Paeds · allergy-and-immunology
Vaccination of immunocompromised children
Also known as Immunisation of the immunocompromised host · Live vaccines in immunosuppression · Vaccination in primary immunodeficiency · Post-transplant vaccination · Vaccination on biologics and chemotherapy
A fellowship approach to vaccinating the immunocompromised child: classify the immune defect first, sort every vaccine into live-attenuated (the danger) versus inactivated (generally safe but may be poorly immunogenic), time each dose to the intensity of immunosuppression, and monitor serology rather than assuming protection — so that a live vaccine is never given before a combined T-cell defect has been excluded.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
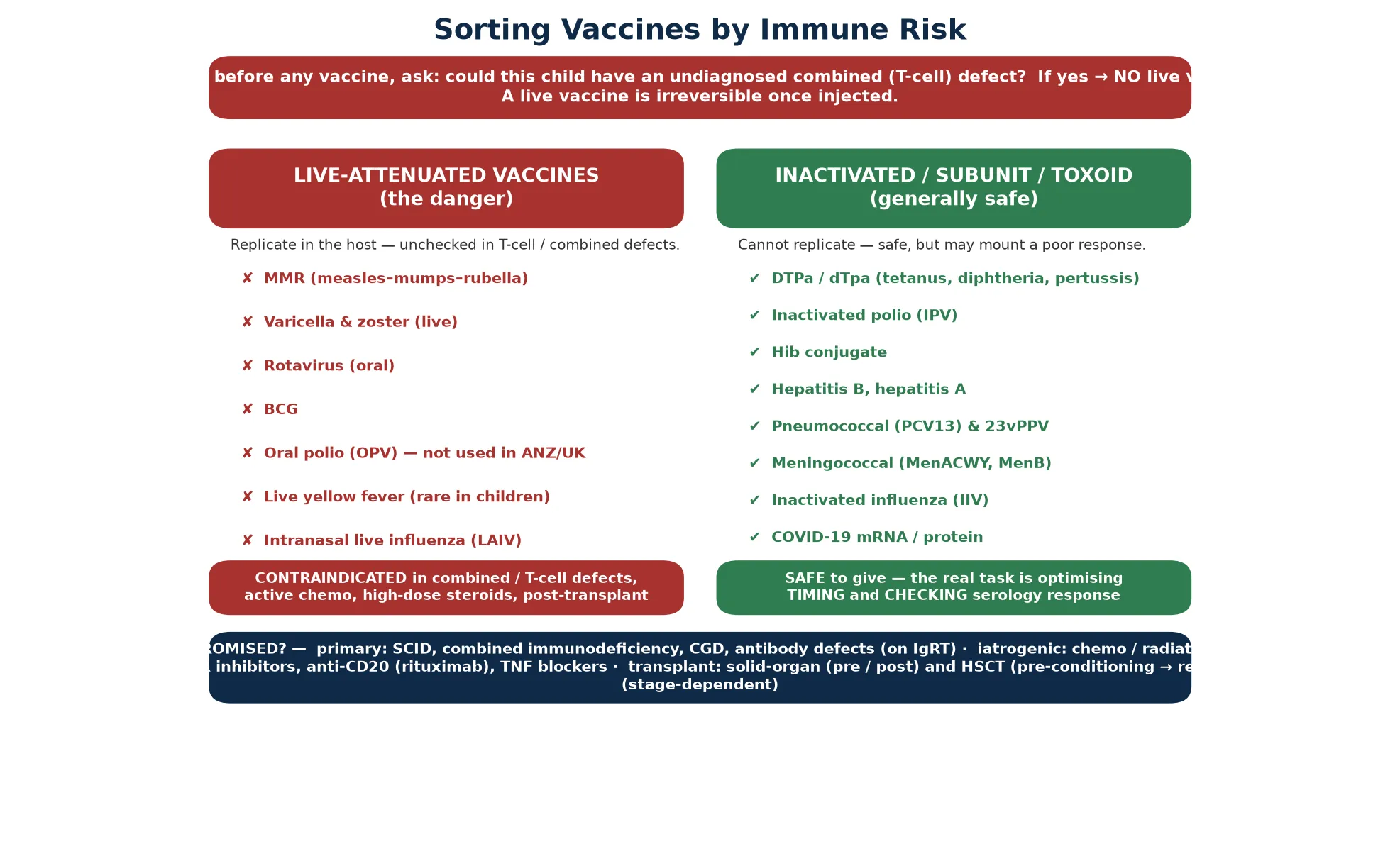
Once the defect is classified, the plan writes itself. Inactivated vaccines are safe and should not be withheld — the real task is optimising timing, giving extra or higher-antigen doses, and checking serology rather than assuming protection. Live vaccines — MMR, varicella, rotavirus, BCG, oral polio, live yellow fever, intranasal influenza — are the danger, contraindicated in combined and T-cell defects, during high-dose chemotherapy, on substantial corticosteroids, and in the early months after transplant. The fellowship mark goes to the candidate who coordinates with immunology, oncology, and the transplant service, vaccinates the household to cocoon the child, and rebuilds the schedule on evidence of immune reconstitution rather than on a calendar date. [1] [2]
L.I.V.E. — when a live vaccine must wait
Overview & Definition
Vaccination of the immunocompromised child is the deliberate matching of every scheduled and catch-up vaccine to the child's immune capacity, so that protection is maximised and harm is avoided. The immunocompromised host cannot be treated as a normal recipient: some vaccines will not work as well, and a small number — the live-attenuated vaccines — can cause the very disease they are meant to prevent. The discipline of this topic is to decide, vaccine by vaccine, what is safe, what is useful, when to give it, and how to confirm it worked. [1]
The population is broad. It includes children with primary immunodeficiencies (severe combined immunodeficiency, combined immunodeficiency, chronic granulomatous disease, antibody deficiencies on immunoglobulin replacement), children on iatrogenic immunosuppression (cytotoxic chemotherapy, high-dose corticosteroids, calcineurin and mTOR inhibitors, anti-CD20 monoclonal antibodies such as rituximab, and tumour-necrosis-factor blockers), children before and after solid organ transplant, children before and after haematopoietic stem cell transplant (HSCT), children with HIV in whom risk is stage-dependent, and children with functional or anatomical asplenia. The principles apply to all of them, but the detail is defect-specific. [1] [3] [8]
Classification
Sort the problem along three axes, because each one changes the plan. First, classify the immune defect into a T-cell or combined defect (where live vaccines are contraindicated), a pure B-cell or humoral defect (where live vaccines are usually safe but poorly immunogenic), an iatrogenic or pharmacologic state (where risk tracks current therapy), or a transplant-related state (where timing dominates). Second, sort every vaccine into live-attenuated versus inactivated, subunit, toxoid, conjugate, or recombinant. Third, classify the timing relative to chemotherapy, transplant conditioning, and immunosuppressive drug troughs. [1] [2]
Epidemiology & Risk Factors
The number of immunocompromised children is rising because transplantation, biological therapies, and cancer survival have all expanded. The risk that concerns a fellowship candidate is not the background prevalence but the consequence of a single error: a live vaccine given into an unrecognised combined defect. The clearest examples come from severe combined immunodeficiency (SCID), where BCG vaccination before diagnosis produces disseminated BCG disease in a substantial fraction of affected infants, and where rotavirus vaccination has been linked to severe, persistent vaccine-strain diarrhoea reported to passive surveillance systems. [5] [6] [7]
Newborn screening for SCID has changed this epidemiology. Where T-cell receptor excision circle (TREC) screening is in place, combined defects are identified in the first weeks of life, before BCG and rotavirus are due, so that the live vaccines are deferred until the defect is characterised and treated. In regions without newborn SCID screening, the first sign of immunodeficiency may be the complication of the live vaccine itself, which is why any disseminated BCG or persistent vaccine-strain rotavirus infection warrants immunological investigation rather than being treated as an isolated infection. [5] [7]
The risk from iatrogenic immunosuppression is dose- and time-dependent, not a fixed label. The ACIP general recommendations set the practical threshold: corticosteroids given at the equivalent of prednisolone 2 mg/kg/day or more (or 20 mg/day or more for children over 10 kg), for 14 days or longer, constitute a level of immunosuppression that contraindicates live vaccines until at least four weeks after the steroids have stopped. Short courses, alternate-day dosing, and inhaled or topical steroids do not. The same principle — that risk tracks current therapy — governs vaccination on biological agents, where EULAR/PRES guidance supports giving inactivated vaccines freely but recommends timing them for when the disease is controlled and the biologic trough is low. [2] [4]
Pathophysiology
Vaccine safety in the immunocompromised child is decided by one mechanism: whether the host can contain the replication that a live vaccine depends on. A live-attenuated vaccine works precisely because the organism replicates enough to evoke a full adaptive response without causing disease. That bargain holds only if the host can terminate the infection. T cells are the principal effectors of that termination, which is why a T-cell or combined defect converts a safe vaccine into disseminated, persistent disease. [5]
The clearest illustration is BCG in SCID. Bacille Calmette–Guérin is a live mycobacterial strain given in many countries at birth. In a child with intact immunity it produces local immunity and, through trained immunity mediated by NOD2-dependent epigenetic reprogramming of innate cells, a degree of non-specific protection against unrelated pathogens. In a child with SCID it disseminates, because there is no T-cell response to control the mycobacterium, producing BCG-osis with lymphadenitis, hepatosplenic disease, and sometimes fatal disseminated infection. The same logic applies to rotavirus, which in SCID causes persistent vaccine-strain enteritis, and to varicella vaccine, which can cause vaccine-strain chickenpox, pneumonitis, or meningitis when given during profound immunosuppression. [5] [6] [7]
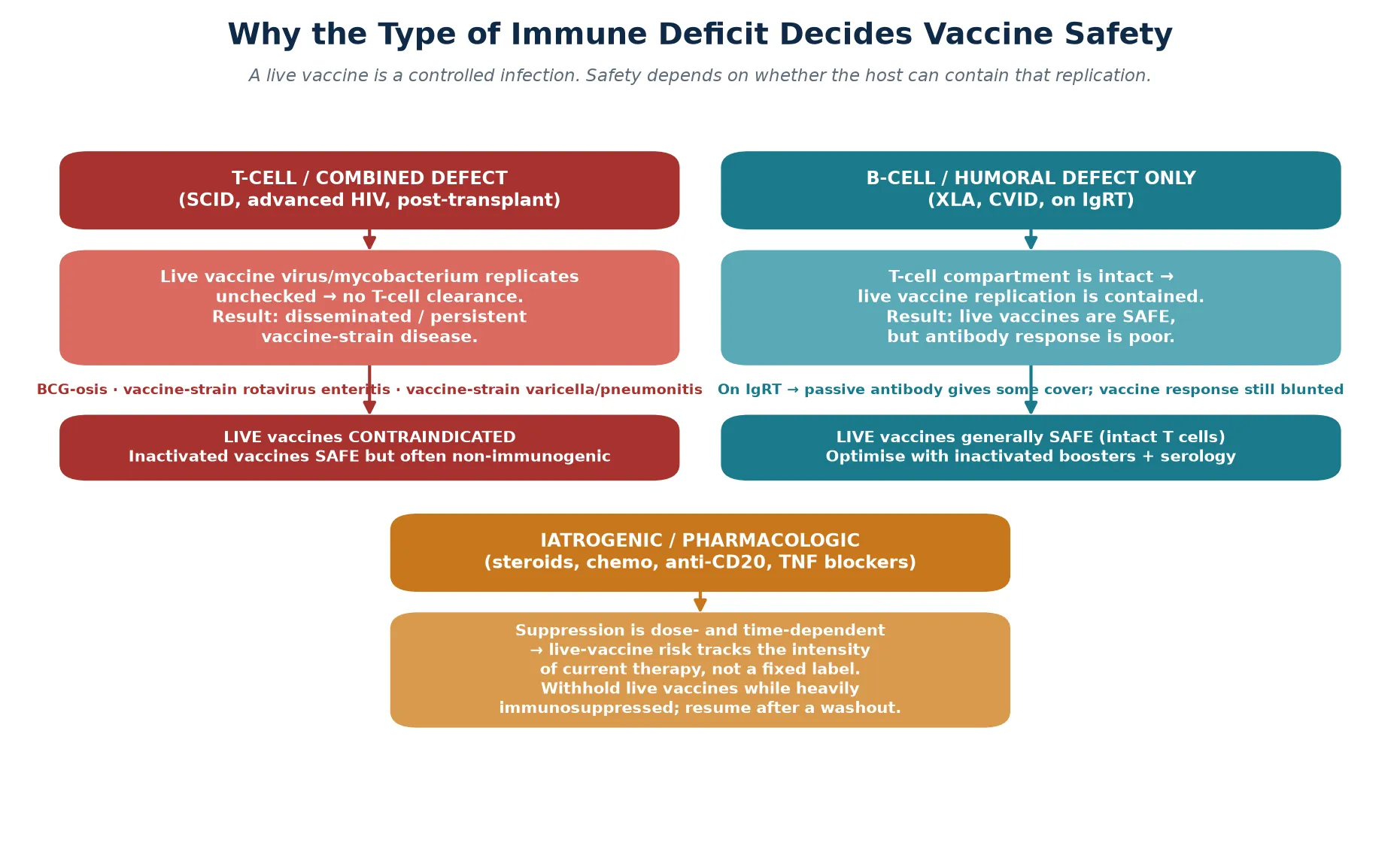
A pure B-cell or humoral defect tells a different story. Because the T-cell compartment is intact, live vaccines are generally contained and therefore safe — the rubella and varicella components of MMR can still replicate and be controlled. The problem in humoral defects is not safety but efficacy: the antibody response is blunted, so serology is unreliable and the child on immunoglobulin replacement receives most protection from the donated immunoglobulin rather than from their own vaccination. Iatrogenic immunosuppression sits between these poles: it is pharmacologically reversible, so live-vaccine risk rises and falls with the intensity of the current regimen rather than with a permanent label. [1] [4]
Clinical Presentation
The clinical relevance of this topic is not a symptom complex but a decision point: the moment a vaccine is due, or has just been given, in a child who is or might be immunocompromised. The "presentation" is therefore the scenario in which the question arises. The first is the infant due for routine immunisation who may have an undiagnosed combined defect — the newborn SCID screen is pending or unavailable, there is a family history of early male death, or the infant has failure to thrive, chronic diarrhoea, or persistent oral thrush. Here the task is to withhold the live vaccines and investigate, not to proceed on schedule. [5] [6]
The second scenario is the child newly diagnosed with a primary immunodeficiency, malignancy, or transplant candidacy, whose immunisation record must be reviewed before therapy begins. Any inactivated vaccines that can be given beforehand should be, because they will immunise better before conditioning than after. Live vaccines, conversely, must be stopped once the diagnosis that warrants them being withheld is established. The third scenario is the child already on immunosuppression who is due a vaccine — here the question is whether the current regimen contraindicates a live vaccine, and whether an inactivated vaccine is likely to immunise or should be deferred to a less immunosuppressed window. [1] [3] [8]
Differential Diagnosis
The differential in this topic is the differential of the immune state itself, because the vaccine plan is dictated by which category the child falls into. The four categories to hold in mind are primary immunodeficiency (combined, antibody, phagocytic, complement), iatrogenic immunosuppression (chemotherapy, corticosteroids, calcineurin and mTOR inhibitors, anti-CD20, TNF blockers), transplant-related (pre- and post-solid organ; pre-conditioning, early, and reconstituting phases of HSCT), and HIV, in which the risk is stage-dependent and live vaccines may even be indicated once immune reconstitution is documented. [1] [3]
| Category | Defining feature | Live-vaccine rule |
|---|---|---|
| Combined / T-cell defect (SCID) | Absent T-cell function; low TREC on newborn screen | Contraindicated — risk of disseminated vaccine-strain disease |
| Antibody defect on IgRT | Intact T cells; blunted antibody response | Usually safe; serology unreliable |
| Active chemotherapy / radiation | Cytopenia, mucositis; within treatment cycles | Hold live vaccines until ≥3 months after therapy ends |
| High-dose corticosteroids | Substantial systemic course meeting the ACIP threshold | Hold live vaccines for ≥4 weeks after stopping |
| Solid organ transplant | On calcineurin / mTOR inhibitors | No live vaccines post-transplant; give inactivated on schedule |
| HSCT | Immunity reset at conditioning | Re-vaccinate from scratch once immune reconstitution is documented |
| HIV, well-controlled | CD4 above age thresholds | MMR and varicella may be given; BCG and rotavirus still avoided |
The practical trap is to treat "immunocompromised" as a single state. A child with well-controlled HIV on antiretroviral therapy and a normal CD4 count may safely receive MMR and varicella, whereas a child with SCID may not; a child on inhaled steroids for asthma is not the same as a child on high-dose systemic steroids for nephrotic relapse. The discipline is to assign the child to the correct category at every visit, because the category — not the label — sets the rule. [1] [2]
Clinical & Bedside Assessment
The bedside task is to run the four-question check before any vaccine is given, and to do it out loud so the plan is auditable. Begin with the threat gate: could this child have a combined T-cell defect? If there is any doubt — pending newborn screen, family history, failure to thrive, lymphopenia, or a clinical syndrome of immunodeficiency — the live vaccines are held and the defect is investigated first. This gate is the single most important move in the whole topic, because the harm from a live vaccine in SCID is irreversible. [1] [5]
Once the gate is cleared, assess the intensity and timing of any current immunosuppression. Quantify the corticosteroid dose and duration against the ACIP threshold, map the chemotherapy cycle, confirm the time since transplant, and list the biological agents with their dosing intervals. Then review the immunisation record: which inactivated vaccines are missing and could be given now or optimised, and which live vaccines are deferred and for how long. Finally, consider the household: cocooning — fully vaccinating siblings and carers with inactivated influenza, COVID-19, MMR, and varicella — is one of the most effective protective measures available, and the household must avoid oral polio and live rotavirus vaccines that shed live virus toward the index child. [1] [2] [9]
Assess the family's practical context at the same time. A child in a remote community, a refugee or migrant family, or a family managing a complex transplant regimen faces additional barriers to a coordinated schedule, and the catch-up plan must be written down, shared with the general practitioner, and reconciled with the specialist service at every visit so that no dose is silently missed. [1] [8]
Investigations
There are two investigation questions. The first, asked before any live vaccine, is does this child have a combined T-cell defect? In an infant this is answered by the newborn SCID screen (TREC) and, where abnormal, by flow cytometry for lymphocyte subsets (T, B, and NK cells) and functional T-cell testing. The second, asked after vaccination, is did this vaccine work? Serology after inactivated vaccines — tetanus, pneumococcal, Hib, and hepatitis B — identifies non-responders who need extra doses, particularly children on anti-CD20 therapy (rituximab) and children after HSCT, in whom antibody responses are blunted for months and the schedule must be rebuilt on evidence rather than assumption. [1] [8]
A baseline immunoglobulin level, full blood count, and lymphocyte subset panel are reasonable where the immune status is uncertain, and they are mandatory when a combined defect has not been excluded. Imaging has no routine role in planning vaccination, but a chest radiograph or CT is part of evaluating suspected disseminated BCG or vaccine-strain varicella, and findings of widespread nodal or pulmonary disease in a recently vaccinated infant should prompt immunological investigation. [5] [6]
Management — Resuscitation
Resuscitation in this context means managing the harm of a live vaccine given in error, and the first step is recognition. A child who develops fever, spreading lymphadenitis, hepatosplenomegaly, chronic diarrhoea, or a disseminated vesicular rash within weeks of BCG, rotavirus, MMR, or varicella vaccination, in the setting of possible immunodeficiency, must be treated as having vaccine-strain disease with an underlying combined defect until proven otherwise. Stop any further immunosuppression that is not essential, obtain specimens for microbiology and molecular strain typing to confirm vaccine-strain origin, and involve immunology, infectious diseases, and (for transplant candidates) the transplant service immediately. [5] [6]
Specific therapy follows the organism and the defect. Disseminated BCG in SCID requires anti-mycobacterial therapy guided by susceptibility and, ultimately, haematopoietic stem cell transplant to correct the immunodeficiency. Vaccine-strain rotavirus enteritis is supportive with nutrition and fluid, but it can persist for many months until immune reconstitution. Vaccine-strain varicella in an immunosuppressed child may warrant aciclovir, and severe disseminated disease may require varicella zoster immunoglobulin where available. The principle in every case is that the long-term answer is correction or reduction of the immune defect, not just treatment of the infection. [6] [7]
Management — Definitive & Stepwise
Definitive management is a five-step ladder that a fellowship candidate can recite and a general practitioner can follow: classify the defect, screen and vaccinate the household, choose the vaccines, time them to the immunosuppression, and monitor serology with a documented catch-up. The discipline is to give inactivated vaccines freely and to make the live vaccine the last thing re-introduced, and only after T-cell competence is confirmed. [1] [2]
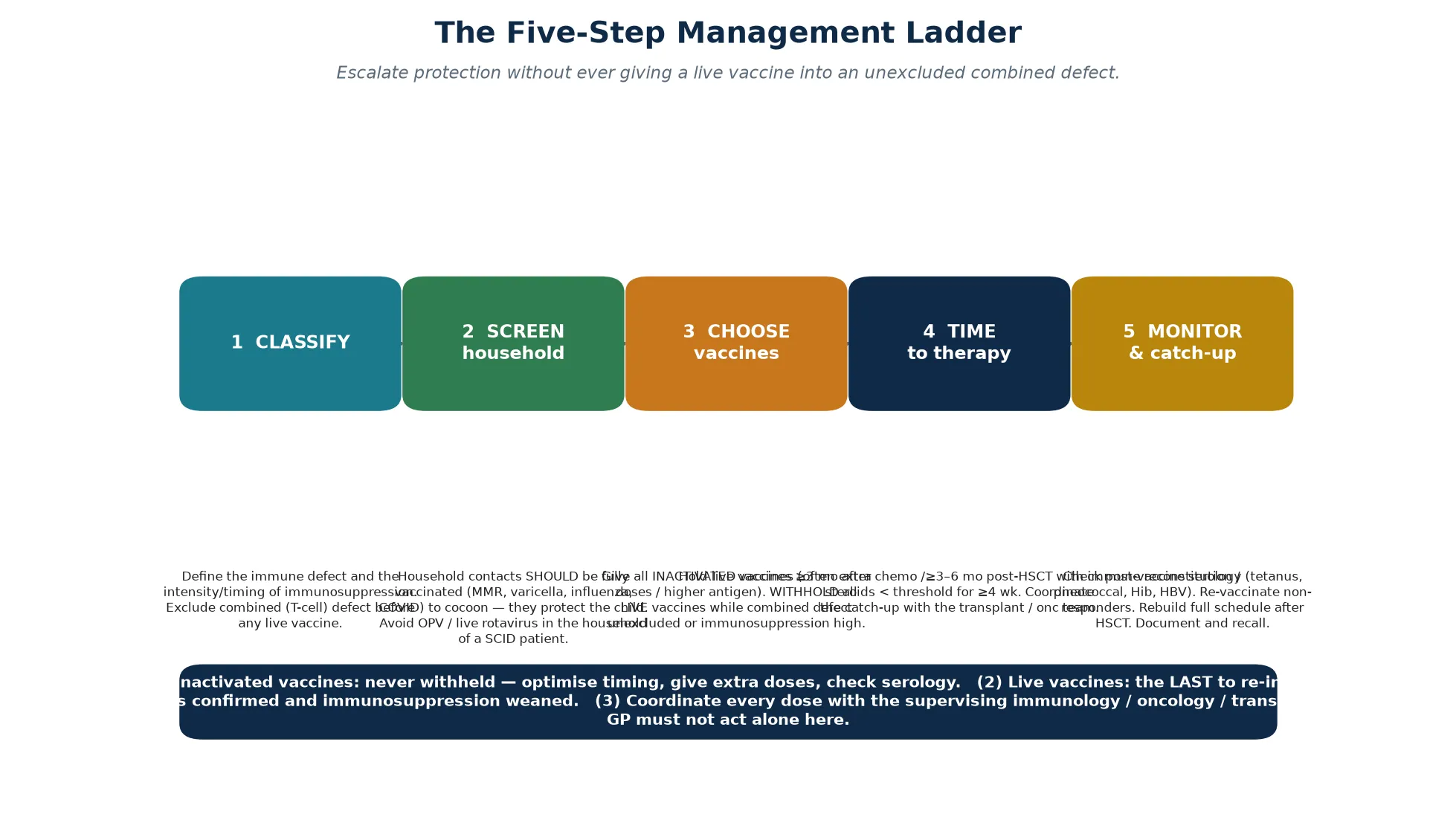
For inactivated vaccines, give them on schedule whenever possible, consider additional or higher-antigen formulations where licensed (for example extra pneumococcal and meningococcal doses in asplenia), prioritise annual inactivated influenza from six months of age, and verify serology for the antigens where non-response is common. For solid organ transplant candidates, complete as much of the inactivated schedule as possible before transplantation and avoid live vaccines entirely thereafter; the post-transplant plan is inactivated vaccines only, timed around immunosuppression. For HSCT, re-vaccinate from scratch beginning three to six months after transplant once immune reconstitution is documented, using inactivated vaccines first and re-introducing live vaccines (MMR, varicella) only after T-cell recovery is confirmed. [3] [8] [10]
For children on biological agents for rheumatic or inflammatory disease, the EULAR/PRES recommendations are explicit: give inactivated vaccines freely, preferably when the disease is controlled and the biologic trough is low; avoid live vaccines while on therapy and for a period after stopping; and do not delay necessary inactivated protection for fear of disease flare. For corticosteroids, apply the ACIP threshold rigorously — live vaccines are held during and for at least four weeks after a course that meets the dose and duration criteria, but short courses and inhaled steroids do not count. For asplenia, ensure pneumococcal (both conjugate and polysaccharide), meningococcal (ACWY and B), Haemophilus influenzae type b, and annual influenza are complete and boosted, alongside antibiotic prophylaxis. [2] [4] [10]
Why 'just delay everything' is the wrong default
Delaying all vaccines in an immunocompromised child is not safer — it leaves the child exposed to influenza, pneumococcus, pertussis, and COVID-19, organisms that cause severe disease precisely in this group. The correct reflex is to give inactivated vaccines promptly and optimally, and to withhold only the live vaccines until the defect and the timing permit. The harm from a missed inactivated vaccine is real; the harm from an unnecessary blanket delay is equally real. [1] [9]
Specific Subtypes & Scenarios
Each immunocompromised state carries a distinctive decision point, and a fellowship answer earns depth by handling them individually. In severe combined immunodeficiency, no live vaccine is given until the defect is treated and immune reconstitution is documented; a child who has already received BCG or rotavirus before diagnosis must be evaluated for vaccine-strain complications and referred urgently for curative HSCT. In antibody deficiencies on immunoglobulin replacement, live vaccines are generally safe because T-cell immunity is intact, but vaccine responses are blunted, so the practical protection comes from the replacement immunoglobulin and the priority shifts to protecting the household. [5] [6]
In solid organ transplantation, the window before transplant is the time to complete inactivated vaccines and to give any live vaccines that will not be possible afterwards (for example, completing MMR and varicella well before listing, where local guidance permits). After transplant, only inactivated vaccines are given, and live vaccines remain contraindicated for life. In HSCT, the conditioning regimen erases prior immunity, so the entire schedule is rebuilt on evidence of reconstitution: inactivated vaccines from around three to six months, live vaccines (MMR, varicella) only after documented T-cell recovery, typically from two years post-transplant in the stable graft-versus-host-disease-free child. [3] [8]
In children on chemotherapy for malignancy, inactivated influenza is given each season because influenza causes excess mortality in this group, while live vaccines are held during therapy and re-introduced at least three months after cytotoxic chemotherapy ends with recovering counts. In HIV, the principle is stage-dependent: a child with suppressed viral load and a CD4 count above age-specific thresholds can receive MMR and varicella, but BCG and rotavirus remain contraindicated, and the inactivated schedule is expanded with additional pneumococcal doses. In functional or anatomical asplenia, the priorities are the encapsulated-organism vaccines — pneumococcal, meningococcal, and Hib — plus annual influenza, with booster schedules and concomitant antibiotic prophylaxis. [1] [9] [10]
Complications & Pitfalls
The complications divide into the consequences of the wrong decision and the consequences of an unverified response. The most serious wrong decision is giving a live vaccine into a combined defect, producing disseminated BCG, vaccine-strain rotavirus enteritis, or vaccine-strain varicella. The second wrong decision is giving a live vaccine during high-dose immunosuppression — for example, varicella vaccine to a child on substantial steroids or during chemotherapy — producing vaccine-strain disease. The third is failing to vaccinate the household, so that a sibling brings influenza or varicella into the home of the immunocompromised child. [1] [5]
The unverified-response complication is silent non-protection: the child is "vaccinated" on paper but has no antibody, because the response was blunted by rituximab, recent HSCT, or intense immunosuppression. The defence is post-vaccine serology for the antigens where non-response is common, and a documented catch-up that re-vaccinates non-responders rather than assuming the record is correct. [8] [1]
Prognosis & Disposition
Prognosis is determined by the underlying condition and by the quality of the vaccine coordination, not by vaccination in isolation. A child whose combined defect is identified by newborn screening, treated by HSCT, and re-vaccinated on evidence of reconstitution can expect near-normal protection and a near-normal life. A child whose defect is first recognised through a complication of a live vaccine has a worse starting point, because the vaccine-strain disease must be managed alongside the immunodeficiency itself. [5] [6]
Disposition is shared care. The specialist immunology, oncology, or transplant service owns the defect-specific rules — particularly the decision on live vaccines and the timing of re-vaccination after HSCT — while the general practitioner and the public or primary health immunisation service own the routine and catch-up schedule, the seasonal influenza programme, and the recall system that prevents silent drops in coverage. Every transition — to adult care, between services, or after a move — is a point at which coverage is lost, so the immunisation record must travel with the child and be reconciled at every handover. [1] [8]
Special Populations
The same vaccine plan behaves differently across populations because access, late presentation, and the burden of vaccine-preventable disease are unevenly distributed. In remote and Indigenous communities, lower coverage, later presentation of combined defects in the absence of newborn screening, and a higher burden of encapsulated and respiratory disease make coordinated catch-up and household cocooning especially important. In refugee, migrant, and asylum-seeking families, the schedule may be incomplete or undocumented, the child may have received different products in another country, and the plan must begin with a careful record reconciliation and serological check where feasible. [1]
In children in out-of-home care and in families managing complex transplant or oncology regimens, fragmentation of care is the chief threat to coverage; a written, shared, and reconciled immunisation plan is the intervention that matters. In adolescents transitioning to adult care, the move is a high-risk point for loss of the expanded schedule (meningococcal, pneumococcal, HPV, annual influenza), so the transition plan must explicitly hand over the immunisation record and the outstanding catch-up, including any live vaccines still to be re-introduced after HSCT or biologic therapy. [8] [1]
Evidence, Guidelines & Regional Differences
The evidence base rests on three pillars: consensus guidelines that codify the rules, surveillance and registry data that quantify the live-vaccine risks, and cohort studies that measure immunogenicity in each immunocompromised state. The 2013 IDSA guideline for vaccination of the immunocompromised host is the most widely cited framework and sets the live-versus-inactivated logic, the corticosteroid threshold, and the HSCT re-vaccination schedule that most national programmes adopt. The ACIP general recommendations supply the operational detail — spacing, minimum ages, and the dose-and-duration rule for corticosteroids. [1] [2]
Disease-specific guidelines refine the rules for particular groups: the American Society of Transplantation guidance for solid organ transplant candidates and recipients, the EULAR/PRES recommendations for paediatric rheumatic disease on biologics, and specialist statements on asplenia and on HSCT immunisation practice. The surveillance data on SCID and rotavirus (VAERS reports) and on BCG-associated complications in SCID cohorts are the evidence that a live vaccine given into an unrecognised combined defect is not a theoretical risk. [3] [4] [7] [10]
In Australia and New Zealand, BCG is not given routinely at birth (it is targeted to high-risk neonates), oral polio is not used, and newborn SCID screening via TREC is being implemented. The Australian Immunisation Handbook sets the live-vaccine contraindications and the catch-up rules, and a specialist clinical immunology service coordinates the more complex plans — HSCT re-vaccination, transplant, and biologics. Household cocooning with inactivated influenza, COVID-19, and pertussis-containing vaccine is emphasised, and the immunisation record is reconciled at every specialist and primary-care visit. Always confirm the current regional schedule and any special-risk funding for additional pneumococcal, meningococcal, and influenza doses.
[1][2]Exam Pearls
A fellowship candidate answering on vaccination of the immunocompromised child should land five anchor points and avoid three classic traps. The anchors are the four-question framework (defect, live or inactivated, timing, verification), the threat gate that excludes a combined defect before any live vaccine, the corticosteroid threshold and its four-week washout, the household cocooning principle, and the HSCT rebuild-on-evidence rule. The traps are giving a live vaccine before excluding SCID, withholding all vaccines under the illusion of safety, and assuming serological protection after HSCT or rituximab without checking titres. [1] [2]
References
- [1]Rubin LG, Levin MJ, Ljungman P, Davies EG, Avery R, Tomblyn M, et al. 2013 IDSA clinical practice guideline for vaccination of the immunocompromised host. Clin Infect Dis, 2014.PMID 24421306
- [2]National Center for Immunization and Respiratory Diseases. General recommendations on immunization: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep, 2011.PMID 21293327
- [3]Danziger-Isakov L, Kumar D, AST Infectious Diseases Community of Practice. Vaccination in solid organ transplantation. Clin Transplant, 2019.PMID 31002409
- [4]Jansen MHA, Wulffraat NM, Kamphuis S, Tengroth L, Ádori M, Balu R, et al. EULAR/PRES recommendations for vaccination of paediatric patients with autoimmune inflammatory rheumatic diseases: 2021 update. Ann Rheum Dis, 2023.PMID 35725297
- [5]Gennery AR. Severe combined immunodeficiency: newborn screening and the BCG vaccination. Arch Dis Child, 2022.PMID 35973752
- [6]Mazzucchelli JT, Hadad R, Cardoso AL, de Souza Freire P, da Silva Pacheco I, de Oliveira JSB, et al. Severe combined immunodeficiency in Brazil: management, prognosis, and BCG-associated complications. J Investig Allergol Clin Immunol, 2014.PMID 25011356
- [7]Bakare N, Menschik D, Tiernan R, Hua W, Martin D. Severe combined immunodeficiency (SCID) and rotavirus vaccination: reports to the Vaccine Adverse Events Reporting System (VAERS). Vaccine, 2010.PMID 20674876
- [8]Hudspeth MP, Morrison VA, Chadwick EG, Moertel CL, Kletzel M, Yusuf U, et al. Post-hematopoietic stem cell transplant immunization practices in the Pediatric Blood and Marrow Transplant Consortium. Pediatr Blood Cancer, 2010.PMID 20135703
- [9]Bosaeed M, Kumar D. Seasonal influenza vaccine in immunocompromised persons. Hum Vaccin Immunother, 2018.PMID 29485353
- [10]Lee GM, Posey R, Bascietto C, Kasser S, Chandler R, Lo console L, et al. Preventing infections in children and adults with asplenia. Hematology Am Soc Hematol Educ Program, 2020.PMID 33275684