Paeds · allergy-and-immunology
Immunoglobulin replacement and antimicrobial prophylaxis
Also known as Immunoglobulin replacement therapy · IVIG and SCIG · Antibody replacement · Prophylactic antibiotics in immunodeficiency · Infection prophylaxis in primary immunodeficiency
A fellowship approach to immunoglobulin replacement and antimicrobial prophylaxis in children with antibody deficiency: confirm the defect and the functional need before committing to lifelong immunoglobulin, choose the route (intravenous versus subcutaneous) around the family's life and the trough goal, dose to clinical outcome rather than a number alone, layer antimicrobial prophylaxis where immunoglobulin is insufficient or not indicated, and protect the lung and the transition to adult care.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A six-year-old boy with X-linked agammaglobulinaemia has been on intravenous immunoglobulin since infancy, dosed every four weeks in a hospital two hours from his home. He has had three breakthrough pneumonias this year despite a trough IgG that looks acceptable on paper. Two questions now decide his future. First, is the trough the wrong target — should his regimen be driven by his infection rate rather than the number? Second, would a switch to home subcutaneous immunoglobulin give him the steady troughs and the life back that his current regimen cannot? Holding those two questions together — dose to outcome, fit the route to the family — is the whole skill of this topic. [2] [7]
D.O.S.E. U.P.
Overview & Definition
Immunoglobulin replacement is the regular administration of pooled human immunoglobulin G to restore the antibody that a child with a significant antibody deficiency cannot make for themselves. Antimicrobial prophylaxis is the scheduled use of an antibiotic, antiviral, or antifungal agent to prevent infection in a child whose immune system cannot reliably clear it. The two are used together, in sequence, or alone, depending on the defect, the infection burden, and the child's response. [1]
The unifying principle is that treatment is matched to a proven functional need, never to a number alone. Immunoglobulin replacement carries real costs and real risks — infusion reactions, headache, the rare but serious thrombotic, haemolytic, and renal events, line-related infection, and the dependence of a child on a blood product for life. Starting it without a confirmed defect trades a reversible or self-limiting problem for a permanent one. The same logic applies in reverse: a child with a real defect who is under-dosed to a textbook trough will keep infecting their lung. [2] [3]
The indications, dosing, and route choice rest on a defined evidence base. The American Academy of Allergy, Asthma and Immunology Primary Immunodeficiency Committee reviews, first in 2006 and updated in 2017, set out who benefits from immunoglobulin and on what evidence; the 2015 practice parameter frames the diagnostic and management standard; and the 2022 International Union of Immunological Societies classification names the conditions that qualify. A fellowship answer is built on these sources, not on a single regimen memorised from a formulary. [1] [4]
Classification
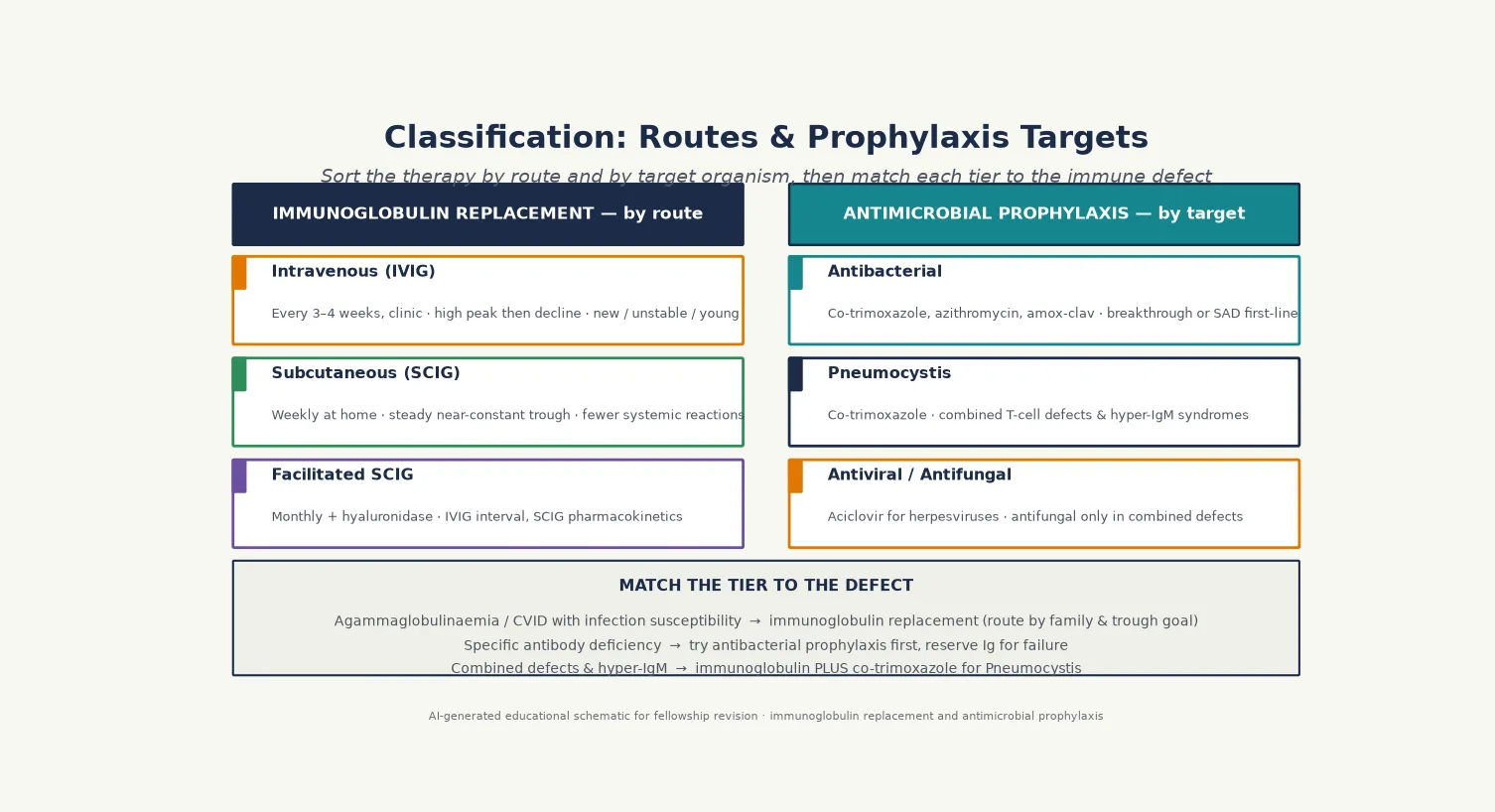
Sort the therapy along two axes: what you give, and how you give it. Immunoglobulin replacement is classified by route, and antimicrobial prophylaxis is classified by the organism it targets. [2]
Intravenous immunoglobulin (IVIG) is infused into a peripheral or central line every three to four weeks in a clinic or hospital. It produces a high peak followed by a slow decline, and it is the original modality. Subcutaneous immunoglobulin (SCIG) is infused into the subcutaneous tissue of the abdomen or thighs, usually weekly, using a pump or rapid push. It produces steady, near-constant trough levels, and it is increasingly the preferred modality for stable, trained patients. Facilitated subcutaneous immunoglobulin adds recombinant hyaluronidase to a single monthly infusion that opens the subcutaneous space, bridging the convenience of an IVIG interval with the steady pharmacokinetics of the subcutaneous route. [3] [9]
Antimicrobial prophylaxis is classified by target. Antibacterial prophylaxis — most often co-trimoxazole, azithromycin, or amoxicillin-clavulanate — suppresses the sinopulmonary and gastrointestinal organisms that antibody deficiency cannot clear. Pneumocystis prophylaxis with co-trimoxazole is reserved for combined T-cell defects and the hyper-IgM syndromes, where cellular immunity is also impaired. Antiviral prophylaxis (aciclovir or valaciclovir) covers chronic or recurrent herpesvirus infection, and antifungal prophylaxis is added only in the combined defects where mould and yeast are a genuine risk. The choice is driven by the immune defect, not by a blanket protocol. [4] [6]
Epidemiology & Risk Factors
The epidemiology of immunoglobulin replacement is the epidemiology of the antibody deficiencies it serves, and the headline is that antibody defects dominate the primary immunodeficiency burden. The European Society for Immunodeficiencies internet database, reporting results from 2006 to 2008, showed that predominantly antibody deficiencies make up the largest single category of registered inborn errors of immunity — which is why this therapy, though given to individually rare children, is collectively common in immunology practice. [10]
The children who receive immunoglobulin are a selected subset of that burden. The clearest indications are the agammaglobulinaemias (X-linked agammaglobulinaemia and its autosomal recessive mimics) and common variable immunodeficiency with documented infection susceptibility. Together these account for the majority of paediatric immunoglobulin recipients, with the hyper-IgM syndromes and some combined defects making up much of the remainder. The risk profile that brings a child to replacement is recurrent, persistent, severe, or unusual infection — the same pattern that earned the immunoglobulin work-up in the first place. [1] [4]
Two groups are at the opposite risk — the children in whom immunoglobulin is the wrong answer. Transient hypogammaglobulinaemia of infancy, with its preserved vaccine response and self-limiting course, accounts for a meaningful fraction of low-IgG referrals in early childhood and should never reach replacement if the diagnosis is correct. Selective IgA deficiency, the commonest primary antibody defect overall, is managed without immunoglobulin in the great majority, with only a small subset of symptomatic children needing any therapy at all. [1]
Pathophysiology
The rationale for immunoglobulin replacement is metabolic, not symbolic: a child who cannot make antibody is given antibody, and the dose is chosen to keep the circulating level high enough to opsonise and neutralise the organisms that antibody handles. Understanding the pharmacokinetics of each route is what lets you dose to outcome rather than to a textbook number. [3]
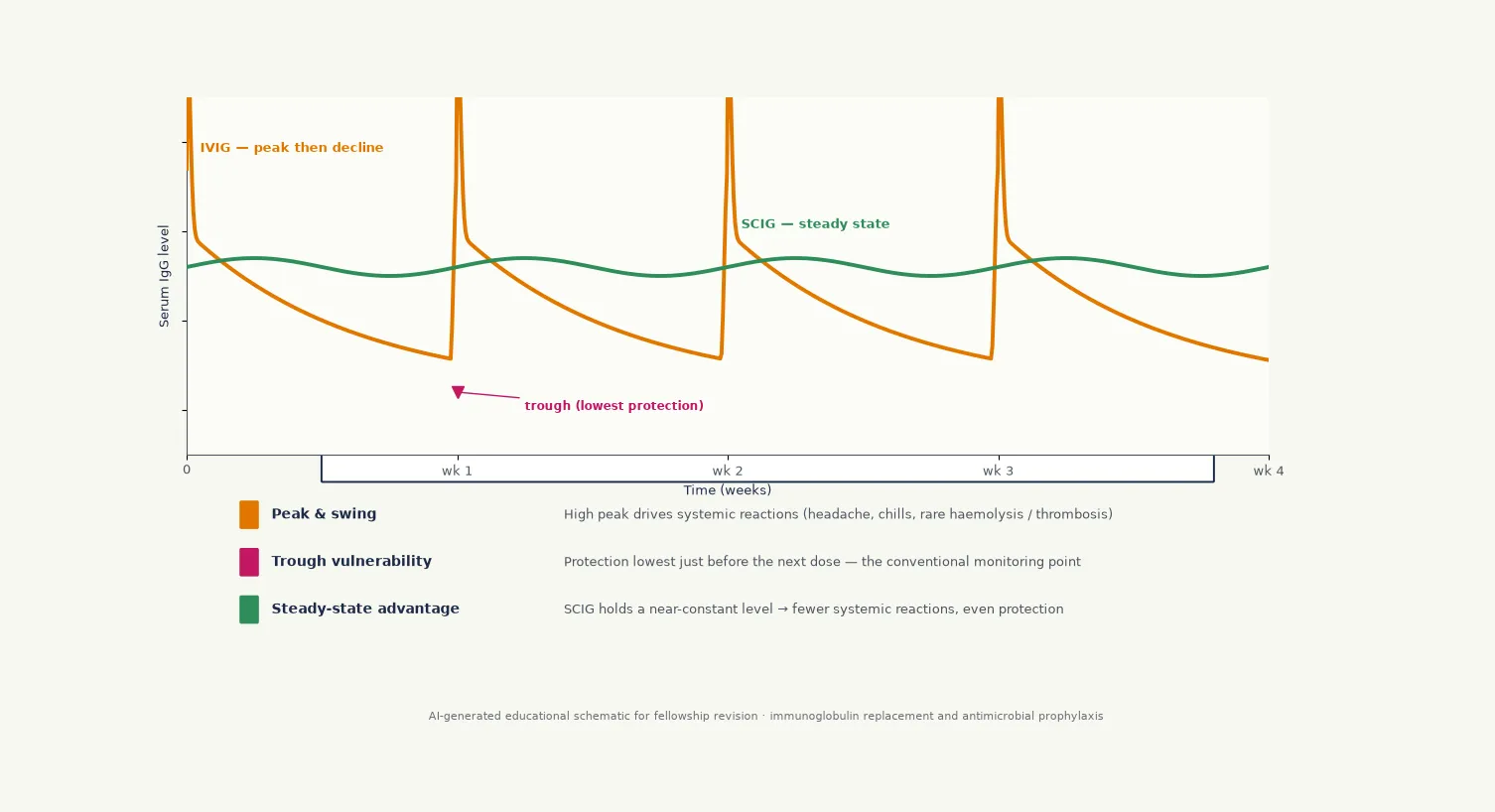
After an intravenous infusion, immunoglobulin G rises to a peak within hours and then declines exponentially, with a half-life of around three to four weeks in most patients. The trough — the level just before the next dose — is the conventional monitoring point, because it represents the lowest protection the child experiences in the cycle. The weakness of the trough as the sole target is that it ignores the peak and the infection rate: a child can sit at an "acceptable" trough and still break through if their individual metabolic handling or their exposure is high. [2]
Subcutaneous immunoglobulin flattens this curve. Because it is absorbed slowly from the subcutaneous depot, the peak is modest and the trough is steady, with far less swing between doses. The pharmacokinetic studies of a 20% subcutaneous immunoglobulin in North American patients with primary immunodeficiency confirmed the steady-state profile, the absence of the high peaks that drive systemic reactions, and the bioequivalence of the weekly dose to the monthly intravenous dose. This pharmacokinetic advantage is the mechanistic basis for the better-tolerated, home-based regimens that have shifted practice over the last decade. [5]
Antimicrobial prophylaxis works on a different mechanism entirely. Antibacterial agents suppress the bacterial load at the mucosal surfaces that antibody would normally clear, buying time and reducing the frequency of breakthrough infection. The rationale in specific antibody deficiency is that the defect is purely functional — immunoglobulin is present but does not work — so adding more antibody through replacement is a poor first move, whereas suppressing the organisms the defective antibody cannot clear is rational. This mechanism is why the comparison of prophylactic antibiotics against immunoglobulin in specific antibody deficiency is the decisive evidence in that condition. [6]
Clinical Presentation
The clinical presentation that earns immunoglobulin replacement is not the therapy itself but the infection pattern that brought the child to immunology: recurrent, persistent, severe, or unusual infection, most often of the sinopulmonary tract. A fellowship answer on this topic is built on recognising which presentations justify starting, which justify escalating, and which signal that the current regimen is failing. [1]
The child who needs to start immunoglobulin presents with proven infection susceptibility alongside a confirmed antibody defect — the boy with X-linked agammaglobulinaemia and his second pneumonia, the teenager with common variable immunodeficiency and chronic sinusitis punctuated by bronchitis. The defect has been quantified, the functional vaccine response is impaired, secondary causes are excluded, and the infection burden is real. This is the presentation the 2017 evidence review addresses directly. [2]
The child who needs to escalate presents with breakthrough infection despite an apparently adequate regimen. New or recurrent pneumonia, chronic diarrhoea, or the appearance of bronchiectasis in a child already on immunoglobulin is a signal to reassess, not to reflexively raise the dose. The questions are whether the trough target is wrong for this individual, whether adherence or timing is the problem (especially with home SCIG), whether an anatomical or different immune component is now contributing, and whether antimicrobial prophylaxis should be added. [3]
The child who is being considered for immunoglobulin but should not receive it presents with a number but no functional defect. A thriving infant with transient hypogammaglobulinaemia of infancy, a well child with isolated low IgA, or a patient with a secondary cause that will resolve all fall in this group. The presentation is a laboratory value; the skill is to resist treating the value and to treat the child instead. [1] [4]
Differential Diagnosis
The differential in this topic is not a list of diseases but a list of reasons a child on immunoglobulin might still be unwell, and a list of conditions that mimic the need for it. Thinking through both is what protects the child from both under- and over-treatment. [1]
When a child on immunoglobulin keeps infecting, consider the regimen first. Non-adherence and dose-timing drift are the commonest culprits in home subcutaneous therapy, and a frank conversation with the family often surfaces them before any laboratory change. A trough measured at the wrong point in the cycle, or an individual whose half-life is shorter than average, can produce a misleadingly reassuring level. An inadequate trough target for that child's infection pattern is a third, and it is the only one solved by raising the dose. [3]
When the regimen is sound, consider that the immune defect has broadened. Some combined defects declare themselves over time, adding cellular failure to a predominantly antibody picture; the hyper-IgM syndromes do this when the T-cell component is significant. An anatomical cause — bronchiectasis already established before therapy began, or an airway anomaly — can drive recurrent infection independent of the antibody level. A different organism, including an opportunist, signals that the immune defect is wider than antibody alone. [4] [6]
The other differential is the child who looks as though they need immunoglobulin but does not. Transient hypogammaglobulinaemia of infancy, selective IgA deficiency without infection susceptibility, secondary antibody loss from nephrotic syndrome or protein-losing enteropathy, and the immunosuppressive effects of malignancy treatment all produce low immunoglobulin without justifying lifelong replacement. The functional vaccine response and the exclusion of secondary causes keep this differential honest. [1]
| Pattern | Likely reason | Key discriminator and action |
|---|---|---|
| Steady trough, but recurrent pneumonia | Adherence or timing drift in home SCIG | Reconcile doses with the family; recheck trough at the correct cycle point |
| Normal IgG, new opportunistic infection | A combined defect emerging beneath the antibody defect | Repeat lymphocyte subsets; add Pneumocystis prophylaxis if indicated |
| Clubbing and daily sputum despite therapy | Established bronchiectasis predating control | Chest CT, intensive physiotherapy, respiratory team input |
| Low IgG, well child, preserved vaccine response | Transient hypogammaglobulinaemia of infancy — do not treat | Observe; the value normalises by age three to four years |
Clinical & Bedside Assessment
The bedside task for a child on, or being considered for, immunoglobulin is to match the therapy to the evidence and the family, and to detect the early signs that the regimen is failing. Begin with the threat gate: breakthrough infection, faltering growth, or new structural lung disease in an established patient is a reassessment trigger, not a routine review. [2]
The history is the instrument that decides the trough target. Document the number, site, severity, and documented microbiology of every infection since the last review, and whether each required oral or intravenous antibiotics or admission. Ask the family exactly how the home therapy is given — who infuses, on which day, at what rate, and what happens to missed doses — because the answer often explains a trough that looked fine on paper. Take a developmental and growth history, because faltering growth alongside breakthrough infection changes the threshold to escalate immediately. [9]
The examination carries the signs of complication. Measure growth and plot it, because the centile trajectory is a vital sign in chronic immunodeficiency. Look for clubbing, chest wall deformity, and localised crackles that signal bronchiectasis, and examine the infusion sites for the local reactions that distinguish subcutaneous from intravenous therapy. Look for the features of a broader immune defect — candidiasis, oral ulcers, lymphadenopathy, hepatosplenomegaly — that would shift the diagnosis and the prophylaxis. [3]
Assess the family's practical context at every visit. A child in a remote community, a refugee family, or a household with socioeconomic disadvantage may have the regimen that fits the textbook but not their life, and adherence will fail silently in that gap. Home subcutaneous therapy, where the family can be trained and supported, is often the route that closes that gap — but only if the family's capacity is assessed honestly and the support is real. [8] [9]
Investigations
The investigations for a child on immunoglobulin replacement are monitoring tools rather than diagnostic ones, and they answer two questions: is the trough adequate for this child, and is the lung being protected? [1]
Trough immunoglobulin G is the principal monitoring test. Measure the IgG just before the next dose — for IVIG, in the days before the infusion; for SCIG, at a steady point in the weekly cycle. The aim is a trough within or above the normal range for age, individualised to the infection pattern. A trough that sits at the lower end of normal in a child who keeps breaking through is not adequate for that child, and the dose should rise even if the number looks "acceptable." The 2017 review is explicit that the dose should be titrated to the clinical outcome, with the trough as a guide rather than a ceiling. [2]
Lung surveillance is the second investigation stream. Baseline spirometry in cooperative children, repeated annually, tracks the lung function trajectory that predicts structural disease. Low-dose chest computed tomography, performed when bronchiectasis is suspected or at defined intervals, documents structural change and guides the intensity of therapy. The aim is to detect bronchiectasis early, because established bronchiectasis is the single largest determinant of long-term morbidity in antibody deficiency and the strongest argument for getting the regimen right. [3]
Re-characterisation of the immune defect belongs in the child who breaks through. Repeat lymphocyte subsets, revisit the functional vaccine response where appropriate, and consider next-generation sequencing if the original genetic diagnosis is incomplete or a combined defect is suspected. The point is to detect a defect that has broadened beyond antibody, because that changes the prophylaxis — most importantly, it brings in Pneumocystis prophylaxis with co-trimoxazole. [4] [6]
Adverse-effect monitoring completes the set. Check a full blood count and renal function periodically, because the rare haemolytic and renal events of immunoglobulin are detectable early. Document any infusion reaction, headache, or thrombotic event, because these drive a route switch or a rate reduction. The safety profile of the 20% subcutaneous immunoglobulin preparations, with their low systemic reaction rate, is part of why the subcutaneous route has expanded — but no route is risk-free, and monitoring is continuous. [5]
Management — Resuscitation
Resuscitation in a child on immunoglobulin means treating acute infection safely while avoiding the harms that are specific to this group: anaphylaxis on blood products in IgA-deficient patients, and the systemic adverse effects of immunoglobulin itself. [3]
A child presenting with acute severe infection receives the standard paediatric sepsis pathway: prompt cultures, empirical intravenous antibiotics, and fluid and oxygen as required. The microbiology is guided by the defect and the documented organisms — encapsulated bacteria in pure antibody deficiency, opportunists in combined defects. Empirical cover should be broadened when an opportunistic organism is suspected. The antibiotic choice takes the child's prophylactic regimen into account, because a child already on co-trimoxazole or azithromycin prophylaxis needs a different empirical agent for a breakthrough infection. [1] [6]
The immunoglobulin-specific resuscitation hazard is anaphylaxis in selective IgA deficiency. Some IgA-deficient patients develop anti-IgA antibodies that can trigger anaphylaxis on exposure to IgA-containing blood products, including — rarely — immunoglobulin preparations themselves. If a patient with known IgA deficiency and anti-IgA antibodies needs transfusion or immunoglobulin, use an IgA-depleted product and ensure the team is aware of the risk. This is a reminder that selective IgA deficiency is usually a reason not to give immunoglobulin, not a reason to give it. [3]
The second resuscitation hazard is the adverse-effect cluster of intravenous immunoglobulin: severe headache, aseptic meningitis, haemolysis, thrombosis, and renal impairment. A child who develops severe headache or chest symptoms during or after an infusion needs the infusion slowed or held, hydration, and assessment for these events. The systemic reaction rate is substantially lower with subcutaneous immunoglobulin, which is one of the reasons a child with recurrent infusion reactions on IVIG is a candidate for a route switch. [2] [5]
Resuscitation of the family's understanding matters as much as the medical resuscitation. A child newly committed to lifelong immunoglobulin, or one whose regimen is being changed after a frightening adverse event, needs an honest, structured explanation of what happened, what the plan is, and what to watch for at home. [9]
Management — Definitive & Stepwise
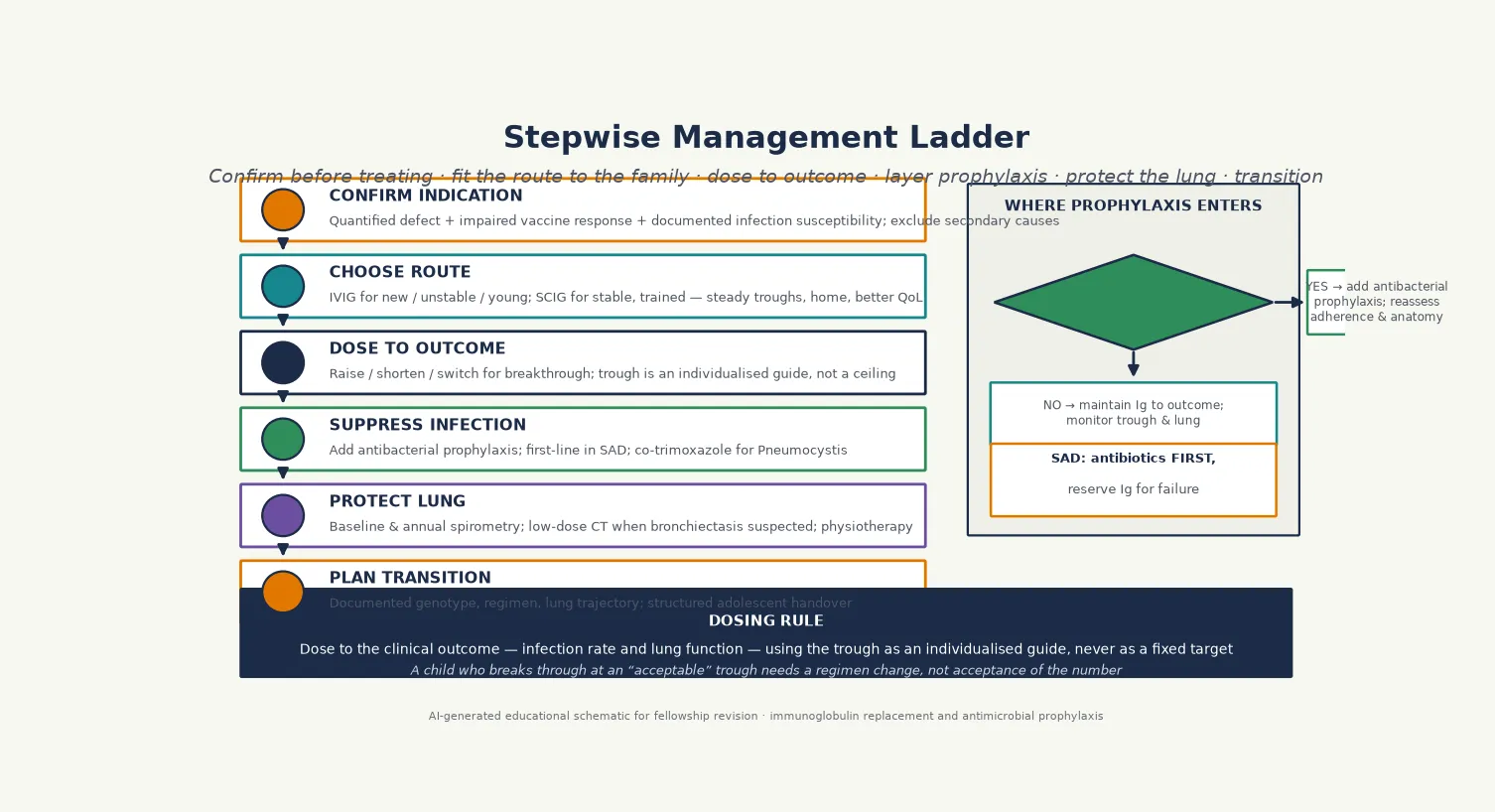
Definitive management follows a six-step ladder that a fellowship candidate can recite: confirm the indication, choose the route, dose to outcome, suppress infection, protect the lung, and plan the transition. The discipline is to escalate only the steps the child needs. [1] [2]
Step one is to confirm the indication before starting. Immunoglobulin replacement is a lifelong, resource-intensive therapy with real risks, and it should not begin on the basis of a single low number. Confirm the defect with quantified immunoglobulins plus an impaired functional vaccine response, exclude secondary causes, and document the infection burden. The clearest indications are the agammaglobulinaemias and common variable immunodeficiency with documented infection susceptibility. [1] [2]
Step two is to choose the route around the family and the trough goal. Intravenous immunoglobulin is the starting point for newly diagnosed, unstable, or very young patients and for those who need a rapid boost; it is given every three to four weeks in a clinic at a dose in the range of 400 to 600 mg/kg per infusion, titrated to the trough and the infection rate. Subcutaneous immunoglobulin is the preferred long-term option for stable, trained patients: a weekly infusion of roughly 100 to 200 mg/kg, given at home, producing steady troughs and fewer systemic reactions. The systematic review of home-based subcutaneous against hospital-based intravenous therapy found comparable infection outcomes with better quality of life and convenience for the subcutaneous route. [3] [8]
Step three is to dose to the clinical outcome. Measure the trough, but weigh it against the infection rate and the lung function trajectory. Raise the dose, shorten the interval, or switch the route if the child breaks through — do not accept an "adequate" trough in a child who is unwell. The therapeutic immunoglobulin literature is clear that the dose should be driven by clinical outcome rather than by body weight or a fixed trough alone, and individualising the regimen to the child's infection pattern is the heart of long-term management. [2] [7]
Step four is to suppress infection with antimicrobial prophylaxis. Add antibacterial prophylaxis — most often co-trimoxazole, azithromycin, or amoxicillin-clavulanate — when breakthrough infection persists despite an individually adequate trough, or when immunoglobulin is not indicated (as in specific antibody deficiency). The comparison of prophylactic antibiotics against immunoglobulin in specific antibody deficiency showed that a trial of antibiotic prophylaxis is the rational first move in that condition, reserving immunoglobulin for those who fail it. Add Pneumocystis prophylaxis with co-trimoxazole for combined T-cell defects and the hyper-IgM syndromes, and antiviral prophylaxis for chronic herpesvirus infection. [6] [4]
Step five is lung protection. Establish baseline and repeat annual spirometry, perform low-dose chest computed tomography when bronchiectasis is suspected, and involve physiotherapy and a respiratory team for children with established structural lung disease. The aim is to detect and treat bronchiectasis early, because established bronchiectasis is the largest determinant of long-term morbidity and the strongest argument for an intensive, individualised regimen. [3]
Step six is planned transition to adult immunology. A structured handover in adolescence — with documented genotype, vaccination history, lung function trajectory, individualised immunoglobulin regimen, and prophylaxis plan — preserves continuity and adherence through the vulnerable adolescent years. Transition is not a single appointment; it is a planned process that begins years before the actual transfer of care. [7] [9]
Specific Subtypes & Scenarios
Each major indication carries a distinctive decision point, and a fellowship answer earns depth by handling them individually rather than as a single block. [1]
X-linked agammaglobulinaemia and the other agammaglobulinaemias are the archetype of obligatory immunoglobulin replacement. The defect is profound and permanent, the infection susceptibility is high, and replacement begins at diagnosis and continues for life. The route is chosen for practicality and family preference, with many families moving to home subcutaneous therapy once the child is stable and the family is trained. Carrier testing of maternal female relatives belongs here, because each carrier son has a one-in-two chance of being affected and will need the same therapy from infancy. [3]
Common variable immunodeficiency is the commonest symptomatic indication, and the decision to start replacement rests on documented infection susceptibility rather than on the IgG number alone. CVID also carries a substantial burden of autoimmune, granulomatous, and lymphoproliferative disease, so surveillance for these is part of routine care alongside the immunoglobulin regimen. The quality-of-life study of patients with CVID under different immunoglobulin schedules found that the route and schedule affect daily life substantially, which is why the choice is individualised rather than protocolised. [2] [7]
Specific antibody deficiency is the condition that tests the discipline of this topic. The immunoglobulin levels are normal and the defect is purely functional, so adding immunoglobulin is a poor first move. The rational approach is a trial of antibacterial prophylaxis first, reserving immunoglobulin for the minority who continue to break through despite prophylaxis. The Hajjar comparison of prophylactic antibiotics against immunoglobulin in specific antibody deficiency is the decisive evidence here, and a fellowship candidate who handles this scenario correctly demonstrates that they understand the difference between treating a number and treating a child. [6]
Combined immunodeficiencies and the hyper-IgM syndromes combine antibody replacement with cellular prophylaxis. These children receive immunoglobulin for their antibody component and additional co-trimoxazole for Pneumocystis prophylaxis, and some require antiviral or antifungal cover. The intensity of prophylaxis scales with the depth of the T-cell defect, and the definitive treatment may be haematopoietic stem cell transplantation, which changes the long-term picture entirely. Live vaccines must be avoided until the immune status is clarified, because they can cause disseminated disease. [4]
Secondary antibody deficiency is managed case by case. A child on rituximab, with malignancy under treatment, or with protein loss from nephrotic syndrome may need temporary immunoglobulin if the infection burden is high, but the long-term answer is usually treatment of the underlying cause. The decision is individualised to the infection pattern, the expected duration of the secondary cause, and the risk of the immunoglobulin itself, and it is reviewed as the underlying condition changes. [1] [2]
Why treating specific antibody deficiency with immunoglobulin first is a mistake
In specific antibody deficiency the immunoglobulin levels are normal — the defect is that the antibody the child makes does not respond to polysaccharide antigens. Giving more of a product that the child is already failing to use is mechanistically weak, and it commits the child to lifelong therapy with its attendant risks before the cheaper, lower-risk option of antibiotic prophylaxis has been tried. The evidence supports a trial of prophylactic antibiotics first, with immunoglobulin reserved for those who fail it. [6]
Complications & Pitfalls
The complications divide into the consequences of the disease, the adverse effects of immunoglobulin, and the pitfalls of the decision-making itself. A fellowship answer handles all three. [2]
Bronchiectasis is the dominant disease complication and the strongest argument for getting the regimen right. Recurrent or undertreated sinopulmonary infection progressively destroys the airway wall, and established bronchiectasis drives long-term morbidity and mortality. Surveillance imaging and an individualised, outcome-driven regimen are the safeguards, and a child who develops bronchiectasis despite therapy needs a structured reassessment of the whole plan. [3]
The adverse effects of intravenous immunoglobulin are well characterised. Headache is common; severe headache and aseptic meningitis are less so but important. Haemolysis, thrombosis, and renal impairment are rare but serious and are detectable early with routine blood count and renal monitoring. Systemic infusion reactions — chills, fever, myalgia, hypotension — are managed by slowing or interrupting the infusion and pre-medicating for subsequent doses. The substantially lower systemic reaction rate of subcutaneous immunoglobulin is part of why a child with recurrent IVIG reactions is a candidate for a route switch. [5]
Local site reactions are the principal adverse effect of subcutaneous immunoglobulin: redness, swelling, and discomfort at the infusion sites, usually mild and self-limiting. They are managed by rotating sites, adjusting the rate, and reassuring the family. They rarely require discontinuation of the subcutaneous route, and they are the trade-off for the better systemic tolerability and the steady troughs. [9]
The pitfalls of decision-making are where marks are lost. Starting immunoglobulin for a single low IgG without a functional defect or documented infection susceptibility commits a child with transient hypogammaglobulinaemia of infancy to lifelong unnecessary therapy. Giving immunoglobulin to specific antibody deficiency before a trial of antibiotics ignores the evidence. Failing to add antimicrobial prophylaxis when a child breaks through, and instead only raising the trough, leaves the lung undefended. And forgetting to vaccinate household contacts — while remembering never to give live vaccines to a child with a possible combined defect — is a preventable error that costs real infections. [1] [4]
Prognosis & Disposition
Prognosis for a child on immunoglobulin replacement is dictated by the underlying defect, the timeliness of diagnosis, and the quality of the regimen and the lung surveillance. With early diagnosis and consistent, outcome-driven therapy, children with X-linked agammaglobulinaemia survive into adulthood and lead near-normal lives, dependent on lifelong therapy. [3]
Common variable immunodeficiency carries a more guarded prognosis because of its autoimmune, granulomatous, and lymphoproliferative complications, and because structural lung disease is often already present at diagnosis. Survival is reduced relative to the general population, driven principally by bronchiectasis and lymphoma, which is why surveillance and prompt treatment of complications matter as much as the replacement therapy itself. Getting the regimen right and protecting the lung are the two interventions that move the prognosis. [2] [7]
The prognosis is also shaped by the route and the adherence. Home subcutaneous therapy, where the family is trained and supported, improves adherence and quality of life and reduces the travel burden that erodes consistent care — particularly for families in remote communities or with socioeconomic disadvantage. A regimen that fits the family's life is a regimen that is actually given, and adherence is a prognostic factor in its own right. [8]
Disposition for a general paediatrician is shared care with a clinical immunology service. The immunologist owns the diagnostic characterisation, the immunoglobulin regimen and product, and the genetic counselling; the general paediatrician owns the acute-infection management, the growth and development surveillance, the coordination of transition, and the day-to-day partnership with the family. Early referral at the point of suspicion — rather than after a confirmed label — is the disposition rule, because the work-up and the lifelong therapy are specialist-led. [1] [9]
Special Populations
Immunoglobulin replacement interacts with the child's social and developmental context, and the same regimen behaves differently across populations. Access, adherence, and late presentation all shape outcome as much as the dose itself. [9]
Indigenous children, particularly in Australia and New Zealand, face a high background burden of recurrent respiratory infection, crowded housing, and reduced access to specialist services. Structural lung disease is common in these communities, so a confirmed antibody deficiency must be managed intensively to prevent rapid progression to bronchiectasis. Home subcutaneous therapy, where the family can be trained and supported, is often the route that delivers consistent care across distance. [8]
Migrant, refugee, and asylum-seeking families may have incomplete vaccination records, uncertain family history, and barriers to consistent immunoglobulin access. A careful reconstruction of the infection and vaccination history, a plan that accounts for mobility and language, and interpreter use and trauma-informed communication are essential. The regimen must survive a family's mobility, which means choosing a route and a supply arrangement that travel with the child where possible. [1]
Socioeconomically disadvantaged families carry a disproportionate burden of recurrent infection and late presentation, and the travel and time cost of hospital-based intravenous therapy can quietly erode adherence. Subcutaneous home therapy, where feasible, improves adherence and reduces travel burden, and should be discussed as an option for stable patients. The aim is to fit the therapy to the family's reality rather than the reverse. [8] [9]
Adolescents in transition are a population in their own right. Adherence to immunoglobulin therapy declines in adolescence, the risk-taking that accompanies chronic illness rises, and the handover to adult care is a vulnerable point. A structured, documented transition that preserves continuity of the immunoglobulin regimen, the prophylaxis, and the lung-surveillance trajectory is the safeguard, and it begins years before the actual transfer of care. [7]
Evidence, Guidelines & Regional Differences
The evidence base rests on three pillars: the consensus guidelines that set the indications, the trial and registry data that describe the regimens and their outcomes, and the quality-of-life and route-comparison studies that individualise the choice. [1]
The American Academy of Allergy, Asthma and Immunology Primary Immunodeficiency Committee reviews are the central evidence documents. The 2006 review by Orange and colleagues, and its 2017 update by Pérez and colleagues, set out the conditions for which immunoglobulin is indicated, the strength of the evidence, and the dosing principles. Together with the 2015 practice parameter for primary immunodeficiency, they define the standard of care. A fellowship answer should reference the most recent of these rather than an older edition. [2] [3]
Route comparison and quality-of-life data individualise the choice. The systematic review of home-based subcutaneous against hospital-based intravenous therapy found comparable infection outcomes with better quality of life for the subcutaneous route. The pharmacokinetic and safety studies of the 20% subcutaneous immunoglobulin preparations confirmed the steady-state profile and the low systemic reaction rate that underpin that advantage. The CVID quality-of-life study under different schedules showed that the schedule itself shapes daily life, which is why the route is individualised. [5] [7] [8]
The prophylaxis evidence is decisive for specific antibody deficiency. The Hajjar comparison of prophylactic antibiotics against immunoglobulin in specific antibody deficiency established that antibiotic prophylaxis is the rational first move in that condition, with immunoglobulin reserved for those who fail it. This single study changes the management of a defined subgroup and is a model of how evidence should drive the decision rather than reflex. [6]
Regional differences are practical rather than scientific. Australia and New Zealand follow the AAAAI and IUIS frameworks, with national blood arrangements funding the immunoglobulin product and shaping the choice between intravenous and subcutaneous therapy. Subcutaneous home therapy is increasingly used for stable patients to improve adherence and reduce travel, particularly in remote communities. The product availability and funding arrangements specific to the region shape the regimen, but the principles — confirm the indication, dose to outcome, layer prophylaxis, protect the lung — are universal. [4] [9]
In Australia and New Zealand, immunoglobulin is a national-blood-arrangements-funded product prescribed and monitored by a specialist clinical immunology service. The choice between intravenous and subcutaneous therapy is made with the family around adherence, travel, and the trough goal, with home subcutaneous therapy increasingly preferred for stable, trained patients — particularly in remote communities. Antimicrobial prophylaxis is added or substituted by the immunology team guided by the defect and the breakthrough pattern. Always involve the regional immunology centre early; the work-up, the product, and the lifelong monitoring are specialist-led. [1] [9]
Exam Pearls
A fellowship candidate answering on immunoglobulin replacement and antimicrobial prophylaxis should land five anchor points and avoid four classic traps. The anchors are the framework examiners listen for; the traps are where candidates lose easy marks. [1] [2]
Anchor one: confirm the indication before treating. Immunoglobulin replacement is for a confirmed antibody defect with documented infection susceptibility, not for a low number. The agammaglobulinaemias and CVID with infection susceptibility are the clearest indications; transient hypogammaglobulinaemia of infancy and most selective IgA deficiency are not. [1]
Anchor two: dose to the outcome, not the trough alone. The trough is a guide you adjust, not a target you worship. A child who breaks through at an "acceptable" trough needs a dose change, a route change, or prophylaxis — not acceptance of the number. [2]
Anchor three: fit the route to the family. Subcutaneous home therapy gives steady troughs, fewer systemic reactions, and better quality of life and adherence in stable patients; intravenous therapy suits the newly diagnosed, unstable, or very young. The choice is individualised. [8] [7]
Anchor four: layer antimicrobial prophylaxis where it belongs. Add antibacterial prophylaxis for breakthrough infection despite an adequate trough, and try antibiotics first in specific antibody deficiency. Add Pneumocystis prophylaxis for combined defects and the hyper-IgM syndromes. [6] [4]
Anchor five: protect the lung and plan the transition. Bronchiectasis is the dominant long-term complication, and a structured adolescent handover to adult immunology preserves continuity and adherence. [3]
The four traps to avoid are starting immunoglobulin on a low IgG alone, treating specific antibody deficiency with immunoglobulin before antibiotics, treating breakthrough infection only by raising the trough, and giving live vaccines before excluding a combined immunodeficiency. Avoid these and the rest of the answer falls into place. [1] [2]
References
- [1]Bonilla FA, Barlan I, Chapel H, Costa-Carvalho BT, Cunningham-Rundles C, de la Morena MT, et al. Practice parameter for the diagnosis and management of primary immunodeficiency. J Allergy Clin Immunol, 2015.PMID 26371839
- [2]Perez EE, Orange JS, Bonilla F, Chinen J, Chinn IK, Dorsey M, et al. Update on the use of immunoglobulin in human disease: A review of evidence. J Allergy Clin Immunol, 2017.PMID 28041678
- [3]Orange JS, Hossny EM, Weiler CR, Ballow M, Berger M, Bonilla FA, et al. Use of intravenous immunoglobulin in human disease: a review of evidence by members of the Primary Immunodeficiency Committee of the American Academy of Allergy, Asthma and Immunology. J Allergy Clin Immunol, 2006.PMID 16580469
- [4]Bousfiha A, Moundir A, Tangye SG, Picard C, Ochs HD, Al-Herz W, et al. The 2022 Update of IUIS Phenotypical Classification for Human Inborn Errors of Immunity. J Clin Immunol, 2022.PMID 36198931
- [5]Suez D, Borte M, Ritchie B, Iacob E, Espanola T, Huls G, et al. Efficacy, Safety, and Pharmacokinetics of a Novel Human Immune Globulin Subcutaneous, 20% in Patients with Primary Immunodeficiency Diseases in North America. J Clin Immunol, 2016.PMID 27582171
- [6]Hajjar J, Perez EE, Orange JS. Prophylactic Antibiotics Versus Immunoglobulin Replacement in Specific Antibody Deficiency. J Clin Immunol, 2020.PMID 31758281
- [7]Pulvirenti F, Sacco P, Valente M, Milito C, Capitani M, Santostefano M, et al. Health-Related Quality of Life in Patients with CVID Under Different Schedules of Immunoglobulin Administration: Prospective Multicenter Study. J Clin Immunol, 2019.PMID 30644015
- [8]Abolhassani H, Sadaghiani MS, Aghamohammadi A, Ochs HD, Rezaei N. Home-based subcutaneous immunoglobulin versus hospital-based intravenous immunoglobulin in treatment of primary antibody deficiencies: systematic review and meta analysis. J Clin Immunol, 2012.PMID 22730009
- [9]Duff C, Brown M, Vago M, Keet C. Nuts and Bolts of Subcutaneous Therapy. Immunol Allergy Clin North Am, 2020.PMID 32654697
- [10]Gathmann B, Binder N, Ehl S, Kindle G; ESID Database Working Group. The European internet-based patient and research database for primary immunodeficiencies: results 2006-2008. Clin Exp Immunol, 2009.PMID 19630863