Rheumatology · Rheumatology
Ankylosing Spondylitis
Also known as Ankylosing spondylitis · AS · Radiographic axial spondyloarthritis (r-axSpA) · Morbus Bechterew · Marie-Strumpell disease · Spondyloarthritis, ankylosing
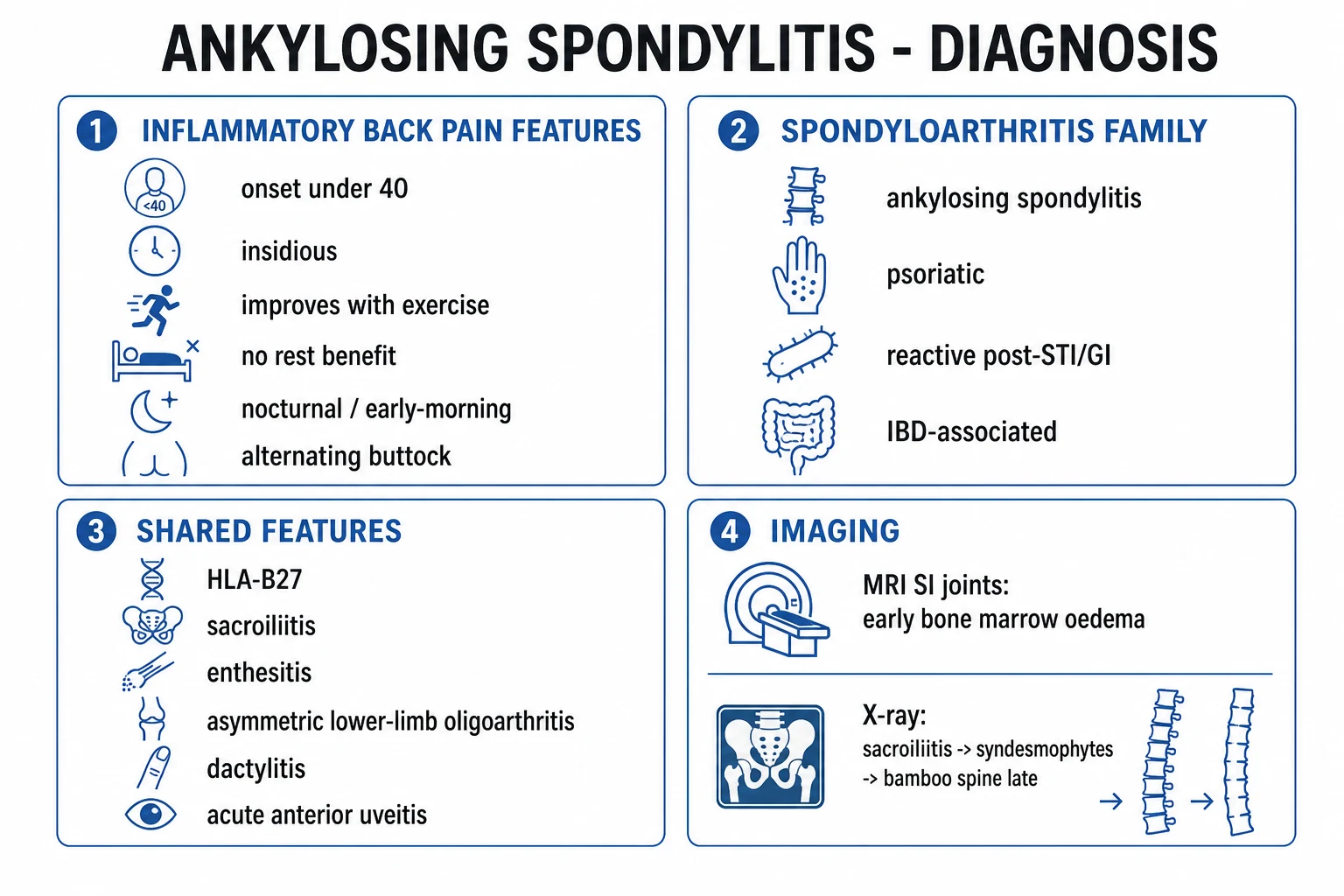
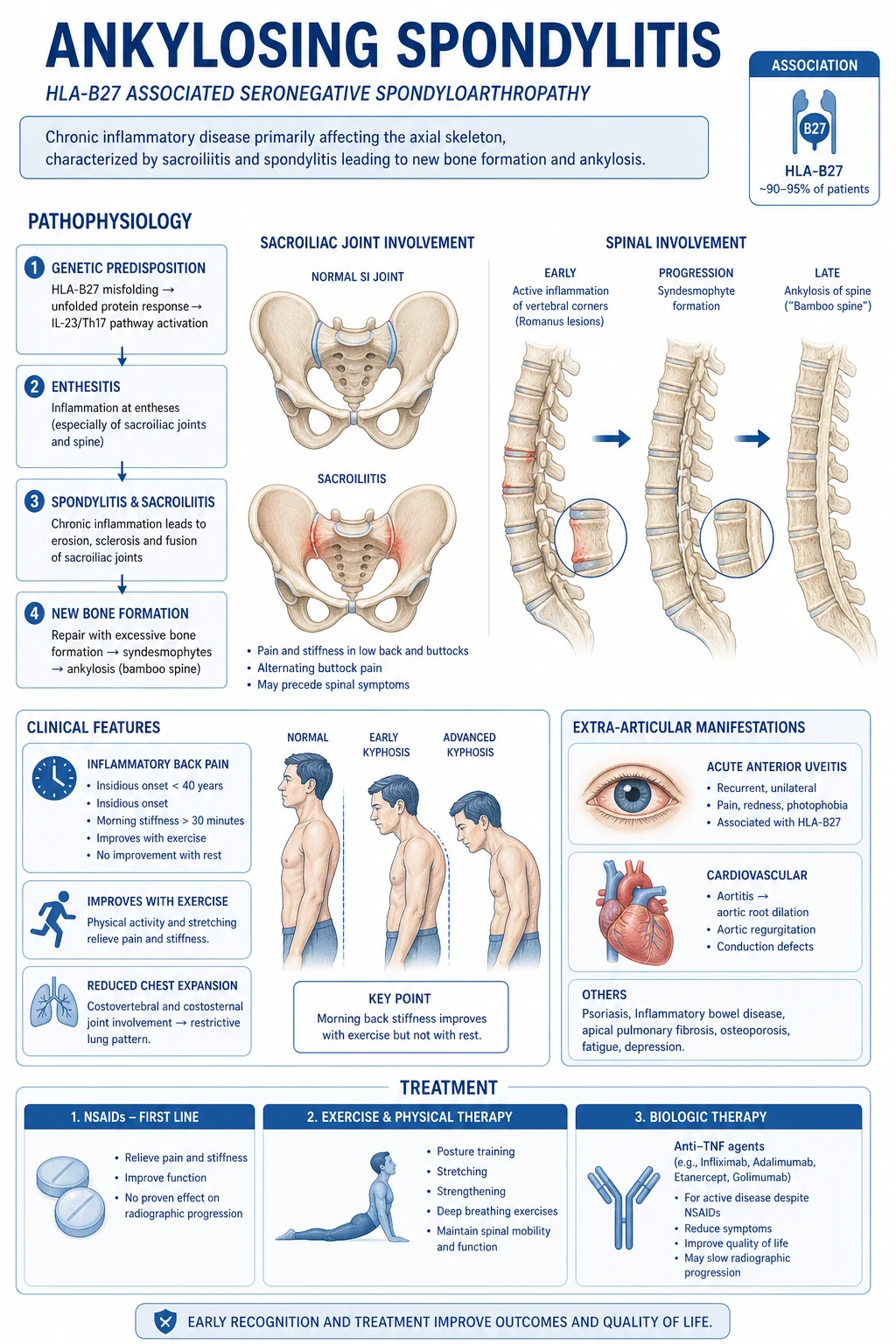
Ankylosing spondylitis (AS) is a chronic, progressive inflammatory disease of the axial skeleton and entheses — the prototype of the seronegative spondyloarthropathies. Strongly associated with HLA-B27 (about 90 percent). Presents as inflammatory back pain (insidious onset under 40 years, worse with rest, better with exercise, morning stiffness over 30 minutes, alternating buttock pain) with sacroiliitis (often bilateral and symmetric) and, late, a bamboo spine. Extra-articular: acute anterior uveitis (unilateral painful red eye), aortic regurgitation, apical lung fibrosis, secondary amyloidosis. Diagnosis by the modified New York criteria (1984) for established AS, or the ASAS 2009 criteria for the wider axial spondyloarthritis spectrum (which includes non-radiographic disease detectable on MRI). Management: continuous full-dose NSAIDs plus physiotherapy first-line; TNF inhibitors (adalimumab, etanercept, infliximab, golimumab, certolizumab) or IL-17 inhibitors (secukinumab, ixekizumab) for active disease; total hip replacement for hip arthritis. Treat to target: ASDAS under 1.3 or low disease activity.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags

Overview & Definition
Ankylosing spondylitis (AS) is a chronic, progressive, inflammatory disease of the axial skeleton (sacroiliac joints, spine) and the entheses (the sites where tendons, ligaments and joint capsules insert into bone) — and the prototype of the seronegative spondyloarthropathies (SpA).[1] The term seronegative denotes that both rheumatoid factor (RF) and antinuclear antibodies (ANA) are absent, in contrast to rheumatoid arthritis. The core pathological process is enthesitis (inflammation at enthesis) which evolves into erosion, repair, new-bone formation and finally ankylosis (bony fusion of a joint).[1]
AS is now understood as the radiographic end of a single continuous spectrum called axial spondyloarthritis (axSpA):[3]
- Non-radiographic axial spondyloarthritis (nr-axSpA) — active sacroiliitis on MRI (bone-marrow oedema) but a normal plain pelvic X-ray.
- Radiographic axial spondyloarthritis (r-axSpA) — classical AS — definite sacroiliitis on plain X-ray (bilateral grade 2 or unilateral grade 3 or more). [1]
The two are not different diseases; nr-axSpA may — but does not always — progress to AS over years. The clinical skill in AS is recognising inflammatory back pain (most back pain in the community is mechanical), requesting the right imaging (plain X-ray plus MRI of the sacroiliac joints), and escalating to a biologic when conventional therapy fails — while remaining alert to the extra-articular emergencies (acute anterior uveitis, spinal fracture in a fused spine, cauda equina syndrome). [1]
Classification
Seronegative spondyloarthropathies — the family
The seronegative SpAs share a unifying set of features and are grouped because of overlapping genetics, clinical pattern and pathology:[1]
- Ankylosing spondylitis — axial prototype (this topic).
- Psoriatic arthritis — skin/nail psoriasis; DIP involvement; pencil-in-cup deformity; asymmetric oligoarthritis.
- Reactive arthritis (formerly Reiter syndrome) — 1 to 4 weeks after a GI (Salmonella, Shigella, Campylobacter, Yersinia) or GU (Chlamydia) infection; classic triad of arthritis, urethritis, conjunctivitis; keratoderma blennorrhagicum and circinate balanitis.
- Enteropathic (IBD-associated) arthritis — associated with Crohn disease and ulcerative colitis; axial pattern mirrors AS; peripheral pattern mirrors the bowel flare.
- Undifferentiated spondyloarthritis — features of SpA that do not fulfil a specific subtype. [1]
Shared (unifying) features of the SpA family — the high-yield list: [1]
- Inflammatory back pain; sacroiliitis (often bilateral in AS).
- Asymmetric, predominantly lower-limb oligoarthritis.
- Enthesitis (especially Achilles tendon and plantar fascia insertions — heel pain).
- Dactylitis ("sausage digit").
- HLA-B27 association and positive family history.
- Acute anterior uveitis.
- Mucocutaneous features (psoriasis, oral ulcers, keratoderma, balanitis, nail dystrophy).
- RF negative, ANA negative (seronegative). [1]
Diagnostic and classification criteria (reproduced verbatim)
Modified New York criteria (1984) for the diagnosis of established AS — used when X-ray sacroiliitis is already present:[2]
- Diagnosis requires the radiographic criterion PLUS at least one clinical criterion:
- Radiographic criterion: sacroiliitis on X-ray graded bilateral grade 2 or more, OR unilateral grade 3 or more.
- Clinical criteria (any one):
- Low back pain and stiffness for more than 3 months that improves with exercise but is not relieved by rest.
- Limitation of motion of the lumbar spine in both the sagittal and frontal planes.
- Limitation of chest expansion relative to normal values corrected for age and sex. [1]
Sacroiliitis radiographic grade (mNY system): [1]
| Grade | Appearance |
|---|---|
| 0 | Normal |
| 1 | Suspicious change |
| 2 | Minimal abnormality — small localised areas with erosion or sclerosis, without alteration in joint width |
| 3 | Unequivocal abnormality — moderate or advanced sacroiliitis with one or more of erosions, evidence of sclerosis, widening, narrowing or partial ankylosis |
| 4 | Severe abnormality — total ankylosis |
ASAS classification criteria for axial spondyloarthritis (2009) — for patients where plain X-ray may be normal (i.e. to capture nr-axSpA):[3]
- Entry criterion: back pain (greater than or equal to 3 months) with onset under 45 years.
- Then either arm:
- Imaging arm: sacroiliitis on imaging (X-ray — high grade — or active inflammation on MRI) PLUS at least one SpA feature.
- Clinical arm: HLA-B27 positive PLUS at least two other SpA features.
- SpA features (11): inflammatory back pain; arthritis; enthesitis (heel); uveitis (anterior); dactylitis; psoriasis; Crohn disease / ulcerative colitis; good response to NSAIDs; family history of SpA; HLA-B27 positive; elevated CRP.
- Sensitivity about 83 percent overall; 97 percent with HLA-B27-positive disease; specificity 84 to 94 percent (the imaging arm is more specific). [1]
ASAS classification criteria for peripheral spondyloarthritis (2011) — for patients with predominantly peripheral disease (arthritis or enthesitis or dactylitis):[5]
- Entry: arthritis or enthesitis or dactylitis.
- PLUS (a) at least two of: psoriasis, prior infection, HLA-B27, sacroiliitis on imaging; OR (b) at least one of those four PLUS at least two of: arthritis, enthesitis, dactylitis, inflammatory back pain, family history (with elevated CRP). [1]
Criteria for inflammatory back pain
The two widely used IBP criteria sets, both reproduced because they are examiner favourites: [1]
- Calin criteria (1977) — requires 4 of 5: (1) age of onset under 35; (2) duration over 3 months; (3) insidious onset; (4) morning stiffness; (5) improvement with exercise. (Sensitivity high, specificity modest.)
- ASAS (Berlin) criteria (2006) — requires 2 of 4: (1) morning stiffness over 30 minutes; (2) improvement with exercise, not with rest; (3) back pain waking the patient in the second half of the night; (4) alternating buttock pain. (Sensitivity 70 percent, specificity 81 percent.) [1]
Epidemiology & Risk Factors
AS is the commonest inflammatory rheumatic disease in young men, with a global prevalence that closely tracks the population carriage of HLA-B27:[1]
- Prevalence: about 0.1 to 0.4 percent of European adults; 0.5 percent in the USA; 0.1 to 0.2 percent in India; rare in Japan and sub-Saharan Africa (low HLA-B27 carriage).
- HLA-B27 carriage in the general population: about 8 percent of white Europeans and Americans, up to 14 percent in some Northern European groups; 6 to 8 percent in North India, but only 1 to 2 percent in South India and Japan, and near zero in Australian Aboriginal, African and Inuit populations — explaining the geography of AS.
- Among HLA-B27-positive individuals, only about 1 to 5 percent develop AS; in those with an affected first-degree relative the risk rises to about 10 to 20 percent. [1]
Sex ratio: historically quoted as 3:1 male:female; modern series are closer to 2:1. Women are increasingly recognised because their disease is milder, more peripheral, less radiographically advanced, and chronically under-diagnosed.[1]
Age of onset: the typical patient is in the late teens to mid-thirties; onset over 45 years excludes the ASAS axSpA entry criterion and should prompt a search for another cause (DISH, malignancy, fracture, infection). [1]
Risk factors (high-yield): [1]
- Genetic: HLA-B27 is the dominant genetic factor (explains about 30 percent of total heritability). HLA-B27 subtypes: B*2705 (whites, Africans, Indians), B*2704 (Chinese, Japanese, Thai), B*2702 (Mediterranean), B*2707 — all disease-associated; B*2706 (South-East Asia) and B*2709 (Sardinia) are protective. Additional loci: ERAP1, ERAP2, IL23R, TNFRSF1A, RUNX3, KIF21B — together over 100 loci.
- ERAP1-HLA-B27 epistasis (exam favourite): ERAP1 (an endoplasmic-reticulum aminopeptidase that trims peptides before HLA loading) only increases AS risk in HLA-B27-positive patients — strong genetic evidence that the disease mechanism is peptide-presentation dependent.
- Family history: first-degree relative risk is 5- to 16-fold higher.
- Smoking: the strongest modifiable risk factor for radiographic progression; smokers progress about twice as fast on the mSASSS scoring of syndesmophytes.
- Gut microbiome / Klebsiella hypothesis: an ecological (but unproven) link between intestinal Klebsiella and disease flares; the modern view focuses on dysbiosis and IL-23-driven gut-enthesis axis rather than a single organism.
- Male sex, family history, elevated CRP at baseline, smoking, hip arthritis and young onset are the predictors of severe radiographic progression. [1]
Pathophysiology
The enthesis is the primary lesion
AS is fundamentally a disease of the enthesis — the insertion of tendon, ligament or joint capsule into bone. The enthesis is a mechanically stressed transition zone (fibrocartilage over mineralised fibrocartilage over subchondral bone). Mechanical stress, microdamage and bacterial/gut antigens in a genetically susceptible host trigger a sterile inflammatory cascade at the enthesis, which then secondarily involves the adjacent joint (e.g. the sacroiliac joint).[1]
The classic morphological cascade in the spine: [1]
- Enthesitis at the annulus fibrosus attachment to the vertebral rim.
- Erosion of the vertebral corner — the Romanus lesion ("shiny corner" on lateral X-ray).
- Repair with new bone — the syndesmophyte grows in the direction of the annulus fibrosus, delicately and symmetrically (in contrast to the bulky, asymmetric, asymmetrically-flowing new bone of DISH).
- Bridging of adjacent vertebrae → bamboo spine.
- In the sacroiliac joint the same erosion-sclerosis-ankylosis sequence produces bilateral symmetric sacroiliitis. [1]
Cellular and cytokine players
The inflammatory infiltrate in active lesions comprises CD4+ and CD8+ T lymphocytes, macrophages, mast cells and innate lymphoid cells, producing a TNF-alpha and IL-17A-rich milieu. IL-23 (produced locally and derived from entheseal-resident gamma-delta T cells and type-3 innate lymphoid cells) drives IL-17A and IL-22 production, which promote both inflammation and pathological osteoproliferation.[1]
How HLA-B27 drives disease (three hypotheses)
The mechanism by which HLA-B27 causes AS is one of the great unsolved problems in immunology. Three non-mutually-exclusive hypotheses:[1]
- Arthritogenic-peptide hypothesis: HLA-B27 presents a specific (bacterial or self) peptide to CD8+ T cells that cross-reacts with an entheseal self-antigen. Supported by clonal T-cell expansions in the joints.
- Misfolding / unfolded-protein-response (UPR) hypothesis: HLA-B27 folds slowly in the endoplasmic reticulum, accumulating misfolded heavy chains that trigger the UPR and downstream IL-23 production.
- Free heavy-chain / cell-surface homodimer hypothesis: HLA-B27 heavy-chain homodimers on the cell surface engage KIR3DL2 on NK and Th17 cells, expanding the IL-17-producing Th17 compartment and activating innate immunity independent of peptide presentation. [1]
The bone-formation paradox
A cardinal puzzle: anti-inflammatory therapy (NSAIDs, TNF inhibitors) controls inflammation and symptoms but does not reliably halt radiographic progression — new bone continues to form. Current understanding implicates the Wnt/beta-catenin signalling pathway: inflammation upregulates DKK-1 and sclerostin (Wnt antagonists) which then fall as inflammation resolves, removing the brake on osteoblasts and permitting syndesmophyte formation. This explains why suppressive therapy alone cannot prevent ankylosis. [1]
Earliest lesion — bone marrow oedema on MRI
The earliest detectable lesion is bone-marrow oedema (osteitis) of the subchondral bone of the sacroiliac joint, visible on STIR or T2 fat-saturated MRI as bright signal. This precedes plain X-ray changes by several years and is the basis on which nr-axSpA is diagnosed.[4]
Gut-enthesis axis
Subclinical intestinal inflammation is found on ileocolonoscopy in up to two-thirds of AS patients, with IL-23 over-expression in the gut mucosa. This links the enthesis to a dysregulated mucosal immune system and helps explain why IL-23 pathway blockade helps psoriasis and peripheral SpA but — paradoxically — has failed in axSpA (see Evidence section). [1]
Clinical Presentation
The cardinal feature — inflammatory back pain
The typical patient is a young man (under 40) with insidious-onset low-back and buttock pain that has been present for more than 3 months. The pain is worse at rest and at night (often waking the patient in the second half of the night) and is relieved by exercise and movement; it is accompanied by morning stiffness of more than 30 minutes (often 1 to 2 hours). It may alternate between the two buttocks (a key distinguishing feature from mechanical pain).[1]
This inflammatory pattern is the single highest-yield clinical observation — most back pain in the community is mechanical (worse with activity, better with rest). Use the ASAS (Berlin) criteria for IBP (2 of 4 — see Classification). [1]
Other axial and chest-wall features
- Sacroiliac pain — deep, dull, over the SI joints.
- Reduced spinal mobility in all planes (flexion, extension, lateral flexion, rotation).
- Reduced chest expansion — enthesis-driven costovertebral and sternocostal inflammation — causing restrictive chest-wall mechanics (lungs remain structurally normal; the problem is mechanical). Often an early symptom.
- Cervical involvement — late; progressive loss of rotation and extension, with risk of atlantoaxial subluxation.
- Kyphotic deformity in advanced disease — "question-mark" posture with fixed forward gaze. [1]
Peripheral musculoskeletal features
- Asymmetric, predominantly lower-limb oligoarthritis (hip, knee, ankle) — hips are particularly important because hip involvement is the strongest predictor of poor functional outcome.
- Enthesitis — pain at the Achilles tendon insertion and the plantar fascia origin ("heel pain") is highly characteristic.
- Dactylitis — "sausage digit" of a toe or finger.
- Arthritis of the shoulder — frequently affected (glenohumeral enthesitis). [1]
Extra-articular manifestations
The extra-articular triad and beyond — every system is examinable:[1]
Ocular (20 to 40 percent): [1]
- Acute anterior uveitis (AAU, iritis) — classically unilateral, acute onset, painful red eye with photophobia, lacrimation and blurred vision. May precede the spinal symptoms by years. A medical emergency — untreated attacks cause posterior synechiae, glaucoma and cataract. [1]
Cardiovascular: [1]
- Aortic regurgitation (aortic root dilatation and aortitis) — about 2 to 10 percent; may need valve replacement.
- Conduction defects — first-degree AV block, complete heart block, bundle-branch block.
- Increased risk of ischaemic heart disease and stroke (chronic inflammation accelerates atherosclerosis). [1]
Respiratory: [1]
- Apical pulmonary fibrosis — upper-lobe fibrotic change that can cavitate and be colonised by Aspergillus or mycobacteria (often mistaken for TB).
- Restrictive defect from chest-wall ankylosis. [1]
Renal: [1]
- Secondary (AA) amyloidosis — the most serious renal complication; presents as proteinuria, nephrotic syndrome or renal failure; biopsy shows apple-green birefringence with Congo red.
- IgA nephropathy. [1]
Neurological: [1]
- Cauda equina syndrome — late, due to expansion of the lumbosacral spinal canal by chronic dural inflammation; presents with progressive lower-limb weakness, sensory disturbance, saddle anaesthesia and sphincter dysfunction.
- Atlantoaxial subluxation with cervical cord compression.
- Spinal fracture with cord injury (see Complications). [1]
Gastrointestinal: [1]
- Clinical or subclinical inflammatory bowel disease (Crohn, UC) in 5 to 10 percent. [1]
Skin / mucous membranes: [1]
- Psoriasis association (overlap with psoriatic arthritis). [1]
Constitutional: [1]
- Fatigue is a major, often disabling symptom and a core component of disease activity scores; low-grade fever and weight loss may occur. [1]
Atypical presentations
- Juvenile-onset (JAS / enthesitis-related arthritis, ERA): children/adolescents; enthesitis and asymmetric lower-limb oligoarthritis dominate, with axial involvement appearing years later; uveitis is usually acute (in contrast to the chronic asymptomatic uveitis of JIA).
- Female sex: milder, less radiographic damage, more peripheral arthritis, often delayed diagnosis by 5 to 10 years.
- Late-onset AS in the elderly: rare; may present with advanced silent disease (kyphosis, bamboo spine) discovered after a fracture.
- Immunocompromised host: atypical infection (TB, fungal) and biologic complications complicate interpretation; normal CRP does not exclude active disease. [1]
Differential Diagnosis
A young person with back pain is not always AS. The complete differential with distinguishing features:[1]
The SpA family — mnemonic
PAIR
skin/nail psoriasis, DIP pencil-in-cup, asymmetric oligoarthritis
inflammatory back pain, bilateral sacroiliitis, HLA-B27, uveitis
Crohn/UC-associated; or 1 to 4 weeks after GI/GU infection
post-infectious triad — arthritis, urethritis, conjunctivitis; keratoderma blennorrhagicum, circinate balanitis
Mechanical / degenerative low back pain — the commonest mimic. Acute onset, worse with activity, better with rest, no morning stiffness, no night pain, normal inflammatory markers, normal SI imaging. The single discriminator question is "is the pain worse with rest and better with exercise?" — yes points to AS. [1]
Lumbar disc herniation — radicular pain following a dermatome, worse on sitting, positive straight-leg raise, neurological signs (reflex change, motor or sensory deficit). No morning stiffness. [1]
Lumbar spinal stenosis — older patient, neurogenic claudication (leg pain on walking relieved by sitting/forward flexion), narrow canal on MRI. [1]
Diffuse idiopathic skeletal hyperostosis (DISH, Forestier disease) — older men (over 50), flowing ossification along the anterolateral spine (at least 4 contiguous vertebrae) on X-ray, normal SI joints, normal inflammatory markers, no HLA-B27 association. The bone is bulky and asymmetric (vs delicate symmetric syndesmophytes of AS). Often an incidental finding. [1]
Osteitis condensans ilii — typically postpartum women, triangular sclerosis on the iliac side of the SI joint with a normal joint space; sacroiliac joint is otherwise intact. Often asymptomatic. [1]
Psoriatic arthritis (axial) — skin/nail psoriasis, asymmetric sacroiliitis, DIP involvement, pencil-in-cup deformity, J-sign/ivory phalanx. Distinguish by skin and the asymmetric, bulky new bone. [1]
Reactive arthritis — 1 to 4 weeks after GI or GU infection, oligoarthritis of the lower limbs, enthesitis, dactylitis, plus mucocutaneous features (keratoderma blennorrhagicum, circinate balanitis, painless oral ulcers) and conjunctivitis/urethritis. Often self-limiting over months. [1]
IBD-associated arthritis — axial pattern mirrors AS; peripheral pattern mirrors the bowel disease (flares with colitis). Distinguish by bowel symptoms and endoscopy. [1]
Infectious sacroiliitis (pyogenic, tuberculous) — unilateral, severe pain, systemically unwell, fever, raised CRP, positive blood/culture, MRI shows collection/osteomyelitis. TB should be considered where TB is endemic (e.g. India). [1]
Vertebral malignancy (metastases, multiple myeloma) — older patient, nocturnal pain, systemic features, weight loss, lytic or blastic lesions on imaging. No morning stiffness; SI joints usually spared. [1]
Osteoporotic vertebral compression fracture — elderly or chronic-steroid patient, acute onset, wedge deformity on X-ray. [1]
Fibromyalgia — widespread pain, fatigue, sleep disturbance, normal inflammatory markers and normal imaging; tender points. [1]
Clinical & Bedside Assessment
A focused examination is the single most reliable bedside tool in established AS. Always assess spinal mobility, chest expansion, SI-joint provocation, entheses, eyes, heart, chest, skin, peripheral joints and neurology.[1]
Spinal mobility — the named measurements
Modified Schober test (lumbar flexion): patient stands erect; mark the midpoint of a line joining the two posterior superior iliac spines (the lumbosacral dimples, ~at L5); mark a second point 10 cm above the first; ask the patient to flex forward as far as possible; measure the new distance between the marks. Increase of less than 5 cm (i.e. final distance under 15 cm) indicates reduced lumbar flexion. (The "modified" version adds marks 5 cm below and 10 cm above to improve reliability.) Sensitive for lumbar flexion. [1]
Occiput-to-wall distance (Moll-Wright test, cervical and thoracic extension): patient stands with heels and back against a wall, head in natural position. Measure the distance from the occiput to the wall. More than 5 cm indicates fixed flexion deformity of the cervical and upper thoracic spine. [1]
Chest expansion: measure at the fourth intercostal space (or just below the axillae) at maximal inspiration minus maximal expiration. Less than 2.5 cm (some standards use less than 5 cm) indicates reduced chest-wall mobility — an early sign. [1]
Cervical rotation: total degrees of rotation of the head with the shoulders fixed. [1]
Lateral lumbar flexion: distance from fingertip to floor on lateral bending. [1]
Intermalleolar distance: maximal distance between the medial malleoli with the legs abducted — reflects hip mobility. [1]
BASMI (Bath Ankylosing Spondylitis Metrology Index): combines 5 measurements — cervical rotation, tragus-to-wall distance, lumbar flexion (modified Schober), lumbar side flexion, and intermalleolar distance — into a 0 to 10 score of spinal mobility. [1]
SI-joint provocation manoeuvres
- Gaenslen's test — patient supine, one leg flexed to chest, the other leg dropped off the table; the examiner applies downward pressure on the dropped leg. Pain in the SI joint on the extended side is positive.
- FABER (Patrick) test — affected leg Flexed, ABducted, Externally Rotated; pain in the SI joint or hip is positive.
- Compression / distraction tests of the pelvis. [1]
These manoeuvres are sensitive but poorly specific (mechanical back pain also reproduces them); use to support, not to confirm. [1]
Entheses, peripheral joints and extra-articular exam
- Palpate the Achilles tendon insertion and plantar fascia origin — tenderness = enthesitis.
- Examine hips (loss of internal rotation is earliest), knees, ankles.
- Ophthalmology: red eye, photophobia, cataract, synechiae.
- Cardiac: aortic regurgitation murmur (early diastolic, decrescendo at the left sternal edge).
- Respiratory: apical crackles, reduced chest expansion.
- Abdomen: hepatosplenomegaly (IBD overlap).
- Skin and nails: psoriasis, keratoderma, nail dystrophy.
- Neurology: long-tract signs, sphincter dysfunction (cauda equina). [1]
Investigations
No single test diagnoses AS — diagnosis is clinical plus imaging, with HLA-B27 and inflammatory markers in a supporting role.[1][3]
Imaging
Plain X-ray — sacroiliac joints (AP pelvis and dedicated oblique SI views; Ferguson view): the radiographic progression follows the pathological cascade: [1]
- Blurring of the subchondral bone plate.
- Erosions and juxta-articular osteoporosis.
- Sclerosis (especially on the iliac side, which has thinner cartilage).
- Joint-space narrowing, then partial ankylosis, then complete ankylosis.
- The process is classically bilateral and symmetric (unlike the asymmetric sacroiliitis of psoriasis/reactive arthritis, or unilateral change of infection). [1]
Plain X-ray — lumbar and thoracic spine: [1]
- Romanus lesion (shiny corner) — erosions with sclerosis at the anterosuperior vertebral corner (the enthesitis lesion); an early finding.
- Squaring of vertebral bodies (erosion of the normal concavity of the anterior vertebral body).
- Syndesmophytes — delicate, vertical bony outgrowths bridging adjacent vertebrae along the annulus fibrosus.
- Bamboo spine — late; a row of bridging syndesmophytes gives a "bamboo" appearance on AP view.
- Dagger sign — ossification of the supraspinous and interspinous ligaments seen as a central vertical radio-opacity on AP view.
- Trolley-track sign — three vertical lines on AP view (one central, two lateral — ossified ligaments and facet joints). [1]
MRI — sacroiliac joints (the cornerstone for nr-axSpA): STIR or T2 fat-saturated sequences show high signal bone-marrow oedema (osteitis) indicating active inflammation — the earliest lesion, preceding X-ray by years. T1-weighted sequences show structural damage (erosions, fat metaplasia, ankylosis). The ASAS/OMERACT consensus definition of active sacroiliitis on MRI requires bone-marrow oedema (high signal on STIR/T2FS), highly suggestive of SpA, visible on at least two consecutive slices OR present on a single slice if more than one lesion is seen. Plain X-ray shows only the late consequence; MRI changes the game for early diagnosis.[4]
MRI — spine: reveals corner inflammatory lesions (Romanus lesions) and discover other early changes invisible on X-ray. [1]
DEXA (bone densitometry): osteoporosis is common (chronic inflammation plus immobility). The lumbar-spine BMD is falsely elevated by syndesmophytes — always measure the femoral neck. [1]
Laboratory
- HLA-B27 — positive in about 90 percent of patients with AS (sensitivity high). Supportive, not diagnostic — about 8 percent of the general population are HLA-B27-positive but never develop AS, and a negative result does not exclude AS (especially in non-white populations). Most useful in nr-axSpA with IBP when imaging is equivocal.
- CRP and ESR — elevated in about 50 to 70 percent of patients with active disease. A normal CRP does NOT exclude AS. CRP is a component of ASDAS (below).
- Rheumatoid factor (RF) and ANA — negative (the definition of "seronegative").
- CBC — anaemia of chronic disease (normocytic normochromic); thrombocytosis in active disease.
- Renal and liver function, urinalysis — baseline before therapy; watch for amyloidosis (proteinuria).
- Pre-biologic screen: tuberculosis (interferon-gamma release assay / IGRA — Quantiferon-TB Gold — plus chest X-ray), hepatitis B and C, HIV, complete blood count and liver function; ECG in patients with cardiac involvement before TNF inhibitors. [1]
Disease-activity and metrology scores (reproduced verbatim)
ASDAS (Ankylosing Spondylitis Disease Activity Score) — the preferred composite, ASDAS-CRP:[8]
ASDAS-CRP = 0.12 × √(back pain) + 0.06 × (duration of morning stiffness) + 0.07 × CRP(mg/L) + 0.12 × (peripheral pain/swelling) + 0.06 × (patient global, 0–10) (Back pain, peripheral pain, and patient global are 0 to 10 patient-reported visual analogue scales; morning stiffness is 0 to 10.) [1]
Disease-activity bands (ASDAS): [1]
- Less than 1.3 — inactive disease.
- 1.3 to under 2.1 — moderate disease activity.
- 2.1 to under 3.3 — high disease activity.
- 3.3 or more — very high disease activity. [1]
Improvement: [1]
- Clinically important improvement — change of 1.1 or more.
- Major improvement — change of 2.0 or more. [1]
BASDAI (Bath Ankylosing Spondylitis Disease Activity Index) — six 0 to 10 patient questions (fatigue, spinal pain, joint pain/swelling, enthesitis, morning stiffness severity and duration), averaged; a BASDAI over 4 (on two occasions) supports starting a biologic. [1]
BASFI (Bath Ankylosing Spondylitis Functional Index) — 10-item functional measure. [1]
BASMI — spinal mobility (see Clinical Assessment). [1]
Management — Resuscitation
AS is not usually a resuscitation diagnosis — but several complications are time-critical: [1]
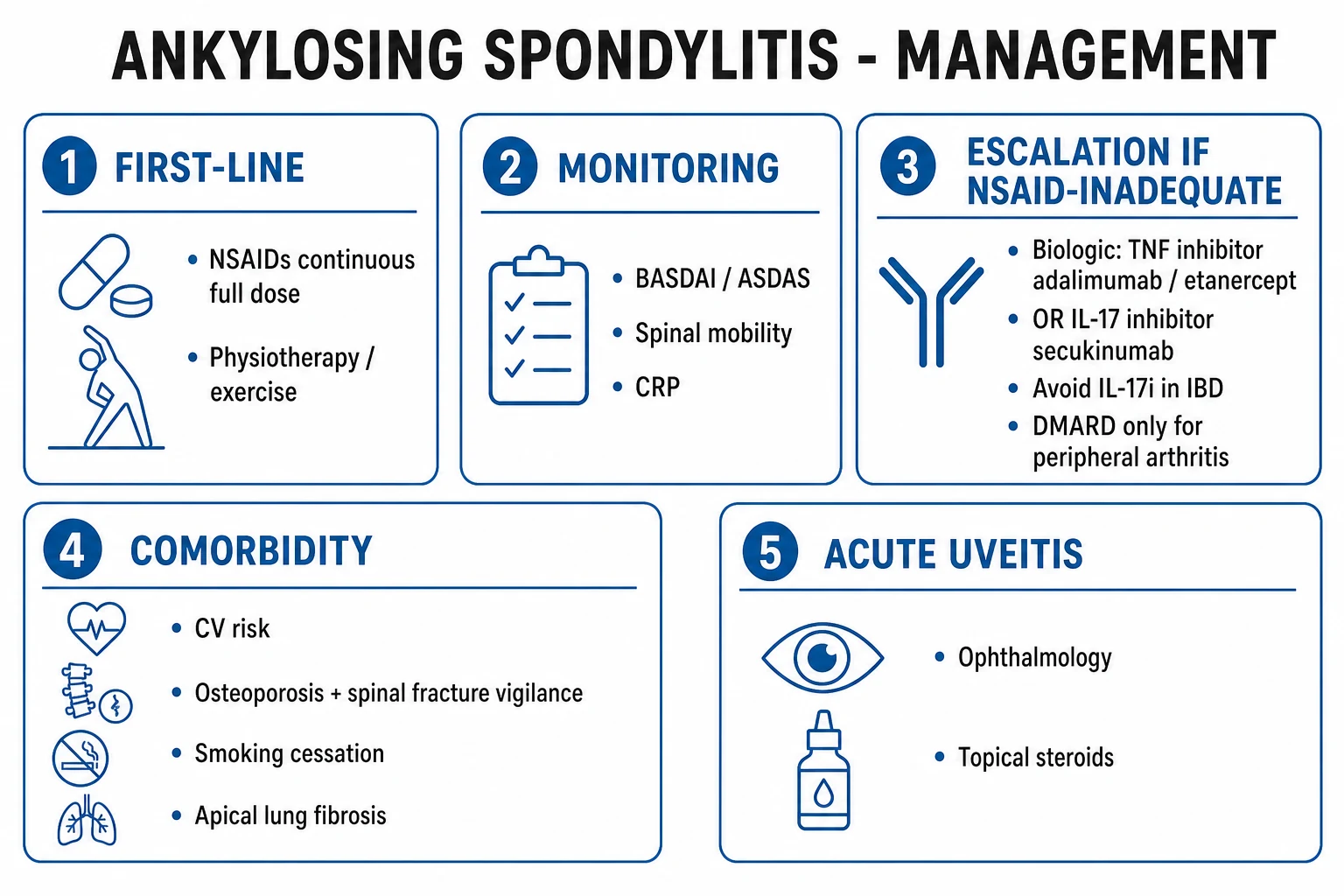
- Acute anterior uveitis — ophthalmology referral within 24 hours. Treatment: topical corticosteroid (prednisolone acetate 1 percent drops hourly while awake for severe attacks, then taper) and a cycloplegic (homatropine 2 percent or cyclopentolate 1 percent drops twice daily) to relieve ciliary spasm and prevent posterior synechiae. Periocular or systemic steroids for severe or non-responsive cases. Untreated attacks cause synechiae, glaucoma and cataract. Recurrent AAU is an indication to favour an anti-TNF monoclonal antibody (adalimumab, infliximab, certolizumab) over etanercept, which paradoxically worsens or fails to control uveitis.[10]
- Suspected cervical-spine fracture in a fused spine — assume instability; immobilise in-line (rigid collar, sandbags, manual in-line stabilisation), obtain whole-spine CT and MRI (X-rays are unreliable in a fused spine), and involve neurosurgery/orthopaedic spinal surgery. Even minor trauma (e.g. a fall from standing, a low-speed RTA) can produce a highly unstable fracture with high paraplegia and mortality. Patients should be counselled about this risk before any trauma.
- Cauda equina syndrome — urgent MRI and neurosurgical referral; usually surgical decompression. Presents insidiously with leg weakness, sensory change, sphincter dysfunction.
- Aortic regurgitation with heart failure — cardiology, echocardiography; may require aortic valve replacement and root repair. High-grade AV block — cardiology, pacemaker.
- Pre-biologic latent TB — if the IGRA is positive or CXR suggests old TB, treat latent TB (per national guidelines: e.g. isoniazid 300 mg daily for 6 to 9 months or rifampicin 600 mg daily for 4 months) before starting any TNF inhibitor; defer biologic at least 1 month after starting LTBI therapy.
Management — Definitive & Stepwise
AS is managed by a multidisciplinary team (rheumatologist, physiotherapist, ophthalmologist, orthopaedic surgeon, with cardiology and gastroenterology as needed) using a treat-to-target approach.[6][8][10]
Treat-to-target (ASAS-EULAR 2022)
The target is clinical remission or low disease activity — operationally an ASDAS under 1.3 (or, where ASDAS is unavailable, a BASDAI under 4 with normal CRP). The decision is shared with the patient, with regular monitoring of disease activity, function, drug toxicity and comorbidity. [1]
Step 1 — NSAIDs (first-line, at full dose, continuous)
NSAIDs are first-line for symptom control and — at full anti-inflammatory dose, given continuously rather than on demand — may slow radiographic progression (Cochrane/modest effect, strongest for patients with elevated CRP).[7][8] Try two different NSAIDs over 4 weeks before declaring failure. Options:
| NSAID | Dose | Frequency |
|---|---|---|
| Naproxen | 500 mg oral | twice daily |
| Diclofenac | 50 to 75 mg oral | twice to three times daily |
| Indometacin | 25 to 50 mg oral | three times daily (often favoured for AS) |
| Ibuprofen | 400 to 800 mg oral | three to four times daily |
| Celecoxib | 100 to 200 mg oral | twice daily (COX-2 selective) |
| Etoricoxib | 60 to 90 mg oral | once daily (COX-2 selective; not available in USA) |
Add a proton-pump inhibitor (omeprazole 20 mg daily) for patients with GI risk. Avoid NSAIDs in significant renal impairment (CKD stage 3B or worse), severe heart failure, active peptic ulcer, anticoagulation, late pregnancy (after 28 to 30 weeks — premature closure of the ductus arteriosus and oligohydramnios), and prior NSAID hypersensitivity. [1]
Step 2 — Physiotherapy and exercise (non-negotiable)
Daily stretching, postural exercises, spinal-mobility drills, swimming, and deep-breathing exercises to maintain chest expansion — are as important as drugs. Supervised group physiotherapy (or hydrotherapy) is cost-effective and is the only intervention with long-term outcome benefit on mobility. Smoking cessation is mandatory. [1]
Step 3 — Local glucocorticoid injections
Intra-articular glucocorticoid injections (e.g. triamcinolone acetonide 40 mg into the SI joint under imaging, or into a peripheral joint or enthesis) are useful for focal inflammation. Systemic (oral or IV) glucocorticoids are NOT recommended for axial disease — they are ineffective and high-toxicity.[10]
Step 4 — Biologic DMARDs (bDMARDs)
Indicated for persistent high disease activity despite an adequate trial of NSAIDs (and csDMARDs where there is peripheral arthritis) — operationalised as ASDAS 2.1 or more (or BASDAI over 4) on two occasions.[6][8][10]
TNF inhibitors (first-line biologic) — equivalent efficacy; choice often dictated by comorbidity: [1]
| Agent | Dose and route | Notes |
|---|---|---|
| Adalimumab | 40 mg subcutaneous every 2 weeks | Monoclonal antibody; effective for AAU and IBD |
| Etanercept | 50 mg subcutaneous weekly | Fusion protein; avoid for AAU and IBD |
| Infliximab | 5 mg/kg IV every 6 to 8 weeks (loading at weeks 0, 2, 6) | Monoclonal; effective for AAU and IBD |
| Golimumab | 50 mg subcutaneous monthly | Convenient; effective for AAU and IBD |
| Certolizumab pegol | 400 mg at weeks 0, 2, 4, then 200 mg every 2 weeks (or 400 mg every 4 weeks) | Monoclonal; minimal placental transfer — preferred in pregnancy; effective for AAU and IBD |
Pre-biologic screen: TB (IGRA and CXR), HBV/HCV, HIV, CBC, LFT, renal, pregnancy test, vaccine update (see below). Contraindications: active infection (including latent TB untreated), demyelinating disease (multiple sclerosis — TNFi relative contraindication), moderate-to-severe heart failure (NYHA III/IV — TNFi caution), recent or active malignancy (case-by-case), live vaccines. [1]
IL-17 inhibitors (second-line biologic; first-line if TNFi contraindicated): [1]
| Agent | Dose and route | Notes |
|---|---|---|
| Secukinumab | 150 mg SC at weeks 0, 1, 2, 3, 4, then monthly (some use 300 mg in psoriasis overlap) | MEASURE 1–4 trials; rapid response |
| Ixekizumab | 160 mg loading SC, then 80 mg every 2 weeks for 12 weeks, then every 4 weeks | COAST-V/W trials |
| Brodalumab | (IL-17RA) | Used in psoriasis overlap |
Caution with IL-17 inhibitors: avoid in inflammatory bowel disease (case reports of new-onset or flared IBD), candidiasis (mucocutaneous), caution in latent TB (less reactivation than TNFi). JAK inhibitors (tofacitinib, upadacitinib, filgotinib) are approved in some regions for AS — they share the antiviral/herpes zoster cautions of the class. [1]
Switching: if the first biologic fails (at 12 to 16 weeks), switch to another class (TNFi to IL-17i or vice-versa); about 40 to 50 percent respond to the second agent. [1]
Step 5 — Conventional synthetic DMARDs (csDMARDs)
Sulfasalazine and methotrexate are NOT effective for axial disease — they are used only when there is peripheral arthritis that has failed NSAIDs.[6][10]
- Sulfasalazine 2 to 3 g per day orally in divided doses (start 500 mg daily, titrate up). Monitoring: CBC and LFT monthly for the first 3 months then 3-monthly; warn about orange staining of urine and contact lenses, sulpha allergy, haemolysis in G6PD deficiency (screen), male infertility (reversible on discontinuation — counsel men planning a family). Useful in IBD overlap.
- Methotrexate 7.5 to 25 mg once weekly orally or subcutaneously, with folic acid 5 mg weekly (not on the methotrexate day). Monitoring: CBC, LFT, renal monthly for 3 months then 3-monthly; teratogenic — reliable contraception. [1]
Step 6 — Surgery
- Total hip replacement — the single best functional intervention in AS with hip arthritis; dramatically improves mobility, pain and independence.
- Corrective spinal surgery — pedicle-subtraction osteotomy or vertebral-column decancellation for severe kyphotic deformity that prevents forward gaze or severely impairs function; high-risk, specialist spinal centres only. [1]
Adjuncts
- Pain control: paracetamol and short-course weak opioids only; avoid chronic opioids.
- Smoking cessation — reduces progression and improves biologic response.
- Osteoporosis prevention and treatment: calcium and vitamin D; bisphosphonate (e.g. alendronate 70 mg weekly with calcium/vitamin D) for documented osteoporosis.
- Vaccination before biologics: pneumococcal, influenza, hepatitis B, COVID-19; avoid live vaccines (MMR, yellow fever, BCG, oral polio) on biologic. [1]
Specific Subtypes & Scenarios
- Non-radiographic axial SpA (nr-axSpA) — back pain under 45 years with active sacroiliitis on MRI (or HLA-B27 positive with multiple SpA features) but normal plain X-ray. Treat identically to AS. About 10 to 30 percent progress to radiographic AS over 10 years; progression is not inevitable. Predictors of progression: male sex, HLA-B27, elevated CRP, smoking, baseline structural lesions on MRI.
- Juvenile-onset AS / enthesitis-related arthritis (ERA, ILAR) — onset under 16 years; enthesitis and asymmetric lower-limb oligoarthritis dominate; axial involvement appears 5 to 10 years later. Uveitis is usually acute and symptomatic (unlike JIA). Treat NSAIDs, PT, biologics.
- Late-onset AS — over 45 years; rare. May present with advanced silent disease discovered after a fracture; NSAID toxicity and comorbidity dominate management.
- AS with IBD overlap — avoid NSAIDs (can trigger IBD flares); favour a TNF monoclonal (adalimumab, infliximab, golimumab, certolizumab); avoid IL-17 inhibitors (worsen IBD); consider IL-12/23 (ustekinumab) or JAK inhibitors (tofacitinib, upadacitinib) which treat both.
- AS with psoriasis overlap — IL-17 inhibitors are attractive (they treat both psoriasis and AS); TNFi also effective.
- Refractory axial pain despite biologic — reassess disease activity (ASDAS), check adherence, re-image (MRI) for active inflammation; exclude mechanical pain (fracture, instability, stenosis), fibromyalgia overlay, and infection; consider biologic switch or addition of csDMARD for peripheral component. [1]
Complications & Pitfalls
Complications
- Spinal fracture — the rigid, osteoporotic, fused spine fractures easily; even minor trauma can produce an unstable fracture (often cervical, often through a disc or ossified ligament) with high risk of paraplegia and death. Always image after trauma.
- Acute anterior uveitis — recurrent attacks cause posterior synechiae, secondary glaucoma, cataract.
- Aortic regurgitation and AV block — may require valve replacement and pacemaker.
- Apical pulmonary fibrosis — may cavitate and be colonised by Aspergillus or TB.
- Secondary (AA) amyloidosis — proteinuria, nephrotic syndrome, renal failure; biopsy to confirm.
- Cauda equina syndrome — late, from expanded lumbar canal; insidious leg weakness and sphincter dysfunction.
- Atlantoaxial subluxation with cervical cord compression.
- Osteoporosis and vertebral compression fractures.
- Fatigue, depression, work disability. [1]
Common pitfalls
- Missing nr-axSpA because the plain X-ray is normal — MRI is required.
- Over-reliance on HLA-B27 (positive in only 8 percent of the general population; negative does not exclude AS).
- Assuming a normal CRP excludes AS — CRP is normal in 30 to 50 percent.
- Missing a spinal fracture after minor trauma in a fused spine.
- Using csDMARDs (sulfasalazine, methotrexate) for axial disease — ineffective.
- Using etanercept for uveitis or IBD — relatively contraindicated; choose a TNFi monoclonal.
- Not screening for latent TB before a biologic — high reactivation risk.
- Treating only pain, not function — physiotherapy is mandatory.
- Continuing NSAIDs in CKD or late pregnancy. [1]
Prognosis & Disposition
Natural history is highly variable: some patients have mild disease controlled on NSAIDs with exercise; others progress to a severe kyphotic, bamboo-spine deformity with hip ankylosis and systemic complications. Modern biologic therapy has transformed outcomes — earlier functional recovery and employment preservation.[1]
Predictors of severe radiographic and functional progression (high-yield): [1]
- Male sex, young onset, family history, HLA-B27 positive.
- Elevated CRP at baseline, baseline structural damage on imaging (especially early syndesmophytes).
- Smoking (the strongest modifiable risk factor — about doubles progression rate).
- Hip arthritis (the strongest predictor of poor functional outcome).
- Diagnostic delay (longer delay → more damage). [1]
Mortality is modestly increased (standardised mortality ratio about 1.5 to 2) — driven by cardiovascular disease (chronic inflammation), spinal fracture, complications of advanced disease and amyloidosis. Cardiovascular risk assessment and aggressive risk-factor modification (smoking, lipids, blood pressure) are part of routine care. [1]
Functional impact and work: work disability was historically common (up to 30 to 40 percent); modern treat-to-target and biologics reduce this substantially. Workplace modifications, ergonomic seating and avoidance of stooping occupations are important. [1]
Special Populations
Pregnancy and lactation
- NSAIDs are safe in the first and second trimester but should be avoided after 28 to 30 weeks (premature closure of the ductus arteriosus and oligohydramnios); ibuprofen and diclofenac are low-risk in lactation.
- Anti-TNF monoclonal antibodies (adalimumab, infliximab, golimumab) are actively transported across the placenta in the third trimester via FcRn; certolizumab pegol lacks the Fc fragment and is the preferred anti-TNF in pregnancy and lactation (minimal placental transfer).
- Etanercept — avoid (limited data; active in uveitis/IBD context not relevant).
- Sulfasalazine is safe in pregnancy and lactation (continue; supplement folic acid 5 mg daily); note reversible male infertility — counsel men planning conception.
- Methotrexate, leflunomide, mycophenolate — absolutely contraindicated (teratogenic); stop 3 months before conception (methotrexate/leflunomide) and avoid in lactation.
- IL-17 and JAK inhibitors — limited data; avoid unless essential.
- Live vaccines should be avoided in the neonate if the mother was on a biologic in the third trimester (delay rotavirus vaccine by 6 months).
- Delivery: if the sacroiliac joints and lumbar spine are fused, neuraxial (spinal/epidural) anaesthesia may be technically difficult and the airway may be challenging if the cervical spine is fused — early anaesthetic review is essential. [1]
Children (ERA/JAS)
- Enthesitis and asymmetric lower-limb oligoarthritis dominate; axial disease appears later.
- Treat NSAIDs and physiotherapy first; biologics (TNFi, IL-17i) for refractory disease.
- Screen eyes — uveitis in ERA is usually acute and symptomatic (unlike the chronic asymptomatic uveitis of antinuclear-antibody-positive JIA). [1]
Elderly
- Late-onset AS is rare; advanced silent disease discovered after a fracture is the typical scenario.
- NSAID toxicity (renal, GI, cardiovascular) is higher — prefer COX-2 selective agents at the lowest effective dose, or IL-17 inhibitors (less renal/Cardiovascular concern than TNFi).
- Fracture risk and osteoporosis — assess and treat (calcium, vitamin D, bisphosphonates).
- Comorbidity (cardiovascular disease, diabetes) modifies drug choice. [1]
Immunocompromised / on-biologic host
- Vaccinate before starting the biologic (pneumococcal, influenza, hepatitis B, COVID-19).
- Avoid live vaccines while on biologic.
- TB reactivation risk — screen and treat latent TB before TNFi.
- Hepatitis B reactivation — screen HBsAg, anti-HBc; antiviral prophylaxis (entecavir/tenofovir) if positive before biologic.
- Bacterial infection — early treatment; consider holding the biologic during severe infection. [1]
Evidence, Guidelines & Regional Differences
ASAS-EULAR 2022 recommendations (international)[8]
- Treat-to-target (remission or low activity; ASDAS under 1.3).
- NSAIDs at maximum tolerated dose, continuously, first-line for all patients; trial at least two NSAIDs before declaring failure.
- Physiotherapy for all patients.
- Local glucocorticoid injections for focal inflammation; avoid systemic glucocorticoids.
- csDMARDs (sulfasalazine, methotrexate) only for peripheral arthritis.
- Biologic DMARDs (TNFi or IL-17i) for persistent high disease activity; switch class if first biologic fails. JAKi as an option.
- Surgery (hip replacement, spinal osteotomy) for refractory structural disease.
- Treat comorbidity (cardiovascular risk, osteoporosis, IBD, psoriasis, uveitis). [1]
ACR/SAA/SPARTAN 2019 recommendations (USA)[10]
- Strongly recommend NSAIDs (full dose, continuous) and physical therapy.
- Conditionally recommend a TNFi or IL-17i for persistent active disease after NSAID failure.
- Strongly recommend a TNFi monoclonal over etanercept when there is recurrent uveitis or IBD.
- Conditionally recommend against systemic glucocorticoids.
- Conditionally recommend against csDMARDs for axial disease. [1]
NICE NG65 (UK, 2017)[11]
- NSAID at maximum tolerated dose for at least 4 weeks before declaring failure.
- Biologic (TNFi) if ASDAS 2.4 or more (or BASDAI 4 or more, plus objective inflammation on CRP/MRI), twice, 12 weeks apart.
- Switch biologic on inadequate response at 12 weeks; IL-17i if TNFi contraindicated or failed. [1]
Regional note — India
- AS is not uncommon in India; HLA-B27 subtype B*2705 predominates in the North, with prevalence rising north-to-south with B27 carriage.
- Tuberculosis is endemic — mandatory IGRA and chest X-ray before any biologic; treat latent TB.
- Biologic access is limited by cost; NSAID and physiotherapy remain the backbone for most patients.
- Axial MRI is increasingly available in tertiary centres, enabling earlier diagnosis of nr-axSpA. [1]
Controversies and landmark trials
- NSAIDs slow radiographic progression: the Wienands/Wanders analyses of the GESPIC and ALERT cohorts suggested a modest reduction in mSASSS progression with continuous vs on-demand NSAIDs, strongest in patients with elevated CRP. The effect is real but modest and debated.
- IL-23 inhibitors (ustekinumab, risankizumab) failed in axSpA despite a strong IL23R genetic signal and dramatic efficacy in psoriasis and IBD — a landmark paradox that challenges the centrality of the IL-23 axis in established axial disease and focuses attention on the IL-17 arm downstream of IL-23.
- Tumour necrosis factor inhibitors and IL-17 inhibitors are roughly equivalent in efficacy (ASAS 20 response about 60 percent at 12 to 16 weeks); IL-17i may be preferred in patients with IBD-incompatible TNFi or those with psoriasis overlap.
- Secukinumab MEASURE 1 (NEJM 2015): 150 mg SC at weeks 0, 1, 2, 3, 4 then monthly produced ASAS 20 response in about 60 percent of patients at week 16 vs 29 percent placebo — a pivotal registration trial.[9]
Exam Pearls
Ankylosing spondylitis — the numbers that decide an answer
Inflammatory back pain — the Calin 5
CALIN
duration over 3 months
young onset
lumbar and buttock location
gradual onset; improves with exercise, not rest
nocturnal pain and morning stiffness
Extra-articular AS — mnemonic
EYES
acute anterior uveitis — unilateral painful red eye
aortic regurgitation and aortitis; AV block
apical lung fibrosis (and Heberden-style peripheral arthritis)
secondary (AA) amyloidosis, fatigue, IgA nephropathy
- Seronegative = RF negative AND ANA negative. If either is positive, rethink.
- HLA-B27 is associated (90 percent) but NOT diagnostic — only 1 to 5 percent of HLA-B27-positive individuals develop AS.
- Earliest imaging finding is MRI bone-marrow oedema of the SI joint (STIR/T2FS); plain X-ray changes lag by years.
- X-ray progression: blurring, erosion, sclerosis (iliac side first), joint-space change, ankylosis.
- Vertebral findings: Romanus lesion (shiny corner), squared body, syndesmophyte, bamboo spine, dagger sign, trolley-track sign.
- Schober under 5 cm; occiput-to-wall over 5 cm; chest expansion under 2.5 cm.
- Acute anterior uveitis is unilateral and painful — ophthalmology within 24 hours; topical steroid plus cycloplegic; favour a TNFi monoclonal, NOT etanercept.
- Spinal fracture even after minor trauma in a fused spine — image, immobilise.
- csDMARDs (sulfasalazine, methotrexate) do NOT work for axial disease — only for peripheral arthritis.
- Systemic glucocorticoids do NOT work for axial AS — use local injections.
- ERAP1 risk only matters if HLA-B27 positive (epistasis).
- Treat to target: ASDAS under 1.3 (or low activity); biologic if ASDAS 2.1 or more despite NSAIDs. [1]
Exam application bank (NEET-PG / INICET)
One-line answer
Ankylosing spondylitis (AS) is a chronic, progressive inflammatory disease of the axial skeleton and entheses — the prototype of the seronegative spondyloarthropathies. Strongly associated with HLA-B27 (about 90 percent). Presents as inflammatory back pain (insidious onset under 40 years, worse with rest, better with exercise, morning stiffness over 30 minutes, alternating buttock pain) with sacroiliitis (often bilateral and symmetric) and, late, a bamboo spine. Extra-articular: acute anterior uveitis (unilateral painful red eye), aortic regurgitation, apical lung fibrosis, secondary amyloidosis. Diagnosis by the modified New York criteria (1984) for established AS, or the ASAS 2009 criteria for the wider axial spondyloarthritis spectrum (which includes non-radiographic disease detectable on MRI). Management: continuous full-dose NSAIDs plus physiotherapy first-line; TNF inhibitors (adal
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Ankylosing Spondylitis.
References
- [1]Braun J, Sieper J. Ankylosing spondylitis Lancet, 2007.PMID 17448825
- [2]van der Linden S, Valkenburg HA, Cats A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria Arthritis Rheum, 1984.PMID 6231933
- [3]Sieper J, Rudwaleit M, Baraliakos X, et al. The Assessment of SpondyloArthritis international Society (ASAS) handbook: a guide to assess spondyloarthritis Ann Rheum Dis, 2009.PMID 19433414
- [4]Rudwaleit M, Jurik AG, Hermann KG, et al. Defining active sacroiliitis on magnetic resonance imaging (MRI) for classification of axial spondyloarthritis: a consensual approach by the ASAS/OMERACT MRI group Ann Rheum Dis, 2009.PMID 19454404
- [5]Rudwaleit M, van der Heijde D, Landewe R, et al. The Assessment of SpondyloArthritis International Society classification criteria for peripheral spondyloarthritis and for spondyloarthritis in general Ann Rheum Dis, 2011.PMID 21109520
- [6]Braun J, van den Berg R, Baraliakos X, et al. 2010 Update of the international ASAS recommendations for the use of anti-TNF agents in patients with axial spondyloarthritis Ann Rheum Dis, 2011.PMID 21540200
- [7]Ramiro S, Gossec L, van Tubergen A, et al. Efficacy and safety of non-pharmacological and non-biological pharmacological treatment: a systematic literature review informing the 2016 update of the ASAS/EULAR recommendations for the management of axial spondyloarthritis RMD Open, 2017.PMID 28176966
- [8]Ramiro S, Nikiphorou E, Sepriano A, et al. Efficacy and safety of biological DMARDs: a systematic literature review informing the 2022 update of the ASAS-EULAR recommendations for the management of axial spondyloarthritis Ann Rheum Dis, 2023.PMID 36270657
- [9]Baeten D, Sieper J, Braun J, et al. Secukinumab, an Interleukin-17A Inhibitor, in Ankylosing Spondylitis N Engl J Med, 2015.PMID 26699169
- [10]Ward MM, Deodhar AA, Akl EA, et al. 2019 Update of the American College of Rheumatology/Spondylitis Association of America/Spondyloarthritis Research and Treatment Network Recommendations for the Treatment of Ankylosing Spondylitis and Nonradiographic Axial Spondyloarthritis Arthritis Care Res (Hoboken), 2019.PMID 31436026
- [11]Chesterton LS, Rushton A. Appraisal of Clinical Practice Guideline: NICE Guidance on Spondyloarthritis in over 16s: diagnosis and management [NG65] J Physiother, 2019.PMID 31477501