Paeds · cardiology
Syncope and orthostatic intolerance
Also known as Syncope · Fainting · Vasovagal syncope · Orthostatic intolerance · Postural orthostatic tachycardia syndrome · POTS · Orthostatic hypotension · Reflex syncope
Fellowship guide to syncope and orthostatic intolerance in children and adolescents: transient loss of consciousness from global cerebral hypoperfusion, the benign reflex (vasovagal) and orthostatic (POTS, orthostatic hypotension) causes that dominate, the red-flag history that screens out the rare dangerous cardiac causes, an ECG for every child, orthostatic vital signs, and stepwise management from fluid and counter-pressure to urgent cardiology and sport restriction.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The idea that holds the whole topic together is the separation of benign from dangerous collapse. A faint that happens after standing too long in a hot assembly hall, with pallor and nausea beforehand and a full recovery within a minute, is almost certainly vasovagal and is safe. A faint that happens mid-sprint, or in the swimming pool, or with no warning at all, or in a child whose father died at thirty, is cardiac until you have proved otherwise. [5] [11] Everything in this page — the history, the standing test, the ECG criteria, the management — serves that single triage decision.
This page covers the definition and the mechanism-based classification, the vasovagal and orthostatic-intolerance pathophysiology, the red-flag history and the orthostatal vital signs, the investigations (and the ones to avoid), the stepwise management of benign and of cardiac syncope, and the long-term follow-up and sport advice. It links to the long-QT, hypertrophic cardiomyopathy and sudden-cardiac-death leaves for the cardiac work-up, and to the seizure leaf for the seizure-versus-syncope distinction, rather than duplicating those pathways. [6] [11]
Overview & Definition
Syncope is a transient loss of consciousness — "transient" means it comes on fast and leaves fast — caused by a temporary failure of blood flow to the whole brain, with rapid, spontaneous and complete recovery. [1] The key words are global cerebral hypoperfusion: the whole brain is briefly starved, which is why recovery is complete and quick. A focal problem (a stroke) does not behave this way, and a brain that has seized does not recover in seconds.
A simple way to think about it at the bedside: the child was upright, the blood drained to the legs, the heart could not push enough back up to the brain, the brain switched off for a few seconds, the child fell, gravity and the supine posture refilled the heart, and the child woke up. That is the common pathway for almost every faint, whatever the trigger. [6]
Before going further, separate three terms the examiner uses interchangeably but should not. Syncope is the actual loss of consciousness. Presyncope is the warning — the lightheaded, nauseated, vision-greying feeling — without actually passing out; it shares the same mechanism and work-up as syncope. [2] Orthostatic intolerance is the broader basket of symptoms (lightheadedness, palpitations, nausea, fatigue, brain fog) that appear on standing and ease on lying down; syncope is only one possible end-point of it, and many adolescents with orthostatic intolerance never actually faint. [8] [9]
Why this matters clinically: most children you see will have presyncope or orthostatic intolerance rather than a true collapse, and the same triage logic — benign autonomic versus dangerous cardiac — applies to all of them. [9]
Classification
Sort syncope by the mechanism that drops the cerebral blood flow, because the mechanism tells you both the prognosis and the management. The figure below splits the causes into three mechanism-based groups. [1] [6]
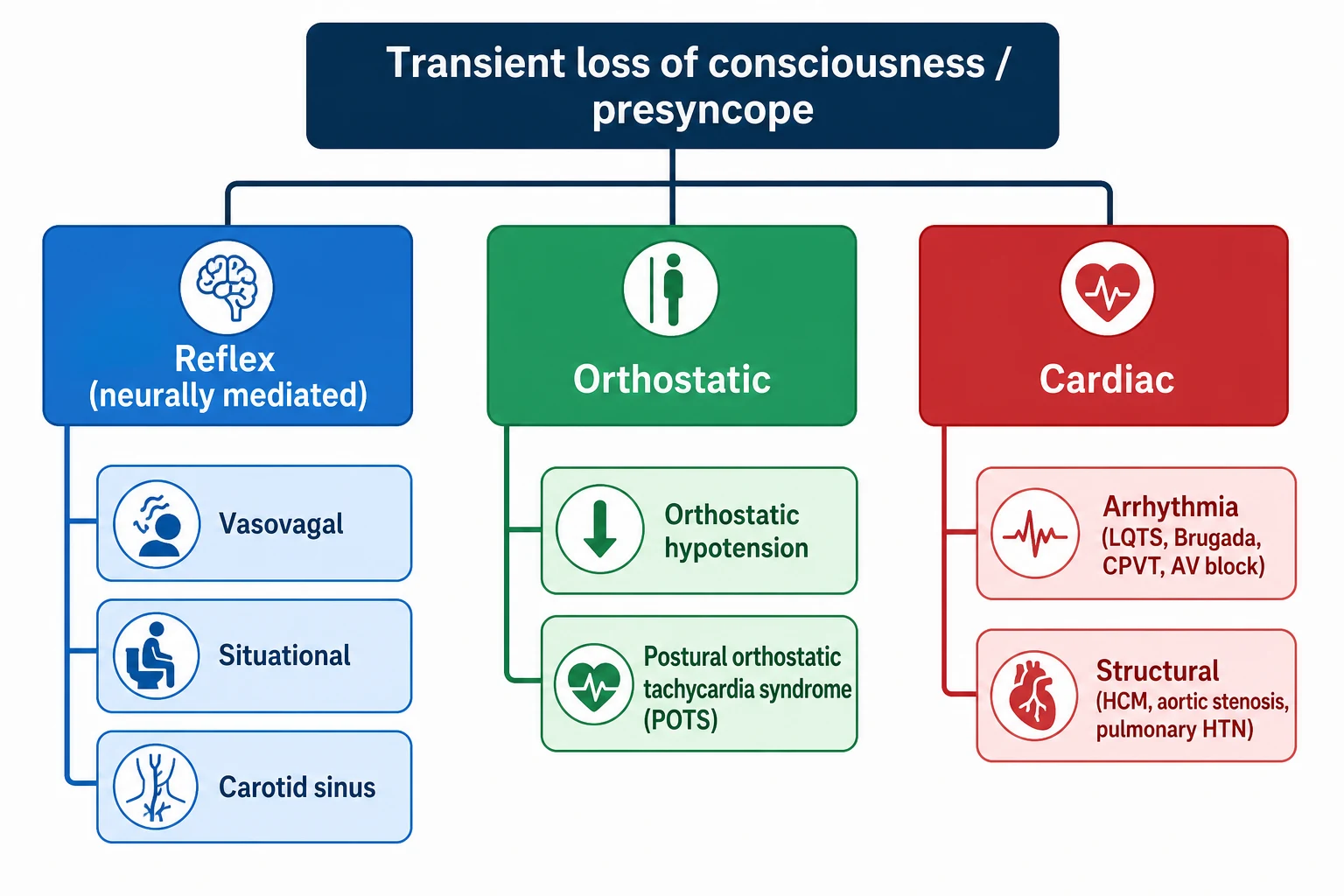
Reflex (neurally mediated) — commonest, benign
- Vasovagal syncope: standing, heat, emotion, venepuncture; clear prodrome; rapid full recovery
- Situational syncope: venepuncture, micturition, defaecation, cough, hair-grooming
- Driven by the Bezold-Jarisch reflex: vagal output rises, heart rate and vascular tone fall together
- Managed with reassurance, fluid, salt, counter-pressure, lying down at the prodrome
Orthostatic — chronic, usually adolescent girls
- Orthostatic hypotension: blood pressure falls ≥20 mmHg systolic on standing within 3 minutes
- POTS: heart rate rises ≥40 bpm in children (≥30 in adolescents) without a blood-pressure drop
- Daily lightheadedness, palpitations, fatigue, brain fog; worse standing, eased lying down
- Managed with hydration, salt, reconditioning, compression; medications second-line
Cardiac — uncommon, dangerous
- Arrhythmia: long-QT, Brugada, CPVT, WPW, congenital complete heart block
- Structural: hypertrophic cardiomyopathy, aortic stenosis, pulmonary hypertension
- Exertional, supine, no-prodrome syncope; palpitations at collapse; family history of sudden death
- Urgent cardiology, ECG, echo, exercise test; sport restriction; treat the underlying lesion
The proportions are what make the triage safe. Reflex (vasovagal) syncope is by far the commonest cause of collapse in young people. Orthostatic intolerance and POTS are common in adolescent girls. Cardiac syncope is uncommon — but it is the cause that can kill, and the one you must not miss. [3] [5]
Epidemiology & Risk Factors
Syncope is extremely common in young people. A large proportion of children and adolescents will faint at least once, and the incidence peaks in adolescence, especially in girls. [1] [3] A teenager who has fainted in assembly is a normal clinical event, not a crisis — provided the screen is clean.
Vasovagal syncope is the single commonest cause. The triggers are the familiar ones: standing for a long time, a hot or crowded room, hunger, the sight of blood, a needle, a strong emotion. A family history of fainting is common and is reassuring, not worrying. [6]
POTS sits at the other end of the autonomic spectrum. It predominantly affects adolescent females, and it often begins after a viral illness, an operation, a growth spurt, or a period of bed rest and deconditioning. It is commonly associated with joint hypermobility and hypermobile Ehlers-Danlos syndrome. [9] [10]
The cardiac causes are individually rare but collectively important: long-QT syndrome, hypertrophic cardiomyopathy, arrhythmogenic cardiomyopathy, catecholaminergic polymorphic ventricular tachycardia (CPVT), Brugada syndrome, Wolff-Parkinson-White, and congenital complete heart block. [11] [5] These are the diagnoses you are screening for every time you take a fainting history.
Pathophysiology
Every syncope ends the same way: global cerebral blood flow falls below the level needed to keep consciousness. What differs is the mechanism that drops the flow. [1]
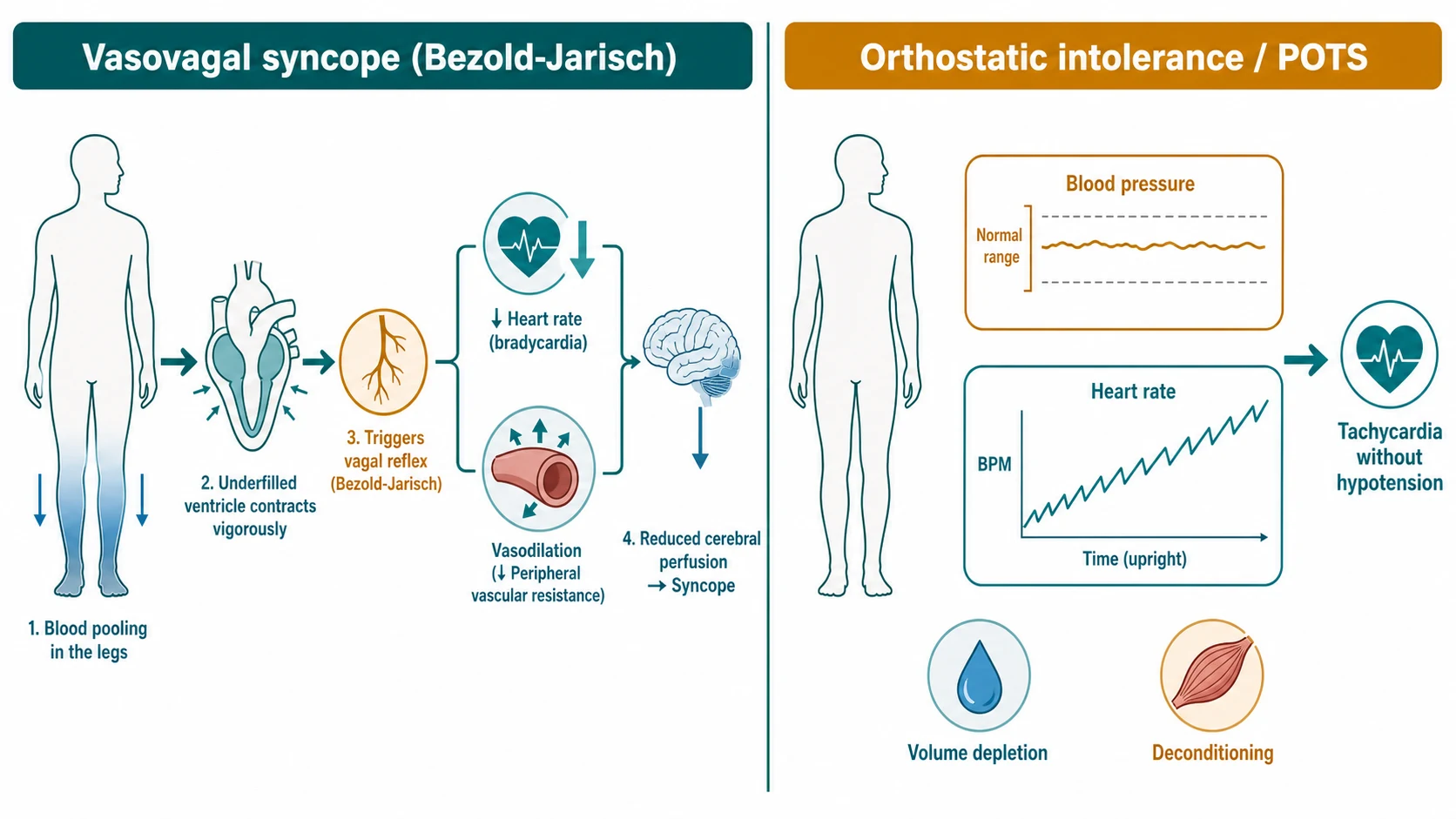
The vasovagal (Bezold-Jarisch) reflex is the mechanism behind the common faint. The reasoning chain runs like this. The child stands; blood pools in the legs and the splanchnic bed; venous return drops; the ventricle is underfilled but contracts hard against an almost empty chamber; that vigorous contraction fires the left-ventricular mechanoreceptors (the vagal C-fibres that normally sense high filling pressure). The reflex read this wrongly as high pressure and switch off the sympathetic drive and switch on the vagus. [6] [7] The result is the paradox of a faint: the heart slows and the blood vessels open at the same time, so pressure collapses. This is why the prodrome — pallor, nausea, sweating, tunnel vision, warmth — is the autonomic system warning you the pressure is going. [2] It is also why lying down immediately aborts the episode: gravity refills the heart, the reflex switches off, and pressure returns.
Classic orthostatic hypotension is a different and simpler failure. On standing the body should constrict the veins and arteries to hold pressure against gravity; in orthostatic hypotension that vasoconstrictor response fails, and the blood pressure simply drops. The threshold to call it is a systolic fall of at least twenty millimetres of mercury, or a diastolic fall of at least ten, within three minutes of standing, with symptoms. [7]
POTS is the one that confuses candidates. On standing the blood pressure does not fall — instead the heart rate climbs far too much. The standing heart rate rises by at least forty beats per minute in children (at least thirty in adolescents and adults, or to an absolute rate above one hundred and twenty), sustained over the first ten minutes of standing, with symptoms but no blood-pressure drop. [7] [8] The mechanism is a combination of peripheral venous pooling, relative hypovolaemia, deconditioning, and sometimes a small-fibre neuropathy; the heart races to compensate for blood that will not return from the legs. [8]
Cardiac syncope is the abrupt mechanical failure of cardiac output. A tachyarrhythmia (ventricular tachycardia in long-QT or CPVT) or a bradyarrhythmia (complete heart block) stops forward flow dead, or a structural obstruction (hypertrophic cardiomyopathy, aortic stenosis, pulmonary hypertension) prevents the heart generating enough output — especially when exertion demands more. The onset is sudden, there is often no prodrome, and the collapse is dangerous. [5] [11]
Clinical Presentation
The history is the single most useful diagnostic tool in paediatric syncope, and it resolves the cause in most children on its own. [2] Get the story right and the rest follows.
The classic vasovagal episode has a recognisable shape. There is a clear precipitant — prolonged standing, heat, a crowded room, hunger, the sight of blood, a needle, a strong emotion. There is a prodrome: the child goes pale, feels nauseated or hot, sweats, the vision dims or tunnels, hearing fades. Then a brief loss of consciousness with a slump, pallor, occasionally a few brief myoclonic jerks (see the pitfall below). Recovery is rapid and complete within seconds to a couple of minutes once the child is flat, though nausea and fatigue can linger. [1] [2]
POTS presents differently — not as discrete faints but as a chronic daily orthostatic syndrome in an adolescent (often female). Lightheadedness, palpitations, exercise intolerance, fatigue, brain fog, nausea and headache, worse on standing and in the morning, eased by lying down. There is often a viral trigger, a growth spurt, or a period of deconditioning beforehand, and joint hypermobility is common. [9] [8]
Now the red-flag features that point to a cardiac cause. Learn this list cold, because it is the heart of the topic. [5] [2]
The red flags matter because the cardiac causes are clinically silent between events. A child with long-QT syndrome looks completely well and has a normal examination until the moment the heart goes into torsades. The only clues are the trigger (exertion, noise, swimming, fright), the absent prodrome, and the family history — and the ECG. [11]
In the younger child, remember breath-holding spells as a distinct entity. A cyanotic or pallid breath-holding spell in an infant or toddler can produce a brief loss of consciousness, and you must distinguish it from syncope and from seizure. [12]
Finally, recognise the seizure mimic. A true seizure leaves postictal confusion and drowsiness lasting minutes to hours, lateral tongue biting, incontinence, a prolonged tonic-clonic phase, and a slow, incomplete recovery. Syncope recovers in seconds and the child is back to normal almost immediately. [1] [12]
Differential Diagnosis
The first fork is the most important: is this syncope at all, or a mimic? Seizure, breath-holding, hypoglycaemia, hyperventilation and conversion disorder can all look like a faint. Syncope is defined by the rapid, complete recovery; anything that leaves a child drowsy or confused for more than a minute or two is not simple syncope. [1] [12]
Within true syncope, the fork is benign autonomic versus dangerous cardiac. A clear precipitant, a typical prodrome, an upright posture, a rapid recovery and a clean family history point to vasovagal. Exertional, supine, no-prodrome collapse with palpitations or a family history of sudden death points to cardiac and demands cardiology. [5]
Distinguish the three benign autonomic patterns with the standing test. Vasovagal syncope is episodic with a prodrome. Orthostatic hypotension shows a blood-pressure fall on standing. POTS shows a sustained heart-rate rise without a blood-pressure fall. [7] [9]
Always keep the cardiac mimics on the list for the dangerous collapse, because each has a specific treatment: long-QT syndrome, hypertrophic cardiomyopathy, aortic stenosis, pulmonary hypertension, arrhythmogenic cardiomyopathy, Brugada syndrome, CPVT, Wolff-Parkinson-White, and congenital complete heart block. [11] [5]
Clinical & Bedside Assessment
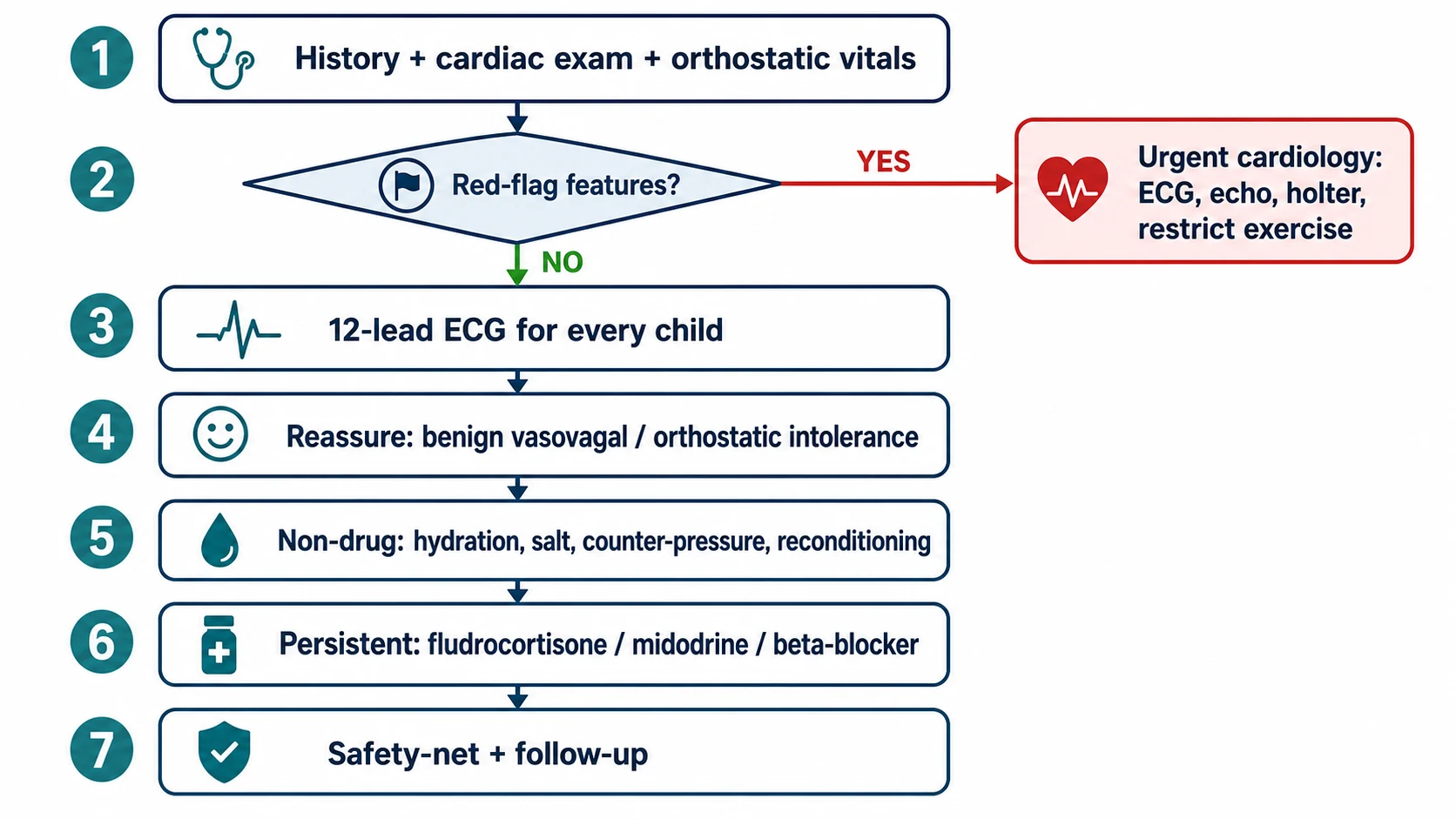
Start with the history, because in paediatric syncope it resolves more than the examination ever will. Establish the circumstances (where, standing or supine, exertional or not), the prodrome (pallor, nausea, visual change, palpitations), the posture, the recovery (rapid and complete, or slow and confused), and the family history (sudden death, drowning, arrhythmia, fainting). [2]
Then do the orthostatic vital signs — the standing test. Lay the child flat for five to ten minutes and record the heart rate and blood pressure. Then stand the child up and repeat the measurements at one, three, five and ten minutes (or use continuous monitoring). Watch the numbers move. A systolic blood-pressure fall of at least twenty millimetres of mercury (or diastolic at least ten) within three minutes is orthostatic hypotension. A heart-rate rise of at least forty beats per minute in a child (at least thirty in an adolescent) sustained over ten minutes, with symptoms but no blood-pressure drop, is POTS. [7] [9]
Do the cardiac examination next. Feel all four limb pulses and measure four-limb blood pressures (to exclude coarctation). Auscultate for the murmur of hypertrophic cardiomyopathy or a left-heart obstruction. Look for the stigmata of Marfan syndrome and joint hypermobility. [1]
The red-flag history screen is the decisive move. Exertional syncope, supine syncope, syncope in water, syncope from noise or fright, no prodrome, chest pain, palpitations at collapse, a family history of sudden death under about fifty, and recurrent syncope with injury — any one of these mandates cardiac investigation. [5]
Avoid the common technique error of diagnosing a seizure from the brief myoclonic jerks that accompany a vasovagal collapse. These are cerebral-hypoperfusion myoclonus, not epilepsy; they settle within seconds and the child recovers fully. Starting antiepileptics here is a recognised misadventure. [1]
Investigations
Every child presenting with syncope gets a 12-lead ECG. This is non-negotiable. The ECG is cheap, safe, painless and detects the dangerous arrhythmia substrate that may be completely silent on history and examination. [1] [5] No child is discharged after a collapse without an ECG read and signed off.
What the syncope ECG must exclude
On the ECG, measure the corrected QT interval (Bazett correction) and look for the long-QT thresholds: borderline around four hundred and fifty milliseconds in males and four hundred and sixty in females, definite at four hundred and eighty. [11] Look for the delta wave and short PR of Wolff-Parkinson-White, the coved ST elevation of a Brugada pattern in V1 to V3, and any heart block or pathologic QRS widening. Deep T-wave inversions or striking voltage raise hypertrophic cardiomyopathy. [6]
For the child with a clear vasovagal history, a clean family history, a normal examination and a normal ECG, stop investigating. Routine blood tests (glucose, electrolytes, full blood count) and neuroimaging (CT, MRI) are not indicated, and ordering them is a recognised source of low-value care. [1] [3]
Order an echocardiogram when any cardiac red flag is present, when the ECG is abnormal, when there is a murmur suggesting obstruction, when syncope is exertional, or when the family history is positive for cardiomyopathy or sudden death. [6]
Reserve ambulatory ECG monitoring (Holter or an event recorder) and exercise stress testing for recurrent unexplained syncope, a suspected arrhythmia, exertional collapse (the exercise test is specifically useful here), or a high-risk family history. [5]
The head-up tilt test is not a first-line investigation. It is reserved for a small group with recurrent unexplained syncope in whom the diagnosis remains unclear after a careful history and basic testing. [7]
Management — Resuscitation
If you witness the collapse, lay the child flat and elevate the legs to restore venous return and cerebral perfusion, protect the airway, and confirm rapid full recovery. Most vasovagal episodes resolve within seconds once the child is supine. [1]
Obtain the ECG before discharge for any child who has presented with syncope, because the dangerous causes may be silent. [5]
A child with a cardiac cause, an abnormal ECG, exertional syncope, or a high-risk family history is not sent home. They need urgent cardiology referral, admission for monitoring, and exercise restriction until a cardiac cause is excluded. [6] [5]
Likewise, a child who has not fully recovered, who has chest pain, dyspnoea, a new murmur, an arrhythmia, or an abnormal ECG, stays in hospital and is managed as a potentially cardiac collapse until proven otherwise. [5]
Management — Definitive & Stepwise
The first-line management of vasovagal syncope is non-pharmacological. Educate and reassure the child and family — the single most therapeutic intervention is the explanation that this is benign and not a seizure or a heart problem. Avoid triggers and dehydration. Increase fluid intake (around two to three litres per day for an adolescent) and dietary salt. Teach the child to recognise the prodrome and to apply physical counter-pressure manoeuvres (leg-crossing, hand-grip, arm-tensing) at the first warning — and above all to lie down immediately, which is the most reliable way to abort an episode. [7] [2]
Pharmacotherapy is reserved for recurrent refractory syncope that impairs quality of life despite these measures. Options include fludrocortisone, midodrine and a beta-blocker; the evidence for drug therapy in children is limited, and it is not routine. [6] [4] Metoprolol has been specifically studied in paediatric vasovagal syncope with a multivariable predictive model to identify responders, which supports selective rather than universal beta-blocker use. [13]
POTS needs a more sustained programme. The pillars are aggressive hydration (two to three litres daily), salt supplementation (up to around ten grams per day in adolescents), a structured graduated exercise and reconditioning programme (the most evidence-based component, because deconditioning perpetuates the tachycardia), compression garments, and head-up sleeping. Medications — a beta-blocker, midodrine or fludrocortisone — are second-line. [8] [9]
Cardiac syncope is managed by treating the underlying arrhythmia or structural lesion. That means beta-blockade or an implantable cardioverter-defibrillator for high-risk channelopathies and cardiomyopathies, catheter ablation for an accessory pathway, and surgical or catheter relief of a structural obstruction — and competitive-sport restriction throughout. [11]
Every patient with benign syncope gets a clear safety-net and follow-up. Tell the family the warning signs that should bring them back (exertional syncope, chest pain, palpitations, a family event), agree a plan for driving and swimming once recovered, and review if the episodes change in character. [1]
Specific Subtypes & Scenarios
Classic vasovagal syncope in the adolescent is the scenario you will see most. A precipitant, a prodrome, a brief collapse and a rapid full recovery. Manage with reassurance and the non-pharmacological measures above. [1]
POTS in the adolescent female is the chronic orthostatic syndrome: daily lightheadedness and palpitations, a post-viral or post-growth-spurt onset, joint hypermobility, and functional limitation. Manage with hydration, salt, reconditioning and compression, and set realistic expectations — improvement comes over months. [9] [10]
Exertional syncope is the cardiac red flag that must never be dismissed. Syncope during or immediately after sport demands exclusion of hypertrophic cardiomyopathy, long-QT syndrome, CPVT, arrhythmogenic cardiomyopathy and aortic stenosis before any return to play. [5]
Syncope with a family history of sudden death is long-QT syndrome or another inherited channelopathy until proved otherwise. Take the ECG, screen the family, and refer to cardiology for genetic and clinical evaluation. [11]
Breath-holding spells in the infant or toddler — cyanotic or pallid — are a benign mimic of syncope. Reassure the family, check a full blood count and ferritin for iron-deficiency anaemia in pallid spells, and distinguish the spell from seizure and cardiac syncope. [12]
Complications & Pitfalls
The principal pitfall is missing a cardiac cause by assuming that every paediatric syncope is vasovagal. Exertional, supine and no-prodrome syncope with a family history of sudden death must be investigated, not reassured away. [5]
The opposite pitfall is over-investigating a clear vasovagal presentation with neuroimaging and routine bloods, which is low-value and does not improve outcomes when the ECG and history are reassuring. [3]
A third pitfall is mislabelling the brief myoclonic jerks of a vasovagal collapse as a seizure and starting antiepileptics. The jerks settle in seconds and the child recovers fully; treat the history, not the twitch. [1]
The complications of recurrent syncope are injury from the collapse and impaired quality of life and school attendance. The complication of untreated POTS is deconditioning and functional decline — the less the child moves, the worse the tachycardia, and the cycle deepens. [9]
The complication of a missed cardiac cause is sudden cardiac death, especially during exertion. That is the single most important preventable harm in this topic, and the reason the screen exists. [5] [11]
Prognosis & Disposition
Vasovagal syncope has an excellent prognosis. It is benign, it often recurs, but it is not life-threatening, and it usually improves with education, hydration and counter-pressure. [1]
POTS in adolescents has a chronic relapsing course but a favourable long-term outlook with a structured reconditioning programme; many young people improve substantially over months to a few years. [9]
Cardiac syncope carries a risk of sudden death set by the underlying lesion. Prognosis depends on prompt diagnosis and treatment — medication, ablation or a device — and on sport restriction. [11]
The disposition is where the triage decision lands. A clear vasovagal syncope with a normal ECG and no red flags is discharged with safety-netting and primary-care follow-up. [1] Syncope with a cardiac red flag, an abnormal ECG, or an uncertain cause is admitted or referred urgently to cardiology for monitoring and work-up. [5]
Special Populations
Adolescents are the peak group for both vasovagal syncope and POTS. They carry the added risks of dehydration, dieting, menstrual blood loss, rapid growth and competitive sport — address the modifiable ones. [1] [9]
The athletic child or adolescent is the group in whom exertional syncope must be treated as cardiac until excluded. Sport is restricted pending evaluation, because sudden cardiac death in the young athlete is often preceded by exertional warning symptoms that were dismissed. [5]
The child with joint hypermobility or hypermobile Ehlers-Danlos syndrome is predisposed to POTS and dysautonomia, often alongside chronic pain and fatigue, and needs an integrated autonomic and musculoskeletal approach. [10]
The child with a family history of sudden cardiac death or a known channelopathy is high-risk and needs ECG screening, family evaluation and cardiology-led surveillance. [11]
The rural or remote child with syncope can often be managed locally when the ECG is normal and the history is clearly vasovagal, with telehealth support; a cardiac red flag requires telehealth-supported urgent referral and safe retrieval. [1]
Evidence, Guidelines & Regional Differences
The general paediatric syncope evidence rests on the review of Anderson (2016), the history-focused review of Yeom (2023), the systematic review of Zavala (2020) and the cardiology-clinics review of Kanjwal (2015). These anchor the diagnostic approach and the benign-versus-dangerous distinction. [1] [2] [3] [6]
The POTS and orthostatic-intolerance evidence rests on the Heart Rhythm Society expert consensus (Sheldon 2015), the NIH expert consensus (Vernino 2021) and the adolescent-focused review of Soroken (2022); together they set the diagnostic criteria and the stepwise management. [7] [8] [9] The recent Chinese guidance for neurally mediated syncope in children and adolescents, revised in 2024 (Wang), gives an up-to-date operational pathway. [4]
The selective pharmacotherapy evidence comes from the metoprolol predictive model of Cui (2025). [13] The hEDS–POTS link is set out by Kucharik (2020), the long-QT review by Goldenberg (2008), and the loss-of-consciousness differential — including breath-holding spells — by Villafane (2021). [10] [11] [12]
The main controversies are the role and threshold of the head-up tilt test in children; the place of pharmacotherapy (beta-blocker, midodrine, fludrocortisone) versus non-pharmacological measures; the optimal intensity of the POTS reconditioning programme; and the threshold for sport restriction in borderline channelopathies. [7] [8] [11]
Exam Pearls
Hold the one-sentence viva: syncope is transient loss of consciousness from global cerebral hypoperfusion; the vast majority in young people is benign vasovagal; the one job that matters is to screen out the cardiac causes with the history, the orthostatic vital signs and an ECG on every child. [1] [5]
The red-flag screen to quote verbatim: exertional, supine or swimming syncope; syncope from noise or fright; no prodrome; chest pain; palpitations at collapse; family history of sudden death under about fifty; recurrent syncope with injury. [2] [5]
The orthostatic thresholds to know to the number: orthostatic hypotension is a systolic blood-pressure fall of at least twenty millimetres of mercury (or diastolic at least ten) within three minutes of standing; POTS is a heart-rate rise of at least forty beats per minute in children (at least thirty in adolescents, or an absolute rate above one hundred and twenty) over ten minutes of standing, without a blood-pressure drop. [7]
The management pairs: vasovagal syncope gets fluid, salt, counter-pressure and lying down at the prodrome; POTS gets hydration, salt, reconditioning and compression; cardiac syncope gets urgent cardiology, sport restriction and treatment of the lesion. [8] [11]
The mimic pairs: seizure has postictal confusion, lateral tongue biting and incontinence; breath-holding spells occur in infants and toddlers; and the brief myoclonic jerks of a vasovagal collapse are not epilepsy. [1] [12]
References
- [1]Anderson JB; Czosek RJ; Knilans TK; et al The Evaluation and Management of Pediatric Syncope. Pediatr Neurol, 2016.PMID 26706050
- [2]Yeom JS Pediatric syncope: pearls and pitfalls in history taking. Clin Exp Pediatr, 2023.PMID 36789491
- [3]Zavala R; Moffa M; Stahlschmidt J; et al Pediatric Syncope: A Systematic Review. Pediatr Emerg Care, 2020.PMID 32530839
- [4]Wang C; Wu L; Liao Z; et al Guidelines for the diagnosis and treatment of neurally mediated syncope in children and adolescents (revised 2024). World J Pediatr, 2024.PMID 39110332
- [5]Schunk PC Pediatric Syncope: High-Risk Conditions and Reasonable Approach. Emerg Med Clin North Am, 2018.PMID 29622324
- [6]Kanjwal K; Calkins H Syncope in Children and Adolescents. Cardiol Clin, 2015.PMID 26115826
- [7]Sheldon RS; Grubb BP; Olshansky B; et al 2015 heart rhythm society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm, 2015.PMID 25980576
- [8]Vernino S; Stiles LE; Low P; et al Postural orthostatic tachycardia syndrome (POTS): State of the science and clinical care from a 2019 National Institutes of Health Expert Consensus Meeting - Part 1. Auton Neurosci, 2021.PMID 34144933
- [9]Soroken C; Lesavre N; Tard C; et al Postural tachycardia syndrome among adolescents. Arch Pediatr, 2022.PMID 35523634
- [10]Kucharik AH; Maurer K The Relationship Between Hypermobile Ehlers-Danlos Syndrome (hEDS), Postural Orthostatic Tachycardia Syndrome (POTS), and Mast Cell Activation Syndrome (MCAS). Clin Rev Allergy Immunol, 2020.PMID 31267471
- [11]Goldenberg I; Moss AJ; Zareba W Long QT syndrome. J Am Coll Cardiol, 2008.PMID 18549912
- [12]Villafane J; FE; Baffa F; et al Loss of Consciousness in the Young Child. Pediatr Cardiol, 2021.PMID 33388850
- [13]Cui Y; Qin H; Zhang L; et al Multivariate predictive model of the therapeutic effects of metoprolol in paediatric vasovagal syncope: a multi-centre study. EBioMedicine, 2025.PMID 39946834