Paeds · adolescent-and-young-adult-medicine
Adolescent risk assessment and harm minimisation
Also known as Adolescent harm reduction · Youth risk screening · SBIRT in adolescents · HEEADSSS risk assessment · Harm minimisation in young people · Adolescent risk formulation
A fellowship approach to assessing adolescent risk across all domains and applying harm-minimisation principles: structured screening, risk formulation, brief intervention, and pragmatic domain-specific harm reduction that meets young people where they are across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A registrar sees a 16-year-old for a sports check. Vaping is "just social," mood is "fine," and the visit closes in eight minutes. Six weeks later the same teenager is in resus after a fentanyl overdose. The missed work was not a rare diagnosis. It was risk that nobody asked about, and a plan that demanded abstinence the young person could not yet give. [5] [7]
Adolescent risk assessment is structured inquiry across the domains that actually drive morbidity and mortality in young people — substance use, mental health and suicide, sexual and reproductive health, injury and violence, digital exposure, and social determinants. HEADSS (and its HEEADSSS expansion) is the interview framework; validated instruments are the adjuncts that sharpen specific domains. [1] [2]
Harm minimisation (often called harm reduction) is a pragmatic public-health stance: reduce the adverse consequences of a risk behaviour even when the behaviour itself continues. It does not abandon abstinence as one possible goal — it stops treating abstinence as the only acceptable outcome, because that stance pushes away the young people at greatest risk. [5] [7]
The clinical skill is the marriage of the two: assess risk thoroughly, then meet the young person at their readiness with a response that lowers harm today while keeping the door open for bigger change later. [4] [8]
Core sequence of risk assessment and harm minimisation
Engage
Youth-friendly, time alone, conditional confidentiality, non-judgemental stance.
Assess
HEADSS/HEEADSSS plus validated screens where a lead appears.
Formulate
Integrate into a risk tier: universal, selected, or indicated.
Brief intervention
Motivational interviewing; personalised feedback; explore readiness.
Harm-reduction bundle
Pragmatic, domain-specific: naloxone, condoms, cut-down, means restriction.
Follow-up
Safety plan, low-threshold re-access, timed review, build transition.
Classification
Classify by risk domain, assessment intensity, and risk tier. The domain tells you what to ask; the intensity tells you how deep to go; the tier tells you how to respond. [1] [4]
Risk domains
The six domains that matter most in adolescence are substance use, mental health and suicide, sexual and reproductive health, injury and violence, digital and online exposure, and social determinants. Each has its own screening tools and its own harm-reduction options. A visit that covers only one domain has not assessed risk. [1] [5]
Assessment intensity
Universal inquiry means asking every adolescent, lightly, across all domains. Selective screening means adding a validated tool when a positive lead or a risk amplifier appears. Indicated or diagnostic assessment means formal evaluation after a positive screen. You move right only when the history pushes you there. [4] [2]
Risk tiers and readiness
Risk is not binary. Stratify into low (no active risk, protective factors strong), moderate (risk behaviour present, function preserved), and high (impairment, danger, or instability). Pair the tier with the young person's stage of change, because the right intervention for a precontemplative vaper is not the right one for someone asking to quit. [8] [7]
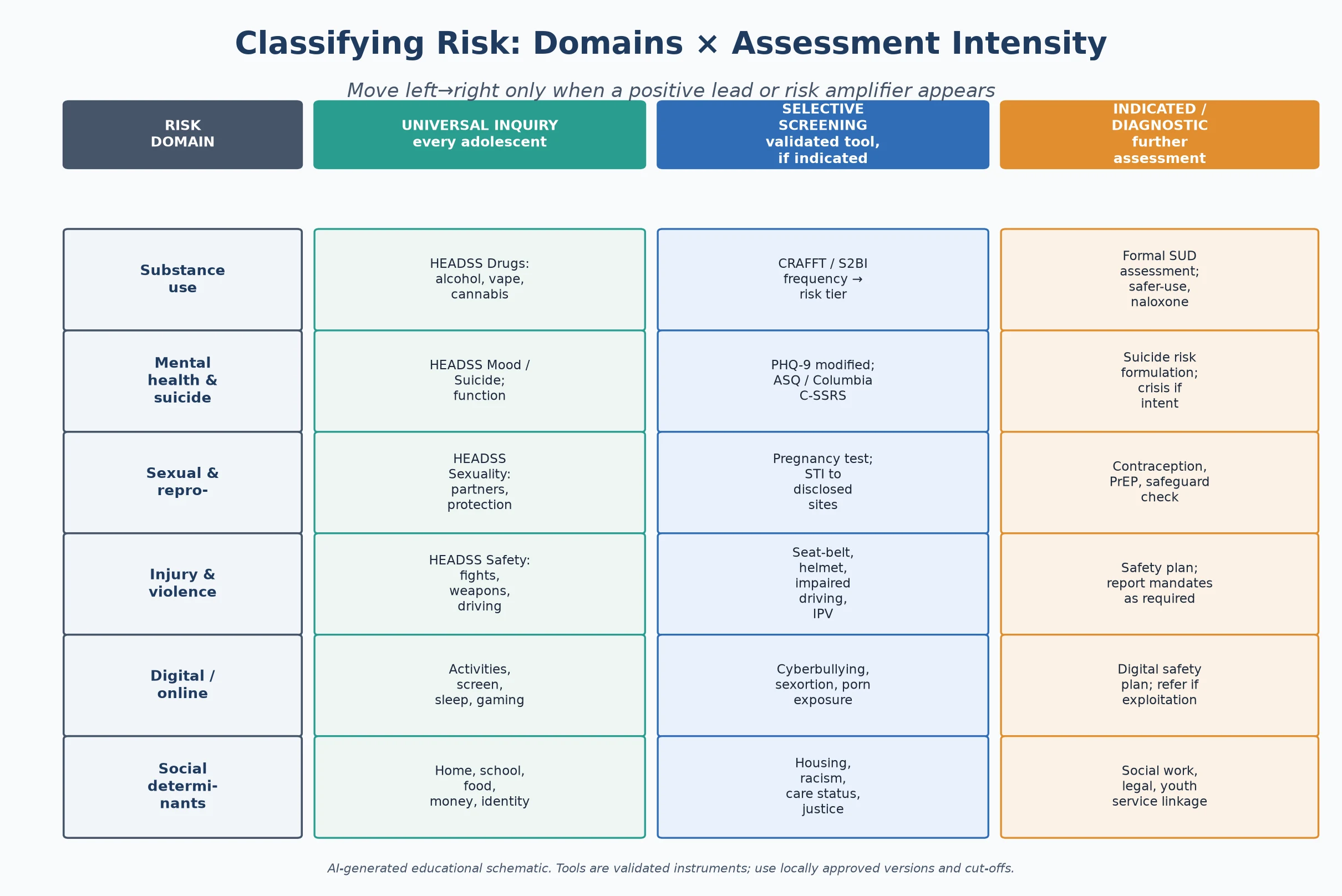
Read the figure like this: if every adolescent gets a universal HEADSS pass but nobody ever moves into the selective-screening column, risk assessment is incomplete. Positive leads must trigger the next instrument. [4]
Abstinence-only
Narrow goal
- Demands behaviour stops now
- Single acceptable outcome
- Disengages high-risk youth
- No safety net if behaviour continues
Harm minimisation
Pragmatic stance
- Reduce consequences today
- Abstinence is one option, not the only one
- Keeps youth engaged
- Builds toward bigger change
SBIRT
Structured workflow
- Screen all, intervene briefly
- Refer indicated cases
- Brief intervention ≠ punishment
- Embeds harm reduction in routine care
Epidemiology & Risk Factors
The leading drivers of adolescent death and disability across high-income settings are injury, suicide, substance-related harm, sexual and reproductive outcomes, and mental disorder. These are exactly the risks a structured visit can surface. [7] [12]
Risk is not evenly distributed. Poverty, racism, housing instability, rural isolation, family rejection, out-of-home care, youth-justice involvement and refugee or migrant status all amplify exposure and reduce access to confidential care. LGBTQ+ minority stress and neurodiversity add further risk that is often missed through diagnostic overshadowing. [5] [6]
The fentanyl era has changed the overdose picture. A young person who believes they are taking a pill or a powder may be exposed to a potent opioid they never chose. This makes naloxone availability and overdose education a routine harm-reduction conversation, not a fringe one. [9] [5]
Suicide remains a leading cause of adolescent death, and emergency-department tools can help stratify near-term risk — but no instrument replaces a same-visit clinical assessment of intent, plan, means and protection. [11] [12]
Pathophysiology
You do not need a neuroscience lecture to counsel well. You do need a usable model of why adolescents take risks, because it explains why harm reduction works and why abstinence-only often fails. [3]
The dual-systems model describes two developmental curves. The reward and socio-emotional system matures early and peaks through mid-adolescence. The cognitive-control system, anchored in the prefrontal cortex, matures later. The gap between them is the window of heightened risk-taking, especially under peer presence and emotional arousal. [3]
This matters clinically. Under affective and social load, an adolescent may genuinely intend not to use, and still use. Counselling that treats a broken promise as a moral failure ignores the biology. Counselling that reduces access to means, delays exposure and builds skills works with the biology rather than against it. [3] [5]
Harm reduction fits the neuroscience precisely. Where a young person is not ready to stop, lowering the consequences — naloxone for overdose, condoms for STI, a cut-down plan for vaping, restricted access to lethal means — keeps them alive and in contact long enough for the control system to catch up and for bigger change to become possible. [5] [9]
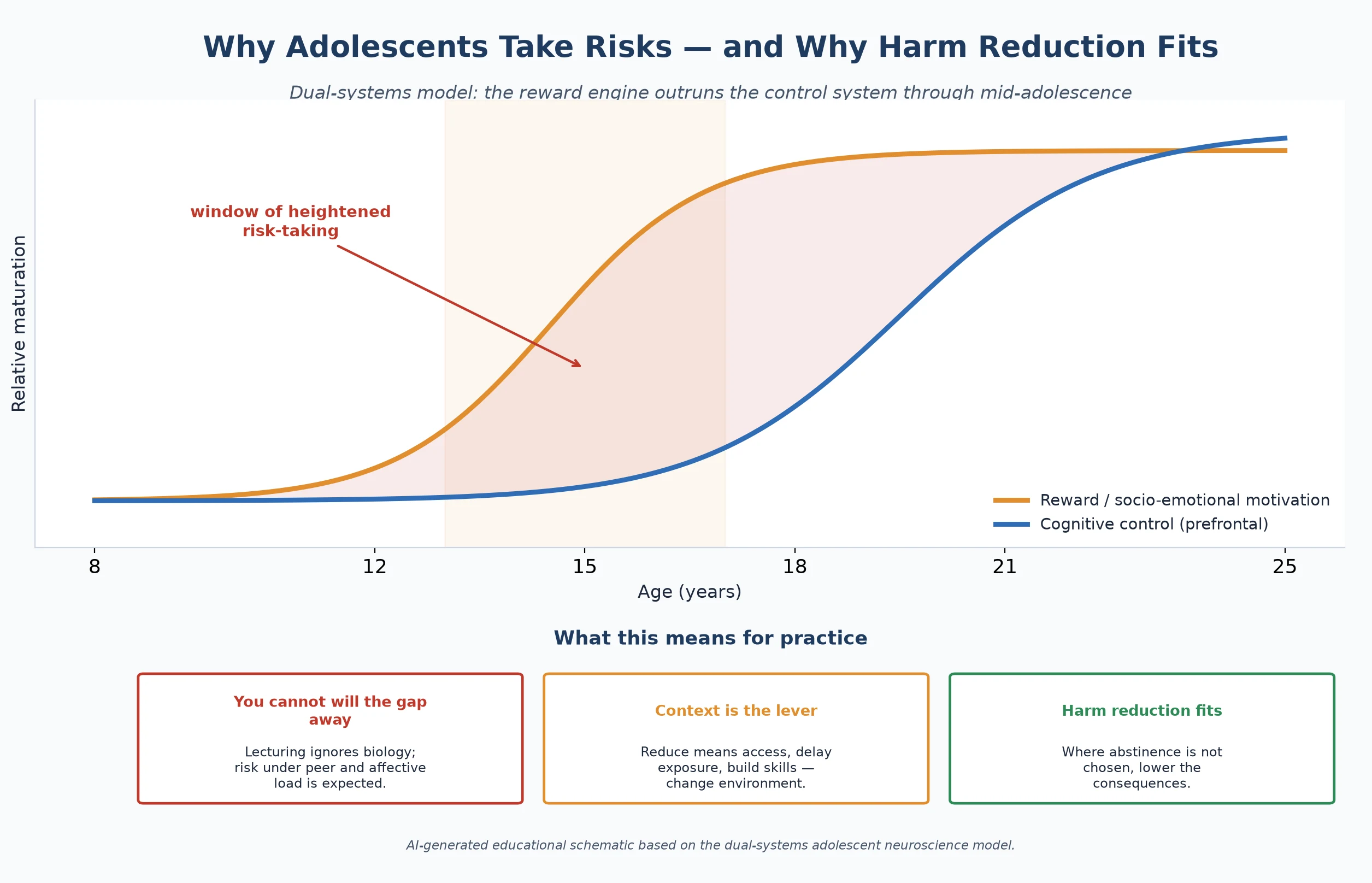
Read the figure like this: the shaded gap is not a character flaw. It is a developmental fact. Your job is to narrow the harm inside that gap, not to lecture it shut. [3]
Clinical Presentation
Risk presents across a spectrum, from the openly disclosed to the completely hidden. The most dangerous presentations are often the quiet ones, because nobody looked. [1]
Organised low-risk presentation: the young person engages, private time is secured, HEADSS is completed, and the only finding is normative exploration with intact function. The task is brief reinforcement and a safety net. [4]
High-risk patterns hiding inside ordinary visits: the parent who answers every question; recurrent somatic complaints with school decline; sleep reversal dismissed as attitude; weight-loss pride or rigid food rules; "social" vaping or riding with an impaired driver; a confidential request for STI testing; an older teen with a chronic illness and no transition plan. Each is a door into a domain that needs assessment, not closure. [6] [2] [11]
Acute risk presentations arrive in ED or crisis: overdose, self-harm, assault disclosure, intoxication with danger, or a positive suicide screen with plan and intent. These exit the routine pathway immediately and enter resuscitation and safety care. [11] [12]
Differential Diagnosis
In risk assessment the differential is less "which disease" and more "what is driving the behaviour, and is it dangerous." [7]
| What it looks like | Safer framing question | Do not miss |
|---|---|---|
| "Recreational" vaping | Frequency, dependence, nicotine withdrawal | Escalating to other substances; co-occurring mood disorder |
| Low mood and withdrawal | Suicidal ideation, plan, means, intent | Active suicide risk needing same-visit action |
| Risky sexual behaviour | Coercion, trafficking, capacity to consent | Exploitation or assault masquerading as choice |
| School refusal | Bullying, family violence, untreated anxiety | Safeguarding concern underneath the attendance label |
| Binge drinking | Frequency, context, impaired driving | Fentanyl exposure in counterfeit pills or powders |
The core discriminator is function: does the behaviour sit alongside intact home, school and peer function, or is it accompanied by impairment, danger and instability? Normative exploration does not need treatment. Impairment and danger do. [7] [8]
Clinical & Bedside Assessment
1. Open and frame
Greet the young person first, set a joint agenda, then secure time alone. State conditional confidentiality with its limits out loud and check understanding. Without this frame, the assessment will return false negatives. [1] [4]
2. Run HEADSS/HEEADSSS
Work the domains with open then focused questions: Home, Education/Employment, Eating, Activities, Drugs, Sexuality, Suicide/mood/Safety, and strengths. Follow every positive lead deeper rather than ticking the box. [1]
3. Add validated screens where a lead appears
For substance use, apply CRAFFT or a frequency-based tool such as S2BI to stratify risk. For suicide, use ASQ or Columbia as a trigger, then move immediately to a full risk assessment if positive. A positive screen is a prompt for clinical thinking, never a diagnosis on its own. [2] [11] [4]
4. Assess suicide risk fully when mood is low
Cover ideation, plan, intent, prior attempts, access to means, protective factors, and the ability to keep safe until follow-up. A positive depression or suicide screen without this assessment is incomplete practice. [11] [12]
5. Build the risk formulation
Integrate the findings into a picture that names the drivers, the protective factors, and a risk tier. The formulation, not the screen score, drives the plan. Share it with the young person in plain language. [4] [7]
6. Document with care
Record enough for safety and continuity, and protect sensitive detail according to local record and portal rules. A billing or portal leak of confidential content is a system-level harm. [4]
Investigations
Most risk assessment needs few laboratory tests; it needs a thorough history and the right screens. Investigation is selective and history-led. [4]
Useful adjuncts include validated instruments (CRAFFT, S2BI, ASQ, Columbia, mood and anxiety scales), pregnancy testing when indicated, and STI testing matched to the sites and practices disclosed. For young people who inject drugs or have escalating opioid exposure, testing for blood-borne viruses and linkage to needle-syringe and opioid-substitution services are part of the work-up. [2] [10] [9]
Urine drug screening has a narrow, consent-governed role and is not a substitute for a confidential interview. Surprise or punitive testing damages trust and suppresses future disclosure. [4] [6]
Low-value patterns: routine broad blood panels on every asymptomatic adolescent; repeating STI panels without indication; treating a screen score as a diagnosis; punitive toxicology. [4]
Management — Resuscitation
A routine risk visit can become an emergency in one disclosure. Recognise the exit point and use it. [11]
- Stabilise physiology first: airway, breathing, circulation, glucose, and reversal of opioid toxicity with naloxone where indicated. [9]
- Secure immediate safety for suicide risk: remove access to means, do not leave the young person alone, and activate the crisis or mental-health pathway. [11] [12]
- Respond to disclosure of abuse, assault or exploitation by following local safeguarding and mandatory-reporting duties, sharing the minimum necessary and telling the young person what must happen and why. [5]
- Document the decisions, who was informed, and the safety plan. [4]
Naloxone is both a resuscitation drug and a harm-reduction tool: the same molecule that reverses an overdose today is the take-home dose that may reverse the next one. [9]
Management — Definitive & Stepwise
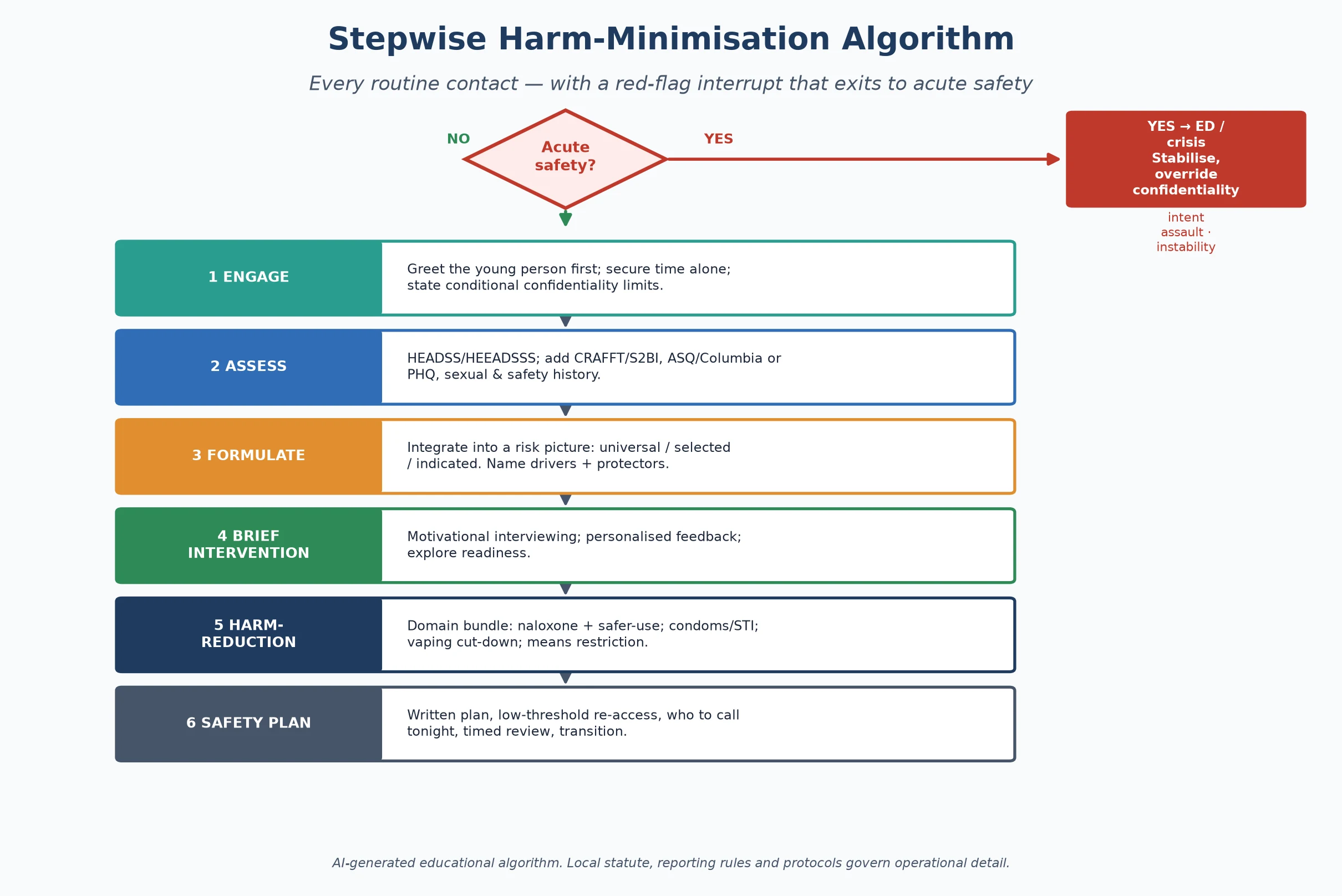
Read the figure like this: the red diamond is not decoration. Any acute-safety finding exits the routine path before you reach brief intervention. [11]
Stepwise routine pathway
- Engage and set the frame: time alone, conditional confidentiality, non-judgemental stance. [1]
- Assess: complete HEADSS/HEEADSSS, then add CRAFFT/S2BI, ASQ or Columbia, and sexual and safety history where leads appear. [2] [11]
- Formulate and stratify: name the drivers, protective factors and risk tier. [7]
- Brief intervention: use motivational interviewing, give personalised feedback, and explore readiness rather than lecture. [8]
- Harm-reduction bundle: offer the domain-specific measures below, matched to the tier and the stage of change. [5]
- Safety plan and follow-up: a written plan, low-threshold re-access, who to call tonight, and a timed review. [4]
Brief intervention technique
Motivational interviewing uses open questions, affirmation, reflective listening and summaries to help the young person articulate their own reasons for change. A meta-analysis shows benefit for adolescent health behaviours beyond substance use alone. The skill is to evoke, not to impose. [8]
Domain-specific harm-reduction bundle
Substance use
Overdose and dependence
- Take-home naloxone + overdose education
- Needle-syringe access and safe disposal
- Safer-use messaging; route and dose
- Opioid-substitution linkage where indicated
Sexual & reproductive
STI and pregnancy
- Condoms and contraception
- STI testing to disclosed sites
- PrEP eligibility discussion
- Emergency contraception access
Mental health & suicide
Self-harm
- Means restriction (lethal means counselling)
- Written safety plan
- Same-visit risk assessment
- Crisis-line and follow-up secured
Vaping & nicotine
Daily-use harm
- Cut-down rather than cold-turkey demand
- Address dependence and withdrawal
- Behavioural support
- Step-down where pharmacotherapy applies
Specific Subtypes & Scenarios
The fentanyl-era opioid exposure. A young person may be exposed to a potent opioid without intending to use one. Offer take-home naloxone and overdose education to the young person and, with consent, to family or peers, and linkage to treatment. [9] [5]
Injecting or escalating drug use. Needle and syringe provision, safe-disposal advice, and opioid-substitution treatment reduce blood-borne virus transmission and overdose death. Reviews of the evidence support these measures; they are clinical care, not moral endorsement. [10]
Suicide risk after a positive screen. Move from screen to structured risk assessment in the same visit. Means restriction — reducing access to lethal methods — is one of the most evidence-supported harm-reduction actions in suicide care. [11] [12]
Vaping and nicotine dependence. Meet daily-use harm with a cut-down plan and dependence management rather than an abstinence ultimatum that the young person cannot meet and then disengages. [7]
Sexual and reproductive risk. Offer condoms, contraception, STI testing matched to practices disclosed, and emergency-contraception access. Always ask about coercion separately — consent is not optional to assess. [5]
Youth justice and out-of-home care. Assume incomplete history, high trauma load, fragmented records, and elevated risk across every domain. Reconstruct the story actively and clarify consent. [6]
Rural, remote and telehealth. Dual relationships threaten confidentiality. On telehealth, deliberately create a private audio space and ask who else is in the room. [4]
Chronic disease clinics. Disease metrics are not a full risk assessment. Young people with chronic illness still need HEADSS, sexual-health and substance-use inquiry, and a transition plan. [6]
Complications & Pitfalls
- Demanding abstinence as the only acceptable outcome, then labelling relapse as failure. [5] [7]
- Running a screen and filing the result without acting on a positive lead. [4] [11]
- A judgemental or punitive stance that suppresses disclosure at the next visit. [6]
- Breaking confidentiality inappropriately, or refusing to break it when safety demands. [5]
- Missing exploitation, trafficking or coercion behind "risk-taking behaviour." [5]
- Confusing a screen score with a diagnosis, or using toxicology punitively. [4]
- Offering harm reduction for one domain while ignoring the others. [1]
Prognosis & Disposition
Prognosis here means the trajectory of risk and engagement, not a disease stage. [7]
Routine disposition: a complete low-risk visit with intact function and strong protective factors; brief reinforcement, a safety net, and a planned interval. [4]
Early-review disposition: new mood or substance concerns, unstable housing, recent relationship violence without current emergency, or an incomplete assessment needing a return visit with trust built. [6]
Urgent disposition: active suicide risk, overdose, assault, or medical instability — ED, crisis, or safeguarding as indicated, with follow-up loops closed. [11] [12]
Engagement is fragile across adolescence and young adulthood, so disposition should always name the next contact and a low-threshold way back in. Harm reduction succeeds when the young person returns. [5] [7]
Special Populations
Youth-justice-involved and out-of-home-care young people. Highest cross-domain risk, most fragmented records, most trauma. Lead with reconstruction of the history and clarification of consent. [6]
Gender and sexual diversity. Tailor sexual-health harm reduction to anatomy and practices, affirm identity, and watch for minority stress, bullying and family rejection. [5]
Indigenous young people. Cultural safety, connection to community, and racism as a health exposure matter as much as any screening tool. Partner with local services. [7]
Migrant and refugee youth. Use a professional interpreter for confidential content; family interpreters are not equivalent. Apply trauma-informed pacing. [6]
Neurodiverse and disabled young people. Offer easy-read materials, longer slots, sensory adjustments, and capacity assessment. Avoid overshadowing mental-health and substance risk. [4]
Socioeconomic disadvantage. Ask about food, transport, money and device access before attributing "non-adherence" to character. Harm reduction must be affordable and reachable. [7]
Evidence, Guidelines & Regional Differences
Risk-assessment instruments. HEADSS remains the foundational published psychosocial risk framework; services expand it as HEEADSSS without abandoning the core. CRAFFT is the most validated adolescent substance-use screen. The ASQ brings brief suicide screening into paediatric emergency settings. [1] [2] [11]
SBIRT. The American Academy of Pediatrics endorses screening, brief intervention and referral to treatment as a routine paediatric workflow, embedding brief intervention and referral into ordinary care rather than reserving it for specialist services. [4]
Harm reduction for young people. Recent paediatric statements set out the principles of harm reduction for young people who use drugs, arguing that pragmatic, non-judgemental, low-threshold care engages the highest-risk adolescents and lowers overdose, infection and disengagement. A public-health prevention framing makes the case explicitly. [5] [7]
Naloxone and injecting-drug harm reduction. Youth naloxone access is framed as the next frontier of adolescent harm reduction. Reviews of needle-syringe provision, opioid-substitution therapy and related interventions show evidence of reduced HIV and HCV transmission among people who inject drugs. [9] [10]
Brief intervention method. Motivational interviewing has meta-analytic support for adolescent health behaviours beyond substance use. [8]
Suicide risk stratification. Emergency-department screening and prediction tools can help stratify near-term suicide risk, but every positive result needs a same-visit clinical assessment. [11] [12]
Care integration. Integrating substance-use and harm-reduction care into primary care for adolescents and young adults is feasible and improves engagement, though staffing, funding and confidentiality-protection barriers persist. [6]
ANZ: youth-friendly confidential care culture, local consent and mandatory-reporting statutes, RCH-linked adolescent resources, and expanding take-home naloxone programs. UK: NICE self-harm and depression pathways; apply Gillick/Fraser capacity concepts with current local legal teaching; local safeguarding duties. US: AAP SBIRT policy, ASQ and Columbia dissemination, naloxone access laws that vary by state, and open-notes portal confidentiality tensions. Canada: CPS-aligned harm-reduction guidance and provincial consent variation; strong supervised-consumption and naloxone-access infrastructure in many regions.
Exam Pearls
- Open every answer with time alone + conditional confidentiality before any risk question. [1] [4]
- Define harm minimisation in one line: reduce adverse consequences of a risk behaviour even when the behaviour continues. [5]
- Name the tools by domain: CRAFFT/S2BI (substance), ASQ/Columbia (suicide), HEADSS (universal). [2] [11]
- Always pair a positive screen with same-visit clinical action, never "file and refer." [4] [11]
- Offer naloxone, condoms, cut-down plans and means restriction as named harm-reduction actions. [9] [5]
- Cite the dual-systems model to explain why abstinence-only fails and why harm reduction fits. [3]
- Ask about coercion and exploitation separately from "risk-taking." [5]
- State the principle that local statute governs consent ages, reporting triggers and naloxone laws — do not invent universal cut-offs. [4]
HARMLESS risk response
References
- [1]Cohen E, Mackenzie RG, Yates GL HEADSS, a psychosocial risk assessment instrument: implications for designing effective intervention programs for runaway youth. Journal of adolescent health : official publication of the Society for Adolescent Medicine, 1991.PMID 1772892
- [2]Knight JR, Sherritt L, Shrier LA, Harris SK, Chang G Validity of the CRAFFT substance abuse screening test among adolescent clinic patients. Archives of pediatrics & adolescent medicine, 2002.PMID 12038895
- [3]Steinberg L A Social Neuroscience Perspective on Adolescent Risk-Taking. Developmental review : DR, 2008.PMID 18509515
- [4]Levy SJ, Williams JF, COMMITTEE ON SUBSTANCE USE AND PREVENTION Substance Use Screening, Brief Intervention, and Referral to Treatment. Pediatrics, 2016.PMID 27325634
- [5]Kimmel SD, Gaeta JM, Hadland SE, Hallett E, Marshall BDL Principles of Harm Reduction for Young People Who Use Drugs. Pediatrics, 2021.PMID 33386326
- [6]Bagley SM, Hadland SE, Schoenberger SF, Gai MJ, Topp D, Hallett E Integrating substance use care into primary care for adolescents and young adults: Lessons learned. Journal of substance abuse treatment, 2021.PMID 34080547
- [7]Winer JM, Yule AM, Hadland SE, Bagley SM Addressing adolescent substance use with a public health prevention framework: the case for harm reduction. Annals of medicine, 2022.PMID 35900132
- [8]Cushing CC, Jensen CD, Miller MB, Leffingwell TR Meta-analysis of motivational interviewing for adolescent health behavior: efficacy beyond substance use. Journal of consulting and clinical psychology, 2014.PMID 24841861
- [9]Chadi N, Hadland SE Youth Access to Naloxone: The Next Frontier? The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 2019.PMID 31648752
- [10]MacArthur GJ, van Velzen E, Palmateer N, Kimber J, Pharris A, Hope V Interventions to prevent HIV and Hepatitis C in people who inject drugs: a review of reviews to assess evidence of effectiveness. The International journal on drug policy, 2014.PMID 23973009
- [11]Horowitz LM, Bridge JA, Teach SJ, Ballard E, Klima J, Rosenstein DL Ask Suicide-Screening Questions (ASQ): a brief instrument for the pediatric emergency department. Archives of pediatrics & adolescent medicine, 2012.PMID 23027429
- [12]Brent DA, Horowitz LM, Grupp-Phelan J, Bridge JA, Gibbons R, Chernick LS Prediction of Suicide Attempts and Suicide-Related Events Among Adolescents Seen in Emergency Departments. JAMA network open, 2023.PMID 36790810