EM · Behavioural and mental health emergencies
Deliberate self-harm and suicide risk assessment
Also known as Deliberate self-harm · Self-harm presentation · Suicide attempt · Suicide risk assessment · Psychosocial assessment after self-harm · SAD PERSONS scale · Safety planning after self-harm
The patient who presents after deliberate self-harm — the sequence of medical clearance before psychosocial assessment, the structured suicide risk assessment (ideation, plan, intent, means, protective factors), the SAD PERSONS and Columbia tools, and the risk-stratified disposition (psychiatric admission for high risk, crisis team for moderate risk, GP follow-up with a safety plan for low risk). Covers the toxicological workup and antidotes (N-acetylcysteine for paracetamol, naloxone for opioid, sodium bicarbonate for tricyclic), the differential of accidental injury and intoxication, and the legal authority to detain. ACEM-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Related topics
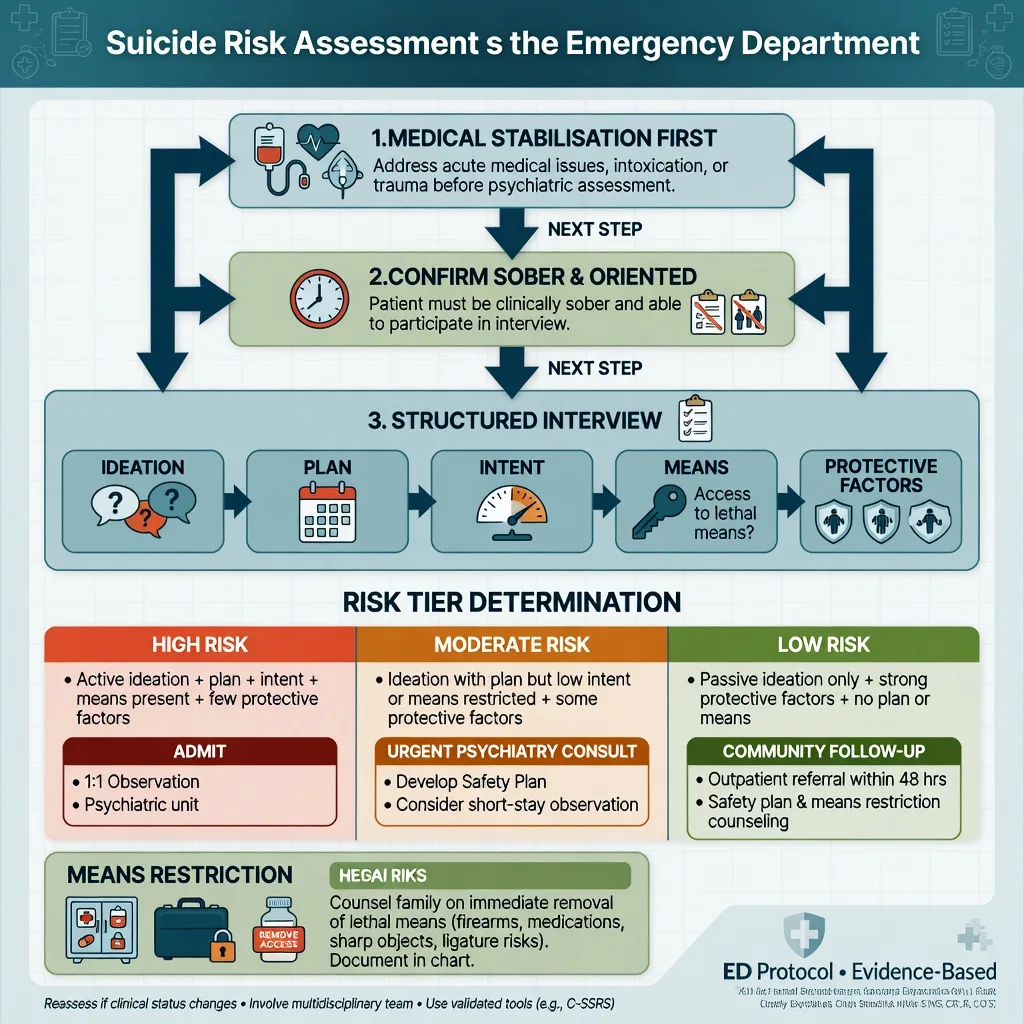
Deliberate self-harm is one of the commonest and the most scrutinised behavioural presentations in the emergency department, and it is examined relentlessly at Fellowship because it sits at the junction of toxicology, psychiatry and the law. The emergency clinician's task is sequential and unambiguous: treat the medical or toxicological emergency first, then conduct the structured psychosocial and suicide-risk assessment, then match the disposition to the risk stratification. The discipline rests on one principle that the Fellowship examiner returns to every year — a patient who dies of an untreated paracetamol hepatotoxicity while awaiting the mental-health team has been failed at the first step, and a patient discharged with active intent and a plan has been failed at the last.[1]
Definition and classification
Self-harm is any intentional act of self-poisoning or self-injury, regardless of the motive or the stated intent to die. The terminology is contested and the candidate must use it precisely. Deliberate self-harm (DSH) is the operational umbrella used in the United Kingdom and Australasian tradition for any intentional self-injury or self-poisoning presenting to health services, and it carries no assumption that the patient wished to die. A suicide attempt is an act of self-harm undertaken with the intent to die; non-suicidal self-injury (NSSI) is the deliberate destruction of body tissue without suicidal intent, used for affect regulation or coping, common in borderline personality disorder and in adolescents. Suicidal ideation ranges from passive (the wish to be dead) to active (the thought of taking one's own life), and it lies on a continuum from ideation through plan and intent to attempt and, in the most severe cases, completed suicide.[15]
The distinctions matter because the management differs. A patient who has taken a near-lethal overdose with the express intent to die is managed as a psychiatric emergency with admission; a patient who has made superficial lacerations to relieve distress without any intent to die may be managed with brief intervention and community follow-up. The same act — an overdose, a laceration — sits in different risk tiers depending on the intent, the lethality, the access to means and the protective factors, and the structured assessment exists to make those distinctions explicit and reproducible.[5]
Epidemiology and the risk of repetition
Self-harm accounts for around 150,000 to 200,000 emergency department attendances each year in England alone, and the rates have risen over the last decade, most steeply in young women. Self-poisoning is the commonest method (around four-fifths of presentations), self-laceration the second commonest, and other methods — hanging, firearm, carbon monoxide, jumping — are rarer in survivors but disproportionately represented among those who die. Women present more often after self-harm, but men die by suicide more often — the so-called gender paradox of suicidal behaviour.[3]
The patient who presents after self-harm is at markedly elevated risk of future suicide. The 12-month repetition rate for self-harm is around 15 to 25 percent, and suicide mortality in this population is elevated 10 to 30 times above the background rate and persists for decades. The systematic review and meta-analysis of suicide-reattempt risk factors identifies a prior suicide attempt as the single strongest predictor of a future attempt, alongside depression and hopelessness, alcohol and substance misuse, sleep disturbance, social isolation, recent loss, and recent discharge from psychiatric care.[3] The repetition risk is greatest in the first three months, and the first four weeks after a psychiatric discharge are the highest-risk window of all — a patient who re-presents in this window is treated as an emergency until a full reassessment proves otherwise.
The principle: medical clearance first, psychosocial assessment second
The single most important rule in the self-harm encounter is the sequence. The overdose, the laceration, the fall or the hanging is a medical emergency first and a psychiatric presentation second, and the medical workup is completed and the toxicity treated before the psychosocial assessment begins. A focused medical screening — the history of the act and the substances taken, the time of ingestion, the observations, a bedside glucose, a focused examination, and the specific toxicological investigations — excludes or treats the medical threat.[1] The paracetamol level is taken at four hours post-ingestion and plotted on the treatment nomogram, the salicylate level is sent, a 12-lead ECG is performed for any tricyclic or QT-prolonging agent, a venous gas is checked for acidosis, and the specific antidote is started where indicated. The medical screening of the psychiatric patient confirms that indiscriminate routine investigation is low-yield in the well patient, but that a focused, history-guided assessment identifies the organic and toxicological threats that matter.[1]
A specific and high-yield rule follows from this: never perform the psychosocial assessment on the intoxicated patient. The history, the stated intent, the capacity assessment and the risk stratification are all unreliable while the patient is intoxicated, and an underestimate made through alcohol is a recurring cause of death. The intoxicated patient is observed under the doctrine of necessity (or the relevant mental-health legislation) until sober, the means of further harm are removed, and the structured assessment is undertaken only when the patient can give a reliable account.[1]
Pathophysiology and the pathway to an attempt
The stress-diathesis model frames self-harm and suicide as the product of an underlying vulnerability — genetic loading, serotonergic dysfunction, traits of impulsivity and hopelessness — activated by an acute stressor. The pathway to an attempt proceeds through escalating stages: a precipitating crisis (loss, conflict, legal or financial trouble, relapse of mental illness) generates suicidal ideation, which consolidates into a plan, which acquires intent, which is enacted when disinhibition — by intoxication, by access to means, by acute distress — overcomes the protective factors.[15]
Two clinical points follow. Hopelessness — the conviction that the future holds nothing — predicts suicide more strongly than the severity of the depression itself, and it is assessed explicitly. Intoxication is an acute disinhibitor and is present in around two-fifths of self-harm acts; it both enables the act in the moment and renders the after-event assessment unreliable, which is the basis for the sober-before-assessment rule. Alcohol and substance misuse are among the most consistent risk factors for both attempt and completed suicide.[3]
Clinical presentation and the atypical
The typical presentation is straightforward: a patient, a history of self-poisoning or self-laceration, an account of the events leading to the act, and a variable degree of current distress or regret. The emergency clinician documents the agent, the dose, the time, the route, the intent at the time of the act (distinguished from the intent now), the precautions against discovery, any last-minute rescue attempt, and any substance coingested.[12]
The atypical presentations are the ones that catch the unwary. The masked self-harm presentation — the vague history of "I took some pills", the single tablet that is denied as significant, the "accidental" overdose in a patient with a stockpile — conceals a genuine attempt beneath minimisation. The chronic repeater numbs the clinician into therapeutic nihilism, yet each episode is treated on its merits because repetition is itself the strongest predictor. The elderly single-act attempter uses a high-lethality method on a first presentation and carries the highest completed-suicide rate of any group. The intoxicated patient gives an unreliable history until sober. And the patient who presents with an "accident" — the fall, the single-car collision, the accidental overdose — may in fact have self-harmed, and a low threshold for a direct, non-judgemental enquiry about suicidal intent uncovers a substantial minority.[15]
Methods of self-harm — the five clinical scenarios
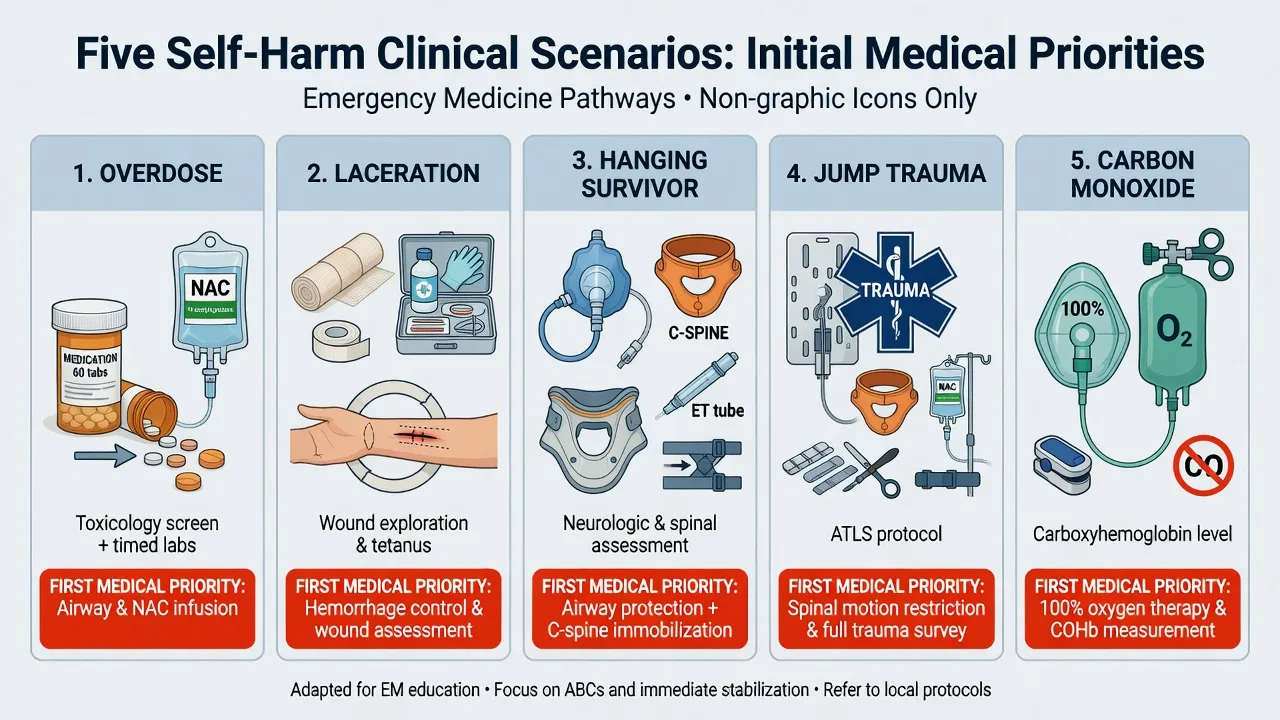
The method of self-harm determines the medical workup, the toxicological treatment, and — through its lethality — part of the risk stratification. Self-poisoning is the commonest method seen alive in the emergency department (around four-fifths of presentations), self-laceration the second commonest, and the violent methods — hanging, jumping, carbon monoxide, firearm — are rarer in survivors but disproportionately represented among those who die. The candidate must be able to run through each scenario: the immediate threats, the specific investigations, the antidote or the intervention, and the disposition logic. The UK national data on suicide methods among mental-health patients between 2000 and 2022 confirm the shifting landscape — hanging has overtaken self-poisoning as the commonest method of completed suicide, while opiate and antidepressant overdose dominate among survivors presenting to health services.[14]
Self-poisoning — overdose
Overdose is the commonest method of self-harm seen alive, and paracetamol is the single commonest agent in the United Kingdom and Australasia, followed by antidepressants (tricyclics, SSRIs, mirtazapine), benzodiazepines, opioids, and non-steroidal anti-inflammatory drugs. The emergency workup is agent-specific: the time of ingestion, the dose, the coingestants, and the specific antidote. Paracetamol dominates the Fellowship examination because it is common, the toxicity is delayed and treatable, and the nomogram is a testable algorithm. The four-hour level is plotted on the Rumack-Matthew treatment nomogram; N-acetylcysteine is started if the level is above the line or if the ingestion is staggered or the time is unknown. The NACSTOP 2 non-inferiority trial has informed current practice on the duration of the NAC regimen, confirming that shorter validated regimens are non-inferior in selected low-risk patients but that the standard regimen remains the default in the uncertain or the high-risk case.[11]
Tricyclic antidepressant overdose is the classic cardiotoxic presentation: a widened QRS beyond 100 ms, a prominent R wave in aVR, a right-axis deviation, hypotension, and the risk of ventricular tachycardia and asystole. Sodium bicarbonate 1 to 2 mmol/kg IV bolus is given for QRS widening, ventricular arrhythmia or hypotension, the target serum pH is 7.45 to 7.55, and class Ia and Ic antiarrhythmics are avoided because they prolong the sodium-channel blockade. Benzodiazepine overdose produces sedation, ataxia and slurred speech but is rarely fatal in isolation — flumazenil is avoided in the mixed or tricyclic overdose because it precipitates seizures and ventricular arrhythmia, and is reserved for the isolated iatrogenic over-sedation. SSRI overdose causes the serotonin syndrome in the severe case — clonus, hyperreflexia, rigidity, autonomic instability and hyperthermia — managed with cooling, benzodiazepines and cyproheptadine. Opioid overdose produces the classic triad of coma, pin-point pupils and respiratory depression, reversed with naloxone 0.4 to 0.8 mg IV titrated to a total of 10 mg. Salicylate overdose produces tinnitus, hyperventilation and a mixed respiratory alkalosis with metabolic acidosis; the level guides alkaline diuresis and haemodialysis. The safety profile of N-acetylcysteine itself has been scrutinised — the scoping review of iatrogenic acetylcysteine overdose confirms that the adverse reactions (nausea, flushing, bronchospasm, anaphylactoid reaction) are dose-related and usually self-limiting, and they do not outweigh the benefit in the patient at risk of hepatotoxicity.[16]
Self-cutting — laceration
Self-laceration is the second commonest method of self-harm seen alive. The clinical task is to distinguish the superficial repetitive non-suicidal self-injury — typically on the forearms or thighs, multiple scars of varying age, low lethality, used for affect regulation in borderline personality disorder or adolescence — from the deep suicidal laceration — a single, deeper wound that may involve tendons, nerves or vessels. The retrospective analysis of 41 wrist-cutting suicide attempts confirms the surgical importance: a substantial proportion involve deep structure injury requiring hand-surgical or plastic-surgical repair, and the emergency clinician examines for tendon, nerve and vessel injury, controls the bleeding with direct pressure, and refers for definitive repair.[12] The psychosocial assessment distinguishes the NSSI pattern (no intent to die, repetitive, affect regulation) from the suicidal laceration (intent to die, high lethality), because the risk tier and the disposition differ.
Hanging and strangulation
Hanging is the commonest method of completed suicide in many high-income countries and a presentation with devastating physiological consequences in the survivor. The mechanism combines vascular occlusion (jugular venous compression producing cerebral congestion and hypoxia) with airway obstruction and, in the suspended hanging, a cervical spine injury from the fall. The survivor presents with cerebral hypoxic injury, pulmonary oedema, aspiration pneumonitis, and the possibility of a cervical spine fracture. The UK intensive-care case series of hanging and asphyxia survivors documents the high mortality and the prolonged intensive-care stay, and it supports the current approach: a trauma call with cervical spine immobilisation in the suspended hanging, early intubation for the comatose patient, targeted temperature management at 36 degrees for the comatose post-cardiac-arrest patient, and a neuro-prognostication strategy that defers definitive prognostication for at least 72 hours of observation and investigation.[10] The psychosocial assessment is deferred until the neurological recovery permits a reliable assessment.
Jumping — falls from height
Jumping from a height produces the pattern of blunt polytrauma: calcaneal and spinal compression fractures, pelvic and long-bone fractures, intra-abdominal and intrathoracic injury, and traumatic brain injury. The patient who survives a jump is managed as a major trauma patient with a full primary and secondary survey, the trauma team activation, and the standard imaging — and the self-harm assessment is undertaken once the medical and surgical stabilisation is complete. The distinction between a suicidal jump and an accidental fall is made from the history, the scene, the collateral and the mental state, and a low threshold for a direct enquiry about intent is maintained.[15]
Carbon monoxide poisoning
Carbon monoxide poisoning — the deliberate inhalation of motor-vehicle exhaust, charcoal combustion or a faulty heater — produces the insidious presentation of headache, nausea, dizziness, confusion and progressive loss of consciousness. The carboxyhaemoglobin level confirms the diagnosis, the ECG screens for the myocardial injury, and the neuropsychological testing at follow-up screens for the delayed encephalopathy. The severe case — syncope, seizure, coma, cardiac ischaemia, pregnancy, or a high carboxyhaemoglobin level — is referred for hyperbaric oxygen therapy. The recent case series on the cardiac and thrombotic effects of severe carbon monoxide poisoning documents the frequency of myocardial injury, arrhythmia and thrombosis, reinforcing that the cardiac assessment is a core part of the workup alongside the neurological assessment.[19]
Overdose (self-poisoning)
- Commonest method seen alive — paracetamol #1, then antidepressants, benzodiazepines, opioids, salicylates, NSAIDs
- Workup: agent, dose, time, route, coingestants; paracetamol level at 4 hours, salicylate level, ECG for TCA, venous gas, glucose
- Antidotes: NAC for paracetamol, naloxone for opioid, sodium bicarbonate for TCA, charcoal within 1 hour; flumazenil avoided in mixed overdose
- Disposition: admit for medical treatment if toxic; psychiatric assessment once stable and sober
Self-cutting (laceration)
- Second commonest method — forearms and thighs; distinguish NSSI (superficial, repetitive, affect regulation) from suicidal laceration (deep, single, high lethality)
- Workup: examine for tendon, nerve, vessel injury; control bleeding with direct pressure; photograph and measure depth
- Intervention: wound repair, suturing or surgical referral for deep-structure injury; tetanus prophylaxis
- Disposition: brief intervention for NSSI; full psychosocial assessment and risk stratification for any suicidal laceration
Hanging and strangulation
- Commonest method of completed suicide; survivors have cerebral hypoxic injury, pulmonary oedema, aspiration, possible cervical spine fracture
- Workup: trauma call with C-spine immobilisation in suspended hanging; early intubation if comatose; CT brain and C-spine
- Management: targeted temperature management at 36 degrees for the comatose post-arrest patient; treat aspiration pneumonitis
- Disposition: ICU admission; defer psychosocial assessment until neurological recovery permits reliable assessment
Jumping (falls from height)
- Blunt polytrauma — calcaneal and spinal fractures, pelvic and long-bone fractures, intra-abdominal and intrathoracic injury, TBI
- Workup: full trauma primary and secondary survey; trauma team activation; CT trauma series
- Management: standard trauma resuscitation and surgical intervention as indicated; treat the injuries first
- Disposition: admit for trauma care; psychosocial assessment once surgically stable; the scene and the mental state distinguish a jump from an accidental fall
Carbon monoxide poisoning
- Insidious onset — headache, nausea, dizziness, confusion, progressive loss of consciousness; deliberate exhaust or charcoal inhalation
- Workup: carboxyhaemoglobin level; ECG for myocardial injury; arterial blood gas for acidosis; pregnancy test
- Management: 100 percent oxygen via non-rebreather; hyperbaric oxygen for syncope, seizure, coma, cardiac ischaemia, pregnancy or high COHb
- Disposition: admit for cardiac and neurological monitoring; psychosocial assessment once recovered; screen for delayed encephalopathy at follow-up
Differential diagnosis — the four corners
The differential of the self-harm presentation divides into four corners, distinguished by the intent, the lethality and the mental state. The emergency clinician assigns the presentation to one corner because the management differs, and the assignment is made from the history, the collateral and the mental state examination — never from the act alone. Accidental injury and intoxication must be distinguished from intentional self-harm, and self-harm with intent to die must be distinguished from non-suicidal self-injury, because the risk tier and the disposition follow the intent rather than the behaviour.[15]
Suicide attempt (self-harm with intent to die)
- An act undertaken with the explicit intention of ending life — overdose, hanging, firearm, jumping, carbon monoxide, wrist or neck laceration
- Planned, rehearsed, precautions against discovery, a note, final arrangements made; high lethality and low rescue potential
- Active suicidal ideation persists at assessment; the intent is to die, distinguished from a cry for help or ambivalence
- High-risk tier: psychiatric admission, voluntary or involuntary; remove means and observe one-to-one
Non-suicidal self-injury (NSSI)
- Deliberate destruction of body tissue without intent to die — superficial laceration, burning, scratching; used for affect regulation
- Repetitive, low lethality, often in borderline personality disorder or adolescence; the act relieves distress rather than aiming at death
- No active suicidal intent at assessment; ideation, if present, is passive; protective engagement with services often established
- Manage the injury, brief intervention, community follow-up; a safety plan and means restriction still apply, and any escalation of intent moves the patient up the risk ladder
Accidental injury or intoxication
- No intent to self-harm — the fall, the accidental overdose, the single-vehicle collision, the recreational overdose
- Distinguished by the history, the collateral, the scene and the mental state; a low threshold for direct enquiry about intent is mandatory
- Screen for alcohol, drugs and a contributory medical cause; the "accident" that is in fact self-harm is a recurring missed diagnosis
- Treat the injury or toxicity, address any contributory substance use, and arrange follow-up appropriate to the underlying cause
Self-harm in an altered mental state
- The act occurs during delirium, intoxication, acute psychosis or profound cognitive impairment — intent is clouded or absent
- Command hallucinations or persecutory delusions drive the act in psychosis; delirium or intoxication may erase any memory of intent
- Treat the underlying organic or psychotic cause first; the capacity assessment is deferred until the mental state clears
- Admit for the medical or psychiatric illness; the risk assessment is repeated as the mental state resolves, and the patient is not discharged from an unresolved delirium
Immediate management — medical stabilisation and the toxicological workup
The immediate management begins with the airway, breathing and circulation, and proceeds to the specific toxicological treatment. The agent, the dose, the time and the route are established from the patient, the family, the ambulance crew and the medication containers brought in. A bedside glucose is checked in every patient. The specific antidote is started where the agent and the dose warrant it, and the treatment is not delayed for a confirmatory level when the clinical picture is severe.[1]
The patient who has taken a paracetamol overdose above the treatment line is admitted for the full N-acetylcysteine regimen; the psychiatric assessment is deferred until the medical treatment is underway and the patient is stable. The ECG is reviewed for the tricyclic pattern — a wide QRS, a prominent R wave in aVR, and right-axis deviation — and sodium bicarbonate is given for any QRS beyond 100 ms. Glucose is rechecked, the salicylate level is sent for the tinnitus and hyperventilation of salicylate toxicity, and a venous gas screens for the acidosis of toxic alcohol, metformin or iron overdose. The medical management is documented and the patient is reassessed before the psychosocial assessment begins.[1]
[16] [1]The psychosocial assessment
Once the patient is medically stable and sober, the psychosocial assessment is undertaken by a trained clinician — the emergency clinician in the smaller centre, the mental-health liaison team in the larger one. The assessment has three components: a full history of the act and its context, a mental state examination, and a structured suicide-risk assessment, supported by collateral from the family, the general practitioner, the police and the prior record. The aim is to understand the act, to assess the current risk, to identify the treatable contributors, and to plan the aftercare. National guidance recommends a compassionate psychosocial assessment for every self-harm presentation, the involvement of the family or carer wherever possible, and a written safety plan before discharge.[5]
The history of the act elicits, in order: the events leading up to it (the trigger — loss, conflict, relapse, legal or financial crisis); the intent at the time (did the patient intend to die, and do they now?); the planning (was it considered in advance, rehearsed, prepared?); the precautions against discovery (was it timed to be found, or not?); the lethality of the method; the role of alcohol or drugs; and any last-minute rescue attempt. The mental state examination looks for the treatable illnesses — depression, bipolar disorder, psychosis, alcohol and substance misuse, and the personality disorders — and for hopelessness, the conviction that the future holds nothing, which predicts suicide more strongly than the depression itself. The structured suicide-risk assessment then evaluates the ideation, the plan, the intent, the access to means, and the protective factors, and it is the basis on which the risk tier and the disposition are assigned.[5]
The structured suicide-risk assessment — the domains
SUICIDE
Presence, frequency, intensity, duration — passive (the wish to be dead) distinguished from active (the thought of acting)
Alcohol and substance use — present at the act, ongoing; an acute and a chronic risk amplifier
The stated determination to die, distinguished from ambivalence or a cry for help; the intent at the time of the act and the intent now
Depression, hopelessness, psychosis with command hallucinations, delirium; capacity to consent to or refuse admission and treatment
Specificity, lethality, preparation, rehearsal; a note, final arrangements, stockpiled medication, a chosen method
Family, children, faith, future orientation, engagement with services; reasons for living buffer the risk
Prior attempts — the single strongest predictor — recent psychiatric discharge, recent loss, known mental illness, current treatment
The psychosocial assessment — the full structure
The psychosocial assessment is more than the structured suicide-risk score. It is a comprehensive biopsychosocial evaluation that takes 45 to 60 minutes, undertaken by a trained clinician (the mental-health liaison nurse or the emergency clinician in the smaller centre), and it covers six domains that together build the picture of the precipitant, the vulnerability, the current risk, and the protective factors. The national guidance — NICE NG225 in the UK — requires a compassionate psychosocial assessment for every self-harm presentation, not only for those who screen positive on a risk scale.[5]
The precipitant is the immediate trigger — a relationship breakdown, a financial crisis, a legal problem, a bereavement, a job loss, a relapse of mental illness, or an anniversary of a loss. The precipitant is not the cause of the suicide, but it is the match that lights the tinder, and understanding it directs the aftercare (relationship counselling, debt advice, legal support, bereavement services). The psychiatric history elicits any current or past mental illness — depression (the commonest, present in up to 90 percent of those who die by suicide), bipolar disorder, schizophrenia, anxiety disorders, eating disorders, alcohol and substance use disorders, and the personality disorders, particularly borderline personality disorder. The treatment history — current medications, adherence, recent changes, the last psychiatric review, recent discharge — is documented. The substance use history quantifies the alcohol intake, the drug use, the pattern and the dependence, because alcohol is present in around two-fifths of self-harm acts and is among the most consistent risk factors for both attempt and completed suicide.[3]
The family history elicits suicide, mental illness and substance use in the family — the genetic and the environmental loading that contributes to the vulnerability. The access to means is asked directly: firearms, a medication stockpile, a chosen location, access to a vehicle for carbon monoxide. The answer drives the means-restriction conversation. The protective factors — family, children, faith, future orientation, engagement with services, reasons for living — buffer the risk and are the foundation on which the safety plan is built. The assessment is supported by collateral from the family, the GP, the police and the prior record, because the patient who minimises is a recurring presentation.[5]
The psychosocial assessment — the six-domain sequence
Establish rapport and set the frame
A private space, enough time (45–60 minutes), a non-judgemental stance, and an explicit statement of the purpose: "I need to understand what happened, what led to it, and how we can help." The patient who feels judged or rushed gives a falsely low account.
History of the act
The events, the precipitant, the intent at the time (distinguished from the intent now), the planning, the precautions against discovery, the lethality, the role of alcohol or drugs, and any last-minute rescue attempt. The history is taken from the patient, the family, the ambulance crew and the medication containers.
Psychiatric history and substance use
Current and past mental illness, current treatment and medications, adherence, recent discharge, alcohol and drug use, dependence. The psychiatric history identifies the treatable contributors and the prior-treatment context.
Family history and access to means
Suicide and mental illness in the family (the loading); direct enquiry about access to firearms, a medication stockpile, a chosen location, a vehicle. The answer drives the means-restriction conversation.
Mental state examination and structured risk assessment
The MSE screens for depression, bipolar disorder, psychosis, cognitive impairment, and hopelessness. The structured suicide-risk assessment (ideation, plan, intent, means, protective factors) assigns the risk tier.
Formulation, safety plan and disposition
Integrate the findings into a formulation: the precipitant, the vulnerability, the current risk, the protective factors. Agree a written safety plan, restrict the means, and match the disposition to the risk tier. Document the reasoning and the follow-up.
Precipitant (the trigger)
- The immediate event — relationship breakdown, financial crisis, legal problem, bereavement, job loss, relapse, anniversary
- Not the cause of the suicide, but the match that lights the tinder; understanding it directs the aftercare
- Elicited through a direct, non-judgemental enquiry: "What was happening in your life in the days and weeks before this?"
- Addressed in the safety plan and the follow-up — relationship counselling, debt advice, legal support, bereavement services
Psychiatric history (the vulnerability)
- Current and past mental illness — depression (up to 90% of completed suicides), bipolar, schizophrenia, anxiety, eating disorders
- Alcohol and substance use disorders; personality disorders, particularly borderline personality disorder
- Current treatment, adherence, recent medication changes, recent psychiatric discharge — the highest-risk window
- The treatment history identifies the treatable contributors and the prior-engagement context for the follow-up plan
Family history (the loading)
- Suicide in the family — the strongest single familial risk factor; a family history of mental illness and substance use
- Identifies the genetic and the environmental vulnerability; a family suicide history raises the baseline risk
- Asked sensitively: "Has anyone in your family ever attempted or died by suicide, or had a mental illness?"
- A positive family history does not determine the tier, but it is a weight in the integrated risk formulation
Access to means (the lethality amplifier)
- Asked directly: firearms, a medication stockpile, a chosen location, a vehicle for carbon monoxide, access to heights
- The availability of a lethal method drives completed suicide more than the strength of the intent
- The answer drives the means-restriction conversation — securing firearms, limiting the dispensed quantity, a trusted holder
- Documented and revisited at every contact; the single most effective ED suicide-prevention intervention
Protective factors (the buffer)
- Family, children, faith, future orientation, engagement with services, reasons for living — the factors that buffer the risk
- The foundation on which the safety plan is built; strong protective factors support a lower-tier disposition
- Asked directly: "What has kept you going? Who or what in your life is most important to you?"
- Reinforced in the safety plan — the social contacts, the reasons for living, the engagement with services
Suicide risk stratification — SAD PERSONS and the clinical judgement
The suicide-risk assessment stratifies the patient into low, moderate or high risk, and the tier drives the disposition. No single score determines the tier; the structured clinical assessment integrates the score, the history, the mental state, the intent, the means and the protective factors. The candidate must be able to name the established risk factors, to reproduce the SAD PERSONS scale, and to apply the tier definitions precisely.[2]
The SAD PERSONS scale is a widely taught mnemonic that estimates the short-term suicide risk from demographic and clinical factors. It was designed as a teaching and screening aid, not as a sole determinant of disposition, and its predictive value is modest. The recent validation of SAD PERSONS alongside the NO HOPE scale confirms that the scale stratifies usefully (a score of five or more denotes high risk) but must never replace the structured clinical assessment of intent, plan, means and protective factors.[2]
The SAD PERSONS suicide-risk score
SAD PERSONS
Male sex — men complete suicide more often, women attempt more often
Age under 19 or over 45 years — the young and the elderly are at elevated risk
A current depressive illness or hopelessness — among the strongest predictors
A prior suicide attempt — the single strongest historical risk factor
Alcohol misuse or current intoxication — disinhibits and impairs judgement
Active psychosis, delusions, command hallucinations, or cognitive impairment
A specific, organised plan and preparation — intent made operational
Social isolation, separation, unemployment, recent loss
Chronic medical illness, terminal illness, or chronic pain
The tier definitions, applied at the bedside, are the load-bearing part of the assessment. High risk is a patient with a plan, access to means and active intent — or a patient who has made a near-lethal attempt, or who has active intent on reassessment. Moderate risk is active ideation with a plan but ambivalent or absent intent, or a recent attempt without current intent, in a patient who can engage with follow-up. Low risk is passive ideation, no plan, no intent, strong protective factors and a willingness to engage with a safety plan and follow-up. The Columbia Suicide Severity Rating Scale offers an alternative, validated structure that grades the ideation and the behaviour separately, and the Manchester Self-Harm rule predicts repetition from a smaller set of factors; both are used in services alongside the clinical assessment. A score never overrides the clinical judgement, and the risk is reassessed whenever the situation changes.[2]
Risk assessment tools — the validated instruments
No single score determines the risk tier, but the candidate must know the instruments that inform the structured assessment: their structure, their evidence base, and their limitations. The Fellowship examiner asks the candidate to name two or three tools, to describe what they measure, and to explain why none replaces the clinical judgement. The multicentre, population-level studies of risk-scale accuracy after self-harm confirm the central finding: the scales have only modest predictive value for repeat self-harm and suicide, their sensitivity is too low to use as a sole discharge screen, and they are clinical aids to be integrated with the full structured assessment, not replacements for it.[8][9]
Columbia Suicide Severity Rating Scale (C-SSRS)
The C-SSRS, developed by Posner and colleagues at Columbia University, is the dominant structured tool in US practice and the prototype of the severity-grading approach. It separates the ideation (rated from 1 — passive wish to be dead — through 5 — intent with a plan) from the behaviour (the actual and interrupted attempts, the aborted attempts, the preparatory acts, and the non-suicidal self-injury), and it grades the intensity and the lethality of each. The C-SSRS is embedded in the screening across the Veterans Health Administration and the Zero Suicide framework, and the Joint Commission Sentinel Event Alert requires a validated screening followed by a structured assessment. The validation study confirms that the lifetime ascertainment of suicidal ideation and behaviour by the C-SSRS predicts future suicidal behaviour in clinical research, supporting its use as both a screening and a research instrument.[7] The key advantage of the C-SSRS over the older scales is that it captures the full continuum — from passive ideation through aborted and interrupted attempts to completed behaviour — rather than collapsing it into a single number.
Beck Scale for Suicide Ideation (BSSI)
The Beck Scale for Suicide Ideation, developed by Aaron Beck from the Suicidal Ideation Questionnaire, is a 19-item self-report scale (with a 21-item clinician-administered variant, the SAD PERSONS-adjacent Scale for Suicide Ideation) that quantifies the intensity of suicidal ideation across three domains: the active and passive suicidal desire, the suicidal plans and preparation, and the suicidal intent. The first five items screen for the presence of any ideation; if none, the scale stops. The psychometric validation of the BSSI confirms its reliability and its convergent validity with the clinician-administered measures of depression and hopelessness, supporting its use in the structured assessment and in the research context.[6] Beck's contribution is the operationalisation of the hopelessness construct and the demonstration that hopelessness — the conviction that the future holds nothing — predicts completed suicide more strongly than the severity of the depression itself.
Manchester Self-Harm rule and the ReACT Self-Harm rule
The Manchester Self-Harm (MASH) rule and the ReACT rule are brief, four-item tools designed to predict repeat self-harm from the history alone, without a clinician judgement. The MASH rule flags four factors — a history of self-harm, a history of psychiatric treatment, benzodiazepine use in the current attempt, and a current psychiatric treatment — and a positive result (any one factor) predicts repeat self-harm with a high sensitivity but a low specificity, confirming its use as a screen rather than a determinant. The multicentre validation of these rules in the UK population-level cohort confirms the trade-off: the sensitivity is high enough to use as a screen to identify who warrants a full psychosocial assessment, but the specificity is too low to use as a sole discharge screen.[9]
SAD PERSONS scale
- 9-item mnemonic score (Sex, Age, Depression, Previous attempt, Ethanol, Rational thinking loss, Organised plan, No social support, Sickness); 1 point each, max 9
- Designed as a teaching and screening aid; modest predictive value; a score of 5 or more denotes high risk
- Quick, memorable, useful for teaching the risk factors; widely used in North American emergency departments
- Limitation: low sensitivity and specificity; the UK multicentre validation confirms it should never replace the structured clinical assessment
Columbia Suicide Severity Rating Scale (C-SSRS)
- Severity-graded tool separating ideation (rated 1–5 from passive wish to intent with plan) from behaviour (actual, interrupted, aborted attempts and preparatory acts)
- Captures the full continuum of suicidal ideation and behaviour; the lifetime version predicts future suicidal behaviour
- The dominant US tool, embedded in the Veterans Health Administration, the Zero Suicide framework, and the Joint Commission Sentinel Event Alert requirements
- Validated in clinical research; available in screener, brief, and full versions; the gold standard for structured severity rating
Beck Scale for Suicide Ideation (BSSI)
- 19-item self-report scale quantifying ideation intensity across desire, plans and intent; first 5 items are a screen
- Psychometrically validated; convergent validity with measures of depression and hopelessness; operationalises Beck hopelessness
- Strong research and clinical tool; the hopelessness construct predicts completed suicide more strongly than depression severity
- Self-report format may underestimate in the patient who minimises; paired with the clinician-administered assessment
Manchester Self-Harm (MASH) rule
- 4-item history-only screen — history of self-harm, psychiatric treatment history, benzodiazepine in current attempt, current psychiatric treatment
- Any one positive flags the patient for a full psychosocial assessment; high sensitivity for repeat self-harm
- Brief, no clinical judgement required, useful as an initial triage screen in the busy emergency department
- Low specificity — flags the majority as positive; a screen, not a determinant of disposition; paired with the full assessment
Quinlivan et al. — predictive accuracy of risk scales following self-harm (multicentre, prospective cohort)
Carter et al. — accuracy of risk scales for predicting repeat self-harm and suicide (multicentre, population-level)
Definitive management — risk-stratified disposition
The disposition follows the risk tier, and it takes one of three paths. The decision is documented with the findings on ideation, plan, intent, means and protective factors, and with the specific tier and the reasoning.[15]
The high-risk patient is admitted to a psychiatric unit — voluntarily if they will accept it, and involuntarily under the Mental Health Act if they refuse and meet the criteria of a mental illness of a nature or degree that warrants hospital treatment, with a risk to their health or safety. The patient is observed one-to-one, the access to means is removed, and the psychiatric team assumes care once the medical treatment is complete. The emergency clinician completes the medical screening, treats the toxicity, arranges the statutory documentation where involuntary detention is required, and hands over with a structured referral.[1]
The moderate-risk patient is managed with the crisis-resolution and home-treatment team, who review within 24 hours and provide intensive community support. A written safety plan is agreed, the means of further harm are removed or secured, the family or carer is involved with consent, and a follow-up appointment is booked before discharge. A brief voluntary admission is considered where the ambivalence, the isolation or the access to means cannot be managed safely at home. The emergency clinician does not discharge a moderate-risk patient without the crisis-team review and the safety plan in place.[15]
The low-risk patient is discharged with a written safety plan, the general-practitioner follow-up arranged within seven days, the crisis-line numbers provided, the means of further harm secured, and the family or carer informed and involved. The discharge is documented, the safety plan is rehearsed with the patient, and the red flags that should prompt a return are explained.[8]
The DSH encounter — the sequential management pathway
Medical stabilisation and toxicological workup
ABC, bedside glucose, focused examination; agent, dose, time, route, coingestants. Paracetamol level at 4 hours, salicylate level, ECG for tricyclic widening, venous gas. Start the specific antidote (NAC, naloxone, sodium bicarbonate, charcoal) without delay where indicated.
Observe the intoxicated patient until sober
Do not assess risk while intoxicated — the history, the intent and the capacity are unreliable. Observe under the doctrine of necessity or the Mental Health Act, remove means, reassess when the patient is sober.
Psychosocial assessment by a trained clinician
The six-domain assessment: history of the act, precipitant, psychiatric history, substance use, family history, access to means and protective factors. Mental state examination. Collateral from family, GP, police and prior record.
Structured suicide-risk assessment and stratification
Ideation, plan, intent, means, protective factors. Apply the risk tools (SAD PERSONS, C-SSRS, Beck) as clinical aids. Assign the risk tier — high, moderate, or low — from the integrated clinical assessment, not from the score alone.
Risk-stratified disposition
High risk: psychiatric admission, one-to-one observation, remove means, involuntarily under the Mental Health Act if the criteria are met. Moderate risk: crisis-team review within 24 hours, safety plan, means restriction. Low risk: GP follow-up within 7 days, safety plan, means restriction.
Safety plan, means restriction and follow-up before discharge
Written Stanley-Brown safety plan rehearsed with the patient. Means-restriction counselling (firearms, medication stockpile, trusted holder). Follow-up contact within 48 hours. Family or carer involved with consent. Document the reasoning and the red flags for return.
High risk — psychiatric admission
- Active intent, a specific plan and access to means; or a near-lethal attempt; or active intent on reassessment
- Admit to a psychiatric unit — voluntarily if accepted, involuntarily under the Mental Health Act if refused and the criteria are met
- One-to-one observation, remove means, psychiatric team assumes care once the medical treatment is complete
- The statutory documentation (Section 2 UK, the statutory hold ANZ, 5150 US) is completed; the structured referral is documented
Moderate risk — crisis team
- Active ideation with a plan but ambivalent or absent intent; or a recent attempt without current intent
- Crisis-resolution and home-treatment team review within 24 hours; intensive community support
- Written safety plan agreed, means restriction, family or carer involved with consent, follow-up appointment booked before discharge
- A brief voluntary admission is considered where the ambivalence, the isolation or the access to means cannot be managed safely at home
Low risk — community follow-up
- Passive ideation, no plan, no intent, strong protective factors, willingness to engage with a safety plan and follow-up
- Discharged with a written safety plan, GP follow-up within 7 days, crisis-line numbers provided
- Means of further harm secured, family or carer informed and involved, the safety plan rehearsed with the patient
- Red flags for return explained; the follow-up contact within 48 hours is arranged; the discharge is documented
Model answer — the disposition after a paracetamol overdose
Safety planning and means restriction
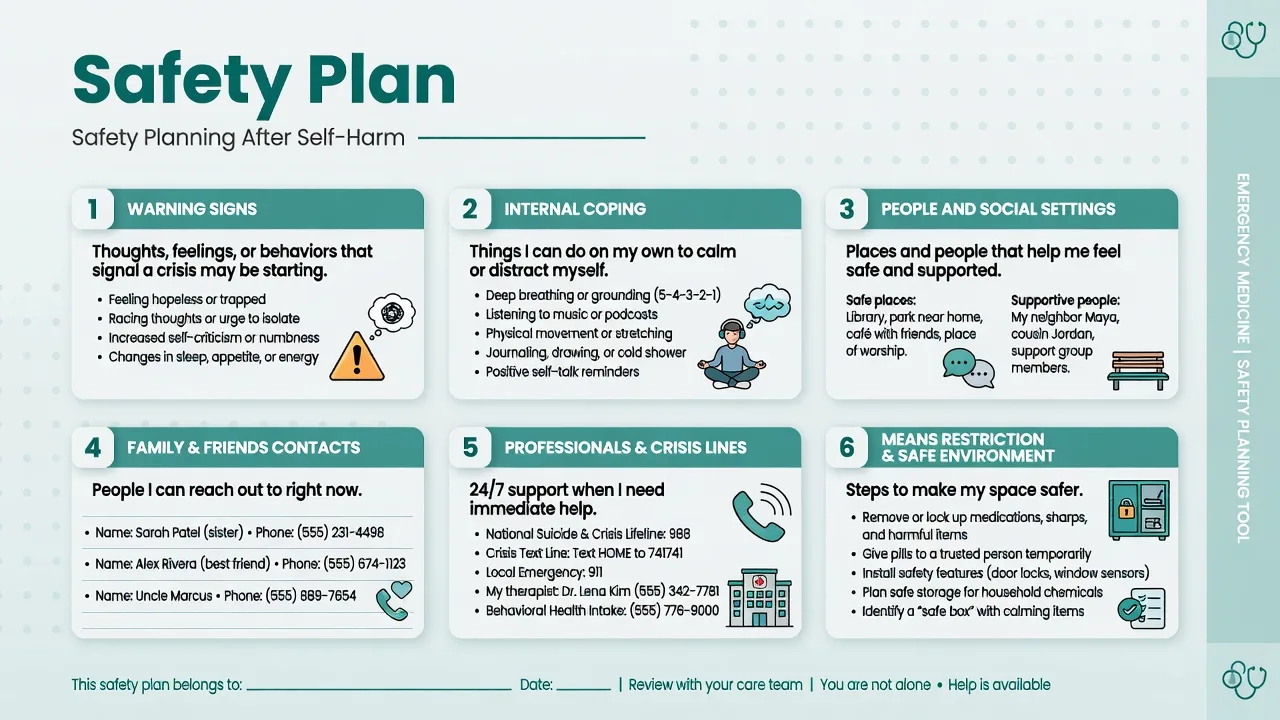
The safety plan and the means-restriction conversation are the two interventions that the emergency clinician delivers in every tier, and the evidence supports them as among the most effective suicide-prevention actions available in the immediate aftermath of an attempt. A safety plan is a written, collaborative document — the Stanley-Brown Safety Planning Intervention is the prototype — that lists the personal warning signs, the internal coping strategies, the social contacts and the professional contacts (including the crisis line) the patient will use if the suicidal thoughts return, and the steps taken to make the environment safe. The systematic review of safety-planning interventions confirms that they reduce suicidal behaviour and improve engagement with follow-up, and the effect is strongest when the plan is written, rehearsed and paired with a rapid follow-up contact.[4]
Means restriction rests on the observation that the availability of a lethal method drives completed suicide far more than the strength of the intent: the patient who survives a suicidal crisis because the chosen method was unavailable rarely substitutes another. The emergency clinician asks about access to means — firearms, a medication stockpile, a chosen location — and acts on the answer: securing firearms with a trusted person, limiting the quantity of medication dispensed, identifying a family member to hold the supply, and agreeing the steps with the patient and the family. Means-restriction counselling is the single most effective intervention the emergency clinician can deliver, and it is documented and revisited at every contact.[4]
Rainbow et al. — safety planning interventions for suicidality in adults (systematic review)
Chiew et al. — NACSTOP 2: early cessation of acetylcysteine after paracetamol overdose
Subtypes and scenarios
The young-female paracetamol overdose is the commonest scenario — usually low in medical toxicity, often a response to an interpersonal crisis, and high in repetition risk; the management is the medical treatment, the psychosocial assessment, and a credible follow-up plan. The elderly single-act attempter uses a high-lethality method on a first presentation and carries the highest completed-suicide rate of any age group; the threshold for admission is low and the regret at assessment does not negate the risk. The chronic repeater is at ongoing risk and the risk of therapeutic nihilism is real; each episode is assessed on its merits, the means are restricted, and an assertive care plan with the community team is maintained. The intoxicated patient is observed until sober before the assessment. The self-lacerator is assessed for the depth and the structures at risk, the surgical need, and the intent — distinguishing the superficial repetitive NSSI from the deep suicidal laceration. The postpartum mother is assessed for postpartum depression and psychosis, with the dual risk of suicide and infanticide, and admitted. The recently discharged psychiatric patient is in the highest-risk window and is treated as an emergency until a full reassessment.[3]
[9] [5]Special populations
Adolescents who self-harm are managed jointly with child and adolescent mental-health services, with attention to family dynamics, bullying, abuse, substance use and the developmental context; the threshold for admission is lower and the family is involved throughout. Older patients carry the highest completed-suicide rate of any group — high-lethality methods, physical illness, depression, social isolation and a powerful first-episode signal — and the threshold for admission is correspondingly low; an antipsychotic, where one is needed, is dosed at the lowest end of the range. Postpartum patients are assessed for perinatal mental illness and admitted where postpartum psychosis is suspected. The intellectually disabled or autistic patient needs a patient, adapted assessment, a familiar carer, and recognition that the behaviour may reflect pain, constipation, infection or sensory overload rather than a primary psychiatric relapse. Culturally and linguistically diverse patients are assessed with a trained interpreter, and a cultural formulation is sought where available. Aboriginal and Torres Strait Islander peoples, and other First Nations peoples with elevated suicide rates, are engaged with cultural support and a social-and-emotional-wellbeing framework alongside the clinical assessment. The repeater is held within an assertive, non-judgemental care plan that treats each presentation as serious.[15]
Special populations — the clinical detail
The risk assessment and the disposition are tailored to the population, because the risk factors, the protective factors, the pharmacology and the legal framework differ. The candidate must be able to describe the specific approach to the adolescent, the elderly patient, the postpartum mother, the patient with chronic medical illness, and the culturally and linguistically diverse patient.[6]
Adolescents have the highest rates of self-harm of any age group, and the rates have risen steeply over the last decade, most in young women. The risk factors include family conflict, bullying (including cyberbullying), abuse, academic pressure, social media exposure, substance use, and the developmental context of identity formation. The JAMA Network Open systematic review and meta-analysis of risk and protective factors for suicide mortality in youths confirms the dominant risk factors — a prior attempt, depression, substance use, access to lethal means, and recent loss — and identifies the protective factors — family connectedness, school engagement, and access to mental-health care.[18] The threshold for admission is lower in the adolescent, the family is involved throughout (with the limits of confidentiality explained), and the management is a joint effort with child and adolescent mental-health services. The umbrella review of therapeutic interventions for adolescent suicidal behaviour confirms the evidence for cognitive-behavioural therapy, dialectical behaviour therapy for adolescents, and the safety-planning intervention, and it supports the brief admission for the acute crisis and the assertive community follow-up.[20]
Older patients carry the highest completed-suicide rate of any age group — the case-fatality of the first attempt is high because the methods are high-lethality (hanging, firearm), the physiological reserve is low, the physical illness and the pain are common, the depression is often untreated, and the social isolation is profound. The depression in the older patient presents atypically — with somatic complaints, cognitive impairment, and agitation rather than the classic low mood — and it is screened for explicitly. The threshold for admission is low: a first-episode elderly self-harm presentation is treated as high risk until a comprehensive assessment proves otherwise. The pharmacology is cautious — an antipsychotic, where one is needed, is started at the lowest dose and titrated slowly, because the elderly patient is vulnerable to the extrapyramidal side effects, the falls, the orthostatic hypotension and the QT prolongation. An SSRI is the first-line antidepressant; tricyclics are avoided in the elderly because of the anticholinergic and the cardiotoxic burden.[15]
Postpartum patients are assessed for perinatal mental illness — the postpartum depression (common, the "blues" progressing to a depressive episode within weeks of delivery) and the postpartum psychosis (rare, a psychiatric emergency presenting within two weeks of delivery with delusions, hallucinations, confusion and the risk of suicide and infanticide). The postpartum psychosis is a psychiatric emergency: the mother is admitted to a mother-and-baby unit, the antipsychotic is started, and the infant is protected. The dual risk of maternal suicide (a leading cause of maternal death in the year after delivery) and infanticide is addressed explicitly — the case report on postpartum psychosis and infanticide documents the catastrophic outcome of the missed diagnosis, reinforcing the low threshold for admission.[13]
Patients with chronic medical illness — cancer, end-stage renal disease, chronic obstructive pulmonary disease, chronic pain, HIV, neurological disease — are at elevated suicide risk, and the physical illness is both a risk factor and a contributor to the depression. The assessment includes the pain, the prognosis, the treatment burden, and the patient understanding of the illness. The palliative-care and the chronic-pain input is sought where appropriate, and the safety plan is adapted to the illness context. The clinician does not assume that the self-harm is a "rational" response to the illness — the depression and the hopelessness are treatable even in the context of the chronic disease, and the risk assessment and the disposition follow the same structured approach.[9]
Adolescents
- Highest rates of self-harm of any age group; rising over the last decade, most in young women; family conflict, bullying, abuse, social media
- Risk factors: prior attempt, depression, substance use, access to means, recent loss; protective factors: family connectedness, school engagement, access to care
- Management: joint with CAMHS; family involved throughout; lower threshold for admission; CBT, DBT-A, safety planning
- Confidentiality: explain the limits; involve the family wherever possible with the adolescent consent; mandatory reporting of abuse
Elderly patients
- Highest completed-suicide rate of any age group; high-lethality methods (hanging, firearm), low physiological reserve, physical illness, social isolation
- Depression presents atypically — somatic complaints, cognitive impairment, agitation; screen for depression explicitly; first-episode attempt is high-risk
- Management: low threshold for admission; SSRI first-line (avoid tricyclics); antipsychotic at the lowest dose if needed; cautious pharmacology
- Do not discharge a first-episode elderly attempt as low risk; the regret at assessment does not negate the high case-fatality of the first attempt
Postpartum patients
- Postpartum depression (common, within weeks) and postpartum psychosis (rare, within 2 weeks, a psychiatric emergency)
- Postpartum psychosis: delusions, hallucinations, confusion; dual risk of maternal suicide (a leading cause of maternal death) and infanticide
- Management: admit to a mother-and-baby unit; antipsychotic; protect the infant; the emergency clinician does not discharge a suspected postpartum psychosis
- Maternal suicide is a leading cause of direct and indirect maternal death in the year after delivery; the diagnosis is clinical and the threshold for admission is zero
Chronic medical illness
- Cancer, ESRD, COPD, chronic pain, HIV, neurological disease; the physical illness is both a risk factor and a contributor to the depression
- Assess the pain, the prognosis, the treatment burden, the patient understanding; do not assume the self-harm is a "rational" response
- Management: palliative-care and chronic-pain input; treat the depression and the hopelessness; adapt the safety plan to the illness context
- The risk assessment and the disposition follow the same structured approach — the chronic illness does not exempt the patient from the full psychosocial assessment
Ruch et al. — risk and protective factors for suicide mortality in youths (JAMA Network Open systematic review)
Witt et al. — therapeutic interventions for adolescent suicidal behaviour (BMC Psychiatry umbrella review)
Complications and pitfalls
The recurring errors are those the structured approach is designed to prevent. Discharging before the medical clearance — sending the patient to the mental-health team before the paracetamol level, the ECG and the toxicity treatment are complete — is the cardinal error, and it kills the patient with missed hepatotoxicity or tricyclic cardiotoxicity. Assessing the intoxicated patient produces a falsely low risk estimate; the patient is observed until sober. Relying on SAD PERSONS alone — applying a number in place of the structured assessment — misclassifies; the scale is a clinical aid, not a determinant.[2] Failing to remove means on discharge returns the patient to the lethal environment and is a recurring cause of completed suicide. Underestimating the elderly or the high-lethality attempter — discharging a first-episode elderly overdose because the patient is "regretful and cooperative" — misses the highest-risk group. Therapeutic nihilism with the chronic repeater — the assumption that "this is just what they do" — abandons a patient at ongoing high risk. Failing to detain the high-risk patient who wants to leave, out of reluctance or time pressure, leaves a high-risk patient in the community. Breaching confidentiality without lawful basis, or failing to involve the family where consent could reasonably be obtained, breaches the statute and the trust. Discharging without follow-up arranged loses the patient to care.
Evidence and regional guidelines
The evidence base for emergency self-harm practice draws on the medical-screening literature, the validated suicide-risk tools, the systematic reviews of risk factors and of safety-planning interventions, and the national guidelines. The medical-screening literature confirms that a focused, history-guided assessment identifies the toxicological threats that matter, and that indiscriminate routine investigation of the well patient is low-yield.[1] The SAD PERSONS scale, validated recently alongside the NO HOPE scale, stratifies short-term suicide risk usefully but with modest predictive value, reinforcing that no score replaces the structured clinical assessment.[2] The systematic review of suicide-reattempt risk factors identifies the prior attempt, depression and hopelessness, alcohol and substance misuse, and recent psychiatric discharge as the dominant predictors.[3] The systematic review of safety-planning interventions confirms that written, rehearsed plans paired with rapid follow-up reduce suicidal behaviour.[4] The psychosocial-assessment literature supports a compassionate, structured assessment for every self-harm presentation, with carer involvement and a safety plan before discharge.[5]
The further evidence informs the modern practice. The multicentre, prospective cohort studies of risk-scale accuracy (Quinlivan 2017, Carter 2018) confirm that the scales have only modest predictive value and should never replace the structured clinical assessment.[8][9] The Columbia Suicide Severity Rating Scale validation (Posner 2013) establishes the lifetime ascertainment of suicidal ideation and behaviour as a predictor of future suicidal behaviour.[7] The psychometric validation of the Beck Scale for Suicide Ideation confirms its reliability and its convergent validity.[6] The NACSTOP 2 non-inferiority trial (Chiew 2026) informs the duration of the acetylcysteine regimen in the selected low-risk paracetamol overdose.[11] The scoping review of acetylcysteine safety (Bateman 2026) documents the adverse-reaction profile.[16] The UK intensive-care case series of hanging and asphyxia survivors (Smith 2018) documents the high mortality and the prolonged intensive-care stay.[10] The wrist-cutting retrospective analysis (Hbaieb 2017) documents the frequency of deep-structure injury requiring surgical repair.[12] The postpartum psychosis case report (Iyengar 2026) documents the catastrophic outcome of the missed diagnosis.[13] The UK national joinpoint analysis of suicide methods (Geulayov 2026) documents the shift from overdose to hanging as the dominant method of completed suicide.[14] The population-level study of repeat self-harm hospitalisation (Hawton 2026) identifies the risk factors for repetition.[15] The perspectives on AI-supported firearm access screening and storage counselling (Betz 2026) documents the evolving means-restriction counselling practice.[17] The JAMA Network Open systematic review of youth suicide risk factors (Ruch 2026) and the umbrella review of adolescent interventions (Witt 2026) inform the adolescent-specific practice.[18][20] The case series on the cardiac and thrombotic effects of severe carbon monoxide poisoning (Rose 2026) documents the cardiac assessment as a core part of the workup.[19]
ANZ practice note. Each Australian state and territory and New Zealand has its own Mental Health Act. In New South Wales the Mental Health Act 2007 allows detention of a mentally ill or mentally disordered person on the certificate of an authorised medical practitioner (the Schedule 1 document), with police assistance under section 9 and transport under section 81. Victoria's Mental Health Act 2014 uses Assessment Orders and Temporary Treatment Orders. The Australasian College for Emergency Medicine publishes guidance on mental-health presentations in the emergency department, emphasising the exclusion of organic and toxicological causes, a recovery-oriented approach, and the role of the emergency clinician in assessment, stabilisation and referral. Capacity is assessed under the common law and the guardianship legislation of each state.[1]
SAQ — Parasuicide risk assessment after a paracetamol overdose in a young woman
10 minutes · 10 marks
A 23-year-old woman is brought to the emergency department by her flatmate three hours after taking 24 tablets of 500 mg paracetamol (12 g) with half a bottle of wine after the breakdown of a two-year relationship. She is tearful and distressed but fully alert (GCS 15), with heart rate 96, blood pressure 118/74, respiratory rate 18, SpO2 98 per cent on room air, temperature 36.8 degrees C, and a bedside glucose of 5.4 mmol/L. She has a single previous overdose at age 18 (paracetamol, no admission) and is prescribed sertraline 50 mg by her general practitioner for a mild depressive illness. She lives alone and has limited social contact. The four-hour paracetamol level is subsequently reported as 90 mg/L.
SAQ — Discharge planning and safety planning after deliberate self-harm
10 minutes · 10 marks
A 45-year-old man presents to the emergency department after lacerating both wrists in the bathroom following the loss of his job three days ago. The lacerations are superficial and he has been medically cleared and sutured. He remains tearful and discloses ongoing suicidal ideation with a vague plan to take his remaining supply of temazepam but states he does not intend to act on it today. His wife has attended with him and is supportive and willing to be involved in the discharge plan. He has no prior psychiatric history and no prior self-harm.
Exam pearls
- Medical clearance first, psychosocial assessment second — the paracetamol level, the salicylate level, the ECG for tricyclic widening and the glucose come before the risk assessment; the patient who dies of untreated toxicity awaiting the mental-health team has been failed at the first step.
- Never assess the intoxicated patient — observe under the doctrine of necessity until sober, then reassess; the history, the intent and the capacity assessment are unreliable while intoxicated.
- A prior suicide attempt is the single strongest predictor of future completed suicide; every self-harm presentation is taken seriously, including the chronic repeater and the single-tablet overdose.
- SAD PERSONS scores Sex, Age, Depression, Previous attempt, Ethanol, Rational thinking loss, Organised plan, No social support, Sickness; a score of 5 or more is high risk, but the scale is a clinical aid, not a determinant of disposition.
- The three tiers: high risk (plan plus means plus intent) is admitted, voluntarily or involuntarily; moderate risk (ideation plus a plan) goes to the crisis team with a safety plan; low risk (ideation only) goes to the GP with a safety plan.
- Means restriction is the single most effective ED suicide-prevention intervention — secure firearms, limit the dispensed quantity, agree a trusted holder; the availability of a lethal method drives completed suicide more than the strength of the intent.
- The safety plan is written, not verbal (Stanley-Brown), rehearsed with the patient, and paired with a follow-up contact within 48 hours.
- The elderly and the high-lethality attempter default to admission — high-lethality methods, low physiological reserve, physical illness and isolation make the first episode in an older person a high-risk presentation.
- The first four weeks after psychiatric discharge are the highest-risk window — a recently discharged patient who re-presents is an emergency until a full reassessment proves otherwise.
- The methods and their workup: paracetamol (level at 4 hours, nomogram, NAC), tricyclic (ECG, QRS > 100 ms, sodium bicarbonate 1–2 mmol/kg), benzodiazepine (flumazenil avoided in the mixed overdose), opioid (naloxone 0.4–0.8 mg), salicylate (level, alkaline diuresis, dialysis); self-cutting (examine for tendon/nerve/vessel injury); hanging (trauma call, C-spine, TTM at 36 degrees, prognosticate at 72 hours); CO (COHb level, ECG, 100% oxygen, hyperbaric for the severe case).
- The Columbia Suicide Severity Rating Scale (C-SSRS) grades the ideation (1–5 from passive wish to intent with plan) and the behaviour (actual, interrupted, aborted attempts and preparatory acts) separately; the dominant US tool, embedded in the Zero Suicide framework.
- The Beck Scale for Suicide Ideation (BSSI) is a 19-item self-report scale; Beck demonstrated that hopelessness predicts completed suicide more strongly than the severity of the depression.
- No risk scale is accurate enough to use as the sole discharge screen — the multicentre validations (Quinlivan 2017, Carter 2018) confirm modest predictive value; the scales support, they do not replace, the structured clinical assessment.
- The six domains of the psychosocial assessment: precipitant (relationship/financial/legal), psychiatric history, substance use, family history, access to means, protective factors — supported by collateral from the family, the GP and the prior record.
- Postpartum psychosis is a psychiatric emergency — delusions, hallucinations and confusion within two weeks of delivery; the dual risk of maternal suicide and infanticide; admit to a mother-and-baby unit, never discharge from the ED.
- The chronic medical illness patient is at elevated risk (cancer, ESRD, COPD, chronic pain); the physical illness is both a risk factor and a contributor to the depression; do not assume the self-harm is a "rational" response — the depression and the hopelessness are treatable.
- The firearm is the highest-lethality means — ask about access directly, document the answer, and act on it (secure with a trusted person, remove from the home); the availability of a firearm drives the case-fatality of a suicide attempt more than any other single factor.[15]
Red flags
[15]References
- [1]Ünlü L, Özdemir F, Akıllı A. Medical screening of adult psychiatric patients presenting to the emergency department. Annals of Emergency Medicine, 2026.PMID 42233919
- [2]Sanz-Gómez S, et al. Predictive validity of the SAD PERSONS and NO HOPE scales in a sample of suicide attempters. Frontiers in Psychology, 2025.PMID 40342345
- [3]Pemau A, Hegerl U, Leischker A, Rummel-Kluge C. Risk factors for suicide reattempt: a systematic review and meta-analysis. Psychological Medicine, 2024.PMID 38623694
- [4]Rainbow E, et al. Safety planning interventions to address suicidality in adults: a systematic review. British Journal of Clinical Psychology, 2026.PMID 41424118
- [5]Quinlivan L, et al. Psychosocial interventions for self-harm and suicide prevention in liaison psychiatry. BMC Psychiatry, 2025.PMID 41310541
- [6]Amini M, et al. Psychometric assessment of Beck Scale for Suicidal Ideation (BSSI) in general population. Medical Journal of the Islamic Republic of Iran, 2015.PMID 26793659
- [7]Posner K, Brown GK, Stanley B, et al. Prediction of suicidal behavior in clinical research by lifetime suicidal ideation and behavior ascertainment — the Columbia Suicide Severity Rating Scale. Journal of Clinical Psychiatry, 2013.PMID 24107762
- [8]Quinlivan L, et al. Predictive accuracy of risk scales following self-harm: multicentre, prospective cohort study. British Journal of Psychiatry, 2017.PMID 28302702
- [9]Carter G, et al. Accuracy of risk scales for predicting repeat self-harm and suicide: a multicentre, population-level cohort study. BMC Psychiatry, 2018.PMID 29699523
- [10]Smith S, et al. Hanging and asphyxia: interventions, patient outcomes and resource utilisation in a UK tertiary intensive care unit. Journal of the Intensive Care Society, 2018.PMID 30159011
- [11]Chiew AL, et al. Early cessation of acetylcysteine treatment after paracetamol overdose (NACSTOP 2): a non-inferiority trial. Medical Journal of Australia, 2026.PMID 41549406
- [12]Hbaieb I, et al. Analysis of 41 suicide attempts by wrist cutting: a retrospective analysis. European Journal of Trauma and Emergency Surgery, 2017.PMID 26626872
- [13]Iyengar R, et al. A critique on maternal insanity: a case of postpartum psychosis and infanticide. Clinical Case Reports, 2026.PMID 42004880
- [14]Geulayov G, et al. Trends in methods of suicide among mental health patients between 2000 and 2022 in the UK: a joinpoint analysis. Journal of Affective Disorders, 2026.PMID 41672151
- [15]Hawton K, et al. Risk factors for repeat self-harm hospitalisation following hospital admissions for suicidal ideation or attempt. Social Psychiatry and Psychiatric Epidemiology, 2026.PMID 41758224
- [16]Bateman DN, et al. Safety of acetylcysteine: a scoping review of iatrogenic overdose cases and their associated complications. Clinical Toxicology, 2026.PMID 42370551
- [17]Betz ME, et al. Perspectives on artificial intelligence supported firearm access screening and storage counseling in the emergency department. American Journal of Emergency Medicine, 2026.PMID 42296675
- [18]Ruch DA, et al. Risk and protective factors for suicide mortality in youths: a systematic review and meta-analysis. JAMA Network Open, 2026.PMID 42390862
- [19]Rose JJ, et al. Cardiac and thrombotic effects of severe carbon monoxide poisoning: a case series. Undersea and Hyperbaric Medicine, 2026.PMID 42365948
- [20]Witt KG, et al. Therapeutic interventions for adolescent suicidal behavior and self-harm: an umbrella review for developing clinical guidelines. BMC Psychiatry, 2026.PMID 42251356