Paeds · cardiology
Cyanotic newborn and critical congenital heart disease screening
Also known as critical congenital heart disease screening · CCHD screening · newborn pulse oximetry screening · duct-dependent congenital heart disease · the cyanotic newborn · congenital cyanotic heart disease
A fellowship approach to the cyanotic newborn and critical congenital heart disease screening: read pulse oximetry as a layered screen that catches what antenatal scanning and the newborn examination miss, apply the ≥24-hour SpO₂ thresholds (≥95% pass, 90–94% repeat, <90% refer), start prostaglandin E1 before the echocardiogram when a duct-dependent lesion is suspected, and distinguish cyanotic congenital heart disease from pulmonary, sepsis and persistent-pulmonary-hypertension mimics using the hyperoxia test and bedside examination.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A baby in the postnatal ward looks dusky at feed time but settles in oxygen; or a term infant collapses at forty-eight hours, grey and gasping, the femoral pulses vanished; or a routine oxygen-saturation check on the second day returns 82 per cent and the nursing staff cannot believe the child looks well. The fellowship task in each is the same: treat a low oxygen saturation in a neonate as a heart lesion until an echocardiogram proves otherwise, apply the pulse-oximetry thresholds without softening them, and reopen the duct before the baby arrests. [1] [3]
Overview & Definition
A cyanotic newborn is an infant whose blood is carrying deoxygenated haemoglobin in the systemic circulation, and the colour is the visible end of a pathophysiological process that may be cardiac, pulmonary, neurological or haematological. Critical congenital heart disease narrows that list to the structural heart defects that threaten life in the first year and need surgery or a catheter procedure, and the cyanotic subgroup of those defects works by shunting venous blood across into the arterial side without passing through the lungs. The fellowship skill is to hold both ideas at once: cyanosis is a sign, and CCHD is the subset of causes where delay kills. [2] [7]
Newborn screening for CCHD is the structured programme that looks for these lesions before they declare themselves as collapse. It has three layers — antenatal ultrasound, the newborn clinical examination, and pulse oximetry at or after 24 hours of age — and the layers fail independently, which is why they are stacked. No single layer is sensitive enough on its own, and the pulse-oximetry layer exists specifically to catch the duct-dependent lesions that look well at birth and close their ductus on the second or third day. [1] [10]
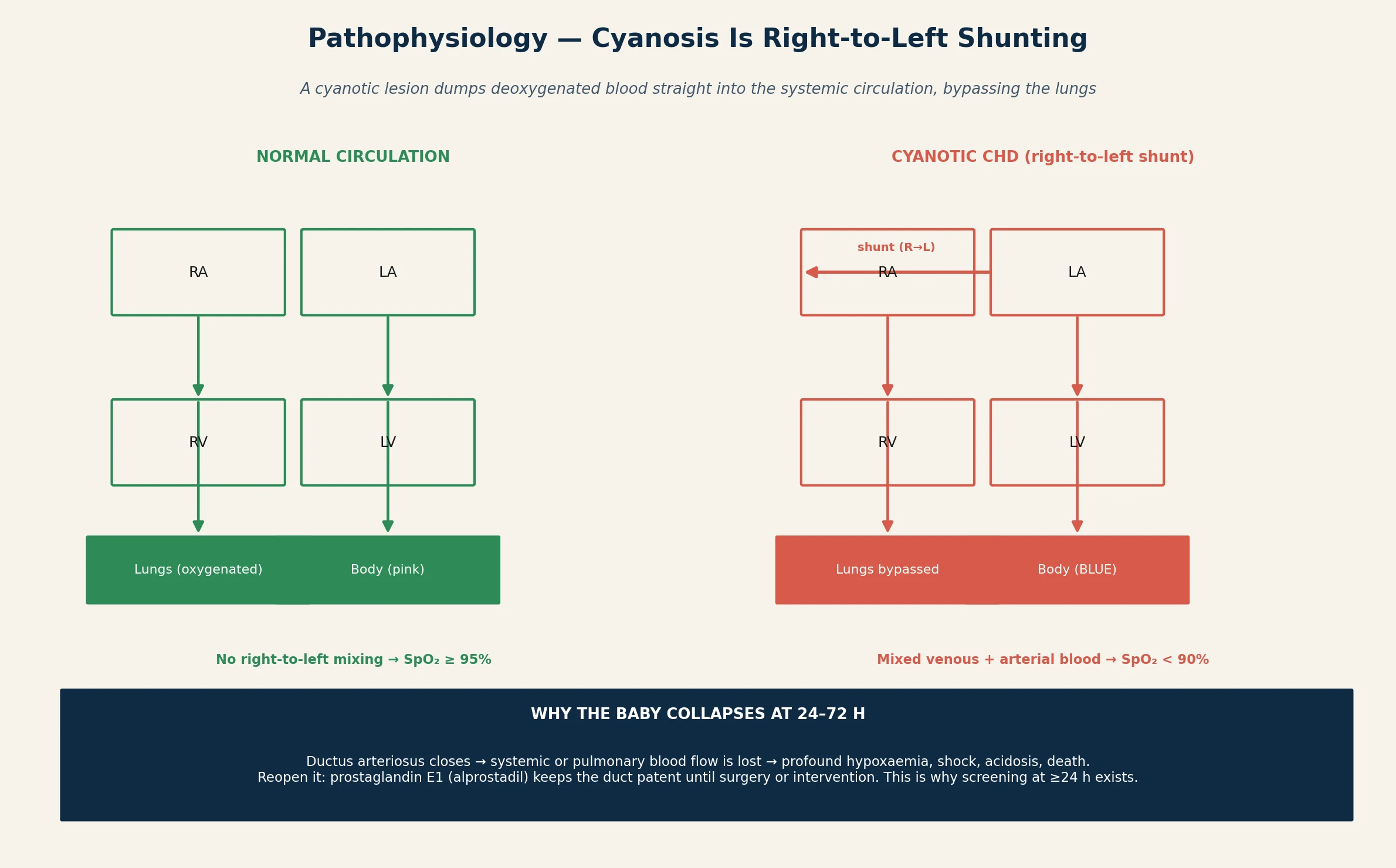
The reason the topic carries critical priority is that the missed lesion behaves as a time bomb. A duct-dependent circulation supplies the body through the ductus arteriosus while it stays open, and the duct closes physiologically in the first days of life. When it closes in a baby who needs it, systemic or pulmonary blood flow is lost, the child becomes profoundly hypoxaemic and acidotic, and without prostaglandin E1 to reopen it the outcome is shock, end-organ injury and death. The whole screening programme exists to find that child before the duct closes, not after. [2] [8]
Classification
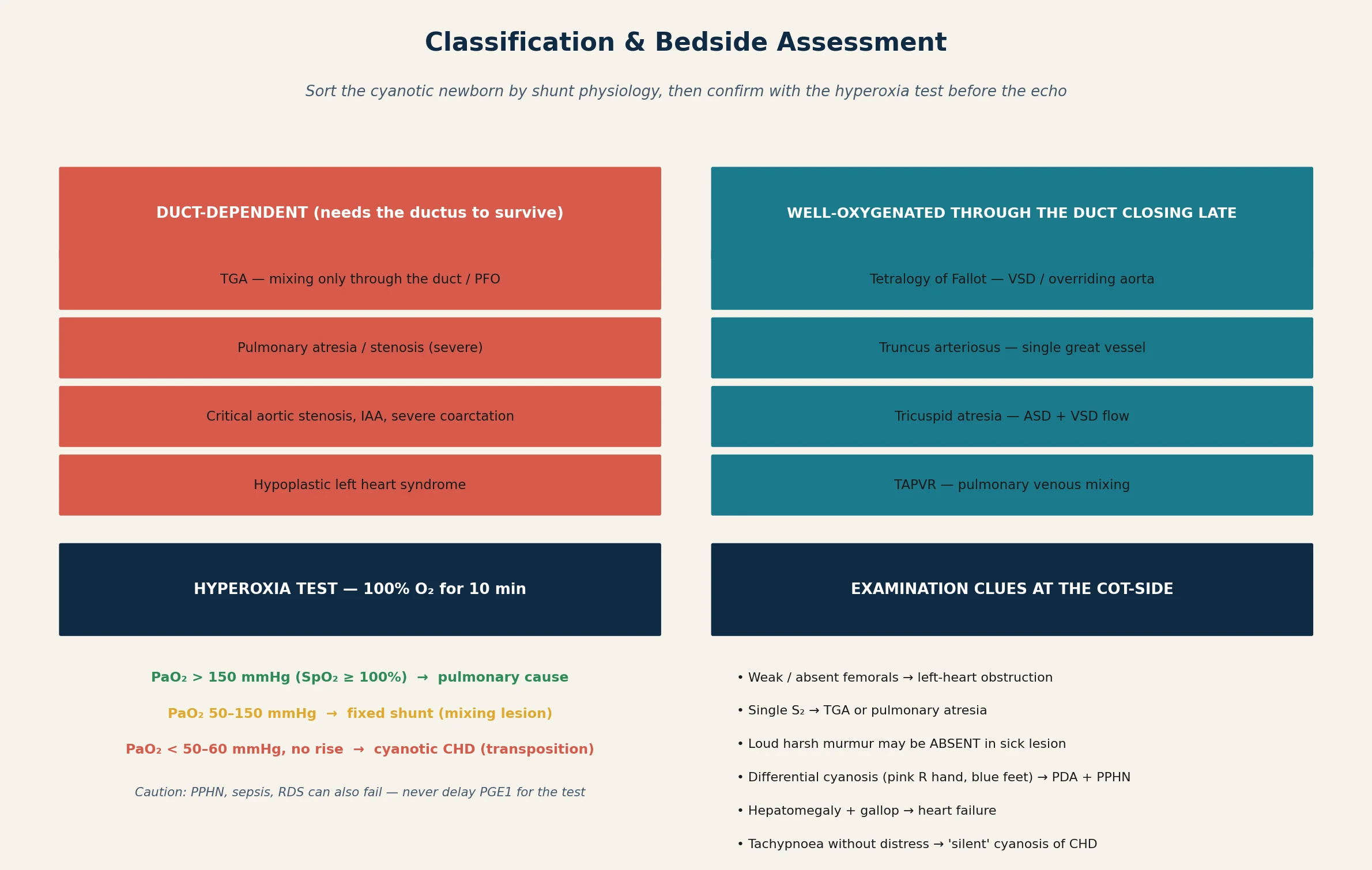
The most useful classification splits congenital heart disease into acyanotic and cyanotic, and then splits the cyanotic group into duct-dependent and non-duct-dependent. Duct-dependent circulation means the baby survives only while the ductus arteriosus stays patent, either because systemic flow depends on it (left-heart obstruction — coarctation, interrupted aortic arch, hypoplastic left heart, critical aortic stenosis) or because pulmonary flow depends on it (right-heart obstruction — pulmonary atresia, severe pulmonary stenosis, tricuspid atresia). Transposition sits beside these because its only mixing route is often the duct. [2] [10]
The classical teaching device for the cyanotic lesions is the 'five Ts': Tetralogy of Fallot, Transposition of the great arteries, Tricuspid atresia, Truncus arteriosus, and Total anomalous pulmonary venous return. They are worth memorising as the list an examiner expects, but they overlap physiologically — tetralogy and truncus are mixing lesions that may tolerate duct closure, while transposition, pulmonary atresia and tricuspid atresia are often duct-dependent. Knowing which physiology applies to each lesion is what tells you whether prostaglandin E1 will rescue the child. [2]
From a screening standpoint the classification that matters is the one that predicts collapse. Duct-dependent lesions are the ones pulse oximetry is designed to catch, because they look well at birth, pass the early newborn examination, and then deteriorate as the duct closes. Non-duct-dependent cyanotic lesions such as a well-compensated tetralogy may present with a murmur or a gradual fall in saturation, and the screen still flags them. The two classifications work together: physiology drives the urgency, anatomy drives the surgery. [1] [4]
Epidemiology & Risk Factors
Congenital heart disease is the most common birth defect, occurring in roughly nine per thousand live births worldwide, and about a quarter of these lesions are critical in the sense of needing intervention in infancy. Within the critical group, roughly half are duct-dependent, which is the subgroup the pulse-oximetry screen is built to find. These figures are why a general paediatrician working anywhere with a postnatal ward will meet this problem. [7] [2]
The reason a dedicated screen is needed is that the two older layers miss a clinically important fraction. Antenatal ultrasound picks up only about half of critical lesions even in high-performing systems, because views are limited by fetal position, maternal habitus and sonographer skill, and the newborn clinical examination misses roughly half of those that present after discharge. The cumulative miss rate of the two traditional layers is what creates the population of infants who collapse at home in the first week, and pulse oximetry was added precisely to close that gap. [1] [3]
Risk factors for congenital heart disease cluster into maternal, fetal and genetic groups. Maternal diabetes, rubella and certain medications (lithium, some antiepileptics, retinoic acid), a family history of congenital heart disease, and syndromal associations — Down syndrome, Turner, Noonan, 22q11.2 deletion, Williams — all raise the probability and should lower the threshold for echocardiography. A murmur or a low saturation in any of these contexts is cardiology, not watchful waiting. [2] [7]
Pathophysiology
Cyanosis from a heart lesion is, at its core, a right-to-left shunt. Deoxygenated venous blood crosses from the right heart into the left side, or mixes in a common chamber, and reaches the systemic arteries without being oxygenated in the lungs. The arterial oxygen content falls, and once the amount of reduced haemoglobin passes about three to five grams per decilitre the skin and mucous membranes look blue. Central cyanosis is therefore a perfusion and shunt problem, not a lung problem alone, and that distinction drives the whole bedside assessment. [2]
The duct-dependent physiology deserves its own explanation because it is the mechanism of collapse. In a normal fetus the ductus arteriosus carries most of the right ventricular output into the descending aorta, bypassing the lungs, and it closes functionally in the first days of life. When the heart is built so that the body or the lungs depend on that duct — an obstructed left heart sending flow forward through the duct, or an obstructed right heart sending pulmonary flow through it — duct closure removes the only route for blood to reach its destination. The child crashes not because the lesion is new but because the lifeline has gone. [2] [8]
Prostaglandin E1 works by reversing that closure. It relaxes the ductal smooth muscle and keeps the ductus patent, restoring whichever flow was lost, and it buys the hours or days needed to reach a cardiac centre, image the anatomy and plan surgery or catheter intervention. The same drug explains why early detection matters so much: a baby who is found before collapse can be resuscitated cleanly, while a baby who arrests at home may arrive acidotic and brain-injured even if the lesion is repairable. [8] [9]
Clinical Presentation
The classic cyanotic-newborn presentation is the well-appearing infant who is blue without respiratory distress. This 'silent cyanosis' is the single most examinable presentation, because it separates congenital heart disease from lung disease: a baby with a serious pulmonary cause is usually working hard to breathe, while a baby with a right-to-left shunt can look comfortable and merely blue. A neonate who is tachypnoeic without distress, or dusky only on feeding or crying, earns a saturation check and an echocardiogram. [2] [10]
The dangerous presentation is sudden collapse between 24 and 72 hours of age. The ductus closes, the duct-dependent circulation loses its flow, and the child becomes grey, mottled, tachypnoeic and then apnoeic, with weak pulses, a metabolic acidosis and progressive shock. This is the presentation the screening programme is trying to prevent, and it is the one where the immediate move is prostaglandin E1, not a diagnostic work-up. Families often describe the baby as 'feeding poorly' or 'going cold' in the hours before arrest, and those prodromal signs are worth teaching to parents as safety-net advice. [2] [8]
Subacute presentations matter too. A tetralogy of Fallot may announce itself with a harsh ejection systolic murmur at the left sternal edge and intermittent cyanotic spells that worsen with crying, and total anomalous pulmonary venous return can present as gradual respiratory distress with hepatomegaly. Truncus arteriosus often presents with a systolic murmur and a single second sound. The common thread is that the murmur may be unimpressive or absent, so its absence never closes the search for heart disease in a cyanotic child. [2] [11]
Differential Diagnosis
The differential of neonatal cyanosis splits into cardiac, pulmonary, neurological and haematological causes, and the bedside skill is to sort them quickly rather than to list them. Cardiac causes are the cyanotic congenital lesions. Pulmonary causes include respiratory distress syndrome, transient tachypnoea, meconium aspiration, congenital diaphragmatic hernia, and persistent pulmonary hypertension of the newborn. Neurological depression from birth asphyxia or sedation causes hypoventilation, and methaemoglobinaemia is the rare but treatable haematological mimic. [2]
The hyperoxia test is the historical bedside discriminator, and it remains a teaching and reasoning tool even where echocardiography is readily available. The baby breathes 100 per cent oxygen for ten minutes, and the response of the partial pressure of oxygen locates the problem. A PaO₂ above 150 mmHg points to a pulmonary cause, a PaO₂ between roughly 50 and 150 mmHg suggests a fixed mixing shunt, and a PaO₂ below 50 to 60 mmHg with no rise is characteristic of transposition. The test is not perfect — persistent pulmonary hypertension and sepsis can also fail to respond — and it must never delay prostaglandin E1 when a duct-dependent lesion is on the cards. [2] [10]
Persistent pulmonary hypertension of the newborn is the most important mimic to separate from cyanotic heart disease, because both produce severe hypoxaemia with minimal radiographic lung disease. The distinguishing clue is differential cyanosis: a pink right hand (pre-ductal) with blue feet (post-ductal) indicates right-to-left flow across the ductus driven by high pulmonary pressures, which is the physiology of persistent pulmonary hypertension as much as of some cardiac lesions. An echocardiogram resolves both the anatomy and the pulmonary pressures, and in a sick neonate it is the single most informative test. [2]
| Cause | Hallmark | Distraction | Resolving move |
|---|---|---|---|
| Cyanotic CHD | Silent cyanosis, single S₂, weak femorals | May have NO murmur | Echo; start PGE1 if duct-dependent |
| RDS / TTN | Grunting, recessions, prematurity | Improves in O₂ | CXR; surfactant if RDS |
| PPHN | Differential cyanosis, loud P2 | Fails hyperoxia test | Echo; consider iNO, oxygen |
| Sepsis / pneumonia | Fever or temperature instability, lethargy | Mimics everything | Bloods, cultures, antibiotics early |
| Methaemoglobinaemia | Cyanosis despite high PaO₂ | Chocolate-brown blood | Methaemoglobin level; methylene blue |
Clinical & Bedside Assessment
The assessment begins with the recognition that a low saturation in a neonate is a cardiology signal, and it proceeds to a focused examination that looks for the anatomy and the physiology. Feel all four limb pulses — weak or absent femorals point to left-heart obstruction, and unequal limb pulses or a blood-pressure gradient between arms and legs point to coarctation or interrupted arch. Listen for the second heart sound: a single or loudly split S₂ suggests transposition or pulmonary atresia, and a normal split with a harsh murmur suggests a mixing lesion such as tetralogy. [2] [11]
Murmurs are a clue, never a gate. General paediatricians detect only a minority of congenital heart disease by auscultation, and the lesions that present with collapse — transposition, hypoplastic left heart — are frequently silent because the obstruction equalises pressures and produces no turbulent flow. A fellow who waits for a murmur before referring will miss the sickest babies. The presence of a murmur moves the work-up toward cardiology, but its absence does not move it away. [11]
The general examination adds the signs of cardiac failure and the syndromal context. Hepatomegaly, a gallop rhythm, poor perfusion and tachypnoea mark the failing circulation, and the dysmorphic features of Down, Turner, Noonan, 22q11.2 and Williams syndromes each raise the pre-test probability of a specific lesion. Plot the growth and feeding pattern, because faltering growth or tiring on feeds is often the earliest sign of an unrecognised lesion, and combine the bedside findings into a problem representation before ordering the echo. [2]
The four-limb blood pressure and the pre-ductal and post-ductal saturations are part of the examination, not an investigation. A systolic pressure difference greater than 10 to 20 mmHg between the arms and the legs suggests aortic coarctation, and a saturation difference greater than 3 per cent between the right hand and a foot is a positive screen regardless of the absolute value. Measuring both is quick, and it converts a vague 'blue baby' into a structured cardiology referral. [2] [3]
Investigations
Pulse oximetry is the screening test, and its thresholds are the most testable numbers in the topic. In a well baby at or after 24 hours of age, measure the saturation in the right hand (pre-ductal) and in either foot (post-ductal). A SpO₂ of 95 per cent or more in both with less than 3 per cent difference is a pass; a SpO₂ between 90 and 94 per cent, or a difference greater than 3 per cent, prompts a repeat in one to two hours; and a SpO₂ below 90 per cent in either site at any time is a fail and a referral. Timing matters, because screening before 24 hours raises the false-positive rate as the normal transitional cyanosis resolves. [2] [4]
The diagnostic test is the echocardiogram, and in a sick neonate it is the single most informative investigation because it defines the anatomy, the ductal dependency and the pulmonary pressures in one study. A chest radiograph adds supportive clues — the 'egg-on-string' boot-shaped heart of transposition, the boot-shaped heart of tetralogy, pulmonary oligaemia or plethora, and the size and shape of the cardiac silhouette — but it never replaces the echo. An electrocardiogram is low-yield in most neonatal lesions but can flag right-heart strain or an ischaemic pattern. [2]
The blood gas and the septic screen are part of the work-up because cyanosis and collapse have a differential, and a child can have both a heart lesion and sepsis. A venous or arterial gas quantifies the hypoxaemia, the carbon dioxide retention and the metabolic acidosis that mark the severity of the circulation, and a lactate tracks the resuscitation. Blood cultures, inflammatory markers and a full blood count are sent early, and broad-spectrum antibiotics are reasonable while the picture clarifies, because the cost of treating presumed sepsis is small and the cost of missing it is large. [2]
The hyperoxia test and the four-limb blood pressures complete the bedside set, and in a centre where echocardiography is delayed they carry real diagnostic weight. The combination of a failed hyperoxia test, differential saturations, weak femoral pulses and a metabolic acidosis is enough to start prostaglandin E1 before the cardiologist arrives, and that decision is the one the fellowship examiner is testing. [2] [10]
Management — Resuscitation
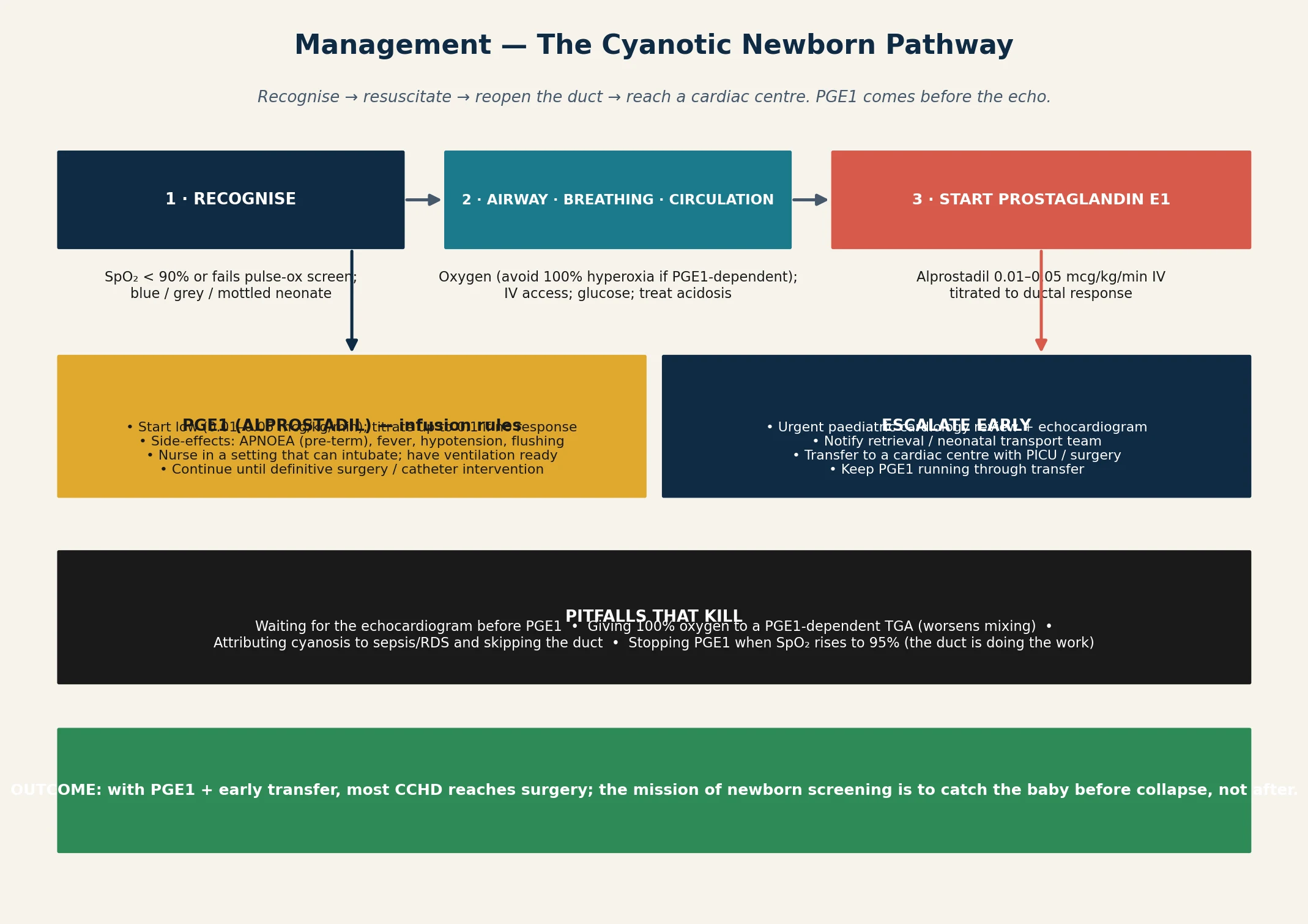
Resuscitation of the cyanotic or collapsing neonate follows a clear order: secure the airway and breathing, support the circulation, and reopen the duct. Give oxygen, but use it judiciously — a baby with a duct-dependent mixing lesion such as transposition may worsen when the afterload falls on high-concentration oxygen, because the systemic-to-pulmonary balance shifts and less blood reaches the body. Establish intravenous access, check and correct the glucose, and treat the acidosis with fluid and ventilation rather than with bicarbonate alone. [2]
The decisive resuscitation drug is prostaglandin E1 (alprostadil), started at a low dose of 0.01 to 0.05 micrograms per kilogram per minute and titrated to the ductal response, increasing toward 0.1 micrograms per kilogram per minute if the saturation does not improve. Low-dose infusion is as effective as higher doses and carries fewer side-effects, which is why the contemporary practice is to start low. The infusion is continued until definitive surgery or catheter intervention, and the baby is nursed where intubation and ventilation are immediately available. [9] [8]
The reason ventilation must be ready is the defining side-effect of prostaglandin E1: apnoea, which is commoner in preterm infants and can be unpredictable. Fever, hypotension, flushing and irritability also occur, and long-term infusion carries a small risk of gastric outlet obstruction and cortical hyperostosis. A baby on the drug who is being retrieved to a cardiac centre is often electively intubated to secure the airway for transport, and that decision sits with the retrieving team. [8] [9]
Sepsis is treated in parallel, not in sequence, because a cyanotic neonate may have both a heart lesion and an infection, and the signs overlap completely. Broad-spectrum antibiotics are started after cultures, the temperature and glucose are supported, and the family is kept informed with honest, early explanation of the working diagnosis and the plan. The resuscitation is judged not by the speed of the echo but by the speed of the duct being reopened and the child being perfused. [2]
Management — Definitive & Stepwise
Definitive management moves from resuscitation to imaging, then to a surgical or catheter-based plan, and it is led by the paediatric cardiologist and the cardiothoracic team. Once the echocardiogram defines the lesion, the team decides between prostaglandin-supported transfer for surgery, an interventional catheter procedure such as a balloon atrial septostomy for transposition, or medical stabilisation and staged repair. The general paediatrician's role is to hold the resuscitation, coordinate the transfer and brief the family while the cardiac plan forms. [2]
Lesion-specific decisions are worth knowing because they change the first hours. Transposition with a restrictive atrial septum needs a balloon atrial septostomy to create mixing, often as an emergency before transfer. Critical coarctation or interrupted aortic arch needs the prostaglandin infusion and a surgical repair. Pulmonary atresia may need a catheter-based intervention or a surgical shunt to secure pulmonary flow. Tetralogy with a favourable anatomy heads toward a complete repair, while a tetralogy with severe cyanosis may need a palliative shunt first. [2] [10]
Transfer to a cardiac centre is a retrieval, not a car journey, and it should be planned with the neonatal or paediatric retrieval team from the moment the diagnosis is suspected. The prostaglandin infusion runs throughout the transfer, the airway is secured if there is any concern about apnoea, and the receiving centre is briefed on the lesion, the saturations, the acid-base status and the family. In rural and remote Australia and Aotearoa New Zealand this step carries real time and distance cost, which is why early local recognition and a low threshold for retrieval matter disproportionately. [2]
Longitudinal care follows the surgery. The repaired child moves into cardiac follow-up with surveillance for residual lesions, arrhythmia, heart failure and neurodevelopmental outcome, and the general paediatrician coordinates growth, immunisation, endocarditis prophylaxis advice and developmental support. The transition from acute neonatal cardiology into a chronic cardiac-life plan is where the topic connects to the wider curriculum, and it begins at the first conversation with the family. [2] [8]
The cyanotic-newborn escalation ladder
Recognise: SpO₂ below 90%, or fails the pulse-ox screen, or collapses at 24–72 h
ABC: oxygen, IV access, glucose, correct acidosis; avoid indiscriminate high-flow O₂ in PGE1-dependent mixing
Start prostaglandin E1 at a low dose; titrate to the ductal response; nurse where intubation is possible
Urgent echocardiogram + paediatric cardiology; treat sepsis in parallel with cultures and antibiotics
Activate retrieval / transfer to a cardiac centre with PGE1 running; secure the airway if needed
Definitive plan: surgery, balloon septostomy, or staged repair; begin cardiac follow-up and family support
Specific Subtypes & Scenarios
Transposition of the great arteries is the archetypal duct-dependent cyanotic lesion, and the one most likely to present as silent cyanosis in a well baby. The aorta arises from the right ventricle and the pulmonary artery from the left, so the systemic and pulmonary circuits run in parallel and survive only where they mix — at the atrial, ductal or ventricular level. Prostaglandin E1 keeps the duct open, a balloon atrial septostomy enlarges the atrial communication if mixing is poor, and the arterial switch operation is the definitive repair. [2] [10]
Tetralogy of Fallot is the commonest cyanotic lesion beyond the neonatal period, combining a ventricular septal defect, an overriding aorta, right ventricular outflow tract obstruction and right ventricular hypertrophy. Neonates may be pink if the obstruction is mild, and the cyanosis deepens as the obstruction progresses or during a 'tet spell'. Severe tetralogy can be duct-dependent for pulmonary flow. Surgical repair is usually definitive, with palliative shunting reserved for unfavourable anatomy or unstable neonates. [2]
The left-heart obstructions — hypoplastic left heart syndrome, critical aortic stenosis, coarctation and interrupted aortic arch — present with shock and poor perfusion as the duct closes, often with weak femoral pulses and a metabolic acidosis rather than striking cyanosis. They are the lesions most easily mislabelled as sepsis, and they depend absolutely on the duct for systemic flow. Prostaglandin E1 is the resuscitation, a staged surgical pathway is the repair, and the general paediatrician's job is to start the drug before the child arrests. [2] [8]
Pulmonary atresia and tricuspid atresia are right-heart obstructions that depend on the duct for pulmonary flow and on an atrial or ventricular communication for any forward flow. They present with cyanosis and a single second sound, they need prostaglandin E1 from the outset, and they follow staged surgical palliation toward a Fontan circulation. Total anomalous pulmonary venous return and truncus arteriosus are mixing lesions that present with cyanosis and cardiac failure; both need early surgical repair, and TAPVR with obstruction is a surgical emergency. [2]
The antenatally detected lesion is its own scenario, and it changes the screening conversation. A fetus with a confirmed cardiac lesion on the anatomy scan is delivered at a centre with neonatal cardiology, the prostaglandin decision is planned in advance, and the pulse-oximetry screen becomes confirmatory rather than discovery. The fellowship teaching is that antenatal detection does not abolish the need for postnatal screening, because views can be limited and lesions can progress — but it does shift the locus of care to a planned, team-based delivery. [2] [7]
Complications & Pitfalls
The cardinal pitfall is waiting for the echocardiogram before starting prostaglandin E1. The drug is safe enough that the risk of giving it to a child who turns out not to have a duct-dependent lesion is far smaller than the risk of withholding it from a child who does, and the duct can close irreversibly during the wait. The fellowship answer is to start the infusion on clinical suspicion and let the echo refine the diagnosis, never the reverse. [8] [9]
The second pitfall is the false reassurance of a normal examination. A baby with transposition can look comfortable, feed normally and have no murmur, and only the saturation check reveals the lesion. Treating the clinical appearance as more reliable than the number is the error that the pulse-oximetry screen was designed to prevent, and it remains the commonest reason a lesion is missed in a baby who has been 'checked'. [2] [11]
Prostaglandin E1 carries its own complications, and they shape how the drug is used. Apnoea is the defining risk and the reason for airway readiness, and it is commoner in preterm infants. Fever, hypotension, flushing and irritability are common and usually manageable with fluids and antipyretics, and long-term infusion is associated with gastric outlet obstruction and cortical hyperostosis. A child on a prolonged infusion before surgery is monitored for these, and the dose is kept at the lowest that maintains the duct. [8] [9]
The oxygen pitfall deserves its own warning. Indiscriminate high-concentration oxygen in a duct-dependent mixing lesion such as transposition can lower systemic vascular resistance, increase pulmonary runoff, and reduce systemic blood flow — worsening the very hypoxaemia it was meant to treat. Oxygen is given to relieve distress and to support the airway, but the saturations are followed and the concentration is not pushed reflexively; the rescue is the prostaglandin, not the oxygen. [2]
Prognosis & Disposition
The prognosis of critical congenital heart disease has transformed over a generation, and the transformation is the argument for screening. Lesions that were uniformly fatal are now repaired in infancy with survival into adulthood, and the single biggest determinant of outcome is whether the child reaches a cardiac centre before collapse. Early detection through antenatal scanning, the newborn examination and pulse oximetry is what shifts a baby from the 'arrested at home' pathway into the 'planned transfer' pathway, and that shift is measured in lives and neurodevelopmental outcomes. [1] [5]
The Swedish cohort that introduced population pulse-oximetry screening showed a fall in the rate of late diagnosis and in mortality from duct-dependent lesions, and that evidence underpinned the global adoption of the screen. Subsequent multicentre and meta-analytic work confirmed a low false-positive rate when screening is done at or after 24 hours, and a detection rate for critical lesions high enough to justify universal implementation. The Cochrane review records pulse oximetry as an accurate, acceptable addition to the existing screens. [1] [4] [5]
Disposition is decided by the lesion and the centre. A confirmed or strongly suspected duct-dependent lesion is transferred to a cardiac centre with the prostaglandin running, while a stable, well-oxygenated child with a non-critical lesion may be managed as an outpatient with early cardiology follow-up. The general paediatrician coordinates the handover, the safety-net advice to the family, and the connection to primary care for the long arc of cardiac surveillance. [2]
Special Populations
Rural and remote communities carry a disproportionate share of the risk, because distance turns a treatable collapse into a retrieval emergency. A baby born hours from a cardiac centre depends entirely on local recognition of a low saturation and a low threshold for starting prostaglandin E1 and activating retrieval. Strengthening the pulse-oximetry screen, the midwifery and nursing education around it, and the retrieval pathways is where the equity gain lies in Australia and Aotearoa New Zealand. [2] [6]
Aboriginal and Torres Strait Islander and Māori populations face higher rates of rheumatic heart disease and congenital heart disease complications compounded by access barriers, and the newborn screen is one point in the life course where equitable, culturally safe care changes outcomes. Migrant, refugee and socioeconomically disadvantaged families may have incomplete antenatal records, language needs and reduced access to postnatal review, all of which raise the chance of a late presentation. Interpreter use, clear safety-net advice and a named coordinator are the practical responses. [2]
The late-preterm and preterm infant is a special population because the pulse-oximetry thresholds behave differently. Preterm babies have a higher baseline of transitional oxygen needs, a higher false-positive rate on early screening, and a higher risk of prostaglandin-induced apnoea, and the screen is often delayed or adapted to the gestational age. The fellowship teaching is to apply the principle — find the duct-dependent lesion before it collapses — while tailoring the timing and the airway readiness to the preterm physiology. [2] [9]
Evidence, Guidelines & Regional Differences
The evidence base for newborn CCHD screening rests on three pillars. The de-Wahl Granelli Swedish prospective study of nearly forty thousand babies demonstrated that adding pulse oximetry reduced the late diagnosis and mortality of duct-dependent lesions, and it changed practice. The Ewer PulseOx test-accuracy study in the United Kingdom quantified the sensitivity and the low false-positive rate of screening at or after 24 hours. The Thangaratinam meta-analysis and the Plana Cochrane review synthesised the global data and confirmed pulse oximetry as an accurate, acceptable screen. [1] [3] [4] [5]
The Mahle scientific statement from the American Heart Association and the American Academy of Pediatrics codified the thresholds and the protocol that most programmes now use, including the right-hand and foot measurement and the 95 per cent pass, 90 to 94 per cent repeat, and below 90 per cent refer rule. The Zhao study from China demonstrated that combining pulse oximetry with clinical assessment improved detection over either alone, which is the contemporary model. The Hu study extended the case for pulse oximetry in neonatal intensive care units, where the lesions also hide. [2] [6] [12]
Regional practice differs in implementation rather than principle. Australia and Aotearoa New Zealand apply the international protocol through national and state newborn-screening guidance, with variation in whether the screen is mandated, how it is recorded, and the retrieval pathways for rural centres. The United States added CCHD screening to the recommended uniform screening panel, the United Kingdom rolled it out through NHS guidance, and Canada and parts of Europe have adopted it with local variation. The prostaglandin dosing conventions have shifted toward lower starting doses on the strength of the low-dose evidence. [2] [9]
The controversies are narrow but real. The optimal timing within the 24-to-48-hour window, the handling of a failed screen in a preterm infant, the role of repeat screening at discharge, and the integration with antenatal detection are still refined locally. The principle — that pulse oximetry finds the duct-dependent lesion the other screens miss, and that prostaglandin E1 is started before the echo — is settled. [5] [10]
Exam Pearls
The five fellowship anchors are: read pulse oximetry as a layered screen, apply the 95/90/90 thresholds without softening them, start prostaglandin E1 before the echo, separate cardiac from pulmonary cyanosis with the hyperoxia test and the bedside signs, and escalate to a cardiac centre while the duct runs. A candidate who holds these five and can recite them in order under pressure will answer almost any question the examiner builds from this topic. [2] [1]
The high-yield numbers are: congenital heart disease in about nine per thousand live births, roughly a quarter critical, antenatal ultrasound detecting about half of critical lesions, and the pulse-oximetry thresholds of 95 per cent to pass, 90 to 94 per cent to repeat, and below 90 per cent to refer. The prostaglandin E1 dose is 0.01 to 0.05 micrograms per kilogram per minute, titrated toward 0.1, with apnoea as the defining side-effect. Hold these and you hold the quantitative core of the topic. [2] [9]
The three classic traps are: waiting for the echo before prostaglandin E1, being reassured by the absence of a murmur, and attributing cyanosis to sepsis or respiratory distress while the duct closes. The discriminating bedside moves are the four-limb pulses, the single second sound, the pre-ductal and post-ductal saturations, and the four-limb blood pressure, and the diagnostic move is the echocardiogram — but the rescuing move is the prostaglandin, and it comes first. [2] [8]
The five Ts of cyanotic congenital heart disease
References
- [1]de-Wahl Granelli A, Wennergren M, Sandberg K, Mellander M, Bejlum C, Inganäs L, Eriksson M, Segerdahl N, Agren A, Ekman-Joelsson BM, Sunnegårdh J, Verdicchio M, Ostman-Smith I. Impact of pulse oximetry screening on the detection of duct dependent congenital heart disease: a Swedish prospective screening study in 39,821 newborns. BMJ, 2009.PMID 19131383
- [2]Mahle WT, Newburger JW, Matherne GP, Smith FC, Hoke TR, Koppel R, Gidding SS, Beekman RH 3rd, Grosse SD. Role of pulse oximetry in examining newborns for congenital heart disease: a scientific statement from the American Heart Association and American Academy of Pediatrics. Circulation, 2009.PMID 19581492
- [3]Ewer AK, Middleton LJ, Furmston AT, Bhoyar A, Daniels JP, Thangaratinam S, Deeks JJ, Khan KS, PulseOx Study Group. Pulse oximetry screening for congenital heart defects in newborn infants (PulseOx): a test accuracy study. Lancet, 2011.PMID 21820732
- [4]Thangaratinam S, Brown K, Zamora J, Khan KS, Ewer AK. Pulse oximetry screening for critical congenital heart defects in asymptomatic newborn babies: a systematic review and meta-analysis. Lancet, 2012.PMID 22554860
- [5]Plana MN, Zamora J, Suresh G, Fernandez-Pineda L, Thangaratinam S, Ewer AK. Pulse oximetry screening for critical congenital heart defects. Cochrane Database Syst Rev, 2018.PMID 29494750
- [6]Zhao QM, Ma XJ, Ge XL, Liu F, Yan WL, Wu L, Ye M, Liang XC, Zhang J, Gao Y, Jia B, Huang GY, Neonatal Congenital Heart Disease screening group. Pulse oximetry with clinical assessment to screen for congenital heart disease in neonates in China: a prospective study. Lancet, 2014.PMID 24768155
- [7]van der Linde D, Konings EE, Slager MA, Witsenburg M, Helbing WA, Takkenberg JJ, Roos-Hesselink JW. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol, 2011.PMID 22078432
- [8]Aykanat A, Yavuz T, Özalkaya E, Topçuoğlu S, Ovalı F, Karatekin G. Long-Term Prostaglandin E1 Infusion for Newborns with Critical Congenital Heart Disease. Pediatr Cardiol, 2016.PMID 26260095
- [9]Vari D, Xiao W, Behere S, Spurrier E, Tsuda T, Baffa JM. Low-dose prostaglandin E1 is safe and effective for critical congenital heart disease: is it time to revisit the dosing guidelines? Cardiol Young, 2021.PMID 33140712
- [10]Ewer AK. Review of pulse oximetry screening for critical congenital heart defects in newborn infants. Curr Opin Cardiol, 2013.PMID 23381095
- [11]Zhao QM, Niu C, Liu F, Wu L, Ma XJ, Huang GY. Accuracy of cardiac auscultation in detection of neonatal congenital heart disease by general paediatricians. Cardiol Young, 2019.PMID 31012400
- [12]Hu XJ, Zhao QM, Ma XJ, Yan WL, Ge XL, Jia B, Liu F, Wu L, Ye M, Huang GY. Pulse oximetry could significantly enhance the early detection of critical congenital heart disease in neonatal intensive care units. Acta Paediatr, 2016.PMID 27540721