EM · Raised intracranial pressure
Raised intracranial pressure
Also known as Intracranial hypertension · ICP · Cerebral herniation syndrome · Intracranial hypertension syndrome
Raised intracranial pressure is the syndrome of the cranial contents exceeding the compensatory reserve of the rigid skull — the Monro-Kelly doctrine and the compliance curve, the cerebral perfusion pressure equation (CPP = MAP minus ICP), the Cushing triad as a late pre-terminal sign, the herniation syndromes (uncal, central, tonsillar), the emergency management ladder (head elevation, osmotherapy with mannitol 0.5 g per kg or hypertonic saline 3 per cent 250 mL, transient hyperventilation to PaCO2 35, neurosurgery), the LP-before-CT contraindication, and the no-steroids-in-trauma rule. ACEM-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Raised intracranial pressure is the syndrome of the cranial contents exceeding the compensatory reserve of the rigid skull. A single principle governs every decision: the brain sits inside a closed, unyielding box, and when any one component expands — a haematoma, a tumour, oedema, or cerebrospinal fluid — the others must first be displaced, and once that reserve is spent, a small further increase in volume produces a steep, dangerous rise in pressure. Left untreated, rising pressure forces brain tissue through the tentorial notch or the foramen magnum — cerebral herniation — and this is the event that kills. The Fellowship candidate must therefore recognise the syndrome early, lower the pressure with osmotherapy when it threatens, and refer for definitive neurosurgical decompression, all while protecting the cerebral perfusion pressure (CPP = MAP minus ICP).[1][3]
Definition and classification
Intracranial pressure is normally 5 to 15 mmHg measured supine. Raised ICP is conventionally defined as a sustained pressure above 22 mmHg, the treatment threshold at which outcomes in severe brain injury deterior and at which therapy is initiated.[1] Three clinical contexts share the same pathophysiology and demand the same response. Acute raised ICP develops over hours — an expanding extradural haematoma, an intracerebral haemorrhage, an acute hydrocephalus, or fulminant hepatic failure with cerebral oedema — and presents the immediate herniation threat. Subacute raised ICP develops over days to weeks — a brain tumour, a chronic subdural haematoma, or a brain abscess — and presents with headache, vomiting and papilloedema in a patient who is still alert. Idiopathic intracranial hypertension (IIH) is a chronic, alert-patient variant of raised pressure with papilloedema and progressive visual loss, common in young obese women, with no mass on imaging and a high opening pressure on lumbar puncture.
Pathophysiology — the Monro-Kelly doctrine and the Cushing reflex
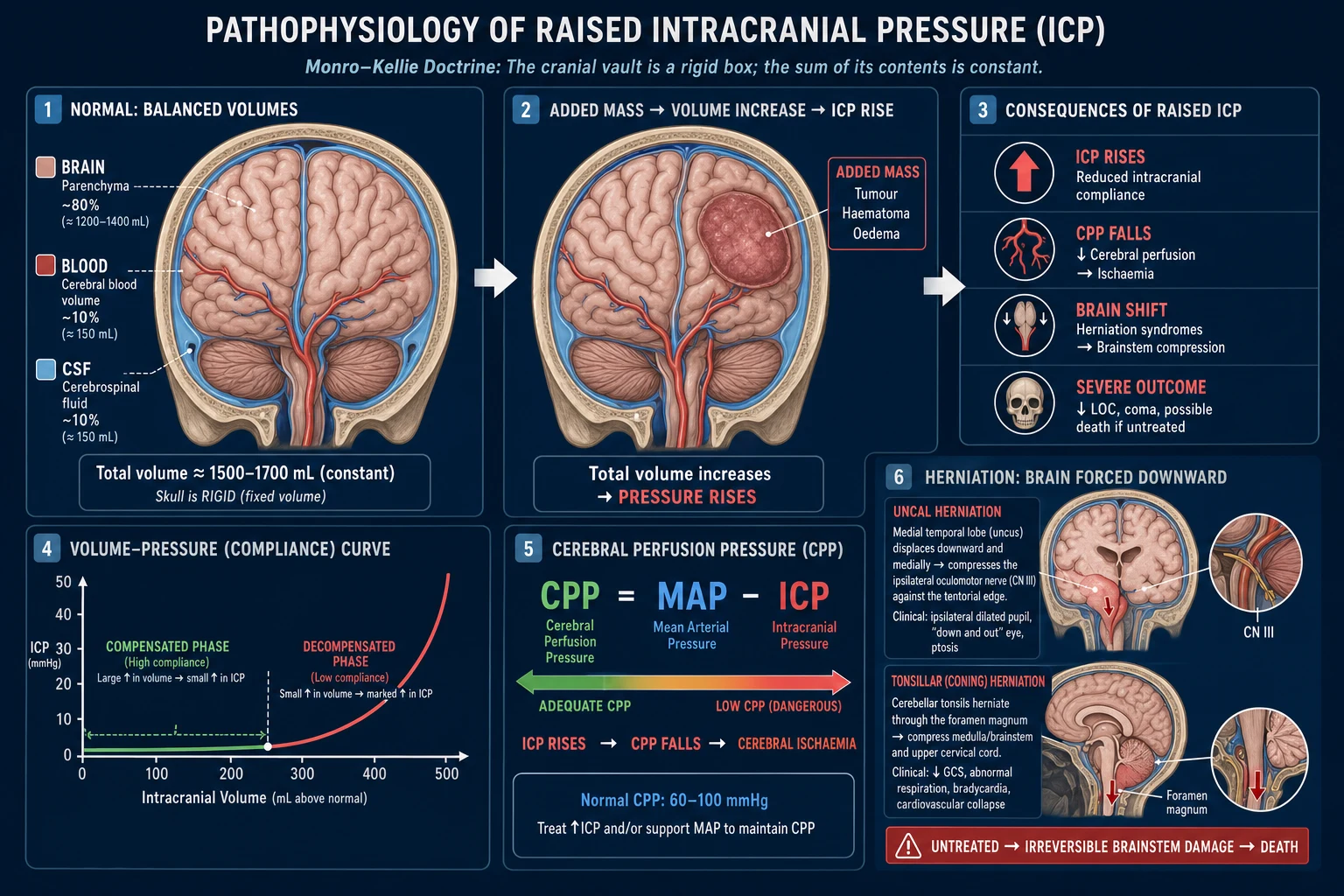
The skull is a rigid box containing three incompressible components: the brain parenchyma, the blood, and the cerebrospinal fluid, fixed at a combined total volume. This is the Monro-Kelly doctrine. When one component increases in volume — a tumour, a haematoma, oedema, or extra CSF in hydrocephalus — an equivalent volume must be displaced to keep the total constant. Initially, cerebrospinal fluid is shunted into the spinal canal and venous blood is compressed out of the dural sinuses, so the pressure rises only slightly (the flat part of the compliance curve). Once these reserves are exhausted, further volume expansion produces a steep, near-vertical rise in pressure — the decompensated phase. This is why a small additional increase (a cough, a hypoxic episode, a minor bleed) can precipitate sudden herniation in a patient who seemed stable.[9]
The pressure target the clinician actually defends is not the ICP alone but the cerebral perfusion pressure — CPP = MAP minus ICP — the driving gradient that delivers blood to the brain. As the ICP rises, the CPP falls, and below a CPP of about 60 mmHg cerebral ischaemia develops; this is the mechanism by which raised ICP causes secondary brain injury.[3]
[3]The Cushing reflex is the haemodynamic response to critical, pre-terminal intracranial hypertension. As the pressure rises and cerebral perfusion falls, medullary ischaemia triggers a sympathetic surge that raises systemic blood pressure (the hypertension); the carotid baroreceptors then sense this hypertension and trigger a vagal, compensatory bradycardia; and direct compression of the medullary respiratory centres produces the irregular (Cheyne-Stokes or ataxic) respiration. Together these form the Cushing triad — hypertension, bradycardia, and irregular breathing. Examiners stress one point above all: the Cushing triad is a late, pre-terminal sign, present in only a minority of patients with truly raised ICP, and its appearance means herniation is imminent. Its absence does NOT exclude raised ICP.[3]
Aetiology — what is expanding inside the skull
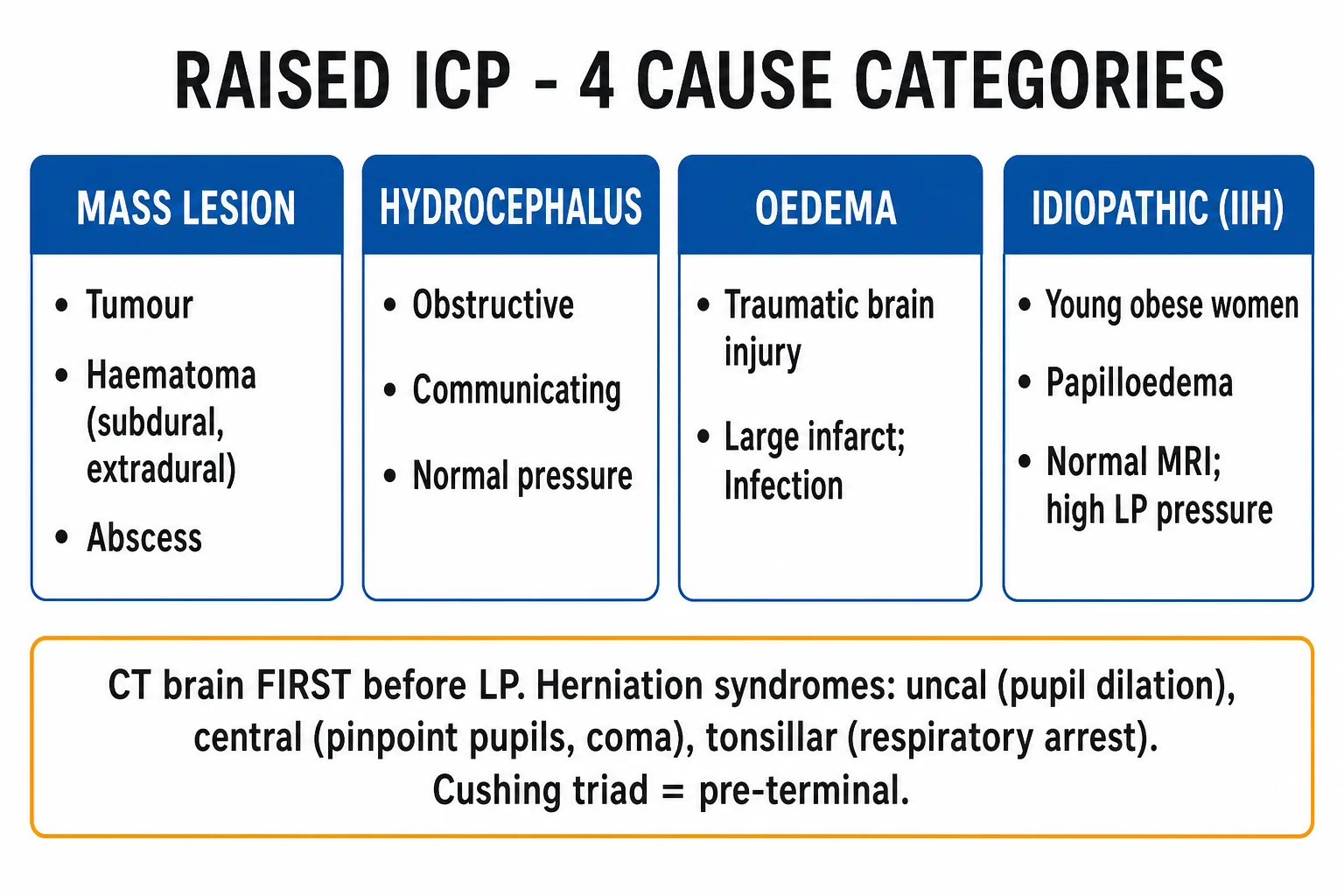
Every cause of raised ICP adds volume to one of the three Monro-Kellie compartments — extra parenchyma (a mass or oedema), extra blood (a haematoma or venous congestion), or extra CSF (hydrocephalus). Naming the compartment that is expanding tells you which definitive treatment follows: surgery for the mass, drainage for the hydrocephalus, dexamethasone for vasogenic oedema, or disease-specific therapy for the metabolic cause. The Fellowship candidate should be able to map any presenting scenario to one of these mechanisms.[3]
Trauma (most common acute)
- Extradural / subdural / intracerebral haematoma, contusions, traumatic oedema
- Mass lesion + midline shift on CT; the surgical lesion needs urgent craniotomy
- Diffuse axonal injury produces cytotoxic oedema and a slower ICP rise
- Cervical collar / head-down positioning can worsen venous outflow and ICP
Tumour
- Primary (glioma, meningioma) or metastatic (lung, breast, melanoma)
- Vasogenic oedema surrounds the mass — responsive to dexamethasone
- Subacute course; morning headache, vomiting, papilloedema
- Posterior-fossa tumours obstruct the fourth ventricle → hydrocephalus
Hydrocephalus
- Obstructive (posterior-fossa mass, aqueduct stenosis, 4th-ventricle haemorrhage) or communicating (SAH, meningitis)
- Acute obstructive hydrocephalus deteriorates over hours
- Definitive: external ventricular drain (also measures ICP)
- CT shows dilated ventricles, effaced cisterns, peri-ventricular lucency
Infection
- Brain abscess (ring-enhancing mass with oedema), subdural empyema, severe meningitis/encephalitis
- Abscess behaves as a mass with surrounding vasogenic oedema
- Empirical antibiotics + neurosurgical drainage for the abscess
- Meningitis raises ICP diffusely — LP contraindicated until CT excludes a mass
Hepatic encephalopathy
- Fulminant hepatic failure → cytotoxic cerebral oedema (astrocyte ammonia accumulation)
- Rapid ICP rise is the leading cause of death in acute liver failure
- Hypernatraemia (Na 145 to 155), osmotherapy, ICP monitor; urgent transplant assessment
- Distinct from the chronic confusion of cirrhotic encephalopathy
Metabolic / other
- Diabetic ketoacidosis (cerebral oedema, especially in children during fluid resuscitation)
- Severe hyponatraemia (osmotic water shift), hypoxic-ischaemic encephalopathy
- Hypertensive encephalopathy / PRES (vasogenic oedema, posterior-predominant)
- Idiopathic intracranial hypertension — young obese woman, no mass, high LP opening pressure
Clinical presentation and the herniation syndromes
The general features of raised ICP are headache (characteristically worse in the morning, on bending forward, coughing or straining, and relieved by vomiting), projectile vomiting (often without preceding nausea), papilloedema on fundoscopy, a decreased Glasgow Coma Score, focal neurological deficit, and occasionally a sixth-nerve palsy (a false localising sign from stretching of the abducens nerve). The headache of raised ICP is distinguished from tension-type and migraine headache by its progression, its morning predominance, its Valsalva-worsening, and its association with the other features.[3]
The herniation syndromes are the specific clinical patterns produced when brain tissue is displaced through the rigid dural partitions, and the examiner expects each one named.[1]
Uncal (lateral) herniation
- Most common; medial temporal lobe through the tentorial notch
- Ipsilateral fixed dilated pupil (CN III compression) → ptosis, "down and out" eye
- Contralateral hemiparesis (cerebral peduncle); occasionally ipsilateral (Kernohan notch)
- The classic pupil sign of raised ICP — osmotherapy + neurosurgery now
Central transtentorial
- Symmetric downward displacement of the diencephalon
- Bilateral small then fixed pupils; progressive loss of upgaze
- Decorticate → decerebrate posturing; respiratory depression
- A worse prognosis; bilateral brainstem compression
Tonsillar (downward)
- Cerebellar tonsils through the foramen magnum
- Neck stiffness, head tilt, downbeat nystagmus, sudden respiratory arrest
- The fatal mechanism of LP below a supra-tentorial pressure gradient
- Compresses the medulla directly
Subfalcine
- Cingulate gyrus under the falx cerebri
- Often clinically silent; may cause contralateral leg weakness (ACA compression)
- Common early herniation on CT; midline shift
- Precedes uncal herniation in many cases
Signs of raised ICP — the bedside findings to actively seek
The signs divide into those of pressure itself and those of herniation. The pressure signs (headache, vomiting, papilloedema, falling GCS) develop gradually; the herniation signs (the fixed pupil, the posturing, the Cushing triad) are pre-terminal and demand osmotherapy and a neurosurgical call in the same breath as they are found. A sixth-nerve (abducens) palsy is a false localising sign — it reflects stretching of the long, vulnerable nerve against the petrous bone as the brain shifts, not a local lesion.[3]
Decreased GCS
- The single most sensitive bedside marker of a rising ICP
- Reassess every 15 min; a drop of ≥2 points is an emergency
- The motor response (M1–M6) is the most informative component
- GCS ≤ 8 is the threshold for definitive airway protection / RSI
Unilateral dilated pupil
- Ipsilateral CN III compression by the displaced medial temporal lobe (uncus)
- First the pupil is sluggish, then fixed and dilated; ptosis and a "down-and-out" eye follow
- Equals uncal herniation until proven otherwise
- Mannitol 0.5 g/kg or 3% saline 250 mL + neurosurgery now
Papilloedema
- Blurred disc margins, loss of venous pulsation, then elevation and haemorrhages
- Takes hours to days to develop — absent early in acute herniation
- A sign of chronic / subacute pressure, not the acute emergency
- Bilateral; asymmetric visual loss is the threat in IIH
Cushing's triad
- Hypertension (widening pulse pressure) + bradycardia + irregular respiration
- A LATE pre-terminal sign — present in only a minority of raised-ICP patients
- Medullary ischaemia → sympathetic surge (BP) → baroreceptor vagal reflex (HR)
- Its absence does NOT exclude raised ICP
Abnormal posturing
- Decorticate (flexion of arms, extension of legs) — lesions above the red nucleus
- Decerebrate (extension of arms and legs) — lesions at or below the red nucleus
- Progression from decorticate to decerebrate signals descending brainstem compression
- Suggests central transtentorial herniation — worse prognosis than uncal
Differential diagnosis
The headache-and-vomiting or the reduced-conscious-level presentation must be distinguished from several mimics, and the distinction rests on the speed of onset, the pattern of the headache, the presence of focal signs, and the CT.[1]
Raised ICP (mass / oedema)
- Progressive morning headache, projectile vomiting, papilloedema, focal deficit
- CT shows a mass, midline shift, effaced basal cisterns, hydrocephalus
- Head elevation, osmotherapy, neurosurgical decompression
- No LP until a CT excludes the mass
Migraine
- Episodic, throbbing unilateral headache with aura/photophobia
- Normal GCS between attacks; no papilloedema; normal CT
- Treated with analgesia, antiemetic, triptan
- A diagnosis of exclusion in the atypical or first/worst headache
Meningitis / encephalitis
- Fever, neck stiffness, photophobia, altered conscious level, rash
- CT first if any focal sign or reduced GCS, then LP; antibiotics immediately
- Empirical ceftriaxone + aciclovir before the LP
- LP contraindicated if raised ICP is suspected
Hypertensive encephalopathy
- Severe BP with confusion, visual disturbance, seizures (PRES)
- Shifted autoregulation curve; lower BP gradually 10 to 20 per cent
- Titratable IV agent (labetalol, nicardipine)
- CT shows vasogenic oedema, typically posterior
Bedside assessment
Assess the airway, breathing and circulation first — a threatened airway or hypotension is itself a cause of secondary brain injury and demands immediate correction. Perform a focused neurological examination: the Glasgow Coma Score, recorded as its three components — eye opening (4 spontaneous to 1 none), verbal response (5 oriented to 1 none), and motor response (6 obeys commands to 1 none, and the best motor response the most informative single component) — reassessed serially, because a drop of two or more points signals a rising ICP; the pupils (size, symmetry and reactivity — a unilateral dilated unresponsive pupil is uncal herniation); fundoscopy for papilloedema (though acute papilloedema may be absent in the first hours); the vital signs (looking for the Cushing triad — hypertension with a widening pulse pressure, bradycardia, and an irregular respiratory pattern); and a motor examination for focal deficit or abnormal posturing (decorticate, decerebrate). Check the bedside glucose on every patient with a reduced conscious level — hypoglycaemia is a rapid, reversible mimic of raised ICP.[3]
Investigations — CT first, never LP first
The CT head is the definitive investigation and is performed as soon as the patient is stabilised (airway secured, oxygenation and blood pressure maintained). It identifies the cause — a haematoma, tumour, abscess, infarct with oedema, or hydrocephalus — and the signs of raised pressure: midline shift (over 5 mm is significant), effacement of the basal cisterns, sulcal compression, and loss of the grey-white differentiation. A normal CT does not entirely exclude raised ICP but makes a supra-tentorial mass herniation from LP very unlikely.[3]
[3]Blood tests include the full blood count, coagulation (the anticoagulated patient with an intracranial bleed is reversed early), electrolytes (hyponatraemia from SIADH worsens cerebral oedema), and a bedside glucose. An MRI is reserved for the subacute presentation where a tumour or a subtle lesion is suspected and is not the emergency investigation. An intracranial-pressure monitor (parenchymal catheter or external ventricular drain) is inserted in the intensive-care setting for the severe TBI and guides target-directed therapy.[1]
Immediate management and resuscitation
Resuscitation follows the ABCDE framework, with the brain as the priority organ and the protection of the cerebral perfusion pressure as the explicit goal.[9]
[6]The raised-ICP targets
Raised ICP in the ED — the first 30 minutes
Airway and breathing first — intubate if GCS ≤ 8 or airway unprotected; a neuroprotective RSI (avoid hypotension on induction), then ventilate to SpO2 ≥ 94% and PaCO2 35 to 40 mmHg.
Maintain the cerebral perfusion pressure — keep SBP ≥ 110 mmHg (MAP ≥ 80) with isotonic fluid, blood if bleeding, and noradrenaline; CPP target 60 to 70 mmHg. Never let the pressure drop.
Position for drainage — head up 30° and neutral, loosen a tight cervical collar, free the neck veins; check the endotracheal tube tie is not occluding venous return.
Avoid the secondary insults — normoglycaemia, normothermia (treat fever), treat seizures (levetiracetam), reverse anticoagulation if bleeding. Give ONLY isotonic or hypertonic fluids — never hypotonic (it worsens cerebral oedema).
Image urgently — non-contrast CT head as soon as the patient is stable; identify the mass, the midline shift, the effaced cisterns, the hydrocephalus. Do NOT perform an LP.
Give osmotherapy for the signs of herniation (fixed pupil, falling GCS, Cushing triad) — mannitol 0.5 to 1 g/kg IV OR hypertonic saline 3% 250 mL bolus, while neurosurgery is called.
Transient hyperventilation ONLY if actively herniating — brief reduction of PaCO2 to 30 to 35 mmHg as a bridge while osmotherapy and the surgeon are mobilised, for minutes not hours.
Treat the cause and refer — evacuate the surgical mass, drain the hydrocephalus (EVD), dexamethasone for vasogenic (tumour) oedema, and early neurosurgical / neurocritical-care transfer.
Definitive management — the escalation ladder
Therapy is delivered in tiers, escalating as the pressure and the clinical signs demand, with definitive neurosurgical decompression as the endpoint for any surgically correctable cause.[3]
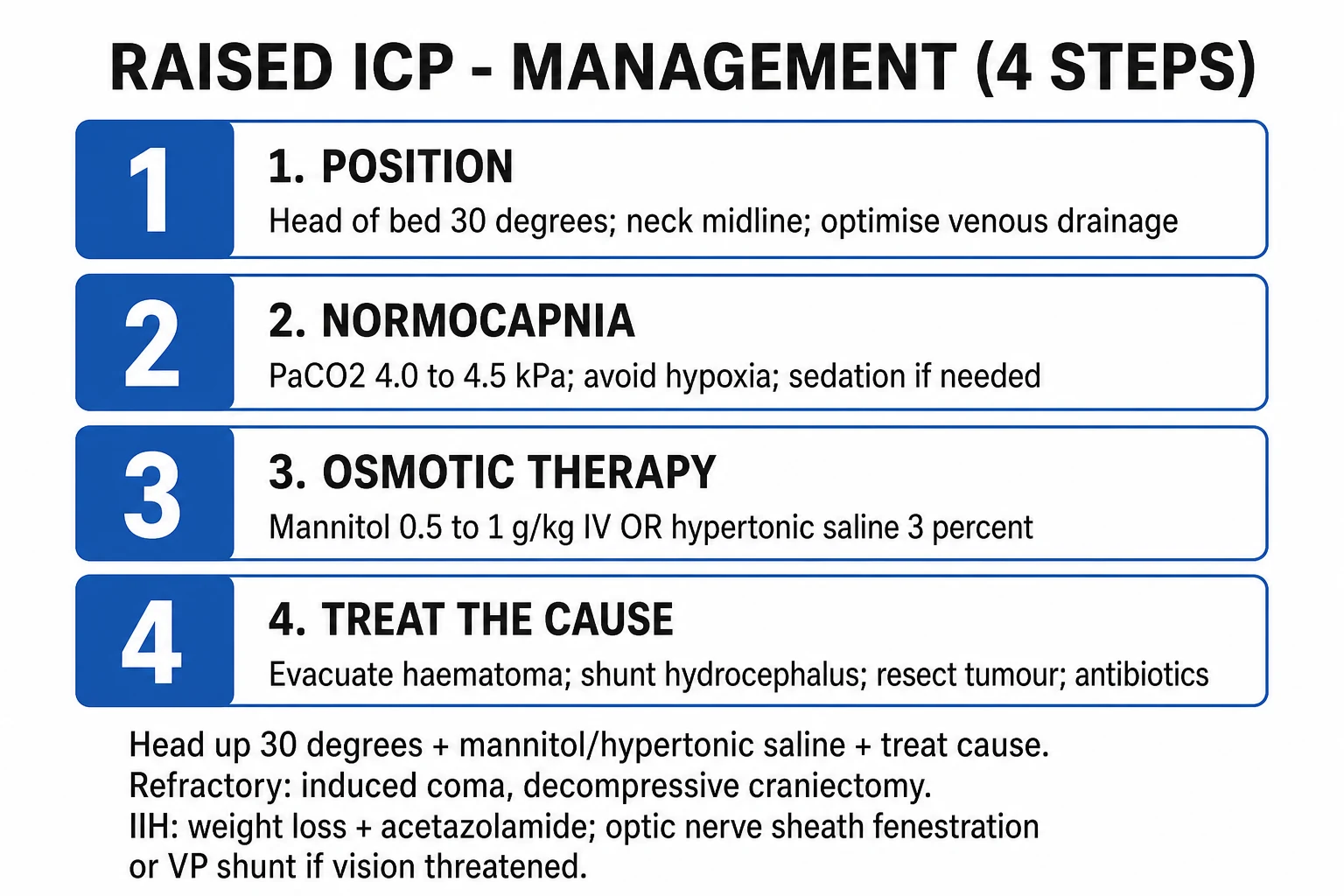
Tier 1 — reduce intrathoracic and venous pressure. Elevate the head to 30 degrees with the head neutral; loosen any cervical collar that obstructs venous return; avoid tight endotracheal-tube ties; ensure adequate sedation and analgesia (propofol or fentanyl) to reduce the metabolic demand and the coughing that raises intrathoracic pressure. Maintain normothermia, normoglycaemia and normocapnia.[3]
Tier 2 — osmotherapy. For the acute signs of herniation (a unilateral fixed pupil, a rapid GCS drop, a Cushing response), give an osmotic agent to draw water out of the brain and into the intravascular space. Mannitol 0.5 g per kg intravenously (typically 1 to 2 mL per kg of 20 per cent solution) is the traditional first agent; monitor the serum osmolarity (hold above 320 mOsm per L) and expect an osmotic diuresis that demands an intravascular-volume replacement and a urinary catheter. Hypertonic saline 3 per cent 250 mL is an effective alternative (or first agent in many trauma centres), drawing water out of the brain and expanding the intravascular volume rather than diuresing it — an advantage in the hypotensive or hypovolaemic patient.[1][3] The two agents are not combined in routine practice.
The two osmotic agents differ in important ways, and the choice is shaped by the haemodynamic state and the unit's practice.[1]
Mannitol 20%
- 0.5 to 1 g/kg IV over 10 to 15 min (1 to 5 mL/kg of 20% solution)
- Established first-line osmotic; rapid ICP reduction within minutes
- Produces an osmotic diuresis → risk of hypovolaemia and hypotension
- Monitor serum osmolarity — hold above 320 mOsm/L; place a urinary catheter; replace intravascular volume
- May induce a rebound rise in ICP if the blood–brain barrier is disrupted
Hypertonic saline 3%
- 250 mL bolus of 3% (or 30 mL of 23.4%) IV over 10 min
- Draws water out of the brain AND expands intravascular volume — preferred if hypotensive or in shock
- No diuresis; restores MAP and therefore CPP simultaneously
- Monitor serum sodium — avoid exceeding 160 mmol/L or a rise >10–15 mmol/L in 24 h
- Increasingly first-line in many trauma centres; less evidence than mannitol but favourable physiology
Combined / sequential
- Not routine — agents are generally used one at a time
- Reserve combined therapy for refractory ICP under neurocritical-care guidance
- Synergy is theoretical; the risk of hypernatraemia and hyperosmolarity rises
- Decide the agent by the haemodynamics, not by habit
Tier 3 — transient hyperventilation (a bridge only). Hyperventilation lowers the PaCO2, which causes cerebral vasoconstriction, reduces cerebral blood volume, and rapidly lowers the ICP. It is reserved as a transient bridge in active, impending herniation — to a PaCO2 of 30 to 35 mmHg — while osmotherapy takes effect and neurosurgery is mobilised, for minutes, not hours. Prophylactic or prolonged hyperventilation is harmful: the vasoconstriction it produces causes cerebral ischaemia and worsens the outcome, as the classic Muizelaar randomised trial showed for prolonged hyperventilation in severe head injury, reaffirmed in contemporary reviews.[6][2][1]
Tier 4 — definitive neurosurgery. Evacuate the surgical mass (craniotomy for an extradural or subdural haematoma, or a haemorrhagic contusion); place an external ventricular drain for hydrocephalus (which both measures and drains CSF); or perform a decompressive craniectomy for refractory intracranial hypertension — the option validated for refractory traumatic ICP in the RESCUEicp trial, which showed lower mortality but higher rates of vegetative and severe-dependency survival versus medical management.[5] Corticosteroids are given ONLY for vasogenic (tumour-related) oedema — dexamethasone 8 to 16 mg loading — and must NOT be given for trauma- or haemorrhage-related oedema, where the CRASH trial demonstrated increased mortality.[4]
Subtypes and scenarios
The acute traumatic scenario is the prototypic emergency — an expanding extradural or subdural haematoma in a deteriorating patient, managed by osmotherapy as a bridge to urgent craniotomy (see the traumatic-brain-injury topic). The tumour-related presentation is subacute — progressive morning headache and vomiting over weeks, papilloedema, a CT showing a ring-enhancing or mass lesion with surrounding oedema — and responds to dexamethasone for the vasogenic oedema plus neurosurgical and oncological referral. The hydrocephalic scenario (acute obstructive hydrocephalus from a posterior-fossa mass or a fourth-ventricular haemorrhage) presents with rapid deterioration and is relieved by an external ventricular drain. Idiopathic intracranial hypertension presents in the young obese woman with headache, visual obscurations and papilloedema, a normal CT/MRI, and a lumbar opening pressure above 25 cm of water; it is managed with acetazolamide and urgent ophthalmology referral to prevent irreversible visual loss. The hepatic-failure patient develops cytotoxic cerebral oedema and a rapidly rising ICP, managed in intensive care with osmotherapy, hypernatraemia and often an ICP monitor.[9]
Complications and pitfalls
The complications are cerebral herniation and death, secondary brain injury from the untreated pressure, and irreversible visual loss in untreated IIH. The recurring pitfalls: performing a lumbar puncture before the CT and precipitating tonsillar herniation; missing the Cushing triad because it is absent (most patients never develop it); giving prophylactic hyperventilation and causing ischaemia; giving corticosteroids in trauma; attributing a reduced GCS to alcohol without imaging; failing to maintain the blood pressure and so dropping the CPP; and delaying the neurosurgical referral for a surgical mass.[4]
Prognosis and disposition
The outcome depends on the cause and the speed of the decompression. An extradural haematoma evacuated before herniation has an excellent prognosis; the same lesion after a prolonged herniation has a poor one. Every patient with acute raised ICP is admitted to a neurosurgical or intensive-care bed, intubated and ventilated if comatose, with an intracranial-pressure monitor and target-directed therapy in the ICU. The patient with IIH is admitted for urgent ophthalmology assessment and acetazolamide. The subacute tumour patient is admitted for dexamethasone and neurosurgical planning.[3]
Special populations
The paediatric patient may show earlier vomiting and behavioural change before headache is articulated, and an open fontanelle in the infant allows some pressure dissipation; non-accidental injury is considered in the inconsistent-history case. The elderly patient has a cerebral-atrophy-expanded cranial space that allows a larger mass (a chronic subdural) to accumulate before symptoms, and a lower physiological reserve. The anticoagulated patient (warfarin or a DOAC) has a higher risk of an expanding intracranial haematoma and is reversed early. In pregnancy, raised ICP from pre-eclampsia or eclampsia follows the magnesium-and-delivery pathway rather than the osmotherapy pathway.[3]
[3] [1] [3] [9] [1] [6]Cerebral autoregulation — why blood pressure control is brain control
The brain defends a constant cerebral blood flow across a wide range of perfusion pressures through cerebral autoregulation — the Lassen curve. Between a MAP of roughly 50 and 150 mmHg in the healthy brain, the cerebral arterioles constrict (at high pressure) or dilate (at low pressure) to hold flow constant. Two consequences follow that drive the entire resuscitation. First, the injured brain loses autoregulation, so cerebral blood flow becomes passively pressure-passive — a falling MAP directly reduces flow and a rising MAP directly increases flow (and oedema). Second, the lower autoregulatory breakpoint is shifted rightward in chronic hypertension, so the hypertensive patient's brain ischaemes at a MAP that would be tolerable in a normotensive person. This is why the SBP floor of 110 mmHg (and the imperative to never let the pressure drop on induction or for a scan) is not arbitrary — it sits above the injured-brain ischaemic threshold.[9]
[9] [9] [9]Cerebral oedema — cytotoxic versus vasogenic
Not all cerebral oedema is the same, and the distinction decides whether steroids will help. Vasogenic oedema results from blood–brain barrier disruption — the vessels leak, plasma water enters the extracellular space, and the oedema is extracellular, predominantly white-matter, and steroid-responsive. It surrounds tumours, abscesses and late infarcts, and shrinks with dexamethasone. Cytotoxic oedema results from cellular energy failure (ischaemia, hypoxia, ammonia in liver failure, trauma) — the Na/K ATPase fails, sodium and water enter the cells, and the oedema is intracellular, grey-and-white-matter, and steroid-resistant. The CRASH trial's harm is now mechanistically understood: steroids cannot reverse ATP-depleted cellular swelling, and they worsen the systemic milieu.[8]
Vasogenic oedema
- Blood–brain barrier disrupted; plasma leaks into extracellular space
- Predominantly white-matter; finger-like extensions on CT/MRI
- Surrounds tumours, abscesses, metastases, late infarct oedema
- STEROID-RESPONSIVE — dexamethasone 8 to 16 mg loading
- Responds to osmotherapy acutely; steroids for the underlying barrier leak
Cytotoxic oedema
- Cellular energy failure; Na/K ATPase fails; water enters cells
- Intracellular; grey AND white matter
- Ischaemic stroke, hypoxia, severe TBI, fulminant hepatic failure, DKA
- STEROID-RESISTANT — do NOT give steroids (CRASH harm in TBI)
- Osmotherapy, hypernatraemia, treat the underlying energy failure
Hydrocephalic (interstitial)
- CSF forced into periventricular white matter under pressure
- Periventricular lucency on CT, transependymal oedema
- Obstructive or communicating hydrocephalus
- Treats with CSF DIVERSION (EVD or shunt), not with drugs
- Osmotherapy and steroids are ineffective — drain the ventricle
Osmotic (rare)
- Rapid fall in serum osmolarity shifts water into the brain
- Iatrogenic — over-rapid correction of hypernatraemia, dialysis disequilibrium
- Prevent by avoiding hypotonic fluids and controlling sodium correction rate
- Treats by restoring the osmotic gradient (hypertonic saline)
The ICP monitor — devices, indications, and the pressure waveform
Invasive ICP monitoring is the bridge between the ED resuscitation and neurocritical-care target-directed therapy. The Brain Trauma Foundation recommends an ICP monitor in severe TBI with an abnormal CT (haematomas, contusions, compression, swelling) and in patients with a normal CT if two or more of: age over 40, unilateral or bilateral motor posturing, or SBP below 90 mmHg. The treatment threshold is a sustained pressure above 22 mmHg.[1]
Parenchymal (Codman / Camino)
- Transducer placed into brain parenchyma via a bolt
- Lowest infection risk (~1%); easy to place; most commonly used
- Measures focal pressure — may miss gradients in different compartments
- Cannot drain CSF — monitor only; small zero-drift over days
External ventricular drain (EVD)
- Catheter into the lateral ventricle — the GOLD STANDARD for accuracy
- Measures AND drains CSF — allows therapeutic CSF removal for high ICP
- Higher infection risk (~5 to 10%); haemorrhage on insertion (~1 to 2%)
- Requires ventricles large enough to cannulate — collapsed ventricles make it hard
Subdural / epidural
- Catheter or transducer on the brain surface
- Less accurate than parenchymal or intraventricular
- Used when ventricles are slit-like or after decompressive craniectomy
- Higher complication profile; less favoured in modern practice
Non-invasive (ultrasound, TCD)
- Optic nerve sheath diameter on POCUS (>5.0 to 5.5 mm suggests raised ICP)
- Transcranial Doppler pulsatility index correlates with ICP
- Screening only — no monitoring; cannot replace invasive measurement
- Useful to escalate urgency when invasive monitoring is delayed or contraindicated
The pupil exam — anatomy, anisocoria, and false alarms
The pupillary light reflex is the single most reliable lateralising sign in raised ICP, and the Fellowship candidate is expected to know its anatomy cold. The afferent limb is the optic nerve (CN II) carrying light input to the pretectal nuclei of the midbrain; both Edinger-Westphal nuclei are then stimulated (consensual response); the efferent limb is the oculomotor nerve (CN III), whose parasympathetic fibres run on the superficial, peripheral surface of the nerve — which is why they are compressed first, before the somatic fibres to the extraocular muscles. As the uncus herniates through the tentorial notch, it stretches and then compresses the ipsilateral CN III against the petroclinoid ligament: first the parasympathetic fibres fail (sluggish then fixed dilation), then the motor fibres fail (ptosis, "down-and-out" eye from unopposed CN IV and VI).[3]
[1] [3] [4]Secondary brain injury — the treatable insults that follow the primary injury
The primary brain injury (the mechanical damage at impact, or the initial bleed) is irreversible from the moment it occurs; almost everything the emergency physician does targets the secondary brain injury — the cascade of insults that worsen the injured brain over the hours that follow. Each is preventable, each is treatable, and each doubles or trebles the harm when missed. The mnemonic is HOTTN — Hypoxia, Hypotension (the two that kill fastest), Temperature (fever and hyperglycaemia), Trauma (seizures), and otheR (sodium derangement, agitation, pain).[1]
Hypoxia
- SpO2 below 90% doubles mortality in severe TBI
- Maintain SpO2 at or above 94%; intubate early if the airway or oxygenation cannot be maintained
- Even a brief desaturation on induction or for transfer is harmful
- Pre-oxygenate fully; use apnoeic oxygenation during RSI
Hypotension
- A SINGLE SBP below 90 mmHg doubles severe-TBI mortality
- Keep SBP at or above 110 mmHg (CPP 60 to 70) with isotonic fluid, blood, noradrenaline
- The most dangerous moment is induction — have vasopressor drawn up
- Avoid the hypotensive RSI: pre-load, choose a cardiovascularly stable induction agent, push noradrenaline on induction
Hyperthermia
- Every 1°C of fever raises cerebral metabolic rate ~10% and cerebral blood volume and ICP with it
- Treat fever aggressively — paracetamol, cooling blankets, treat the source
- Therapeutic hypothermia is NOT recommended in TBI (does not improve outcome and may harm)
- Normothermia is the target, not hypothermia
Hyperglycaemia
- Glucose above 10 worsens outcome (anaerobic metabolism, acidosis, oedema)
- Treat with an insulin infusion; target 6 to 10 mmol/L, avoiding hypoglycaemia
- Check a bedside glucose on EVERY reduced-conscious-level patient — hypoglycaemia is a rapid mimic
- Do not give dextrose-containing fluids unless treating hypoglycaemia
Seizures
- A single seizure doubles cerebral metabolic demand and spikes the ICP
- Prophylactic levetiracetam for severe TBI within 7 days (does NOT improve outcome but prevents early PTS)
- Treat actively seizing patients with benzodiazepines then levetiracetam or phenytoin
- Subclinical seizures in a comatose patient may need continuous EEG
Sodium / osmolar
- Hyponatraemia (SIADH, cerebral salt wasting) worsens cerebral oedema
- Hypotonic fluids are forbidden; use 0.9% saline or hypertonic saline
- Hypernatraemia is therapeutic (Na 145 to 155) in hepatic failure and refractory ICP
- Rapid sodium correction risks central pontine myelinolysis — correct no faster than 8 to 10 mmol/L per 24 h
The surgical masses — extradural, subdural, and intracerebral
The three traumatic surgical masses share the presentation of a deteriorating patient after a head injury but differ in mechanism, imaging, urgency, and prognosis. Naming the lesion on the CT determines whether the patient goes to theatre within the hour.[6]
Extradural (epidural) haematoma
- Arterial — middle meningeal artery torn by a temporal/parietal skull fracture
- Lentiform (biconvex) lens-shaped blood on CT; does NOT cross sutures
- The LUCID INTERVAL — unconscious → alert → unconscious again (classic, seen in a minority)
- Maximal surgical urgency; excellent prognosis if evacuated before herniation
- TA fracture line crossing the middle meningeal groove is the clue
Acute subdural haematoma
- Venous — bridging veins torn by acceleration-deceleration (fall, assault)
- Crescent-shaped blood on CT; CROSSES sutures, tracks along the surface
- Underlying brain injury (contusions, oedema) is common and drives prognosis
- Surgical evacuation if > 10 mm thick or > 5 mm midline shift; worse prognosis than EDH
- Common in the elderly, anticoagulated, and alcoholic
Intracerebral (contusion / ICH)
- Parenchymal — coup and contrecoup contusions (frontal and temporal poles)
- May "blossom" (expand) over 24 to 72 h — repeat the CT if the patient deteriorates
- Surgery if the lesion is large, accessible, and causing mass effect or herniation
- Managed medically (osmotherapy, CPP) if small or deep; prognosis relates to the volume
- Burst lobe = contused brain with overlying subdural — grave prognosis
Traumatic subarachnoid
- Blood in the sulci and cisterns from surface vessel injury
- Not a surgical mass lesion; managed medically
- May contribute to vasospasm and hydrocephalus
- Differentiate from a ruptured aneurysmal SAH (sudden-onset thunderclap, sentinel bleed)
The neuroprotective RSI — drug by drug
Rapid sequence intubation in raised ICP is not simply "secure the airway" — every drug and every manoeuvre is chosen to protect the brain. Laryngoscopy and suctioning surge the ICP by 10 to 30 mmHg; the agent chosen must blunt this, and the dose must not drop the blood pressure.[3]
Pre-treatment / induction
- Propofol (1 to 2.5 mg/kg) — blunts the ICP surge, lowers the CMR; causes hypotension
- Thiopentone (3 to 5 mg/kg) — the classical neuro-induction agent; causes hypotension
- Ketamine (1 to 2 mg/kg) — once feared to raise ICP, now known to be SAFE and cardiovascularly stable; preferred if hypotensive
- Etomidate (0.3 mg/kg) — haemodynamically neutral; adrenal suppression (controversial)
Paralytic
- Rocuronium (1.2 mg/kg) — fast onset, the agent of choice when sux contraindicated; reversible with sugammadex
- Suxamethonium (1.5 mg/kg) — fastest onset; transient ICP rise from fasciculations; risks hyperkalaemia in burns/crush/paralysis
- Both cause a small transient ICP rise; the risk of hypoxia from a delayed intubation is greater
- Defasciculating dose of rocuronium is no longer routinely recommended
Avoid
- Avoid propofol as sole induction in the hypotensive/shocked patient — cardiovascular collapse
- Avoid high-dose fentanyl-only techniques if the patient is hypotensive
- Avoid ketamine historically — modern evidence shows it is safe and often superior
- Avoid any technique that allows the SBP to drop below 110 — the CPP must not fall
Acute uncal herniation in the ED — the 5-minute response
RECOGNISE — unilateral fixed dilated pupil, GCS drop of 2 or more, decerebrate posturing, or a Cushing response. The moment one of these appears, the clock is running.
CALL — alert the senior emergency physician, intensivist, neurosurgeon, anaesthetist, and the trauma team. Two pairs of hands, a clear leader, and a scribe.
OSMOTHERAPY NOW — mannitol 0.5 to 1 g/kg IV OR hypertonic saline 3% 250 mL bolus (prefer the saline if hypotensive or in shock). Do not wait for the CT.
POSITION — head up 30 degrees and neutral, loosen the collar, free the neck veins, check the endotracheal tube tie is not occluding venous return.
TRANSIENT HYPERVENTILATION to PaCO2 30 to 35 mmHg as a BRIDGE only, for minutes, while osmotherapy takes effect and the surgeon is mobilised. Re-check the PaCO2 — do not overshoot.
IMAGE — urgent non-contrast CT head once the patient is stabilised; never delay the CT for a test that does not change the immediate management.
SURGERY — evacuate the surgical mass, place an EVD for hydrocephalus, or decompressive craniectomy for refractory ICP, in parallel with neurocritical-care admission.
The reverse and the rare — atypical herniation patterns
[3] [7] [8] [1]Additional landmark trials — DECRA, HAMLET, BEST-TRIP
Beyond the CRASH, RESCUEicp, and Muizelaar trials already discussed, three further trials shape the modern understanding of decompressive surgery and ICP monitoring in raised pressure.[3]
DECRA — Early decompressive craniectomy for diffuse traumatic brain injury (Cooper 2011, NEJM)
HAMLET — Hemicraniectomy for malignant MCA infarction (Hofmeijer 2009, Lancet Neurol)
BEST-TRIP — ICP monitoring vs imaging-clinical exam in severe TBI (Chesnut 2012, NEJM)
Lumbar puncture revisited — when it IS and is NOT done
[3] [9]Prognostication and the boundaries of care
[7] [3] [3] [4] [1] [1]Evidence and regional guidelines
The contemporary framework is the Brain Trauma Foundation 2020 update of the severe-TBI guidelines, which sets the ICP treatment threshold (above 22 mmHg), the CPP target (60 to 70 mmHg), the SBP threshold (110 or above), the normocapnia target, and the osmotherapy recommendations.[1] The evidence on hyperventilation — transient and harmful when prolonged — is summarised in dedicated neurocritical-care reviews.[2] The emergency-department management of raised ICP across traumatic and non-traumatic causes is reviewed in the standard texts.[3] The agent choices and the CT-first, no-LP rule are global; the neurosurgical pathway and the CT indications follow the local trauma and neurosurgical protocol.
The three landmark trials that shape modern raised-ICP and TBI practice are summarised below.[3]
CRASH — Corticosteroid randomisation after significant head injury (Roberts 2004, Lancet)
RESCUEicp — Decompressive craniectomy for traumatic intracranial hypertension (Hutchinson 2016, NEJM)
Muizelaar 1991 — Adverse effects of prolonged hyperventilation (J Neurosurg)
ANZ practice note. The raised-ICP management ladder follows the Brain Trauma Foundation 2020 update via the local trauma and neurosurgical pathway. The non-negotiable targets are the SBP at or above 110 mmHg, the PaCO2 at 35 to 40 mmHg, the head elevated to 30 degrees, and the mannitol 0.5 g per kg or the hypertonic saline 3 per cent 250 mL for the signs of herniation. The no-LP-before-CT rule and the no-steroids-in-trauma rule are absolute.[3]
Exam pearls
- CPP = MAP − ICP (target 60 to 70) — a rising ICP or a falling MAP both lower the CPP.
- Cushing triad (hypertension, bradycardia, irregular respiration) is LATE and pre-terminal — its absence does not exclude raised ICP.
- A unilateral fixed dilated pupil = uncal herniation — mannitol 0.5 g per kg or hypertonic saline 3 per cent 250 mL + neurosurgery now.
- No LP before a CT when raised ICP is suspected — a supra-tentorial pressure gradient plus an LP equals tonsillar herniation.
- No prophylactic hyperventilation — PaCO2 35 to 40 mmHg; reserve transient hyperventilation to a PaCO2 of about 35 as a bridge in active herniation.
- No steroids in trauma or haemorrhage (CRASH); steroids are for vasogenic (tumour) oedema only.
- Mannitol OR hypertonic saline, not both routinely; check the serum osmolarity.
- Monro-Kellie: three incompressible compartments in a rigid box — when one expands (blood, brain/CSF, mass), the others must give way, then ICP rises steeply once reserve is spent.
- The compliance curve is flat then steep — a "stable" compensated patient can herniate after a single cough, hypoxic episode, or hypotensive event.
- The ICP treatment threshold is 22 mmHg (Brain Trauma Foundation 2020); the CPP target is 60 to 70 mmHg; the SBP floor is 110 mmHg.
- Defend the CPP, not just the ICP — hypotension (SBP < 90) doubles TBI mortality; keep the MAP up with fluid and noradrenaline.
- Head up 30° and neutral lowers ICP by aiding venous drainage — but check the collar and tube tie are not kinking neck veins.
- Give ONLY isotonic or hypertonic fluids — hypotonic fluids (5% dextrose, 0.45% saline) worsen cerebral oedema; dextrose-containing fluids add hyperglycaemia.
- Decorticate = arms flexed (above red nucleus); decerebrate = all four extended (at/below red nucleus) — progression down the brainstem is grave.
- A sixth-nerve palsy is a FALSE localising sign — stretched abducens, not a brainstem lesion.
- Hypertonic saline is preferred over mannitol if the patient is hypotensive or in shock — it expands volume rather than diuresing.
- Decompressive craniectomy (RESCUEicp) lowers mortality but shifts survivors toward dependency — a multidisciplinary, values-based decision.
- Treat the secondary insults in parallel — normoglycaemia, normothermia, seize control, reverse anticoagulation; the brain is killed twice over if you fix only the pressure.
- CT signs of raised ICP: midline shift > 5 mm, effaced basal cisterns, sulcal compression — a normal CT lowers (but does not abolish) the risk of LP-induced herniation.
- Cerebral autoregulation (Lassen) — flow constant between MAP 50 and 150 in the healthy brain; LOST after injury, so flow becomes pressure-passive. Hypotension causes ischaemia, hypertension causes oedema/haematoma expansion.
- Vasogenic vs cytotoxic oedema — vasogenic (tumour, abscess) is extracellular, white-matter, STEROID-responsive (dexamethasone); cytotoxic (ischaemia, TBI, hepatic failure) is intracellular, STEROID-resistant.
- The ICP waveform — P1 (percussion), P2 (tide/compliance), P3 (dicrotic). A rising P2 that equals or exceeds P1 means compliance is exhausted and herniation is imminent even before the absolute ICP crosses 22.
- POCUS optic nerve sheath diameter > 5.0 to 5.5 mm is a bedside screen for ICP > 20 (sensitivity > 90%) — a triage tool, NOT a replacement for invasive monitoring.
- Anisocoria > 1 mm with a falling GCS is uncal herniation; anisocoria in an alert oriented patient is usually benign (physiological, pharmacological, post-surgical).
- Ketamine is SAFE in raised ICP — the old "never give ketamine, it raises ICP" rule is overturned; it is often PREFERRED in the hypotensive brain-injured patient because it preserves the MAP.
- A lucid interval (unconscious → alert → unconscious) after head injury is an expanding extradural haematoma until a CT proves otherwise — do not discharge the "well-looking" head-injured patient.
- Cerebral contusions blossom — repeat the CT in 24 hours for any contusion, and immediately for ANY neurological deterioration (GCS drop ≥ 2, new pupil sign, new weakness).
- DECRA (early diffuse TBI) — early craniectomy WORSENED functional outcome; RESCUEicp (late refractory ICP) — craniectomy lowered mortality at the cost of more dependent survivors. Timing and selection separate the two.
- HAMLET — decompressive hemicraniectomy for malignant MCA infarction is life-saving but outcomes-altering; best under 60 and within 48 hours, with family counselling.
- BEST-TRIP — ICP monitoring did not improve outcome over protocolised imaging-clinical care; the lesson is that PROTOCOLISED care matters, not the monitor alone. ICP monitoring is still standard for the unexaminable patient.
- Upward (cerebellar) herniation — a posterior-fossa mass with pinpoint pupils and upgaze palsy; rapid EVD drainage without decompression can worsen it.
- Neurogenic pulmonary oedema and stunned myocardium can complicate herniation with hypoxia and hypotension — use noradrenaline and PEEP, avoid fluid overload.
- A single SBP < 90 mmHg doubles severe-TBI mortality; the most dangerous moment is induction — have noradrenaline drawn up and never let the pressure drop for a scan.
- The ICP treatment threshold is 22 mmHg and CPP target 60 to 70; an ICP monitor is placed in severe TBI with an abnormal CT, or a normal CT if ≥ 2 of: age > 40, motor posturing, SBP < 90.[8]
Exam practice
SAQ — Acute uncal herniation from an expanding extradural haematoma
10 minutes · 10 marks
A 19-year-old man is brought in after an assault. He was briefly unconscious, then lucid for two hours, and is now drowsy. The GCS has dropped from 14 to 9; the right pupil is fixed and dilated at 6 mm; he has a left hemiparesis. BP 174/92, HR 52, RR 8 and irregular.
SAQ — Tumour-related vasogenic oedema with raised intracranial pressure
10 minutes · 10 marks
A 62-year-old woman presents with three weeks of progressive morning headache, vomiting and blurred vision. She has the papilloedema and a right homonymous hemianopia. The CT shows a left occipital mass with the surrounding oedema and 6 mm of midline shift. GCS 14, the observations are normal.
Red flags
[3]References
- [1]Carney N, Totten AM, O'Reilly C, et al. Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition. Neurosurgery, 2017.PMID 27654000
- [2]Godoy DA, Seifi A, Garza D, Lubillo-Montenegro S, Murillo-Cabezas F. Hyperventilation Therapy for Control of Posttraumatic Intracranial Hypertension. Frontiers in Neurology, 2017.PMID 28769857
- [3]Ramesh Kumar R. Raised intracranial pressure (ICP): management in emergency department. Indian Journal of Pediatrics, 2012.PMID 22218806
- [4]Roberts I, Yates D, Sandercock P, et al. Effect of intravenous corticosteroids on death within 14 days in 10008 adults with clinically significant head injury (MRC CRASH trial): randomised placebo-controlled trial. Lancet, 2004.PMID 15474134
- [5]Hutchinson PJ, Kolias AG, Timofeev IS, et al. Trial of Decompressive Craniectomy for Traumatic Intracranial Hypertension. New England Journal of Medicine, 2016.PMID 27602507
- [6]Muizelaar JP, Marmarou A, Ward JD, et al. Adverse effects of prolonged hyperventilation in patients with severe traumatic head injury: a randomized clinical trial. Journal of Neurosurgery, 1991.PMID 1919695
- [7]Cooper DJ, Rosenfeld JV, Murray L, et al. Decompressive craniectomy in diffuse traumatic brain injury. New England Journal of Medicine, 2011.PMID 21434843
- [8]Hofmeijer J, Kappelle LJ, Algra A, Amelink GJ, van Gijn J, van der Worp HB. Surgical decompression for space-occupying cerebral infarction (the Hemicraniectomy After Middle Cerebral Artery infarction with Life-threatening Edema Trial [HAMLET]): a multicentre, open, randomised trial. Lancet Neurology, 2009.PMID 19269254
- [9]Chesnut RM, Temkin N, Carney N, et al. A trial of intracranial-pressure monitoring in traumatic brain injury. New England Journal of Medicine, 2012.PMID 23234472