EM · Meningitis and encephalitis
Meningitis and encephalitis (emergency department diagnosis and management)
Also known as Acute meningitis · Bacterial meningitis · Viral meningitis · Herpes simplex encephalitis · Meningococcaemia
Acute meningitis and encephalitis — the clinical triad (fever, headache, neck stiffness), the petechial rash of meningococcaemia, the empiric regimen (ceftriaxone 2 g IV plus vancomycin plus dexamethasone 10 mg IV, with ampicillin added for listeria in the immunocompromised and over-50), aciclovir 10 mg/kg IV three times daily for HSV encephalitis, the LP timing (antibiotics never delayed for imaging), CSF interpretation (bacterial versus viral versus tuberculous), and the complications (cerebral oedema, seizures, DIC, Waterhouse-Friderichsen). ACEM-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Acute central nervous system infection sits on the time-critical edge of emergency medicine: a few hours of delay converts a treatable meningitis into a death or a devastating neurological injury. The Fellowship candidate must recognise the clinical triad, give the empiric regimen without waiting for imaging, interpret the cerebrospinal fluid by its cell count and glucose, and add aciclovir the moment herpes simplex encephalitis enters the differential. Two diseases dominate the workload — bacterial meningitis (pneumococcal, meningococcal, listerial) and herpes simplex encephalitis — and both are managed on probability, not on proof.[1][2]
Definition and classification
Meningitis is inflammation of the meninges lining the brain and spinal cord; encephalitis is inflammation of the brain parenchyma itself, and the two overlap clinically as meningoencephalitis. The decisive split is bacterial versus viral, because bacterial meningitis is destroyed by an hour of the right antibiotic and viral meningitis is largely supportive. Encephalitis is most often viral, and herpes simplex virus type 1 is the treatable, exam-critical cause. Fungal meningitis (cryptococcus) and tuberculous meningitis run a subacute course and are suspected in the immunocompromised and the endemic-risk patient. Aseptic meningitis denotes a lymphocytic CSF with a negative bacterial culture — usually viral, but also partially-treated bacterial, TB, fungal, drug-induced, or autoimmune.[4]
Pathophysiology
Bacterial meningitis begins when a colonising nasopharyngeal organism (pneumococcus, meningococcus) invades the bloodstream and seeds the choroid plexus and the meninges, or reaches the meninges by direct extension from a contiguous focus (otitis media, sinusitis, mastoiditis, a skull-base fracture). Once in the subarachnoid space the bacteria multiply in a compartment that lacks complement and antibody, generating an intense neutrophilic exudate. The inflammatory cascade increases blood–brain barrier permeability, raises CSF protein, consumes glucose, and produces cerebral oedema; the raised intracranial pressure is the mechanism of both the headache and the lethal complication of herniation. Herpes simplex encephalitis is different: the virus reaches the temporal lobe by the olfactory or trigeminal pathway and causes haemorrhagic, necrotising inflammation — typically bilateral but asymmetric in the inferomedial temporal and frontal lobes.[4]
Epidemiology and risk factors
The commonest community-acquired organism in adults is Streptococcus pneumoniae, followed by Neisseria meningitidis, with Haemophilus influenzae now rare since conjugate vaccination. Listeria monocytogenes is the critical exception: it is not covered by ceftriaxone and it targets the over-50 age group, the immunocompromised, the pregnant, and the alcoholic — these patients must have ampicillin added. Risk factors that broaden the differential include asplenia and sickle-cell disease (encapsulated organisms), HIV and immunosuppression (cryptococcus, listeria, TB), a CSF shunt or recent neurosurgery (staphylococci and Gram-negatives), and uncontrolled alcohol excess (listeria and pneumococcus). Herpes simplex encephalitis is the commonest sporadic viral encephalitis at any age, with a mortality that exceeds 70 per cent untreated.[1][4][9]
Clinical presentation
The classic triad is fever, headache and neck stiffness, but all three are present together in only about 44 per cent of cases; at least two appear in roughly 95 per cent, and almost every patient has a fever with a headache. The decisive additional feature is an altered mental status — confusion, drowsiness or coma — which distinguishes encephalitis or severe bacterial meningitis from simple viral meningitis and which independently predicts a poor outcome. Meningism is elicited by neck stiffness, a positive Kernig sign (resistance to knee extension with the hip flexed), and a positive Brudzinski sign (involuntary hip flexion on neck flexion), though both are insensitive. A petechial or purpuric rash with a fever is meningococcaemia until proven otherwise and demands immediate empiric therapy. Herpes simplex encephalitis presents with fever, an altered consciousness, behavioural change, dysphasia, focal temporal-lobe seizures, or olfactory and gustatory hallucinations — a clinical pattern, not a single sign.[4]
Bacterial meningitis
- Fever, headache, neck stiffness; rapid onset over hours
- GCS depressed; petechial rash if meningococcal
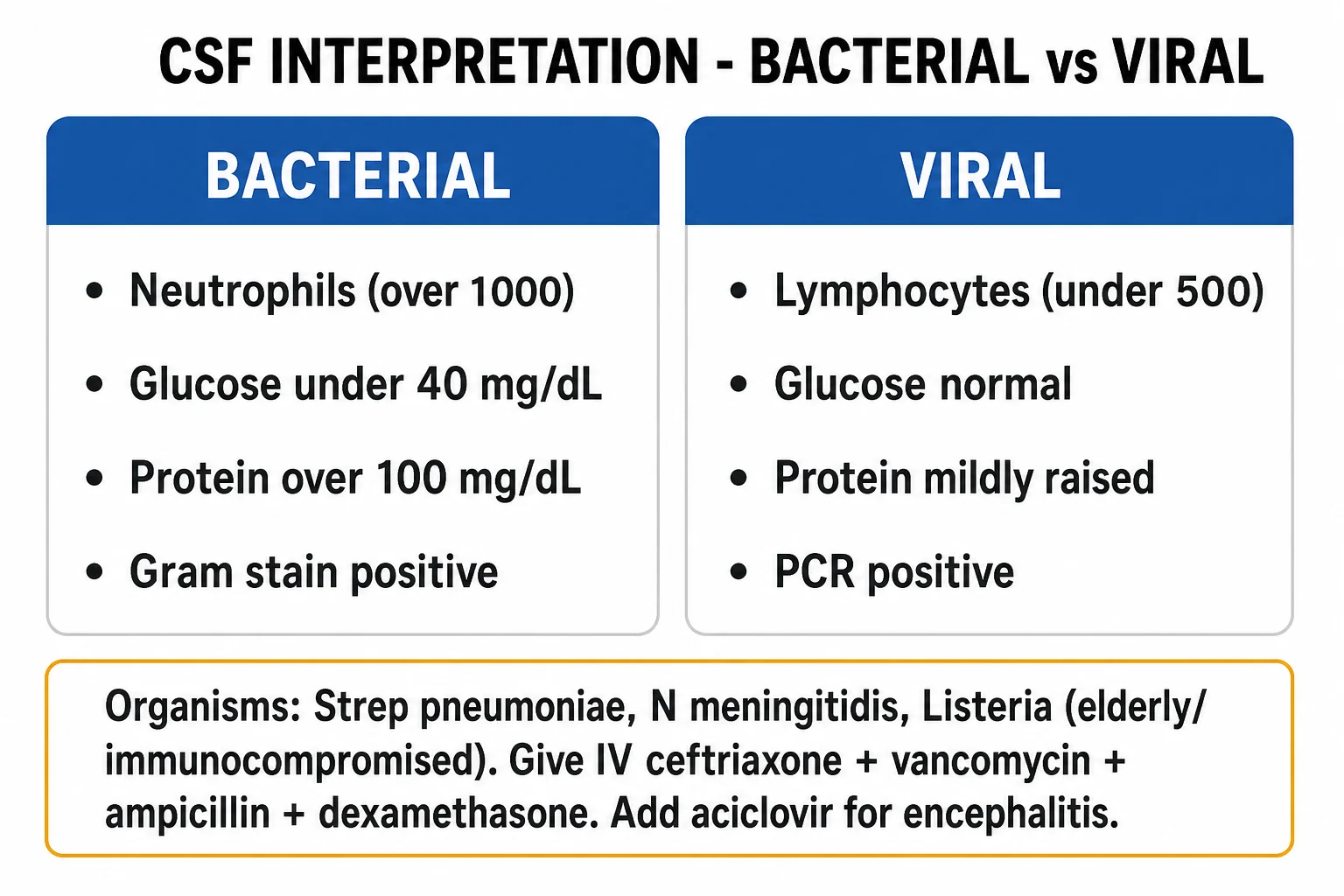
- CSF: neutrophils, high protein, low glucose
- Empiric antibiotics + dexamethasone, now
Viral meningitis
- Fever, headache, neck stiffness; patient looks well
- GCS normal; no focal deficit
- CSF: lymphocytes, normal glucose
- Supportive; self-limiting in days
HSV encephalitis
- Fever + altered consciousness, seizures, behavioural change
- Temporal-lobe features: dysphasia, hallucinations
- CSF: lymphocytes, mild protein rise; PCR positive
- Aciclovir 10 mg/kg IV TDS — do not wait for PCR
Tuberculous meningitis
- Subacute; days to weeks of headache, malaise, fever
- Cranial nerve palsies; basal exudate on imaging
- CSF: lymphocytes, very high protein, very low glucose
- Quadruple therapy; steroids; high mortality
Differential diagnosis
The febrile patient with a headache and an altered or normal consciousness generates a differential that the history, the imaging and the CSF resolve — but several mimics are time-critical in their own right.[8]
Subarachnoid haemorrhage
- Thunderclap headache at onset; reaching maximum within seconds
- Meningism develops over hours; low-grade fever possible
- CT head shows subarachnoid blood; xanthochromia in CSF
- Not an infection — needs neurosurgery, not antibiotics
Migraine
- Pulsating unilateral headache with aura, photophobia, phonophobia
- No fever; GCS normal; no neck stiffness
- Normal CT and CSF
- Analgesia, antiemetic, triptan; no antibiotics
Cerebral abscess
- Headache, fever, focal deficit or seizures; often an ENT or cardiac source
- Ring-enhancing lesion on contrast CT or MRI
- LP is contraindicated — risk of herniation
- Neurosurgical drainage; targeted antibiotics
Autoimmune encephalitis
- Subacute psychiatric change, seizures, movement disorder
- NMDA-receptor antibody; young women, ovarian teratoma
- CSF often near-normal; MRI may be normal
- Immunotherapy — steroids, IVIG, plasma exchange
Metabolic or toxic encephalopathy
- Confusion without fever or meningism
- Hypoglycaemia, hyponatraemia, sepsis, drug toxicity
- Normal CT; CSF normal
- Treat the underlying metabolic or toxic cause
Bedside assessment
Assess and secure the airway, breathing and circulation first — a depressed Glasgow Coma Scale, particularly below 9, threatens the airway and mandates intubation. Record the GCS in its eye, verbal and motor components, examine for a petechial or purpuric rash, look for a focal neurological deficit, and search for a contiguous source (otitis media, sinusitis, mastoiditis, a CSF leak or a cochlear implant). Fundoscopy for papilloedema is recommended but is unreliable and must not delay therapy. The early task is to decide whether this is septic shock (manage with the Hour-1 sepsis bundle) or a stable patient suitable for an urgent lumbar puncture after blood cultures.[4]
Investigations
The cerebrospinal fluid is the diagnostic centrepiece, but it is never allowed to delay the antibiotic. Blood cultures are drawn first (positive in around half of bacterial meningitis), then a coagulation screen and full blood count (the platelet count and INR screen for the disseminated intravascular coagulation of meningococcaemia). A serum glucose is taken with the LP so the CSF-to-serum ratio can be calculated. The CT before the LP is reserved for the high-risk patient (see below); a normal CT does not guarantee a safe LP. For suspected HSV, the CSF HSV polymerase chain reaction is highly sensitive but can be negative in the first 48 hours, so a negative PCR with a compatible picture warrants a repeat at three to seven days and empirical aciclovir in the meantime. A CT or MRI head with contrast and an electroencephalogram support the diagnosis of HSV encephalitis when the temporal-lobe picture is clear.[8]
[8]CSF interpretation — bacterial versus viral versus tuberculous
The CSF cell count, differential, protein and glucose resolve the aetiology. A traumatic tap is corrected by subtracting one white cell for every 700 red cells, and the CSF glucose is always interpreted against a simultaneous serum glucose.[1]
Typical CSF profiles in acute meningitis
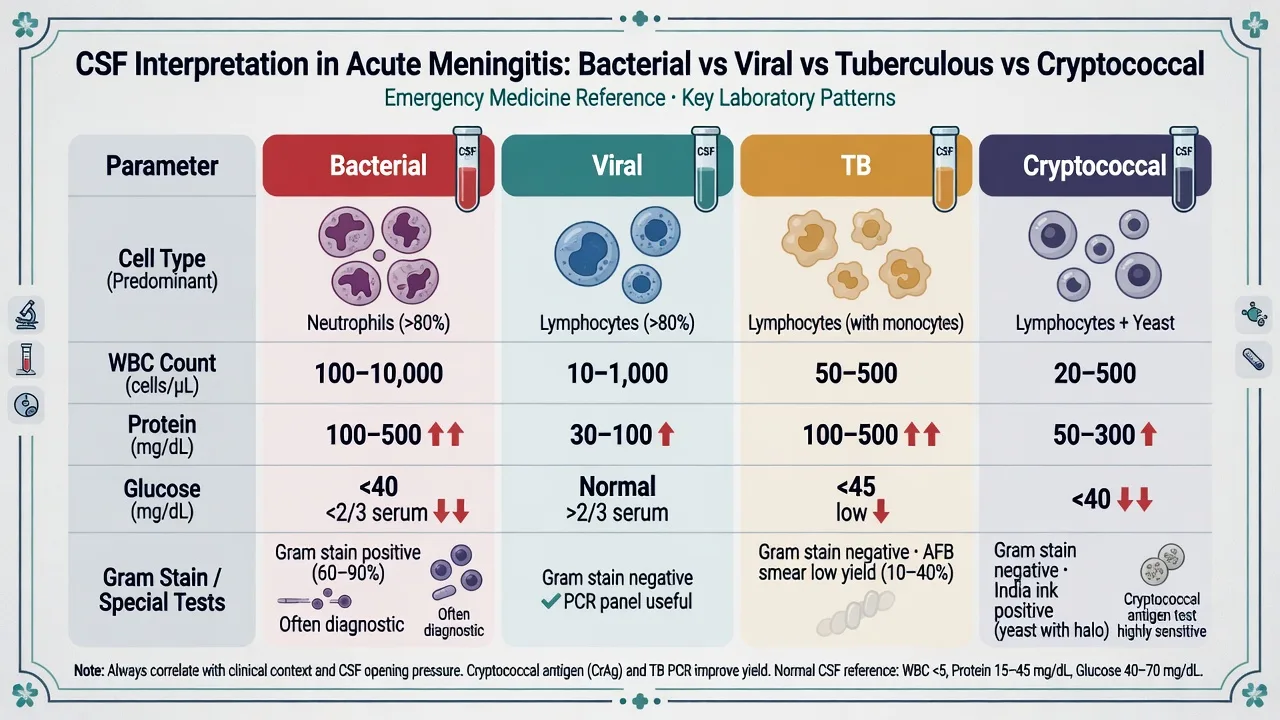
A neutrophil-predominant pleocytosis with a low glucose and a high protein is bacterial until proven otherwise; a lymphocytic picture with a normal glucose is viral, TB (low glucose) or fungal; a frankly normal CSF with a strong clinical story does not exclude early bacterial meningitis or HSV encephalitis and the empiric therapy continues.[1]
Immediate management and resuscitation
Stabilise the airway, give oxygen, establish intravenous access and treat shock with fluid boluses and vasopressors by the sepsis pathway. Draw blood cultures, then give the first dose of the empiric regimen immediately — within the first hour — and before the lumbar puncture whenever the LP will be delayed. Dexamethasone 10 mg intravenously is given just before or with the first antibiotic dose when pneumococcal meningitis is suspected, because the steroid blunts the inflammatory surge released by antibiotic-mediated bacterial lysis. If the LP cannot be performed within an hour, the antibiotic and the steroid are given regardless; the CSF is then obtained when practical, accepting a lower culture yield.[8]
[8]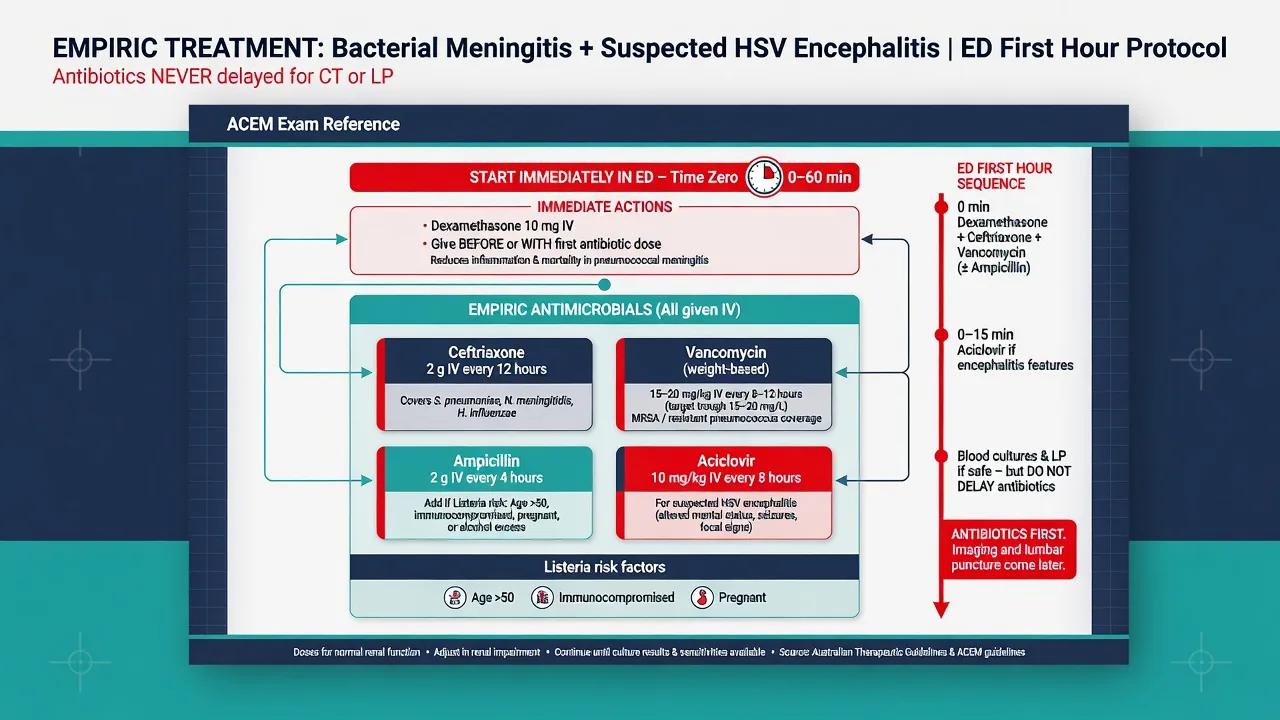
Definitive management and the antiviral
Once the organism is identified, therapy is narrowed. Pneumococcal meningitis receives ceftriaxone 2 g every 12 hours (with vancomycin until sensitivity confirms penicillin susceptibility), meningococcal meningitis receives ceftriaxone 2 g every 12 hours for seven days, and listerial meningitis receives ampicillin or amoxicillin plus gentamicin for at least three weeks. Herpes simplex encephalitis receives aciclovir 10 mg/kg intravenously every 8 hours for 14 to 21 days, with hydration to protect against the nephrotoxicity; the dose is weight-based and the course is long because relapse follows an abbreviated course. Tuberculous meningitis is treated with quadruple therapy (rifampicin, isoniazid, pyrazinamide, ethambutol) plus adjunctive corticosteroids, and cryptococcal meningitis with amphotericin B plus flucytosine induction then fluconazole consolidation. Chemoprophylaxis of the close contacts of a meningococcal case — rifampicin 600 mg every 12 hours for two days, or a single oral dose of ciprofloxacin 500 mg — is a public-health responsibility that begins from the emergency department.[4]
Subtypes and specific scenarios
Meningococcaemia progresses within hours from a febrile flu-like illness to a purpuric rash, septicaemic shock and multi-organ failure; the Waterhouse-Friderichsen syndrome is the bilateral adrenal haemorrhage of disseminated intravascular coagulation that drives the refractory shock. Herpes simplex encephalitis is the time-critical, treatable encephalitis — the clinical pattern is temporal-lobe, the MRI shows oedema in the inferomedial temporal lobe, and the CSF HSV PCR is the diagnostic test. Tuberculous meningitis runs a basal, vasculitic course with cranial-nerve palsies and a very low CSF glucose. Cryptococcal meningitis complicates advanced HIV with an insidious headache and a raised opening pressure. Post-neurosurgical or shunt-related meningitis is caused by staphylococci and Gram-negative bacilli and demands vancomycin plus a cephalosporin or meropenem with Gram-negative cover.[4]
Complications and pitfalls
The complications are systemic and neurological. Cerebral oedema and raised intracranial pressure progress to tentorial herniation — the feared complication of a lumbar puncture performed against a raised pressure, which the CT-before-LP criteria exist to prevent. Seizures may be generalised or focal and require standard anticonvulsants. Disseminated intravascular coagulation accompanies meningococcaemia and drives the purpura, the adrenal haemorrhage and the digital ischaemia. Waterhouse-Friderichsen syndrome is the adrenal failure of that haemorrhage and demands stress-dose hydrocortisone in the shocked patient. Long-term sequelae include sensorineural deafness, cognitive impairment, epilepsy and hydrocephalus. The pitfalls are the dangerous inverse of the management: delaying the antibiotic for the CT or the LP; omitting dexamethasone or giving it after the antibiotic; forgetting ampicillin for listeria in the over-50; failing to start aciclovir empirically in suspected HSV; performing an LP against a raised pressure; and forgetting chemoprophylaxis and public-health notification.[8]
Prognosis and disposition
Community-acquired bacterial meningitis carries an in-hospital mortality around 20 per cent, and a further 30 per cent survive with neurological sequelae; pneumococcal disease and an altered consciousness at presentation are the worst prognostic markers. Herpes simplex encephalitis kills around 70 per cent of untreated patients and, even with aciclovir, leaves roughly 30 per cent dead or severely disabled — the outcome tracks the time to the antiviral. Disposition is to a ward bed for the stable patient with a normal GCS, and to intensive care for any patient with a GCS of 8 or below, recurrent seizures, respiratory failure, or septic shock. Public-health notification of a confirmed or suspected meningococcal case is mandatory and triggers contact tracing and chemoprophylaxis.[9]
Special populations
The neonate presents with non-specific signs (lethargy, poor feeding, a bulging fontanelle, apnoea) and the organisms are group B streptococcus, Escherichia coli and Listeria; the empiric regimen is ampicillin plus a third-generation cephalosporin (or ampicillin plus gentamicin). The elderly and the immunocompromised present atypically — confusion without fever, or a subtle meningeal sign — and mandate ampicillin for listeria on top of the standard regimen. The pregnant patient has a heightened listeria risk and receives ampicillin; aciclovir is safe in pregnancy and is not withheld. The asplenic patient is at extreme risk of overwhelming pneumococcal or meningococcal sepsis and receives ceftriaxone empirically at any febrile presentation. The post-neurosurgical or shunt patient has a different flora and a different regimen, focused on staphylococci and Gram-negatives.[8]
The empiric regimen in detail
The empiric regimen is the single most exam-critical therapeutic decision in central nervous system infection, and it is built from three questions: which organism, which host, and which syndrome (meningitis versus encephalitis). The backbone is a third-generation cephalosporin (ceftriaxone or cefotaxime) at meningitic dosing; vancomycin is added for the penicillin-resistant pneumococcus; ampicillin is added for listeria in the at-risk host; and aciclovir is added the moment herpes encephalitis is plausible. The mnemonic below fixes the agent and the dose in memory.[1][2][7]
VANDAL — the empiric CNS-infection regimen, agent by agent
VANDAL
Vancomycin 15 to 20 mg/kg IV every 8 to 12 hours — for the penicillin-resistant pneumococcus; target a trough or an AUC, given alongside the beta-lactam
Ampicillin 2 g IV every 4 hours (or amoxicillin) — for Listeria in any patient over 50, immunocompromised, pregnant, or alcoholic; ceftriaxone does NOT cover Listeria
Ceftriaxone 2 g IV every 12 hours (or cefotaxime 2 g every 6 hours) — the backbone for pneumococcus, meningococcus, H. influenzae, group B strep, and the Gram-negative bacilli
Dexamethasone 10 mg IV every 6 hours for 4 days — given just BEFORE or WITH the first antibiotic dose; the benefit is concentrated in pneumococcal disease
Aciclovir 10 mg/kg IV every 8 hours — for suspected HSV encephalitis; start empirically, do not wait for the PCR
LP after the antibiotics if the imaging or the clinical criteria demand it — the antibiotics never wait for the LP or the CT; cultures may still be positive for hours after a dose
The ED first hour in suspected bacterial meningitis
Triage to the resuscitation bay; the ABC first; high-flow oxygen only if hypoxic; full monitoring; secure two large-bore cannulae.
The focused assessment: the triad (fever, headache, neck stiffness), the GCS in its components, a petechial or purpuric rash, a focal neurological deficit, a seizure, and a contiguous source (otitis, sinusitis, mastoiditis, a CSF leak, a cochlear implant).
Draw two sets of blood cultures, a venous lactate, a full blood count, a coagulation screen, a U&E, an LFT, a glucose, and a venous blood gas — before the antibiotics if it can be done within minutes, but NEVER let the bloods delay the antibiotic.
Give the empiric regimen immediately and within the first hour — ceftriaxone 2 g IV plus vancomycin 15 to 20 mg/kg IV, with dexamethasone 10 mg IV given just before or with the first antibiotic; add ampicillin 2 g IV for listeria in the over-50 or the immunocompromised; add aciclovir 10 mg/kg IV if HSV encephalitis is suspected.
Apply the CT-before-LP criteria: image first if immunocompromised, a new seizure within a week, a history of CNS disease, papilloedema, an abnormal conscious level, or a focal deficit. If none apply, proceed to the LP after the antibiotics.
Perform the lumbar puncture: measure the opening pressure, collect four tubes (a cell count and differential, a protein and glucose with a simultaneous serum glucose, a Gram stain and culture, and a spare for PCR or special studies), and send the HSV PCR if encephalitis is suspected.
Reassess for the septic shock — the Hour-1 sepsis bundle (30 mL/kg crystalloid, the vasopressors to a MAP of 65, the lactate-guided resuscitation) runs in parallel; intubate for a GCS of 8 or below, a respiratory failure, or a loss of the airway protection.
Notify public health for any confirmed or suspected meningococcal case; identify the close contacts for the chemoprophylaxis; admit to ICU if the GCS is 8 or below, the seizures are recurrent, or the shock is refractory.
Organism-specific definitive therapy
Once the organism and the sensitivities return, the regimen narrows. The table below fixes the agent, the dose, and the duration for each of the common pathogens — the duration matters because an abbreviated course of aciclovir or of listerial therapy relapses.[4]
S. pneumoniae
- Ceftriaxone 2 g IV 12-hourly for 10 to 14 days
- Vancomycin continued until the penicillin susceptibility is confirmed
- Dexamethasone 10 mg IV 6-hourly for 4 days
- The commonest adult organism (around 68 per cent); the mortality is 18 to 30 per cent
N. meningitidis
- Ceftriaxone 2 g IV 12-hourly for 7 days
- Rifampicin or a single-dose ciprofloxacin to eradicate the nasopharyngeal carriage before discharge
- The dexamethasone benefit is uncertain; many units give it empirically until the organism is known
- The public-health notification is mandatory; the chemoprophylaxis of the close contacts
Listeria monocytogenes
- Ampicillin 2 g IV 4-hourly (or amoxicillin) PLUS gentamicin for synergy, for at least 21 days
- The cephalosporins do NOT cover listeria — the trap
- Targets the over-50, the immunocompromised, the pregnant, the alcoholic
- The mortality is the highest of the common organisms — up to 32 per cent
H. influenzae
- Ceftriaxone 2 g IV 12-hourly for 7 days
- Now rare since the conjugate vaccination; consider in the asplenic and the unvaccinated adult
- The dexamethasone benefit is better established than for pneumococcus
- The chemoprophylaxis of the household contacts if an unvaccinated child under 4 is present
HSV encephalitis
- Aciclovir 10 mg/kg IV 8-hourly for 14 to 21 days
- Pre-hydrate to prevent the crystallisation nephrotoxicity; dose-adjust for the renal function
- Do NOT truncate the course — the relapse follows an abbreviated 10-day course
- Repeat the CSF PCR at 3 to 7 days if initially negative but clinically compatible
The role of dexamethasone
Adjunctive dexamethasone blunts the inflammatory cytokine surge released by the antibiotic-mediated bacterial lysis. The benefit is real but narrow: it reduces the neurological sequelae and, in pneumococcal disease, the mortality, but ONLY when it is given before or with the first antibiotic dose — given after the antibiotic it is ineffective because the inflammatory cascade has already been triggered. The Cochrane meta-analysis confirmed the mortality benefit in pneumococcal meningitis and the hearing-loss reduction in Haemophilus disease.[3][5][6] The trial that established the practice — the European Dexamethasone in Adulthood Bacterial Meningitis Study — showed a reduction in the unfavourable outcome from 25 per cent to 15 per cent in pneumococcal meningitis, with the benefit disappearing when the steroid was given after the antibiotic.[5]
de Gans and van de Beek — Dexamethasone in adults with bacterial meningitis
New England Journal of Medicine, 2002
A multicentre randomised double-blind placebo-controlled trial of dexamethasone 10 mg IV every 6 hours for 4 days, started before or with the first antibiotic dose, in 301 adults with suspected bacterial meningitis.
Key finding
Dexamethasone reduced the unfavourable outcome (death or severe disability) from 25 per cent to 15 per cent overall, and reduced the mortality in pneumococcal meningitis from 34 per cent to 14 per cent. The benefit was abolished when the steroid was given after the antibiotic.
Practice change
Dexamethasone 10 mg IV before or with the first antibiotic dose, for 4 days, is the standard of care in the suspected pneumococcal meningitis — the timing is non-negotiable.
Lumbar puncture timing and technique
The lumbar puncture is the diagnostic centrepiece, but its timing is governed by one overriding principle: the antibiotic is never delayed for the LP or for the CT. If the LP cannot be performed within an hour, the empiric regimen is given regardless, and the LP follows when practical — accepting that the Gram-stain and culture yields fall after antibiotics, but the cell count, the protein, the glucose ratio, and the HSV PCR remain informative for days. The CSF bacterial culture is rendered sterile within 4 to 8 hours of an effective antibiotic dose, but the white-cell differential and the biochemistry are preserved.[8]
When to CT before the LP
The CT-before-LP criteria exist to prevent the cerebral herniation — the feared, often fatal complication of performing an LP against a raised intracranial pressure from a space-occupying lesion or a cerebral oedema. The six criteria are drawn from the IDSA and the ESCMID frameworks.[7][2] A normal CT does NOT guarantee a safe LP, but the absence of all six criteria in an immunocompetent patient with a normal GCS and no focal deficit makes the LP safe to proceed without imaging.
CT before LP (any one)
- Immunocompromised state (HIV, transplant, chemotherapy, chronic steroids)
- A new-onset seizure within one week
- An abnormal level of consciousness (a reduced GCS, or a confused/drowsy patient)
- A focal neurological deficit (a cranial nerve, a motor, or a sensory)
- Papilloedema on the fundoscopy
- A history of CNS disease (a mass, a stroke, an infection) or a CSF shunt
LP without CT
- Alert and oriented (a normal GCS)
- No immunocompromise
- No new seizure
- No focal deficit
- No papilloedema
- No history of CNS disease — proceed to the LP after the antibiotics
The lumbar puncture procedure in the ED
Confirm the indications are met and the CT-before-LP criteria are negative; obtain the consent; check the platelet count (above 50) and the INR (under 1.4).
Position the patient in the lateral decubitus position with the knees drawn to the chest and the neck flexed for the opening pressure — or seated and leaning forward if the lateral position is impractical.
Identify the L3–L4 or L4–L5 interspace (the spinal cord ends at L1–L2 in the adult; Tuffier's line joins the iliac crests at L4); sterilise and drape; raise a wheal with 1 per cent lidocaine.
Advance the spinal needle with the stylet in place, the bevel oriented to open parallel to the longitudinal dural fibres (to spread rather than cut them); feel the "pop" of the ligamentum flavum and the dura.
Remove the stylet and confirm the CSF flow; attach the manometer and measure the opening pressure in the lateral position (a normal adult pressure is 8 to 20 cm of water; raised in meningitis and the cryptococcal disease); do NOT measure in the seated position.
Collect four tubes of 1 to 2 mL each: tube 1 for the cell count and the differential, tube 2 for the protein and the glucose (with a simultaneous serum glucose), tube 3 for the Gram stain, the culture and the sensitivity, tube 4 for the special studies (the HSV PCR, the cryptococcal antigen, the TB PCR, the cytology) and a spare.
Re-insert the stylet before the withdrawal (to reduce the risk of a post-dural puncture headache and the nerve-root entrapment); dress the site; lay the patient flat for 1 to 2 hours.
Send the samples immediately with a clear request form — the cell count degrades within an hour, and the Gram stain is most informative before any antibiotic has diffused into the CSF.
CSF opening pressure and the Gram stain
The opening pressure is measured only in the lateral decubitus position with the legs relaxed — a normal adult pressure is 8 to 20 cm of water, and a raised pressure above 25 cm is characteristic of the acute bacterial meningitis, the cryptococcal meningitis, and any space-occupying lesion. The CSF is interpreted by its cell count and differential, its glucose against a simultaneous serum glucose, and its protein — the Gram stain and the culture are confirmatory but rarely available in the first hour. A traumatic tap is corrected by subtracting one white cell for every 700 red cells.[2]
The CSF Gram-stain yield by organism
Chemoprophylaxis and public health
The meningococcal disease is notifiable in every jurisdiction, and the chemoprophylaxis of the close contacts is a public-health responsibility that begins in the emergency department. The contacts at risk are the household and the kissing contacts, the healthcare worker who performed the mouth-to-mouth resuscitation or who was exposed to the droplets during an intubation without protection, and the index case themselves before discharge (to eradicate the nasopharyngeal carriage). The window is short — the chemoprophylaxis is most effective within 24 hours of the index case's diagnosis and is generally not recommended after 7 days.[2]
Rifampicin
- 600 mg orally every 12 hours for 2 days (4 doses) in adults; 10 mg/kg in the children
- Reduces the orange body fluids; induces the hepatic enzymes (reduces the contraceptive pill)
- Effective against both the meningococcus and the H. influenzae carriage
Ciprofloxacin
- A single oral dose of 500 mg in adults; preferred in the mass-prophylaxis settings
- Does not reduce the body fluids; no enzyme induction
- Preferred where the adherence to a 2-day rifampicin course is a concern
Ceftriaxone
- A single intramuscular dose of 250 mg in adults; useful in the pregnancy
- Safe in the pregnancy where the rifampicin and the ciprofloxacin are avoided or counselled
- No reduction of body fluids; a reliable eradication
Viral encephalitis in depth
The viral encephalitis is distinguished from the viral meningitis by the involvement of the brain parenchyma — an altered consciousness, a seizure, a focal deficit, or a behavioural change, in addition to the fever and the headache. The herpes simplex virus type 1 is the commonest sporadic cause and the only one with a time-critical, mortality-reducing therapy, so the empiric aciclovir is started the moment the diagnosis is plausible and is continued until the CSF HSV PCR is negative at 3 to 7 days. The other viral causes — the varicella-zoster, the enterovirus, the Epstein–Barr, the mumps, and the arboviruses (the Japanese encephalitis, the Murray Valley encephalitis, the West Nile) — are managed supportively, though the aciclovir is empirically continued until the HSV is excluded because the clinical overlap is complete.[4]
[4] [4]Whitley et al — Vidarabine versus acyclovir in herpes simplex encephalitis
New England Journal of Medicine, 1986
A randomised collaborative trial of the acyclovir versus the vidarabine in 208 patients with a biopsy-proven herpes simplex encephalitis — the definitive study that established aciclovir as the treatment.
Key finding
Acyclovir reduced the 6-month mortality from 54 per cent (vidarabine) to 19 per cent, and increased the proportion returning to a normal function from 13 per cent to 38 per cent. The outcome tracked the Glasgow Coma Scale at the presentation — the earlier the therapy, the better the outcome.
Practice change
Aciclovir 10 mg/kg IV every 8 hours for 14 to 21 days is the standard of care for the HSV encephalitis; start empirically and do not wait for the PCR.
Drost et al — Outcomes of adults with community-acquired bacterial meningitis (the Netherlands nationwide cohort)
Lancet Regional Health Europe, 2026
A prospective nationwide cohort of 2974 adults with a CSF-confirmed community-acquired bacterial meningitis in the Netherlands over 2006 to 2024.
Key finding
The S. pneumoniae caused 68 per cent, the N. meningitidis 11 per cent, the L. monocytogenes 6 per cent. The overall mortality was 17 per cent and stable over 18 years; the Listeria had the highest mortality at 32 per cent. An unfavourable outcome occurred in 39 per cent, with a hearing impairment in 31 per cent and a cognitive impairment in 23 per cent of the survivors; the absence of the adjunctive dexamethasone was a predictor of the unfavourable outcome.
Practice change
The mortality and the morbidity remain high despite the modern therapy — the timely recognition, the correct empiric regimen, and the adjunctive dexamethasone are the modifiable levers in the ED.
Pitfalls at the bedside
The errors in the meningitis and the encephalitis are the inverse of the correct management, and they are the recurrent themes of the Fellowship viva and the morbidity-and-mortality meeting.[8]
[8] [8] [1] [8] [8] [1] [4] [8] [8] [8]Evidence and regional guidelines
The contemporary framework is the ESCMID 2016 guideline on the diagnosis and treatment of acute bacterial meningitis[2] and the landmark New England Journal review of community-acquired bacterial meningitis in adults.[1] Adjunctive dexamethasone is supported by the Cochrane meta-analysis, which shows a mortality and morbidity benefit concentrated in pneumococcal disease when the steroid is given before or with the first antibiotic dose.[3] Aciclovir for herpes simplex encephalitis rests on the classic vidarabine-versus-aciclovir trial that established the mortality advantage of aciclovir.[4]
ANZ practice note. The empiric regimen and the dexamethasone timing follow the Therapeutic Guidelines (eTG) and the local infectious-diseases protocol, aligned with the ESCMID framework. Meningococcal disease and tuberculosis are notifiable in all Australian states and New Zealand; chemoprophylaxis of close contacts uses rifampicin or single-dose ciprofloxacin, and the public-health unit is notified from the emergency department.[7]
Exam pearls
- The classic triad (fever, headache, neck stiffness) is all present in only 44 per cent — fever plus headache is present in 95 per cent; an altered consciousness is the red flag for severity.
- Antibiotics before the LP, always — give the empiric dose within the first hour and before any CT if there is any delay; a normal CT does not guarantee a safe LP.
- Dexamethasone 10 mg IV before or with the first antibiotic dose, for four days — benefit is in pneumococcal disease.
- Add ampicillin (2 g IV every 4 hours) for listeria in any patient over 50, immunocompromised, pregnant, or alcoholic — ceftriaxone does not cover it.
- Aciclovir 10 mg/kg IV every 8 hours for suspected HSV — start empirically, do not wait for the PCR.
- CSF: neutrophils and low glucose means bacterial; lymphocytes and normal glucose means viral; lymphocytes and very low glucose means tuberculous.
- Chemoprophylaxis for meningococcal contacts: rifampicin 600 mg twice daily for two days, or a single dose of ciprofloxacin 500 mg — and notify public health.
- S. pneumoniae is the commonest community-acquired organism in adults (around 68 per cent), followed by N. meningitidis (11 per cent); Listeria targets the over-50 and the immunocompromised and is not covered by any cephalosporin.
- The CSF Gram stain is positive in 60 to 90 per cent of untreated bacterial meningitis and becomes negative within hours of the first antibiotic dose — send the CSF early.
- The CSF bacterial culture is sterilised within 4 to 8 hours of an effective antibiotic, but the cell count, the glucose, the protein and the HSV PCR remain informative — never withhold the antibiotic for the LP.
- The opening pressure is measured only in the lateral decubitus position — a normal adult range is 8 to 20 cm of water; a raised pressure is typical of bacterial and of cryptococcal meningitis.
- A traumatic tap is corrected by subtracting one white cell for every 700 red cells, and the CSF glucose is always interpreted against a simultaneous serum glucose (a ratio below 0.4 favours bacterial).
- The CSF lactate (above 4 mmol/L bacterial, below 3 mmol/L viral) is a useful adjunct in the ambiguous or the partially-treated CSF.
- The dexamethasone is futile if given after the antibiotic — the inflammatory cascade from the bacterial lysis is already running; give it before or with the first dose.
- The CSF HSV PCR can be negative in the first 48 hours — a compatible picture with a negative early PCR warrants a continued aciclovir and a repeat LP at 3 to 7 days.
- Aciclovir is crystalline-nephrotoxic — pre-hydrate with a litre of normal saline and dose-adjust for the renal function; the 14 to 21-day course must not be truncated (the relapse follows an abbreviated course).
- Tuberculous meningitis is the great mimic of the subacute case — a lymphocytic CSF, a very high protein, and a glucose often below 1 mmol/L; treat empirically on the suspicion and do not wait for the culture.
- Cryptococcal meningitis in the CD4-below-100 patient may have a bland CSF — the India ink, the cryptococcal antigen, and the opening pressure are the keys; a raised pressure is decompressed by the repeated therapeutic LPs.
- The neonate has non-specific signs and a different flora (the group B strep, the E. coli, the Listeria) — the empiric regimen is ampicillin plus a third-generation cephalosporin or plus gentamicin.
- Meningococcaemia may present with the rash before the neck stiffness — any febrile petechial or purpuric rash is treated empirically; the Waterhouse-Friderichsen adrenal haemorrhage demands the stress-dose hydrocortisone in the refractory shock.
- A normal CT does NOT guarantee a safe LP — apply the six CT-before-LP criteria, but the priority in a deteriorating patient is the intubation, the CT, and the neurosurgery, not the LP.[9]
Exam practice
SAQ — Empiric management of community-acquired bacterial meningitis with dexamethasone timing
10 minutes · 10 marks
A 42-year-old woman is brought to the emergency department by her husband 6 hours after the sudden onset of severe generalised headache, fever and neck stiffness. She has been vomiting for 4 hours and has become progressively drowsy. On arrival she is alert but confused (GCS 13 — E3 V4 M6), temperature 39.4 degrees C, heart rate 118, BP 102/68 (MAP 79), RR 22, SpO2 96 per cent on room air. A non-blanching petechial rash is noted on the lower limbs and trunk. Neck stiffness and a positive Kernig sign are present; the pupils are equal and reactive, there is no focal neurological deficit and the fundi are normal. She has no drug allergies and takes no regular medications.
SAQ — Empiric workup and management of suspected herpes simplex encephalitis
10 minutes · 10 marks
A 58-year-old man with a past history of well-controlled epilepsy on sodium valproate presents to the emergency department at 02:00 with 36 hours of fever (38.5 degrees C at home), worsening confusion, and a new-onset generalised tonic-clonic seizure witnessed by his wife 30 minutes before arrival. On examination he is drowsy (GCS 11 — E3 V3 M5), temperature 38.8 degrees C, HR 108, BP 138/82, SpO2 96 per cent on room air. He is unable to follow commands but localises to pain symmetrically. There is no neck stiffness, no rash, the pupils are equal and reactive, and the bedside glucose is 6.4 mmol/L. His wife reports he has been 'odd and quiet' over the last 24 hours and has been smelling burning rubber that is not there — an olfactory hallucination.
Red flags
[8]References
- [1]van de Beek D, de Gans J, Tunkel AR, Wijdicks EFM. Community-acquired bacterial meningitis in adults. New England Journal of Medicine, 2006.PMID 16394301
- [2]van de Beek D, Cabellos C, Dzupova O, et al. ESCMID guideline: diagnosis and treatment of acute bacterial meningitis. Clinical Microbiology and Infection, 2016.PMID 27062097
- [3]Brouwer MC, McIntyre P, de Gans J, Prasad K, van de Beek D. Corticosteroids for acute bacterial meningitis. Cochrane Database of Systematic Reviews, 2010.PMID 20824838
- [4]Whitley RJ, Alford CA, Hirsch MS, et al. Vidarabine versus acyclovir therapy in herpes simplex encephalitis. New England Journal of Medicine, 1986.PMID 3001520
- [5]de Gans J, van de Beek D, European Dexamethasone in Adulthood Bacterial Meningitis Study Investigators. Dexamethasone in adults with bacterial meningitis. New England Journal of Medicine, 2002.PMID 12432041
- [6]Brouwer MC, McIntyre P, Prasad K, van de Beek D. Corticosteroids for acute bacterial meningitis. Cochrane Database of Systematic Reviews, 2015.PMID 26362566
- [7]Tunkel AR, Hartman BJ, Kaplan SL, et al. Practice guidelines for the management of bacterial meningitis. Clinical Infectious Diseases, 2004.PMID 15494903
- [8]Auburtin M, Wolff M, Charpentier J, et al. Detrimental role of delayed antibiotic administration and penicillin-nonsusceptible strains in adult intensive care unit patients with pneumococcal meningitis. Critical Care Medicine, 2006.PMID 16915106
- [9]Drost EHGM, Schepers EN, Chekrouni N, et al. Outcomes of adults with community-acquired bacterial meningitis in the Netherlands: a prospective nationwide cohort study. Lancet Regional Health Europe, 2026.PMID 41323877