EM · Infective endocarditis
Infective endocarditis (emergency department diagnosis and management)
Also known as IE · Bacterial endocarditis · Subacute bacterial endocarditis · SBE
Infective endocarditis — the Duke diagnostic criteria (the major and the minor, reproduced), the predisposing conditions (the prosthetic valve, the intravenous drug use, the congenital heart disease, the indwelling lines), the clinical presentation (the fever, the new murmur, the embolic and the immunological phenomena), the investigation strategy (the blood cultures before the antibiotics, the echocardiography), the empiric and the targeted antibiotic regimens with doses (the flucloxacillin, the vancomycin, the gentamicin, the rifampicin), the surgical indications, and the antibiotic prophylaxis for the high-risk dental procedures. ACEM-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Related topics
Infective endocarditis is the microbial infection of the endocardial surface — usually a heart valve — and it is a condition that ranges from the insidious (a month of a low-grade fever and a new murmur) to the fulminant (an acute valve destruction with a heart failure and a septic shock within days). The Fellowship candidate must know the Duke diagnostic criteria, the investigation strategy (the blood cultures before the antibiotics, the echocardiography), and the empiric antibiotic regimens, because the early diagnosis and the appropriate antibiotic choice are the determinants of the survival.[1][2][3]
Definition and classification
Infective endocarditis is a microbial infection of the endocardial surface, most commonly involving a heart valve (native or prosthetic) but also the mural endocardium, a septal defect or an indwelling device. It is classified by the tempo (the acute — a virulent organism like the Staphylococcus aureus destroying a valve within days; and the subacute — a less virulent organism like the Streptococcus viridans over weeks), by the valve (the native vs the prosthetic — a critical distinction because the management differs), and by the predisposition (the intravenous drug use, the congenital heart disease, the prosthetic material, the healthcare-associated).[6]
A useful further subdivision is by the timing of the prosthetic valve infection: the early prosthetic valve endocarditis (within 60 days of the surgery — a nosocomial or a perioperative organism, the coagulase-negative Staphylococcus and the S. aureus), the intermediate (60 days to 12 months), and the late (over 12 months — a community organism, the viridans streptococci and the enterococci, similar to a native valve). The timing predicts the organism and so it dictates the empiric regimen. Healthcare-associated endocarditis now accounts for over a third of all cases, and it carries a higher mortality than the community-acquired disease.[5]
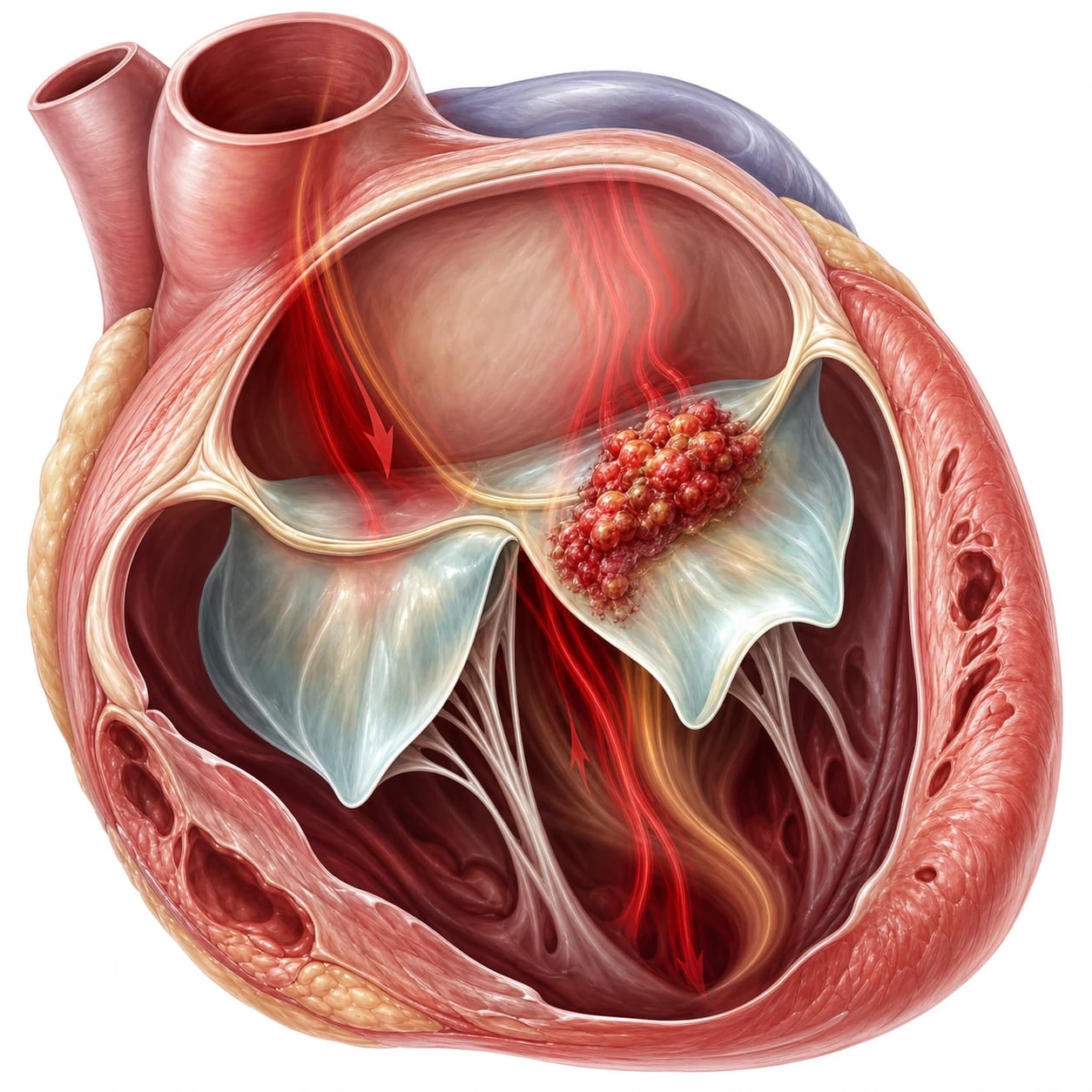
Pathophysiology — the vegetation and the embolism
The endocarditis begins when a microorganism in the bloodstream (a transient bacteraemia from a dental procedure, an intravenous injection, an indwelling line or a skin infection) colonises a damaged area of the endocardium or a prosthetic surface. The damaged endothelium (from a turbulent jet, a regurgitant valve, or a foreign body) accumulates platelets and fibrin — a sterile vegetation — which is then seeded by the circulating bacteria. The infected vegetation grows, and its fragments embolise to the brain (the stroke), the spleen (the infarct), the kidney, the mesentery, the limbs, or the coronary arteries (the myocardial infarction). The local destruction of the valve produces a regurgitation and, in the severe case, a heart failure. The immune response to the persistent bacteraemia produces the immunological phenomena (the Osler nodes, the Roth spots, the glomerulonephritis).[8]
The vegetation is also the physical substrate of the antibiotic failure — the bacteria within it are sequestered from the host defences and in a state of a reduced metabolic activity (the biofilm on the prosthetic material, the stationary phase in the deep layers). This is why the bactericidal, concentration-independent beta-lactams and the synergistic aminoglycoside combinations are required, and why the rifampicin (which penetrates the biofilm) is added for the prosthetic material.[5]

Differential diagnosis — the Duke criteria
The diagnosis of the infective endocarditis is made by the Duke criteria, and the Fellowship candidate must reproduce them. The Duke criteria combine the clinical, the microbiological and the echocardiographic evidence into a definite, a possible or a rejected diagnosis.[3]
Major criteria (2)
- A positive blood culture for a typical organism (two separate cultures for viridans strep, Strep gallolyticus, HACEK, Staph aureus, or community-acquired enterococcus)
- Echo evidence: a vegetation, an abscess, a new partial dehiscence of a prosthetic valve, or a new regurgitation
Minor criteria (5)
- A predisposition: a predisposing heart condition or an IV drug use
- A fever (38 degrees Celsius or above)
- A vascular phenomenon: a major arterial embolus, a septic pulmonary infarct, a mycotic aneurysm, an intravenous haemorrhage, a conjunctival haemorrhage, a Janeway lesion
- An immunologic phenomenon: a glomerulonephritis, an Osler node, a Roth spot, a rheumatoid factor
- A microbiological evidence not meeting a major criterion
Definite IE
- 2 major OR 1 major + 3 minor OR 5 minor criteria
- Or a pathological or a surgical confirmation
- The echo is the key investigation
- Blood cultures before the antibiotics
Possible IE
- 1 major + 1 minor OR 3 minor
- A clinical suspicion not meeting the definite criteria
- Needs the further investigation (the TOE, the repeat cultures)
- May still warrant the empiric antibiotics
Definite endocarditis is 2 major, or 1 major and 3 minor, or 5 minor criteria (or a pathological confirmation from a surgery or an autopsy). Possible endocarditis is 1 major and 1 minor, or 3 minor. The diagnosis is rejected if a firm alternative diagnosis is made, or the resolution occurs with less than 4 days of the antibiotics.[2]
The two major criteria are worth memorising verbatim, because the Fellowship viva rewards the precise wording. Major one — the blood culture: a typical endocarditis organism (the viridans streptococci, the Streptococcus gallolyticus, the HACEK group, the Staphylococcus aureus, or the community-acquired enterococci) recovered from two separate blood cultures drawn at different times; OR a persistent bacteraemia (two positive cultures drawn more than 12 hours apart, or three of three or a majority of four or more cultures drawn over the first hour); OR a single positive Coxiella burnetii blood culture or a phase-I IgG titre above 1:800. Major two — the endocardial involvement: the echocardiogram positive for IE — an oscillating intracardiac mass on a valve or supporting structures, in the path of regurgitant jets, or on implanted material; an abscess; a new partial dehiscence of a prosthetic valve; a new valvular regurgitation (a worsening of a pre-existing murmur is not sufficient).[2]
The ED diagnostic pathway for the suspected infective endocarditis
Recognise the syndrome
Draw the blood cultures BEFORE the antibiotics
The baseline investigations
The transthoracic echo (TTE)
The transoesophageal echo (TOE)
Apply the Duke criteria and admit
The predisposing conditions and the organisms
The predisposing conditions include the prosthetic valve (the highest risk), the previous infective endocarditis, the congenital heart disease (especially the cyanotic and the unrepaired), the rheumatic heart disease, the bicuspid aortic valve, the mitral valve prolapse with a regurgitation, the hypertrophic cardiomyopathy, the intravenous drug use, and the indwelling intravascular devices (the central lines, the pacemakers, the haemodialysis catheters).[4]
The causative organisms follow predictable patterns, and the Fellowship candidate must pair the organism with the clinical context because it dictates the empiric regimen.[4]
Viridans streptococci (the #1 cause of the native-valve IE)
- The commonest cause overall of the community-acquired native-valve IE (25 to 40 per cent)
- The subacute presentation — a dental origin, a month of a low-grade fever
- Usually penicillin-sensitive — benzylpenicillin or ceftriaxone; a 4-week course
- Includes the S. sanguinis, S. mutans, S. mitis, S. oralis groups
Staphylococcus aureus (the acute aggressive)
- The commonest cause of the healthcare-associated and the IVDU endocarditis
- The acute fulminant course — a rapid valve destruction, a sepsis, a high mortality (25 to 40 per cent)
- Right-sided (tricuspid) in the IVDU; left-sided and destructive in the nosocomial
- MSSA: flucloxacillin/nafcillin + gentamicin for 3 to 5 days; MRSA: vancomycin. A bacteraemia mandates the echo.
Enterococci
- A genitourinary or a gastrointestinal origin — the older man with the prostatic disease, the woman with a UTI
- E. faecalis is the usual; often a subacute course
- Intrinsically and acquired-resistant — ampicillin + gentamicin (or ceftriaxone), a 6-week course
- VRE: linezolid or daptomycin — involve the infectious-diseases team
Fungi (Candida — the IVDU and the prosthetic)
- The Candida species in the IVDU and in the long-term central-line/prosthetic patients
- The large friable vegetations with a catastrophic embolism — the surgery is usually required
- Blood cultures are often negative; the serology and the valve histology make the diagnosis
- Liposomal amphotericin B +/- flucytosine, then long-term fluconazole suppression — and the early surgical referral
HACEK and the culture-negative
- HACEK (Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella) — the fastidious, slow-growing oropharyngeal organisms
- Culture-negative: the Coxiella burnetii (Q fever), the Bartonella, the Brucella — request the serology and the PCR
- A typical organism plus the negative routine cultures plus a prosthetic valve = think the culture-negative group
- Empiric: vancomycin + gentamicin + ceftriaxone while the extended cultures and the serology are pending
Investigations — the cultures and the echo
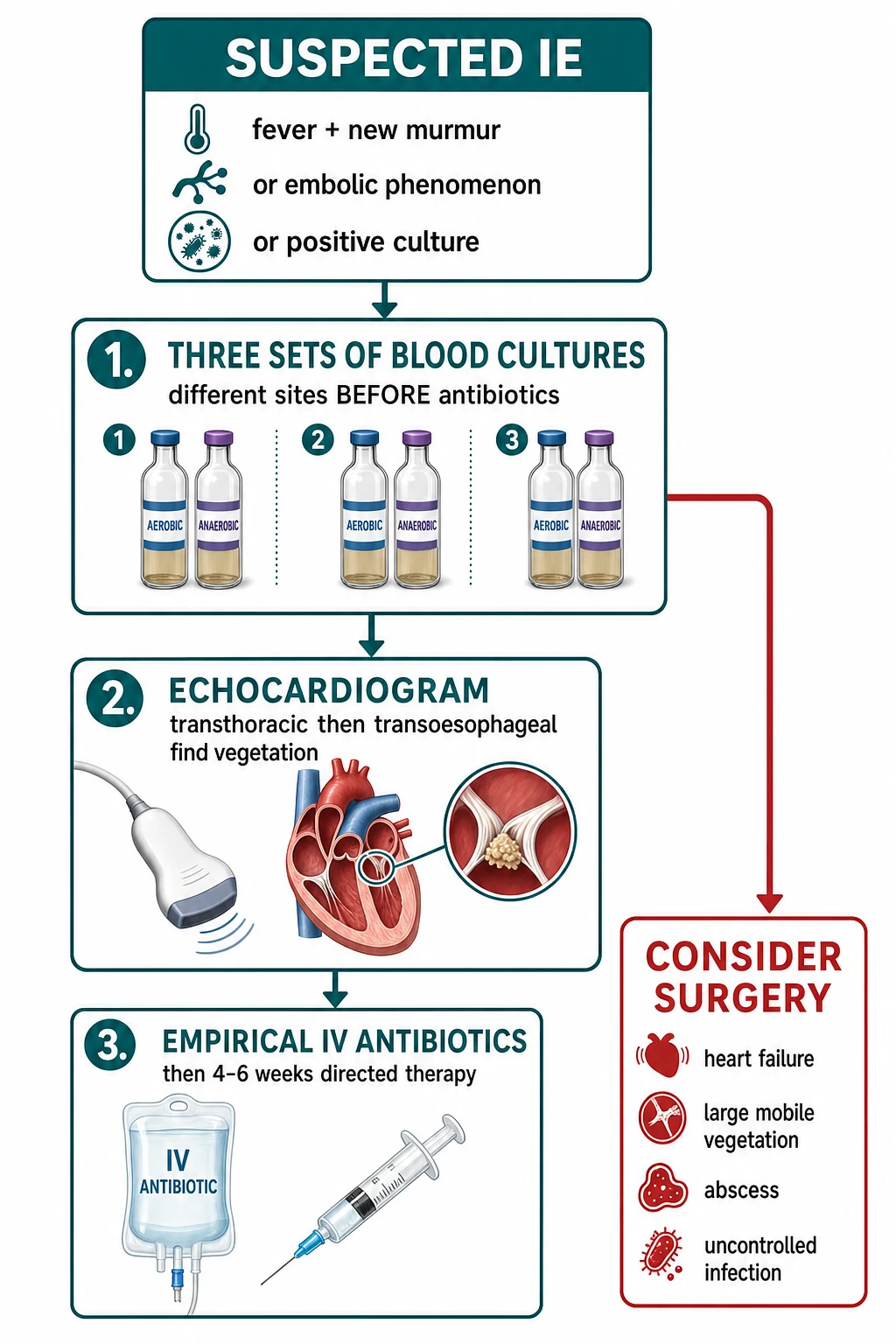
The blood cultures are taken BEFORE the antibiotics — three sets from three different venepuncture sites, spaced at least one hour apart, with a volume of 10 mL per bottle (the adult). A single set or a single site is a common error that reduces the sensitivity. If the antibiotics have been given already, the cultures are still taken (the yield is lower but not zero) and the antibiotic is withheld if the clinical situation allows. The full blood count may show an anaemia (the chronic disease), a raised white cell count, and a raised CRP. The urinalysis may show a haematuria (the glomerulonephritis). The ECG may show a conduction block (the aortic-root abscess extending into the septum). The chest radiograph may show the heart failure or the septic emboli. The echocardiography is the key investigation: the transthoracic echo (the TTE) is the first-line (the sensitivity 50 to 60 per cent for the native valve, lower for the prosthetic); the transoesophageal echo (the TOE) is performed if the TTE is negative but the suspicion persists (the sensitivity over 90 per cent). The echo looks for a vegetation, an abscess, a new regurgitation, and a prosthetic dehiscence.[8]
Transthoracic echo (TTE)
- The first-line imaging for every suspected case
- Sensitivity 50 to 60 per cent for a native-valve vegetation; 25 to 40 per cent for a prosthetic
- A quick, bedside, non-invasive study — and it assesses the haemodynamic consequence (the regurgitation, the ventricular function)
- A negative TTE never excludes the endocarditis — proceed to the TOE if the suspicion persists
Transoesophageal echo (TOE)
- Sensitivity over 90 per cent for a native-valve vegetation; 85 to 95 per cent for a prosthetic
- Mandatory for: the prosthetic valve, the suspected abscess/perivalvular extension, the staphylococcal bacteraemia, the negative TTE with a persistent suspicion, and before any surgical decision
- Better defines the abscess, the fistula, the perforation, and the prosthetic dehiscence
- A negative TOE with a high clinical suspicion should be repeated in 3 to 7 days — the vegetation may grow
Immediate management — the antibiotic regimen
The empiric antibiotic regimen depends on the valve and the likely organism, and it is de-escalated to the targeted regimen once the culture and the sensitivity are known.[4]
[8]The broad-spectrum empiric regimen — the vancomycin + gentamicin + cefepime — is reserved for the severely ill or the healthcare-associated native-valve presentation where the gram-negative (including the Pseudomonas) and the MRSA must all be covered until the cultures return. The cefepime (2 g intravenously every 8 hours) gives the anti-pseudomonal cover; the gentamicin and the vancomycin cover the staphylococci and the streptococci. This regimen is de-escalated to the targeted therapy within 48 to 72 hours of the culture result.[5]
The antibiotic escalation — from the empiric to the targeted regimen
Empiric (the first 48 to 72 hours)
Identify and de-escalate
The targeted therapy by the organism
Duration and the monitoring
The definitive (targeted) therapy is the organism-specific regimen, and the Fellowship candidate must pair the organism with the agent and the duration:[4]
Viridans streptococci (penicillin-sensitive)
- Benzylpenicillin 1.2 g IV every 4 to 6 hours, OR ceftriaxone 2 g IV daily
- A 4-week course (2 weeks of ceftriaxone + gentamicin is an option for the selected uncomplicated case)
- The MIC to the penicillin determines the regimen — the relatively-resistant (MIC 0.12 to 0.5) needs the gentamicin synergy
- The prognosis is the best of the IE organisms
Staphylococcus aureus (MSSA)
- Flucloxacillin or nafcillin or oxacillin 2 g IV every 6 hours (the drug of choice)
- Plus gentamicin 1 mg/kg every 8 hours for the first 3 to 5 days (the synergy — no longer routine for the whole course)
- A 6-week course for the left-sided; a 2-week option for the selected right-sided (IVDU) case
- The mortality is 25 to 40 per cent — the highest of the common organisms
Staphylococcus aureus (MRSA)
- Vancomycin 1 g IV every 12 hours (trough 15 to 20 mg/L)
- The gentamicin synergy is NOT routinely added for the MRSA (the nephrotoxicity)
- Consider daptomycin 6 to 10 mg/kg daily if the vancomycin MIC is high or the patient has a renal failure
- A 6-week course — and a higher failure rate than the MSSA
Enterococcus (ampicillin-sensitive)
- Ampicillin 2 g IV every 4 hours PLUS gentamicin 1 mg/kg every 8 hours
- A 6-week course (the 4-week option only for the symptoms under 3 months and the uncomplicated)
- Ampicillin + ceftriaxone is a less nephrotoxic alternative for the older patient
- VRE: linezolid or daptomycin — the infectious-diseases consult
The surgical indications
The emergency or the urgent surgery is indicated for: the heart failure from the valve destruction (the commonest cause of death and the strongest indication); the uncontrolled infection (the persistent bacteraemia despite 7 to 10 days of the appropriate antibiotics, the fungal or the highly resistant organism); the perivalvular extension (the abscess, the fistula, the heart block); the large mobile vegetation with a high embolic risk (over 10 mm with a prior embolus, or over 15 mm); and the prosthetic valve endocarditis with a dehiscence (the prosthetic endocarditis is a surgical disease). The surgery involves the valve repair or the replacement (the mechanical or the bioprosthetic), the debridement of the infected tissue, and the closure of the abscess.[8]
The Fellowship candidate should be able to reproduce the surgical indications as a structured list, because the viva rewards the categorisation. The five indications fall into three categories — the haemodynamic, the infective, and the embolic.[6]
Heart failure (the haemodynamic indication — the strongest)
- The commonest indication for the surgery and the commonest cause of the death
- The valve destruction causes a regurgitation that is not manageable with the medical therapy alone
- A NEW YORK HEART ASSOCIATION class III to IV heart failure from the IE is an urgent surgery — do not wait
- The early surgery in the heart failure halves the mortality compared to the delayed surgery
Uncontrolled infection (the infective indication)
- A persistent bacteraemia or a fever despite 7 to 10 days of the appropriate, bactericidal antibiotics
- The fungal, the multi-drug-resistant gram-negative, or the Brucella endocarditis — the antibiotics alone fail
- A prosthetic-valve infection with a persistent bacteraemia — the biofilm prevents the eradication
- The culture-negative with a relentless course — re-examine for the abscess and the fistula
Perivalvular extension (the infective/anatomical indication)
- The aortic-root or the annular abscess, the fistula, the prosthetic dehiscence
- A NEW heart block or a bundle-branch block on the ECG — the abscess has invaded the conduction tissue
- The TOE is the diagnostic test — the TTE misses the abscess
- A surgical emergency — the medical cure is not possible once the abscess has formed
Large mobile vegetation with the embolism (the embolic indication)
- A vegetation over 10 mm with a PRIOR embolic event — the recurrence risk is high
- A vegetation over 15 mm in isolation (the larger the vegetation, the higher the embolic risk)
- The vegetation over 10 mm plus the severe valve dysfunction (a combined embolic + haemodynamic indication)
- The embolic risk falls sharply after the first 2 weeks of the antibiotics — but the very-large mobile vegetation is still an urgent surgery
Prosthetic-valve endocarditis with the dehiscence
- The prosthetic endocarditis is a surgical disease — the antibiotic-only failure rate is up to 50 per cent
- A new or a worsening paravalvular leak, the prosthetic dehiscence, or the abscess mandates the surgery
- The early prosthetic infection (within 60 days) is the worst — the nosocomial organism, the high mortality
- The surgery is the debridement, the repair or the replacement, and the reconstruction of the annulus
Complications and pitfalls
The complications are the heart failure (the commonest cause of death), the embolic events (the stroke, the splenic, the renal, the mesenteric, the limb — the risk falls sharply after the first 2 weeks of the antibiotics), the perivalvular abscess (the aortic root, the heart block), the mycotic aneurysm (the cerebral — may rupture late), the glomerulonephritis, and the immune-complex phenomena. The pitfalls are: the antibiotics given before the blood cultures; a single blood culture set; relying on the TTE alone for a prosthetic valve (the TOE is needed); not screening for the colonic malignancy in the S. gallolyticus; the delayed TOE when the TTE is negative but the suspicion persists; and not referring early for the surgery when the heart failure develops.[4]
The complication surveillance during the treatment
The embolic risk window
The conduction surveillance
The renal surveillance
The persistent fever
Prognosis and disposition
The in-hospital mortality of the infective endocarditis is 15 to 20 per cent (higher for the Staph aureus, the prosthetic valve, and the elderly); the 1-year mortality approaches 30 per cent. The patient is admitted to the cardiology or the infectious-diseases service with the intravenous antibiotics for 4 to 6 weeks; the surgery is the decision for the cardiology and the cardiothoracic team; the follow-up includes the repeat echo, the blood cultures, the renal function, and the long-term valve surveillance. The antibiotic prophylaxis for the high-risk patients (the prosthetic valve, the previous IE, the congenital cyanotic) before the high-risk dental procedures (the scaling, the extraction, the root canal) is the standard — the amoxicillin 2 to 3 g orally one hour before (or the clindamycin 600 mg if allergic).[7]
Special populations
The intravenous drug user has a right-sided (tricuspid) endocarditis from the S. aureus — presenting with the fever, the cough, the septic pulmonary emboli (the chest radiograph shows the multiple cavitating lesions) and a murmur; the management is the flucloxacillin/vancomycin, and the 2-week course may be considered for the uncomplicated right-sided case. The prosthetic valve patient has a higher mortality and a surgical disease — the echo needs the TOE, the antibiotic regimen includes the rifampicin for the biofilm, and the surgery is the early consideration. The pregnant patient receives the beta-lactam antibiotics (the penicillins and the cephalosporins are safe; the gentamicin is used with caution; the rifampicin is avoided). The healthcare-associated endocarditis (from the indwelling lines, the haemodialysis) is increasingly common and the MRSA is the concern.[8]
[2] [6]Key trials and evidence
The modified Duke criteria (Li et al., 2000)
Clinical Infectious Diseases
PMID 10770721
A retrospective validation of the proposed modifications to the original 1994 Duke criteria, on a cohort of the pathologically-confirmed cases
Population: The patients with the suspected infective endocarditis, validated against the surgical and the autopsy pathology
Key finding
The modifications — the inclusion of the Coxiella serology as a major criterion, the redefinition of the possible IE, and the echocardiographic definition — improved the sensitivity for the definite IE without sacrificing the specificity. The modified Duke criteria became the global diagnostic standard.
Practice change
The modified Duke criteria of 2000 are the examination backbone for the diagnosis of the infective endocarditis — reproduce the two major and the five minor criteria verbatim.<Cite id="3"/>
The ICE-PCS: Staphylococcus aureus native-valve endocarditis (Miro et al., 2005)
Clinical Infectious Diseases
PMID 16028160
A prospective, multinational cohort from the International Collaboration on Endocarditis
Population: 566 episodes of the definite S. aureus native-valve infective endocarditis
Key finding
The S. aureus IE was aggressive: the acute presentation in over half, the heart failure in a third, the CNS embolisation in 20 per cent, and the in-hospital mortality of 22 per cent for the left-sided disease. The healthcare-associated acquisition and the left-sided involvement were the independent predictors of the mortality.
Practice change
The Staphylococcus aureus bacteraemia mandates the echocardiogram — the endocarditis is common, the disease is destructive, and the left-sided involvement is the lethal.<Cite id="6"/>
2015 ESC infective-endocarditis guideline (Habib et al.)
Heart
PMID 27288022
A multidisciplinary consensus guideline from the European Society of Cardiology
Population: The full spectrum of the infective endocarditis — the native, the prosthetic, and the device-related
Key finding
The guideline formalised the early-surgery pathway, the empiric-antibiotic regimens by the valve and the risk, the routine use of the TOE, the multidisciplinary endocarditis team, and the centre-of-excellence model. The antimicrobial prophylaxis was restricted to the highest-risk patients before the highest-risk procedures.
Practice change
The 2015 ESC guideline remains the contemporary framework for the management — the early-surgery pathway and the multidisciplinary team are the Fellowship-relevant messages.<Cite id="1"/>
Evidence and regional guidelines
The contemporary framework is the 2015 ESC infective-endocarditis guideline[1] and the 2023 Duke-ISCVID criteria (the updated diagnostic framework).[2] The 2015 AHA scientific statement[5] and the 2007 AHA prophylaxis guideline[7] are the North-American counterparts. The empiric regimen and the surgical pathway follow the local cardiology and the infectious-diseases protocol.
ANZ practice note. The Duke criteria, the blood cultures before the antibiotics, the echocardiography (the TTE then the TOE), and the empiric antibiotic regimens follow the ESC framework via the local cardiology and the infectious-diseases pathway; the antibiotic prophylaxis for the prosthetic valve and the previous IE before the dental procedures follows the NHMRC guidance. The Therapeutic Guidelines (eTG) antibiotic recommendations for the empiric cover — the flucloxacillin or the vancomycin, the gentamicin, and the rifampicin for the prosthetic — align with the ESC and are the examination standard for the ACEM candidate.[2]
Exam pearls
- Duke criteria: 2 major (positive blood culture for a typical organism + echo evidence) or 1 major + 3 minor or 5 minor → definite.
- Blood cultures BEFORE the antibiotics: 3 sets, 3 sites, 1 hour apart.
- A Staph aureus bacteraemia needs an echo — even the apparently uncomplicated case.
- Native valve: flucloxacillin 2 g IV 6-hourly + gentamicin; prosthetic: vancomycin + gentamicin + rifampicin (start after 3-5 days); IVDU: vancomycin + gentamicin.
- Heart failure from the valve destruction = the emergency surgery.
- S. gallolyticus (bovis) → colonoscopy (the colonic malignancy).
- Prophylaxis: amoxicillin 2-3 g orally 1 h before the dental procedure (prosthetic valve, previous IE, cyanotic congenital).
- Viridans streptococci are the #1 cause of the community-acquired native-valve IE; Staph aureus is the #1 cause of the healthcare-associated and the IVDU IE.
- A new AV block or a PR prolongation in a febrile patient = the aortic-root abscess — the TOE and the surgical referral.
- The empiric broad-spectrum (the vancomycin + gentamicin + cefepime) is for the severe or the healthcare-associated native-valve presentation; de-escalate at 48-72 hours.
- The definitive therapy: penicillin/ceftriaxone for the streptococci, nafcillin/oxacillin + gentamicin for the staphylococci; the duration is 4-6 weeks (2 weeks for the selected right-sided IVDU).
- The 5 surgical indications: the heart failure, the uncontrolled infection, the perivalvular extension, the large mobile vegetation with the embolism, and the prosthetic dehiscence.
- The rifampicin for the prosthetic valve is delayed 3-5 days to prevent the resistance; it penetrates the biofilm.
- The Candida endocarditis (the IVDU, the prosthetic, the long-term line) → the large friable vegetations, the early surgery, the amphotericin + flucytosine.
- The culture-negative IE: the Coxiella, the Bartonella, the Brucella — request the serology and the PCR; the empiric is the vancomycin + gentamicin + ceftriaxone.
- The early surgery after an ischaemic embolic stroke (once the haemorrhage is excluded); delay 4 weeks for the intracranial haemorrhage.
- The CIED (pacemaker/ICD) endocarditis → the complete lead and the generator extraction — the antibiotics alone do not cure the biofilm.[5]
Exam practice
SAQ — Diagnosis of infective endocarditis in the febrile IV drug user with septic pulmonary emboli
10 minutes · 10 marks
A 32-year-old man with active intravenous heroin use presents to the emergency department with five days of fever, a non-productive cough and two episodes of small-volume haemoptysis. On arrival he is febrile 39.1 degrees C, HR 118, BP 118/72, RR 24, SpO2 94 per cent on room air, GCS 15. Cardiovascular examination is technically difficult; no murmur is clearly heard. The chest is clear. The abdomen is soft. There are multiple peripheral, bilateral, wedge-shaped cavitating pulmonary infiltrates on the chest radiograph. The ECG is sinus tachycardia at 118 with a normal PR interval and no conduction abnormality. Finger-prick glucose 5.6, WCC 15.8, CRP 168, creatinine 78. Three separate sets of blood cultures have been drawn from three different venepuncture sites over the first hour, each 10 mL into aerobic and anaerobic bottles, with antibiotic administration deliberately withheld pending the results. The bedside transthoracic echo is technically poor and the vegetation is not seen.
SAQ — Empirical antibiotic selection and the surgical referral in early prosthetic-valve endocarditis
10 minutes · 10 marks
A 64-year-old man presents to the emergency department three weeks after an elective aortic-valve replacement (mechanical prosthesis) for bicuspid aortic stenosis, with seven days of low-grade fevers, malaise, anorexia and a new early-diastolic decrescendo murmur at the left sternal edge. He denies rigors, dental work or IV drug use. On arrival he is febrile 38.4 degrees C, HR 96, BP 118/68, RR 18, SpO2 97 per cent on room air, GCS 15. Surgical wound is intact and healed. Cardiovascular examination confirms the new early diastolic murmur (aortic regurgitation). The chest is clear. Abdomen soft. ECG shows sinus rhythm with a normal PR interval. WCC 12.6, CRP 92, creatinine 108, haemoglobin 118. Three sets of blood cultures from three sites have been drawn before antibiotic administration and are incubating. His transthoracic echo performed from a peripheral hospital last week was reported as technically difficult; the valve is not well visualised.
Red flags
[8]References
- [1]Habib G, Lancellotti P, Antunes MJ, et al. 2015 ESC Guidelines on the management of infective endocarditis. Heart, 2016.PMID 27288022
- [2]Papadimitriou-Olivgeris M, Iriart X, Laforêt C, et al. Evaluation of the 2023 Duke-ISCVID criteria for infective endocarditis. Clinical Infectious Diseases, 2024.PMID 38330243
- [3]Li JS, Sexton DJ, Mick N, et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clinical Infectious Diseases, 2000.PMID 10770721
- [4]Baddour LM, Wilson WR, Bayer AS, et al. Infective endocarditis: diagnosis, antimicrobial therapy, and management of complications. Circulation, 2005.PMID 15956145
- [5]Baddour LM, Wilson WR, Bayer AS, et al. Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications: a scientific statement for healthcare professionals. Circulation, 2015.PMID 26373316
- [6]Miro JM, Anguera I, Cabell CH, et al. Staphylococcus aureus native valve infective endocarditis: report of 566 episodes from the International Collaboration on Endocarditis Merged Database. Clinical Infectious Diseases, 2005.PMID 16028160
- [7]Wilson W, Taubert KA, Gewitz M, et al. Prevention of infective endocarditis: guidelines from the American Heart Association. Circulation, 2007.PMID 17446442
- [8]El-Ahdab F, Benjamin DK Jr, Wang A, et al. Risk of endocarditis among patients with prosthetic valves and Staphylococcus aureus bacteremia. American Journal of Medicine, 2005.PMID 15745719