Paeds · acute-care-resuscitation-and-toxicology
Fluid bolus therapy and vasoactive support
Also known as Paediatric fluid resuscitation · Fluid bolus in children · Vasoactive infusions in paediatric shock · Inotrope and vasopressor therapy in children · Fluid-refractory shock management
A fellowship approach to fluid bolus therapy and vasoactive support in the shocked child. Give 10 to 20 mL per kilogram of isotonic crystalloid in aliquots with reassessment after each, stop for overload or no benefit, escalate to adrenaline or noradrenaline for fluid-refractory shock, and keep the first-hour fluid total as a ceiling rather than a target. The FEAST trial anchors why fluid strategy must stay population-specific.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Fluid bolus therapy and vasoactive support are the two circulatory tools that resuscitate the shocked child. A fluid bolus is a measured aliquot of isotonic crystalloid, given rapidly with the intention of restoring effective circulating volume, improving perfusion, and buying time while the cause is treated. Vasoactive support is the infusion of an catecholamine or vasopressor that restores vascular tone, cardiac contractility, or both, when fluid alone has not reversed shock. Neither is a protocol you drive toward a fixed endpoint; each is a treatment you give, measure, and either continue or stop based on whether the child improved. [4] [2]
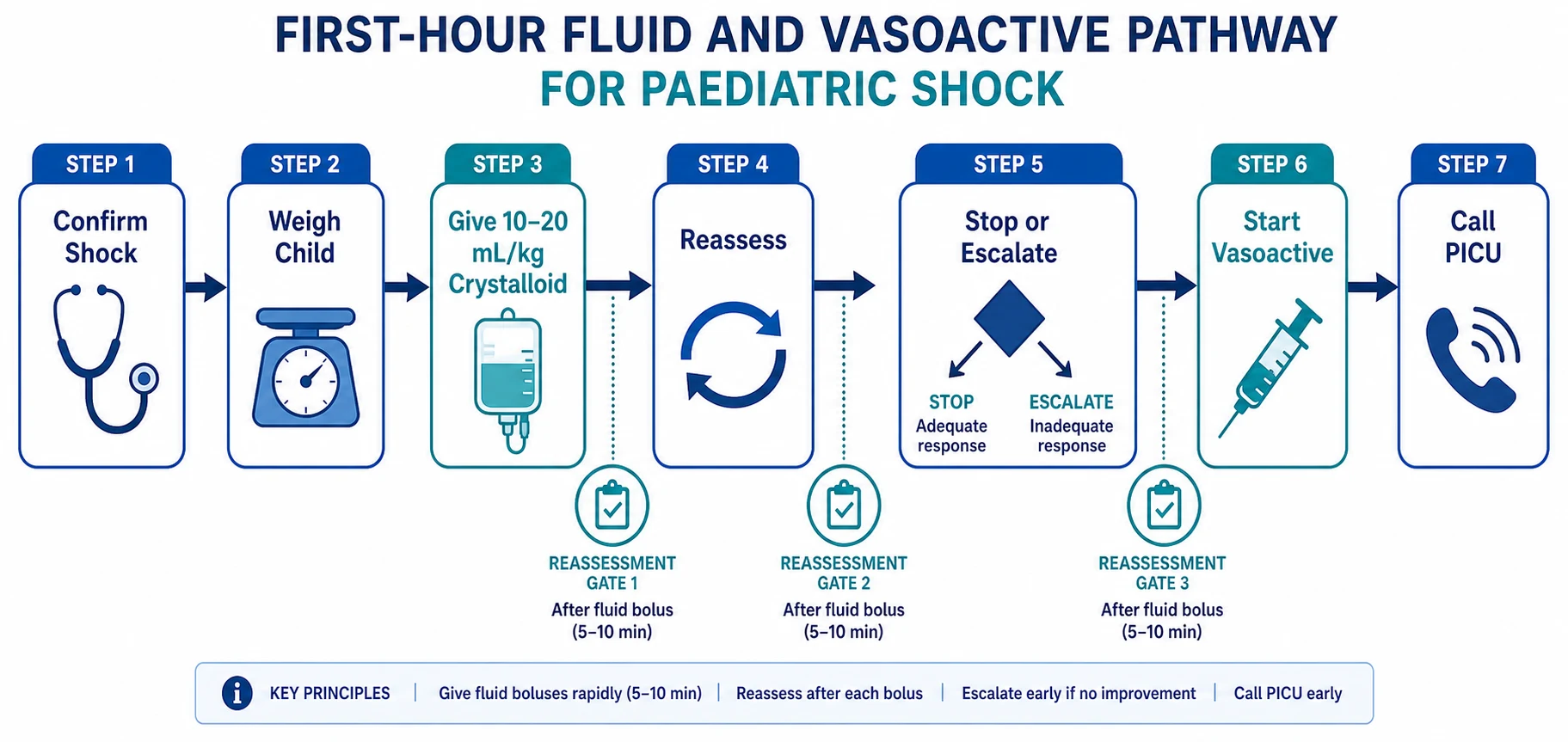
The disciplined sequence is assess, give an aliquot, reassess, repeat or stop, and escalate to vasoactive support when shock is fluid-refractory. This is a closed loop, not a checklist. Before every bolus you state the improvement you expect in heart rate, perfusion, interaction, urine output or lactate. After every bolus you check whether that improvement happened. If it did not, you do not blindly repeat the same treatment — you reconsider the shock type, the fluid volume already given, and whether it is time to start a vasoactive infusion. [4] [9]
The fluid-and-vasoactive loop
Confirm shock and set a goal
Diagnose shock from the whole circulation assessment, decide what improvement you expect from fluid, and state it before you give it.
Give 10 to 20 mL per kilogram
Administer isotonic crystalloid over 5 to 20 minutes, not as a slow drip, and not as a blind push without reassessment.
Reassess the whole child
After each aliquot, check heart rate, pulses, skin colour and temperature, capillary refill, mental state, urine output, lactate and respiratory status.
Repeat or stop
If shock persists and there is no overload, repeat up to the ceiling. Stop immediately for no benefit, worsening, or any sign of fluid overload.
Escalate to vasoactive
When shock is fluid-refractory or overload is developing, start adrenaline or noradrenaline and call PICU or retrieval.
This topic focuses on the fluid and vasoactive tools themselves. It complements the shock classification, septic shock and ABCDE assessment pages, which cover recognition, pathophysiology and cause-specific pathways. Here the clinical question is narrower and more dangerous: once you have decided to give fluid or start an infusion, exactly what do you give, how much, how fast, when do you stop, and when do you switch to vasoactive support? [4]
Classification
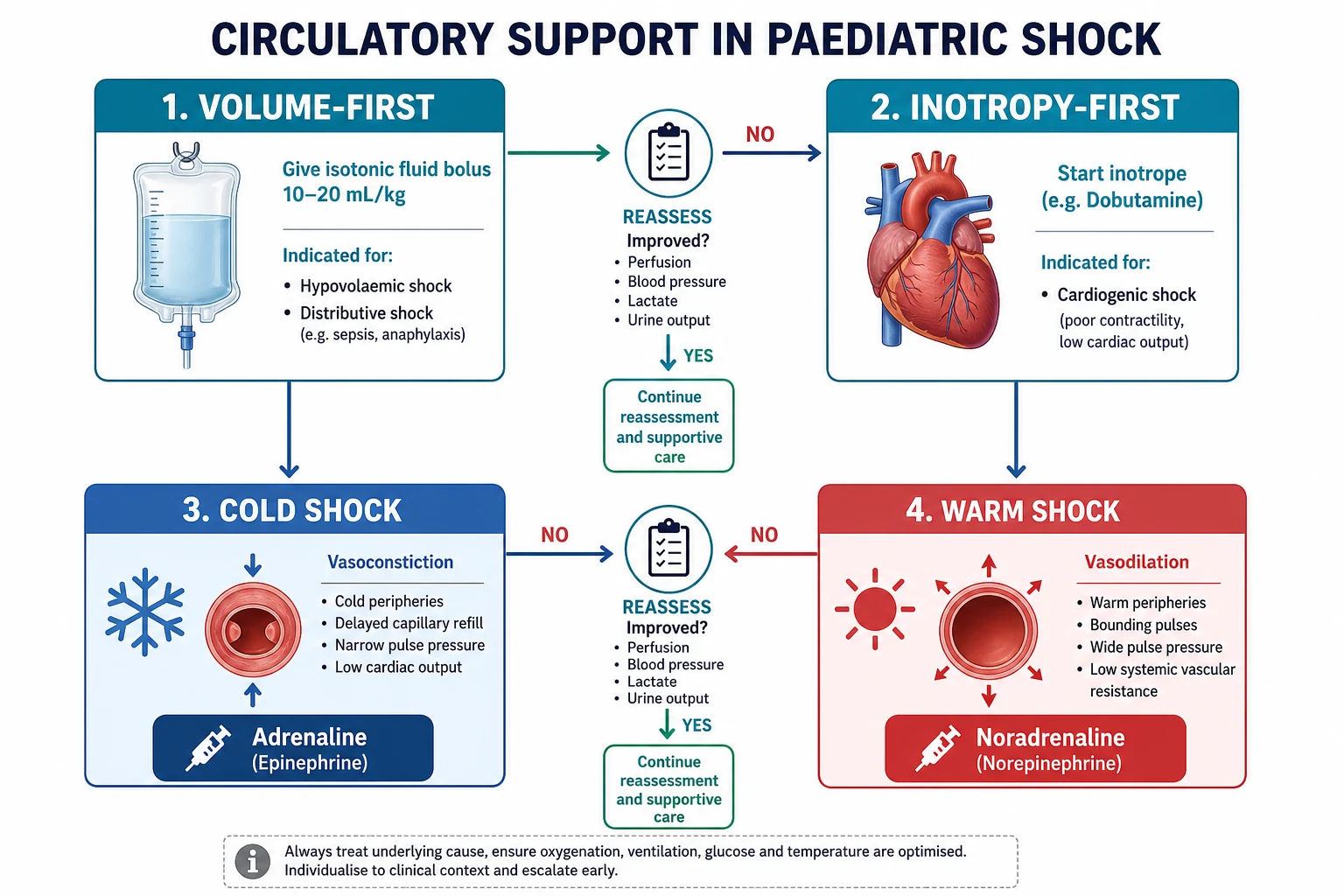
Fluid and vasoactive therapy maps onto the shock type and the physiological target. The two decisions that shape treatment are whether the child needs volume first or inotropy first, and whether the shock is cold or warm once fluid has been optimised. [4]
| Shock type | Fluid strategy | Vasoactive first agent | Key caution |
|---|---|---|---|
| Hypovolaemic (dehydration, haemorrhage) | 10 to 20 mL per kilogram aliquots up to the ceiling | Rarely needed if volume deficit corrected | Control bleeding first in haemorrhagic shock |
| Distributive (septic, anaphylactic) | 10 to 20 mL per kilogram aliquots up to the ceiling | Adrenaline if cold, noradrenaline if warm | Do not drive toward a fixed volume; watch for overload |
| Cardiogenic | 5 to 10 mL per kilogram aliquots, cautious | Adrenaline for low output; milrinone if not acutely unstable | Large boluses can precipitate pulmonary oedema |
| Obstructive (tamponade, pneumothorax) | Small cautious aliquots while treating the obstruction | Noradrenaline as bridge to definitive therapy | Fluid does not fix the obstruction; treat the cause |
Cold shock versus warm shock
The distinction between cold and warm shock decides the first vasoactive agent once fluids have been optimised. Cold shock is the more common pattern in children: the child is vasoconstricted with cold clammy skin, weak thready pulses, prolonged capillary refill, oliguria and altered consciousness. Cardiac output is low and systemic vascular resistance is high. The first-line agent is adrenaline, which increases contractility and vascular tone. [3] [4]
Warm shock is vasodilatory: the child has warm dry skin, bounding pulses, flash capillary refill and a wide pulse pressure. Cardiac output may be high but systemic vascular resistance is low, so perfusion is ineffective despite the flushed appearance. The first-line agent is noradrenaline, which restores vascular tone. Children can move between these patterns during resuscitation, so reassessment after each vasoactive change is essential. [3] [8]
Cold shock
Low output, vasoconstricted
- Cold clammy skin, weak pulses, prolonged capillary refill
- Oliguria, altered consciousness
- Narrow pulse pressure
- First-line vasoactive: adrenaline 0.05 to 0.5 micrograms per kilogram per minute
Warm shock
Vasodilatory, low resistance
- Warm dry skin, bounding pulses, flash capillary refill
- Wide pulse pressure
- May look deceptively well perfused
- First-line vasoactive: noradrenaline 0.05 to 0.5 micrograms per kilogram per minute
Epidemiology & Risk Factors
Fluid bolus therapy is one of the most common acute interventions in paediatric emergency and critical care, yet the evidence base for how much fluid, in which population, and with what rescue capability, remains contested. The risk of harm from fluid is not theoretical — it is the lesson of the FEAST trial and the accumulated evidence on fluid accumulation. [1] [10]
Children most likely to be harmed by a fixed-volume fluid strategy share features: young age, septic or distributive shock, pre-existing cardiac or renal dysfunction, a setting without timely access to intensive care or vasoactive agents, and any sign of evolving fluid overload. The risk of fluid harm is amplified when reassessment is incomplete, when boluses are repeated reflexively without measuring the response, or when the child has a cardiogenic or obstructive component that volume alone cannot fix. [7] [10]
Child at risk of fluid harm
- Young infant with limited cardiovascular reserve
- Septic shock with capillary leak and evolving overload
- Pre-existing cardiac, renal or hepatic disease
- Duct-dependent congenital heart disease
- Technology-dependent child with altered baseline
System at risk of fluid harm
- No timely access to PICU or vasoactive agents
- Rural or remote setting with delayed retrieval
- No reliable weight or fluid-balance tracking
- Single operator without reassessment discipline
- Protocol-driven fluid without individual assessment
Child likely to benefit from fluid
- Clear hypovolaemia from dehydration or haemorrhage
- Distributive shock with signs of poor perfusion
- Available intensive care and vasoactive rescue
- Structured reassessment after each aliquot
- Early escalation when response is inadequate
Pathophysiology
To understand why fluid and vasoactive therapy work, and why both can harm, you need to trace what happens to circulating volume, cardiac output and vascular tone in shock. Shock is the state where oxygen and substrate delivery to tissues fails to meet metabolic demand. The body compensates first by raising heart rate, then by redistributing flow to vital organs through vasoconstriction. These mechanisms preserve blood pressure and cerebral perfusion for a while, but they consume reserve and mask the severity of the deficit. [4] [9]
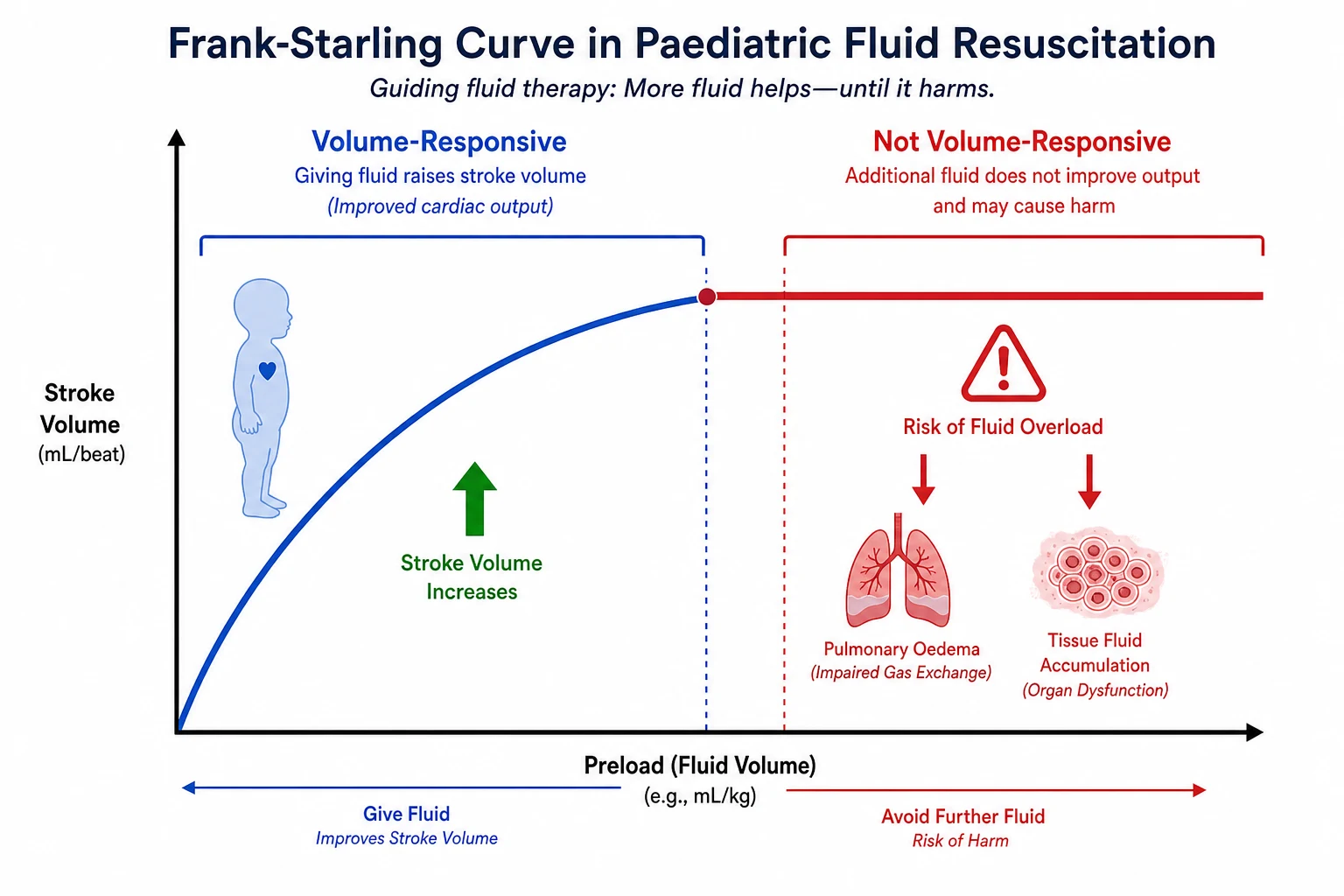
A fluid bolus works by expanding the intravascular volume, increasing venous return (preload), and thereby increasing stroke volume through the Frank-Starling mechanism. In a volume-responsive child, this raises cardiac output, improves tissue perfusion, and reduces the compensatory tachycardia and vasoconstriction. In a child who is not volume-responsive — because the problem is pump failure (cardiogenic), obstruction, or already exhausted reserve — additional fluid does not improve stroke volume. Instead, it accumulates in the interstitial space, increases the risk of pulmonary oedema, and worsens outcome. [4] [10]
Vasoactive agents work at different points in this physiology. Adrenaline stimulates beta-1 receptors to increase heart rate and contractility, and alpha-1 receptors to increase vascular tone. Noradrenaline is predominantly an alpha-1 agonist that restores vascular tone in vasodilatory shock. Dopamine acts on dopamine, beta-1 and alpha-1 receptors in a dose-dependent manner but was downgraded by the Surviving Sepsis Campaign 2020 because adrenaline and noradrenaline showed better outcomes. Dobutamine is a selective beta-1 agonist that increases contractility with less tachycardia, useful for low cardiac output when blood pressure is maintained. [3] [8]
The transition from fluid to vasoactive support is the critical decision point. Fluid-refractory shock is defined as persistent shock after 40 to 60 mL per kilogram of crystalloid in the first hour. At this point, continuing to give fluid without a vasoactive infusion risks driving the child further along the flat portion of the Starling curve. The Surviving Sepsis Campaign 2020 and 2026 guidelines both direct early initiation of vasoactive support within the first hour for children with fluid-refractory septic shock, ideally through central access but through intraosseous access if central is not immediately available. [2] [3]
[3]Clinical Presentation
The child who needs fluid bolus therapy presents with signs of inadequate tissue perfusion. Before giving any fluid, integrate the whole circulation assessment: heart rate and pulse quality at central and peripheral sites, skin colour and temperature, capillary refill with the technique stated, blood pressure, mental state and urine output. Do not diagnose shock from any single sign, and do not exclude it because blood pressure is normal — children maintain blood pressure until late. [4] [5]
What to look for before each bolus
Before the first bolus, establish the baseline you will measure against. State the heart rate, capillary refill time (with site, compression pressure and ambient temperature), pulse quality, skin temperature, mental state and, if available, blood pressure, lactate and urine output. These become the reference points for every reassessment. If you cannot state what you expect to change, you are not ready to give the bolus. [4]
After each bolus, look for the expected improvement: heart rate trending toward the normal range for age, stronger central and peripheral pulses, shorter capillary refill, warmer and drier skin, improved interaction or consciousness, improving lactate and evidence of urine output. If the child improved, decide whether another aliquot is warranted or whether you have reached the point to hold fluids and monitor. [9]
Signs that mean stop
Certain findings mean you must stop giving fluid immediately, regardless of how many boluses you have given. New basal crackles on auscultation, increasing hepatomegaly, a gallop rhythm, rising work of breathing or oxygen requirement, and any deterioration in the mental state after a bolus are signs of fluid overload or a failing pump. These are not relative contraindications — they are hard stops. At this point the child needs a vasoactive infusion and critical care support, not more crystalloid. [2] [10]
| Sign after bolus | What it means | What to do |
|---|---|---|
| Heart rate falling toward normal range | Improving perfusion and reduced compensatory demand | Continue reassessment; consider whether another aliquot is needed |
| Shorter capillary refill, warmer skin | Improved peripheral perfusion | Continue if shock persists and no overload; hold if resolved |
| No change in any perfusion sign | Fluid-refractory or non-volume-responsive shock | Stop blind repetition; consider vasoactive infusion; call PICU |
| New crackles, hepatomegaly or gallop | Fluid overload or developing pulmonary oedema | Stop fluids immediately; start vasoactive; escalate to critical care |
| Worsening respiratory distress | Pulmonary fluid accumulation or cardiac decompensation | Stop fluids; support breathing; urgent critical care review |
| Falling blood pressure despite boluses | Decompensating shock; fluid alone is insufficient | Start vasoactive infusion now; call PICU or retrieval |
Differential Diagnosis
The differential for a child needing fluid and vasoactive support is the differential of shock itself, classified by mechanism. The mechanism determines whether volume is the primary tool, a secondary tool, or potentially harmful. This is why identifying shock type is inseparable from the fluid strategy. [4] [9]
HIDCO
The critical distinction at the bedside is whether the child is volume-responsive. Hypovolaemic and early distributive shock are typically volume-responsive: each bolus produces a measurable improvement. Cardiogenic and obstructive shock are less volume-responsive: small aliquots may help marginally, but large volumes risk causing harm. Mixed physiology is common, especially in septic shock with myocardial depression, where the child has elements of both distributive and cardiogenic shock. [9] [8]
Volume-responsive
- Hypovolaemic: dehydration, haemorrhage, DKA
- Early distributive: septic and anaphylactic shock
- Measurable improvement after each bolus
- Heart rate falls, perfusion improves, lactate trends down
Cautious volume
- Cardiogenic: myocarditis, cardiomyopathy, arrhythmia
- Obstructive: tamponade, tension pneumothorax
- Give 5 to 10 mL per kilogram aliquots
- Early vasoactive support; avoid driving toward a volume target
Not volume-responsive
- Late distributive shock with capillary leak and overload
- Established myocardial failure
- Further fluid does not improve output and causes harm
- Start vasoactive support; call critical care immediately
Clinical & Bedside Assessment
Assessment is continuous and structured around the same loop: measure, give an aliquot, reassess, decide. The purpose is not to complete a form but to judge whether the treatment is working in real time. Every team member should be able to state the current heart rate, capillary refill, pulse quality and mental state at any moment. [4] [5]
Weighing the child accurately
Every fluid bolus and every vasoactive dose is weight-based, so an accurate weight is essential from the first minute. Use a measured weight if the child can be safely weighed immediately. Otherwise announce and document one temporary working weight in kilograms, including its source and method. Published weight-estimation methods vary in accuracy and are not interchangeable; always confirm with the local paediatric cognitive aid and re-weigh at the first safe opportunity. A weight error propagates through every subsequent calculation. [11]
Vascular access
Gain vascular access early without allowing repeated failed attempts to delay resuscitation. A large-bore peripheral intravenous cannula is sufficient for fluid boluses. For vasoactive infusions, central venous access is preferred, but intraosseous access is an acceptable and rapid alternative when central access is not immediately available. Do not delay the first vasoactive dose to establish central access in a child with fluid-refractory shock. [5] [8]
Monitoring during resuscitation
Continuous electrocardiographic monitoring, pulse oximetry, non-invasive blood pressure and capnography form the minimum monitoring set for a child receiving fluid and vasoactive therapy. In a critically ill child, add an arterial line for beat-to-beat blood pressure and a central venous line for central venous pressure and mixed venous saturation where available. Point-of-care blood gas, lactate, electrolytes and glucose should be checked at baseline and repeated after each significant intervention. [4] [9]
[4]Investigations
Investigations during fluid and vasoactive therapy serve three purposes: to quantify the severity of shock, to guide the type and dose of support, and to detect complications of treatment. They never replace the clinical reassessment loop. [9]
Bedside and immediate
- Point-of-care blood gas and lactate for ventilation, perfusion and metabolic state
- Bedside glucose for every shocked child
- Electrolytes including sodium, potassium, calcium and magnesium
- Blood count and coagulation for bleeding or DIC
Guiding support
- Central venous oxygen saturation if a line is placed
- Arterial blood gas for acid-base and ventilation
- Echocardiography to assess cardiac function and guide inotrope choice
- Serum cortisol if adrenal insufficiency is suspected
Detecting complications
- Repeat electrolytes for iatrogenic disturbance
- Blood gas for worsening acidosis despite resuscitation
- Chest imaging for pulmonary oedema
- Renal function and urine output for fluid overload and AKI
Interpret the results as trend and physiology. A falling lactate suggests improving perfusion; a persistently elevated or rising lactate warns that resuscitation is incomplete or the cause is worsening. A widening base deficit carries the same message. An arterial or venous pH reflects both respiratory and metabolic contributions — always read the gas with the clinical picture and the capnography. Central venous oxygen saturation below 70 per cent suggests inadequate oxygen delivery. None of these numbers, in isolation, should end your clinical reassessment. [4] [8]
[4]Management — Resuscitation
The resuscitation phase covers the first hour of circulatory support. The goal is to restore effective perfusion as quickly as possible while avoiding the harms of excessive fluid. Call for senior, PICU or retrieval help at the outset if the child may need support unavailable locally — do not wait until local options are exhausted. [2] [5]
Fluid bolus: what, how much, how fast
Give isotonic crystalloid — 0.9 per cent sodium chloride or a balanced crystalloid such as Hartmann solution (compound sodium lactate) or Plasma-Lyte. The dose is 10 to 20 mL per kilogram per aliquot, given over 5 to 20 minutes using a push-pull technique, rapid infuser or pressure bag, not as a slow gravity drip. After each aliquot, perform the full reassessment described above. The Surviving Sepsis Campaign 2026 children guideline supports up to 40 to 60 mL per kilogram in the first hour for septic shock, with careful reassessment after each bolus and explicit attention to fluid balance. [2] [3]
When to stop fluids
Stop giving fluid boluses when any of the following occurs: shock has resolved and perfusion is adequate; there is no improvement after two or three aliquots (fluid-refractory shock); there is any sign of fluid overload (new crackles, hepatomegaly, gallop, rising respiratory distress); or the first-hour ceiling of 40 to 60 mL per kilogram has been reached. Stopping is not failure — it is the decision that converts a volume strategy into a vasoactive strategy. [2] [10]
When to stop fluid and start vasoactive
Shock resolved
Perfusion is adequate, heart rate is normalising, interaction and urine output are improving. Hold fluids, monitor, and treat the cause.
No improvement after boluses
Two or three aliquots have produced no measurable improvement. Stop blind repetition. This is fluid-refractory shock.
Signs of overload
New crackles, hepatomegaly, gallop or worsening respiratory status. Stop fluids immediately and start a vasoactive infusion.
Ceiling reached
The child has received 40 to 60 mL per kilogram in the first hour and shock persists. Do not exceed this without critical care assessment.
Vasoactive agents: which, when, how much
Start a vasoactive infusion when shock is fluid-refractory or when signs of overload develop before the ceiling is reached. The Surviving Sepsis Campaign 2020 guideline recommends using either adrenaline or noradrenaline rather than dopamine as the first-line vasoactive agent for children with septic shock. Choose based on the shock phenotype: adrenaline for cold shock, noradrenaline for warm shock. [3] [8]
Adrenaline (epinephrine) infusion
Dose
0.05 to 0.5 micrograms per kilogram per minute; titrate to clinical response (per local protocol, some centres titrate up to 1.0 microgram per kilogram per minute in refractory shock)
Noradrenaline (norepinephrine) infusion
Dose
0.05 to 0.5 micrograms per kilogram per minute; titrate to clinical response
Dopamine infusion
Dose
5 to 10 micrograms per kilogram per minute; titrate to clinical response
Access for vasoactive infusions
Central venous access is the preferred route for vasoactive infusions because it reduces the risk of extravasation injury and allows reliable drug delivery. However, intraosseous access is an acceptable and rapid alternative when central access is not immediately available in a child with fluid-refractory shock. Do not delay the first vasoactive dose to place a central line — start through IO and convert when safe. If extravasation occurs, stop the infusion immediately, aspirate if possible, and follow the local antidote and review pathway. [5] [8]
Management — Definitive & Stepwise
After the first hour, the strategy shifts from rapid resuscitation to titrated, monitored support in a critical care environment. The principles remain the same: assess, treat, reassess, and adjust based on the child's trajectory, not a fixed protocol. [2] [9]
From first hour to ongoing support
Establish the response
After the first hour, state whether shock has resolved, improved but persists, or is refractory. This sets the intensity of ongoing support.
Titrate vasoactive to clinical goals
Adjust the infusion dose to achieve target perfusion: normal heart rate for age, warm extremities, capillary refill under 2 seconds, adequate urine output, and improving lactate.
Manage fluid balance
Track all input and output meticulously. Once shock is resolving, move from bolus therapy to maintenance and replacement fluids, and consider diuretics or renal replacement therapy for established fluid overload.
Treat the cause
Give antimicrobials within the first hour for septic shock. Control bleeding in haemorrhagic shock. Treat arrhythmia, myocarditis or pericardial effusion in cardiogenic shock. Resolve obstruction in obstructive shock.
De-escalate when safe
Reduce vasoactive support as perfusion stabilises and the cause is treated. Wean slowly with continuous monitoring to detect any rebound.
Crystalloid choice
The choice between 0.9 per cent sodium chloride and balanced crystalloids (Hartmann solution or Plasma-Lyte) remains an area of active study. The Surviving Sepsis Campaign 2026 guideline supports either buffered or non-buffered crystalloid, while noting that balanced solutions may reduce the risk of hyperchloraemic metabolic acidosis and may be associated with better outcomes in some studies. In practice, either is acceptable for the initial bolus; local protocol and availability usually determine the choice. Avoid hypotonic fluids (such as 5 per cent dextrose or 0.45 per cent sodium chloride) for bolus therapy, because they do not stay in the intravascular space and can cause hyponatraemia. [2] [7]
Albumin and colloid
Albumin is not routinely recommended over crystalloid for initial fluid resuscitation in paediatric shock. The Surviving Sepsis Campaign guidelines find no consistent survival advantage for albumin over crystalloid in the first hour. Albumin may be considered for specific situations such as severe hypoalbuminaemia or where crystalloid alone has been inadequate, but it is not the default first bolus agent. The FEAST trial compared both saline and albumin bolus against no bolus and found increased mortality with both, reinforcing that the harm was from the bolus strategy itself in that population, not from one fluid type over another. [1] [3]
Maintenance fluid after resuscitation
Once shock has resolved and perfusion is stable, transition from bolus therapy to maintenance and replacement fluids. Use isotonic maintenance fluid to avoid hyponatraemia, particularly in the acute setting where antidiuretic hormone levels are often elevated. Monitor sodium closely, and replace ongoing losses (drainage, fever, insensible losses) separately from the maintenance prescription. Over-resuscitation with maintenance fluid is a common source of iatrogenic fluid overload in the days following the acute presentation. [9] [10]
| Phase | Fluid goal | Vasoactive goal | Monitoring |
|---|---|---|---|
| First hour (resuscitation) | 10 to 20 mL per kilogram aliquots up to 40 to 60 mL per kilogram ceiling | Start adrenaline or noradrenaline if fluid-refractory | Continuous heart rate, blood pressure, capillary refill, lactate after each aliquot |
| Hours 2 to 6 (stabilisation) | Reduce bolus frequency; begin tracking fluid balance | Titrate infusion dose to target perfusion markers | Arterial line if possible; central venous saturation; urine output |
| Day 1 to 3 (ongoing care) | Maintenance isotonic fluid; replace losses separately | Wean as perfusion stabilises and cause is treated | Daily weights, strict input-output, electrolytes and renal function |
| Recovery | Return to age-appropriate maintenance | Discontinue infusion when stable off support | Monitor for rebound and fluid redistribution |
Specific Subtypes & Scenarios
The fluid and vasoactive strategy adapts to the shock type, the child's age and baseline, and the setting. In each scenario, the reassessment loop stays the same, but the starting fluid volume, the first vasoactive agent, and the escalation threshold change. [4] [9]
Septic shock
- 10 to 20 mL per kilogram aliquots up to 40 to 60 mL per kilogram ceiling
- Adrenaline for cold shock, noradrenaline for warm shock
- Antimicrobials within the first hour
- Watch for myocardial depression and mixed physiology
Hypovolaemic and haemorrhagic
- 10 to 20 mL per kilogram aliquots of crystalloid
- Control bleeding early; use blood products in haemorrhagic shock
- Rarely needs vasoactive if volume deficit corrected
- Reassess for ongoing loss after each aliquot
Cardiogenic shock
- 5 to 10 mL per kilogram aliquots only
- Early adrenaline for low cardiac output
- Avoid driving toward a volume target
- Echocardiography to guide inotrope choice
Obstructive shock
- Small cautious aliquots as a bridge
- Noradrenaline to maintain perfusion while treating the cause
- Treat tamponade or pneumothorax definitively
- Fluid does not fix the obstruction
Anaphylactic shock
- Intramuscular adrenaline is the first treatment, not fluid
- Give 10 to 20 mL per kilogram crystalloid for persistent hypotension
- Noradrenaline infusion for refractory vasodilatory shock
- Identify and remove the trigger
DKA and shock
- Give 10 mL per kilogram aliquot only if in shock
- Avoid aggressive fluid resuscitation; gradual rehydration over 24 to 48 hours
- Risk of cerebral oedema with rapid fluid shifts
- Insulin and potassium management are co-priorities
Burns resuscitation
- Uses formula-based resuscitation, not standard bolus therapy
- Parkland formula: 3 to 4 mL per kilogram per per cent TBSB over 24 hours
- Titrate to urine output of 0.5 to 1 mL per kilogram per hour
- See the dedicated burns topic for the complete algorithm
Neonate
- 10 mL per kilogram aliquots of crystalloid or blood
- Duct-dependent lesions: prostaglandin E1, avoid excessive fluid
- Early volume and inotrope support for neonatal septic shock
- Use Newborn Life Support rather than older-child PALS at birth
Duct-dependent congenital heart disease
A child with a duct-dependent lesion who presents in shock needs prostaglandin E1 (alprostadil) to maintain ductal patency, not large volumes of fluid. Give cautious aliquots of 5 to 10 mL per kilogram if hypovolaemic, start an adrenaline infusion for low cardiac output if needed, and arrange urgent cardiology and PICU input. Driving toward a 40 to 60 mL per kilogram ceiling in this child risks causing harm. [4] [9]
Resource-limited settings
The FEAST trial fundamentally changed how fluid strategy is applied in resource-limited settings. In African children with severe febrile illness and impaired perfusion, bolus fluid with either saline or albumin increased 48-hour mortality compared with no bolus. The critical lesson is not that bolus fluid is universally harmful, but that a fluid algorithm cannot be transplanted across populations, shock types and rescue resources without considering what happens when the child does not improve. In a setting without access to intensive care or vasoactive agents, give fluids cautiously, reassess rigorously, and call for retrieval early. [1] [1]
Complications & Pitfalls
The complications of fluid and vasoactive therapy fall into two groups: those caused by giving too much fluid, and those caused by delaying vasoactive support. Both are preventable through disciplined reassessment and early escalation. [10] [9]
| Complication | Cause | Prevention |
|---|---|---|
| Pulmonary oedema | Excessive or repeated fluid boluses beyond volume responsiveness | Stop at signs of overload; track fluid balance; use vasoactive earlier |
| Fluid accumulation and worse outcome | Driving toward a volume target rather than treating the child | Treat the ceiling as a maximum, not a goal; reassess after each aliquot |
| Delay in starting vasoactive support | Waiting for all fluid options to fail before escalating | Start adrenaline or noradrenaline at fluid-refractory shock within the first hour |
| Hyponatraemia | Hypotonic maintenance fluid in acute illness | Use isotonic maintenance fluid; monitor sodium closely |
| Extravasation injury | Vasoactive agent through fragile peripheral access | Use central or IO access; monitor infusion site; act immediately on extravasation |
| Iatrogenic hyperglycaemia | Adrenaline-induced glycogenolysis | Monitor glucose; treat per local protocol |
| Electrolyte disturbance | Large-volume crystalloid dilution | Check electrolytes after each major fluid intervention |
The systematic review by Alobaidi and colleagues found a consistent association between a positive fluid balance and worse outcomes in critically ill children, including increased mortality and longer duration of mechanical ventilation. This does not prove causation, but it reinforces the principle that fluid accumulation is a signal of harm, not merely an incidental finding. Track fluid balance from the first bolus, and treat a rising positive balance as a reason to review the strategy, not to continue the same treatment. [10]
[2] [3] [10]Prognosis & Disposition
The outcome of fluid and vasoactive therapy depends on early recognition, the correct shock type identification, prompt and measured fluid resuscitation, timely escalation to vasoactive support, and definitive treatment of the cause. Children who receive appropriate early fluid with rigorous reassessment and early vasoactive support for fluid-refractory shock have better outcomes than those who receive delayed or unmonitored treatment. [2] [9]
Critical care or retrieval
- Fluid-refractory shock needing ongoing vasoactive support
- Signs of fluid overload or worsening despite treatment
- Need for advanced monitoring or organ support unavailable locally
- Uncertain trajectory requiring specialist assessment
High dependency
- Shock resolving but needs close monitoring
- Recently weaned from vasoactive support
- Ongoing fluid balance concerns
- Pending results that may change management
Ward
- Shock resolved, stable perfusion
- No ongoing vasoactive requirement
- Maintaining adequate urine output
- Cause identified and being treated
Disposition also depends on the capability of the receiving service. A child in a rural hospital who needs vasoactive support must be retrieved to a PICU; waiting for all local options to fail before calling retrieval is the most dangerous delay. Discuss the child early with the retrieval service, agree the support to continue during transport, and prepare a contingency plan for deterioration during transfer. [5] [4]
Special Populations
Fluid and vasoactive strategy adapts to the child's baseline physiology, but the standard for recognising and treating shock does not change. The adaptations below change what you give and how fast, not whether you treat. [9] [4]
| Population | Adaptation | Boundary |
|---|---|---|
| Neonate | 10 mL per kilogram aliquots; early inotrope for neonatal septic shock; prostaglandin for duct-dependent lesions | Use Newborn Life Support at birth; state the local NLS to PLS boundary |
| Congenital heart disease | Cautious 5 to 10 mL per kilogram aliquots; individual saturation baseline; early cardiology input | Do not apply a universal oxygen or fluid target |
| Chronic kidney disease or AKI | Cautious aliquots; meticulous fluid balance; early nephrology input; consider renal replacement therapy for overload | Standard 10 to 20 mL per kilogram aliquots may precipitate overload |
| Technology-dependent child | Establish personal baseline; assess the child and the device in parallel; use the personal emergency plan | A chronically abnormal observation is not automatically safe |
| Immunocompromised | Absence of fever does not exclude septic shock; sample and escalate on context | Do not delay time-critical treatment for complete sampling |
| Malnourished child | Cautious fluid; WHO recommends slower resuscitation in severe acute malnutrition; monitor for heart failure | Standard bolus volumes may overload a compromised myocardium |
In malnutrition specifically, the World Health Organization recommends a more cautious approach to fluid resuscitation, because the malnourished myocardium has limited reserve and is vulnerable to fluid overload. Give half the standard bolus volume, give it more slowly, and monitor closely for signs of heart failure. This is the same lesson that FEAST teaches in a different population: the fluid strategy must fit the child and the available rescue. [1] [9]
Evidence, Guidelines & Regional Differences
What the evidence can and cannot support
The strongest evidence in paediatric fluid and vasoactive therapy comes from two landmark sources. The FEAST trial remains the defining study on the risks of fluid bolus in resource-limited settings. The Surviving Sepsis Campaign guidelines, updated in 2020 and again in 2026, provide the current international recommendations for fluid and vasoactive support in paediatric septic shock. [1] [2]
FEAST
New England Journal of Medicine
Randomised controlled trial of fluid bolus (saline or albumin) versus no bolus in African children with severe febrile illness and impaired perfusion
Key finding
Bolus fluid increased 48-hour mortality compared with no bolus (10.6 per cent saline and 10.5 per cent albumin versus 6.3 per cent control).
Practice change
Fluid strategy must stay specific to the population, shock type and available rescue resources. Do not transplant a fluid algorithm from one setting to another without considering what happens when the child does not improve.
The Surviving Sepsis Campaign 2026 children guideline continues to support up to 40 to 60 mL per kilogram of crystalloid in the first hour for septic shock, with careful reassessment after each bolus, early initiation of vasoactive support for fluid-refractory shock, and explicit attention to fluid balance and the risk of fluid accumulation. The choice of adrenaline or noradrenaline as first-line over dopamine, established in the 2020 guideline, remains in 2026. [2] [3]
The systematic review by Sankar and colleagues examined fluid resuscitation in children with severe infection and septic shock and highlighted the ongoing uncertainty about optimal fluid volumes and the need for individualised, reassessment-driven approaches. The Alobaidi meta-analysis found a consistent association between positive fluid balance and worse outcomes, reinforcing the harm of excessive fluid accumulation without proving that fluid is the sole cause. [7] [10]
Jurisdictional implementation
Australia and Aotearoa New Zealand: ANZCOR Guideline 12.2 provides the 2026 regional paediatric advanced life support framework. The Royal Children's Hospital Melbourne shock guideline and the inotropes and vasopressors guideline support local implementation with specific infusion concentrations and dosing tables. Retrieval systems and vasoactive agent availability vary by state, territory and service.
Global and low-resource settings: WHO ETAT adapts emergency triage, assessment and treatment for low-resource hospitals, with a more cautious fluid approach that reflects the FEAST evidence. The population-specific fluid strategy and slower resuscitation must stay attached to that context.
Exam Pearls
Fluid facts
- 10 to 20 mL per kilogram of isotonic crystalloid per aliquot over 5 to 20 minutes
- Up to 40 to 60 mL per kilogram in the first hour — a ceiling, not a target
- 0.9 per cent sodium chloride or balanced crystalloid (Hartmann or Plasma-Lyte)
- Reassess after every bolus; stop for overload or no benefit
Vasoactive facts
- Fluid-refractory shock: persistent shock after 40 to 60 mL per kilogram
- First-line: adrenaline (cold shock) or noradrenaline (warm shock) — NOT dopamine
- Adrenaline 0.05 to 0.5 micrograms per kilogram per minute
- Noradrenaline 0.05 to 0.5 micrograms per kilogram per minute
- Central access preferred; IO acceptable if central not available
FEAST
- Bolus fluid increased mortality in African children with severe febrile illness
- Both saline and albumin bolus caused harm compared with no bolus
- Lesson: do not transplant fluid algorithms across populations and resources
- In well-resourced settings with PICU access, up-front boluses remain standard with rigorous reassessment
Pitfalls
- No driving toward a fixed volume
- No blind repetition without reassessment
- No dopamine as first-line when adrenaline or noradrenaline available
- No hypotonic fluid as bolus
- No delay in retrieval or vasoactive initiation
Shock phenotype
- Cold shock: adrenaline — cold skin, weak pulses, prolonged capillary refill
- Warm shock: noradrenaline — warm skin, bounding pulses, flash capillary refill
- Mixed physiology is common in septic shock with myocardial depression
“Confirm shock and weigh the child → give 10 to 20 mL per kilogram aliquots with reassessment after each → stop for overload or no benefit → start adrenaline or noradrenaline at fluid-refractory shock → call PICU or retrieval in parallel → treat the cause and de-escalate when safe.”
Viva: when do you stop giving fluid and start a vasoactive infusion?
I stop fluid and start a vasoactive infusion in three situations. First, if there is no improvement in perfusion after two or three boluses — this is fluid-refractory shock. Second, if there is any sign of fluid overload: new crackles, hepatomegaly, gallop rhythm, or worsening respiratory distress. Third, if the first-hour ceiling of 40 to 60 mL per kilogram has been reached and shock persists. I choose adrenaline for cold shock and noradrenaline for warm shock, both starting at 0.05 to 0.5 micrograms per kilogram per minute. I do not delay the first dose to place central access — IO is acceptable. I call PICU or retrieval in parallel.
Viva: explain the FEAST trial and what it changed
FEAST was a randomised controlled trial in African children with severe febrile illness and impaired perfusion. It compared bolus fluid (saline or albumin) against no bolus and was stopped early because bolus fluid increased 48-hour mortality. Both saline and albumin caused harm compared with no bolus. The correct lesson is not that bolus fluid is universally harmful, but that a fluid algorithm cannot be transplanted across populations, shock types and rescue resources. In a well-resourced setting with PICU access, I still give up-front boluses for septic shock, but I reassess rigorously after each, stop early for overload or no benefit, and escalate to vasoactive support within the first hour rather than driving toward a fixed volume.
Structured oral: a child in septic shock who is not improving after three boluses
I confirm that this is fluid-refractory shock: three boluses of 10 to 20 mL per kilogram each, totalling 30 to 60 mL per kilogram, have produced no sustained improvement in perfusion. I stop giving further fluid. I reassess for signs of overload — crackles, hepatomegaly, gallop, respiratory distress. I choose the vasoactive agent based on the shock phenotype: if cold shock with vasoconstriction, I start adrenaline at 0.05 to 0.5 micrograms per kilogram per minute; if warm shock with vasodilatation, I start noradrenaline at the same range. I use central access if immediately available, otherwise intraosseous. I call PICU or retrieval now, not after trying every local option. I check that antimicrobials were given within the first hour and that the cause is being treated. I continue reassessing and titrating the infusion to target perfusion markers.
References
- [1]Maitland, Kathryn Mortality after fluid bolus in African children with severe infection The New England journal of medicine, 2011.PMID 21615299
- [2]Weiss, Scott L Surviving Sepsis Campaign International Guidelines for the Management of Sepsis and Septic Shock in Children 2026 Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies, 2026.PMID 41869844
- [3]Weiss, Scott L Surviving Sepsis Campaign International Guidelines for the Management of Septic Shock and Sepsis-Associated Organ Dysfunction in Children Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies, 2020.PMID 32032273
- [4]Bjorklund, Ashley Pediatric Shock Review Pediatrics in review, 2023.PMID 37777656
- [5]Topjian, Alexa A Part 4: Pediatric Basic and Advanced Life Support 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Pediatrics, 2021.PMID 33087552
- [6]Schlapbach, Luregn J International Consensus Criteria for Pediatric Sepsis and Septic Shock JAMA, 2024.PMID 38245889
- [7]Sankar, Jhuma Fluid resuscitation in children with severe infection and septic shock: a systematic review and meta-analysis European journal of pediatrics, 2024.PMID 38916738
- [8]Burgunder, Lauren Medication and Fluid Management of Pediatric Sepsis and Septic Shock Paediatric drugs, 2022.PMID 35307800
- [9]Gupta, Siddharth Advances in Shock Management and Fluid Resuscitation in Children Indian journal of pediatrics, 2023.PMID 36715864
- [10]Alobaidi, Rashid Association Between Fluid Balance and Outcomes in Critically Ill Children: A Systematic Review and Meta-analysis JAMA pediatrics, 2018.PMID 29356810
- [11]Young, Kelly D Weight Estimation Methods in Children: A Systematic Review Annals of emergency medicine, 2016.PMID 27105839