Paeds · acute-care-resuscitation-and-toxicology
Poisoned child: structured assessment and decontamination
Also known as Paediatric poisoning assessment · Toxidromes in children · Activated charcoal in paediatric overdose · Gastrointestinal decontamination in children · Poisons Information Centre consultation
A fellowship approach to the poisoned child. Resuscitate with ABCDE and treat life-threatening toxin effects first, then take a structured ingestion history, recognise the toxidrome from vital signs, pupils and mental state, and call the Poisons Information Centre early. Give activated charcoal 1 g/kg within the first hour only when the airway is safe and the toxin is adsorbable; reserve whole bowel irrigation for iron, lithium, sustained-release and packet ingestions, and enhanced elimination for the few toxins it helps. Most children need observation and supportive care, and safeguarding runs in parallel for intentional and non-accidental exposure.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A poisoned child is any infant, child or young person who has been exposed to a substance that can cause harm, whether by ingestion, inhalation, skin or eye contact, or injection. The exposure may be accidental in a curious toddler, recreational in an adolescent, intentional in self-harm, or non-accidental in an abused child. The exposure that walks through the door is usually benign, occasionally lethal, and frequently uncertain, so the discipline of the assessment is what keeps the rare dangerous case from being missed. [9] [10]
The aim of care is not to name the toxin first. It is to keep the child alive while the substance, dose and time are worked out, to remove or neutralise what can be removed, to give an antidote where one exists, and to support organ function while the toxin clears. Decontamination is a small but examined part of this, and it always follows resuscitation, never precedes it. The child who is aspirating or in shock is harmed, not helped, by a dose of charcoal. [1] [12]
[9] [12]Classification
Classify the poisoned child on three axes at once: how unwell the child is, which toxidrome the physiology points to, and whether decontamination or an antidote applies. The first axis is clinical urgency, read from the primary survey, not from the reported substance. A well-looking toddler two hours after swallowing an unknown liquid and a drowsy, tachycardic child after the same report are in completely different risk bands. [1] [9]
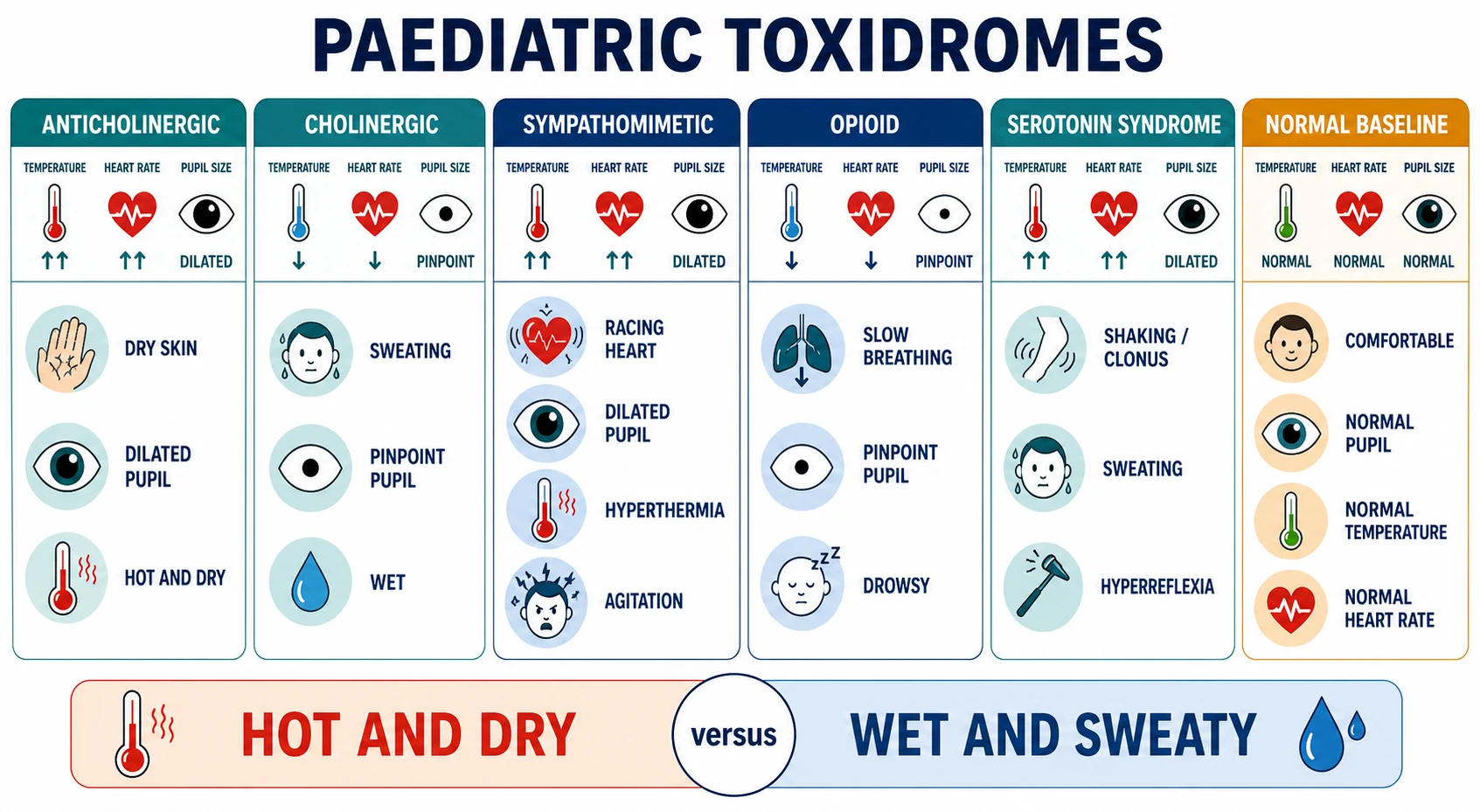
The second axis is the toxidrome, a recognisable cluster of physiological signs produced by a class of toxin acting on a shared receptor or pathway. Reading the toxidrome from the vital signs, pupils, secretions and mental state narrows the differential fast, points to the right antidote, and flags the child whose ingestion story is incomplete or misleading. A toxidrome is a hypothesis generated at the bedside, confirmed and refined as the history and tests return. [1] [2]
| Toxidrome | Hallmark signs | Representative agents | First response |
|---|---|---|---|
| Anticholinergic | Hot, dry, flushed; dilated pupils; agitated then obtunded; urinary retention | Antihistamines, tricyclics, atropine, plant alkaloids | Cool, sedate, control agitation; treat cardiotoxicity if tricyclic |
| Cholinergic | Wet: salivation, lacrimation, urination, defecation, sweating; pinpoint pupils; bradycardia; fasciculations | Organophosphate and carbamate pesticides, nerve agents | Atropine and pralidoxime per toxicology pathway; decontaminate skin |
| Sympathomimetic | Hyperthermia, tachycardia, hypertension, dilated pupils, agitation, sweating | Amphetamines, cocaine, pseudoephedrine, caffeine | Cool aggressively, benzodiazepines for agitation and hyperthermia |
| Opioid and sedative-hypnotic | Pinpoint pupils, respiratory depression, drowsiness or coma, hypotension | Opioids, benzodiazepines, ethanol, gamma-hydroxybutyrate | Naloxone for opioid respiratory depression; support the airway |
| Serotonin syndrome | Hyperthermia, clonus (inducible or spontaneous), hyperreflexia, agitation, autonomic instability | SSRIs, tramadol, triptans, linezolid in combination | Cool, benzodiazepines; consider cyproheptadine; stop serotonergic agents |
| Neuroleptic malignant | Hyperthermia, lead-pipe rigidity, altered conscious state, autonomic instability, raised creatine kinase | Antipsychotics, withdrawal of dopamine agents | Cool, benzodiazepines; supportive critical care; consider dantrolene or bromocriptine |
The third axis is the decontamination and antidote question, which depends on the substance, the dose, the time since ingestion, and the child's physiology. Most children need no gastrointestinal decontamination at all; a minority benefit from activated charcoal; a smaller minority need whole bowel irrigation or enhanced elimination; and a few need a specific antidote given early. Holding these four possibilities in order is the point of the structured assessment. [5] [12]
Epidemiology & Risk Factors
Poisoning is one of the commonest reasons a child presents to acute care. In large poison-centre datasets, the overwhelming majority of paediatric exposures are unintentional, occur at home, involve a single substance, and are managed with observation alone or simple first aid. Deaths are rare but cluster in two groups: the exploring toddler who reaches a dangerous medicine or household chemical, and the adolescent who takes an intentional or recreational overdose. [11]
Exploring infant and toddler
- Unintentional, at home, single substance, often a medication within reach
- Cosmetics, cleaning agents, plants and Grandparent's medicines are common
- Most are asymptomatic and need observation
- Dose is usually small because the container limits intake
School-age child
- Accidental ingestion of adult medications and household chemicals
- Intentional ingestion begins to appear in emotional-distress contexts
- Carbon monoxide and inhalational exposure join the differential
- Safeguarding must be considered when the story does not fit
Adolescent
- Intentional self-harm and recreational substance use dominate
- Co-ingestants, delayed-release formulations and unknown dose are common
- Higher lethality: paracetamol, psychotropics, cardiotoxic drugs
- Create private history time; assess mental-health risk and safeguarding
Context and access
- Decanted chemicals, unlabeled containers and shared housing increase risk
- Mental-health strain, family violence and prior self-harm raise concern
- Rural and remote settings change decontamination and retrieval timing
- Communication barriers and unsafe storage delay recognition
Certain exposures are high-harm regardless of age and must be actively sought. These include button batteries, corrosives, hydrocarbons, iron, tricyclic antidepressants, opioids, cardiac medications, toxic alcohols and sustained-release preparations. A child who has taken one of these, or whose substance cannot be identified, is observed and reassessed longer, and decontamination or an antidote is decided with the Poisons Information Centre. [5] [9]
Pathophysiology
A toxin harms a child by one of several mechanisms: receptor binding that over-stimulates or blocks a physiological pathway, direct chemical injury to tissue, interference with cellular metabolism, or displacement of oxygen from haemoglobin. The pattern of organ injury follows the mechanism: a receptor toxin produces a toxidrome, a corrosive burns the tissue it touches, a metabolic toxin poisons the cell from within, and an asphyxiant starves it of oxygen. Knowing the mechanism predicts the time-course and the treatment. [1] [2]
Absorption is the central event the decontamination methods target. After an oral exposure, most substances are absorbed from the small intestine over minutes to hours, and the amount that reaches the circulation depends on the dose, the formulation, gastric emptying, and gut motility. Activated charcoal works by adsorbing the toxin in the gut lumen so it cannot cross the mucosa, which is why it must be given early and is useless once absorption is complete. [3] [12]
Distribution and elimination follow absorption, and they decide which enhanced-elimination methods apply. A toxin that remains in the blood or is protein-bound may be removed by haemodialysis or haemoperfusion; a weak acid excreted in the urine, such as salicylate, may be trapped and removed by alkalinising the urine. These methods help only the few toxins that fit the pharmacology, which is why decontamination and elimination decisions are made with the toxicologist or Poisons Information Centre. [5] [9]
The clinical course is also shaped by the formulation. Sustained-release and enteric-coated preparations can continue to absorb for many hours, delaying and prolonging toxicity; drugs with enterohepatic recirculation may be reabsorbed after an apparent response. These properties justify multiple-dose activated charcoal for a small group of toxins and extended observation for sustained-release ingestions. [3] [4]
Clinical Presentation
The presentation ranges from a completely well toddler whose parent found an open bottle, to a child brought in obtunded, fitting, or in respiratory failure. Begin with the first impression and the primary survey, and describe what you see objectively. "This two-year-old is alert, pink, with a normal respiratory rate and a smell of menthol on the breath" tells the team far more than "this child may have swallowed something". The child who is unwell on arrival, or who deteriorates during observation, is managed as an emergency regardless of the reported substance. [9] [10]
The structured ingestion history
Once the airway, breathing and circulation are secure, take a structured history focused on the toxin. The goal is to answer four questions: what was taken, how much, when, and by what route, plus what else might have been co-ingested. This history drives every decontamination and antidote decision. [9] [10]
[9]Use a SAMPLE frame to keep the history complete: Substance and exposure details, Allergies, Medications and access in the home, Past history including baseline, mental-health and developmental context, Last meal (which affects absorption and aspiration risk), and Events leading up. Ask about unlabeled and decanted containers, shared or grandparent medications, and what other people in the household take. For an adolescent, create private history time to ask about substances, self-harm intent and pregnancy. [9] [10]
Examination and the toxidrome
Examine the child with the toxidrome in mind. Record the temperature, heart rate, blood pressure, respiratory rate, oxygen saturation and conscious level, then examine the pupils, skin and secretions, muscle tone, bowel sounds and reflexes. The pattern of these findings generates the toxidrome hypothesis and directs the immediate response: naloxone for an opioid picture, cooling and benzodiazepines for a hyperthermic sympathomimetic, atropine for a cholinergic, and sodium bicarbonate for a wide-complex cardiotoxic rhythm. [1] [2]
| Finding | What it suggests | First response |
|---|---|---|
| Pinpoint pupils with slow shallow breathing | Opioid toxidrome with respiratory depression | Naloxone and airway and ventilation support |
| Hyperthermia with rigidity or clonus | Serotonin syndrome, neuroleptic malignant or sympathomimetic toxicity | Cool actively, benzodiazepines, stop the trigger, critical care |
| Wide QRS or prolonged QT on ECG | Cardiotoxic drug poisoning (sodium-channel or potassium-channel block) | Sodium bicarbonate for wide QRS, electrolyte correction, cardiac monitoring |
| Hypoglycaemia | Sulfonylurea, ethanol, beta-blocker or salicylate poisoning | Correct glucose now; investigate and treat the cause |
| Drooling, stridor or oral burns | Corrosive ingestion with airway threat | Protect the airway; do not induce vomiting or give charcoal |
| Chemical smell, contaminated skin or clothing | Dermal or inhalational exposure (pesticide, hydrocarbon) | Remove clothing and decontaminate skin; protect staff |
Differential Diagnosis
The differential is built in two layers. First, the toxin class, read from the toxidrome and the history. Second, and just as important, the non-toxic causes that can mimic poisoning: sepsis, meningitis or encephalitis, metabolic disturbance including hypoglycaemia, raised intracranial pressure, seizure and post-ictal state, and head injury. A drowsy, tachycardic child with an unclear history is not assumed to be poisoned until infection and metabolic causes are excluded, because the two can coexist. [9] [10]
Toxin classes by toxidrome
- Anticholinergic, cholinergic, sympathomimetic patterns
- Opioid and sedative-hypnotic depression
- Serotonin syndrome and neuroleptic malignant states
- Cardiotoxic, metabolic and asphyxiant poisons
Non-toxic mimics
- Sepsis, meningitis and encephalitis with altered conscious state
- Metabolic encephalopathy: hypoglycaemia, electrolyte disturbance
- Seizure and post-ictal state; non-convulsive status
- Head injury and raised intracranial pressure
Covert and safeguarding
- Non-accidental poisoning and fabricated or induced illness
- Recreational and polysubstance exposure
- Carbon monoxide and environmental exposure
- Inconsistent history for the developmental stage
Formulation-driven
- Sustained-release and enteric-coated delayed toxicity
- Co-ingestants that change the time-course
- Drugs with enterohepatic recirculation
- Transdermal and inhalational routes
A defensible synthesis sounds like this: "This adolescent has taken an unknown number of her mother's tablets about ninety minutes ago. She is tachycardic with dilated pupils and a widening QRS, so I am treating cardiotoxic poisoning while I identify the drug, and I have called the Poisons Information Centre. I have secured her airway and given sodium bicarbonate, and I am keeping hypoglycaemia, sepsis and self-harm risk open in parallel." [1] [9]
Clinical & Bedside Assessment
Assess every poisoned child through the primary survey, then the focused toxin assessment. The primary survey is unchanged from any acutely ill child: secure the airway, give oxygen, support ventilation, treat shock, correct hypoglycaemia, and control seizures. The trap specific to poisoning is to skip the airway in the rush to give charcoal or an antidote; the airway comes first, every time. [9] [12]
Primary survey and resuscitation
State your concern, call for help, name a leader and allocate roles, and bring age- and weight-appropriate equipment and monitoring. Treat opioid respiratory depression with naloxone while supporting the airway and ventilation. Treat hypoglycaemia immediately. Control seizures. Treat cardiotoxic rhythms with sodium bicarbonate for wide QRS and electrolyte correction for long QT. Only when the airway, breathing and circulation are safe does the decontamination assessment begin. [1] [9]
[1] [2]Focused toxin assessment and decontamination decision
Once stable, assess the child for decontamination. The decision rests on four facts: the substance (is it adsorbed by charcoal?), the time since ingestion (are we within the charcoal window?), the airway (is it safe enough to give charcoal?), and the dose (is the exposure large enough to justify intervention). Document each, and where there is uncertainty, consult the Poisons Information Centre before acting. [3] [9]
After each action, state and document one sentence: what the toxidrome is, what you expected from the last action and what actually happened, and what you will do next. This spoken synthesis keeps the team coordinated and is exactly what examiners listen for during the decontamination decision. [1] [9]
Investigations
Stabilise first, then order a test for a named question. Most poisoned children need few tests; a small number need targeted toxicology and metabolic panels. A normal panel never overrules a child who is worsening. [9] [10]
Immediate and bedside
- Point-of-care glucose in every child
- ECG for any cardiotoxic concern or collapse
- Blood gas to quantify ventilation, perfusion and acid-base state
- Paracetamol level at four hours when exposure is possible
Conditional on a question
- Electrolytes, renal and liver function for metabolic or organ-specific toxicity
- Salicylate, iron, lithium, toxic alcohol and methaemoglobin levels when the substance suggests them
- Lipase for corrosive or alcohol exposure
- Pregnancy test for adolescent self-harm presentations
Targeted and confirmatory
- Quantitative drug levels that change management (paracetamol, salicylate, iron, lithium, valproate)
- Carboxyhaemoglobin and methaemoglobin for inhalational or methaemoglobin-forming agents
- Chest radiograph after hydrocarbon aspiration or corrosive ingestion
- Never delay time-critical treatment for complete sampling in an unstable child
Interpret the results as physiology and risk, not as binary reassurance. A four-hour paracetamol level plotted on the treatment nomogram decides whether N-acetylcysteine is given. A salicylate level paired with an acid-base assessment decides between urinary alkalinisation and haemodialysis. An iron level with a white-cell count and glucose guides the decontamination and chelation decision. Each test answers one named question; do not order panels that will not change the immediate plan. [9] [10]
Management — Resuscitation
A poisoned child with physiological compromise triggers the resuscitation team. State your concern, call for help, name a leader, allocate roles, use closed-loop communication, and prepare age- and weight-appropriate equipment and monitoring. Treat the life-threatening toxin effects in parallel with the primary survey, and only then move to decontamination. [1] [9]
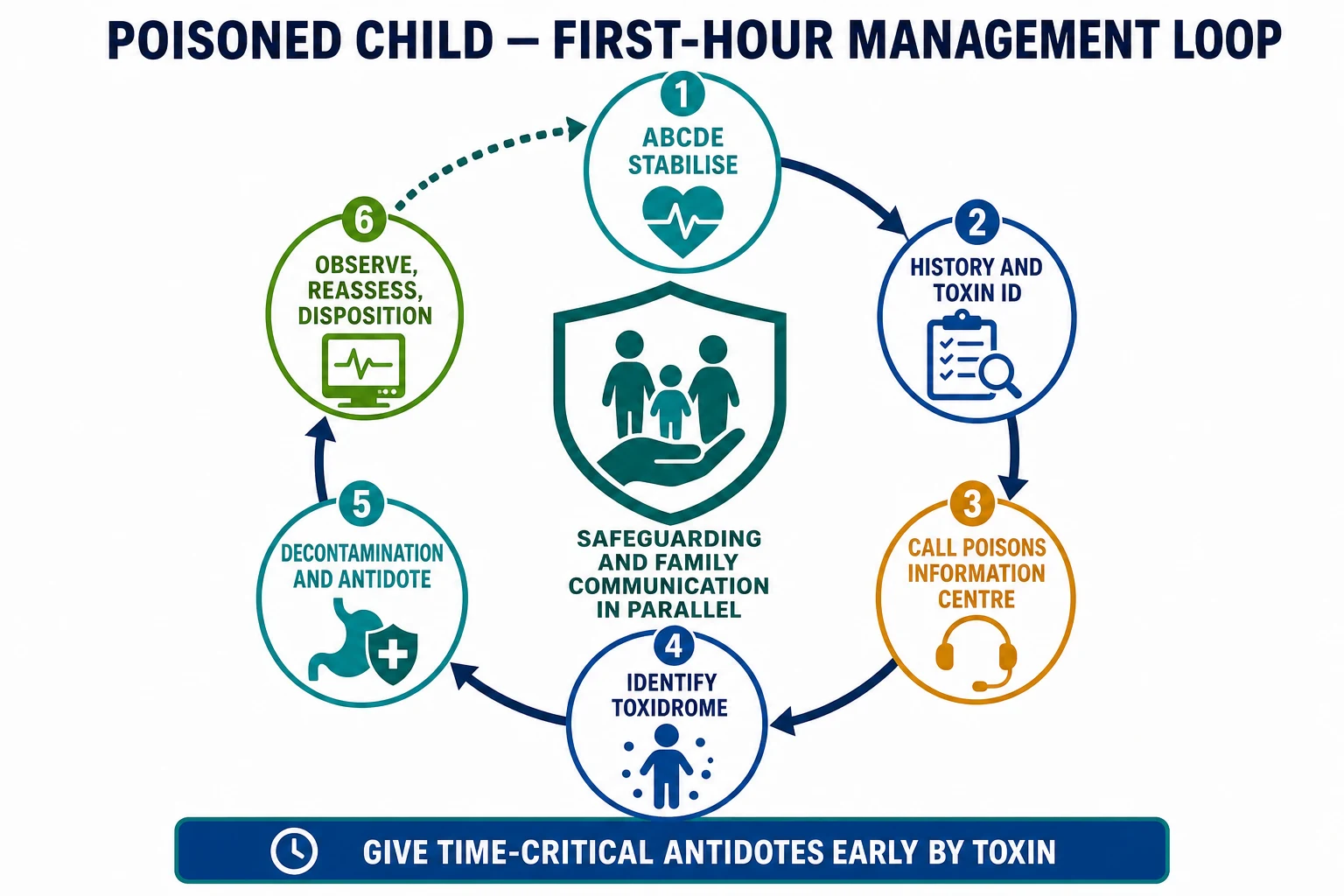
The first minutes when the substance is uncertain
Call and organise
Declare concern, call senior, resuscitation and toxicology or retrieval help, identify the leader and allocate tasks.
A, B, C and glucose
Position and protect the airway, give oxygen, support ventilation, treat shock, correct hypoglycaemia and control seizures.
Treat life-threatening toxin effects
Give naloxone for opioid respiratory depression, sodium bicarbonate for a wide-complex cardiotoxic rhythm, and cool the hyperthermic child actively.
History and toxidrome
Take the structured ingestion history and read the toxidrome from the vital signs, pupils and mental state.
Consult the Poisons Information Centre
Call early with the substance, dose, time, weight and physiology to shape the decontamination and antidote plan.
Decontaminate, antidote, observe
Decide on activated charcoal, whole bowel irrigation or enhanced elimination, give any specific antidote, and observe for delayed toxicity.
Call the Poisons Information Centre early. In Australia the number is 13 11 26; in Aotearoa New Zealand 0800 764 766; the United Kingdom uses the National Poisons Information Service and Toxbase; Ireland uses the National Poisons Information Centre. The centre gives current, product-specific advice on toxicity, decontamination, antidotes, observation times and thresholds, and it is the single most useful consult in paediatric poisoning. Document the call, the advice, and the consultant's name or reference. [9]
[3] [12]Management — Definitive & Stepwise
After resuscitation, move into the toxin-specific plan without stopping reassessment. This hub covers the structured approach and decontamination shared by every poisoning; treat the most dangerous problem first and link to the dedicated paracetamol, iron, salicylate, opioid, cardiotoxic, caustic and hydrocarbon pages for complete algorithms. [1] [9]
Activated charcoal
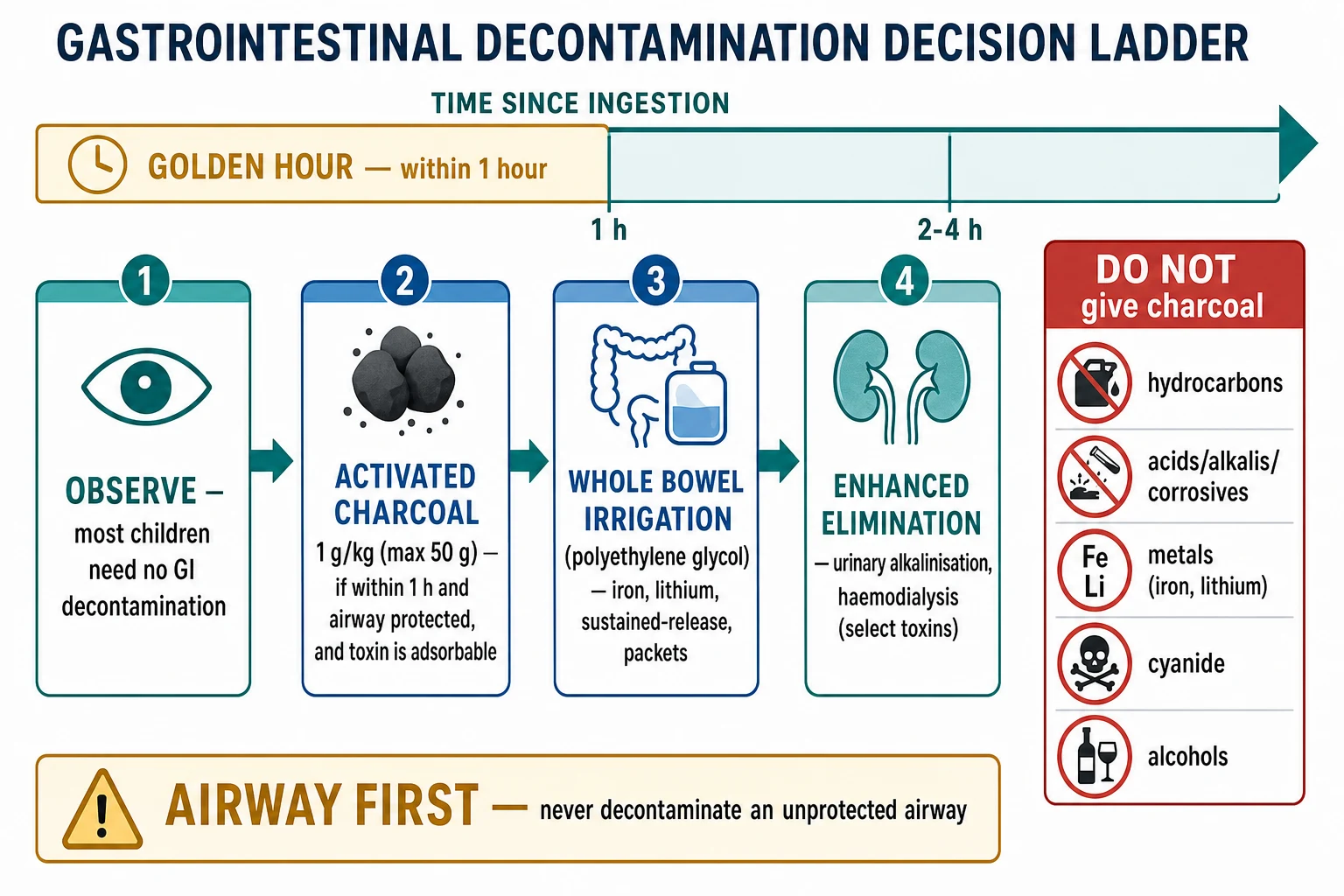
Activated charcoal adsorbs many drugs in the gut lumen and reduces their absorption. Give it at 1 g/kg body weight to a maximum of 50 g as a single dose, ideally within one hour of ingestion, when the airway is protected, the toxin is adsorbable, and the exposure is significant. It is not given after corrosive or hydrocarbon ingestion, and it does not adsorb iron, lithium, metals, toxic alcohols, cyanide or hydrocarbons. Multiple-dose activated charcoal, given at intervals, enhances elimination for a small group of toxins with enterohepatic recirculation such as theophylline, carbamazepine, phenobarbital and dapsone, and is guided by the toxicologist. [3] [4]
Activated charcoal (single dose)
Whole bowel irrigation and enhanced elimination
Whole bowel irrigation with polyethylene glycol solution flushes the gut and is reserved for ingestions of iron, lithium, sustained-release formulations, and packets of illicit drugs, where the toxin is not adsorbed by charcoal or is likely to continue absorbing. It is given via nasogastric tube until the effluent is clear, and it needs a protected airway and close monitoring. Enhanced elimination by urinary alkalinisation helps salicylate poisoning by trapping the weak acid in the urine; haemodialysis removes a small set of toxins including salicylate, methanol, ethylene glycol, metformin, lithium and valproate. Both are toxicologist-guided and chosen for the specific toxin. [7] [5]
Gastric emptying and skin decontamination
Gastric lavage and induced emesis with ipecac are rarely used in modern paediatric practice, because the benefit is small and the risks of aspiration, oesophageal injury and deterioration outweigh it in almost all cases. For dermal exposure, remove contaminated clothing and wash the skin with copious water, protecting staff from secondary contamination. For ocular exposure to a corrosive or irritant, irrigate the eye immediately with water or saline for at least fifteen minutes and assess for injury. Inhalational exposure needs removal from the source and oxygen; carbon monoxide and cyanide have specific pathways. [5] [12]
Choosing the decontamination method
Most children
Observe and give supportive care; no gastrointestinal decontamination is needed for the majority of paediatric exposures.
Activated charcoal
1 g/kg to a maximum of 50 g within the first hour for a significant adsorbable toxin, only when the airway is protected.
Whole bowel irrigation
Polyethylene glycol via nasogastric tube for iron, lithium, sustained-release and packet ingestions.
Enhanced elimination
Urinary alkalinisation for salicylate; haemodialysis for salicylate, toxic alcohols, metformin, lithium and valproate, as guided by the toxicologist.
Skin, eye and inhalational
Remove clothing and wash skin; irrigate the eye for at least fifteen minutes; remove from source and give oxygen for inhalational exposure.
Improvement must make sense across several findings. A child given naloxone must be watched for re-sedation as the opioid outlasts the antagonist. A child given activated charcoal must be observed for delayed toxicity from sustained-release formulations. Reassess after each action and meaningful change, not on a fixed schedule, and agree the observation time with the Poisons Information Centre. [1] [9]
Specific Subtypes & Scenarios
The structured approach stays the same, but age, substance and intent change what you look for and how early you escalate. In each scenario: resuscitate first, identify the toxin and toxidrome, activate the correct pathway, and state which facts are specific to that substance or setting. [1]
Exploring toddler
- Usually unintentional, single substance, small dose
- Bring the container; observe for the expected time
- High-harm agents: button battery, corrosive, hydrocarbon, iron
- Keep safeguarding open when the story does not fit
Adolescent self-harm
- Intentional, often polysubstance, delayed-release formulations
- Higher lethality: paracetamol, psychotropics, cardiotoxic drugs
- Assess mental-health risk and safeguarding; create private history time
- Observe longer for delayed and co-ingested toxicity
Corrosive or hydrocarbon
- Drooling, stridor or oral burns in corrosive ingestion
- Respiratory distress and cough after hydrocarbon aspiration
- No charcoal, no induced emesis, no gastric lavage
- Protect the airway; decontaminate skin and eyes
Sustained-release or packet ingestion
- Delayed and prolonged toxicity; extended observation
- Whole bowel irrigation for sustained-release and packets
- Risk of packet rupture in body-packing
- Toxicologist and surgical input for packet complications
Rural or remote
- Call the Poisons Information Centre and retrieval early
- State distance, weather, staff and equipment limits
- Agree observation time against transport risk
- Package monitoring and access for transport
Opioid respiratory depression
- Pinpoint pupils, slow shallow breathing, reduced conscious level
- Naloxone titrated to restore adequate breathing, not full wakefulness
- Watch for re-sedation as the opioid outlasts naloxone
- Support the airway and ventilation before and during antidote
Cardiotoxic drug poisoning
- Wide QRS from sodium-channel block; long QT from potassium-channel block
- Sodium bicarbonate for wide QRS; correct electrolytes
- Continuous cardiac monitoring and critical care
- Avoid class Ia antiarrhythmics
Hyperthermic toxidrome
- Serotonin syndrome, neuroleptic malignant, sympathomimetic
- Cool actively, benzodiazepines, stop the trigger
- Consider cyproheptadine for serotonin syndrome
- Critical care for rigidity, rhabdomyolysis and organ failure
Pesticide and organophosphate
- Cholinergic toxidrome: wet, pinpoint pupils, fasciculations
- Decontaminate skin and clothing; protect staff
- Atropine and pralidoxime per toxicology pathway
- Extended observation for delayed effects
Carbon monoxide
- Headache, nausea, reduced conscious level; cherry-red skin is late
- Measure carboxyhaemoglobin; give high-flow oxygen
- Hyperbaric therapy is centre- and case-specific
- Consider co-exposed family members
Complications & Pitfalls
Most harm in paediatric poisoning begins when resuscitation is delayed for decontamination, or when a single reassuring feature ends the assessment. The most preventable errors are giving charcoal to an unprotected airway, failing to treat opioid respiratory depression, missing cardiotoxicity on the ECG, and closing the differential on the reported substance while a second dangerous cause is present. [1] [9]
| Pitfall | Why it harms | Corrective behaviour |
|---|---|---|
| Decontamination before resuscitation | An unstable child is destabilised by the intervention | Secure the airway, breathing and circulation before any decontamination |
| Charcoal to an unprotected airway | Aspiration pneumonitis can be severe | Protect the airway first; never give charcoal to a vomiting or obtunded child without a plan |
| Opioid apnoea not treated | Preventable respiratory arrest | Give naloxone and support ventilation while confirming the cause |
| Cardiotoxicity missed on the ECG | Wide-complex or long-QT arrhythmia deteriorates | ECG early for any cardiotoxic concern; sodium bicarbonate for wide QRS |
| Charcoal for the wrong toxin | Iron, lithium, metals, alcohols and corrosives are not adsorbed | Confirm the toxin is adsorbable before giving charcoal |
| Premature closure on the history | A second or co-ingested cause is missed | Keep toxin, infection, metabolic and safeguarding causes open in parallel |
| Under-observation of sustained-release | Delayed toxicity occurs after apparent stability | Observe for the formulation-specific time; consult the Poisons Information Centre |
| Safeguarding postponed for diagnosis | Immediate safety and evidence are lost | Stabilise first while safeguarding proceeds in parallel |
| Adult doses or equipment | Age and weight are ignored | Use weight-based dosing and paediatric cognitive aids |
| Poor handover | Substance, dose, time and observation plan are lost | Use a structured transfer with read-back and named ownership |
Watch for anchoring on the referral diagnosis and carrying forward a label that silences bedside concern. After stabilisation, look actively for harm from treatment: aspiration after charcoal, fluid and electrolyte shifts, repeated sampling, and medication error. The fact that the child did not arrest does not prove an intervention was harmless. [3] [12]
[1] [3] [9]Prognosis & Disposition
Most poisoned children recover fully with supportive care, and disposition follows the trend, the substance, the formulation and the response. Consider the child's age and reserve, the dose and toxicity of the substance, the time since ingestion, the need for antidote or enhanced elimination, local support, transport risk, and whether the family can carry out the plan. [9] [11]
Critical care or retrieval
- Airway, breathing or circulation compromise, or anticipated deterioration
- Need for intubation, vasoactive support, dialysis or toxicologist-led care unavailable locally
- Cardiotoxic, hyperthermic or sustained-release high-lethality ingestion
- Transport risk that needs early specialist planning
Ward or high-dependency
- Symptomatic but stable, or awaiting the observation window for delayed toxicity
- Monitoring and staffing can detect and respond to failure
- Pending levels or results that change disposition
- A named escalation pathway exists
Discharge only when defensible
- Asymptomatic through the substance-specific observation window
- No unresolved immediate threat or high-harm cause
- Toxin identified, level reassuring, and antidote not required
- Mental-health and safeguarding assessment complete where relevant
A safety net states what change to watch for, how urgently to act, and exactly where to get help. For poisoning, it states the expected time of delayed toxicity, when to return, and who owns pending results. "Return if worried" alone is never enough. For intentional self-harm, a mental-health and safeguarding assessment must be complete before discharge, and the family and primary care or community team are connected. After a critical event, explain what happened and what remains uncertain, invite questions, and consider debriefing. [9] [10]
Special Populations
Adapt how you observe, communicate and decontaminate, but never lower the standard for recognising deterioration. Evidence for decontamination in disability, neurodiversity, technology dependence and many low-resource settings is sparse; present these adaptations as safer practice, not as proven improvements in outcome. [9]
| Population or context | Adaptation that changes care | Boundary |
|---|---|---|
| Exploring toddler | Bring the container; observe for the substance-specific time; keep safeguarding open | Do not assume a small reported dose excludes a high-harm agent |
| Complex or technology-dependent child | Establish personal baseline and medication list; assess child and device in parallel | A chronically abnormal level is not automatically safe; compare with the personal baseline |
| Severe neurodisability | Establish usual interaction and pain expression; treat caregiver-described change as evidence | Toxidrome signs may be altered; rely on vital-sign trends |
| Adolescent | Create private time; ask about substances, self-harm and pregnancy; explain confidentiality limits | Confidentiality has safety limits; safeguarding duties still apply |
| Indigenous, migrant or remote family | Use cultural safety and a professional interpreter; address access and transport barriers | Retrieval and safeguarding routes remain jurisdiction-specific |
| Out-of-home care and youth justice | Treat inconsistent history and repeated exposure as high-risk; involve carers and the care team | Safeguarding and statutory notification duties apply |
Safeguarding runs in parallel with medical care, but immediate stabilisation and safety come first. Consider non-accidental poisoning and fabricated or induced illness when the history is inconsistent with the developmental stage, when the substance is unusual, or when there are repeated presentations. Ask only necessary open, non-leading questions. Explain confidentiality and information sharing, document objective findings and spontaneous words, preserve evidence when safe, and use the local safeguarding pathway. Reporting thresholds, consent rules and agencies differ by Australian state or territory, UK nation, US state and Canadian province or territory. [9]
Evidence, Guidelines & Regional Differences
What the evidence can and cannot support
The structure of the assessment — resuscitation first, then history, toxidrome, decontamination and antidote — is consensus across the major toxicology sources. The use of activated charcoal is supported by a systematic review and current Clinical Toxicology Recommendations Collaborative guidance, which emphasise early single-dose charcoal for adsorbable toxins within the first hour when the airway is safe, and multiple-dose charcoal for a defined group with enterohepatic recirculation. What remains debated is the exact benefit in children for specific substances, the role of charcoal beyond one hour in large or sustained-release ingestions, and the observation times that fit every formulation. [3] [4]
Hoegberg et al. — Activated charcoal for gastrointestinal decontamination (systematic review and 2026 recommendations)
Clinical Toxicology
Systematic review of activated charcoal in acute oral overdose, followed by a Clinical Toxicology Recommendations Collaborative consensus on administration
Key finding
Single-dose activated charcoal is most effective within one hour of an adsorbable toxin; benefit beyond one hour is small and substance-specific. Multiple-dose charcoal enhances elimination for toxins with enterohepatic recirculation. Charcoal is not indicated for corrosives, hydrocarbons, iron, lithium, metals or toxic alcohols.
Practice change
Give activated charcoal 1 g/kg to a maximum of 50 g within the first hour to a child with a protected airway after a significant adsorbable ingestion; reserve multiple-dose charcoal and extended-observation decisions for toxicologist-guided cases.
Whole bowel irrigation is endorsed by the American Academy of Clinical Toxicology and the European Association of Poison Centres and Clinical Toxicologists for a narrow set of ingestions, and a paediatric retrospective review supports its use for iron, lithium, sustained-release and packet ingestions. Gastric lavage and induced emesis have largely left modern paediatric practice because the small benefit is outweighed by the risks. [7] [8]
There is no universal charcoal window, observation time, or decontamination threshold that fits every substance and formulation. Attach each rule to its population, purpose and source, and quote the local Poisons Information Centre advice rather than inventing precision. [3] [9]
Jurisdictional implementation
Australia and Aotearoa New Zealand: the Royal Children's Hospital Melbourne acute management of poisoning guideline and the Poisons Information Centre (Australia 13 11 26; New Zealand 0800 764 766) support local implementation. Retrieval systems, observation charts, mandatory reporting and consent remain state-, territory- or nation-specific.
Global and low-resource settings: WHO and national poison-control services adapt toxicology assessment for low-resource hospitals and non-specialists. Population-specific substances, slower resource escalation and limited decontamination options must stay attached to that context.
Exam Pearls
Resuscitation first
- ABCDE: secure airway, oxygen, treat shock, correct glucose, control seizures
- Treat opioid apnoea with naloxone; cardiotoxic wide QRS with sodium bicarbonate
- Decontamination never precedes resuscitation
- Hyperthermia is an emergency: cool actively
Structured assessment
- Four questions: what, how much, when, what else
- Read the toxidrome from vital signs, pupils and mental state
- Call the Poisons Information Centre early (Australia 13 11 26)
- ECG for any cardiotoxic concern; glucose in every child
Decontamination
- Most children need no GI decontamination
- Activated charcoal 1 g/kg max 50 g within 1 hour if airway safe and toxin adsorbable
- No charcoal for corrosives, hydrocarbons, iron, lithium, metals, toxic alcohols
- Whole bowel irrigation for iron, lithium, sustained-release, packets
Antidotes and elimination
- Naloxone for opioid; N-acetylcysteine for paracetamol; atropine for cholinergic
- Urinary alkalinisation for salicylate; haemodialysis for salicylate, alcohols, metformin, lithium, valproate
- Multiple-dose charcoal for enterohepatic recirculation toxins
- Skin and eye decontamination for dermal and ocular exposure
Pitfalls and safeguarding
- No charcoal to an unprotected airway
- No missing opioid apnoea or cardiotoxicity
- No closing the differential on the reported substance
- Safeguarding and family communication run in parallel
- Observe sustained-release ingestions for the full window
“Resuscitate first; take the structured ingestion history; read the toxidrome; call the Poisons Information Centre early; give activated charcoal 1 g/kg within the first hour only when the airway is safe and the toxin is adsorbable; reserve whole bowel irrigation and enhanced elimination for the few cases they help; observe for delayed toxicity; and run safeguarding and family communication in parallel.”
Viva: the toddler with an open bottle
Do not anchor on the label alone. Resuscitate with ABCDE, take the four-question history with the container, read the toxidrome, check a glucose and an ECG, and call the Poisons Information Centre. Decide on activated charcoal only if the airway is safe and the toxin is adsorbable and within the window. Observe for the substance-specific time, keep safeguarding open, and discharge only with a defensible safety net.
Viva: the drowsy adolescent with dilated pupils
Resuscitate first. The drowsy adolescent with dilated pupils and a widening QRS has a cardiotoxic or anticholinergic toxidrome until proven otherwise. Secure the airway, give sodium bicarbonate for a wide QRS, run a glucose and ECG, take a private history about substances and self-harm, and call the Poisons Information Centre. Identify the drug, treat the toxidrome, and complete a mental-health and safeguarding assessment before any disposition.
Structured oral: the child who aspirated charcoal
The harm of charcoal is aspiration pneumonitis. Stabilise the airway and breathing, assess the extent of lung injury with a chest radiograph and gas, and escalate to critical care if there is respiratory failure. Review the decision that led to charcoal: the airway should have been protected first. Document the event, inform the family, and feed the lesson back into the unit's decontamination protocol.
References
- [1]Hoffman, Robert J Toxidromes and a general approach to poisoning Archives of disease in childhood, 2025.PMID 39978865
- [2]Hui, Wai Fu An Overview of the Pediatric Toxidromes and Poisoning Management Current reviews in clinical and experimental pharmacology, 2021.PMID 33261543
- [3]Hoegberg, Lotte C G Systematic review on the use of activated charcoal for gastrointestinal decontamination following acute oral overdose Clinical toxicology (Philadelphia, Pa.), 2021.PMID 34424785
- [4]Hoegberg, Lotte C G Recommendations from the Clinical Toxicology Recommendations Collaborative on the administration of activated charcoal in acute oral overdose Clinical toxicology (Philadelphia, Pa.), 2026.PMID 41906697
- [5]Zhao, Xiaoyan Decontamination of the pediatric patient Current opinion in pediatrics, 2016.PMID 27031659
- [6]Lapus, Rance M Activated charcoal for pediatric poisonings: the universal antidote? Current opinion in pediatrics, 2007.PMID 17496769
- [7]Tenenbein, Milton Position statement: whole bowel irrigation. American Academy of Clinical Toxicology; European Association of Poisons Centres and Clinical Toxicologists Journal of toxicology. Clinical toxicology, 1997.PMID 9482429
- [8]Lo, Jonathan C A retrospective review of whole bowel irrigation in pediatric patients Clinical toxicology (Philadelphia, Pa.), 2012.PMID 22578074
- [9]Berg, Sara E Pediatric Toxicology: An Updated Review Pediatric annals, 2023.PMID 37036778
- [10]Ross, Jennifer A Pediatric Toxicology Emergency medicine clinics of North America, 2022.PMID 35461621
- [11]Gummin, Daniel D 2022 Annual Report of the National Poison Data System (NPDS) from America's Poison Centers: 40th Annual Report Clinical toxicology (Philadelphia, Pa.), 2023.PMID 38084513
- [12]Bond, George R The role of activated charcoal and gastric emptying in gastrointestinal decontamination: a state-of-the-art review Annals of emergency medicine, 2002.PMID 11867980