ICU · Cardiovascular
Cardiac arrhythmia management in the ICU
Also known as Atrial fibrillation · Ventricular tachycardia · Bradycardia and heart block · Cardiac arrhythmia · Supraventricular tachycardia · Atrial flutter · Torsades de Pointes · Complete heart block · Ventricular fibrillation · Antiarrhythmic pharmacology
Arrhythmias are common in ICU (up to 20% of patients). Types: atrial fibrillation (1 — new-onset AF in ICU is associated with worse outcomes), ventricular tachycardia/fibrillation (life-threatening — usually cardiac origin), bradyarrhythmias (heart block, sinus bradycardia), supraventricular tachycardia (AVNRT/AVRT), atrial flutter. Management principles: (1) is the patient haemodynamically unstable? → cardiovert/defibrillate immediately. (2) Identify and treat underlying cause (electrolytes, ischaemia, sepsis, drugs). (3) Rate vs rhythm control. AF: rate control (beta-blocker, diltiazem) usually first; rhythm control (amiodarone, DC cardioversion) if unstable. VT/VF: defibrillate + amiodarone. Bradycardia: atropine → adrenaline/pacing. SVT: vagal manoeuvres → adenosine 6→12→12 mg. Torsades: IV magnesium, stop QT-prolonging drugs, overdrive pacing.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags

General approach — first principles
The first decision in any arrhythmia is NOT the ECG diagnosis — it is haemodynamic stability. This single decision bifurcates management: the unstable patient needs an electrical therapy immediately, regardless of rhythm; the stable patient has time for systematic diagnosis and pharmacological management. [1]
Universal arrhythmia algorithm
Step 1 — Assess haemodynamic stability
Unstable = ANY of: hypotension (SBP <90), acutely altered mental status, signs of shock (cold, mottled, oliguric), ischaemic chest pain, acute heart failure/pulmonary oedema. If unstable and tachyarrhythmia → immediate SYNCHRONISED cardioversion. If unstable and VF/pulseless VT → UNSYNCHRONISED defibrillation + CPR. Do NOT wait for IV access, drugs, bloods, or a 12-lead ECG.
Step 2 — 12-lead ECG + rhythm strip
In the stable patient, obtain a 12-lead ECG. Key questions: (a) Regular or irregular? (b) Narrow (<120 ms) or wide (>120 ms) QRS? (c) Is atrial activity visible (P waves, flutter waves, fibrillation)? (d) Rate? This 2×2 grid (regular/irregular × narrow/wide) generates the differential diagnosis.
Step 3 — Identify and treat the precipitant
POCKET-ACID mnemonic: Potassium/magnesium/calcium, Oxygen (hypoxia), Cardiac ischaemia, Ketoacidosis and other metabolic, EPS/drugs (inotropes, bronchodilators, QT-prolonging), Alcohol/sepsis/stress (catecholamine surge), Ischaemia/Infection, Dehydration/hypovolaemia. Send K+, Mg2+, Ca2+, troponin, VBG (lactate, K+), TFTs. Review the drug chart — inotropes, dopamine, dobutamine, milrinone, salbutamol, azoles, macrolides, antipsychotics all provoke arrhythmia.
Step 4 — Choose rate vs rhythm control
For AF/flutter: rate control is usually first-line (beta-blocker or diltiazem). Rhythm control (cardioversion, amiodarone) if: haemodynamically unstable, heart failure (tachycardia-induced cardiomyopathy), symptomatic despite rate control, or first presentation <48 h duration. EAST-AFNET 4: early rhythm control (within 1 year) improves outcomes in newly diagnosed AF.
Step 5 — Anticoagulation and long-term plan
Assess stroke risk (CHA2DS2-VASc) and bleeding risk (HAS-BLED). In ICU, balance against bleeding (recent surgery, coagulopathy, procedures). New-onset AF <48 h: anticoagulate if high risk. AF >48 h or unknown duration: anticoagulate for 3 weeks before AND 4 weeks after cardioversion (or TOE-guided). Involve cardiology for ablation/definitive management.
Arrhythmia epidemiology in ICU
Atrial fibrillation
AF is the commonest arrhythmia in ICU and a high-yield exam topic. New-onset AF in the ICU is not benign — it independently predicts longer ventilation, longer stay, stroke, and death. The intensivist's task is threefold: decide rate vs rhythm control, anticoagulate appropriately, and treat the precipitant. [1]
Pathophysiology and ICU triggers
AF is sustained by trigger firing (usually from the pulmonary vein ostia) and an arrhythmogenic substrate (atrial dilation and fibrosis). ICU patients have a surplus of both: catecholamine surges (sepsis, pain, agitation, inotropes), volume overload and atrial stretch, electrolyte depletion (K+, Mg2+ from diuresis and redistribution), hypoxia, acidosis, sympathetic withdrawal/withdrawal, and direct atrial injury (post-cardiotomy, central line/PA catheter irritation). [1]
[1]Rate versus rhythm control
Rate control (first-line in most ICU AF)
Beta-blocker or non-DHP CCB
- Beta-blocker: metoprolol 5 mg IV over 2 min, repeat q5 min × 3 (max 15 mg); OR esmolol 500 mcg/kg loading then 50–200 mcg/kg/min (short half-life — ideal to titrate in unstable/anaesthetised patients)
- OR non-dihydropyridine CCB: diltiazem 0.25 mg/kg IV (≈20 mg) over 2 min, repeat 0.35 mg/kg after 15 min if needed, then infusion 5–15 mg/h. AVOID verapamil/diltiazem in HFrEF (negative inotrope)
- OR digoxin 500 mcg IV over 30 min (additive with beta-blocker; slow onset 2–6 h; useful in HF/AF and when beta-blockers contraindicated). AVOID in renal failure, hypokalaemia, WPW
- Target: HR <110 (lenient) or <80 (strict). RACE II: lenient is non-inferior and easier to achieve; strict reserved for ongoing symptoms or tachycardia-mediated cardiomyopathy
- Caveat: rate control is harder in hyperadrenergic states (sepsis, post-op) — may need combination therapy or amiodarone
Rhythm control (cardioversion)
If unstable, HF, failed rate control, <48 h
- Pharmacological: amiodarone 300 mg IV over 20–60 min, then 900 mg/24 h infusion. Useful in HF, structural disease, renal failure. Slower than electrical (6–24 h)
- OR flecainide 2 mg/kg IV over 10 min (AVOID in structural/IHD — pro-arrhythmic)
- OR ibutilide 1 mg IV over 10 min (QT prolongation — do NOT use if QTc >440 ms)
- Electrical: synchronised DC cardioversion — AF: 120–200 J biphasic (escalating); flutter: 50–100 J. Sedate (propofol/ketamine + midazolam) if awake. Anterior–posterior pads more effective
- EAST-AFNET 4 (NEJM 2020): early rhythm control within 1 year of diagnosis improved composite CV outcome (HR 0.79). Strengthens case for rhythm control in newly diagnosed AF
Practical AF management in the ICU
1. Stabilise — is the patient unstable?
Hypotension/shock/ischaemia/HF → immediate synchronised DC cardioversion (200 J biphasic, escalating). Ensure sedation if awake. Pre-cardioversion anticoagulation is NOT a reason to delay if unstable.
2. Identify and correct precipitant
Check K+ (target >4.0), Mg2+ (>0.8), Ca2+. Treat hypoxia, sepsis, pain, agitation, withdraw inotrope if possible. Give K+/Mg2+ replacement even if borderline (magnesium potentiates rate control). Stop dopamine if causing the AF — switch to noradrenaline.
3. Rate control
Metoprolol 5 mg IV q5 min × 3 (avoid in severe asthma, decompensated HF with low EF). If HF/AF: diltiazem is safer (or digoxin/amiodarone). Target HR <110 (lenient) or <80 if HF/tachycardiomyopathy.
4. Rhythm control if indicated
Amiodarone 300 mg IV over 20–60 min, then 900 mg/24 h. OR synchronised DC cardioversion if AF duration <48 h (or TOE-guided to exclude LAA thrombus if >48 h/unknown).
5. Anticoagulate
CHA2DS2-VASc ≥2 in men (≥3 women) → anticoagulate. In ICU: therapeutic LMWH (enoxaparin 1 mg/kg BD, reduce for renal) or UFH (better if procedural/reversible). Switch to DOAC once stable and oral route restored. Hold anticoagulation only for active bleeding/procedures — NOT for rhythm control alone.
6. Long-term plan
Continue rate or rhythm control. Most new-onset ICU AF reverts within 48 h of treating the precipitant. Refer cardiology for ablation if recurrent/symptomatic. Initiate GDMT for HFrEF (beta-blocker, MRA, SGLT2i, ARNI — "four pillars") — these reduce AF.
Anticoagulation in the ICU patient with AF
Anticoagulation decisions in ICU are harder than the outpatient CHA2DS2-VASc calculation because of competing bleeding risk (recent surgery, coagulopathy, central lines, planned procedures) and rapidly changing renal function. [1]
[1]CHA2DS2-VASc (stroke risk)
Score → anticoagulate if ≥2 (men) / ≥3 (women)
- **C** — CHF/LV dysfunction (1)
- **H** — Hypertension (1)
- **A2** — Age ≥75 (2)
- **D** — Diabetes (1)
- **S2** — Stroke/TIA/thromboembolism (2)
- **V** — Vascular disease (MI, PAD, aortic plaque) (1)
- **A** — Age 65–74 (1)
- **Sc** — Sex category female (1)
- Score 0 (men) / 1 (women): omit. Score 1 (men) / 2 (women): consider. ≥2 (men) / ≥3 (women): anticoagulate.
HAS-BLED (bleeding risk)
≥3 = high bleeding risk — review/correct, not a reason to withhold
- **H** — Hypertension (SBP >160) (1)
- **A** — Abnormal renal/liver function (1 each)
- **S** — Stroke history (1)
- **B** — Bleeding history/predisposition (1)
- **L** — Labile INR (not applicable to DOAC) (1)
- **E** — Elderly (>65) (1)
- **D** — Drugs (antiplatelet/NSAID) or alcohol excess (1)
- A high score is NOT a reason to deny anticoagulation — it is a reason to correct modifiable factors (BP, NSAIDs, alcohol).
Specific ICU scenarios in AF
- Post-cardiac surgery AF (POAF): occurs in 30–40% of CABG/valve patients, peaks on day 2–3. Prophylaxis: amiodarone or beta-blocker (restore if withheld). Treat: rate control + anticoagulate (high stroke risk). Usually self-limited (<2 months) but anticoagulate for at least the perioperative period.
- Sepsis-associated AF: reflects catecholamine surge + electrolyte loss. Correct the sepsis, replace Mg2+/K+, switch dopamine to noradrenaline. Beta-blockade in septic shock is contentious — esmolol (titratable) preferred if needed. AF usually reverts with recovery.
- AF with HFrEF: AVOID diltiazem/verapamil (negative inotrope). Use digoxin, amiodarone, or a cardioselective beta-blocker (metoprolol/bisoprolol). Long-term: beta-blocker + MRA + SGLT2i + ARNI ("four pillars") reduce AF burden and mortality.
- AF with WPW (pre-excited): AVOID AV-nodal blockers (adenosine, verapamil, diltiazem, digoxin, beta-blocker) — they preferentially block the AV node and allow unrestricted antegrade conduction down the accessory pathway → pre-excited AF → VF. Use synchronised cardioversion if unstable, or procainamide/flecainide/ibutilide if stable (block the accessory pathway).
- Thyroid storm with AF: high-output, fast AF. Treat the storm (PTU, iodine, beta-blocker, steroids) — AF reverts with euthyroidism. Propranolol/esmolol preferred (blocks T4→T3 conversion). [1]
Atrial flutter
Atrial flutter is a macro-reentrant atrial tachycardia, classically around the cavotricuspid isthmus (typical, counterclockwise — "sawtooth" flutter waves at 300/min in inferior leads, 2:1 block → ventricular rate 150). Management mirrors AF in most respects, but with three key differences. [1]
[1]Atrial flutter management
1. Identify typical flutter
Sawtooth flutter waves (best in II, III, aVF, V1) at ~300/min. Usually 2:1 AV block → ventricular rate ~150. If rate is exactly 150 with regular narrow complex — flutter until proven otherwise. Carotid sinus massage/adenosine (transient AV block) unmask the flutter waves.
2. Stability assessment
Unstable → synchronised DC cardioversion at 50–100 J biphasic. Stable → proceed to pharmacological management.
3. Rate control
Beta-blocker (metoprolol, esmolol) or diltiazem. Often inadequate — flutter circuits are robust. Add digoxin or consider amiodarone.
4. Rhythm control
Synchronised cardioversion 50–100 J (most reliable). OR ibutilide 1 mg IV (effective but QT-prolonging — do NOT use if QTc >440 ms). OR overdrive atrial pacing if a permanent pacemaker/atrial wire in situ (post-cardiac surgery).
5. Anticoagulation
Same as AF — CHA2DS2-VASc. Anticoagulate before/after cardioversion per AF rules.
6. Definitive cure
Cavotricuspid isthmus ablation is curative for typical flutter (success >90%) — refer for electrophysiology once the ICU insult resolves.
Supraventricular tachycardia (SVT)
SVT refers to any tachycardia originating at or above the AV node. In practice the ICU SVT is AV nodal re-entrant tachycardia (AVNRT, ~60%) or AV re-entrant tachycardia (AVRT, e.g. WPW, ~30%), both presenting as a regular narrow-complex tachycardia at 150–250/min with no visible P waves. [1]
AVNRT (commonest SVT)
AV node has dual pathways
- Mechanism: dual AV nodal pathways (slow and fast) form a re-entrant circuit within the AV node
- ECG: regular narrow QRS at 150–250/min, P waves buried in QRS or pseudo R' in V1 / pseudo S in inferior leads (retrograde P)
- No accessory pathway — antegrade AND retrograde via AV node
- Cardiac arrest risk: low. Treat with AV-nodal blockade.
AVRT / WPW
Accessory pathway
- Mechanism: accessory pathway connects atrium to ventricle (e.g. bundle of Kent in WPW) — re-entry via AV node + pathway
- Orthodromic AVRT: antegrade AV node, retrograde pathway → narrow QRS, regular
- Antidromic AVRT: antegrade pathway → WIDE QRS (looks like VT) — dangerous
- WPW with AF: chaotic broad irregular QRS — DO NOT give adenosine/CCB/digoxin (risk of VF). Cardiovert or use procainamide/flecainide.
SVT termination — the adenosine protocol
1. Vagal manoeuvres (first-line, stable)
Modified Valsalva: forceful expiration against closed glottis for 15 s while semi-recumbent, then reposition supine with passive leg raise (or cough, carotid sinus massage if no bruits). Terminates ~25% of AVNRT. Establish IV access and run a continuous ECG strip during the manoeuvre.
2. Adenosine 6 mg rapid IV bolus
Draw up 6 mg, follow IMMEDIATELY with a 20 mL saline flush via a large proximal vein (antecubital fossa). Warn the patient: "you will feel a sense of doom, chest tightness, flushing — this lasts 10–15 s". Run continuous ECG. Adenosine half-life <10 s — speed of administration is critical.
3. Adenosine 12 mg if no response
If 6 mg fails to terminate, give 12 mg by the same rapid technique after 1–2 min. Use a 3-way tap or dual-syringe push technique to ensure the bolus reaches the heart in <5 s.
4. Adenosine 12 mg — second attempt
A second 12 mg dose can be given if the first 12 mg produced partial AV block but no termination. Maximum single dose 12 mg. Some patients need higher doses (18–24 mg) or are adenosine-resistant.
5. If adenosine fails or contraindicated
Verapamil 5 mg IV over 2 min (AVOID in HFrEF, broad-complex tachy, WPW). OR diltiazem. OR metoprolol 5 mg IV. OR amiodarone 300 mg IV if HF/structural disease. Synchronised DC cardioversion 50–100 J if unstable.
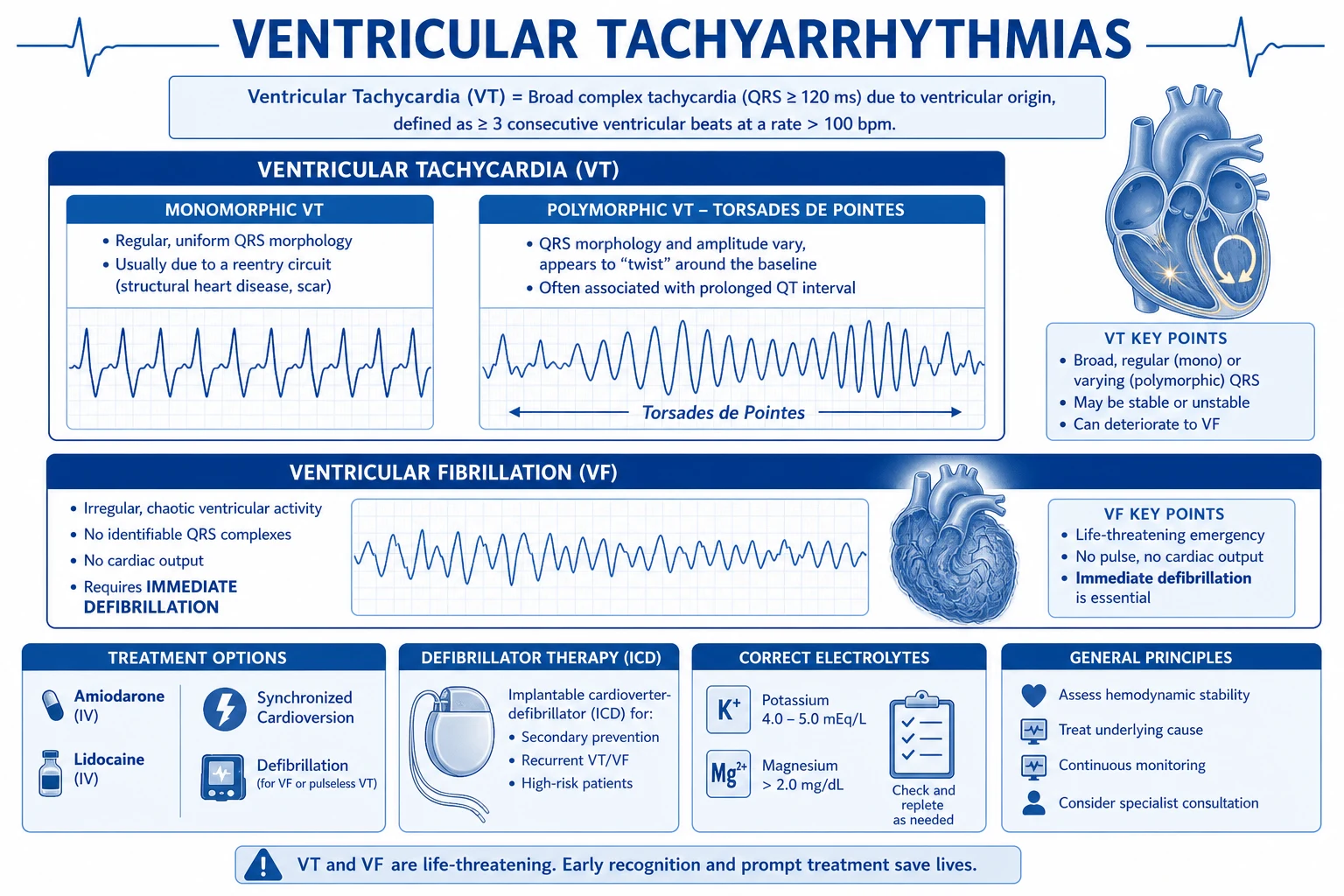
Ventricular arrhythmias
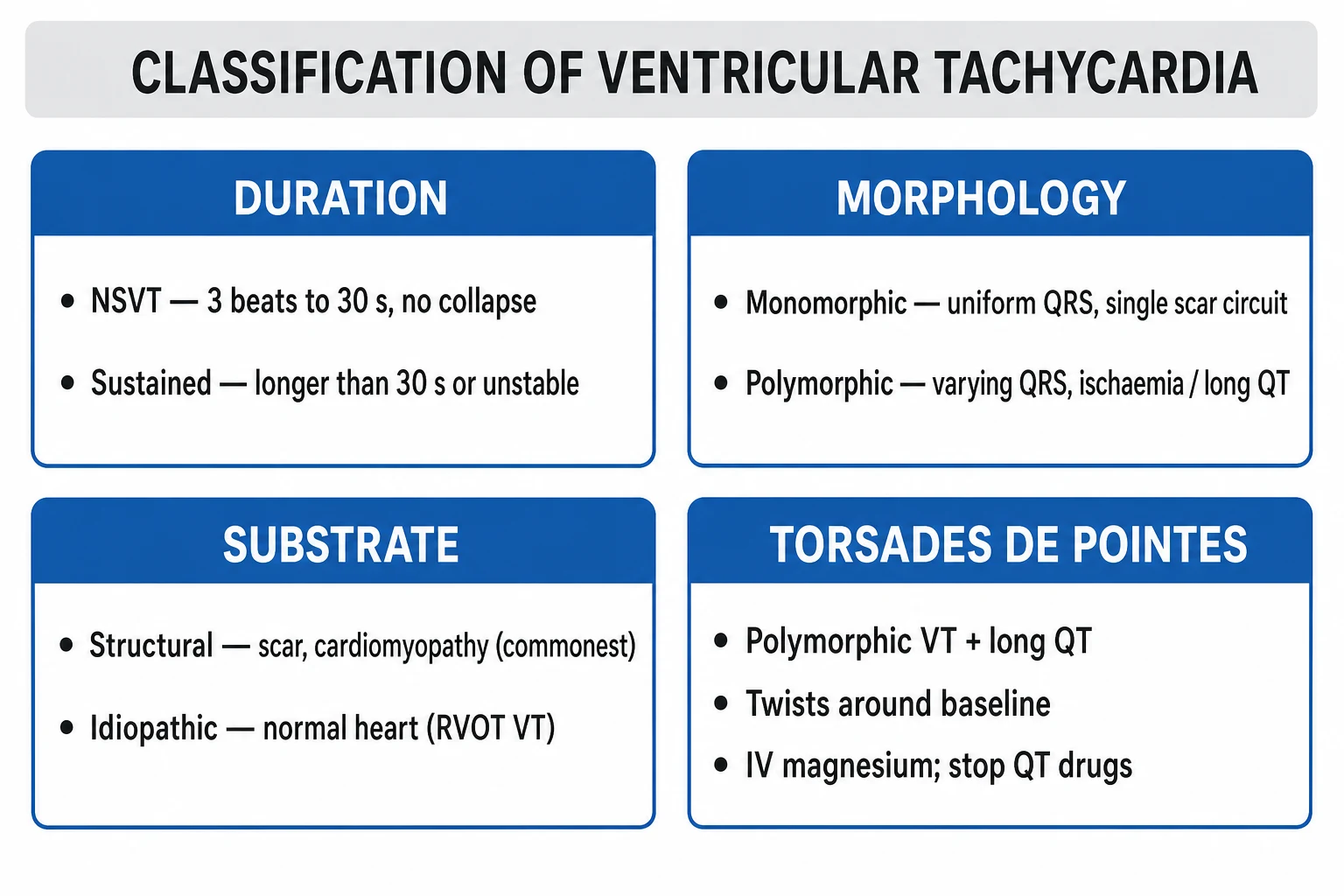
Ventricular arrhythmias in ICU are nearly always secondary — ischaemia, electrolyte derangement, drug toxicity, or the substrate of structural heart disease (post-MI scar, cardiomyopathy). The intensivist must distinguish monomorphic VT (single reentrant circuit, uniform QRS) from polymorphic VT (multiple foci, varying QRS axis), and from VF (disorganised, no identifiable QRS). [1]
Monomorphic vs polymorphic VT
Monomorphic VT
Uniform, regular wide QRS
- Regular, wide (>120 ms) QRS at 100–250/min, uniform morphology
- Mechanism: scar-related reentry (post-MI, cardiomyopathy, ARVC) OR bundle branch reentry OR idiopathic (RVOT, fascicular)
- AV dissociation, capture beats, fusion beats = pathognomonic (but often absent)
- Stable: amiodarone 150 mg IV over 10 min, then infusion 900 mg/24h. Alternatives: procainamide, lidocaine. Unstable: synchronised cardioversion 100 J escalating.
- Prognosis depends on substrate — post-MI scar VT ablation/ICD often indicated.
Polymorphic VT
Varying QRS morphology — ask: is QT long?
- Irregular, rapidly varying QRS morphology/axis at 200–300/min
- Two forms by QT: (1) **Torsades de Pointes** — prolonged QTc (>440 m / >460 f), twisting QRS around baseline, bradycardia-dependent. (2) **Normal-QT polymorphic VT** — usually ischaemia-driven (acute MI), or catecholaminergic (CPVT)
- Torsades treatment: IV magnesium 2 g, STOP all QT-prolonging drugs, correct K+ (>4.5), overdrive pacing / isoprenaline if bradycardia-dependent
- Normal-QT polymorphic VT: treat ischaemia (PCI), beta-blockade, correct electrolytes. Often degenerates to VF — be ready to defibrillate.
Stable vs unstable VT
The defining decision in VT is haemodynamic stability: [1]
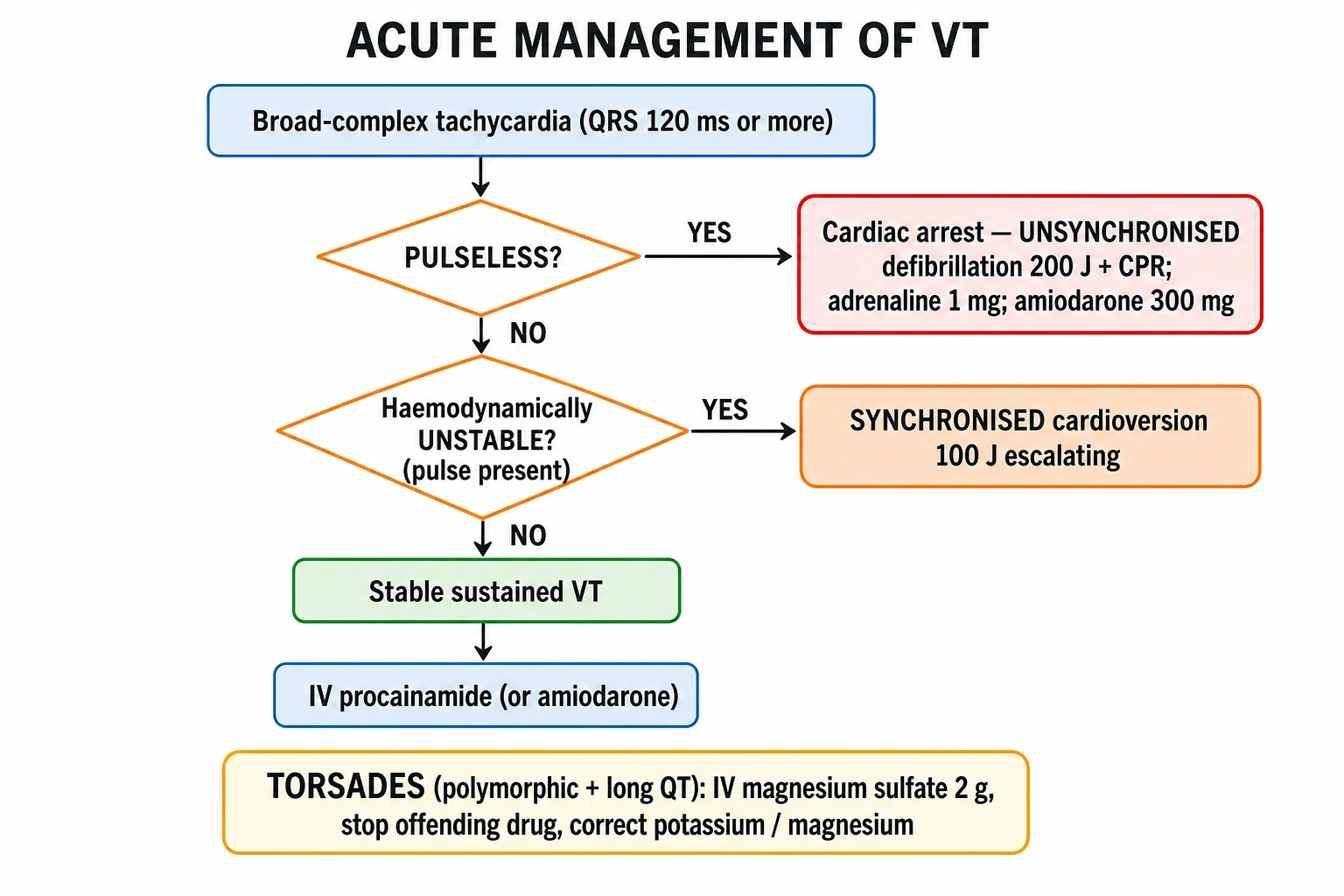
VT management algorithm
1. Is the patient pulseless?
NO pulse with VT = pulseless VT = cardiac arrest → UNSYNCHRONISED defibrillation 200 J biphasic immediately + CPR + ALS algorithm (adrenaline 1 mg q3–5 min, amiodarone 300 mg after 3rd shock).
2. Is the patient unstable (but with a pulse)?
Hypotension/shock/ischaemia/HF/altered mental status with a pulse → SYNCHRONISED DC cardioversion 100 J biphasic escalating (100→150→200 J). Sedate (propofol/ketamine + midazolam) if awake. Ensure the defibrillator is in SYNCH mode (syncs to R wave) — unsynchronised shock during the T wave can induce VF.
3. Stable VT — pharmacological termination
Amiodarone 150 mg IV over 10 min (then 1 mg/min × 6 h, then 0.5 mg/min). OR procainamide 20–50 mg/min until response/toxicity (hypotension, QRS widening 50%). OR lidocaine 1–1.5 mg/kg IV (repeat to 3 mg/kg). If fails → synchronised cardioversion.
4. Identify and treat the cause
Acute ischaemia → urgent PCI. Electrolytes → correct K+/Mg2+/Ca2+. Drug toxicity (digoxin, TCAs, cocaine) → specific antidotes. Long QT → stop offending drugs. Cardiomyopathy/scar → ICD referral.
5. Electrical storm — recurrent VT
≥3 episodes of VT/VF in 24 h. Treatment: beta-blockade (metoprolol/esmolol — most effective single agent), amiodarone + lidocaine infusion, deep sedation (propofol reduces sympathetic tone), correct K+/Mg2+, consider mechanical support (IABP/VA-ECMO) if cardiogenic. Ablation if scar-mediated.
Amiodarone vs lidocaine for VT/VF
Amiodarone (first-line)
Class III (mixed I–IV)
- Mechanism: blocks K+ channels (Class III) + Na+ (I) + beta (II) + Ca (IV) — broad-spectrum
- Dose: cardiac arrest 300 mg IV after 3rd shock, 150 mg after 5th; stable VT 150 mg over 10 min then infusion
- ALIVE trial (NEJM 2002): amiodarone superior to lidocaine for shock-resistant VF — survival to hospital 22.8% vs 12.0%
- ARREST trial (NEJM 1999): amiodarone improved survival to hospital vs placebo in OHCA VF (44% vs 34%)
- Acute SE: hypotension (solvent — give slowly), bradycardia. Chronic: pulmonary fibrosis, thyroid dysfunction, hepatitis, corneal deposits, photosensitivity, blue-grey skin, peripheral neuropathy. QT prolongation (low torsades risk as also blocks Ca).
Lidocaine (alternative)
Class Ib
- Mechanism: fast Na+ channel blocker (binds inactivated channels — preferential in ischaemic tissue)
- Dose: 1–1.5 mg/kg IV bolus, repeat 0.5–0.75 mg/kg q5–10 min to max 3 mg/kg, then infusion 1–4 mg/min
- Most useful for ischaemic VT (binds preferentially to depolarised ischaemic myocardium)
- SE: CNS — tinnitus, perioral tingling, seizures, altered mental state (dose-dependent). Avoid in severe hepatic disease, 2nd/3rd-degree block.
- On the way out for cardiac arrest (amiodarone preferred) but still useful for ischaemic VT and amiodarone-intolerant patients.
Torsades de Pointes
Torsades is polymorphic VT with prolonged QTc, classically with a twisting QRS axis around the baseline and bradycardia dependence (long-short initiating sequences, "pause-dependent"). It is the cardiac arrest rhythm you can actively cause and actively terminate. [1]
Torsades de Pointes — recognise and treat
Recognise
Polymorphic VT with QTc prolongation (>440 m / >460 f) on baseline ECG. Twisting QRS amplitude around isoelectric baseline. Often "pause-dependent" — long-short RR interval sequence precedes each episode (e.g. post-PVC pause). May be self-terminating or degenerate to VF.
IV magnesium sulphate 2 g over 10 min
FIRST-LINE and works even when serum Mg is normal — magnesium suppresses early afterdepolarisations (the trigger for torsades) by blocking Ca channels. Repeat 2 g if recurrent (up to 4–6 g total). Serum level is NOT a guide to efficacy.
STOP all QT-prolonging drugs
Review every drug: macrolides (erythro/clarithro/azithro), fluoroquinolones (moxifloxacin worst), antifungals (fluconazole), antipsychotics (haloperidol, droperidol, ziprasidone), methadone, antiarrhythmics (sotalol, amiodarone, quinidine, procainamide, ibutilide), TCAs, ondansetron. Use www.crediblemeds.org / www.qtdrugs.org for the full list. Stop one — stop them all.
Correct potassium aggressively
Target K+ >4.5 mmol/L (higher than usual — hypokalaemia prolongs QT and worsens torsades). Replace orally and IV.
Accelerate the heart rate (overdrive suppression)
Torsades is bradycardia-dependent — accelerating HR shortens QT and terminates the rhythm. Options: (a) isoprenaline infusion 1–4 mcg/min (if no ischaemia), (b) temporary pacing at 90–110 bpm (most reliable — transvenous if sustained), (c) atropine 0.5–1 mg (less reliable). Pacing rate should be set to keep QTc as short as possible.
If degenerates to VF — defibrillate
Unsynchronised 200 J biphasic + CPR + ALS. Torsades is a "shockable rhythm" if pulseless.
QTc thresholds and torsades risk
Channelopathies and inherited arrhythmia syndromes
[1]Bradyarrhythmias and AV block
Bradycardia in ICU spans the spectrum from benign sinus bradycardia (athlete, vasovagal, drugs) to life-threatening complete heart block. The key question is again stability: symptomatic bradycardia needs treatment; asymptomatic bradycardia needs monitoring and aetiology work-up. [1]
Classification of AV block
[1]Bradycardia management algorithm
Symptomatic bradycardia — stepwise management
1. Recognise symptomatic bradycardia
HR <60 (often <40) with hypotension, shock, syncope, ischaemic chest pain, acute HF, or altered mental status due to low cardiac output. Asymptomatic bradycardia in an athlete or during sleep is NOT an emergency.
2. Atropine 500 mcg IV
500 mcg IV every 3–5 min, max 3 mg (6 doses). Mechanism: muscarinic blockade → removes vagal tone → accelerates sinus node and AV conduction. Works in: sinus bradycardia, 1st-degree block, Mobitz I, symptomatic bradycardia after inferior MI (vagally mediated). Ineffective in: Mobitz II, complete heart block (block is below AV node — no vagal input there), denervated transplanted heart (no vagal tone to block).
3. Catecholamine infusion
Adrenaline 2–10 mcg/min (start 2, titrate to HR >60 and SBP >90). OR dopamine 5–20 mcg/kg/min. OR isoprenaline 1–4 mcg/min (pure beta — increases HR but drops diastolic BP; useful for bradycardia-dependent torsades and beta-blocker overdose). Choice depends on BP: adrenaline/dopamine if hypotensive, isoprenaline if normotensive.
4. Specific antidotes
Beta-blocker overdose: glucagon 3–5 mg IV over 2 min, then infusion 2–5 mg/h (bypasses beta-receptor — activates adenylyl cyclase via glucagon receptor → cAMP). Calcium channel blocker overdose: calcium chloride 1 g IV (repeated), high-dose insulin/euglycaemia (1 U/kg then 0.5–1 U/kg/h with glucose), lipid emulsion in refractory cases. Digoxin toxicity: Digoxin Fab antibody fragments (DigiFab) — see toxicology topic.
5. Transcutaneous pacing (TCP)
External pacing pads (anterior–posterior or anterior–left lateral). Set rate 60–80, mA gradually above capture threshold (typically 40–80 mA). Always confirm ELECTRICAL capture (wide QRS after each pacing spike) AND MECHANICAL capture (palpable pulse matching paced rate). Bridge only — may be painful (sedate), unreliable in obese/emphysema.
6. Transvenous pacing (definitive bridge)
Semi-floating bipolar pacing wire via right IJV (or subclavian/femoral) into RV apex under fluoroscopy or ECG guidance. Set rate 60, output above capture threshold (typically 1–3 mA — the lower the capture threshold the more stable). Sensitivity set so the pacemaker senses intrinsic R waves. Indications: complete heart block, Mobitz II with symptoms, symptomatic bradycardia not responding to atropine/catecholamines, bradycardia-dependent torsades, post-cardiac arrest bradycardia. Permanent pacemaker for definitive treatment.
Transcutaneous pacing (TCP)
Bridge only
- Quick, non-invasive, can be done by any clinician
- Pads anterior–posterior or anterior–left lateral. Set rate 60–80, mA above capture threshold
- Often painful — sedate (ketamine/fentanyl/midazolam)
- Capture unreliable in obesity, emphysema, large effusions
- Use while arranging transvenous pacing — NEVER a destination therapy
Transvenous pacing (TVP)
Definitive temporary pacing
- Bipolar wire via right IJV → RV apex (under fluoroscopy/echo or ECG guidance)
- More reliable, less painful, allows patient mobility
- Set rate 60, output 1–3 mA above threshold, sensitivity 1.5–2.5 mV
- Risks: pneumothorax (IJV/subclavian), infection, myocardial perforation/tamponade, diaphragmatic pacing, lead displacement
- Bridge to permanent pacemaker in complete heart block. Permanent pacemaker is the definitive treatment for symptomatic high-grade block.
Junctional rhythms
A junctional escape rhythm (narrow QRS, 40–60, no preceding P or retrograde P after QRS) is the AV node/junction protecting the heart when the sinus node fails or AV block prevents conduction. Junctional rhythm is rarely the primary problem — it is a marker of sinus node dysfunction, AV block, or drug effect (beta-blocker, CCB, digoxin). [1]
[1]ACLS integration — shockable vs non-shockable rhythms
The full ALS algorithm is covered in the arrhythmia-cardiac-arrest topic. The arrhythmia-specific elements relevant here: [1]
Shockable rhythms
VF / pulseless VT
- Unsynchronised defibrillation 200 J biphasic immediately + CPR
- Adrenaline 1 mg IV q3–5 min (after 3rd shock)
- Amiodarone 300 mg IV after 3rd shock, 150 mg after 5th (or lidocaine 100 mg if amiodarone unavailable)
- Reversible causes: 4 Hs (hypoxia, hypovolaemia, hypo/hyperkalaemia, hypothermia) and 4 Ts (tension pneumothorax, tamponade, thrombosis, toxins)
Non-shockable rhythms
Asystole / PEA
- Adrenaline 1 mg IV q3–5 min immediately (do NOT wait for 3rd shock)
- CPR 30:2 (or continuous if advanced airway)
- NO defibrillation — rhythm is non-shockable
- Identify and treat the reversible cause (4 Hs and 4 Ts) — this is the ONLY thing that works in PEA. Consider bedside ultrasound to find the cause (tamponade, RV dilatation in PE, empty hyperdynamic LV in hypovolaemia).
Antiarrhythmic pharmacology — the Vaughan-Williams classes
The intensivist must know the Vaughan-Williams classification, but also its limitations (most useful drugs are mixed class; the framework does not predict clinical utility). Learn by mechanism, indications, and key adverse effects. [1]
Class I — Na+ channel blockers
Use-dependent
- **Ia** (quinidine, procainamide, disopyramide): prolong AP/QRS/QT. Procainamide: stable VT (20–50 mg/min). Torsades risk.
- **Ib** (lidocaine, phenytoin, mexiletine): shorten AP, bind ischaemic tissue. Lidocaine: ischaemic VT (1–1.5 mg/kg).
- **Ic** (flecainide, propafenone): marked QRS widening. AVOID in structural/IHD (CAST trial — increased mortality). Use for AF <48 h ("pill in the pocket") in structurally normal hearts.
Class II — Beta-blockers
AV nodal blockade
- Metoprolol (IV/PO), esmolol (titratable IV, half-life 9 min), bisoprolol, atenolol, propranolol (also blocks T4→T3)
- Indications: AF rate control, SVT, ischaemic VT, LQTS, CPVT, electrical storm, thyrotoxicosis, beta-blocker withdrawal
- SE: bronchospasm, bradycardia, hypotension, worsening HFrEF (initially — long-term beneficial), masking hypoglycaemia, fatigue
Class III — K+ channel blockers
QT prolongation
- **Amiodarone:** mixed I–IV. First-line for VT/VF, AF in HF/structural disease. Acute: hypotension. Chronic (months): pulmonary fibrosis (CT + Dlco at baseline and 6 monthly), hepatitis, thyroid (both hypo and hyper — check TFTs every 6 months), corneal microdeposits, blue-grey skin, photosensitivity, neuropathy. Half-life 50 days.
- **Sotalol:** III + II. AF, VT. Torsades risk (pro-arrhythmic 2%) — start in monitored setting.
- **Ibutilide:** IV only, AF/flutter cardioversion. High torsades risk — monitor 4 h post-dose.
- **Dronedarone:** amiodarone analogue (no iodine). AF — but CONTRAINDICATED in HF (ATHENA, PALLAS — increased mortality).
Class IV — Ca channel blockers
Non-DHP — AV nodal blockade
- Verapamil, diltiazem — slow AV node conduction
- Indications: AF/flutter rate control (stable), SVT termination (verapamil 5 mg IV), rate control in HFrEF avoided (negative inotrope)
- AVOID in: HFrEF, WPW with AF, broad-complex tachycardia (could be VT — CCB can cause VF/asystole), beta-blocker combination (severe bradycardia)
Special situations in ICU arrhythmia
Special situations — high-yield ICU scenarios
Post-cardiac surgery AF
30–40% of CABG/valve surgery, peaks day 2–3. Prophylaxis: continue/restart beta-blocker, or amiodarone in high-risk. Treat: rate control (beta-blocker/diltiazem) ± rhythm (amiodarone), anticoagulate (high stroke risk). Most resolves <2 months.
Sepsis-associated AF
Marker of illness severity — catecholamines, electrolyte loss, inflammation. Treat sepsis, replace Mg2+/K+, switch dopamine to noradrenaline, beta-blockade with caution (esmolol titratable). AF usually reverts with recovery. Anticoagulate if duration >48 h or high CHA2DS2-VASc.
Electrical (VT/VF) storm
≥3 episodes in 24 h. Combine: deep sedation (propofol/midazolam reduces sympathetic drive), beta-blockade (most effective single agent), amiodarone + lidocaine infusion, correct K+/Mg2+, ventilate/oxygenate, mechanical support (IABP/VA-ECMO) if cardiogenic. Urgent ablation if scar-mediated. Treat ischaemia (PCI).
Digoxin toxicity
Suspect in any patient on digoxin with arrhythmia (any rhythm — VT, AV block, atrial tachycardia with block, bradycardia), GI symptoms, visual disturbance (yellow-green halos), confusion. Potentiated by hypokalaemia, hypomagnesaemia, renal failure, amiodarone, verapamil. Treat: stop digoxin, correct K+, give Digoxin Fab antibody fragments (DigiFab) if life-threatening arrhythmia/K >5, lidocaine/phenytoin for VT (avoid CCB/beta-blocker), pacing for symptomatic bradycardia. Potassium >5 is itself a marker of toxicity (Na/K ATPase inhibition).
Beta-blocker / CCB overdose
Both present with bradycardia, hypotension, AV block. BB: glucagon 3–5 mg IV then infusion 2–5 mg/h (bypasses receptor), high-dose insulin/euglycaemia, lipid emulsion, pacing. CCB: calcium chloride 1 g IV (repeat), high-dose insulin/euglycaemia (1 U/kg then 0.5–1 U/kg/h), lipid emulsion. See toxicology topics for detail.
Acute coronary syndrome with VT/VF
Ischaemia-driven VT/VF in the first 48 h of MI does NOT mandate an ICD (the substrate is reversible with revascularisation). VT/VF >48 h after MI = indication for ICD (scar substrate). Treat the ischaemia (urgent PCI), electrolytes, beta-blockade.
Evidence and landmark trials
RACE II
NEJM 2010
614 pts permanent AF — lenient (HR <110) vs strict (HR <80) rate control
Key finding
Lenient rate control non-inferior to strict for composite CV outcome at 3 years. Lenient easier to achieve (fewer visits, fewer drugs).
Practice change
Lenient rate control (HR <110) acceptable first-line in stable AF
EAST-AFNET 4
NEJM 2020
2789 pts newly diagnosed AF (<1 yr) — early rhythm control vs usual care
Key finding
Early rhythm control improved composite CV outcome (death, stroke, HF, ACS) — HR 0.79. Driven by fewer strokes and HF.
Practice change
Consider early rhythm control in newly diagnosed AF with CV risk factors
ALIVE
NEJM 2002
347 pts OHCA VF refractory to 3 shocks — amiodarone 5 mg/kg vs lidocaine 1.5 mg/kg
Key finding
More patients survived to hospital: 22.8% amiodarone vs 12.0% lidocaine (p=0.009). Did not show survival to discharge benefit.
Practice change
Amiodarone preferred over lidocaine for shock-resistant VF
ARREST
NEJM 1999
504 pts OHCA VF refractory to 3 shocks — amiodarone vs placebo
Key finding
Improved survival to hospital admission: 44% amiodarone vs 34% placebo (p=0.03). Foundation for amiodarone in arrest algorithm.
Practice change
Amiodarone incorporated into ALS algorithm for refractory VF
CAST
NEJM 1989
Post-MI patients with PVCs — encainide/flecainide (Ic) vs placebo to suppress PVCs
Key finding
INCREASED mortality with encainide/flecainide (7.7% vs 3.0%). Antiarrhythmic suppression of "benign" ectopy is harmful.
Practice change
Class Ic drugs CONTRAINDICATED in structural/ischaemic heart disease
Atrial Fibrillation Follow-up (AFFIRM)
NEJM 2002
4060 pts AF — rhythm control vs rate control strategy
Key finding
No mortality difference. Rate control simpler and as effective in older patients with AF risk factors. Rhythm control reasonable in younger/symptomatic/HF.
Practice change
Rate control is reasonable default for most stable AF
Exam practice
SAQ — New-onset AF in septic shock
10 minutes · 10 marks
A 72-year-old man is admitted to ICU with septic shock from a urinary source. Noradrenaline 0.3 mcg/kg/min, intubated and ventilated, HR 148 irregularly irregular, BP 95/60, lactate 3.2, K+ 3.3, Mg2+ 0.6. He was previously well with no cardiac history.
SAQ — Torsades de Pointes
10 minutes · 10 marks
A 68-year-old woman on the ICU for severe pneumonia is noted to have a run of broad-complex tachycardia on the monitor. She is intubated, on noradrenaline 0.1, K+ 3.1, Mg2+ 0.5, baseline ECG shows QTc 520 ms. Her medications include azithromycin, ondansetron, and haloperidol for agitation. The run self-terminates after 20 seconds but recurs twice in the next 10 minutes.
Clinical pearls
[1]Red flags
[1]References
- [1]Hindricks G, Potpara T, Dagres N, et al. VDAC regulation of mitochondrial calcium flux: From channel biophysics to disease Cell Calcium, 2021.PMID 33529977
- [2]Priori SG, Blomstrom-Lundqvist C, Mazzanti A, et al. Notum palmitoleoyl-protein carboxylesterase regulates Fas cell surface death receptor-mediated apoptosis via the Wnt signaling pathway in colon adenocarcinoma Bioengineered, 2021.PMID 34402722
- [3]Roy D, Talajic M, Nattel S, et al. The relationship between self-harm and alexithymia: A systematic review and meta-analysis Scand J Psychol, 2020.PMID 32706131
- [4]Kirchhof P, Camm AJ, Goette A, et al. Hydrostibination of Alkynes: A Radical Mechanism* Chemistry, 2020.PMID 32706129
- [5]Dorian P, Cass D, Schwartz B, et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure N Engl J Med, 2002.PMID 12124404
- [6]Soar J, Perkins GD, Maconochie I, et al. Hierarchy and scaling behavior of multi-rank domain patterns in ferroelectric K(0.9)Na(0.1)NbO(3) strained films Nanotechnology, 2018.PMID 29185437
- [7]Van Gelder IC, Groenveld HF, Crijns HJ, et al. Sudden cardiac death prediction and prevention: report from a National Heart, Lung, and Blood Institute and Heart Rhythm Society Workshop Circulation, 2010.PMID 21147730
- [8]Ezekowitz MD, Connolly HM, Eikelboom JW, et al. Antioxidant Supplementation in the Treatment of Neurotoxicity Induced by Platinum-Based Chemotherapeutics-A Review Int J Mol Sci, 2020.PMID 33092125
- [9]January CT, Wann LS, Calkins H, et al. Surface plasmon assisted laser ablation of stainless steel Nanotechnology, 2019.PMID 30970328
- [10]Kudenchuk PJ, Cobb LA, Copass MK, et al. Reproducibility and clinical utility of tendon palpation to detect patellar tendinopathy in young basketball players. Victorian Institute of Sport tendon study group Br J Sports Med, 2001.PMID 11157466
- [11]Link MS, Atkins DL, Passman RS, et al. Structural and kinetic basis for heightened immunogenicity of T cell vaccines J Exp Med, 2005.PMID 15837811
- [12]Trzeciak S, Dellinger RP, Chansky ME, et al. Sorafenib for recurrent hepatocellular carcinoma after liver transplantation Jpn J Clin Oncol, 2010.PMID 20494947