Paeds · adolescent-and-young-adult-medicine
Eating disorders: refeeding and multidisciplinary care
Also known as Refeeding syndrome · Nutritional rehabilitation in anorexia nervosa · Family-based treatment · Maudsley model · Multidisciplinary eating-disorder care · Higher-calorie refeeding · Eating disorder inpatient management
A fellowship approach to refeeding the malnourished adolescent with an eating disorder and to the multidisciplinary team that carries recovery: refeeding-syndrome risk stratification and prevention, phosphate–magnesium–potassium and thiamine management, the conservative-versus-higher-calorie evidence, family-based treatment as first-line therapy, and tiered care across outpatient, day-program and inpatient settings across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 14-year-old girl is admitted at 71% median BMI after months of restriction. The temptation is to see the job as "feed her until she is a safe weight and send her home". That framing is how patients relapse, develop refeeding syndrome, or die. Refeeding an eating-disordered adolescent is two jobs done by one overlapping team: medical stabilisation — correcting the physiology so the body can tolerate food again — and nutritional rehabilitation — restoring weight and the psychological scaffold that keeps it on. The clinician who does only the first has failed. [1] [3]
Refeeding syndrome is the metabolic and electrolyte collapse that follows the reinstatement of nutrition after a period of deprivation. The trigger is carbohydrate: glucose drives an insulin surge, and insulin shifts phosphate, potassium and magnesium into cells. Serum phosphate falls first and most predictably, and a falling phosphate in the first days of feeding is the sentinel marker that the patient is refeeding too fast. The syndrome is preventable, and prevention — thiamine, electrolyte correction, a matched calorie start, and serial biochemistry — is the whole point of this topic. [3] [4]
The evidence base has moved. For decades the dogma was to start very low and advance slowly. A series of trials — the multicentre STRONG trial and its follow-ups — has shown that higher-calorie refeeding shortens admission and accelerates weight gain, provided monitoring is intensive and phosphate is replaced proactively rather than reactively. The modern answer is not "high calories for everyone" or "low calories for everyone"; it is risk-matched calories with monitoring matched to the dose. [7] [8] [6]
[9] [1]Classification
Start with the patient in front of you, then classify on the axes that change the refeeding plan: refeeding risk, disorder type, and level of care needed. [6]
Refeeding risk
A patient is at high risk of refeeding syndrome when several of these stack together: a very low %median BMI; little or no intake for more than a few days; rapid recent weight loss; already-low baseline phosphate, potassium or magnesium; purging, laxative or diuretic use; significant comorbidity; or alcohol misuse. A patient with none of these is lower risk. The distinction sets the calorie starting point, the thiamine route, and whether you check phosphate daily or twice-daily. Atypical anorexia — significant weight loss from a higher starting weight, now at a normal or higher BMI — carries the same refeeding risk and must not be reassured by the weight number. [6] [4]
Disorder type
The plan differs by diagnosis. Anorexia nervosa, restricting type is the archetypal refeeding challenge. Anorexia nervosa, binge-purge type adds purging-driven electrolyte loss and a different meal-plan structure. Atypical anorexia hides behind a normal weight. Bulimia nervosa rarely needs weight restoration; the work is normalising eating, usually as an outpatient. Avoidant/restrictive food-intake disorder (ARFID) needs nutritional rehabilitation without body-image distortion, framed around sensory and anxiety drivers rather than weight and shape. [1] [11]
Level of care
Care is tiered: outpatient for the medically stable and motivated; intensive outpatient or day program when outpatient is insufficient but admission is not yet needed; medical inpatient for instability, refeeding-syndrome risk that cannot be safely managed lower, or failure of outpatient care; psychiatric or specialist eating-disorder inpatient when the medical risk is managed but the mental illness is severe. The tier is chosen on medical stability, refeeding risk, psychological state, and the capacity of the family and local team — never on weight alone. [1] [11]
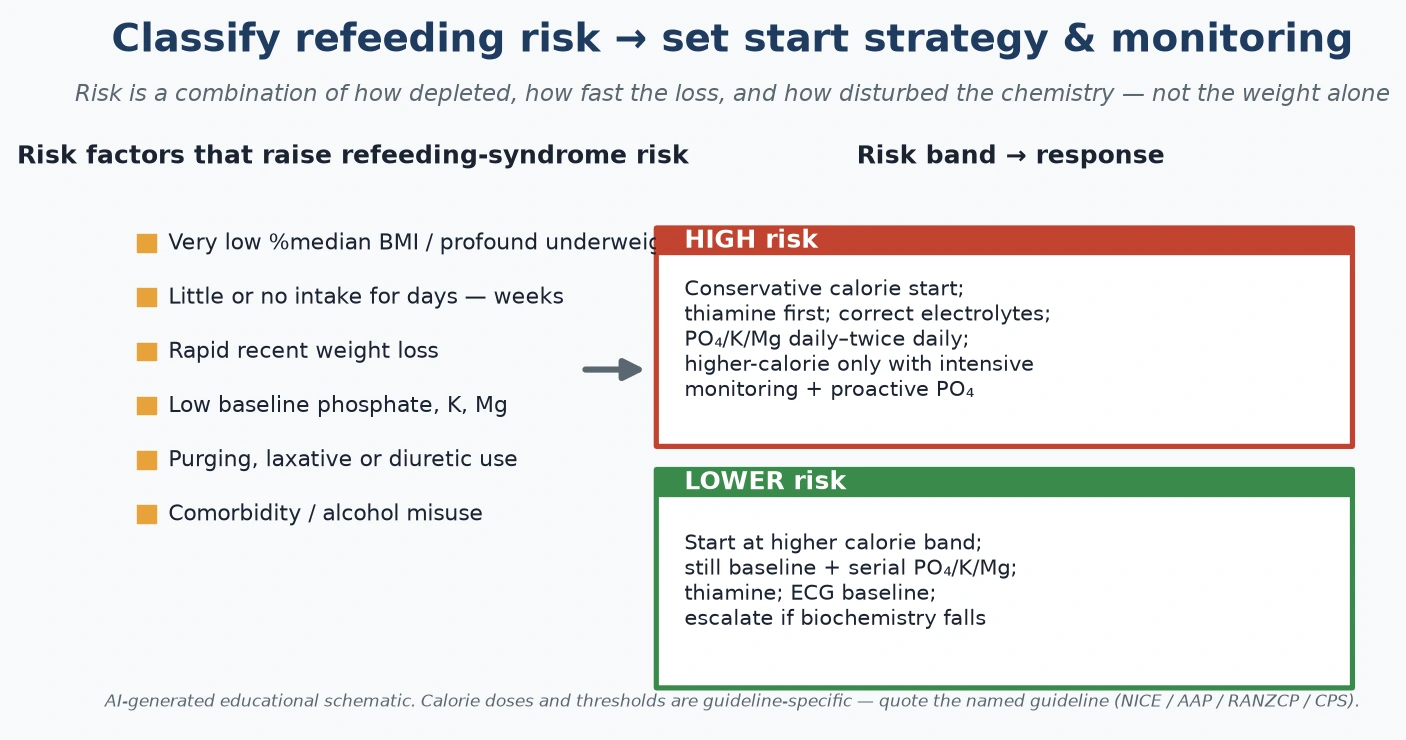
Read the figure like this: if you have not actively stacked the risk factors, you are guessing at the calorie start; if you have not checked baseline electrolytes, you cannot know your starting position; atypical anorexia belongs in the same risk grid as classic anorexia, not dismissed by the weight number. [6]
Epidemiology & Risk Factors
Eating disorders in young people are common and rising. British national surveillance found an incidence of around 1.4 per 100 000 for early-onset anorexia nervosa but, more importantly, documented a rise in presentations and a worrying number of medically unstable cases reaching specialist services late. The pattern is echoed across ANZ, North America and Europe: classic restricting anorexia persists, while atypical anorexia and ARFID are increasingly recognised, and the COVID-19 era accelerated presentations. [2] [1]
The risk of refeeding syndrome is not spread evenly. It concentrates in the profoundly underweight, the chronically starved, those who have lost weight rapidly, those who are already biochemically deranged, and those who purge or misuse laxatives, diuretics or alcohol. Hypophosphataemia during refeeding is common enough — a systematic review confirms it is the most frequent and most predictive biochemical disturbance — that every high-risk refeeding patient is assumed to be at risk until the biochemistry proves otherwise. [4] [5]
Mortality in anorexia nervosa is among the highest of any psychiatric disorder, driven by medical complications of starvation and by suicide. The modifier is early, coordinated, multidisciplinary care: outcomes are substantially better in adolescents than adults, and early intervention with family-based treatment changes the trajectory. Service factors matter too — specialist eating-disorder units and well-coordinated teams do better than fragmented general care, and rural and remote access gaps delay treatment. [1] [2]
Pathophysiology
To refeed safely you need a usable model of why refeeding hurts the patient who most needs it. The model is simple, and it predicts everything you monitor. [3]
During starvation, insulin is low and the body runs on fat and protein. Cells are depleted of phosphate, potassium and magnesium, but serum levels can look deceptively normal because the total body stores are run down — the deficit is hidden. Then you feed carbohydrate. Glucose drives a sudden insulin surge, and insulin does three things at once: it switches the cell back to glucose metabolism, it drives phosphate, potassium and magnesium into the cell for ATP synthesis and glycogen storage, and it promotes renal sodium and water retention. The serum phosphate — already precarious — falls. [3] [4]
Why phosphate? Because every cell rebuilding itself after starvation needs phosphate to make ATP and 2,3-diphosphoglycerate. The sudden metabolic demand strips phosphate from the blood faster than the depleted body can replenish it. Hypophosphataemia then expresses itself as the failure of every energy-hungry system: respiratory muscle weakness and respiratory failure, cardiac dysfunction and arrhythmia, rhabdomyolysis, haemolysis, and altered mental state. Potassium and magnesium follow the same intracellular shift and add their own arrhythmia risk. [3] [5]
Thiamine is the often-forgotten cofactor. Refeeding massively increases the demand for thiamine in carbohydrate metabolism, and a chronically malnourished patient is already depleted. Giving carbohydrate without thiamine can precipitate Wernicke encephalopathy — confusion, ataxia and ophthalmoplegia — which is why thiamine is given before or with the first feed in high-risk patients. Fluid retention, meanwhile, expands the extracellular space; in the thin, weak myocardium of a starved adolescent, that extra volume can tip into heart failure. [3]
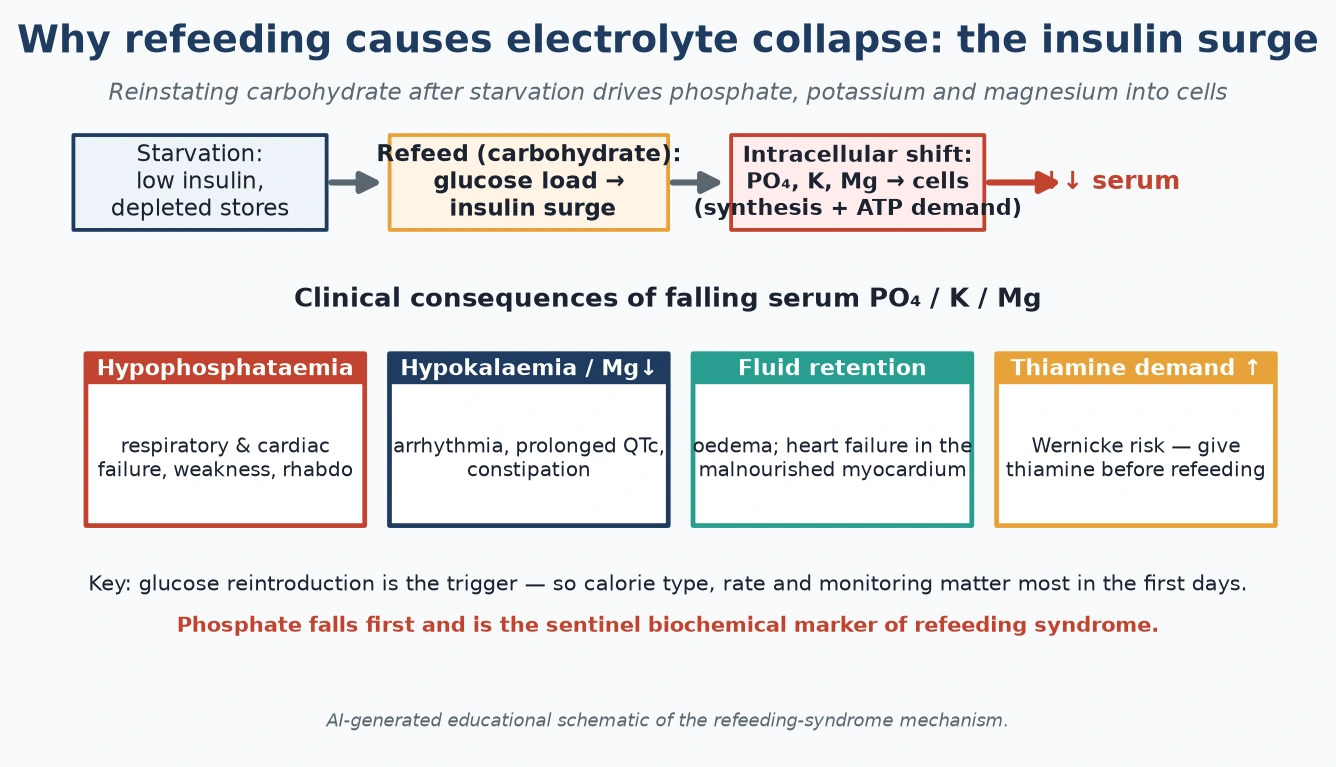
Read the figure like this: the trigger is the glucose load, so the levers you control are calorie type, calorie rate and the intensity of monitoring. Phosphate falls first and is the sentinel; monitor it before the patient tells you, with weakness or a falling respiratory rate, that it is too late. [3]
Clinical Presentation
The patient about to be refed usually arrives in one of three shapes, and the shape tells you the risk and the tempo. [1]
The medically unstable restricting patient presents with the physiology of starvation: bradycardia, hypotension, orthostatic rise in heart rate or fall in blood pressure on standing, hypothermia, dry skin with lanugo, peripheral acrocyanosis, and the cognitive blunting of chronic under-nutrition. Russell's sign (knuckle calluses from induced vomiting) marks a purging subtype. This is the patient in whom refeeding must be cautious and monitored, because the very act of feeding is the danger. [1] [11]
The developing refeeding syndrome declares itself in the first three to five days of feeding, and the first signal is usually in the biochemistry, not the bedside. A falling phosphate on the day-one or day-two bloods, with or without falling potassium or magnesium, is the warning. The clinical signs follow: oedema, palpitations, a new or widening tachycardia, weakness, and in the worst case respiratory compromise or arrhythmia. By the time these are obvious, the syndrome is advanced. [3] [4]
The behavioural presentation is the eating disorder intruding into the ward. Food rituals, covert exercise (in bed, in the bathroom, at night), water-loading before weigh-in, hiding or throwing away food, and post-meal vomiting are common and must be contained by consistent nursing practice. The atypical anorexia presentation is the trap: a patient at a normal or higher weight who has lost a large amount rapidly, with bradycardia and electrolyte disturbance, is at the same refeeding risk as the underweight patient and is routinely under-recognised. [1] [12]
[4] [3]Differential Diagnosis
In this topic the differential answers two questions: what else could this finding be, and what must I not miss alongside the refeeding. [1]
| Finding during refeeding | Consider alongside | Do not miss |
|---|---|---|
| Falling phosphate | Diuretic/laxative loss, DKA recovery, sepsis, alcohol withdrawal | Refeeding syndrome (the default in this setting) |
| New oedema | Cardiac failure, hypoalbuminaemia, water-loading by patient | Refeeding oedema; evolving heart failure in the malnourished myocardium |
| Tachycardia or arrhythmia | Anxiety, pain, dehydration, thyrotoxicosis | Hypokalaemia/hypophosphataemia arrhythmia; refeeding cardiomyopathy |
| Abdominal pain on feeding | Constipation, gastroparesis, early-satiety syndrome | Superior mesenteric artery syndrome; pancreatitis |
| Rapid weight gain | Genuine nutritional recovery | Water-loading; oedema rather than real tissue gain |
| Persistent confusion | Depression, medication effect | Wernicke encephalopathy (thiamine) |
Two traps recur. The first is attributing all deterioration to "expected refeeding" and missing sepsis, superior mesenteric artery syndrome (which complicates profound weight loss), or pancreatitis. The second is trusting the weight — a rapid gain may be water-loading or oedema rather than real recovery, and discharging on a falsely reassuring weight is a classic error. When in doubt, investigate; do not reassure on assumption. [1] [3]
Clinical & Bedside Assessment
The assessment has one aim: to quantify the risk so the refeeding plan fits, and to detect deterioration early. Do it the same way every time. [1]
1. Weight, height and %median BMI
Weigh in a gown, first thing, after voiding, with the same scales and the same nurse, watching for water-loading. Plot weight and height and calculate %median BMI — the ratio of the patient's BMI to the median BMI for age and sex. This single number frames the risk conversation. Examine for orthostatic vital signs: heart rate and blood pressure lying and standing. An orthostatic rise in heart rate (>20–30 bpm) or fall in blood pressure signals medical instability. [1]
2. Baseline biochemistry
Before the first feed, check phosphate, magnesium, potassium, sodium, urea and creatinine, glucose, liver function, full blood count, and consider zinc and vitamin D. Correct any baseline deficit before or as you start — refeeding a patient who is already hypophosphataemic or hypokalaemic is asking for the syndrome. A baseline ECG is mandatory: measure the QTc and look for bradycardia and low voltage. [1] [4]
3. Serial monitoring matched to risk
In high-risk refeeding, check phosphate, potassium and magnesium daily, and consider twice-daily in the first 48–72 hours of the highest-risk regimens. Daily weight, lying and standing heart rate and blood pressure, and temperature. Repeat the ECG if there is any biochemical derangement or new symptom. The monitoring intensity is dictated by the risk band and the calorie dose — higher calories demand more intense biochemistry. [4] [7]
4. Behavioural observation
The eating disorder does not leave the patient at the ward door. Supervise meals and the period after meals (to prevent vomiting), restrict exercise, monitor bathroom use, and weigh in a way that defeats water-loading. Consistency between nurses, doctors and the dietitian is the containment — inconsistency is exploited by the illness. [1]
5. Assess the family
Assess whether the family can do family-based treatment: their emotional capacity, their understanding, their availability. FBT asks parents to take full charge of their adolescent's nutrition for a time — a demanding task — and the bedside assessment of family readiness begins at admission, not at discharge. [9]
Investigations
Investigations serve two purposes: to stratify refeeding risk before you start, and to detect refeeding syndrome once you have. [4]
The baseline panel is phosphate, magnesium, potassium, sodium, urea, creatinine, glucose, liver function, full blood count, and calcium; zinc and vitamin D are reasonable additions. Each abnormality raises the risk and may need correction before feeding. The serial panel in high-risk refeeding is phosphate, potassium and magnesium daily (twice-daily in the first days of the highest-risk patients), with renal function and glucose as indicated. The ECG is baseline and as clinically indicated — a prolonged QTc is a danger signal that mandates cardiology input and correction of potassium and magnesium before proceeding. [4] [1]
Phosphate
Sentinel marker
- Falls first in refeeding
- Monitor daily in high-risk
- Replace proactively if falling
- Low → respiratory & cardiac failure
Potassium
Arrhythmia risk
- Insulin shifts K into cells
- Compounded by purging
- Monitor with phosphate
- Replace IV if symptomatic/low
Magnesium
Co-factor
- Depleted by starvation
- Hard to correct K without Mg
- Monitor alongside PO₄/K
- Replace to enable K correction
Thiamine
Give first
- Demand rises on refeeding
- Deficit → Wernicke
- Give before first feed
- Parenteral if high-risk
Additional tests are selective: troponin if there is chest pain or arrhythmia; amylase and lipase for abdominal pain (pancreatitis, or the spurious amylase rise of starvation); DEXA for bone density in persistent amenorrhoea; and zinc level where deficiency is suspected. In atypical anorexia, the investigations reveal the hidden risk that the weight number conceals — bradycardia, electrolyte disturbance, and the same refeeding vulnerability. [1] [12]
Management — Resuscitation
When refeeding syndrome declares itself, the response is immediate and protocolised. The principle is simple: stop the driver, replace what has fallen, protect the heart, and escalate. [3]
First, slow or pause the feed. If the phosphate is falling fast or the patient is symptomatic, reduce the calorie rate; a brief hold is reasonable in severe derangement while you correct. Do not abandon nutritional rehabilitation — the risk of starvation returns — but modulate the rate to what the biochemistry tolerates. Replace electrolytes intravenously for severe or symptomatic derangement: phosphate, potassium and magnesium per local protocol, recognising that magnesium must be adequate before potassium will correct. Give thiamine if it has not already been given, parenterally in the profoundly malnourished, because the patient may be precipitating Wernicke. [3] [4]
[3] [4]Manage fluid carefully. The malnourished myocardium cannot tolerate volume overload, so avoid aggressive fluid boluses; treat refeeding oedema with fluid restriction and slow feeding rather than diuretics in the first instance. Escalate to higher acuity — high-dependency or PICU — for haemodynamic instability, dangerous arrhythmia, respiratory failure, seizures or Wernicke encephalopathy. The resuscitation principle that trumps all others is the one in the build rule: never abruptly over-feed a high-risk patient, never start refeeding without baseline electrolytes and thiamine, and never ignore a falling phosphate. [3]
Management — Definitive & Stepwise
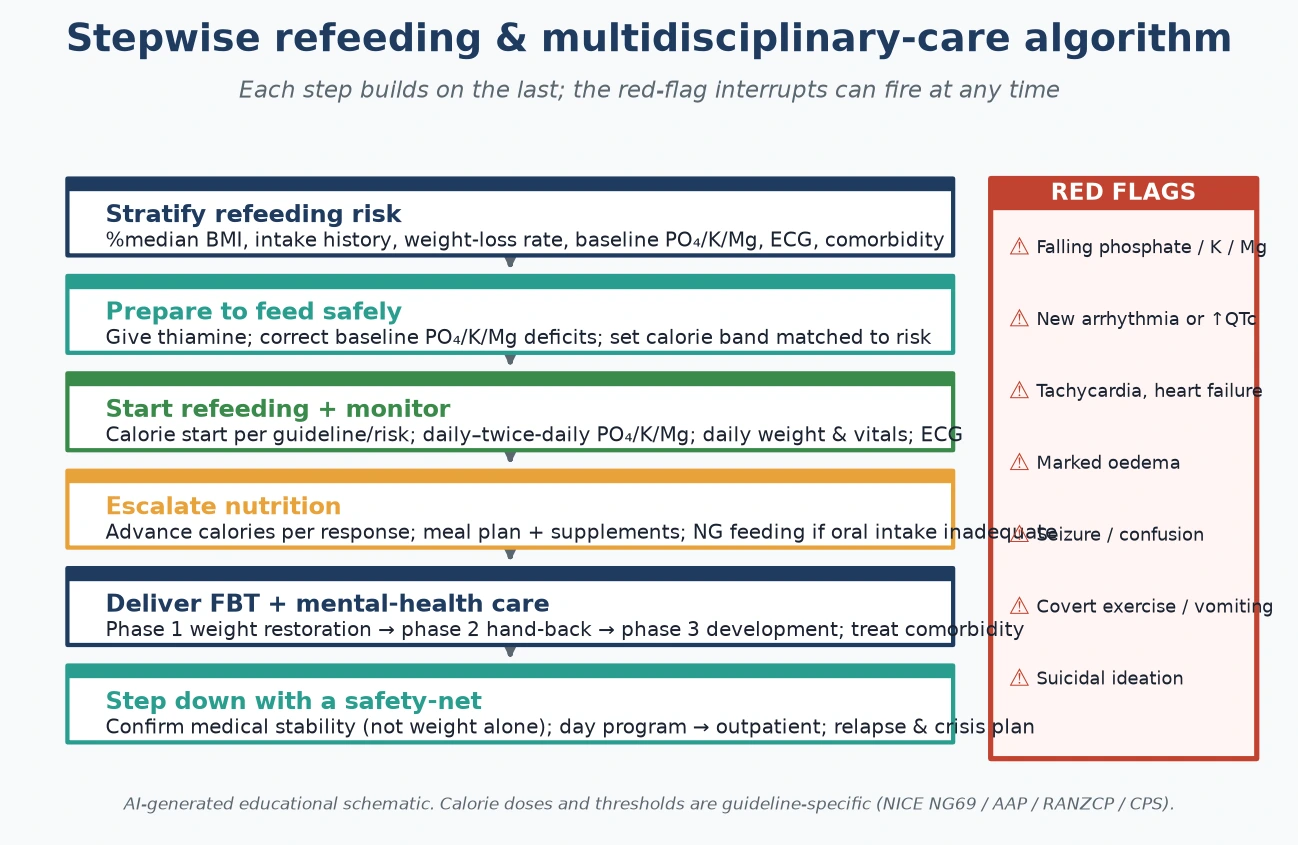
Definitive care is a stepwise protocol that builds risk-stratification, micronutrient cover, calorie escalation, psychological therapy and step-down into one coordinated plan. [6]
Step 1 — Risk-stratify and prepare
Stack the risk factors and assign a band. Correct any baseline phosphate, potassium or magnesium deficit. Give thiamine before or with the first feed (parenteral in high-risk). Set the calorie starting point matched to the risk. This is the preparation that makes the rest safe. [6] [3]
Step 2 — Start refeeding at a matched calorie level
There is no single universally agreed starting dose. The conservative historical approach begins at a low calorie level and advances slowly; the modern higher-calorie evidence begins higher. The multicentre STRONG trial and the 1-year outcomes RCT showed that higher-calorie refeeding achieves faster weight gain and shorter admissions — but only with intensive phosphate, magnesium and potassium monitoring and proactive replacement. The defensible position is to match the calorie band to the risk and the monitoring to the dose: a higher start is reasonable when the biochemistry can be watched and replaced intensively, and a conservative start remains right for the highest-risk, most depleted patient. Name your guideline (NICE NG69, AAP clinical report, RANZCP, CPS) and the trial you are relying on. [7] [8] [6]
STRONG — Study of Refeeding to Optimize Inpatient Gains
JAMA Pediatrics
Multicentre randomised clinical trial in adolescents and young adults hospitalised with anorexia nervosa
Key finding
Higher-calorie refeeding from the start achieved faster weight gain and shorter length of stay; safe when paired with intensive biochemical monitoring and proactive phosphate replacement.
Practice change
Higher-calorie refeeding is evidence-supported, but the safety precondition is monitoring and proactive electrolyte management — not simply feeding more.
Step 3 — Escalate nutrition with monitoring
Advance calories per the patient's biochemical and clinical response. Design a meal plan with the dietitian — structured meals and snacks, often supplemented with oral nutritional supplements, escalating the volume and energy density as tolerance improves. Where oral intake is insufficient or unsafe, nasogastric feeding bridges the gap; it is a tool, not a punishment, and is weaned as oral intake consolidates. Monitor phosphate, potassium and magnesium daily (twice-daily in the highest risk) and replace proactively. [1] [7]
Step 4 — Deliver family-based treatment and mental-health care
Psychological therapy runs in parallel from day one. Family-based treatment (FBT), the Maudsley model, is first-line for adolescent anorexia nervosa: a randomised trial showed it superior to adolescent-focused individual therapy for full remission. FBT has three phases. In phase 1 the parents take full, supported charge of the adolescent's nutrition to restore weight. In phase 2, as weight recovers and thinking clears, eating is gradually handed back to the adolescent. In phase 3 the focus shifts to normal adolescent development and identity beyond the eating disorder. The clinician's job is to coach the family through phase 1's resistance, which is expected and is not failure. [9] [1]
Step 5 — Step down with a safety-net
Confirm medical stability before discharge — and stability is not weight alone. It is stable vital signs without orthostasis, an acceptable heart rate, normalising biochemistry, a normal QTc, sustained weight gain on an oral plan, psychological readiness, and a family and outpatient team with the capacity to continue care. Step down to a day program or intensive outpatient, with a named clinician holding the longitudinal plan, a weight and biochemistry monitoring schedule, and a crisis and relapse pathway. [1] [11]
Pharmacotherapy
There is no drug licensed to restore weight in anorexia nervosa, and SSRIs do not treat the eating disorder itself at low weight. Olanzapine has some adjunctive evidence for weight gain and anxiety in anorexia nervosa and is used selectively. SSRIs have a role for genuine comorbid depression and anxiety once weight is restored. The pitfall is medicalising a relational illness: medication is an adjunct to refeeding and FBT, never a substitute for them. [10] [11]
Specific Subtypes & Scenarios
Each subtype reframes the same scaffold. [1]
Anorexia nervosa, binge-purge type layers purging-driven electrolyte loss onto refeeding risk: potassium and chloride depletion from vomiting and laxatives raise arrhythmia risk and demand closer electrolyte monitoring and a meal plan that does not trigger binges. Atypical anorexia — significant weight loss from a higher starting weight, now at a normal or higher BMI — is the most under-recognised high-risk subtype. The refeeding plan is the same as for classic anorexia at the same degree of physiological derangement; do not be reassured by the weight number. [12] [1]
Bulimia nervosa usually does not need weight restoration. The work is evidence-based cognitive-behavioural therapy for bulimia, normalising eating patterns, mostly as an outpatient; admission is reserved for medical instability or severe electrolyte disturbance. ARFID needs nutritional rehabilitation without body-image distortion: the psychological frame is sensory sensitivity, fear-based restriction and rigidity, often in a neurodivergent child, and the dietetic and psychological approach is adapted accordingly. [1] [11]
The treatment-resistant or severe-and-enduring patient reframes the goal. When full recovery is not achievable in the near term, the aim shifts to harm reduction, medical safety, quality of life and containment — a different ethical conversation that must be held openly with the patient and family, often with specialist eating-disorder and ethics input. The patient with comorbid diabetes (insulin omission, sometimes called "diabulimia") is doubly at risk: altered refeeding metabolism and diabetic complications, and needs joint endocrine and eating-disorder management from the outset. [1] [10]
Complications & Pitfalls
The complications cut both ways: under-treatment leaves the patient in the pathology of starvation; over-rapid refeeding causes the syndrome this topic exists to prevent. [3]
The medical complications of persistent starvation include osteoporosis and fragility fractures, growth failure and delayed puberty, amenorrhoea and infertility, refeeding relapse, and the cardiac and haematological derangements of severe malnutrition. The complications of over-rapid refeeding are refeeding syndrome itself — electrolyte collapse, arrhythmia, heart failure, oedema — and acute gastric dilatation from feeding too fast. The art is the corridor between them. [3] [1]
The classic errors are well catalogued. Starting calories too high in a high-risk patient without monitoring is the cardinal sin. Failing to give thiamine, chasing a falling phosphate reactively rather than preventing it, ignoring the ECG, and trusting water-loaded weights are the recurring failures. The procedural pitfalls include nasogastric tube complications and inconsistent containment of covert exercise and vomiting between staff — the illness thrives on inconsistency. [4] [3]
Before the first feed: STOP refeeding syndrome
STOP
%median BMI, intake, weight loss, baseline electrolytes, comorbidity
Give before or with the first feed
Baseline phosphate, potassium, magnesium, ECG; correct deficits first
The sentinel marker — monitor daily, replace proactively
The deepest pitfall is psychological: medicalising a disorder that is fundamentally relational. Stabilising the body and discharging without the family-based and psychological scaffold guarantees relapse — and relapse after each admission makes the next recovery harder. The medicolegal pitfall is treating a reluctant adolescent against their wishes: when life is at risk and capacity is impaired, the duty to treat — including life-saving feeding under legal authority where applicable — sits alongside the duty to engage the young person and family with respect and transparency. [9] [1]
Prognosis & Disposition
Prognosis in adolescent anorexia nervosa is better than the folklore suggests — provided care is early, coordinated and sustained. [9]
Roughly half to two-thirds of adolescents treated with early, family-based multidisciplinary care achieve full recovery, a minority run a chronic or relapsing course, and a small proportion do poorly. Predictors of better outcome include early age at intervention, shorter illness duration before treatment, family engagement, absence of binge-purge behaviour, and higher baseline weight. Predictors of worse outcome include late presentation, comorbidity, purging, and fragmented care. [9] [2]
Relapse after inpatient refeeding is common, and what reduces it is structured step-down — a day program or intensive outpatient — sustained FBT, and continuity of dietetic and psychological care. The long-term medical outlook with adequate weight restoration is encouraging: bone density can recover, reproductive function and menstruation return, and cardiovascular physiology normalises — but these recoveries are incomplete if weight is not sustained. [1] [9]
Disposition by medical stability
Medical inpatient — instability or high refeeding risk
Refeeding with monitoring; admit for the safety of the feed itself
Disposition is chosen on medical stability, refeeding risk, psychological state, and the capacity of the family and local team — never on weight alone. The safety-net after discharge is explicit: a named clinician holding the longitudinal plan, a weight and biochemistry monitoring schedule, and a crisis pathway for relapse. [1]
Special Populations
The scaffold is constant; the adjustments are in the team and the frame. [1]
The profoundly underweight and chronically starved are the highest refeeding-syndrome risk: the most conservative start, the most intensive monitoring, and the lowest threshold for proactive electrolyte replacement and high-dependency escalation. Neurodivergent young people — autism, ADHD — often present with ARFID framed by sensory sensitivity and rigidity rather than body-image distortion; the dietetic and psychological approach must be adapted, and a generic body-image FBT model can misfire. [1] [11]
Gender-diverse youth bring the added complexity of weight and body composition in the context of gender dysphoria: weight restoration may intensify gender distress, and the team must hold both the eating disorder and the gender-affirming frame without one displacing the other. Indigenous, migrant and refugee, and rural-remote access factors change the MDT plan: telehealth, cultural safety, distance from specialist services, and the involvement of family and community can determine whether the plan survives discharge. [1]
Young people in out-of-home care or youth justice carry attachment disruption and a fundamental question for FBT — who holds the "family" role when family is fractured? A trusted adult, a carer or a worker may take that role, and continuity of that relationship across placements is the scaffold that prevents relapse. The pre-adolescent child and the older young person approaching transition to adult services need age-adapted frames: family-led care is even more central in the youngest, and structured transition planning is essential for the oldest to avoid the well-documented cliff-edge at transfer. [9] [1]
Evidence, Guidelines & Regional Differences
The landmark evidence has reshaped refeeding practice in the last decade, and the regional guidelines are converging on its implications while still differing in operational detail. [7]
The STRONG multicentre randomised trial established that higher-calorie refeeding in hospitalised adolescents with anorexia nervosa achieves faster weight gain and shorter stays than a conservative start, with no excess of complications when paired with intensive phosphate, magnesium and potassium monitoring and proactive replacement. The 1-year follow-up confirmed durable weight outcomes. The FBT randomised trial established family-based treatment as superior to adolescent-focused individual therapy for adolescent anorexia nervosa, anchoring it as first-line. The systematic reviews of refeeding approaches and of refeeding hypophosphataemia frame the monitoring that makes higher calories safe. [7] [8] [9] [4]
The regional guidelines agree on the principles — risk-stratify, give thiamine, correct electrolytes, monitor biochemistry, deliver FBT — and differ on the operational calorie doses. NICE NG69 (UK) and the Junior MARSIPAN framework give detailed, conservative, risk-banded refeeding and admission criteria. The AAP clinical report (US) and the APA practice guideline frame assessment, medical management and the evidence base. The RANZCP clinical practice guidelines (ANZ) and CPS guidance (Canada) set the regional standard for tiered care and team composition. The defensible practice is to name the guideline you follow and match the calorie dose and monitoring to the patient's risk band and your service's capability — not to apply a memorised universal number. [1] [11] [10]
| Region | Guideline frame | Operational note |
|---|---|---|
| ANZ | RANZCP clinical practice guidelines | Tiered MDT care; FBT first-line; telehealth bridges rural/remote gaps; services unevenly distributed |
| UK | NICE NG69 and Junior MARSIPAN | Detailed, risk-banded refeeding and admission/discharge criteria; conservative start with intensive monitoring is the default |
| US | AAP clinical report and APA practice guideline | STRONG trial (US centres) drives the shift to higher-calorie refeeding with intensive monitoring |
| Canada | Canadian Paediatric Society guidance | Tiered care; consent and the legal authority to feed a reluctant adolescent follow provincial statute |
The evidence is still maturing. The optimal precise calorie start dose by risk band, the ideal phosphate replacement schedule, the equivalence of day-program and inpatient for moderate cases, and the long-term outcomes of higher-calorie protocols remain areas of active study. Where the evidence is weak, the principle holds: risk-match the calories, monitor the biochemistry, and replace proactively. [6] [4]
Exam Pearls
- Refeeding syndrome is driven by the insulin surge of reinstated carbohydrate: phosphate, potassium and magnesium shift intracellularly — phosphate falls first and is the sentinel marker. [3]
- Give thiamine before or with the first feed in high-risk patients; replace phosphate proactively, not reactively after the patient collapses. [3] [4]
- Family-based treatment (the Maudsley model) is first-line psychological therapy for adolescent anorexia nervosa; no drug is licensed to restore weight. [9] [10]
- Higher-calorie refeeding (STRONG trial and 1-year outcomes) shortens admission and accelerates weight gain — but only with intensive phosphate, magnesium and potassium monitoring and proactive replacement. [7] [8]
- QTc prolongation and bradycardia are the cardiac signals; the malnourished myocardium cannot tolerate fluid overload — be cautious with fluids and never over-resuscitate. [1] [3]
- Atypical anorexia carries the same physiological and refeeding risk at a normal or higher weight — do not be reassured by the number. [12]
- Medical stability for discharge is not weight alone: stable vital signs without orthostasis, normalising biochemistry, normal QTc, sustained oral weight gain, and a family and team with capacity. [1]
- The eating disorder is relational: discharging a stabilised patient without the family-based and psychological scaffold is a planned relapse. [9]
References
- [1]Rosen DS; American Academy of Pediatrics Committee on Adolescence Identification and management of eating disorders in children and adolescents. Pediatrics, 2010.PMID 21115584
- [2]Nicholls DE; Lynn R; Viner RM Childhood eating disorders: British national surveillance study. British Journal of Psychiatry, 2011.PMID 21972279
- [3]Mehanna HM; Moledina J; Travis J Refeeding syndrome: what it is, and how to prevent and treat it. BMJ, 2008.PMID 18583681
- [4]O'Connor G; Nicholls D Refeeding hypophosphatemia in adolescents with anorexia nervosa: a systematic review. Nutrition in Clinical Practice, 2013.PMID 23459608
- [5]Ornstein RM; Golden NH; Jacobson MS; Shenker IR Hypophosphatemia during nutritional rehabilitation in anorexia nervosa: implications for refeeding and monitoring. Journal of Adolescent Health, 2003.PMID 12507806
- [6]Garber AK; Sawyer SM; Golden NH; Guarda AS A systematic review of approaches to refeeding in patients with anorexia nervosa. International Journal of Eating Disorders, 2016.PMID 26661289
- [7]Garber AK; Cheng J; Accurso EC; Adams SH Short-term Outcomes of the Study of Refeeding to Optimize Inpatient Gains for Patients With Anorexia Nervosa: A Multicenter Randomized Clinical Trial. JAMA Pediatrics, 2021.PMID 33074282
- [8]Golden NH; Cheng J; Kapphahn CJ; Buckelew SM Higher-Calorie Refeeding in Anorexia Nervosa: 1-Year Outcomes From a Randomized Controlled Trial. Pediatrics, 2021.PMID 33753542
- [9]Lock J; Le Grange D; Agras WS; Moye A Randomized clinical trial comparing family-based treatment with adolescent-focused individual therapy for adolescents with anorexia nervosa. Archives of General Psychiatry, 2010.PMID 20921118
- [10]American Psychiatric Association Treatment of patients with eating disorders, third edition. American Psychiatric Association. American Journal of Psychiatry, 2006.PMID 16925191
- [11]Hay P; Chinn D; Forbes D; Madden S Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the treatment of eating disorders. Australian and New Zealand Journal of Psychiatry, 2014.PMID 25351912
- [12]Accurso EC; Cheng J; Machen VI; Buckelew S Hospital-based higher calorie refeeding and mealtime distress in adolescents and young adults with anorexia nervosa or atypical anorexia nervosa. International Journal of Eating Disorders, 2023.PMID 36919264