suicide; a strong therapeutic relationship; and concrete "reasons for living."[1]
Pathophysiology
Suicide is not the inevitable endpoint of a single disease; it is the product of a stress-diathesis model in which a fixed vulnerability (the diathesis — genetic loading, early-life adversity, trait impulsivity) interacts with proximal stressors (loss, intoxication, insomnia, acute psychiatric relapse) to cross a threshold. The biological substrate is increasingly understood at the neurotransmitter, endocrine, and circuit levels, and these mechanisms are examinable because they explain why particular drugs (lithium, clozapine) and particular methods of prevention (means restriction) work.[1]
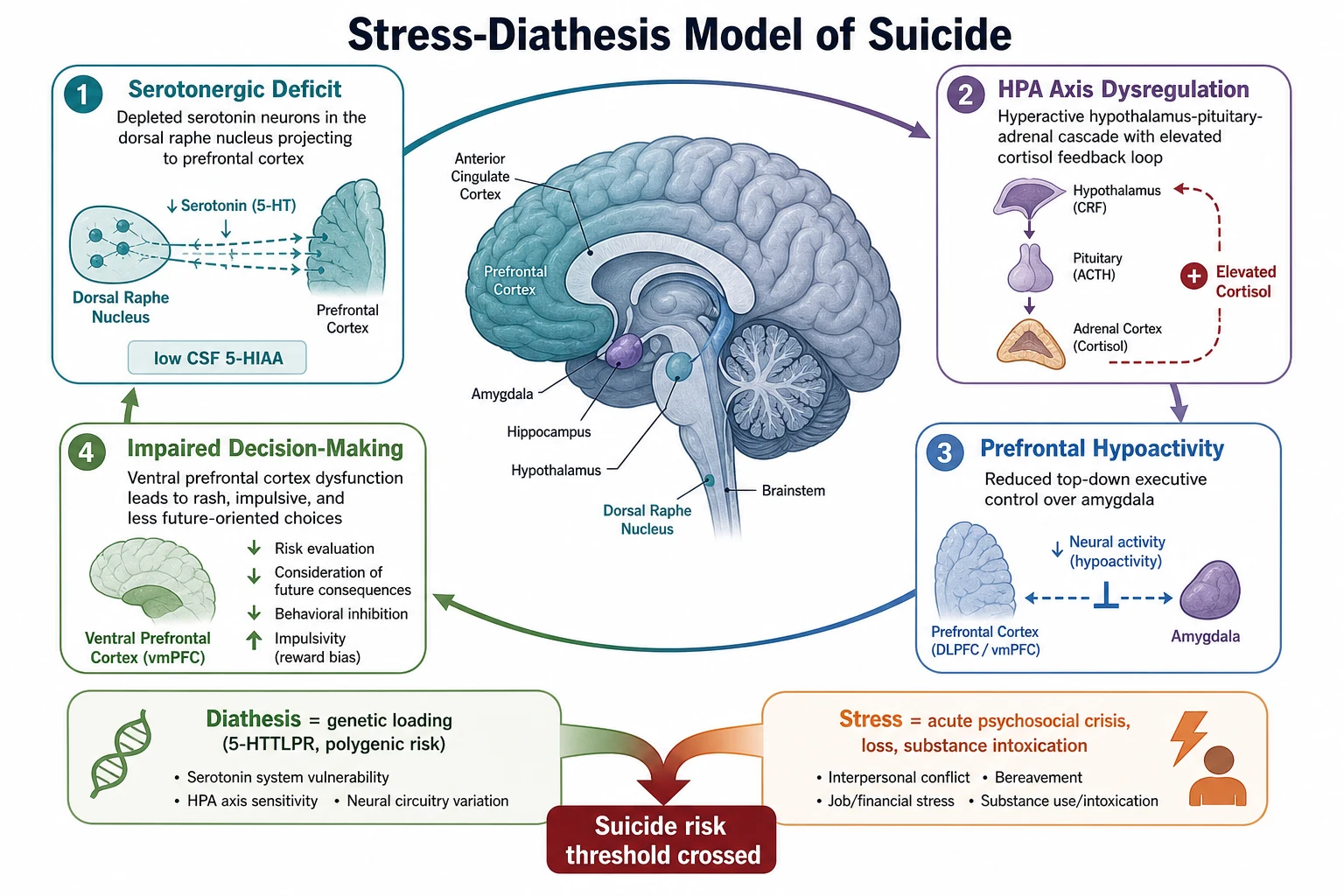
Serotonergic system
- Low 5-HIAA in CSF of attempters (most replicated finding)
- Blunted prolactin response to fenfluramine challenge
- Serotonin transporter 5-HTTLPR short allele = impulsivity/aggression phenotype
- Dorsal raphe to prefrontal projection deficits
HPA axis
- Non-suppression on dexamethasone suppression test predicts completed suicide
- Chronic early adversity sensitises the stress axis
- Hyper-cortisolaemia drives depressive and agitated states
Prefrontal circuitry
- Ventral/orbitofrontal prefrontal hypoactivity on fMRI/PET
- Reduced executive control over amygdala = poor inhibition of aggressive impulse
- Impaired decision-making (Iowa Gambling Task deficits)
Inflammation & neuroplasticity
- Raised IL-6 and TNF-alpha; microglial activation
- Reduced BDNF in suicide completers
- Links depression biology to vascular and metabolic comorbidity
Psychological theories translate the biology into testable clinical constructs. Beck's hopelessness theory holds that stable negative expectations about the future mediate the link between depression and suicide — and predict it better than symptom severity. Joiner's interpersonal theory proposes that suicide emerges from the convergence of thwarted belongingness (I am alone), perceived burdensomeness (I am a burden), and the acquired capability for suicide (fearlessness about death, learned through painful and provocative experiences, including prior self-harm). Williams' cry of pain / arrested flight model reframes suicide as a defeated, trapped state in which escape appears impossible rather than a goal-directed act. Each theory maps onto modifiable targets — belongingness can be built, burdensomeness can be reframed, means can be restricted, and acquired capability can be left unprovoked.[1]
Clinical Presentation
There is no pathognomonic sign of suicide risk. The presentation is a pattern assembled from the history, the mental state, the circumstances of any attempt, and collateral information. Patients commonly conceal intent — many who die by suicide denied suicidal thoughts at their last contact — so absence of stated ideation never excludes risk, and collateral history is mandatory whenever obtainable.[2]
The suicidal patient may present in any of several ways: [1]
- Ongoing ideation, volunteered or elicited, ranging from passive ("life isn't worth it") to active with a plan.
- A recent suicide attempt, brought to the emergency department by ambulance after an overdose, hanging, wrist-cutting, ingestion of organophosphate, or a fall/jump.
- A worsening of a known psychiatric disorder in which risk is recognised as a complication (e.g. severe insomnia and agitation in melancholic depression; command hallucinations in schizophrenia; dysphoric alcohol withdrawal).
- Behavioural change flagged by family — giving away possessions, writing a will or farewell notes, settling affairs, saying goodbye, obtaining the means (buying rope, hoarding pills), researching methods online, sudden unexplained calm after a period of torment. [1]
Atypical and deceptive presentations are deliberately tested: [1]
- The deceptive calm. A patient who has been agitated and hopeless who suddenly appears serene and at peace may have made the decision and feels relief that the suffering will end. Any abrupt improvement in mood in a recently suicidal patient is a red flag, not a recovery — reassess before congratulating yourself.
- The elderly patient. Depression is under-recognised in older adults; somatic complaints, cognitive change, and social withdrawal may dominate. Method lethality is high and the attempt-to-completion ratio is low, so even low-grade ideation in an isolated elderly man after bereavement is dangerous.
- The intoxicated patient. Alcohol acutely disinhibits and is involved in up to a third of suicides; an assessment performed while the patient is intoxicated is invalid for discharge decisions — reassess once sober.
- The adolescent. Risk may present as behavioural dyscontrol, school refusal, self-harm, or running away rather than verbalised ideation; bullying, sexual orientation distress, and social media exposure are common precipitants.
- The postpartum woman. Postnatal depression with intrusive thoughts of harming the infant or herself is a psychiatric emergency; psychotic postpartum depression carries additional risk of infanticide.
- The concealed attempt. A patient may present with a vague physical complaint that is in fact an incomplete or low-lethality attempt (e.g. a "minor" paracetamol ingestion days earlier) — take any inconsistent or unexplained injury seriously. [1]
Differential Diagnosis
The task is twofold: distinguish a genuine suicide attempt from behaviours that mimic it, and identify the underlying psychiatric driver that must be treated if risk is to fall. [1]
Suicidal self-harm
- Intent to die present
- Method chosen for lethality, low rescue likelihood
- Triggers: hopelessness, defeat, entrapment
- Drives admission and safety planning
Non-suicidal self-injury (NSSI)
- No intent to die
- Function: affect regulation, self-punishment, anti-dissociation, communication
- Often repetitive, low-lethality (cutting, burning)
- Still raises future suicide risk — assess intent each time
Accidental injury
- No self-harm intent
- History, scene, and pattern fit an accident
- Exclude concealed attempt in ambiguous cases
Self-harm in psychosis / delirium
- Driven by command hallucinations or persecutory delusions
- Or disorganised, impaired-consciousness acts in delirium
- Treat the psychosis/delirium as the primary emergency
Munchausen / factitious / malingering
- Self-injury staged for secondary gain (admission, opioids, shelter, avoidance)
- Pattern of recurrent dramatic presentations
- Genuine suicide risk may still coexist — never dismiss
Ego-dystonic obsessions (OCD)
- Intrusive unwanted thoughts of harm/harming — distressing, resisted
- Patient appalled by the thoughts, no true intent
- Distinguish from suicidal ideation by ego-dystonicity and resistance
The underlying driver differential is critical because treatment is disorder-specific: melancholic depression (ECT if severe); bipolar depression (beware antidepressant-induced switching; lithium's anti-suicide effect); psychotic depression (antipsychotic plus antidepressant, or ECT); schizophrenia (treat positive symptoms, akathisia, and post-psychotic depression — clozapine if treatment-resistant); substance use disorder (detoxification, relapse-prevention); acute stress or adjustment disorder (brief intervention, problem-solving); borderline personality disorder (DBT, structured specialist care); delirium (treat the underlying organic cause). A suicide risk assessment that does not land on a treatable driver is incomplete.[1]
Clinical & Bedside Assessment
The structured suicide risk interview is a clinical skill built on engagement, direct enquiry, and formulation. The aim is not to elicit a yes/no answer but to construct a narrative of the person's suffering, their reasons for living, and the specific factors that raise or lower the probability they will act. [1]
A practical sequence, suitable for any setting from the emergency department to the outpatient clinic: [1]
- Engage. Privacy, time, sitting at the patient's level, an open, non-judgemental stance. "I ask all my patients about this because it's important."
- Ask directly. "Have you had thoughts that life isn't worth living, or thoughts of ending your life?" Move from passive to active ideation without flinching.
- Characterise the ideation. Frequency, intensity, duration, controllability — can the patient dismiss the thought, or does it feel intrusive and compelling?
- Elicit the plan. Method, time, place, rehearsal, preparations, and lethal means already obtained. Specificity scales with danger.
- Estimate intent. How likely does the patient believe they are to act? What has stopped them so far? What do they imagine would happen?
- Identify preparatory acts. Giving away possessions, writing a will or note, saying goodbye, settling debts, researching methods, practising, obtaining the means.
- Assess access to means. Firearms at home, medication hoards, pesticides, ligature points. Means restriction begins at the bedside.
- Weigh protective factors. Reasons for living, children, faith, social support, therapeutic engagement.
- Obtain collateral. From family, carers, the GP, prior records — with consent where the patient has capacity, and in the patient's best interest where risk justifies it.
- Examine the mental state. Look for hopelessness, psychomotor agitation, severe insomnia, anhedonia, persecutory delusions, and command hallucinations — the items most strongly associated with imminent risk.
- Formulate and document. Integrate static and dynamic risks, protective factors, and a stratified level of risk (low, moderate, high), with explicit reasoning and a safety plan. [1]
The mental state examination deserves emphasis. Among depressed patients, the features that predict suicide beyond mood severity are hopelessness, panic and psychic anxiety, global insomnia, severe anhedonia, and agitation — the so-called "anxious-agitated" phenotype in which the energising misery of melancholia is most dangerous. In psychosis, command hallucinations telling the patient to harm themselves, and persecutory delusions in which death seems an escape, raise risk acutely.[1]
SAD PERSONS risk scale (know it, but know its limits)
SAD PERSONS
Male
Under 19 or over 45
Or hopelessness
Or psychiatric care
Excess alcohol use
Psychosis
Lacking / isolated / widowed / divorced
Or no spouse
Splits with social support above
Investigations
Suicide risk is a clinical assessment. There is no blood test, scan, or biomarker — present or foreseeable — that can reliably rule suicide risk in or out for an individual. Investigations are therefore ancillary: they identify the organic contributors to a mental state, quantify the toxic consequences of an attempt, and stage comorbid disease. They never substitute for the interview. [1]
The panel obtained in a patient presenting with suicidal ideation or after an attempt typically includes: [1]
- Drug and alcohol screen — to detect intoxication (which invalidates the assessment and must be allowed to resolve) and to identify a substance use disorder driving risk.
- Bloods — full blood count, urea and electrolytes, liver function tests, glucose, calcium, magnesium, thyroid function (hypothyroidism can mimic or worsen depression), vitamin B12 and folate, and an infection screen where indicated.
- ECG — if a tricyclic or other cardiotoxic overdose is suspected, and as a baseline before psychotropic prescribing.
- Neuroimaging (CT brain) — for a first presentation of psychosis, atypical features, cognitive impairment, new neurological signs, or suspected delirium.
- Specific toxic assays after an attempt: a 4-hour paracetamol level (treat with N-acetylcysteine per the treatment nomogram), salicylate level, lithium level, digoxin, iron, methaemoglobin (dapsone or nitrite overdose), and plasma cholinesterase (organophosphate poisoning). These are time-critical and protocolised — see the overdose topics. [1]
Screening tool
- C-SSRS: ideation severity (1-5) + behaviour subscale (actual / aborted / interrupted attempts, preparatory acts, NSSI)
- Beck Scale for Suicidal Ideation (BSS): 19 items, self-report
- Beck Hopelessness Scale (BHS): 20 items; cut-off 9
- IS PATH WARM: warning-sign mnemonic, not a score
Predictive value
- Positive predictive value for individual suicide is very low (well under 1 percent for most tools)
- Sensitivity modest; specificity modest
- Use to STRUCTURE the assessment and document, not to discharge
- NICE (UK) explicitly discourages risk-tool-driven discharge decisions
Biological correlates (research)
- Low CSF 5-HIAA (not bedside)
- Dexamethasone non-suppression (research marker)
- Polygenic risk scores (emerging, not clinical)
- None validated for individual prediction
The key teaching point, and a frequent SAQ trap, is that a low score on a risk scale never permits discharge against clinical judgement, and a high score never mandates admission on its own. The tools are scaffolding for a clinical formulation. Document the formulation — the risk and protective factors, the warning signs, the dynamic changes, and the reasoning behind your disposition — not merely a number. [1]
Management — Resuscitation
The post-attempt patient is a medical emergency first and a psychiatric patient second. Resuscitation follows ABCDE, then poison-specific antidotal therapy, then — and only then — psychiatric assessment. [1]
Resuscitation of the post-attempt patient
Secure the airway, give high-flow oxygen if hypoxic, support breathing and circulation, assess disability (GCS, pupils, glucose), expose and examine. Take a focused history of the agent, dose, time, and route from the patient, paramedics, and family.
Activated charcoal within 1 hour for relevant ingestions (not paracetamol-only protocols, not hydrocarbons). Paracetamol: 4-hour level, start N-acetylcysteine per nomogram. Tricyclic: intravenous sodium bicarbonate for QRS widening, hypotension, or arrhythmia. Opioid: naloxone titrated to respiratory rate. Organophosphate: atropine plus pralidoxime. Lithium: aggressive normal saline, haemodialysis if severe. Benzodiazepine: flumazenil only with great caution (seizure risk).
Treat seizures, arrhythmias, hypotension, hypoglycaemia, and hypothermia. Address the airway in hanging victims (cervical spine, laryngeal injury, airway oedema, anoxic brain injury).
Once medically stable, place the patient on constant (one-to-one) nursing observation. Remove ligature points, sharps, belts, cords, and medications. Do not leave the patient to use the bathroom unattended. The medical bed is also a psychiatric observation bay.
No patient who has attempted suicide is discharged without a psychiatric assessment. If the patient tries to leave against advice with ongoing risk, assess capacity; if lacking capacity or if risk is imminent, invoke the Mental Health Act (UK), the Mental Healthcare Act 2017 (India), or the equivalent statute — the duty of care overrides autonomous refusal when death is imminent.
Means restriction at the point of care is resuscitation-adjacent and must not wait: do not prescribe tricyclic antidepressants in bulk to a patient at risk (dispense small quantities; the SSRI sertraline is the safer default); do not co-prescribe with large benzodiazepine supplies; counsel families to remove or secure firearms and medications before the patient returns home. [1]
Management — Definitive & Stepwise
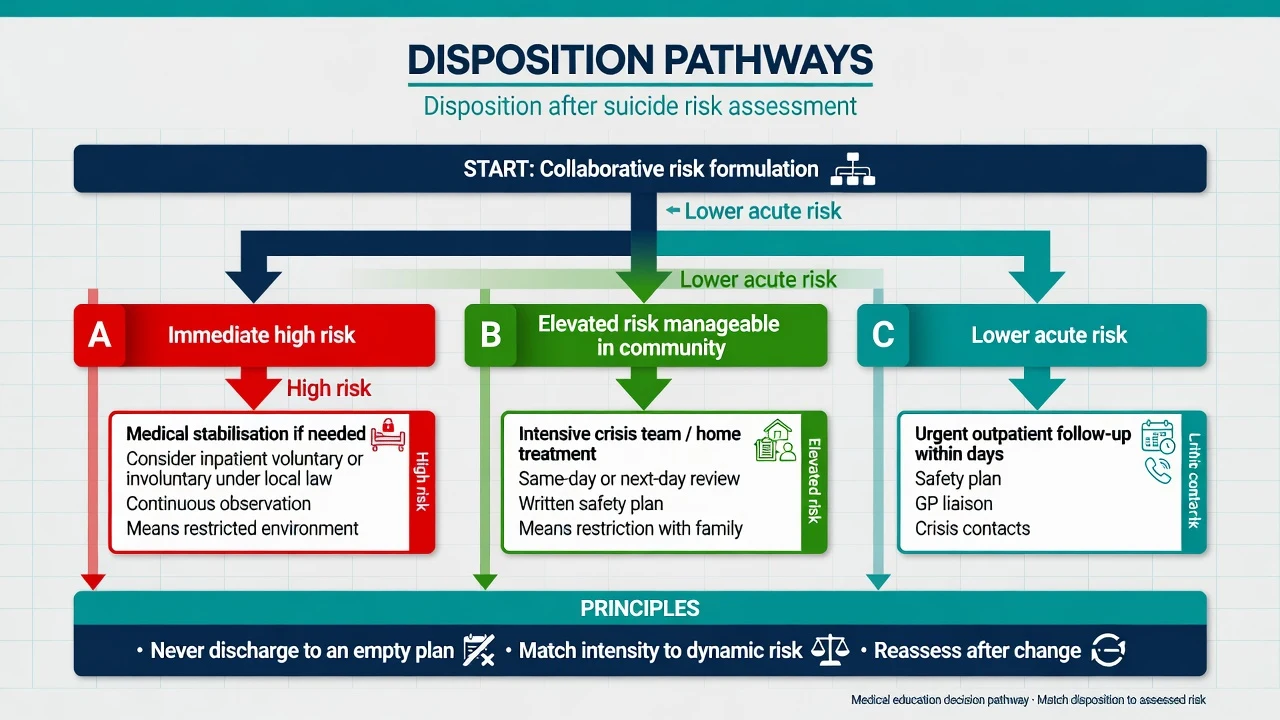
Once the patient is medically stable and the risk is formulated, management is risk-stratified and disorder-specific. The two pillars are (1) safety and disposition matched to risk level, and (2) treatment of the underlying psychiatric disorder and the suicidality itself. [1]
HIGH risk
- Active ideation + specific plan + intent + access to means
- OR recent high-lethality attempt with ongoing ideation
- Urgent psychiatric admission — involuntary if refused and imminent
- Constant one-to-one observation initially; remove all means
- Treat underlying disorder aggressively (ECT for severe psychotic depression)
MODERATE risk
- Active ideation without a clear plan, or plan without intent
- Crisis resolution / home treatment team (CRHT) or intensive outpatient
- Remove access to means (firearms secured; small medication quantities)
- Written safety plan (Stanley-Brown): warning signs, coping, contacts, crisis lines
- Follow-up within 24 to 48 hours
LOW risk
- Passive ideation, no plan, no intent, strong protective factors
- Outpatient management with GP and mental health team
- Safety plan + crisis line + means counselling
- Follow-up appointment within 7 days
- Reassess at every contact — risk is dynamic
Disorder-specific pharmacotherapy targeting suicidality: [1]
- Mood disorders (depression, bipolar). Treat the depression aggressively, but choose agents with low lethality in overdose. Lithium has the best evidence for an anti-suicide effect in mood disorders: meta-analytic data (Cipriani et al., BMJ 2013) show lithium reduces suicide and suicide-related events versus placebo and several comparators, and the effect persists in observational cohorts. The mechanism likely combines mood stabilisation, reduction of impulsivity, and serotonergic effects.[4] SSRIs (especially sertraline, first-line; fluoxetine is the SSRI with the strongest safety evidence in under-18s) are the default antidepressant — warn of initial activation and the small early increase in suicidal thoughts in young people, and review at 1 to 2 weeks. Avoid tricyclics as first-line in those at risk because of their high lethality in overdose.
- Schizophrenia. Treat positive symptoms, akathisia (a profoundly distressing and under-recognised driver of suicide — reduce or change the antipsychotic, not just add an anticholinergic), and post-psychotic depression. Clozapine is the only antipsychotic with proven anti-suicide effect: the InterSePT trial (Meltzer et al., 2003) randomised schizophrenia patients with suicidality to clozapine or olanzapine and found clozapine reduced suicide attempts and hospitalisations to save lives — a finding now embedded in international guidance.[3]
- Substance use disorders. Detoxification, relapse-prevention pharmacotherapy (naltrexone, acamprosate for alcohol; opioid agonist therapy for opioid use disorder), and integrated dual-diagnosis care. Intoxication is a proximal disinhibitor and must be addressed before any other plan is reliable.
- Borderline personality disorder. Dialectical behaviour therapy (DBT) is the best-evidenced intervention for recurrent self-harm and suicidality in BPD, reducing both suicide attempts and hospitalisation. Avoid prolonged inpatient admission as a routine (it can reinforce the behaviour); use brief crisis admission with clear goals.
Suicide-specific psychological and system interventions with trial evidence include cognitive-behavioural therapy for suicide prevention (CBT-SP) (reduces repeat attempts), brief follow-up contact and "caring letters" (the WHO SUPRE-MISS agenda and several trials show that a few contacts in the weeks after discharge cut subsequent suicide), and structured safety planning (the Stanley-Brown Safety Plan, now recommended by NICE as a central element of care after self-harm).[1][2]
Specific Subtypes & Scenarios
Adolescents / students
- Rising rates; bullying, cyberbullying, academic stress, sexual-orientation distress, social media contagion
- Screen at every contact (e.g. ASQ, HEADSS framework)
- Involve family and school; CAMHS referral
- Fluoxetine is the SSRI with best paediatric safety evidence
Older adults
- Highest completion rate; high-lethality methods; low attempt-to-completion ratio
- Depression under-recognised; somatic and cognitive presentations
- Bereavement, isolation, chronic pain, sensory impairment drive risk
- Sertraline preferred SSRI (fewer interactions, lower hyponatraemia than some); avoid tricyclics
Schizophrenia
- Lifetime risk 5 to 10 percent; peak early, in young single males
- Drivers: command hallucinations, persecutory delusions, akathisia, post-psychotic depression, loss during recovery
- Clozapine for treatment-resistant illness and suicidality (InterSePT)
Substance use
- Alcohol disinhibition in up to a third of suicides
- Opioid overdose epidemic
- Methamphetamine psychosis, withdrawal dysphoria
- Integrated dual-diagnosis treatment essential
Borderline PD
- Recurrent DSH / NSSI, impulsivity, ambivalent intent
- DBT is first-line evidence-based therapy
- Avoid prolonged routine admission; use brief crisis admissions with clear goals
Physicians / health workers
- High-stress occupation; depression, burnout, substance use
- Access to means and self-prescribing
- Confidential treatment pathways reduce barrier to help-seeking
Prisoners / military / veterans
- Trauma, PTSD, depression, isolation
- High firearm access
- Trauma-informed, means-focused care
A note on method and region that examiners in India emphasise: in rural India and much of south and east Asia, pesticide (organophosphate) ingestion is among the leading means of suicide death — resuscitation requires prompt atropine and pralidoxime alongside atropine-titrated airway and secretion control. In the United States, firearms dominate (over half of suicide deaths). Globally, hanging is the most common method. Means restriction therefore looks different in different settings — pesticide bans and secure storage, firearm legislation, barrier installation on bridges, and paracetamol pack-size limits have all reduced method-specific suicide at population scale.[1]
Complications & Pitfalls
The complications of suicide and its management extend beyond the immediate medical: [1]
- Completed suicide — the catastrophic outcome; non-fatal repeat attempts with escalating lethality; permanent physical and neurological deficit from the attempt (hypoxic brain injury after hanging or near-drowning, hepatic failure after paracetamol, limb loss after vascular injury).
- Family and carer trauma — bereavement by suicide carries a markedly elevated risk of complicated grief, depression, and suicide contagion within families and communities (suicide clusters).
- Clinician consequences — countertransference, vicarious trauma, and the medico-legal and professional consequences of a missed or mismanaged case. A patient suicide is among the most distressing events in a clinician's career; structured peer support and case review matter. [1]
The classic pitfalls are examinable because they recur: [1]
- Relying on a single point-in-time assessment. Risk is dynamic; the most dangerous day may be the day after discharge, not the day of assessment.
- Trusting a scale over judgement. A low score does not make a patient safe.
- Failing to obtain collateral. Patients conceal intent; family often holds the decisive information.
- Failing to restrict means. Prescribing a bulk tricyclic, leaving a firearm accessible, or discharging a patient to a home full of hoarded pills converts a plan into an outcome.
- Relying on a no-suicide contract. No protective value; may even increase risk through false reassurance.
- Missing the deceptive calm. Sudden serenity after torment is the decision, not the cure.
- Discharging an intoxicated patient. The assessment is invalid until the patient is sober.
- Ignoring akathisia. In a schizophrenic patient recently started on a first-generation or high-dose antipsychotic, unbearable restlessness is a treatable, iatrogenic driver of suicide.
- Forgetting the discharge window. The first one to two weeks after psychiatric discharge carry the highest suicide risk of any clinical period — schedule and ensure a concrete follow-up before the patient leaves. [1]
Prognosis & Disposition
The prognosis of a suicidal patient is not a single trajectory but a function of whether the underlying disorder is treated, whether means are restricted, and whether the patient is held in care through the high-risk windows. The strongest prognostic facts: [1]
- A previous suicide attempt remains the dominant prognostic marker lifelong; repeat self-harm is common, and roughly 1 percent per year of recurrent self-harm patients eventually die by suicide.
- The highest-risk windows are the days to weeks after a recent attempt, after discharge from psychiatric admission, after a major loss or crisis, and during intoxication.
- Protective factors (engagement with treatment, social integration, responsibility for dependants, reasons for living) improve prognosis and are themselves modifiable targets of care. [1]
Disposition follows risk: high risk is admitted; moderate risk is managed by the crisis resolution and home treatment team (UK) or intensive outpatient equivalent with 24-to-48-hour review; low risk is managed by the GP and mental health team with a 7-day appointment. Every patient leaves with a safety plan, a named crisis pathway, and a booked follow-up — the absence of any of these is a system failure, not a clinical preference.[1][2]
Special Populations
- Adolescents. Use weight-based dosing where relevant; fluoxetine is the SSRI with the best paediatric safety evidence. Involve parents and school; refer to CAMHS. Recognise that NSSI in adolescence raises future suicide risk and must be assessed seriously at every contact.
- Pregnancy and postpartum. Untreated maternal depression is dangerous for mother and infant. Mother-and-baby admission is preferred where available. In psychotic postpartum depression, ECT is both safe and rapidly effective, and the risk of infanticide must be assessed. Lithium's teratogenicity (Ebstein anomaly) must be balanced against its anti-suicide benefit; sertraline is the SSRI with the lowest breast-milk transfer.
- Elderly. Smaller signs matter — a quiet, isolated man giving things away after bereavement is at high risk even without florid ideation. Sertraline is the preferred SSRI (fewer drug interactions, lower hyponatraemia risk than citalopram). Avoid tricyclics (anticholinergic load, orthostatic hypotension and falls, cardiac conduction effects). Treat pain, sensory impairment, and insomnia aggressively.
- Substance use. Integrated dual-diagnosis care; detoxification; relapse-prevention pharmacotherapy; never prescribe lethal quantities.
- Intellectual disability and autism. Adapt the assessment (behavioural equivalents, collateral from carers, visual supports); recognise that self-injury may serve a communicative function and that distress may not be verbally expressed.
- Cultural and Indigenous groups. Some communities (Indigenous Australians, Native Americans, several tribal and marginalised communities in India) carry disproportionately high rates rooted in intergenerational trauma, dispossession, and disconnection. Culturally safe, community-led services are not optional politeness — they are effective, and population-level approaches (community gatekeeper training, land-based healing, restriction of means) have the best evidence in these settings. [1]
Evidence, Guidelines & Regional Differences
The evidence base for suicide prevention is mature in some domains and deliberately humble in others. [1]
- Lithium and mood disorders. Cipriani and colleagues' updated meta-analysis (BMJ 2013) pooled randomised data and demonstrated that lithium reduces suicide and all-cause mortality in mood-disorder patients versus placebo and several active comparators. The anti-suicide effect is one of the few robustly replicated pharmacological findings in psychiatry.[4]
- Clozapine and schizophrenia. The InterSePT trial (Meltzer et al., Archives of General Psychiatry, 2003) randomised nearly 1,000 schizophrenia patients with suicidality to clozapine or olanzapine and showed clozapine superior on a composite suicide-prevention outcome, with fewer suicide attempts and rescue interventions.[3]
- Means restriction at population scale. Detoxification of domestic coal gas in mid-20th-century Britain, the UK 1998 paracetamol pack-size legislation (which cut paracetamol-related deaths and liver-unit admissions), firearm legislation after mass-casualty events, and barrier installation on high-suicide bridges all reduced method-specific suicide without full method substitution — strong natural-experiment evidence that restricting access to lethal means saves lives.[1]
- Brief contact interventions. The WHO SUPRE-MISS agenda and several randomised trials of brief follow-up contact (telephone, text, "caring letters") after discharge reduced subsequent suicide mortality, making follow-up contact a cheap, scalable, evidence-based intervention.
- Psychological therapies. CBT for suicide prevention and DBT reduce repeat self-harm in their target populations.
The controversy that examiners probe is the predictive validity of risk assessment. Systematic reviews (including Saab et al.) and methodological critiques (Large and colleagues) show that no risk-assessment tool or clinician judgement achieves positive predictive values above the very low single figures for individual suicide. This has driven a paradigm shift — articulated most clearly in NICE NG225 (UK, 2022) — from "predict and stratify" toward "needs assessment, collaborative safety planning, and compassionate continuity of care."[2]
[1] [1]Australia's LifeSpan trial and the National Suicide Prevention Strategy layer GP training, gatekeeper training, school programs, means restriction, and aftercare, recognising that no single intervention suffices and that population and clinical strategies must combine.
India — Mental Healthcare Act 2017. Attempted suicide is decriminalised; a person who attempts suicide is presumed to be "under severe stress" and entitled to rehabilitation by the state, not prosecution. The Act is rights-based, mandates advance directives, and decouples access to care from a criminal-justice gateway. Clinicians in India must frame suicide as a health event, not a crime.
Exam Pearls
- Previous attempt = single strongest predictor of future suicide (5 to 10-fold risk).
- Hopelessness predicts suicide better than depressive severity (Beck).
- Asking about suicide never increases risk — always ask directly.
- Lithium reduces suicide in mood disorders (Cipriani meta-analysis); clozapine reduces suicide in schizophrenia (InterSePT).
- Men complete suicide 3 to 4x more than women; women attempt more (gender paradox).
- High-lethality / low-rescue attempts and use of guns or hanging indicate high intent.
- Never discharge a post-attempt patient without psychiatric review.
- Means restriction (firearms, pack sizes, pesticide bans, bridge barriers) is one of the most effective population-level interventions.
- No-suicide contracts have NO protective value and are discouraged — use a safety plan.
- SAD PERSONS, IS PATH WARM, C-SSRS — know what each measures; know that none predicts individual suicide reliably.
- Acute risk window: first 1 to 2 weeks after psychiatric discharge; after a recent attempt; after loss or crisis; during intoxication.
- Suicide is not a crime in India since the Mental Healthcare Act 2017 — the person is presumed to be under severe stress and entitled to rehabilitation.
- Organophosphates are the leading means in rural India/Asia — resuscitate with atropine plus pralidoxime.
- Akathisia in a patient newly started on antipsychotics is a treatable, iatrogenic driver of suicide — do not miss it.
- Lithium has the best anti-suicide evidence; sertraline is the SSRI of choice in adults (and fluoxetine in under-18s); avoid tricyclics as first-line in those at risk because of lethality in overdose.
- Postvention — care for those bereaved by suicide — is part of prevention; bereaved relatives carry elevated suicide risk themselves. [1]
Exam application bank (NEET-PG / INICET)
One-line answer
Suicide is a leading cause of death worldwide. Risk assessment is a core clinical skill: ask directly about ideation, plan, intent, means, and preparatory acts. Risk factors (male sex, older/young adult age, psychiatric disorder — depression in 60 percent, previous attempt = strongest predictor, hopelessness, substance use, access to lethal means) are weighed against protective factors (social support, reasons for living). Risk stratification drives disposition: high risk = urgent admission; moderate = crisis team, remove means, safety plan; low = outpatient plus safety plan. ALWAYS document.
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Suicide Risk Assessment & Prevention.
References
- [1]Turecki G, Brent DA, Gunnell D, et al. Suicide and suicide risk Nat Rev Dis Primers, 2019.PMID 31649257
- [2]Saab MM, Murphy M, Meehan E, et al. Suicide and Self-Harm Risk Assessment: A Systematic Review of Prospective Research Arch Suicide Res, 2022.PMID 34193026
- [3]Meltzer HY, Alphs L, Green AI, et al. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT) Arch Gen Psychiatry, 2003.PMID 12511175
- [4]Cipriani A, Hawton K, Stockton S, Geddes JR. Lithium in the prevention of suicide in mood disorders: updated systematic review and meta-analysis BMJ, 2013.PMID 23814104