Paeds · cardiology
Adult congenital heart disease transition
Also known as ACHD transition · Transition of care in congenital heart disease · Grown-up congenital heart disease (GUCH) · Paediatric to adult cardiology transfer · Lifelong congenital heart disease follow-up · Transition readiness in congenital heart disease
Fellowship guide to the transition of the adolescent with congenital heart disease from paediatric to lifelong adult ACHD care: why transition is a planned process and not a single transfer clinic; how to build and measure transition readiness from early adolescence using tools such as the TRAQ; the anatomic-physiologic complexity classification that sets the surveillance interval and the care setting; the lesion-specific residua and sequelae that make follow-up lifelong even in the well-feeling patient; the danger of loss to follow-up and the gaps-in-care evidence; contraception matched to thrombotic and haemodynamic risk and pre-pregnancy counselling built on the modified WHO risk classes; the narrowed indications for infective endocarditis prophylaxis in the highest-risk lesions; and the 2018 AHA/ACC and 2020 ESC guidance that anchors ANZ practice.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a seventeen-year-old who was born with tetralogy of Fallot, repaired as a toddler, and followed all his childhood at the children's hospital. He feels completely well, plays club soccer, and has just finished school. His paediatric cardiologist retires, the last clinic letter says "review in two years," and no adult appointment is ever booked. Four years later he arrives in an emergency department with palpitations and breathlessness, in atrial flutter, with a dilated right ventricle and free pulmonary regurgitation that a timely valve intervention could have pre-empted. That silent gap between paediatric discharge and adult re-engagement is the problem this topic solves. [3] [4]
ACHD transition is the planned, purposeful, staged preparation of the adolescent with congenital heart disease for a move to adult-oriented, lifelong cardiac care. It is deliberately distinguished from transfer, which is the single administrative event of the first adult appointment. Transition is the years of work on either side of that event: building knowledge, independence, and a therapeutic relationship so that the transfer does not become a cliff edge. [3] [1]
This matters because congenital heart disease is now overwhelmingly a condition of adults. Survival of even complex lesions into adulthood is the norm, and adults with congenital heart disease outnumber children with it. The population that paediatric cardiology once cured and discharged is instead a growing cohort needing decades of specialised surveillance, and the transition is the hinge on which that lifelong care turns. [5] [13]
Classification
The single most useful framework is the anatomic-physiologic complexity classification, because it tells you how often to review a patient and where. The 2018 AHA/ACC guideline grades lesions as simple, moderate, or complex (great), and pairs that grade with the surveillance interval and the care setting. Getting this grade right is the practical core of the transition plan. [1]
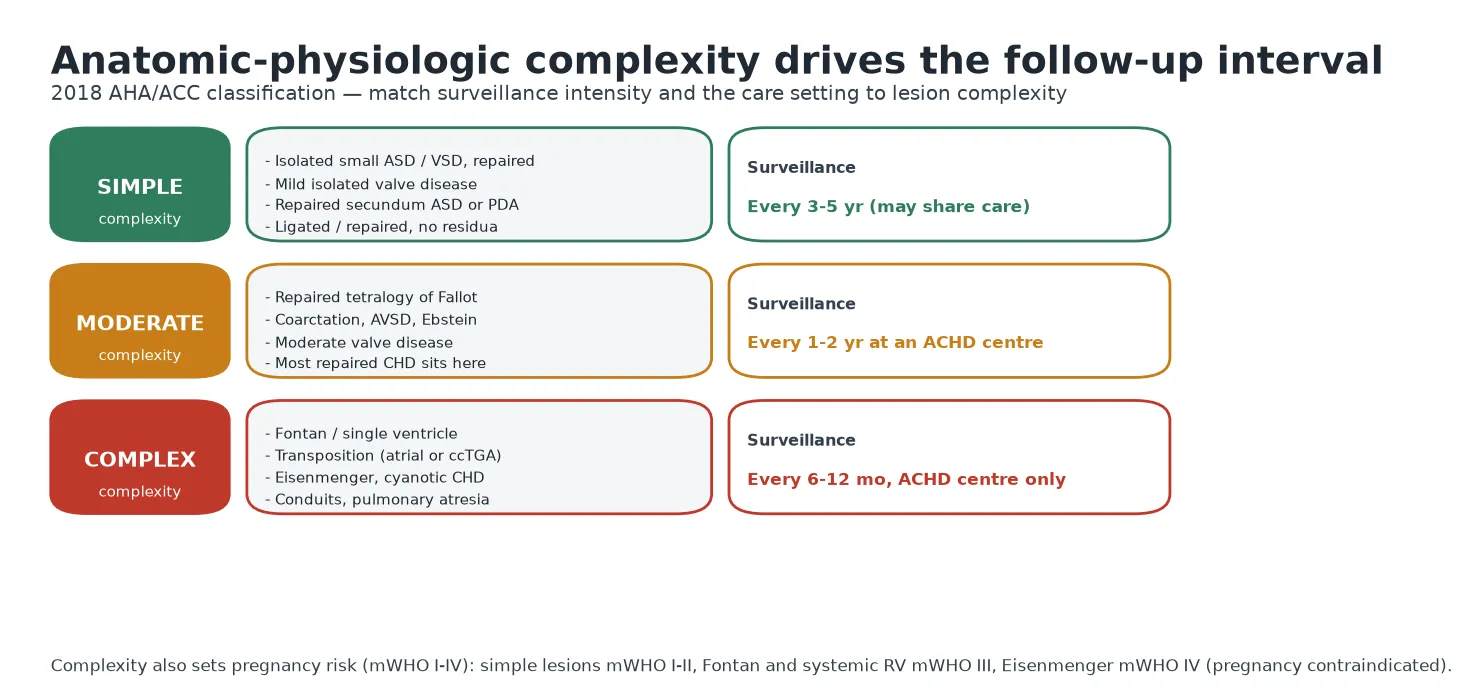
Simple lesions include a repaired small septal defect, an isolated mild valve lesion, and a repaired secundum atrial septal defect or ligated duct with no residua. These patients can often be reviewed every three to five years and their care shared with a well-informed primary care team, provided the young person knows the warning symptoms that should prompt earlier review. [1] [13]
Moderate lesions — the large middle group — include repaired tetralogy of Fallot, coarctation of the aorta, atrioventricular septal defect, Ebstein anomaly, and moderate valve disease. These need review at an ACHD centre every one to two years, because the residual and progressive problems (pulmonary regurgitation, recoarctation, atrial arrhythmia, valve deterioration) are common and are best managed by teams who see them often. [1] [2]
Complex or "great" lesions include the Fontan or single-ventricle circulation, transposition of the great arteries after an atrial switch or in its congenitally corrected form, Eisenmenger syndrome, and other cyanotic disease and conduit-dependent lesions. These need six-to-twelve-monthly review at a specialist ACHD centre only, because the physiology is fragile, complications are frequent, and the margin for error is small. The same complexity grade also predicts pregnancy risk, which is why the classification threads through the whole topic. [1] [8]
Epidemiology & Risk Factors
Congenital heart disease affects roughly eight or nine per thousand live births, and modern surgical and catheter treatment means the great majority now survive to adulthood. The result is a demographic shift: population data from Quebec show that between 2000 and 2010 the prevalence of congenital heart disease rose across all ages, and that adults came to outnumber children among those living with it, with the fastest growth in the most complex lesions. [5] [13]
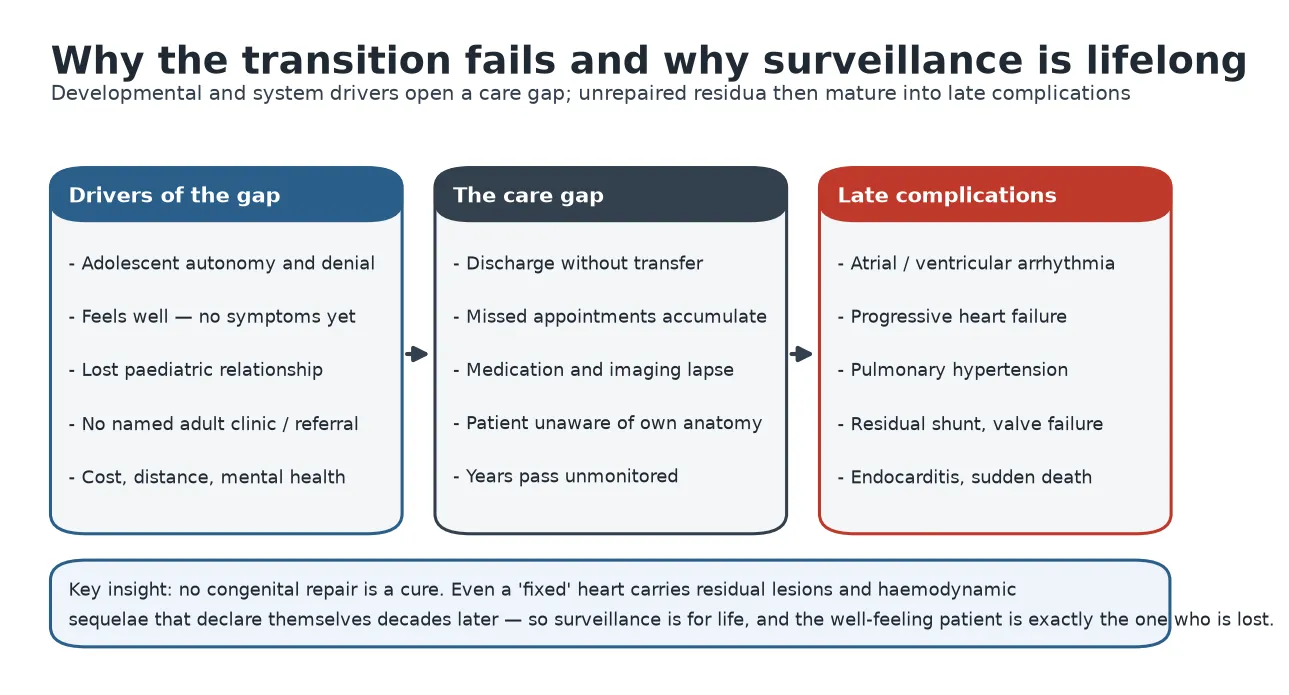
That growing adult population is precisely the group most at risk of falling out of care. Studies of patients who should be in lifelong follow-up find that a substantial proportion have a gap in specialist care, and that these gaps are more common in adolescence and young adulthood, in those with less complex-appearing lesions, and in those who feel well. Feeling well is a risk factor for disengagement, not a marker of safety. [4] [6]
The numbers that frame the transition problem
The risk factors for loss to follow-up are worth committing to memory because they identify who to protect. They include a transfer of care that is never completed, a patient who feels well and sees no need, geographic distance and cost, poor understanding of the diagnosis, mental-health and neurodevelopmental difficulty, socioeconomic disadvantage, and the lack of a named adult clinic to receive the patient. Each is a lever a structured transition programme can pull. [4] [6]
Pathophysiology
The conceptual engine of this topic is simple to state and central to everything that follows: no congenital heart repair is a cure. A repair converts a lethal or disabling anatomy into a survivable one, but it almost always leaves residual lesions and imposes new haemodynamic sequelae that progress over decades. The well-looking adult carries a heart that is still abnormal. [1] [13]
Consider the substrates the surveillance is looking for. Repaired tetralogy of Fallot leaves chronic pulmonary regurgitation that slowly dilates the right ventricle and generates atrial and ventricular arrhythmia. An atrial switch for transposition leaves the morphological right ventricle pumping to the body, and that systemic right ventricle fails over time. A Fontan circulation runs the venous return to the lungs without a pumping ventricle, and decades later produces arrhythmia, protein-losing enteropathy, liver disease, and thromboembolism. Each is a delayed, predictable consequence of the original physiology. [1] [2]
[4] [6]The transition failure and the pathophysiology therefore interlock. The developmental push toward autonomy, the absence of symptoms, and a care system that discharges rather than transfers open a gap; the untreated natural history of the residual lesion fills that gap with a complication. Preventing the gap is preventing the complication. [3] [13]
Clinical Presentation
The young person in transition usually presents in one of a few recognisable ways, and each shapes the consultation. Most common is the well adolescent attending a routine review, where the clinical task is preventive: build readiness, counsel on adult-life issues, and secure the onward referral before anything goes wrong. This is the presentation where the future is decided. [3] [1]
Less welcome is the young adult who returns after a gap in care, often prompted by a new symptom, a pregnancy, or an incidental finding. Here the task is to re-stage the lesion, catch up the missed surveillance, and re-establish the therapeutic relationship without judgement. The history should map when and why care lapsed, because that story guides how to keep them engaged this time. [4] [6]
The most concerning presentation is the symptomatic patient. New palpitations point to atrial arrhythmia, which is poorly tolerated in many ACHD circulations. Falling exercise tolerance, exertional breathlessness, oedema, or syncope point to ventricular dysfunction, a failing valve or conduit, or pulmonary hypertension. Any of these in a patient with moderate or complex disease is an urgent ACHD problem, not a routine one. [1] [2]
[1] [8]Differential Diagnosis
The "differential" in transition is less about competing diagnoses and more about correctly attributing a new symptom in a patient whose baseline is already abnormal. Breathlessness in a repaired tetralogy patient could be pulmonary regurgitation with right-ventricular failure, atrial arrhythmia, a residual shunt, or a wholly non-cardiac cause such as asthma or anxiety. The discipline is to test each against the known anatomy rather than to reassure by pattern. [1] [2]
New palpitations
- Atrial flutter or tachycardia (common in ACHD)
- Poorly tolerated in Fontan and systemic RV
- Needs ECG, Holter, and urgent ACHD review
- Not to be dismissed as benign ectopy
Breathlessness or reduced tolerance
- Ventricular dysfunction or failing conduit
- Progressive valve disease or shunt
- Pulmonary hypertension
- Non-cardiac: asthma, anaemia, deconditioning
Cyanosis or falling saturation
- Right-to-left shunt, Eisenmenger physiology
- Fontan fenestration or collateral
- Demands ACHD assessment
- Never assume it is chronic and stable
A second differential worth naming is the distinction between a lesion that is stable and one that is silently progressing. Because ACHD substrates fail without symptoms, the answer often lies not in the history but in comparing current imaging and rhythm monitoring with the patient's own previous studies. The most useful comparator in ACHD is the same patient a year or two earlier. [1] [6]
Finally, the psychosocial differential deserves equal weight. Non-adherence, mental-health difficulty, substance use, and disengagement can present as "missed appointments" or as somatic symptoms, and they are as much a part of the transition assessment as the echocardiogram. Naming them opens the door to the support that keeps the patient in care. [3] [6]
Clinical & Bedside Assessment
The transition consultation has two layers that run side by side: the cardiac assessment of the lesion and the developmental assessment of the young person's readiness. Both deserve deliberate attention, and it is easy to do the first well and neglect the second. Start by seeing the adolescent for part of the visit without the parent, because independence is built, not assumed. [3] [14]
The cardiac bedside assessment is lesion-specific but always includes the resting oxygen saturation, the blood pressure in the arm (and legs where coarctation is relevant), the rhythm, the presence and character of murmurs and prosthetic sounds, and signs of heart failure or cyanosis. A structured record of the baseline lets the next clinician recognise change. The examination is also the moment to confirm the patient can describe their own anatomy and operations. [1] [2]
[14] [3]The developmental assessment asks whether the young person knows their diagnosis and its name, can list their medications and why they take them, can book and attend an appointment, knows the warning symptoms, and understands the adult-life issues of contraception, pregnancy, exercise, and endocarditis risk. Each gap identified is a teaching target for the visits that remain before transfer. [3] [14]
Investigations
Investigation in ACHD is lesion-specific surveillance rather than a single diagnostic test, and its purpose is to detect silent progression in time to act. Every patient has a baseline of a twelve-lead ECG and a resting oxygen saturation, and most have periodic transthoracic echocardiography as the workhorse of anatomical and functional follow-up. The interval follows the complexity grade. [1] [2]
The lesion-specific surveillance toolkit
Twelve-lead ECG and resting oxygen saturation at every visit as the cheap, sensitive baseline.
Transthoracic echocardiography as the routine assessment of chamber size, function, valves, and shunts.
Cardiac MRI for right-ventricular volumes in repaired tetralogy and for anatomy that echocardiography cannot see.
Holter or extended rhythm monitoring for palpitations and for scheduled arrhythmia surveillance in high-risk lesions.
Cardiopulmonary exercise testing to quantify functional capacity and track decline objectively over time.
Blood tests including natriuretic peptides, full blood count, iron studies, and liver and renal function where relevant.
Liver assessment (imaging, and fibrosis surveillance) in the Fontan circulation.
Compare every study with the patient's own previous results — the trend is the finding.
Cardiac magnetic resonance imaging has become central to ACHD surveillance because it quantifies right-ventricular volumes and function and pulmonary regurgitant fraction, which drive the timing of pulmonary valve replacement in repaired tetralogy of Fallot far better than echocardiography can. Cardiopulmonary exercise testing adds an objective, reproducible measure of functional decline that often precedes symptoms. Together they turn "the patient feels well" into measurable data. [1] [2]
Specific circulations demand specific surveillance. The Fontan patient needs periodic liver assessment for Fontan-associated liver disease, and monitoring for arrhythmia, thromboembolism, and protein-losing enteropathy. The cyanotic patient needs a full blood count and iron studies, because iron-deficient erythrocytosis is both common and treatable. Building these lesion-specific schedules into the transfer document is part of a safe handover. [2] [13]
Management — Resuscitation
When a patient with ACHD decompensates acutely, the resuscitation is shaped by the underlying physiology, and the single most important early move is to reach the ACHD service and the patient's own records fast, because a generic approach can harm a fragile circulation. The commonest acute event is a fast atrial arrhythmia, which many ACHD circulations tolerate badly and which can precipitate rapid haemodynamic collapse. [1] [2]
New atrial flutter or tachycardia in a patient with a Fontan circulation or a systemic right ventricle is an emergency, not a nuisance, because loss of atrial transport and the rapid rate can drop cardiac output steeply. Early rate or rhythm control, anticoagulation, and prompt discussion with the ACHD electrophysiology service are the priorities, and cardioversion is often needed sooner than in a structurally normal heart. Treat the rhythm as a haemodynamic emergency. [1] [2]
[2] [8]For any ACHD patient who has a cardiac arrest, standard advanced life support applies, but the reversible causes must be read through the lens of the anatomy — arrhythmia, shunt, obstruction, hypoxia, and thrombosis are all more likely than in the general population, and early expert input changes the plan. The overarching principle is that the records and the ACHD team are part of the resuscitation. [1] [13]
Management — Definitive & Stepwise
The definitive management of transition is the structured programme itself, delivered stepwise across adolescence. The goal is a young adult who understands and owns their condition, arrives at a named adult clinic without a gap, and is equipped for the medical and social realities of adult life. The steps run from early preparation, through readiness-building, to a deliberate transfer, into lifelong adult care. [3] [1]
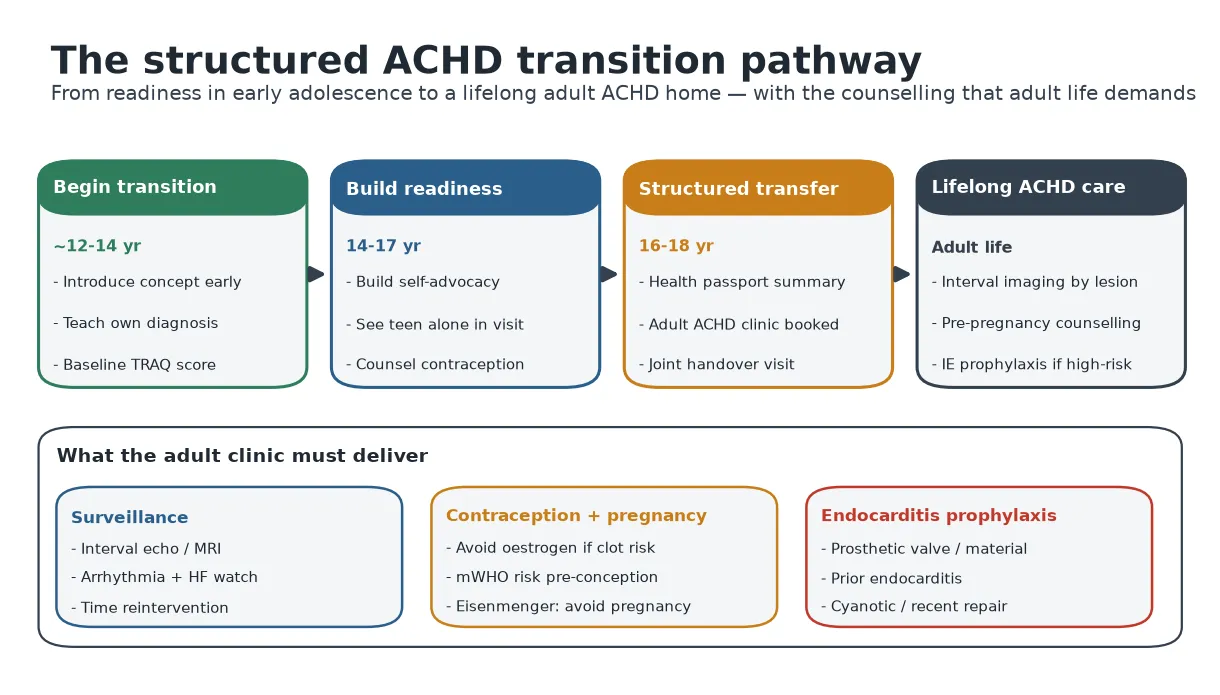
Begin early. From around twelve to fourteen years, introduce the idea that care will one day move to an adult service, and start teaching the young person the name and nature of their own condition. This is also the point to take a baseline readiness measure so progress can be tracked. Early, gentle framing prevents the transfer feeling like abandonment. [3] [14]
Build readiness through the middle-adolescent years. See the young person alone for part of each visit, hand over responsibility for knowing their medications and booking appointments, and cover the adult-life topics of contraception, exercise, alcohol and drugs, tattoos and piercings, careers, and insurance. Readiness, measured and documented, should determine when transfer happens, ideally at a stable time rather than during a crisis or an exam year. [3] [14]
The transition timeline
Deliver the transfer deliberately, not administratively. Prepare a written health summary — a portable record of the diagnosis, operations, current medications, allergies, surveillance plan, and warning symptoms — that the patient carries and understands. Identify the specific adult ACHD clinic, book the first appointment, and where possible use a joint or overlapping clinic so the young person meets the adult team before the paediatric relationship ends. Confirm attendance rather than assuming a referral equals engagement. [3] [1]
Then sustain lifelong care. The adult clinic delivers the lesion-specific surveillance, times reinterventions early rather than late, and carries the adult-life counselling — contraception, pre-pregnancy risk assessment, and endocarditis prophylaxis — that the following sections detail. Active recall and re-engagement of anyone who lapses is a standing task, not an afterthought. [1] [6]
Specific Subtypes & Scenarios
The adult-life counselling that transition must deliver has three high-yield strands, and each is examinable in its own right: contraception, pregnancy, and infective endocarditis prophylaxis. Handle each explicitly, because they are the areas where a well-meaning generalist most easily gives dangerous advice. [7] [11]
Contraception must be matched to the lesion. Combined oestrogen-containing methods raise thrombotic risk and are contraindicated in lesions with a Fontan circulation, cyanosis, pulmonary arterial hypertension, prior thromboembolism, or atrial arrhythmia. Progestogen-only methods and long-acting reversible contraception — the progestogen implant and intrauterine devices — are generally safe and effective and are the preferred options for most higher-risk lesions. The intrauterine device is highly effective, and although a vasovagal reaction at insertion is a theoretical concern in fragile circulations, insertion can be planned safely. An effective method matters most in the very lesions where pregnancy is most dangerous. [7] [1]
Pregnancy risk is stratified with the modified WHO classification, which is the single most useful pregnancy tool in this population. Class I lesions (a repaired simple defect) carry near-normal risk; class II–III lesions need specialist care; class III lesions (a Fontan circulation, a systemic right ventricle, cyanotic disease) carry high risk needing expert shared maternal-cardiac care; and class IV lesions (Eisenmenger syndrome, severe pulmonary arterial hypertension, severe left heart obstruction, a systemic ventricle with poor function) carry prohibitive maternal mortality and pregnancy is contraindicated. Counsel before conception, not at the first antenatal visit. [7] [8]
| mWHO class | Example lesions | Counselling |
|---|
The registry evidence underpins this counselling. The ROPAC registry showed that maternal and fetal outcomes worsen with lesion severity and are worst in pulmonary hypertension, and the CARPREG II study refined the predictors of maternal cardiac events into a practical risk score. These data let you give a woman a realistic, individualised figure rather than a vague reassurance, which is the essence of pre-pregnancy counselling. [10] [9]
Infective endocarditis prophylaxis is now reserved for the highest-risk lesions and highest-risk procedures only. The high-risk group is a prosthetic heart valve or prosthetic material used in valve repair, previous infective endocarditis, unrepaired cyanotic congenital heart disease, and the first six months after any prosthetic repair (or lifelong if a residual defect persists next to prosthetic material). For these patients, antibiotic prophylaxis is given before dental procedures involving the gingiva or the periapical region or perforation of the oral mucosa. Standard adult prophylaxis is amoxicillin 2 g orally (children 50 mg/kg, maximum 2 g) taken 30 to 60 minutes before the procedure, with clindamycin or another agent for the penicillin-allergic. Good oral and skin hygiene matters more than antibiotics for lifetime risk. [11] [12]
Complications & Pitfalls
The defining complication of poor transition is loss to follow-up leading to a late, advanced, and often irreversible presentation. The patient who disappears for years returns not with the early atrial ectopy that a clinic would have caught but with established atrial flutter and a dilated, failing ventricle, or with pulmonary hypertension that has become fixed. The complication is the natural history of the lesion, uncorrected because nobody was watching. [4] [6]
The pitfalls that cost marks and patients
Several avoidable pitfalls recur in examinations and in clinic. Discharging rather than transferring — sending a letter and assuming engagement — is the central error. Giving combined oestrogen contraception to a woman with a thrombotic-risk lesion is a dangerous default. Prescribing endocarditis prophylaxis for everyone with a murmur, rather than the narrow high-risk group, is both wrong and a missed teaching opportunity about oral hygiene. And attributing a well-feeling patient's normal examination to a stable heart, without comparing surveillance imaging, misses silent progression. Each pitfall has a simple antidote embedded in a structured programme. [1] [7]
A final pitfall is neglecting the psychosocial and neurodevelopmental dimension. Adults with complex congenital heart disease have higher rates of anxiety, depression, and neurodevelopmental difficulty, and these both worsen adherence and are complications in their own right. A transition that treats only the heart and not the person will lose the person. [3] [13]
Prognosis & Disposition
With a structured transition and sustained specialist follow-up, the outlook for most adults with congenital heart disease is good, and many lead full working, social, and reproductive lives. Prognosis tracks the complexity of the lesion and, crucially, whether surveillance catches progression in time to intervene. Continuity of care is itself prognostic. [1] [13]
Disposition is lifelong shared care anchored at an ACHD centre, with the intensity set by the complexity grade. Simple lesions may be shared with a well-briefed primary care team; moderate and complex lesions belong at a specialist centre at the intervals already described. The disposition plan is only safe if it is written down, given to the patient, and received by a named clinic that expects them. [1] [6]
The re-engagement of patients who have lapsed is a distinct and important disposition task. When a young adult returns after a gap, the plan is to re-stage the lesion fully, resume the appropriate surveillance interval, address the reason for disengagement, and rebuild the relationship so the next gap does not occur. A patient found again is a success to be protected, not a defaulter to be scolded. [4] [6]
Special Populations
Adolescents with neurodevelopmental or intellectual disability need transition planning that involves carers and adult disability and cardiac services together, with communication pitched to the young person's understanding and decision-making capacity assessed and supported. Readiness tools may need adaptation, and the goal is the greatest possible autonomy with the right scaffolding rather than a one-size transfer. [3] [13]
Indigenous, rural, and remote young people face distance, cost, and cultural barriers that raise the risk of loss to follow-up, and Aboriginal and Torres Strait Islander and Māori and Pasifika communities also carry a high burden of rheumatic heart disease alongside congenital disease. Telehealth-linked shared care, culturally safe services, active recall, and a portable health summary are practical protections, and the transition plan should name a local contact as well as the distant specialist centre. [6] [13]
Young women approaching reproductive age are a priority population for the contraception and pregnancy counselling detailed above, because an unplanned pregnancy in a high-risk lesion is one of the most dangerous events in ACHD. Proactive, repeated, and non-judgemental discussion of contraception and pre-pregnancy risk from mid-adolescence is core transition work, not an optional add-on. [7] [8]
Socioeconomically disadvantaged and mentally unwell young people are over-represented among those lost to follow-up, and mental-health difficulty both drives disengagement and worsens outcomes. Integrating psychological support, addressing cost and transport, and flagging these patients for active recall are part of an equitable transition programme. [6] [3]
Evidence, Guidelines & Regional Differences
The AHA scientific statement on best practices in transition set out the process model — start early, build readiness, transfer deliberately — that underpins modern programmes, and validated tools such as the TRAQ made readiness measurable. The gaps-in-care and loss-to-follow-up studies provide the epidemiological justification, quantifying how many young people fall out of care and when, and identifying the modifiable risk factors a programme can target. [3] [14]
| Issue | Consensus | Regional variation |
|---|
The main area of genuine change over recent decades has been endocarditis prophylaxis, which contracted sharply from the broad indications of earlier eras to the current narrow high-risk group, on the reasoning that daily bacteraemia from ordinary activities outweighs procedural bacteraemia and that antibiotic harms and resistance matter. A residual transatlantic nuance persists in exactly which procedures and lesions are covered, but the principle — prophylaxis for the highest-risk lesions and dental procedures, with oral hygiene as the mainstay — is shared. ANZ practice follows this consensus and adapts it to the geography of a small number of ACHD centres serving dispersed populations. [11] [12]
Exam Pearls
References
- [1]Stout KK, Daniels CJ, Aboulhosn JA, Bozkurt B, Broberg CS, et al. 2018 AHA/ACC Guideline for the Management of Adults With Congenital Heart Disease J Am Coll Cardiol, 2019.PMID 30121239
- [2]Baumgartner H, De Backer J, Babu-Narayan SV, Budts W, Chessa M, et al. 2020 ESC Guidelines for the management of adult congenital heart disease. Eur Heart J, 2021.PMID 32860028
- [3]Sable C, Foster E, Uzark K, Bjornsen K, Canobbio MM, et al. Best practices in managing transition to adulthood for adolescents with congenital heart disease: the transition process and medical and psychosocial issues: a scientific statement from the American Heart Association. Circulation, 2011.PMID 21357825
- [4]Mackie AS, Ionescu-Ittu R, Therrien J, Pilote L, Abrahamowicz M, Marelli AJ Children and adults with congenital heart disease lost to follow-up: who and when? Circulation, 2009.PMID 19597053
- [5]Marelli AJ, Ionescu-Ittu R, Mackie AS, Guo L, Dendukuri N, Kaouache M Lifetime prevalence of congenital heart disease in the general population from 2000 to 2010. Circulation, 2014.PMID 24944314
- [6]Gurvitz M, Valente AM, Broberg C, Cook S, Stout K, et al. Prevalence and predictors of gaps in care among adult congenital heart disease patients: HEART-ACHD J Am Coll Cardiol, 2013.PMID 23542112
- [7]Regitz-Zagrosek V, Roos-Hesselink JW, Bauersachs J, Blomström-Lundqvist C, Cífková R, et al. 2018 ESC Guidelines for the management of cardiovascular diseases during pregnancy. Eur Heart J, 2018.PMID 30165544
- [8]Canobbio MM, Warnes CA, Aboulhosn J, Connolly HM, Khanna A, et al. Management of Pregnancy in Patients With Complex Congenital Heart Disease: A Scientific Statement for Healthcare Professionals From the American Heart Association. Circulation, 2017.PMID 28082385
- [9]Silversides CK, Grewal J, Mason J, Sermer M, Kiess M, et al. Pregnancy Outcomes in Women With Heart Disease: The CARPREG II Study. J Am Coll Cardiol, 2018.PMID 29793631
- [10]Roos-Hesselink JW, Ruys TP, Stein JI, Thilén U, Webb GD, et al. Outcome of pregnancy in patients with structural or ischaemic heart disease: results of a registry of the European Society of Cardiology. Eur Heart J, 2013.PMID 22968232
- [11]Wilson W, Taubert KA, Gewitz M, Lockhart PB, Baddour LM, et al. Prevention of infective endocarditis: guidelines from the American Heart Association Circulation, 2007.PMID 17446442
- [12]Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, et al. 2015 ESC Guidelines for the management of infective endocarditis Eur Heart J, 2015.PMID 26320109
- [13]Bhatt AB, Foster E, Kuehl K, Alpert J, Brabeck S, et al. Congenital heart disease in the older adult: a scientific statement from the American Heart Association. Circulation, 2015.PMID 25896865
- [14]Sawicki GS, Lukens-Bull K, Yin X, Demars N, Huang IC, et al. Measuring the transition readiness of youth with special healthcare needs: validation of the TRAQ J Pediatr Psychol, 2011.PMID 20040605